
Efficacy and Safety of Amrubicin in Small Cell Carcinoma Previously Treated with Immune Checkpoint Inhibitors and Chemotherapy

 , , ,
, , , 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
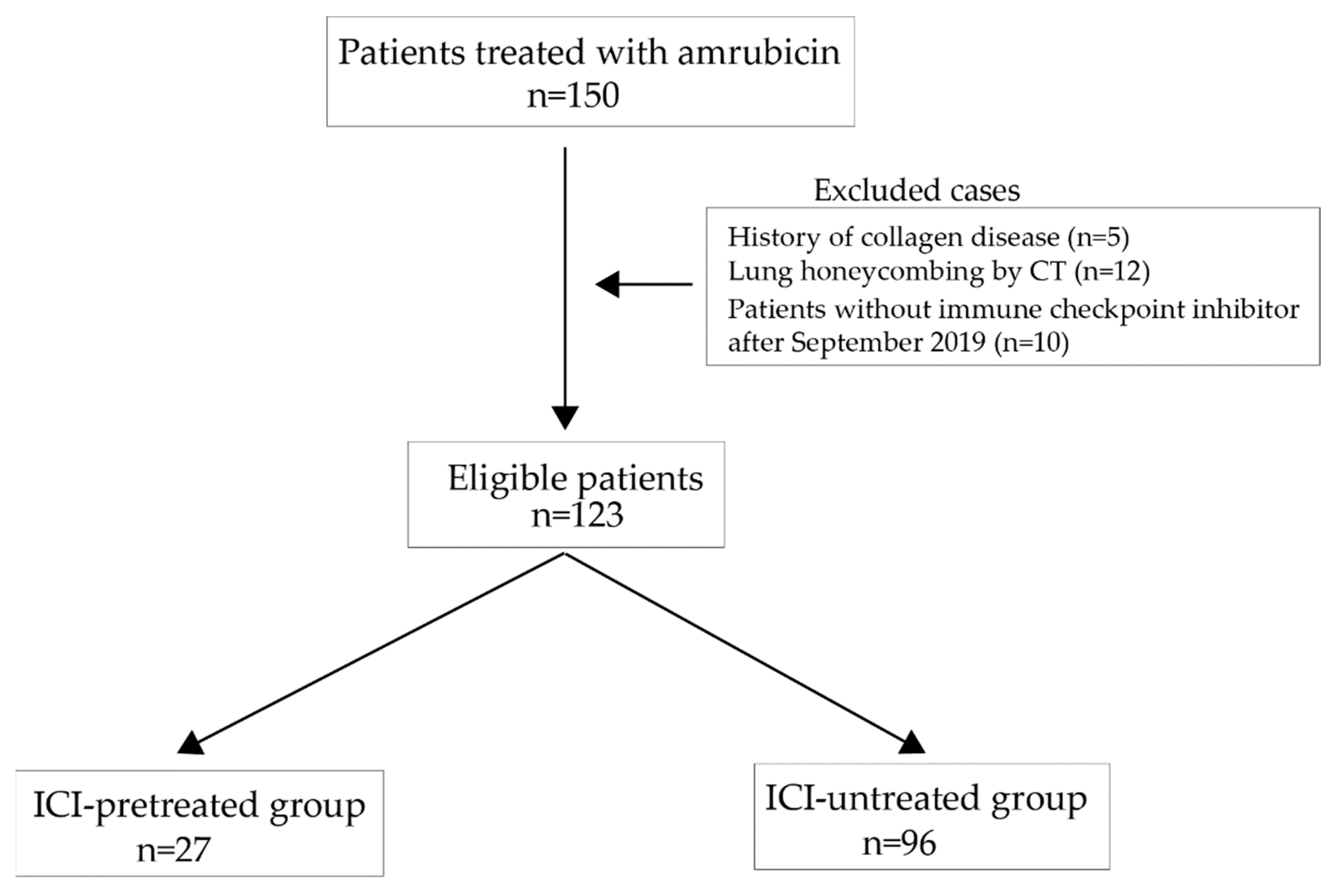
2.1. Patients and Study Design
2.2. Ethical Statement
2.3. Statistical Analysis
3. Results
3.1. Patients’ Characteristics
3.2. No Difference in Tumor Response between ICI-Pretreated and ICI-Untreated Groups
3.3. No Difference in Time-to-Treatement Failure, Progression-Free Survival, and Overall Survival between ICI-Pretreated and ICI-Untreated Groups
3.4. Performance Status, Adrenal Metastasis, and Pleural Effusion Predicted a Poor Prognosis
3.5. Pretreatment with ICIs Exerted No Influence on Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Govindan, R.; Page, N.; Morgensztern, D.; Read, W.; Tierney, R.; Vlahiotis, A.; Spitznagel, E.L.; Piccirillo, J. Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: Analysis of the surveillance, epidemiologic, and end results database. J. Clin. Oncol. 2006, 24, 4539–4544. [Google Scholar] [CrossRef] [PubMed]
- Horn, L.; Mansfield, A.S.; Szczęsna, A.; Havel, L.; Krzakowski, M.; Hochmair, M.J.; Huemer, F.; Losonczy, G.; Johnson, M.L.; Nishio, M.; et al. First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N. Engl. J. Med. 2018, 379, 2220–2229. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Özgüroğlu, M.; Ji, J.H.; et al. Durvalumab Plus Platinum-Etoposide versus Platinum-Etoposide in First-Line Treatment of Extensive-Stage Small-Cell Lung Cancer (CASPIAN): A Randomised, Controlled, Open-Label, Phase 3 Trial. Lancet 2019, 394, 1929–1939. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31590988 (accessed on 3 March 2022). [CrossRef]
- Goldman, J.W.; Dvorkin, M.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Ozguroglu, M.; Ji, J.H.; et al. Durvalumab, with or without Tremelimumab, plus Platinum-Etoposide versus Platinum-Etoposide Alone in First-Line Treatment of Extensive-Stage Small-Cell Lung Cancer (CASPIAN): Updated Results from a Randomised, Controlled, Open-Label, Phase 3 Trial. Lancet Oncol. 2021, 22, 51–65. Available online: http://www.ncbi.nlm.nih.gov/pubmed/33285097 (accessed on 3 March 2022). [CrossRef]
- Liu, S.V.; Reck, M.; Mansfield, A.S.; Mok, T.; Scherpereel, A.; Reinmuth, N.; Garassino, M.C.; De Castro Carpeno, J.; Califano, R.; Nishio, M.; et al. Updated Overall Survival and PD-L1 Subgroup Analysis of Patients With Extensive-Stage Small-Cell Lung Cancer Treated With Atezolizumab, Carboplatin, and Etoposide (IMpower133). J. Clin. Oncol. 2021, 39, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Chen, Y.; Reinmuth, N.; Hotta, K.; Trukhin, D.; Statsenko, G.; Hochmair, M.J.; Ozguroglu, M.; Ji, J.H.; Garassino, M.C.; et al. Durvalumab, with or without tremelimumab, plus platinum-etoposide in first-line treatment of extensive-stage small-cell lung cancer: 3-year overall survival update from CASPIAN. ESMO Open 2022, 7, 100408. [Google Scholar] [CrossRef]
- Chen, Y.; Paz-Ares, L.; Reinmuth, N.; Garassino, M.C.; Statsenko, G.; Hochmair, M.J.; Özgüroğlu, M.; Verderame, F.; Havel, L.; Losonczy, G.; et al. Brief report: Impact of brain metastases on treatment patterns and outcomes with first-line durvalumab plus platinum-etoposide in extensive-stage SCLC (CASPIAN). JTO Clin. Res. Rep. 2022, 3, 100330. [Google Scholar] [CrossRef]
- Jotte, R.; Conkling, P.; Reynolds, C.; Galsky, M.D.; Klein, L.; Fitzgibbons, J.F.; McNally, R.; Renschler, M.F.; Oliver, J.W. Randomized phase II trial of single-agent amrubicin or topotecan as second-line treatment in patients with small-cell lung cancer sensitive to first-line platinum-based chemotherapy. J. Clin. Oncol. 2011, 29, 287–293. [Google Scholar] [CrossRef]
- Murakami, H.; Yamamoto, N.; Shibata, T.; Takeda, K.; Ichinose, Y.; Ohe, Y.; Yamamoto, N.; Takeda, Y.; Kudoh, S.; Atagi, S.; et al. A single-arm confirmatory study of amrubicin therapy in patients with refractory small-cell lung cancer: Japan Clinical Oncology Group Study (JCOG0901). Lung Cancer 2014, 84, 67–72. [Google Scholar] [CrossRef]
- Horita, N.; Yamamoto, M.; Sato, T.; Tsukahara, T.; Nagakura, H.; Tashiro, K.; Shibata, Y.; Watanabe, H.; Nagai, K.; Nakashima, K.; et al. Amrubicin for relapsed small-cell lung cancer: A systematic review and meta-analysis of 803 patients. Sci. Rep. 2016, 6, 6–11. [Google Scholar]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Ott, P.A.; Elez, E.; Hiret, S.; Kim, D.-W.; Morosky, A.; Saraf, S.; Piperdi, B.; Mehnert, J.M. Pembrolizumab in patients with extensive-stage small-cell lung cancer: Results from the phase Ib KEYNOTE-028 study. J. Clin. Oncol. 2017, 35, 3823–3829. [Google Scholar] [CrossRef] [PubMed]
- Spigel, D.; Vicente, D.; Ciuleanu, T.; Gettinger, S.; Peters, S.; Horn, L.; Audigier-Valette, C.; Aranda, N.P.; Juan-Vidal, O.; Cheng, Y.; et al. Second-line nivolumab in relapsed small-cell lung cancer: CheckMate 331. Ann. Oncol. 2021, 32, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.C.; Piha-Paul, S.A.; Lopez-Martin, J.; Schellens, J.H.M.; Kao, S.; Miller, W.H., Jr.; Delord, J.-P.; Gao, B.; Planchard, D.; Gottfried, M.; et al. Pembrolizumab After Two or More Lines of Previous Therapy in Patients With Recurrent or Metastatic SCLC: Results From the KEYNOTE-028 and KEYNOTE-158 Studies. J. Thorac. Oncol. 2020, 15, 618–627. [Google Scholar] [CrossRef] [PubMed]
- Akamatsu, H.; Teraoka, S.; Hayashi, H.; Fujimoto, D.; Hayata, A.; Haratani, K.; Ozawa, Y.; Yoshida, T.; Iwasa, T.; Shimokawa, T.; et al. Pembrolizumab Plus Amrubicin in Patients With Relapsed SCLC: Multi-Institutional, Single-Arm Phase 2 Study. JTO Clin. Res. Rep. 2021, 2, 100184. [Google Scholar] [CrossRef]
- Emens, L.A.; Middleton, G. The interplay of immunotherapy and chemotherapy: Harnessing potential synergies. Cancer Immunol. Res. 2015, 3, 436–443. [Google Scholar] [CrossRef]
- Ma, Y.; Mattarollo, S.R.; Adjemian, S.; Yang, H.; Aymeric, L.; Hannani, D.; Portela Catani, J.P.; Duret, H.; Teng, M.W.; Kepp, O.; et al. CCL2/CCR2-dependent recruitment of functional antigen-presenting cells into tumors upon chemotherapy. Cancer Res. 2014, 74, 436–445. [Google Scholar] [CrossRef]
- Sistigu, A.; Yamazaki, T.; Vacchelli, E.; Chaba, K.; Enot, D.P.; Adam, J.; Vitale, I.; Goubar, A.; Baracco, E.E.; Remédios, C.; et al. Cancer cell-autonomous contribution of type I interferon signaling to the efficacy of chemotherapy. Nat. Med. 2014, 20, 1301–1309. [Google Scholar] [CrossRef]
- Park, S.E.; Lee, S.H.; Ahn, J.S.; Ahn, M.J.; Park, K.; Sun, J.M. Increased Response Rates to Salvage Chemotherapy Administered after PD-1/PD-L1 Inhibitors in Patients with Non–Small Cell Lung Cancer. J. Thorac. Oncol. 2018, 13, 106–111. [Google Scholar] [CrossRef]
- Shiono, A.; Kaira, K.; Mouri, A.; Yamaguchi, O.; Hashimoto, K.; Uchida, T.; Miura, Y.; Nishihara, F.; Murayama, Y.; Kobayashi, K.; et al. Improved efficacy of ramucirumab plus docetaxel after nivolumab failure in previously treated non-small cell lung cancer patients. Thorac. Cancer 2019, 10, 775–781. [Google Scholar] [CrossRef]
- Harada, D.; Takata, K.; Mori, S.; Kozuki, T.; Takechi, Y.; Moriki, S.; Asakura, Y.; Ohno, T.; Nogami, N. Previous immune checkpoint inhibitor treatment to increase the efficacy of docetaxel and ramucirumab combination chemotherapy. Anticancer Res. 2019, 39, 4987–4993. [Google Scholar] [CrossRef] [PubMed]
- Kato, R.; Hayashi, H.; Chiba, Y.; Miyawaki, E.; Shimizu, J.; Ozaki, T.; Fujimoto, D.; Toyozawa, R.; Nakamura, A.; Kozuki, T.; et al. Propensity score-weighted analysis of chemotherapy after PD-1 inhibitors versus chemotherapy alone in patients with non-small cell lung cancer (WJOG10217L). J. Immunother. Cancer 2020, 8, e000350. [Google Scholar] [CrossRef] [PubMed]
- Brueckl, W.M.; Reck, M.; Rittmeyer, A.; Kollmeier, J.; Wesseler, C.; Wiest, G.H.; Christopoulos, P.; Stenzinger, A.; Tufman, A.; Hoffknecht, P.; et al. Efficacy of docetaxel plus ramucirumab as palliative second-line therapy following first-line chemotherapy plus immune-checkpoint-inhibitor combination treatment in patients with non-small cell lung cancer (NSCLC) UICC stage IV. Transl. Lung Cancer Res. 2021, 10, 3093–3105. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, T.; Fujimoto, H.; Okano, T.; Naito, M.; Tsuji, C.; Iwanaka, S.; Sakakura, Y.; Yasuma, T.; D’Alessandro-Gabazza, C.N.; Oomoto, Y.; et al. Is the Efficacy of Adding Ramucirumab to Docetaxel Related to a History of Immune Checkpoint Inhibitors in the Real-World Clinical Practice? Cancers 2022, 14, 2970. [Google Scholar] [CrossRef] [PubMed]
- Brahmer, J.R.; Drake, C.G.; Wollner, I.; Powderly, J.D.; Picus, J.; Sharfman, W.H.; Stankevich, E.; Pons, A.; Salay, T.M.; McMiller, T.L.; et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: Safety, clinical activity, pharmacodynamics, and immunologic correlates. J. Clin. Oncol. 2010, 28, 3167–3175. [Google Scholar] [CrossRef] [PubMed]
- Osa, A.; Uenami, T.; Koyama, S.; Fujimoto, K.; Okuzaki, D.; Takimoto, T.; Hirata, H.; Yano, Y.; Yokota, S.; Kinehara, Y.; et al. Clinical implications of monitoring nivolumab immunokinetics in non-small cell lung cancer patients. JCI Insight 2018, 3, e59125. [Google Scholar] [CrossRef]
- Schoenfeld, A.; Arbour, K.; Rizvi, H.; Iqbal, A.; Gadgeel, S.; Girshman, J.; Kris, M.; Riely, G.; Yu, H.; Hellmann, M. Severe immune-related adverse events are common with sequential PD-(L)1 blockade and osimertinib. Ann. Oncol. 2019, 30, 839–844. [Google Scholar] [CrossRef]
- Rudin, C.M.; Poirier, J.T.; Byers, L.A.; Dive, C.; Dowlati, A.; George, J.; Heymach, J.V.; Johnson, J.E.; Lehman, J.M.; MacPherson, D.; et al. Molecular Subtypes of Small Cell Lung Cancer: A Synthesis of Human and Mouse Model Data. Nat. Rev. Cancer 2019, 19, 289–297. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30926931 (accessed on 1 April 2022). [CrossRef]
- Gay, C.M.; Stewart, C.A.; Park, E.M.; Diao, L.; Groves, S.M.; Heeke, S.; Nabet, B.Y.; Fujimoto, J.; Solis, L.M.; Lu, W.; et al. Patterns of transcription factor programs and immune pathway activation define four major subtypes of SCLC with distinct therapeutic vulnerabilities. Cancer Cell 2021, 39, 346–360.e7. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Factor | Group | ICI- Pretreated | ICI- Untreated | p- Value |
|---|---|---|---|---|
| n | 27 | 96 | ||
| Gender | Male | 26 (96.3) | 79 (82.3) | 0.119 |
| Female | 1 (3.7) | 17 (17.7) | ||
| Age (%) | <70 | 10 (37.0) | 48 (50.0) | 0.279 |
| ≥70 | 17 (63.0) | 48 (50.0) | ||
| ECOG performance status (%) | 0 | 8 (29.6) | 34 (35.4) | 0.941 |
| 1 | 16 (59.3) | 49 (51.0) | ||
| 2 | 3 (11.1) | 11 (11.5) | ||
| 3 | 0 (0.0) | 2 (2.1) | ||
| Smoking status (%) | Yes | 27 (100.0) | 96 (100.0) | NA |
| Previous treatment (%) | CBDCA+etoposide | 0 (0.0) | 82 (85.4) | <0.001 |
| CBDCA+etoposide+atezolizumab | 23 (85.2) | 0 (0.0) | ||
| CBDCA+etoposide+durvalumab | 4 (14.8) | 0 (0.0) | ||
| CBDCA+irinotecan | 0 (0.0) | 4 (4.2) | ||
| CDDP+etoposide | 0 (0.0) | 7 (7.3) | ||
| CDDP+irinotecan | 0 (0.0) | 3 (3.1) | ||
| Sensitivity of previous chemotherapy (%) | Sensitive (>90 days of last chemotherapy) | 6 (22.2) | 46 (47.9) | 0.026 |
| Refractory (relapsed ≤90 days of last chemotherapy) | 21 (77.8) | 50 (52.1) | ||
| Brain metastasis (%) | Negative | 19 (70.4) | 60 (62.5) | 0.503 |
| Positive | 8 (29.6) | 36 (37.5) | ||
| Liver metastasis (%) | Negative | 21 (77.8) | 62 (64.6) | 0.248 |
| Positive | 6 (22.2) | 34 (35.4) | ||
| Malignant pleural effusion (%) | Negative | 20 (74.1) | 72 (75.0) | 1 |
| Positive | 7 (25.9) | 24 (25.0) | ||
| Bone metastasis (%) | Negative | 16 (59.3) | 67 (69.8) | 0.354 |
| Positive | 11 (40.7) | 29 (30.2) | ||
| Adrenal metastasis (%) | Negative | 19 (70.4) | 78 (81.2) | 0.285 |
| Positive | 8 (29.6) | 18 (18.8) | ||
| Discontinuation of amrubicin due to adverse effects | Negative | 22 (95.7) | 85 (88.5) | 0.457 |
| Positive | 1 (4.3) | 11 (11.5) |
| ICI-Pretreated | ICI-Untreated | p-Value | |
|---|---|---|---|
| n | 27 | 96 | |
| Complete response (%) | 0 (0.0) | 3 (3.1) | 0.51 |
| Partial response (%) | 8 (29.6) | 17 (17.7) | |
| Stable disease (%) | 8 (29.6) | 40 (41.7) | |
| Progressive disease (%) | 10 (37.0) | 29 (30.2) | |
| Not evaluated (%) | 1 (3.7) | 7 (7.3) | |
| Overall response rate (%) | 8 (30.8, 95% CI 14.3–51.8) | 20 (22.5, 95% CI 14.3–32.6) | |
| Disease control rate (%) | 16 (61.5, 95% CI 40.6–79.8) | 60 (67.4, 95% CI 56.7–77.0) |
| Time-to-Treatment Failure | |||||
| Univariate Analysis | Multivariate Analysis | ||||
| Factors | Hazard Ratio | p Value | Hazard Ratio | p Value | |
| Age | <70 | Referent | 0.57 | Referent | 0.53 |
| >=70 | 1.11 (0.77–1.6) | 1.13 (0.77–1.68) | |||
| Gender | Male | Referent | 0.41 | Referent | 0.53 |
| Female | 0.81 (0.49–1.34) | 0.84 (0.48–1.46) | |||
| Performance status * | 0–2 | Referent | 0.00059 | Referent | 0.00092 |
| 3 | 13.62 (3.07–60.4) | 13.86 (2.93–65.62) | |||
| Brain metastasis | Negative | Referent | 0.21 | Referent | 0.33 |
| Positive | 1.28 (0.87–1.87) | 1.24 (0.81–1.89) | |||
| Liver metastasis | Negative | Referent | 0.0097 | Referent | 0.18 |
| Positive | 1.69 (1.14–2.53) | 1.36 (0.87–2.14) | |||
| M. pleural effusion | Negative | Referent | 0.12 | Referent | 0.23 |
| Positive | 1.41 (0.92–2.15) | 1.32 (0.84–2.07) | |||
| Bone metastasis | Negative | Referent | 0.41 | Referent | 0.48 |
| Positive | 1.18 (0.8–1.74) | 1.17 (0.76–1.79) | |||
| Adrenal metastasis | Negative | Referent | 0.007 | Referent | 0.027 |
| Positive | 1.87 (1.19–2.96) | 1.83 (1.07–3.11) | |||
| Previous treatment | ICI-pretreated | Referent | 0.26 | Referent | 0.11 |
| ICI-untreated | 1.14 (0.9–1.44) | 1.22 (0.95–1.57) | |||
| Progression-Free Survival | |||||
| Univariate Analysis | Multivariate Analysis | ||||
| Factor | Hazard Ratio | p Value | Hazard Ratio | p Value | |
| Age | <70 | Referent | 0.73 | Referent | 0.86 |
| >=70 | 0.93 (0.64–1.37) | 0.97 (0.65–1.44) | |||
| Gender | Male | Referent | 0.94 | Referent | 0.62 |
| Female | 0.98 (0.57–1.67) | 1.16 (0.64–2.12) | |||
| Performance status * | 0–2 | Referent | 0.0051 | Referent | 0.0078 |
| 3 | 21.53 (2.52–184.3) | 20.72 (2.22–193.30) | |||
| Brain metastasis | Negative | Referent | 0.37 | Referent | 0.94 |
| Positive | 1.20 (0.81–1.79) | 0.98 (0.63–1.53) | |||
| Liver metastasis | Negative | Referent | 0.011 | Referent | 0.069 |
| Positive | 1.74 (1.14–2.67) | 1.58 (0.97–2.60) | |||
| M. pleural effusion | Negative | Referent | 0.19 | Referent | 0.47 |
| Positive | 1.35 (0.86–2.1) | 1.19 (0.74–1.91) | |||
| Bone metastasis | Negative | Referent | 0.51 | Referent | 0.96 |
| Positive | 1.15 (0.76–1.75) | 0.99 (0.62–1.58) | |||
| Adrenal metastasis | Negative | Referent | 0.0035 | Referent | 0.021 |
| Positive | 2.06 (1.27–3.34) | 1.90 (1.10–3.27) | |||
| Previous treatment | ICI-pretreated | Referent | 0.91 | Referent | 0.83 |
| ICI-untreated | 1.04 (0.51–2.15) | 0.97 (0.75–1.26) | |||
| Overall Survival | |||||
| Univariate Analysis | Multivariate Analysis | ||||
| Factors | Hazard Ratio | p Value | Hazard Ratio | p Value | |
| Age | <70 | Referent | 0.15 | Referent | 0.036 |
| >=70 | 1.33 (0.9–1.95) | 1.56 (1.03–2.36) | |||
| Gender | Male | Referent | 0.44 | Referent | 0.79 |
| Female | 0.81 (0.47–1.38) | 0.93 (0.52–1.64) | |||
| Performance status * | 0–2 | Referent | 0.000043 | Referent | 0.000025 |
| 3 | 59.87 (8.43–425.1) | 77.60 (10.26–587.10) | |||
| Brain metastasis | Negative | Referent | 0.19 | Referent | 0.17 |
| Positive | 1.30 (0.87–1.93) | 1.34 (0.88–2.04) | |||
| Liver metastasis | Negative | Referent | 0.0021 | Referent | 0.081 |
| Positive | 1.91 (1.27–2.89) | 1.52 (0.95–2.43) | |||
| M. pleural effusion | Negative | Referent | 0.00085 | Referent | 0.00035 |
| Positive | 2.11 (1.36–3.28) | 2.35 (1.47–3.75) | |||
| Bone metastasis | Negative | Referent | 0.42 | Referent | 0.38 |
| Positive | 1.19 (0.79–1.79) | 1.23 (0.78–1.95) | |||
| Adrenal metastasis | Negative | Referent | 0.0056 | Referent | 0.021 |
| Positive | 1.95 (1.22–3.13) | 1.84 (1.10–3.09) | |||
| Previous treatment | ICI-pretreated | Referent | 0.51 | Referent | 0.46 |
| ICI-untreated | 1.10 (0.83–1.45) | 1.11 (0.83–1.49) | |||
| n | Time-to-Treatment Failure | |||
| Hazard Ratio (95% CI) | p-Value | |||
| unadjusted | ICI-pretreated | 27 | Referent | 0.26 |
| ICI-untreated | 96 | 1.14 (0.9–1.44) | ||
| IPTW weighted | ICI-pretreated | 27 | Referent | 0.15 |
| ICI-untreated | 96 | 1.31 (0.91–1.89) | ||
| 1:1 matching | ICI-pretreated | 21 | Referent | 0.71 |
| ICI-untreated | 22 | 1.13 (0.61–2.09) | ||
| Progression-free survival | ||||
| Hazard ratio (95% CI) | p-value | |||
| unadjusted | ICI-pretreated | 27 | Referent | 0.91 |
| ICI-untreated | 96 | 1.04 (0.51–2.15) | ||
| IPTW weighted | ICI-pretreated | 27 | Referent | 0.76 |
| ICI-untreated | 96 | 0.94 (0.64–1.39) | ||
| 1:1 matching | ICI-pretreated | 21 | Referent | 0.88 |
| ICI-untreated | 22 | 1.05 (0.55–2) | ||
| Overall survival | ||||
| Hazard ratio (95% CI) | p-value | |||
| unadjusted | ICI-pretreated | 27 | Referent | 0.51 |
| ICI-untreated | 96 | 1.10 (0.83–1.45) | ||
| IPTW weighted | ICI-pretreated | 27 | Referent | 0.18 |
| ICI-untreated | 96 | 1.65 (0.8–3.42) | ||
| 1:1 matching | ICI-pretreated | 21 | Referent | 0.48 |
| ICI-untreated | 22 | 1.29 (0.64–2.6) | ||
| ICI-Pretreated Group | ICI-Untreated Group | |||
|---|---|---|---|---|
| N | 27 | 96 | ||
| Any Grade | Grade 3 <= | Any Grade | Grade 3 <= | |
| Febrile neutropenia | 6 (22.2) | 6 (22.2) | 23 (24.0) | 23 (24.0) |
| Anemia | 23 (85.2) | 3 (11.1) | 68 (70.8) | 13 (13.5) |
| Neutropenia | 23 (85.2) | 17 (63.0) | 87 (90.6) | 68 (70.8) |
| Thrombocytopenia | 16 (59.3) | 5 (18.5) | 50 (52.1) | 18 (18.8) |
| Pneumonitis | 1 (3.7) | 1 (3.7) | 7 (7.3) | 4 (4.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nishimura, T.; Fujimoto, H.; Fujiwara, T.; Ito, K.; Fujiwara, A.; Yuda, H.; Itani, H.; Naito, M.; Kodama, S.; Yagi, A.; et al. Efficacy and Safety of Amrubicin in Small Cell Carcinoma Previously Treated with Immune Checkpoint Inhibitors and Chemotherapy. Cancers 2022, 14, 3953. https://doi.org/10.3390/cancers14163953
Nishimura T, Fujimoto H, Fujiwara T, Ito K, Fujiwara A, Yuda H, Itani H, Naito M, Kodama S, Yagi A, et al. Efficacy and Safety of Amrubicin in Small Cell Carcinoma Previously Treated with Immune Checkpoint Inhibitors and Chemotherapy. Cancers. 2022; 14(16):3953. https://doi.org/10.3390/cancers14163953
Chicago/Turabian StyleNishimura, Tadashi, Hajime Fujimoto, Takumi Fujiwara, Kentaro Ito, Atsushi Fujiwara, Hisamichi Yuda, Hidetoshi Itani, Masahiro Naito, Shuji Kodama, Akihiko Yagi, and et al. 2022. "Efficacy and Safety of Amrubicin in Small Cell Carcinoma Previously Treated with Immune Checkpoint Inhibitors and Chemotherapy" Cancers 14, no. 16: 3953. https://doi.org/10.3390/cancers14163953
APA StyleNishimura, T., Fujimoto, H., Fujiwara, T., Ito, K., Fujiwara, A., Yuda, H., Itani, H., Naito, M., Kodama, S., Yagi, A., D’Alessandro, V. F., Yasuma, T., Furuhashi, K., Saiki, H., Okano, T., Tomaru, A., Tanigawa, M., D’Alessandro-Gabazza, C. N., Gabazza, E. C., ... Kobayashi, T. (2022). Efficacy and Safety of Amrubicin in Small Cell Carcinoma Previously Treated with Immune Checkpoint Inhibitors and Chemotherapy. Cancers, 14(16), 3953. https://doi.org/10.3390/cancers14163953