
Current Trends in Inpatient Care and In-Hospital Mortality of Cholangiocarcinoma in Germany: A Systematic Analysis between 2010 and 2019




Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Eligibility Criteria and Variables
2.3. Statistical Analysis
3. Results
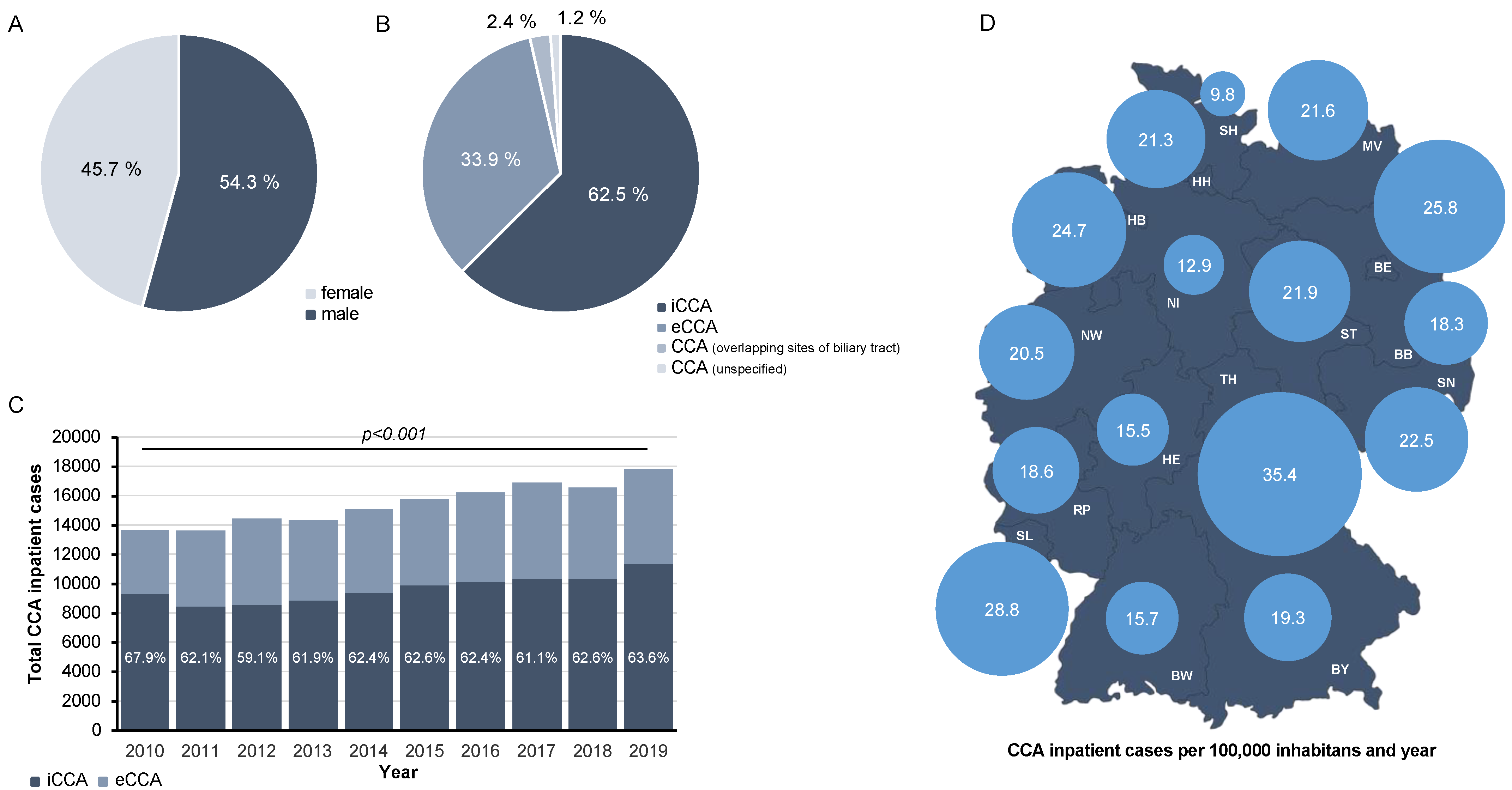
3.1. The Total Number of Inpatient CCA Cases in Germany Is Increasing between 2010 and 2019
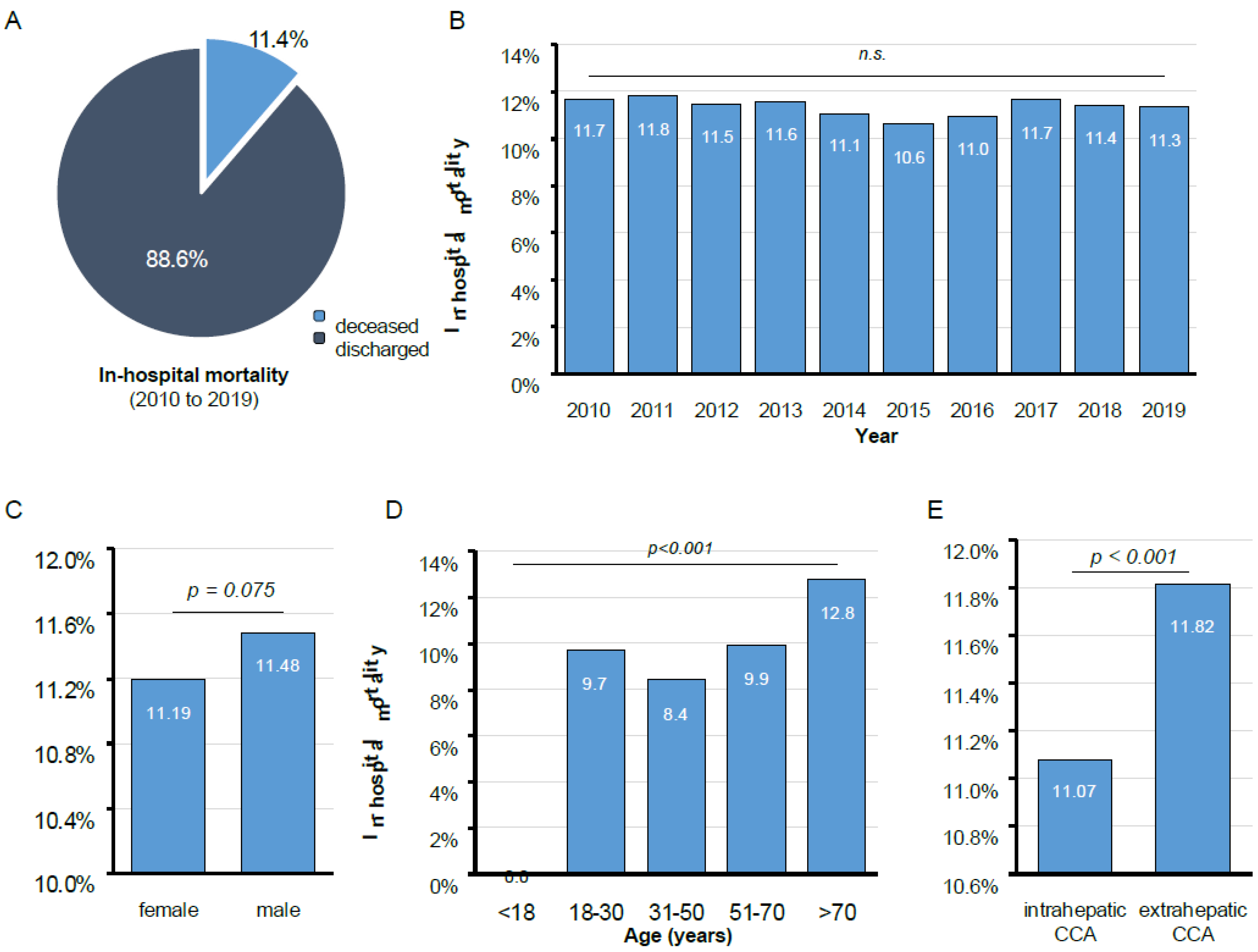
3.2. In-Hospital Mortality of CCA in Germany Is Associated with Patients’ Age and the Anatomical Localization of CCA
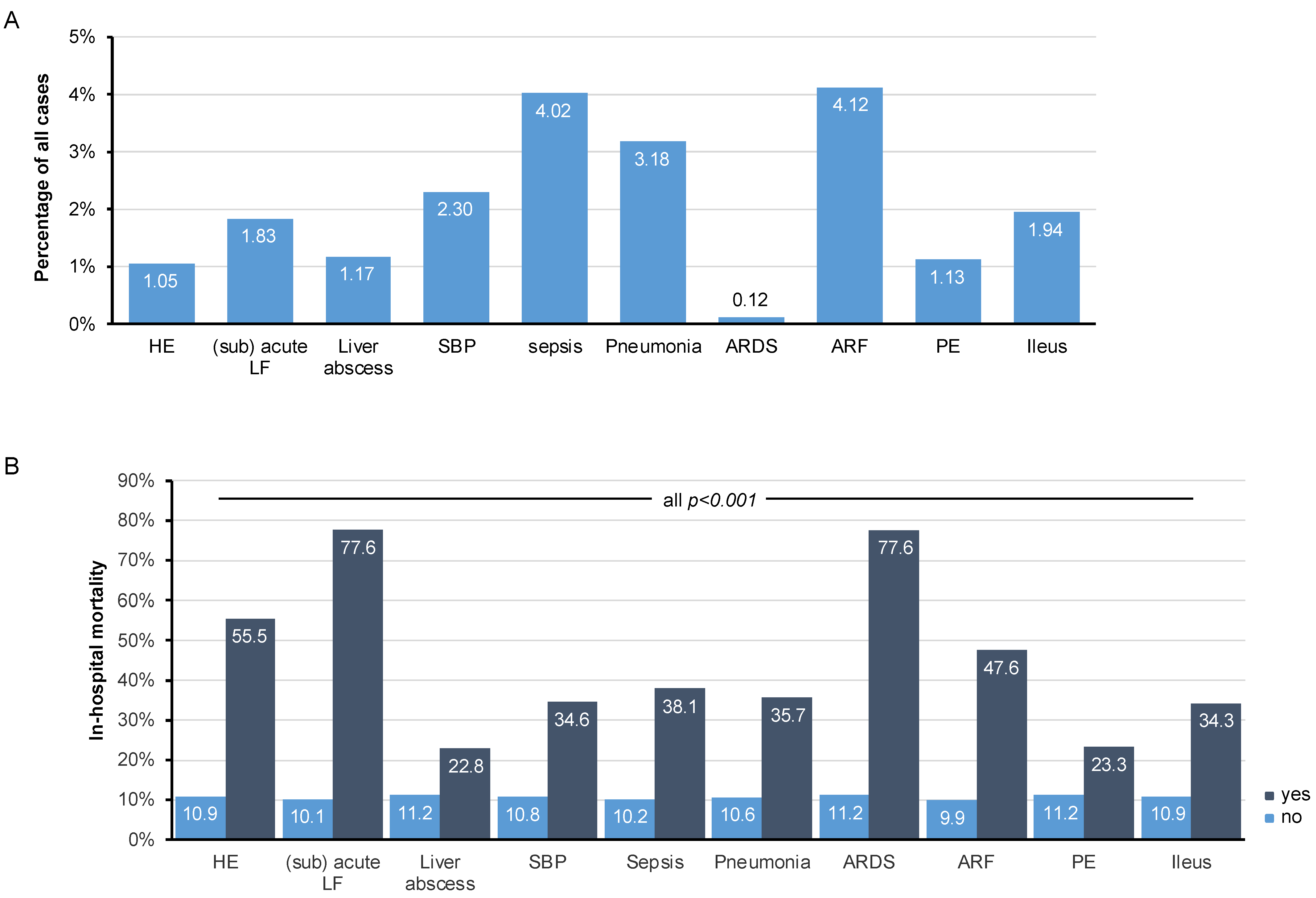
3.3. Pulmonary, Renal, and Infectious Clinical Complications Increase In-Hospital Mortality of CCA
3.4. Chemotherapy Represents the Most Common Treatment Modality for Inpatient CCA Cases in Germany
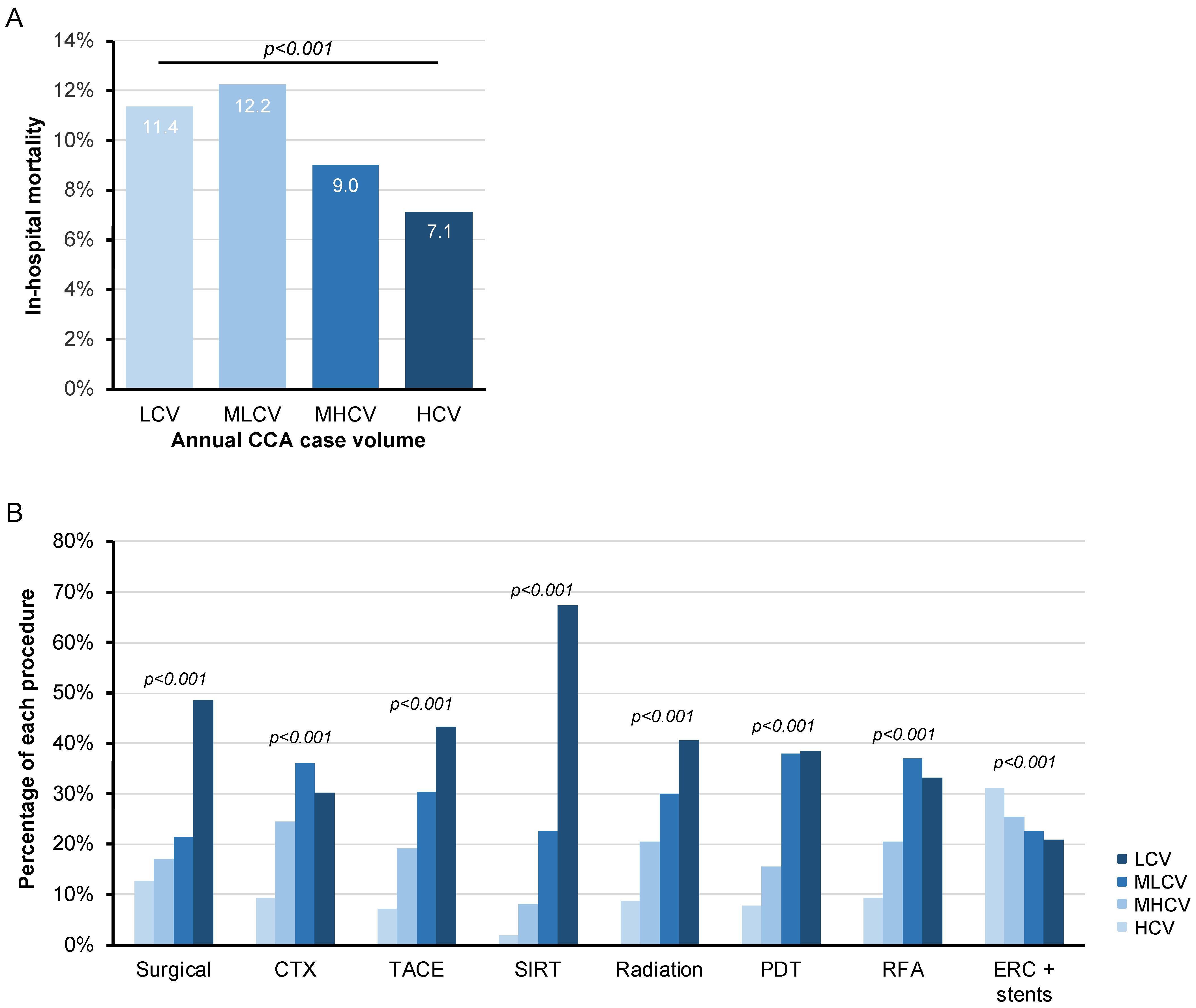
3.5. In-Hospital Mortality Is Significantly Higher among CCA Patients Treated at Low Annual Case Volume Centres
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.Y.; Zhu, A.X. Biliary Tract Cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef]
- Sarcognato, S.; Sacchi, D.; Fassan, M.; Fabris, L.; Cadamuro, M.; Zanus, G.; Cataldo, I.; Capelli, P.; Baciorri, F.; Cacciatore, M.; et al. Cholangiocarcinoma. Pathologica 2021, 113, 158–169. [Google Scholar] [CrossRef] [PubMed]
- Moazzami, B.; Majidzadeh, A.K.; Dooghaie-Moghadam, A.; Eslami, P.; Razavi-Khorasani, N.; Iravani, S.; Khoshdel, A.; Shahi, F.; Dashti, H.; Mehrvar, A.; et al. Cholangiocarcinoma: State of the Art. J. Gastrointest. Cancer 2020, 51, 774–781. [Google Scholar] [CrossRef] [PubMed]
- Renzulli, M.; Ramai, D.; Singh, J.; Sinha, S.; Brandi, N.; Ierardi, A.M.; Albertini, E.; Sacco, R.; Facciorusso, A.; Golfieri, R. Locoregional Treatments in Cholangiocarcinoma and Combined Hepatocellular Cholangiocarcinoma. Cancers 2021, 13, 3336. [Google Scholar] [CrossRef] [PubMed]
- Taylor, A.C.; Maddirela, D.; White, S.B. Role of Radioembolization for Biliary Tract and Primary Liver Cancer. Surg. Oncol. Clin. N. Am. 2019, 28, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, A.; Cusmai, A.; Ricci, A.D.; Brandi, G.; Palmiotti, G. Combination Systemic Therapies with Immune Checkpoint Inhibitors in Biliary Tract Cancer: Effective but Not Enough? Expert Rev. Gastroenterol. Hepatol. 2022, 16, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next Horizon in Mechanisms and Management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef] [PubMed]
- Brindley, P.J.; Bachini, M.; Ilyas, S.I.; Khan, S.A.; Loukas, A.; Sirica, A.E.; Teh, B.T.; Wongkham, S.; Gores, G.J. Cholangiocarcinoma. Nat. Rev. Dis. Primers 2021, 7, 65. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.A.; Emadossadaty, S.; Ladep, N.G.; Thomas, H.C.; Elliott, P.; Taylor-Robinson, S.D.; Toledano, M.B. Rising Trends in Cholangiocarcinoma: Is the ICD Classification System Misleading Us? J. Hepatol. 2012, 56, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A. The 2019 WHO Classification of Tumours of the Digestive System. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaller, K.; Kahnert, S.; Mons, U. Alkoholatlas; Deutsches Krebsforschungszentrum: Heidelberg, Germany, 2017; ISBN 9783958533349. [Google Scholar]
- Bridgewater, J.; Fletcher, P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Long-Term Outcomes and Exploratory Analyses of the Randomized Phase III BILCAP Study. J. Clin. Oncol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Lamarca, A.; Palmer, D.H.; Wasan, H.S.; Ross, P.J.; Ma, Y.T.; Arora, A.; Falk, S.; Gillmore, R.; Wadsley, J.; Patel, K.; et al. Second-Line FOLFOX Chemotherapy versus Active Symptom Control for Advanced Biliary Tract Cancer (ABC-06): A Phase 3, Open-Label, Randomised, Controlled Trial. Lancet Oncol. 2021, 22, 690–701. [Google Scholar] [CrossRef]
- Rizzo, A.; Cusmai, A.; Giovannelli, F.; Acquafredda, S.; Rinaldi, L.; Misino, A.; Palmiotti, G. Fluoropyrimidine-Based Doublet Chemotherapy as Second-Line Treatment for Advanced Biliary Tract Cancer: A Meta-Analysis of ABC-06 and NIFTY. Expert Rev. Gastroenterol. Hepatol. 2022, 16, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Lamarca, A.; Edeline, J.; Goyal, L. How I Treat Biliary Tract Cancer. ESMO Open 2022, 7, 100378. [Google Scholar] [CrossRef] [PubMed]
- Bertuccio, P.; Malvezzi, M.; Carioli, G.; Hashim, D.; Boffetta, P.; El-Serag, H.B.; la Vecchia, C.; Negri, E. Global Trends in Mortality from Intrahepatic and Extrahepatic Cholangiocarcinoma. J. Hepatol. 2019, 71, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Bertuccio, P.; Bosetti, C.; Levi, F.; Decarli, A.; Negri, E.; la Vecchia, C. A Comparison of Trends in Mortality from Primary Liver Cancer and Intrahepatic Cholangiocarcinoma in Europe. Ann. Oncol. 2013, 24, 1667–1674. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Rein, L.; Clarke, C.; Mogal, H.; Tsai, S.; Christians, K.K.; Gamblin, T.C. Comparison of Overall Survival in Gallbladder Carcinoma at Academic versus Community Cancer Centers: An Analysis of the National Cancer Data Base. J. Surg. Oncol. 2020, 122, 176–182. [Google Scholar] [CrossRef] [PubMed]
- Filmann, N.; Walter, D.; Schadde, E.; Bruns, C.; Keck, T.; Lang, H.; Oldhafer, K.; Schlitt, H.J.; Schön, M.R.; Herrmann, E.; et al. Mortality after Liver Surgery in Germany. Br. J. Surg. 2019, 106, 1523–1529. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Population | |
|---|---|
| Total number of CCA cases | 154,515 |
| In-hospital death (total) | 17,540 |
| In-hospital mortality rate (%) | 11.35 |
| Sex (total, (%)) | |
| male | 83,841 (54.26) |
| female | 70,674 (45.74) |
| Age (Mean and SD) | 69.64 (11.15) |
| Age group (total, (%)) | |
| 0–17 Years | 21 (0.01) |
| 18–30 years | 288 (0.19) |
| 31–50 years | 8680 (5.62) |
| 51–70 years | 64,469 (41.72) |
| >70 years | 81,057 (52.46) |
| Federal state (total, (%)) | |
| Baden-Württemberg | 16,923 (10.95) |
| Bavaria | 24,584 (15.91) |
| Berlin | 8947 (5.79) |
| Brandenburg | 4521 (2.93) |
| Bremen | 1645 (1.06) |
| Hamburg | 3763 (2.44) |
| Hesse | 9199 (5.95) |
| Lower Saxony | 10,152 (6.57) |
| Mecklenburg-Western Pomerania | 3478 (2.25) |
| North Rhine-Westphalia | 36,384 (23.55) |
| Rhineland-Palatinate | 7501 (4.85) |
| Saarland | 2864 (1.85) |
| Saxony | 9169 (5.93) |
| Saxony-Anhalt | 4929 (3.19) |
| Schleswig-Holstein | 2777 (1.80) |
| Thuringia | 7679 (4.97) |
| CCA localization (total, (%)) | |
| iCCA | 96,631 (62.38) |
| eCCA | 52,348 (33.88) |
| CCA (overlapping sites of biliary tract) | 3699 (2.39) |
| CCA (unspecified) | 1837 (1.19) |
| Organ Complication (total, (%)) | |
| ARDS | 183 (0.12) |
| ARF | 6120 (3.96) |
| HE | 1622 (1.05) |
| Ileus | 2947 (1.91) |
| Liver abscess | 1790 (1.16) |
| Liver failure | 2827 (1.83) |
| PE | 1722 (1.11) |
| Pneumonia | 4760 (3.08) |
| SBP | 3556 (2.30) |
| Sepsis | 6215 (4.02) |
| Treatment (total, (%)) | |
| CTX | 36,233 (23.45) |
| HIPEC | 25 (0.02) |
| LT | 34 (0.02) |
| PDT | 826 (0.53) |
| RFA | 1152 (0.75) |
| Radiation | 2024 (1.31) |
| Surgery | 9266 (6.00) |
| SIRT | 1149 (0.74) |
| TACE | 2087 (1.35) |
| Annual CCA case volume groups (total, (%)) | |
| LCV (1–16 cases/year) | 40,590 (26.27) |
| MLCV (17–35 cases/year) | 37,119 (24.02) |
| MHCV (36–75 cases/year) | 38,547 (24.95) |
| HCV (>75 cases/year) | 38,259 (24.76) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roderburg, C.; Essing, T.; Kehmann, L.; Krieg, S.; Labuhn, S.; Kandler, J.; Luedde, T.; Loosen, S.H. Current Trends in Inpatient Care and In-Hospital Mortality of Cholangiocarcinoma in Germany: A Systematic Analysis between 2010 and 2019. Cancers 2022, 14, 4038. https://doi.org/10.3390/cancers14164038
Roderburg C, Essing T, Kehmann L, Krieg S, Labuhn S, Kandler J, Luedde T, Loosen SH. Current Trends in Inpatient Care and In-Hospital Mortality of Cholangiocarcinoma in Germany: A Systematic Analysis between 2010 and 2019. Cancers. 2022; 14(16):4038. https://doi.org/10.3390/cancers14164038
Chicago/Turabian StyleRoderburg, Christoph, Tobias Essing, Linde Kehmann, Sarah Krieg, Simon Labuhn, Jennis Kandler, Tom Luedde, and Sven H. Loosen. 2022. "Current Trends in Inpatient Care and In-Hospital Mortality of Cholangiocarcinoma in Germany: A Systematic Analysis between 2010 and 2019" Cancers 14, no. 16: 4038. https://doi.org/10.3390/cancers14164038
APA StyleRoderburg, C., Essing, T., Kehmann, L., Krieg, S., Labuhn, S., Kandler, J., Luedde, T., & Loosen, S. H. (2022). Current Trends in Inpatient Care and In-Hospital Mortality of Cholangiocarcinoma in Germany: A Systematic Analysis between 2010 and 2019. Cancers, 14(16), 4038. https://doi.org/10.3390/cancers14164038