
The Role of [68Ga]Ga-Pentixafor PET/CT or PET/MRI in Lymphoma: A Systematic Review



Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
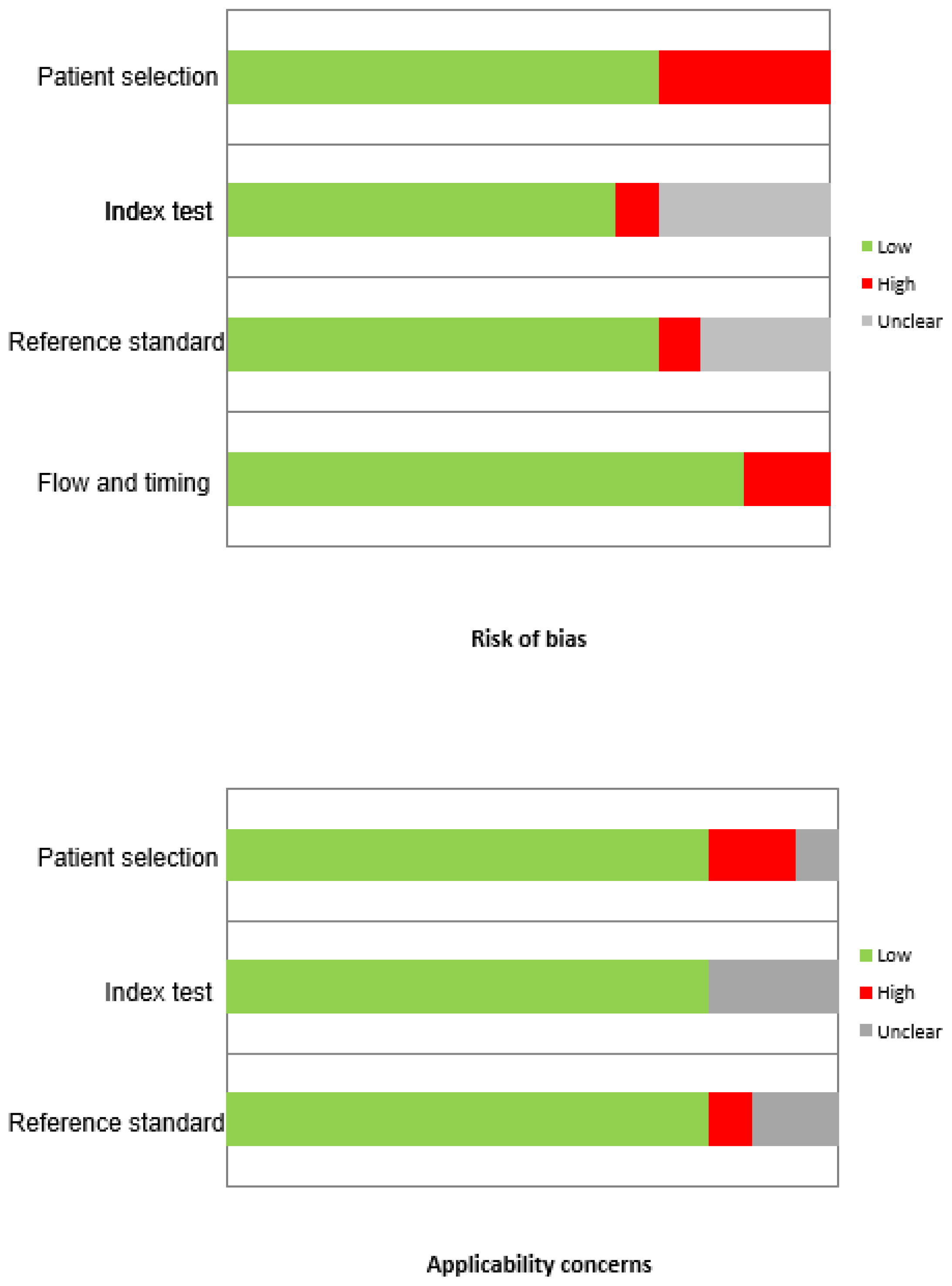
2.3. Quality Assessment
2.4. Data Abstraction
2.5. Statistical Analysis
3. Results
3.1. Literature Search
3.2. Qualitative Analysis
3.3. Lymphoma Variants Analysis
3.4. MZL/MALT
3.5. CNSL
3.6. WM/LPL
3.7. MCL
3.8. Other Lymphomas
4. Discussion
Limitations of the Studies
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Colobran, R.; Pujol-Borrell, R.; Armengol, M.P.; Juan, M. The chemokine network. I. How the genomic organization of chemokines contains clues for deciphering their functional complexity. Clin. Exp. Immunol. 2007, 148, 208–217. [Google Scholar] [CrossRef]
- Balkwill, F. Cancer and the chemokine network. Nat. Rev. Cancer 2004, 4, 540–550. [Google Scholar] [CrossRef]
- Chatterjee, S.; Behnam Azad, B.; Nimmagadda, S. The intricate role of CXCR4 in cancer. Adv. Cancer Res. 2014, 124, 31–82. [Google Scholar]
- Buck, A.K.; Serfling, S.E.; Lindner, T.; Hänscheid, H.; Schirbel, A.; Hahner, S.; Fassnacht, M.; Einsele, H.; Werner, R.A. CXCR4-targeted theranostics in oncology. Eur. J. Nucl. Med. Mol. Imaging 2022. online ahead of print. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Archibald, S.J.; Messiou, C.; Staudenherz, A.; Berzaczy, D.; Schöder, H. MRI and PET/MRI in hematologic malignancies. J. Magn. Reason. Imaging 2020, 51, 1325–1335. [Google Scholar] [CrossRef]
- Demmer, O.; Gourni, E.; Schumacher, U.; Kessler, H.; Wester, H.J. PET imaging of CXCR4 receptors in cancer by a new optimized ligand. Chem. Med. Chem. 2011, 6, 1789–1791. [Google Scholar] [CrossRef] [Green Version]
- Woodard, L.E.; Nimmagadda, S. CXCR4-based imaging agents. J. Nucl. Med. 2011, 52, 1665–1669. [Google Scholar] [CrossRef] [Green Version]
- Nimmagadda, S.; Pullambhatla, M.; Pomper, M.G. Immunoimaging of CXCR4 expression in brain tumor xenografts using SPECT/CT. J. Nucl. Med. 2009, 50, 1124–1130. [Google Scholar] [CrossRef] [Green Version]
- Bertagna, F.; Giubbini, R.; Albano, D. Evidence-Based PET for Haematological Tumours. In Evidence-Based Positron Emission Tomography; Treglia, G., Giovanella, L., Eds.; Springer: Cham, Switzerland. [CrossRef]
- Buck, A.K.; Stolzenburg, A.; Hänscheid, H.; Schirbel, A.; Lückerath, K.; Schottelius, M.; Wester, H.-J.; Lapa, C. Chemokine receptor—directed imaging and therapy. Methods 2017, 130, 63–71. [Google Scholar] [CrossRef]
- Habringer, S.; Lapa, C.; Herhaus, P.; Schottelius, M.; Istvanffy, R.; Steiger, K.; Slotta-Huspenina, J.; Schirbel, A.; Hänscheid, H.; Kircher, S.; et al. Dual targeting of acute leukemia and supporting niche by CXCR4-directed theranostics. Theranostics 2018, 8, 369–383. [Google Scholar] [CrossRef] [Green Version]
- Lapa, C.; Hänscheid, H.; Kircher, M.; Schirbel, A.; Wunderlich, G.; Werner, R.A.; Samnick, S.; Kotzerke, J.; Einsele, H.; Buck, A.K.; et al. Feasibility of CXCR4-directed radioligand therapy in advanced diffuse large B-cell lymphoma. J. Nucl. Med. 2019, 60, 60–64. [Google Scholar] [CrossRef]
- Wester, H.J.; Keller, U.; Schottelius, M.; Beer, A.; Philipp-Abbrederis, K.; Hoffmann, F.; Šimeček, J.; Gerngross, C.; Lassmann, M.; Herrmann, K.; et al. Disclosing the CXCR4 expression in lymphoproliferative diseases by targeted molecular imaging. Theranostics 2015, 5, 618–630. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; Hooft, L.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies. The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Jaeger, U.; Staber, P.; Raderer, M.; Wadsak, W.; Pfaff, S.; Kornauth, C.; Senn, D.; Weber, M.; Wester, H.J.; et al. [68Ga]Ga-Pentixafor PET/MRI for CXCR4 Imaging of Chronic Lymphocytic Leukemia: Preliminary Results. Investig. Radiol. 2018, 53, 403–408. [Google Scholar] [CrossRef]
- Luo, Y.; Cao, X.; Pan, Q.; Li, J.; Feng, J.; Li, F. 68Ga-Pentixafor PET/CT for Imaging of Chemokine Receptor 4 Expression in Waldenström Macroglobulinemia/Lymphoplasmacytic Lymphoma: Comparison to 18F-FDG PET/CT. J. Nucl. Med. 2019, 60, 1724–1729. [Google Scholar] [CrossRef]
- Haug, A.R.; Leisser, A.; Wadsak, W.; Mitterhauser, M.; Pfaff, S.; Kropf, S.; Wester, H.J.; Hacker, M.; Hartenbach, M.; Kiesewetter-Wiederkehr, B.; et al. Prospective non-invasive evaluation of CXCR4 expression for the diagnosis of MALT lymphoma using [68Ga]Ga-Pentixafor-PET/MRI. Theranostics 2019, 9, 3653–3658. [Google Scholar] [CrossRef]
- Pan, Q.; Cao, X.; Luo, Y.; Li, J.; Li, F. Chemokine Receptor 4-Targeted 68Ga-Pentixafor PET/CT in Response Assessment of Waldenström Macroglobulinemia/Lymphoplasmacytic Lymphoma: Comparison to 18F-FDG PET/CT. Clin. Nucl. Med. 2021, 46, 732–737. [Google Scholar] [CrossRef]
- Herhaus, P.; Lipkova, J.; Lammer, F.; Yakushev, I.; Vag, T.; Slotta-Huspenina, J.; Habringer, S.; Lapa, C.; Pukrop, T.; Hellwig, D.; et al. CXCR4-Targeted PET Imaging of Central Nervous System B-Cell Lymphoma. J. Nucl. Med. 2020, 61, 1765–1771. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Haug, A.R.; Jager, U.; Pichler, V.; Pfaff, S.; Wester, H.J.; Hacker, M.; Kaizanka, L.; Staber, P.B. In human visualization of ibrutinib CLL compartment shift. Cancer Immunol. Res. 2020, 8, 984–989. [Google Scholar] [CrossRef]
- Duell, J.; Krummenast, F.; Schirbel, A.; Klassen, P.; Samnick, S.; Rauert-Wunderlich, H.; Rasche, L.; Buck, A.K.; Wester, H.J.; Rosenwald, A.; et al. Improved Primary Staging of Marginal-Zone Lymphoma by Addition of CXCR4-Directed PET/CT. J. Nucl. Med. 2021, 62, 1415–1421. [Google Scholar] [CrossRef] [PubMed]
- Kuyumcu, S.; Kıran, M.Y.; Arıkan, E.A.; Yeğen, G.; Şanlı, Y. [68Ga]-Pentixafor PET/CT imaging of lymphoproliferative malignancies. Clin. Transl. Imaging 2012, 41, 5239–5261. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Raderer, M.; Lamm, W.; Pichler, V.; Pfaff, S.; Weber, M.; Kiesewetter, B.; Hacker, M.; Kazianka, L.; Staber, P.B.; et al. CXCR4 PET imaging of mantle cell lymphoma using [68Ga]Pentixafor: Comparison with [18F]FDG-PET. Theranostics 2021, 11, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Starzer, A.M.; Berghoff, A.S.; Traub-Weidinger, T.; Haug, A.R.; Widhalm, G.; Hacker, M.; Rausch, I.; Preusser, M.; Mayerhoefer, M.E. Assessment of Central Nervous System Lymphoma Based on CXCR4 Expression In Vivo Using 68Ga-Pentixafor PET/MRI. Clin. Nucl. Med. 2021, 46, 16–20. [Google Scholar] [CrossRef]
- Pan, Q.; Luo, Y.; Zhang, Y.; Chang, L.; Li, J.; Cao, X.; Li, J.; Li, F. Preliminary evidence of imaging of chemokine receptor-4-targeted PET/CT with [68Ga]pentixafor in non-Hodgkin lymphoma: Comparison to [18F]FDG. EJNMMI Res. 2020, 10, 89. [Google Scholar] [CrossRef]
- Buck, A.K.; Haug, A.; Dreher, N.; Lambertini, A.; Higuchi, T.; Lapa, C.; Weich, A.; Pomper, M.G.; Wester, H.J.; Zehnder, A.; et al. Imaging of C-X-C Motif Chemokine Receptor 4 Expression in 690 Patients with Solid or Hematologic Neoplasms using 68Ga-PentixaFor PET. J. Nucl. Med. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Chen, Z.; Yang, A.; Zhang, J.; Chen, A.; Zhang, Y.; Huang, C.; Chen, S.; Yao, S.; Miao, W. CXCR4-Directed PET/CT with [68Ga]Pentixafor in Central Nervous System Lymphoma: A Comparison with [18F]FDG PET/CT. Mol. Imaging Biol. 2022, 24, 416–424. [Google Scholar] [CrossRef]
- Mayerhoefer, M.E.; Raderer, M.; Lamm, W.; Weber, M.; Kiesewetter, B.; Rohrbeck, J.; Simonitsch-Klupp, I.; Hacker, M.; Leisser, A.; Nics, L.; et al. CXCR4 PET/MRI for follow-up of gastric mucosa-associated lymphoid tissue lymphoma after first-line Helicobacter pylori eradication. Blood 2022, 139, 240–244. [Google Scholar] [CrossRef]
- Owen, R.G.; Kyle, R.A.; Stone, M.J.; Rawstron, A.; Leblond, V.; Merlini, G.; Garcia-Sanz, R.; Ocio, E.M.; Morra, E.; Morel, P.; et al. Response assessment in Waldenström macroglobulinaemia: Update from the VIth International Workshop. Br. J. Haematol. 2013, 160, 171–176. [Google Scholar] [CrossRef]
- Nayak, T.; Hong, H.; Zhang, Y.; Cai, W. Multimodality imaging of CXCR4 in cancer: Current status towards clinical translation. Curr. Mol. Med. 2013, 13, 1538–1548. [Google Scholar] [CrossRef]
- Kuil, J.; Buckle, T.; van Leeuwen, F.W.B. Imaging agents for the chemokine receptor 4 (CXCR4). Chem. Soc. Rev. 2012, 41, 5239–5261. [Google Scholar] [CrossRef] [PubMed]
- Weiss, I.D.; Jacobson, O. Molecular Imaging of Chemokine Receptor CXCR4. Theranostics 2013, 3, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Kwon, D.; Takata, K.; Zhang, Z.; Chong, L.; Fraser, B.; Zeisler, J.; Miyata-Takata, T.; Merkens, H.; Rousseau, J.; Aoki, T.; et al. Targeting Refractory Mantle Cell Lymphoma for Imaging and Therapy Using C-X-C Chemokine Receptor Type 4 Radioligands. Clin. Cancer Res. 2022, 28, 1628–1639. [Google Scholar] [CrossRef] [PubMed]
- Barrington, S.F.; Mikhaeel, N.G.; Kostakoglu, L.; Meignan, M.; Hutchings, M.; Müeller, S.P.; Schwartz, L.H.; Zucca, E.; Fisher, R.I.; Trotman, J.; et al. Role of imaging in the staging and response assessment of lymphoma: Consensus of the International Conference on Malignant Lymphomas Imaging Working Group. J. Clin. Oncol. 2014, 32, 3048–3058. [Google Scholar] [CrossRef]
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A.; Alliance, Australasian Leukaemia and Lymphoma Group; Eastern Cooperative Oncology Group; European Mantle Cell Lymphoma Consortium; et al. Recommendations for initial evaluation, staging, and response assessment of Hodgkin and non-Hodgkin lymphoma: The Lugano classification. J. Clin. Oncol. 2014, 32, 3059–3068. [Google Scholar] [CrossRef]
- Albano, D.; Treglia, G.; Gazzilli, M.; Cerudelli, E.; Giubbini, R.; Bertagna, F. 18F-FDG PET or PET/CT in Mantle Cell Lymphoma. Clin. Lymphoma Myeloma Leuk 2020, 20, 422–430. [Google Scholar] [CrossRef]
- Albano, D.; Bosio, G.; Bertoli, M.; Giubbini, R.; Bertagna, F. 18F-FDG PET/CT in primary brain lymphoma. J. Neurooncol. 2018, 136, 577–583. [Google Scholar] [CrossRef]
- Albano, D.; Durmo, R.; Treglia, G.; Giubbini, R.; Bertagna, F. 18F-FDG PET/CT or PET Role in MALT Lymphoma: An Open Issue not Yet Solved-A Critical Review. Clin. Lymphoma. Myeloma. Leuk. 2020, 20, 137–146. [Google Scholar] [CrossRef]
- Mondello, P.; Cuzzocrea, S.; Navarra, M.; Mian, M. 90 Y-ibritumomab tiuxetan: A nearly forgotten opportunityr. Oncotarget 2016, 7, 7597–7609. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.; Nicholson, G.; Greenman, J.; Madden, L.; Mc Robbie, G.; Pannecouque, C.; De Clercq, E.; Ullom, R.; Maples, D.L.; Maples, R.D.; et al. Binding optimization through coordination chemistry: CXCR4 chemokine receptor antagonists from ultrarigid metal complexes. J. Am. Chem. Soc. 2009, 131, 3416–3417. [Google Scholar] [CrossRef] [Green Version]
- Burke, B.P.; Lee, R.E.; Nigam, S.; Clemente, G.; Thompson, J.A.; Ruest, T.; D’huys, T.; Schols, D.; Greenman, J.; Cawthorne, C.; et al. CXCR4 chemokine receptor imaging: Evaluation and validation of a new configurationally restricted tetraazamacrocyclic CXCR4 antagonist, Cu-64-CB-bicyclam. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, S146–S147. [Google Scholar]
- Lee, R.E.; Burke, B.P.; Miranda, C.S. Gallium-68 PET imaging of CXCR4 expression in vivo/vitro: Optimised small molecule azamacrocyclic chemokine receptor antagonists. J. Labelled. Comp. Radiopharm. 2018, 61, 463–464. [Google Scholar]


{kind=link}
{kind=link}
| First Author | Year | Country | Study Design | N° Patients | M:F | Age Mean (Range) | Lymphoma Variants |
|---|---|---|---|---|---|---|---|
| Mayerhoefer, M.E. et al. [16] | 2018 | Austria | Prospective | 13 | 7:6 | 65.6 (45–82) | 13 CLL |
| Luo, Y. et al. [17] | 2019 | China | Prospective | 17 | 11:6 | 62.5 (48–87) | 17 WM/LPL |
| Haug, A.R. et al. [18] | 2019 | Austria | Prospective | 36 | 17:19 | 62 (35–87) | 36 MALT |
| Pan, Q. et al. [19] | 2020 | China | Retrospective | 27 | 19:8 | 57.2 (15–76) | 8 LPL; 4 MZL; 3 DLBCL; 2 FL; 6 T-cell; 1 MCL; 3 unclassified indolent B cell |
| Herhaus, P. et al. [20] | 2020 | Germany | Retrospective | 11 | 8:3 | 64.1 (50–80) | 11 CNSL |
| Mayerhoefer, M.E. et al. [21] | 2020 | Austria | Prospective | 9 | na | na | 9 CLL |
| Duell, J. et al. [22] | 2021 | Germany | Retrospective | 22 | 7:15 | 65 (50–80) | 22 MZL (15 MALT) |
| Kuyumcu, S. et al. [23] | 2021 | Turkey | Retrospective | 11 | 7:4 | 56.8 (22–80) | 3 MCL; 1 MALT; 1 DLBCL; 2 CLL; 4 T cell |
| Mayerhoefer, M.E. et al. [24] | 2021 | Austria | Prospective | 22 | 11:11 | 70 (52–82) | 22 MCL |
| Starzer, A.M. et al. [25] | 2021 | Austria | Prospective | 7 | 3:4 | 54.8 (30–79) | 7 CNSL |
| Pan, Q. et al. [26] | 2021 | China | Prospective | 15 | 12:3 | 60.9 (48–76) | 15 WM/LPL |
| Buck, A.K. et al. [27] | 2022 | Germany & Austria | Retrospective | 690 (220 lymphoma) | na | na | 20 MCL; 187 MZL; 10 B-cell lymphoma; 3 T-cell lymphoma |
| Chen, Z. et al. [28] | 2022 | China | Retrospective | 36 | 18:8 | 56.7 (18–77) | 36 CNSL |
| Mayerhoefer, M.E. et al. [29] | 2022 | Austria | Prospective | 26 | 14:12 | 64.1 (40–80) | 26 gastric MALT |
| First Author | Device | Radiotracer Mean Injected Dose MBq | Uptake Time Min | Image Analysis | Semiquantitative Parameters |
|---|---|---|---|---|---|
| Mayerhoefer, M.E. et al. [16] | PET/MRI | 150 | 60 | Visual and semiquantitative | SUVmax; SUVmean |
| Luo, Y. et al. [17] | PET/CT | 84.6 | 47.8 | Visual and semiquantitative | SUVmax |
| Haug, A.R. et al. [18] | PET/MRI | 172 | 60 | Visual and semiquantitative | SUVmax; SUVmean; SUVpeak |
| Pan, Q. et al. [19] | PET/CT | 2.8/Kg | 56 | Visual and semiquantitative | SUVmax; TBRblood; TBRliver |
| Herhaus, P. et al. [20] | PET/CT & PET/MRI | 1–2.9/Kg | na | Visual and semiquantitative | SUVmax; TBR |
| Mayerhoefer, M.E. et al. [21] | PET/MRI | 150 | 60 | Visual and semiquantitative | SUVmax, SUVmean, PTV |
| Duell, J. et al. [22] | PET/CT | 117 | 60 | Visual and semiquantitative | SUVmax |
| Kuyumcu, S. et al. [23] | PET/CT | 185 | 60 | Visual and semiquantitative | SUVmax |
| Mayerhoefer, M.E. et al. [24] | PET/MRI | 150 | 60 | Visual and semiquantitative | SUVmax; SUVmean; TBRblood; TBRliver |
| Starzer, A.M. et al. [25] | PET/MRI | 150 | 60 | Visual and semiquantitative | SUVmax; SUVmean; PTV |
| Pan, Q. et al. [26] | PET/CT | 85.1 | 46 | Visual and semiquantitative | SUVmax |
| Buck, A.K. et al. [27] | PET/CT | 134 | 60 | Visual and semiquantitative | SUVmax; SUVmean, SUVpeak; TBR |
| Chen Z [28] | PET/CT | 107 | 60 | Visual and semiquantitative | SUVmax; T/N |
| Mayerhoefer ME [29] | PET/MRI | 150 | 60 | Visual and semiquantitative | SUVmax; SUVmean; TBRblood; TBRliver |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albano, D.; Dondi, F.; Bertagna, F.; Treglia, G. The Role of [68Ga]Ga-Pentixafor PET/CT or PET/MRI in Lymphoma: A Systematic Review. Cancers 2022, 14, 3814. https://doi.org/10.3390/cancers14153814
Albano D, Dondi F, Bertagna F, Treglia G. The Role of [68Ga]Ga-Pentixafor PET/CT or PET/MRI in Lymphoma: A Systematic Review. Cancers. 2022; 14(15):3814. https://doi.org/10.3390/cancers14153814
Chicago/Turabian StyleAlbano, Domenico, Francesco Dondi, Francesco Bertagna, and Giorgio Treglia. 2022. "The Role of [68Ga]Ga-Pentixafor PET/CT or PET/MRI in Lymphoma: A Systematic Review" Cancers 14, no. 15: 3814. https://doi.org/10.3390/cancers14153814
APA StyleAlbano, D., Dondi, F., Bertagna, F., & Treglia, G. (2022). The Role of [68Ga]Ga-Pentixafor PET/CT or PET/MRI in Lymphoma: A Systematic Review. Cancers, 14(15), 3814. https://doi.org/10.3390/cancers14153814