
The Role of Immunohistochemistry Markers in Endometrial Cancer with Mismatch Repair Deficiency: A Systematic Review

 , ,
, ,
Simple Summary
Abstract
1. Introduction
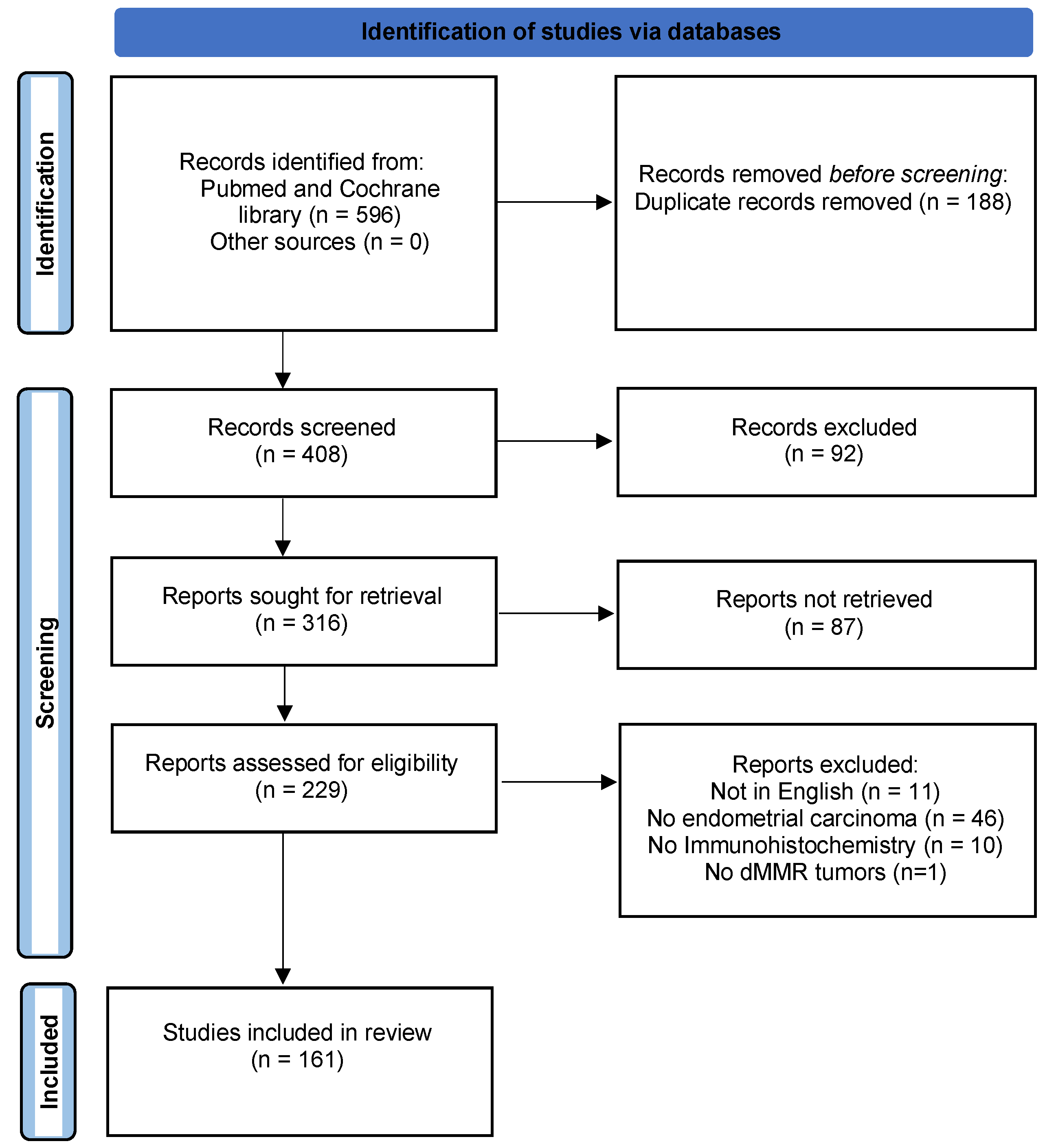
2. Materials and Methods
3. Results
3.1. IHC in the Diagnosis of MMRd Tumors in EC
3.2. IHC in the Prognosis of MMRd Tumors in EC
3.2.1. Survival
3.2.2. Pathologic Characteristics
3.3. IHC in the Theragnostics of MMRd Tumors in EC
4. Discussion
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA A Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Statistics Adapted from the American Cancer Society’s (ACS) Publication, Cancer Facts & Figures 2022, the ACS Website, and the International Agency for Research on Cancer Website. Available online: https://www.cancer.org/research/cancer-facts-statistics/all-cancer-facts-figures/cancer-facts-figures-2022.html (accessed on 1 January 2022).
- Talhouk, A.; McConechy, M.K.; Leung, S.; Yang, W.; Lum, A.; Senz, J.; Boyd, N.; Pike, J.; Anglesio, M.; Kwon, J.S.; et al. Confirmation of ProMisE: A simple, genomics-based clinical classifier for endometrial cancer: Molecular Classification of EC. Cancer 2017, 123, 802–813. [Google Scholar] [CrossRef]
- Travaglino, A.; Raffone, A.; Mascolo, M.; Guida, M.; Insabato, L.; Zannoni, G.F.; Zullo, F. Clear cell endometrial carcinoma and the TCGA classification. Histopathology 2020, 76, 336–368. [Google Scholar] [CrossRef] [PubMed]
- The Cancer Genome Atlas Research Network; Levine, D. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Colle, R.; Cohen, R. Épidémiologie des tumeurs MSI: Fréquence des tumeurs MSI en fonction de la localisation du cancer et de son stade. Bull. Cancer 2019, 106, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Meyer, L.A.; Broaddus, R.R.; Lu, K.H. Endometrial Cancer and Lynch Syndrome: Clinical and Pathologic Considerations. Cancer Control. 2009, 16, 14–22. [Google Scholar] [CrossRef]
- Vasen, H.; Wijnen, J.; Menko, F.; Kleibeuker, J.; Taal, B.; Griffioen, G.; Nagengast, F.; Meijers-Heijboer, E.; Bertario, L.; Varesco, L.; et al. Cancer risk in families with hereditary nonpolyposis colorectal cancer diagnosed by mutation analysis. Gastroenterology 1996, 110, 1020–1027. [Google Scholar] [CrossRef]
- Fishel, R.; Kolodner, R.D. Identification of mismatch repair genes and their role in the development of cancer. Curr. Opin. Genet. Dev. 1995, 5, 382–395. [Google Scholar] [CrossRef]
- Ono, R.; Nakayama, K.; Nakamura, K.; Yamashita, H.; Ishibashi, T.; Ishikawa, M.; Minamoto, T.; Razia, S.; Ishikawa, N.; Otsuki, Y.; et al. Dedifferentiated Endometrial Carcinoma Could be A Target for Immune Checkpoint Inhibitors (Anti PD-1/PD-L1 Antibodies). IJMS 2019, 20, 3744. [Google Scholar] [CrossRef] [PubMed]
- Concin, N.; Matias-Guiu, X.; Vergote, I.; Cibula, D.; Mirza, M.R.; Marnitz, S.; Ledermann, J.; Bosse, T.; Chargari, C.; Fagotti, A.; et al. ESGO/ESTRO/ESP guidelines for the management of patients with endometrial carcinoma. Int. J. Gynecol. Cancer 2021, 31, 12–39. [Google Scholar] [CrossRef] [PubMed]
- Vermij, L.; Smit, V.; Nout, R.; Bosse, T. Incorporation of molecular characteristics into endometrial cancer management. Histopathology 2020, 76, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Piskorz, A.M.; Bosse, T.; Jimenez-Linan, M.; Rous, B.; Brenton, J.D.; Gilks, C.B.; Köbel, M. p53 immunohistochemistry is an accurate surrogate for TP53 mutational analysis in endometrial carcinoma biopsies. J. Pathol. 2020, 250, 336–345. [Google Scholar] [CrossRef] [PubMed]
- Jumaah, A.S.; Salim, M.M.; Al-Haddad, H.S.; McAllister, K.A.; Yasseen, A.A. The frequency of POLE-mutation in endometrial carcinoma and prognostic implications: A systemic review and meta-analysis. J. Pathol. Transl. Med. 2020, 54, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhao, L.; Qi, W.; Shen, D.; Li, X.; Wang, J.; Wei, L. Clinical implications and prognostic value of five biomarkers in endometrial carcinoma. Chin.-Ger J. Clin. Oncol. 2013, 12, 586–591. [Google Scholar] [CrossRef]
- Koh, W.-J.; Abu-Rustum, N.R.; Bean, S.; Bradley, K.; Campos, S.M.; Cho, K.R.; Chon, H.S.; Chu, C.; Cohn, D.; Crispens, M.A.; et al. Uterine Neoplasms, Version 1.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc. Netw. 2018, 16, 170–199. [Google Scholar] [CrossRef]
- Raffone, A.; Travaglino, A.; Cerbone, M.; Gencarelli, A.; Mollo, A.; Insabato, L.; Zullo, F. Diagnostic Accuracy of Immunohistochemistry for Mismatch Repair Proteins as Surrogate of Microsatellite Instability Molecular Testing in Endometrial Cancer. Pathol. Oncol. Res. 2020, 26, 1417–1427. [Google Scholar] [CrossRef]
- Simpkins, S.B.; Bocker, T.; Swisher, E.M.; Mutch, D.G.; Gersell, D.J.; Kovatich, A.J.; Palazzo, J.P.; Fishel, R.; Goodfellow, P.J. MLH1 promoter methylation and gene silencing is the primary cause of microsatellite instability in sporadic endometrial cancers. Hum. Mol. Genet. 1999, 8, 661–666. [Google Scholar] [CrossRef]
- Peiró, G.; Diebold, J.; Mayr, D.; Baretton, G.B.; Kimmig, R.; Schmidt, M.; Löhrs, U. Prognostic relevance of hMLH1, hMSH2, and BAX protein expression in endometrial carcinoma. Mod. Pathol. 2001, 14, 777–783. [Google Scholar] [CrossRef][Green Version]
- Maruyama, A.; Miyamoto, S.; Saito, T.; Kondo, H.; Baba, H.; Tsukamoto, N. Clinicopathologic and familial characteristics of endometrial carcinoma with multiple primary carcinomas in relation to the loss of protein expression of MSH2 and MLH1. Cancer 2001, 91, 2056–2064. [Google Scholar] [CrossRef]
- Berends, M.J.; Hollema, H.; Wu, Y.; van Der Sluis, T.; Mensink, R.G.; ten Hoor, K.A.; Sijmons, R.H.; de Vries, E.G.; Pras, E.; Mourits, M.J.; et al. MLH1 and MSH2 protein expression as a pre-screening marker in hereditary and non-hereditary endometrial hyperplasia and cancer. Int J. Cancer 2001, 92, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Chiaravalli, A.M.; Furlan, D.; Facco, C.; Tibiletti, M.G.; Dionigi, A.; Casati, B.; Albarello, L.; Riva, C.; Capella, C. Immunohistochemical pattern of hMSH2/hMLH1 in familial and sporadic colorectal, gastric, endometrial and ovarian carcinomas with instability in microsatellite sequences. Virchows Arch. 2001, 438, 39–48. [Google Scholar] [CrossRef] [PubMed]
- Hardisson, D.; Moreno-Bueno, G.; Sánchez, L.; Sarrió, D.; Suárez, A.; Calero, F.; Palacios, J. Tissue microarray immunohistochemical expression analysis of mismatch repair (hMLH1 and hMSH2 genes) in endometrial carcinoma and atypical endometrial hyperplasia: Relationship with microsatellite instability. Mod. Pathol. 2003, 16, 1148–1158. [Google Scholar] [CrossRef]
- Sutter, C.; Dallenbach-Hellweg, G.; Schmidt, D.; Baehring, J.; Bielau, S.; von Knebel Doeberitz, M.; Gebert, J. Molecular analysis of endometrial hyperplasia in HNPCC-suspicious patients may predict progression to endometrial carcinoma. Int J. Gynecol. Pathol. 2004, 23, 18–25. [Google Scholar] [CrossRef]
- Irving, J.A.; Catasús, L.; Gallardo, A.; Bussaglia, E.; Romero, M.; Matias-Guiu, X.; Prat, J. Synchronous endometrioid carcinomas of the uterine corpus and ovary: Alterations in the beta-catenin (CTNNB1) pathway are associated with independent primary tumors and favorable prognosis. Hum. Pathol. 2005, 36, 605–619. [Google Scholar] [CrossRef]
- Alvarez, T.; Miller, E.; Duska, L.; Oliva, E. Molecular profile of grade 3 endometrioid endometrial carcinoma: Is it a type I or type II endometrial carcinoma? Am. J. Surg. Pathol. 2012, 36, 753–761. [Google Scholar] [CrossRef] [PubMed]
- Plotkin, A.; Kuzeljevic, B.; De Villa, V.; Thompson, E.F.; Gilks, C.B.; Clarke, B.A.; Köbel, M.; McAlpine, J.N. Interlaboratory Concordance of ProMisE Molecular Classification of Endometrial Carcinoma Based on Endometrial Biopsy Specimens. Int. J. Gynecol. Pathol. 2020, 39, 537–545. [Google Scholar] [CrossRef] [PubMed]
- Planck, M.; Rambech, E.; Möslein, G.; Müller, W.; Olsson, H.; Nilbert, M. High frequency of microsatellite instability and loss of mismatch-repair protein expression in patients with double primary tumors of the endometrium and colorectum. Cancer 2002, 94, 2502–2510. [Google Scholar] [CrossRef]
- Orbo, A.; Nilsen, M.N.; Arnes, M.S.; Pettersen, I.; Larsen, K. Loss of expression of MLH1, MSH2, MSH6, and PTEN related to endometrial cancer in 68 patients with endometrial hyperplasia. Int. J. Gynecol. Pathol. 2003, 22, 141–148. [Google Scholar] [CrossRef]
- Lipton, L.R.; Johnson, V.; Cummings, C.; Fisher, S.; Risby, P.; Eftekhar Sadat, A.T.; Cranston, T.; Izatt, L.; Sasieni, P.; Hodgson, S.V.; et al. Refining the Amsterdam Criteria and Bethesda Guidelines: Testing algorithms for the prediction of mismatch repair mutation status in the familial cancer clinic. J. Clin. Oncol. 2004, 22, 4934–4943. [Google Scholar] [CrossRef]
- Macdonald, N.D.; Salvesen, H.B.; Ryan, A.; Malatos, S.; Stefansson, I.; Iversen, O.E.; Akslen, L.A.; Das, S.; Jacobs, I.J. Molecular differences between RER+ and RER- sporadic endometrial carcinomas in a large population-based series. Int. J. Gynecol. Cancer 2004, 14, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Buttin, B.M.; Powell, M.A.; Mutch, D.G.; Rader, J.S.; Herzog, T.J.; Gibb, R.K.; Huettner, P.; Edmonston, T.B.; Goodfellow, P.J. Increased risk for hereditary nonpolyposis colorectal cancer-associated synchronous and metachronous malignancies in patients with microsatellite instability-positive endometrial carcinoma lacking MLH1 promoter methylation. Clin. Cancer Res. 2004, 10, 481–490. [Google Scholar] [CrossRef]
- Soliman, P.T.; Broaddus, R.R.; Schmeler, K.M.; Daniels, M.S.; Gonzalez, D.; Slomovitz, B.M.; Gershenson, D.M.; Lu, K.H. Women with synchronous primary cancers of the endometrium and ovary: Do they have Lynch syndrome? J. Clin. Oncol. 2005, 23, 9344–9350. [Google Scholar] [CrossRef]
- Cederquist, K.; Emanuelsson, M.; Wiklund, F.; Golovleva, I.; Palmqvist, R.; Grönberg, H. Two Swedish founder MSH6 mutations, one nonsense and one missense, conferring high cumulative risk of Lynch syndrome. Clin. Genet. 2005, 68, 533–541. [Google Scholar] [CrossRef] [PubMed]
- Ollikainen, M.; Abdel-Rahman, W.M.; Moisio, A.-L.; Lindroos, A.; Kariola, R.; Järvelä, I.; Pöyhönen, M.; Butzow, R.; Peltomäki, P. Molecular analysis of familial endometrial carcinoma: A manifestation of hereditary nonpolyposis colorectal cancer or a separate syndrome? J. Clin. Oncol. 2005, 23, 4609–4616. [Google Scholar] [CrossRef]
- Taylor, N.P.; Zighelboim, I.; Huettner, P.C.; Powell, M.A.; Gibb, R.K.; Rader, J.S.; Mutch, D.G.; Edmonston, T.B.; Goodfellow, P.J. DNA mismatch repair and TP53 defects are early events in uterine carcinosarcoma tumorigenesis. Mod. Pathol. 2006, 19, 1333–1338. [Google Scholar] [CrossRef]
- Niessen, R.C.; Sijmons, R.H.; Ou, J.; Olthof, S.G.M.; Osinga, J.; Ligtenberg, M.J.; Hogervorst, F.B.L.; Weiss, M.M.; Tops, C.M.J.; Hes, F.J.; et al. MUTYH and the mismatch repair system: Partners in crime? Hum. Genet. 2006, 119, 206–211. [Google Scholar] [CrossRef][Green Version]
- Rijcken, F.; van der Zee, A.; van der Sluis, T.; Boersma-van Ek, W.; Kleibeuker, J.; Hollema, H. Cell cycle regulators and apoptosis-associated proteins in relation to proliferative activity and degree of apoptosis in HNPCC versus sporadic endometrial carcinoma. Histopathology 2006, 48, 275–285. [Google Scholar] [CrossRef]
- Yoon, S.N.; Ku, J.-L.; Shin, Y.-K.; Kim, K.-H.; Choi, J.-S.; Jang, E.-J.; Park, H.-C.; Kim, D.-W.; Kim, M.A.; Kim, W.H.; et al. Hereditary nonpolyposis colorectal cancer in endometrial cancer patients. Int J. Cancer 2008, 122, 1077–1081. [Google Scholar] [CrossRef]
- Arabi, H.; Guan, H.; Kumar, S.; Cote, M.; Bandyopadhyay, S.; Bryant, C.; Shah, J.; Abdul-Karim, F.W.; Munkarah, A.R.; Ali-Fehmi, R. Impact of microsatellite instability (MSI) on survival in high grade endometrial carcinoma. Gynecol. Oncol. 2009, 113, 153–158. [Google Scholar] [CrossRef]
- Walsh, C.S.; Blum, A.; Walts, A.; Alsabeh, R.; Tran, H.; Koeffler, H.P.; Karlan, B.Y. Lynch syndrome among gynecologic oncology patients meeting Bethesda guidelines for screening. Gynecol. Oncol. 2010, 116, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Yasue, A.; Hasegawa, K.; Udagawa, Y. Effects of tamoxifen on the endometrium and its mechanism of carcinogenicity. Hum. Cell 2011, 24, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-W.; Kuo, C.-T.; Chen, J.-H.; Goodfellow, P.J.; Huang, T.H.-M.; Rader, J.S.; Uyar, D.S. Hypermethylation of miR-203 in endometrial carcinomas. Gynecol. Oncol. 2014, 133, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Nakamura, K.; Nomura, H.; Banno, K.; Irie, H.; Adachi, M.; Iida, M.; Umene, K.; Nogami, Y.; Masuda, K.; et al. Clinicopathologic analysis with immunohistochemistry for DNA mismatch repair protein expression in synchronous primary endometrial and ovarian cancers. Int. J. Gynecol. Cancer 2015, 25, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Ren, C.; Liu, Y.; Wang, Y.; Tang, Y.; Wei, Y.; Liu, C.; Zhang, H. Identification of novel Lynch syndrome mutations in Chinese patients with endometriod endometrial cancer. Cancer Biol. Med. 2020, 17, 458–467. [Google Scholar] [CrossRef] [PubMed]
- Westin, S.N.; Lacour, R.A.; Urbauer, D.L.; Luthra, R.; Bodurka, D.C.; Lu, K.H.; Broaddus, R.R. Carcinoma of the lower uterine segment: A newly described association with Lynch syndrome. J. Clin. Oncol. 2008, 26, 5965–5971. [Google Scholar] [CrossRef]
- Matthews, K.S.; Estes, J.M.; Conner, M.G.; Manne, U.; Whitworth, J.M.; Huh, W.K.; Alvarez, R.D.; Straughn, J.M.; Barnes, M.N.; Rocconi, R.P. Lynch syndrome in women less than 50 years of age with endometrial cancer. Obstet. Gynecol. 2008, 111, 1161–1166. [Google Scholar] [CrossRef]
- Garg, K.; Shih, K.; Barakat, R.; Zhou, Q.; Iasonos, A.; Soslow, R.A. Endometrial carcinomas in women aged 40 years and younger: Tumors associated with loss of DNA mismatch repair proteins comprise a distinct clinicopathologic subset. Am. J. Surg. Pathol. 2009, 33, 1869–1877. [Google Scholar] [CrossRef] [PubMed]
- Garg, K.; Leitao, M.M.; Kauff, N.D.; Hansen, J.; Kosarin, K.; Shia, J.; Soslow, R.A. Selection of endometrial carcinomas for DNA mismatch repair protein immunohistochemistry using patient age and tumor morphology enhances detection of mismatch repair abnormalities. Am. J. Surg Pathol. 2009, 33, 925–933. [Google Scholar] [CrossRef]
- Tafe, L.J.; Garg, K.; Chew, I.; Tornos, C.; Soslow, R.A. Endometrial and ovarian carcinomas with undifferentiated components: Clinically aggressive and frequently underrecognized neoplasms. Mod. Pathol. 2010, 23, 781–789. [Google Scholar] [CrossRef]
- Cossio, S.L.; Koehler-Santos, P.; Pessini, S.A.; Mónego, H.; Edelweiss, M.I.; Meurer, L.; Errami, A.; Coffa, J.; Bock, H.; Saraiva-Pereira, M.L.; et al. Clinical and histomolecular endometrial tumor characterization of patients at-risk for Lynch syndrome in South of Brazil. Fam. Cancer 2010, 9, 131–139. [Google Scholar] [CrossRef]
- Resnick, K.E.; Frankel, W.L.; Morrison, C.D.; Fowler, J.M.; Copeland, L.J.; Stephens, J.; Kim, K.H.; Cohn, D.E. Mismatch repair status and outcomes after adjuvant therapy in patients with surgically staged endometrial cancer. Gynecol. Oncol. 2010, 117, 234–238. [Google Scholar] [CrossRef]
- Shih, K.K.; Garg, K.; Levine, D.A.; Kauff, N.D.; Abu-Rustum, N.R.; Soslow, R.A.; Barakat, R.R. Clinicopathologic significance of DNA mismatch repair protein defects and endometrial cancer in women 40years of age and younger. Gynecol. Oncol. 2011, 123, 88–94. [Google Scholar] [CrossRef]
- Leenen, C.H.M.; van Lier, M.G.F.; van Doorn, H.C.; van Leerdam, M.E.; Kooi, S.G.; de Waard, J.; Hoedemaeker, R.F.; van den Ouweland, A.M.W.; Hulspas, S.M.; Dubbink, H.J.; et al. Prospective evaluation of molecular screening for Lynch syndrome in patients with endometrial cancer ≤ 70 years. Gynecol. Oncol. 2012, 125, 414–420. [Google Scholar] [CrossRef]
- Soslow, R.A.; Wethington, S.L.; Cesari, M.; Chiappetta, D.; Olvera, N.; Shia, J.; Levine, D.A. Clinicopathologic analysis of matched primary and recurrent endometrial carcinoma. Am. J. Surg. Pathol. 2012, 36, 1771–1781. [Google Scholar] [CrossRef]
- Egoavil, C.; Alenda, C.; Castillejo, A.; Paya, A.; Peiro, G.; Sánchez-Heras, A.-B.; Castillejo, M.-I.; Rojas, E.; Barberá, V.-M.; Cigüenza, S.; et al. Prevalence of Lynch syndrome among patients with newly diagnosed endometrial cancers. PLoS ONE 2013, 8, e79737. [Google Scholar] [CrossRef]
- Bosse, T.; ter Haar, N.T.; Seeber, L.M.; v Diest, P.J.; Hes, F.J.; Vasen, H.F.A.; Nout, R.A.; Creutzberg, C.L.; Morreau, H.; Smit, V.T.H.B.M. Loss of ARID1A expression and its relationship with PI3K-Akt pathway alterations, TP53 and microsatellite instability in endometrial cancer. Mod. Pathol 2013, 26, 1525–1535. [Google Scholar] [CrossRef]
- Moline, J.; Mahdi, H.; Yang, B.; Biscotti, C.; Roma, A.A.; Heald, B.; Rose, P.G.; Michener, C.; Eng, C. Implementation of tumor testing for lynch syndrome in endometrial cancers at a large academic medical center. Gynecol. Oncol. 2013, 130, 121–126. [Google Scholar] [CrossRef]
- Peiró, G.; Peiró, F.M.; Ortiz-Martínez, F.; Planelles, M.; Sánchez-Tejada, L.; Alenda, C.; Ceballos, S.; Sánchez-Payá, J.; Laforga, J.B. Association of mammalian target of rapamycin with aggressive type II endometrial carcinomas and poor outcome: A potential target treatment. Hum. Pathol. 2013, 44, 218–225. [Google Scholar] [CrossRef]
- Romero-Pérez, L.; López-García, M.Á.; Díaz-Martín, J.; Biscuola, M.; Castilla, M.Á.; Tafe, L.J.; Garg, K.; Oliva, E.; Matias-Guiu, X.; Soslow, R.A.; et al. ZEB1 overexpression associated with E-cadherin and microRNA-200 downregulation is characteristic of undifferentiated endometrial carcinoma. Mod. Pathol. 2013, 26, 1514–1524. [Google Scholar] [CrossRef]
- Mills, A.M.; Liou, S.; Ford, J.M.; Berek, J.S.; Pai, R.K.; Longacre, T.A. Lynch syndrome screening should be considered for all patients with newly diagnosed endometrial cancer. Am. J. Surg. Pathol. 2014, 38, 1501–1509. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, I.; Martín-Arruti, M.; Lopez-Lopez, E.; Garcia-Orad, A. Lack of association between deficient mismatch repair expression and outcome in endometrial carcinomas of the endometrioid type. Gynecol. Oncol. 2014, 134, 20–23. [Google Scholar] [CrossRef] [PubMed]
- Thoury, A.; Descatoire, V.; Kotelevets, L.; Kannengiesser, C.; Bertrand, G.; Theou-Anton, N.; Frey, C.; Genestie, C.; Raymond, E.; Chastre, E.; et al. Evidence for different expression profiles for c-Met, EGFR, PTEN and the mTOR pathway in low and high grade endometrial carcinomas in a cohort of consecutive women. Occurrence of PIK3CA and K-Ras mutations and microsatellite instability. Histol. Histopathol. 2014, 29, 1455–1466. [Google Scholar] [CrossRef] [PubMed]
- Rabban, J.T.; Calkins, S.M.; Karnezis, A.N.; Grenert, J.P.; Blanco, A.; Crawford, B.; Chen, L.-M. Association of tumor morphology with mismatch-repair protein status in older endometrial cancer patients: Implications for universal versus selective screening strategies for Lynch syndrome. Am. J. Surg. Pathol. 2014, 38, 793–800. [Google Scholar] [CrossRef]
- Long, Q.; Peng, Y.; Tang, Z.; Wu, C. Role of endometrial cancer abnormal MMR protein in screening Lynch-syndrome families. Int. J. Clin. Exp. Pathol. 2014, 7, 7297–7303. [Google Scholar]
- Woo, Y.L.; Cheah, P.L.; Shahruddin, S.I.; Omar, S.Z.; Arends, M. The immunohistochemistry signature of mismatch repair (MMR) proteins in a multiethnic Asian cohort with endometrial carcinoma. Int. J. Gynecol. Pathol. 2014, 33, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Hoang, L.N.; Ali, R.H.; Lau, S.; Gilks, C.B.; Lee, C.-H. Immunohistochemical survey of mismatch repair protein expression in uterine sarcomas and carcinosarcomas. Int. J. Gynecol. Pathol. 2014, 33, 483–491. [Google Scholar] [CrossRef]
- Buchanan, D.D.; Tan, Y.Y.; Walsh, M.D.; Clendenning, M.; Metcalf, A.M.; Ferguson, K.; Arnold, S.T.; Thompson, B.A.; Lose, F.A.; Parsons, M.T.; et al. Tumor mismatch repair immunohistochemistry and DNA MLH1 methylation testing of patients with endometrial cancer diagnosed at age younger than 60 years optimizes triage for population-level germline mismatch repair gene mutation testing. J. Clin. Oncol. 2014, 32, 90–100. [Google Scholar] [CrossRef]
- Allo, G.; Bernardini, M.Q.; Wu, R.-C.; Shih, I.-M.; Kalloger, S.; Pollett, A.; Gilks, C.B.; Clarke, B.A. ARID1A loss correlates with mismatch repair deficiency and intact p53 expression in high-grade endometrial carcinomas. Mod. Pathol. 2014, 27, 255–261. [Google Scholar] [CrossRef]
- Goodfellow, P.J.; Billingsley, C.C.; Lankes, H.A.; Ali, S.; Cohn, D.E.; Broaddus, R.J.; Ramirez, N.; Pritchard, C.C.; Hampel, H.; Chassen, A.S.; et al. Combined Microsatellite Instability, MLH1 Methylation Analysis, and Immunohistochemistry for Lynch Syndrome Screening in Endometrial Cancers From GOG210: An NRG Oncology and Gynecologic Oncology Group Study. J. Clin. Oncol. 2015, 33, 4301–4308. [Google Scholar] [CrossRef]
- Chu, M.M.-Y.; Liu, S.S.; Tam, K.-F.; Ip, P.P.-C.; Cheung, A.N.-Y.; Ngan, H.Y.-S. The Significance of Mismatch Repair Deficiency in Young Patients With Endometrial Cancer. Int. J. Gynecol. Pathol. 2015, 34, 403–410. [Google Scholar] [CrossRef] [PubMed]
- Graham, R.P.; Kerr, S.E.; Butz, M.L.; Thibodeau, S.N.; Halling, K.C.; Smyrk, T.C.; Dina, M.A.; Waugh, V.M.; Rumilla, K.M. Heterogenous MSH6 loss is a result of microsatellite instability within MSH6 and occurs in sporadic and hereditary colorectal and endometrial carcinomas. Am. J. Surg. Pathol. 2015, 39, 1370–1376. [Google Scholar] [CrossRef] [PubMed]
- Dudley, B.; Brand, R.E.; Thull, D.; Bahary, N.; Nikiforova, M.N.; Pai, R.K. Germline MLH1 Mutations Are Frequently Identified in Lynch Syndrome Patients With Colorectal and Endometrial Carcinoma Demonstrating Isolated Loss of PMS2 Immunohistochemical Expression. Am. J. Surg. Pathol. 2015, 39, 1114–1120. [Google Scholar] [CrossRef]
- Stelloo, E.; Bosse, T.; Nout, R.A.; MacKay, H.J.; Church, D.N.; Nijman, H.W.; Leary, A.; Edmondson, R.J.; Powell, M.E.; Crosbie, E.J.; et al. Refining prognosis and identifying targetable pathways for high-risk endometrial cancer, a TransPORTEC initiative. Mod. Pathol. 2015, 28, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Mao, T.-L.; Ayhan, A.; Kuo, K.-T.; Lin, M.-C.; Tseng, L.-H.; Ogawa, H. Immunohistochemical study of endometrial high-grade endometrioid carcinoma with or without a concurrent low-grade component: Implications for pathogenetic and survival differences. Histopathology 2015, 67, 474–482. [Google Scholar] [CrossRef] [PubMed]
- McConechy, M.K.; Talhouk, A.; Li-Chang, H.H.; Leung, S.; Huntsman, D.G.; Gilks, C.B.; McAlpine, J.N. Detection of DNA mismatch repair (MMR) deficiencies by immunohistochemistry can effectively diagnose the microsatellite instability (MSI) phenotype in endometrial carcinomas. Gynecol. Oncol. 2015, 137, 306–310. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.J.R.; Crook, M.L. SWI/SNF complex deficiency and mismatch repair protein expression in undifferentiated and dedifferentiated endometrial carcinoma. Pathology 2015, 47, 439–445. [Google Scholar] [CrossRef]
- Watkins, J.C.; Nucci, M.R.; Ritterhouse, L.L.; Howitt, B.E.; Sholl, L.M. Unusual Mismatch Repair Immunohistochemical Patterns in Endometrial Carcinoma. Am. J. Surg Pathol. 2016, 40, 909–916. [Google Scholar] [CrossRef]
- Pocrnich, C.E.; Ramalingam, P.; Euscher, E.D.; Malpica, A. Neuroendocrine Carcinoma of the Endometrium: A Clinicopathologic Study of 25 Cases. Am. J. Surg Pathol. 2016, 40, 577–586. [Google Scholar] [CrossRef]
- Lin, D.I.; Hecht, J.L. Targeted Screening With Combined Age- and Morphology-Based Criteria Enriches Detection of Lynch Syndrome in Endometrial Cancer. Int. J. Surg. Pathol. 2016, 24, 297–305. [Google Scholar] [CrossRef]
- Mills, A.M.; Sloan, E.A.; Thomas, M.; Modesitt, S.C.; Stoler, M.H.; Atkins, K.A.; Moskaluk, C.A. Clinicopathologic Comparison of Lynch Syndrome-associated and ‘Lynch-like’ Endometrial Carcinomas Identified on Universal Screening Using Mismatch Repair Protein Immunohistochemistry. Am. J. Surg. Pathol. 2016, 40, 155–165. [Google Scholar] [CrossRef] [PubMed]
- Ramalingam, P.; Masand, R.P.; Euscher, E.D.; Malpica, A. Undifferentiated Carcinoma of the Endometrium: An Expanded Immunohistochemical Analysis Including PAX-8 and Basal-Like Carcinoma Surrogate Markers. Int. J. Gynecol. Pathol. 2016, 35, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Shikama, A.; Minaguchi, T.; Matsumoto, K.; Akiyama-Abe, A.; Nakamura, Y.; Michikami, H.; Nakao, S.; Sakurai, M.; Ochi, H.; Onuki, M.; et al. Clinicopathologic implications of DNA mismatch repair status in endometrial carcinomas. Gynecol. Oncol. 2016, 140, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Kato, A.; Sato, N.; Sugawara, T.; Takahashi, K.; Kito, M.; Makino, K.; Sato, T.; Shimizu, D.; Shirasawa, H.; Miura, H.; et al. Isolated Loss of PMS2 Immunohistochemical Expression is Frequently Caused by Heterogenous MLH1 Promoter Hypermethylation in Lynch Syndrome Screening for Endometrial Cancer Patients. Am. J. Surg. Pathol. 2016, 40, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Okoye, E.I.; Bruegl, A.S.; Fellman, B.; Luthra, R.; Broaddus, R.R. Defective DNA Mismatch Repair Influences Expression of Endometrial Carcinoma Biomarkers. Int. J. Gynecol. Pathol. 2016, 35, 8–15. [Google Scholar] [CrossRef]
- Russo, M.; Broach, J.; Sheldon, K.; Houser, K.R.; Liu, D.J.; Kesterson, J.; Phaeton, R.; Hossler, C.; Hempel, N.; Baker, M.; et al. Clonal evolution in paired endometrial intraepithelial neoplasia/atypical hyperplasia and endometrioid adenocarcinoma. Hum. Pathol. 2017, 67, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Bregar, A.; Deshpande, A.; Grange, C.; Zi, T.; Stall, J.; Hirsch, H.; Reeves, J.; Sathyanarayanan, S.; Growdon, W.B.; Rueda, B.R. Characterization of immune regulatory molecules B7-H4 and PD-L1 in low and high grade endometrial tumors. Gynecol. Oncol. 2017, 145, 446–452. [Google Scholar] [CrossRef]
- Pelletier, M.P.; Trinh, V.Q.; Stephenson, P.; Mes-Masson, A.-M.; Samouelian, V.; Provencher, D.M.; Rahimi, K. Microcystic, elongated, and fragmented pattern invasion is mainly associated with isolated tumor cell pattern metastases in International Federation of Gynecology and Obstetrics grade I endometrioid endometrial cancer. Hum. Pathol. 2017, 62, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Stelloo, E.; Jansen, A.M.L.; Osse, E.M.; Nout, R.A.; Creutzberg, C.L.; Ruano, D.; Church, D.N.; Morreau, H.; Smit, V.T.H.B.M.; van Wezel, T.; et al. Practical guidance for mismatch repair-deficiency testing in endometrial cancer. Ann. Oncol. 2017, 28, 96–102. [Google Scholar] [CrossRef] [PubMed]
- Dillon, J.L.; Gonzalez, J.L.; DeMars, L.; Bloch, K.J.; Tafe, L.J. Universal screening for Lynch syndrome in endometrial cancers: Frequency of germline mutations and identification of patients with Lynch-like syndrome. Hum. Pathol. 2017, 70, 121–128. [Google Scholar] [CrossRef]
- Tangjitgamol, S.; Kittisiam, T.; Tanvanich, S. Prevalence and prognostic role of mismatch repair gene defect in endometrial cancer patients. Tumour. Biol. 2017, 39, 1010428317725834. [Google Scholar] [CrossRef] [PubMed]
- Zakhour, M.; Cohen, J.G.; Gibson, A.; Walts, A.E.; Karimian, B.; Baltayan, A.; Aoyama, C.; Garcia, L.; Dhaliwal, S.K.; Elashoff, D.; et al. Abnormal mismatch repair and other clinicopathologic predictors of poor response to progestin treatment in young women with endometrial complex atypical hyperplasia and well-differentiated endometrial adenocarcinoma: A consecutive case series. BJOG 2017, 124, 1576–1583. [Google Scholar] [CrossRef] [PubMed]
- Najdawi, F.; Crook, A.; Maidens, J.; McEvoy, C.; Fellowes, A.; Pickett, J.; Ho, M.; Nevell, D.; McIlroy, K.; Sheen, A.; et al. Lessons learnt from implementation of a Lynch syndrome screening program for patients with gynaecological malignancy. Pathology 2017, 49, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Sloan, E.A.; Ring, K.L.; Willis, B.C.; Modesitt, S.C.; Mills, A.M. PD-L1 Expression in Mismatch Repair-deficient Endometrial Carcinomas, Including Lynch Syndrome-associated and MLH1 Promoter Hypermethylated Tumors. Am. J. Surg. Pathol. 2017, 41, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Watkins, J.C.; Yang, E.J.; Muto, M.G.; Feltmate, C.M.; Berkowitz, R.S.; Horowitz, N.S.; Syngal, S.; Yurgelun, M.B.; Chittenden, A.; Hornick, J.L.; et al. Universal Screening for Mismatch-Repair Deficiency in Endometrial Cancers to Identify Patients With Lynch Syndrome and Lynch-like Syndrome. Int. J. Gynecol. Pathol. 2017, 36, 115–127. [Google Scholar] [CrossRef]
- Chen, W.; Husain, A.; Nelson, G.S.; Rambau, P.F.; Liu, S.; Lee, C.-H.; Lee, S.; Duggan, M.A.; Köbel, M. Immunohistochemical Profiling of Endometrial Serous Carcinoma. Int. J. Gynecol. Pathol. 2017, 36, 128–139. [Google Scholar] [CrossRef]
- Köbel, M.; Meng, B.; Hoang, L.N.; Almadani, N.; Li, X.; Soslow, R.A.; Gilks, C.B.; Lee, C.-H. Molecular Analysis of Mixed Endometrial Carcinomas Shows Clonality in Most Cases. Am. J. Surg. Pathol. 2016, 40, 166–180. [Google Scholar] [CrossRef]
- Pina, A.; Wolber, R.; McAlpine, J.N.; Gilks, B.; Kwon, J.S. Endometrial Cancer Presentation and Outcomes Based on Mismatch Repair Protein Expression From a Population-Based Study. Int. J. Gynecol. Cancer 2018, 28, 1624–1630. [Google Scholar] [CrossRef]
- Adar, T.; Rodgers, L.H.; Shannon, K.M.; Yoshida, M.; Ma, T.; Mattia, A.; Lauwers, G.Y.; Iafrate, A.J.; Hartford, N.M.; Oliva, E.; et al. Universal screening of both endometrial and colon cancers increases the detection of Lynch syndrome. Cancer 2018, 124, 3145–3153. [Google Scholar] [CrossRef]
- Chapel, D.B.; Yamada, S.D.; Cowan, M.; Lastra, R.R. Immunohistochemistry for mismatch repair protein deficiency in endometrioid endometrial carcinoma yields equivalent results when performed on endometrial biopsy/curettage or hysterectomy specimens. Gynecol. Oncol. 2018, 149, 570–574. [Google Scholar] [CrossRef]
- Bosse, T.; Nout, R.A.; McAlpine, J.N.; McConechy, M.K.; Britton, H.; Hussein, Y.R.; Gonzalez, C.; Ganesan, R.; Steele, J.C.; Harrison, B.T.; et al. Molecular Classification of Grade 3 Endometrioid Endometrial Cancers Identifies Distinct Prognostic Subgroups. Am. J. Surg. Pathol. 2018, 42, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Saita, C.; Yamaguchi, T.; Horiguchi, S.-I.; Yamada, R.; Takao, M.; Iijima, T.; Wakaume, R.; Aruga, T.; Tabata, T.; Koizumi, K. Tumor development in Japanese patients with Lynch syndrome. PLoS ONE 2018, 13, e0195572. [Google Scholar] [CrossRef] [PubMed]
- Espinosa, I.; De Leo, A.; D’Angelo, E.; Rosa-Rosa, J.M.; Corominas, M.; Gonzalez, A.; Palacios, J.; Prat, J. Dedifferentiated endometrial carcinomas with neuroendocrine features: A clinicopathologic, immunohistochemical, and molecular genetic study. Hum. Pathol. 2018, 72, 100–106. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Joehlin-Price, A.S.; Rhoades, J.; Ayoola-Adeola, M.; Miller, K.; Parwani, A.V.; Backes, F.J.; Felix, A.S.; Suarez, A.A. Programmed Death Ligand 1 Expression Among 700 Consecutive Endometrial Cancers: Strong Association With Mismatch Repair Protein Deficiency. Int. J. Gynecol. Cancer 2018, 28, 59–68. [Google Scholar] [CrossRef] [PubMed]
- Doghri, R.; Houcine, Y.; Boujelbène, N.; Driss, M.; Charfi, L.; Abbes, I.; Mrad, K.; Sellami, R. Mismatch Repair Deficiency in Endometrial Cancer, Immunohistochemistry Staining and Clinical Implications. Appl. Immunohistochem. Mol. Morphol. 2019, 27, 678–682. [Google Scholar] [CrossRef]
- Hashmi, A.A.; Mudassir, G.; Hashmi, R.N.; Irfan, M.; Asif, H.; Khan, E.Y.; Abu Bakar, S.M.; Faridi, N. Microsatellite Instability in Endometrial Carcinoma by Immunohistochemistry.y, Association with Clinical and Histopathologic Parameters. Asian Pac. J. Cancer Prev. 2019, 20, 2601–2606. [Google Scholar] [CrossRef] [PubMed]
- Saeki, H.; Hlaing, M.T.; Horimoto, Y.; Kajino, K.; Ohtsuji, N.; Fujino, K.; Terao, Y.; Hino, O. Usefulness of immunohistochemistry for mismatch repair protein and microsatellite instability examination in adenocarcinoma and background endometrium of sporadic endometrial cancer cases. J. Obstet. Gynaecol. Res. 2019, 45, 2037–2042. [Google Scholar] [CrossRef] [PubMed]
- Zannoni, G.F.; Santoro, A.; Angelico, G.; Spadola, S.; Arciuolo, D.; Valente, M.; Inzani, F.; Pettinato, A.; Vatrano, S.; Fanfani, F.; et al. Clear cell carcinoma of the endometrium: An immunohistochemical and molecular analysis of 45 cases. Hum. Pathol. 2019, 92, 10–17. [Google Scholar] [CrossRef]
- Abdulfatah, E.; Wakeling, E.; Sakr, S.; Al-Obaidy, K.; Bandyopadhyay, S.; Morris, R.; Feldman, G.; Ali-Fehmi, R. Molecular classification of endometrial carcinoma applied to endometrial biopsy specimens: Towards early personalized patient management. Gynecol. Oncol. 2019, 154, 467–474. [Google Scholar] [CrossRef]
- Chapel, D.B.; Patil, S.A.; Plagov, A.; Puranik, R.; Mendybaeva, A.; Steinhardt, G.; Wanjari, P.; Lastra, R.R.; Kadri, S.; Segal, J.P.; et al. Quantitative next-generation sequencing-based analysis indicates progressive accumulation of microsatellite instability between atypical hyperplasia/endometrial intraepithelial neoplasia and paired endometrioid endometrial carcinoma. Mod. Pathol. 2019, 32, 1508–1520. [Google Scholar] [CrossRef]
- Kahn, R.M.; Gordhandas, S.; Maddy, B.P.; Baltich Nelson, B.; Askin, G.; Christos, P.J.; Caputo, T.A.; Chapman-Davis, E.; Holcomb, K.; Frey, M.K. Universal endometrial cancer tumor typing: How much has immunohistochemistry, microsatellite instability, and MLH1 methylation improved the diagnosis of Lynch syndrome across the population? Cancer 2019, 125, 3172–3183. [Google Scholar] [CrossRef] [PubMed]
- Ryan, N.A.J.; Glaire, M.A.; Blake, D.; Cabrera-Dandy, M.; Evans, D.G.; Crosbie, E.J. The proportion of endometrial cancers associated with Lynch syndrome: A systematic review of the literature and meta-analysis. Genet. Med. 2019, 21, 2167–2180. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Snir, O.; Rottmann, D.; Wong, S.; Buza, N.; Hui, P. Minimal microsatellite shift in microsatellite instability high endometrial cancer: A significant pitfall in diagnostic interpretation. Mod. Pathol. 2019, 32, 650–658. [Google Scholar] [CrossRef] [PubMed]
- Saijo, M.; Nakamura, K.; Ida, N.; Nasu, A.; Yoshino, T.; Masuyama, H.; Yanai, H. Histologic Appearance and Immunohistochemistry of DNA Mismatch Repair Protein and p53 in Endometrial Carcinosarcoma: Impact on Prognosis and Insights Into Tumorigenesis. Am. J. Surg. Pathol. 2019, 43, 1493–1500. [Google Scholar] [CrossRef]
- Sarode, V.R.; Robinson, L. Screening for Lynch Syndrome by Immunohistochemistry of Mismatch Repair Proteins: Significance of Indeterminate Result and Correlation With Mutational Studies. Arch. Pathol. Lab. Med. 2019, 143, 1225–1233. [Google Scholar] [CrossRef]
- Sari, A.; Pollett, A.; Eiriksson, L.R.; Lumsden-Johanson, B.; Van de Laar, E.; Kazerouni, H.; Salehi, A.; Sur, M.; Lytwyn, A.; Ferguson, S.E. Interobserver Agreement for Mismatch Repair Protein Immunohistochemistry in Endometrial and Nonserous, Nonmucinous Ovarian Carcinomas. Am. J. Surg. Pathol. 2019, 43, 591–600. [Google Scholar] [CrossRef]
- Lucas, E.; Chen, H.; Molberg, K.; Castrillon, D.H.; Rivera Colon, G.; Li, L.; Hinson, S.; Thibodeaux, J.; Lea, J.; Miller, D.S.; et al. Mismatch Repair Protein Expression in Endometrioid Intraepithelial Neoplasia/Atypical Hyperplasia: Should We Screen for Lynch Syndrome in Precancerous Lesions? Int. J. Gynecol. Pathol. 2019, 38, 533–542. [Google Scholar] [CrossRef]
- Baniak, N.; Fadare, O.; Köbel, M.; DeCoteau, J.; Parkash, V.; Hecht, J.L.; Hanley, K.Z.; Gwin, K.; Zheng, W.; Quick, C.M.; et al. Targeted Molecular and Immunohistochemical Analyses of Endometrial Clear Cell Carcinoma Show that POLE Mutations and DNA Mismatch Repair Protein Deficiencies Are Uncommon. Am. J. Surg. Pathol. 2019, 43, 531–537. [Google Scholar] [CrossRef]
- Backes, F.J.; Haag, J.; Cosgrove, C.M.; Suarez, A.; Cohn, D.E.; Goodfellow, P.J. Mismatch repair deficiency identifies patients with high-intermediate-risk (HIR) endometrioid endometrial cancer at the highest risk of recurrence: A prognostic biomarker. Cancer 2019, 125, 398–405. [Google Scholar] [CrossRef]
- Dong, F.; Costigan, D.C.; Howitt, B.E. Targeted next-generation sequencing in the detection of mismatch repair deficiency in endometrial cancers. Mod. Pathol. 2019, 32, 252–257. [Google Scholar] [CrossRef]
- Gan, Q.; Crumley, S.; Broaddus, R.R. Molecular Modifiers of Hormone Receptor Action: Decreased Androgen Receptor Expression in Mismatch Repair Deficient Endometrial Endometrioid Adenocarcinoma. Int. J. Gynecol. Pathol. 2019, 38, 44–51. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Tao, X.; Huang, F.; Jia, N.; Du, Y.; Yu, J.; Feng, W. Clinicopathologic features of endometrial cancer in Chinese patients younger than 50 years with a family history of cancer. Medicine (Baltimore) 2018, 97, e12968. [Google Scholar] [CrossRef]
- Ryan, N.A.J.; McMahon, R.; Tobi, S.; Snowsill, T.; Esquibel, S.; Wallace, A.J.; Bunstone, S.; Bowers, N.; Mosneag, I.E.; Kitson, S.J.; et al. The proportion of endometrial tumours associated with Lynch syndrome (PETALS): A prospective cross-sectional study. PLoS Med. 2020, 17, e1003263. [Google Scholar] [CrossRef]
- Rosa, R.C.A.; Santis, J.O.; Teixeira, L.A.; Molfetta, G.A.; Dos Santos, J.T.T.; Ribeiro, V.D.S.; Chahud, F.; Ribeiro-Silva, A.; Brunaldi, M.O.; Silva, W.A.; et al. Lynch syndrome identification in a Brazilian cohort of endometrial cancer screened by a universal approach. Gynecol. Oncol. 2020, 159, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Beinse, G.; Rance, B.; Just, P.-A.; Izac, B.; Letourneur, F.; Saidu, N.E.B.; Chouzenoux, S.; Nicco, C.; Goldwasser, F.; Batteux, F.; et al. Identification of TP53 mutated group using a molecular and immunohistochemical classification of endometrial carcinoma to improve prognostic evaluation for adjuvant treatments. Int. J. Gynecol. Cancer 2020, 30, 640–647. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, S.; Van Rompuy, A.S.; Van Gorp, T.; Vanden Bempt, I.; Brems, H.; Van Nieuwenhuysen, E.; Han, S.N.; Neven, P.; Victoor, J.; Laenen, A.; et al. Analysis of 108 patients with endometrial carcinoma using the PROMISE classification and additional genetic analyses for MMR-D. Gynecol. Oncol. 2020, 157, 245–251. [Google Scholar] [CrossRef]
- Missaoui, N.; Boukhari, N.; Limam, S.; Hmissa, S.; Mokni, M. Utility of the immunohistochemical analysis of DNA mismatch-repair proteins in endometrial hyperplasia. Acta Histochem. 2020, 122, 151505. [Google Scholar] [CrossRef]
- Dasgupta, S.; Ewing-Graham, P.C.; Groenendijk, F.H.; Stam, O.; Biermann, K.E.; Doukas, M.; Dubbink, H.J.; van Velthuysen, M.F.; Dinjens, W.N.M.; Van Bockstal, M.R. Granular dot-like staining with MLH1 immunohistochemistry is a clone-dependent artefact. Pathol. Res. Pract. 2020, 216, 152581. [Google Scholar] [CrossRef]
- Kolehmainen, A.M.; Pasanen, A.M.; Koivisto-Korander, R.L.; Bützow, R.C.; Loukovaara, M.J. Molecular characterization in the prediction of disease extent in endometrial carcinoma. Eur. J. Obstet. Gynecol. Reprod Biol. 2021, 256, 478–483. [Google Scholar] [CrossRef]
- León-Castillo, A.; de Boer, S.M.; Powell, M.E.; Mileshkin, L.R.; Mackay, H.J.; Leary, A.; Nijman, H.W.; Singh, N.; Pollock, P.M.; Bessette, P.; et al. Molecular Classification of the PORTEC-3 Trial for High-Risk Endometrial Cancer, Impact on Prognosis and Benefit From Adjuvant Therapy. J. Clin. Oncol. 2020, 38, 3388–3397. [Google Scholar] [CrossRef]
- Rekhi, B.; Menon, S.; Deodhar, K.K.; Ghosh, J.; Chopra, S.; Maheshwari, A. Clinicopathological features of 50 mismatch repair (MMR)-deficient endometrial carcinomas, tested by immunohistochemistry: A single institutional feasibility study, India. Ann. Diagn Pathol. 2020, 47, 151558. [Google Scholar] [CrossRef]
- Kim, S.R.; Cloutier, B.T.; Leung, S.; Cochrane, D.; Britton, H.; Pina, A.; Storness-Bliss, C.; Farnell, D.; Huang, L.; Shum, K.; et al. Molecular subtypes of clear cell carcinoma of the endometrium: Opportunities for prognostic and predictive stratification. Gynecol. Oncol. 2020, 158, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Pasanen, A.; Ahvenainen, T.; Pellinen, T.; Vahteristo, P.; Loukovaara, M.; Bützow, R. PD-L1 Expression in Endometrial Carcinoma Cells and Intratumoral Immune Cells: Differences Across Histologic and TCGA-based Molecular Subgroups. Am. J. Surg. Pathol. 2020, 44, 174–181. [Google Scholar] [CrossRef] [PubMed]
- Jin, C.; Hacking, S.; Liang, S.; Nasim, M. PD-L1/PD-1 Expression in Endometrial Clear Cell Carcinoma: A Potential Surrogate Marker for Clinical Trials. Int. J. Surg. Pathol. 2020, 28, 31–37. [Google Scholar] [CrossRef]
- Rowe, M.; Krishnan, R.; Mills, A.; Ring, K. β-catenin and PD-L1 expression in mismatch repair deficient endometrial carcinomas. Int. J. Gynecol. Cancer 2020, 30, 993–999. [Google Scholar] [CrossRef] [PubMed]
- Stinton, C.; Fraser, H.; Al-Khudairy, L.; Court, R.; Jordan, M.; Grammatopoulos, D.; Taylor-Phillips, S. Testing for lynch syndrome in people with endometrial cancer using immunohistochemistry and microsatellite instability-based testing strategies-A systematic review of test accuracy. Gynecol. Oncol. 2021, 160, 148–160. [Google Scholar] [CrossRef]
- Pécriaux, A.; Favre, L.; Calderaro, J.; Charpy, C.; Derman, J.; Pujals, A. Detection of microsatellite instability in a panel of solid tumours with the Idylla MSI Test using extracted DNA. J. Clin. Pathol. 2021, 74, 36–42. [Google Scholar] [CrossRef]
- Tjalsma, A.S.; Wagner, A.; Dinjens, W.N.M.; Ewing-Graham, P.C.; Alcalá, L.S.M.; de Groot, M.E.R.; Hamoen, K.E.; van Hof, A.C.; Hofhuis, W.; Hofman, L.N.; et al. Evaluation of a nationwide Dutch guideline to detect Lynch syndrome in patients with endometrial cancer. Gynecol. Oncol. 2021, 160, 771–776. [Google Scholar] [CrossRef]
- Joehlin-Price, A.; Van Ziffle, J.; Hills, N.K.; Ladwig, N.; Rabban, J.T.; Garg, K. Molecularly Classified Uterine FIGO Grade 3 Endometrioid Carcinomas Show Distinctive Clinical Outcomes But Overlapping Morphologic Features. Am. J. Surg. Pathol. 2021, 45, 421–429. [Google Scholar] [CrossRef]
- Yamamoto, A.; Yamaguchi, T.; Suzuki, O.; Ito, T.; Chika, N.; Kamae, N.; Tamaru, J.-I.; Nagai, T.; Seki, H.; Arai, T.; et al. Prevalence and molecular characteristics of DNA mismatch repair deficient endometrial cancer in a Japanese hospital-based population. Jpn J. Clin. Oncol. 2021, 51, 60–69. [Google Scholar] [CrossRef]
- McConechy, M.K.; Talhouk, A.; Leung, S.; Chiu, D.; Yang, W.; Senz, J.; Reha-Krantz, L.J.; Lee, C.-H.; Huntsman, D.G.; Gilks, C.B.; et al. Endometrial Carcinomas with POLE Exonuclease Domain Mutations Have a Favorable Prognosis. Clin. Cancer Res. 2016, 22, 2865–2873. [Google Scholar] [CrossRef] [PubMed]
- Horowitz, N.; Pinto, K.; Mutch, D.G.; Herzog, T.J.; Rader, J.S.; Gibb, R.; Bocker-Edmonston, T.; Goodfellow, P.J. Microsatellite instability, MLH1 promoter methylation, and loss of mismatch repair in endometrial cancer and concomitant atypical hyperplasia. Gynecol. Oncol. 2002, 86, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Strazzullo, M.; Cossu, A.; Baldinu, P.; Colombino, M.; Satta, M.P.; Tanda, F.; De Bonis, M.L.; Cerase, A.; D’Urso, M.; D’Esposito, M.; et al. High-resolution methylation analysis of the hMLH1 promoter in sporadic endometrial and colorectal carcinomas. Cancer 2003, 98, 1540–1546. [Google Scholar] [CrossRef]
- Kanaya, T.; Kyo, S.; Sakaguchi, J.; Maida, Y.; Nakamura, M.; Takakura, M.; Hashimoto, M.; Mizumoto, Y.; Inoue, M. Association of mismatch repair deficiency with PTEN frameshift mutations in endometrial cancers and the precursors in a Japanese population. Am. J. Clin. Pathol. 2005, 124, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Zighelboim, I.; Powell, M.A.; Babb, S.A.; Whelan, A.J.; Schmidt, A.P.; Clendenning, M.; Senter, L.; Thibodeau, S.N.; de la Chapelle, A.; Goodfellow, P.J. Epitope-positive truncating MLH1 mutation and loss of PMS2: Implications for IHC-directed genetic testing for Lynch syndrome. Fam. Cancer 2009, 8, 501–504. [Google Scholar] [CrossRef] [PubMed]
- Koyamatsu, Y.; Sakamoto, M.; Miyake, K.; Muroya, T.; Sugano, K.; Nakao, Y.; Yokoyama, M.; Iwasaka, T. Gene expression profiles and microsatellite instability in uterine corpus endometrioid adenocarcinoma. J. Obstet. Gynaecol. Res. 2010, 36, 336–343. [Google Scholar] [CrossRef]
- Batte, B.A.L.; Bruegl, A.S.; Daniels, M.S.; Ring, K.L.; Dempsey, K.M.; Djordjevic, B.; Luthra, R.; Fellman, B.M.; Lu, K.H.; Broaddus, R.R. Consequences of universal MSI/IHC in screening ENDOMETRIAL cancer patients for Lynch syndrome. Gynecol. Oncol. 2014, 134, 319–325. [Google Scholar] [CrossRef]
- Bruegl, A.S.; Djordjevic, B.; Urbauer, D.L.; Westin, S.N.; Soliman, P.T.; Lu, K.H.; Luthra, R.; Broaddus, R.R. Utility of MLH1 methylation analysis in the clinical evaluation of Lynch Syndrome in women with endometrial cancer. Curr. Pharm. Des. 2014, 20, 1655–1663. [Google Scholar] [CrossRef]
- Goverde, A.; Spaander, M.C.; van Doorn, H.C.; Dubbink, H.J.; van den Ouweland, A.M.; Tops, C.M.; Kooi, S.G.; de Waard, J.; Hoedemaeker, R.F.; Bruno, M.J.; et al. Cost-effectiveness of routine screening for Lynch syndrome in endometrial cancer patients up to 70years of age. Gynecol. Oncol. 2016, 143, 453–459. [Google Scholar] [CrossRef]
- Bruegl, A.S.; Kernberg, A.; Broaddus, R.R. Importance of PCR-based Tumor Testing in the Evaluation of Lynch Syndrome-associated Endometrial Cancer. Adv. Anat. Pathol. 2017, 24, 372–378. [Google Scholar] [CrossRef]
- Zeimet, A.G.; Mori, H.; Petru, E.; Polterauer, S.; Reinthaller, A.; Schauer, C.; Scholl-Firon, T.; Singer, C.; Wimmer, K.; Zschocke, J.; et al. AGO Austria recommendation on screening and diagnosis of Lynch syndrome (LS). Arch. Gynecol. Obstet. 2017, 296, 123–127. [Google Scholar] [CrossRef] [PubMed]
- Parc, Y.R.; Halling, K.C.; Burgart, L.J.; McDonnell, S.K.; Schaid, D.J.; Thibodeau, S.N.; Halling, A.C. Microsatellite instability and hMLH1/hMSH2 expression in young endometrial carcinoma patients: Associations with family history and histopathology. Int. J. Cancer 2000, 86, 60–66. [Google Scholar] [CrossRef]
- Ju, W.; Park, H.M.; Lee, S.N.; Sung, S.H.; Kim, S.C. Loss o.of hMLH1 expression is associated with less aggressive clinicopathological features in sporadic endometrioid endometrial adenocarcinoma. J. Obstet. Gynaecol. Res. 2006, 32, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.D.; Choi, J.; Kim, J.H.; Lee, J.S.; Lee, J.H.; Choi, C.; Choi, H.S.; Lee, M.C.; Park, C.S.; Juhng, S.W.; et al. Microsatellite instability at a tetranucleotide repeat in type I endometrial carcinoma. J. Exp. Clin. Cancer Res. 2008, 27, 88. [Google Scholar] [CrossRef][Green Version]
- Catasus, L.; D’Angelo, E.; Pons, C.; Espinosa, I.; Prat, J. Expression profiling of 22 genes involved in the PI3K-AKT pathway identifies two subgroups of high-grade endometrial carcinomas with different molecular alterations. Mod. Pathol. 2010, 23, 694–702. [Google Scholar] [CrossRef]
- An, H.J.; Kim, K.I.; Kim, J.Y.; Shim, J.Y.; Kang, H.; Kim, T.H.; Kim, J.K.; Jeong, J.K.; Lee, S.Y.; Kim, S.J. Microsatellite instability in endometrioid type endometrial adenocarcinoma is associated with poor prognostic indicators. Am. J. Surg Pathol. 2007, 31, 846–853. [Google Scholar] [CrossRef]
- Kolin, D.L.; Quick, C.M.; Dong, F.; Fletcher, C.D.M.; Stewart, C.J.R.; Soma, A.; Hornick, J.L.; Nucci, M.R.; Howitt, B.E. SMARCA4-deficient Uterine Sarcoma and Undifferentiated Endometrial Carcinoma Are Distinct Clinicopathologic Entities. Am. J. Surg. Pathol. 2020, 44, 263–270. [Google Scholar] [CrossRef]
- Schröer, A.; Köster, F.; Fischer, D.; Dubitscher, R.M.; Woll-Hermann, A.; Diedrich, K.; Friedrich, M.; Salehin, D. Immunohistochemistry of DNA mismatch repair enzyme MSH2 is not correlated with prognostic data from endometrial carcinomas. Anticancer Res. 2009, 29, 4833–4837. [Google Scholar]
- Salvesen, H.B.; MacDonald, N.; Ryan, A.; Jacobs, I.J.; Lynch, E.D.; Akslen, L.A.; Das, S. PTEN methylation is associated with advanced stage and microsatellite instability in endometrial carcinoma. Int. J. Cancer 2001, 91, 22–26. [Google Scholar] [CrossRef]
- Jones, N.L.; Xiu, J.; Rocconi, R.P.; Herzog, T.J.; Winer, I.S. Immune checkpoint expression, microsatellite instability, and mutational burden: Identifying immune biomarker phenotypes in uterine cancer. Gynecol. Oncol. 2020, 156, 393–399. [Google Scholar] [CrossRef]
- Colle, R.; Cohen, R.; Cochereau, D.; Duval, A.; Lascols, O.; Lopez-Trabada, D.; Afchain, P.; Trouilloud, I.; Parc, Y.; Lefevre, J.H.; et al. Immunotherapy and patients treated for cancer with microsatellite instability. Bull. Cancer 2017, 104, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Leach, F.S.; Polyak, K.; Burrell, M.; Johnson, K.A.; Hill, D.; Dunlop, M.G.; Wyllie, A.H.; Peltomaki, P.; de la Chapelle, A.; Hamilton, S.R.; et al. Expression of the human mismatch repair gene hMSH2 in normal and neoplastic tissues. Cancer Res. 1996, 56, 235–240. [Google Scholar]
- Fishel, R.; Lescoe, M.K.; Rao, M.R.; Copeland, N.G.; Jenkins, N.A.; Garber, J.; Kane, M.; Kolodner, R. The human mutator gene homolog MSH2 and its association with hereditary nonpolyposis colon cancer. Cell 1993, 75, 1027–1038. [Google Scholar] [CrossRef]
- Bronner, C.E.; Baker, S.M.; Morrison, P.T.; Warren, G.; Smith, L.G.; Lescoe, M.K.; Kane, M.; Earabino, C.; Lipford, J.; Lindblom, A.; et al. Mutation in the DNA mismatch repair gene homologue hMLH 1 is associated with hereditary non-polyposis colon cancer. Nature 1994, 368, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Nicolaides, N.C.; Papadopoulos, N.; Liu, B.; Weit, Y.-F.; Carter, K.C.; Ruben, S.M.; Rosen, C.A.; Haseltine, W.A.; Fleischmann, R.D.; Fraser, C.M.; et al. Mutations of two P/WS homologues in hereditary nonpolyposis colon cancer. Nature 1994, 371, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Devlin, L.A.; Graham, C.A.; Price, J.H.; Morrison, P.J. Germline MSH6 mutations are more prevalent in endometrial cancer patient cohorts than hereditary non polyposis colorectal cancer cohorts. Ulster Med. J. 2008, 77, 25–30. [Google Scholar]
- Kawaguchi, M.; Banno, K.; Yanokura, M.; Kobayashi, Y.; Kishimi, A.; Ogawa, S.; Kisu, I.; Nomura, H.; Hirasawa, A.; Susumu, N.; et al. Analysis of candidate target genes for mononucleotide repeat mutation in microsatellite instability-high (MSI-H) endometrial cancer. Int. J. Oncol. 2009, 35, 977–982. [Google Scholar] [CrossRef]
- Lemetre, C.; Vieites, B.; Ng, C.K.Y.; Piscuoglio, S.; Schultheis, A.M.; Marchiò, C.; Murali, R.; Lopez-García, M.A.; Palacios, J.C.; Jungbluth, A.A.; et al. RNASeq analysis reveals biological processes governing the clinical behaviour of endometrioid and serous endometrial cancers. Eur. J. Cancer 2016, 64, 149–158. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, D.K.; Alvarez, R.D.; Bakkum-Gamez, J.N.; Barroilhet, L.; Behbakht, K.; Berchuck, A.; Berek, J.S.; Chen, L.-M.; Cristea, M.; DeRosa, M.; et al. NCCN Guidelines Insights: Ovarian Cancer, Version 1.2019. J. Natl. Compr. Canc. Netw. 2019, 17, 896–909. [Google Scholar] [CrossRef]
- Manchanda, R.; Menon, U.; Michaelson-Cohen, R.; Beller, U.; Jacobs, I. Hereditary non-polyposis colorectal cancer or Lynch syndrome: The gynaecological perspective. Curr. Opin. Obstet. Gynecol. 2009, 21, 31–38. [Google Scholar] [CrossRef]
- Senter, L.; Clendenning, M.; Sotamaa, K.; Hampel, H.; Green, J.; Potter, J.D.; Lindblom, A.; Lagerstedt, K.; Thibodeau, S.N.; Lindor, N.M.; et al. The clinical phenotype of Lynch syndrome due to germ-line PMS2 mutations. Gastroenterology 2008, 135, 419–428. [Google Scholar] [CrossRef] [PubMed]
- Snowsill, T.M.; Ryan, N.A.J.; Crosbie, E.J.; Frayling, I.M.; Evans, D.G.; Hyde, C.J. Cost-effectiveness analysis of reflex testing for Lynch syndrome in women with endometrial cancer in the UK setting. PLoS ONE 2019, 14, e0221419. [Google Scholar] [CrossRef] [PubMed]
- Gilson, P.; Levy, J.; Rouyer, M.; Demange, J.; Husson, M.; Bonnet, C.; Salleron, J.; Leroux, A.; Merlin, J.-L.; Harlé, A. Evaluation of 3 molecular-based assays for microsatellite instability detection in formalin-fixed tissues of patients with endometrial and colorectal cancers. Sci. Rep. 2020, 10, 16386. [Google Scholar] [CrossRef]
- Libera, L.; Craparotta, I.; Sahnane, N.; Chiaravalli, A.M.; Mannarino, L.; Cerutti, R.; Riva, C.; Marchini, S.; Furlan, D. Targeted gene sequencing of Lynch syndrome-related and sporadic endometrial carcinomas. Hum. Pathol. 2018, 81, 235–244. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef]
- Motzer, R.J.; Tannir, N.M.; McDermott, D.F.; Arén Frontera, O.; Melichar, B.; Choueiri, T.K.; Plimack, E.R.; Barthélémy, P.; Porta, C.; George, S.; et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2018, 378, 1277–1290. [Google Scholar] [CrossRef]
- Di Tucci, C.; Capone, C.; Galati, G.; Iacobelli, V.; Schiavi, M.C.; Di Donato, V.; Muzii, L.; Panici, P.B. Immunotherapy in endometrial cancer: New scenarios on the horizon. J. Gynecol. Oncol. 2019, 30, e46. [Google Scholar] [CrossRef]
- Nishio, H.; Iwata, T.; Aoki, D. Current status of cancer immunotherapy for gynecologic malignancies. Jpn. J. Clin. Oncol. 2021, 51, 167–172. [Google Scholar] [CrossRef]
- Taylor, M.H.; Lee, C.-H.; Makker, V.; Rasco, D.; Dutcus, C.E.; Wu, J.; Stepan, D.E.; Shumaker, R.C.; Motzer, R.J. Phase IB/II Trial of Lenvatinib Plus Pembrolizumab in Patients With Advanced R.Renal Cell Carcinoma, Endometrial Cancer, and Other Selected Advanced Solid Tumors. J. Clin. Oncol. 2020, 38, 1154–1163. [Google Scholar] [CrossRef]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H.; et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: Prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 2020, 21, 1353–1365. [Google Scholar] [CrossRef]
- Jumaah, A.S.; Al-Haddad, H.S.; Salem, M.M.; McAllister, K.A.; Yasseen, A.A. Mismatch repair deficiency and clinicopathological characteristics in endometrial carcinoma: A systematic review and meta-analysis. J. Pathol. Transl. Med. 2021, 55, 202–211. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Type of Tissue | Germinal Mutation Included | MMRd (n) | MMRd (%) | MLH1 (%) | MSH2 (%) | MSH6 (%) | PMS2 (%) | MLH1 Promoter Methylation (%) | |
|---|---|---|---|---|---|---|---|---|---|---|
| Simpkins 1999 [19] | FPPE + frozen tissue | 0 | 53 | 100 | 14.3 | 86 | - | - | 77 | |
| Peiro 2001 [20] | FFPE | 0 | 12 | 13.5 | 12.4 | 1.1 | - | - | - | |
| Maruyama 2001 [21] | FFPE | 1 | 31 | 37 | 12 | 19 | - | - | - | |
| Berends 2001 [22] | FFPE | 1 | 13 | 27 | 61.5 | 30.7 | - | - | - | |
| Chiaravalli 2001 [23] | FFPE | 1 | 13 | 39.4 | - | - | - | - | - | |
| Hardisson 2003 [24] | FFPE | 0 | 23 | 29.5 | 73.9 | 21.7 | - | - | - | |
| Sutter 2004 [25] | Frozen tissue | 1 | 13 | 39.4 | 20 | 76.9 | - | - | - | |
| Irving 2005 [26] | FFPE | 0 | 6 | 50 | 83.3 | 16.7 | - | - | 83 | |
| Alvarez 2012 [27] | FFPE + frozen Tissue | 0 | 4 | 16 | 75 | 25 | - | - | - | |
| Plotkin 2020 [28] | FFPE | 0 | 11 | 22 | - | - | 0 | 100 | - | |
| Reference | Type of Tissue | Germinal Mutation Included | MMRd (n) | MMRd (%) | MLH1 (%) | MSH2 (%) | MSH6 (%) | PMS2 (%) | MLH1 Promoter Methylation |
|---|---|---|---|---|---|---|---|---|---|
| Planck 2002 [29] | FFPE | 1 | 21 | - | 9.5 | 47.6 | 57.1 | - | - |
| Orbo 2003 [30] | FFPE | 0 | 18 | - | 55.5 | 22.2 | 33.3 | - | - |
| Lipton 2004 [31] | Healthy tissue | 1 | 67 | 27 | 44.8 | 43.3 | 1.5 | - | - |
| Macdonald 2004 [32] | FFPE + frozen | 0 | 164 | 51.9 | 14 | 19 | 17 | - | 69 |
| Buttin 2004 [33] | Frozen tissue + healthy tissue | 1 | 94 | 22.8 | - | - | - | - | 70 |
| Soliman 2005 [34] | FPPE | 1 | 12 | 20 | 58.3 | 41.7 | 41.7 | - | - |
| Cederquist 2005 [35] | FFPE | 1 | 6 | 100 | 0 | 0 | 66.7 | - | - |
| Ollikainen 2005 [36] | FFPE + healthy tissue | 1 | 16 | 48.5 | 43.8 | 25 | 31.3 | - | - |
| Taylor 2006 [37] | FPPE | 0 | 6 | 21 | 33.3 | 0 | 0 | - | - |
| Niessen 2006 [38] | Not described | 0 | 36 | 17.1 | 30.6 | 13.9 | 55.6 | - | - |
| Rijcken 2006 [39] | FFPE | 1 | 18 | 100 | 33.3 | 11.1 | 11.1 | - | - |
| Yoon 2008 [40] | FFPE + healthy tissue | 1 | 50 | 44.2 | 46 | 4 | 2 | - | 14 |
| Arabi 2009 [41] | FFPE + healthy tissue | 0 | 25 | 21 | 22.5 | 18 | 43 | - | - |
| Walsh 2010 [42] | FFPE | 1 | 9 | 12.5 | 12 | 2 | 6 | - | - |
| Yasue 2011 [43] | FFPE + frozen tissue | 0 | 8 | 22.9 | 100 | 25 | 45.8 | - | - |
| Huang 2014 [44] | FFPE | 1 | 29 | - | 27.6 | 55.2 | 17.2 | - | - |
| Kobayashi 2015 [45] | FFPE | 0 | 17 | 53.1 | 82.4 | 11.8 | 64.7 | - | - |
| Ren 2020 [46] | FFPE | 1 | 27 | 12.8 | 38.1 | 37 | 51.8 | - | 33.3 |
| Reference | Type of Tissue | Germinal Mutation Included | MMRd (n) | MMRd (%) | MLH1 (%) | MSH2 (%) | MSH6 (%) | PMS2 (%) | MLH1 Promoter Methylation (%) |
|---|---|---|---|---|---|---|---|---|---|
| Westin 2008 [47] | FFPE | 1 | 12 | 34.3 | 25 | 75 | 75 | 25 | 16.7 |
| Matthews 2008 [48] | FFPE + healthy tissue | 1 | 21 | 34.4 | 85.7 | 95.3 | 23.8 | 76.2 | - |
| Garg 2009 [49] | FFPE | 0 | 9 | 20 | 33.3 | 33.3 | 50 | 44.4 | - |
| Garg 2009 [50] | FFPE | 1 | 32 | 45 | 59.4 | 40.6 | 40.6 | 59.4 | - |
| Tafe 2010 [51] | Not described | 1 | 8 | 47 | 87.5 | 0 | 12.5 | 87.5 | - |
| Cossio 2010 [52] | FFPE + healthy tissue | 1 | 7 | 30 | 28.6 | 14.3 | 71.4 | 28.6 | - |
| Resnick 2010 [53] | FFPE | 0 | 155 | 66.5 | - | - | - | - | |
| Shih 2011 [54] | FFPE | 1 | 9 | 16.1 | 44.4 | 55.6 | 55.6 | 44.4 | - |
| Leenen 2012 [55] | FFPE | 1 | 42 | 23.5 | 76.2 | 23.8 | 23.8 | 23.8 | 73.8 |
| Soslow 2012 [56] | FFPE | 0 | 7 | 31.8 | 100 | 0 | 0 | 100 | - |
| Egoavil 2013 [57] | FFPE | 1 | 61 | 33.5 | 72.1 | 8.2 | 21.3 | 13.1 | 55.7 |
| Bosse 2013 [58] | FFPE | 1 | 36 | 24.7 | - | - | - | - | 88.9 |
| Moline 2013 [59] | FFPE | 1 | 59 | 24.1 | 84.7 | 15.3 | 18.6 | 15.3 | 55.9 |
| Peiro 2013 [60] | FFPE | 1 | 63 | 24.4 | 79.4 | 4.8 | 17.6 | 79.4 | - |
| Romero-Perez 2013 [61] | FFPE | 0 | 39 | 32.5 | 48.7 | 23.1 | 30.8 | 69.2 | - |
| Mills 2014 [62] | FFPE | 1 | 137 | 22.6 | 72.3 | 27 | 27 | 72.3 | - |
| Ruiz 2014 [63] | FFPE | 0 | 64 | 30.2 | 54.7 | 6.3 | 54.7 | 56.3 | - |
| Thoury 2014 [64] | FFPE + healthy tissue | 0 | 17 | 24.6 | 65 | 0 | 23 | 59 | - |
| Rabban 2014 [65] | FFPE | 1 | 41 | 15 | 75.6 | 7.7 | 17 | 7.3 | - |
| Long 2014 [66] | Not described | 1 | 41 | 23.7 | 24.4 | 51.2 | 68.3 | 31.7 | - |
| Woo 2014 [67] | FFPE | 0 | 15 | 19.5 | 86.7 | 13.3 | 13.3 | 86.7 | - |
| Hoang 2014 [68] | FFPE | 0 | 6 | 9.5 | 50 | 16.7 | 16.7 | 83.3 | - |
| Buchanan 2014 [69] | FFPE | 1 | 170 | 24 | 75 | 13 | 24.7 | 75.3 | - |
| Allo 2014 [70] | FFPE | 0 | 63 | 33 | 73 | 15.9 | 23.8 | 73 | - |
| Goodfellow 2015 [71] | FFPE + Frozen tissue | 1 | 360 | 38.4 | 75.2 | 3.1 | 11.9 | 7.5 | 70.3 |
| Chu 2015 [72] | FFPE + frozen tissue + healthy tissue | 0 | 22 | 32.8 | 27.2 | 22.7 | 72.3 | 27.2 | - |
| Graham 2015 [73] | FFPE + healthy tissue | 1 | - | - | - | - | - | - | - |
| Dudley 2015 [74] | FFPE | 1 | 72 | 33.4 | - | - | - | 20.8 | - |
| Stelloo 2015 [75] | FFPE | 0 | 19 | 16.4 | 63.2 | - | - | - | 47.4 |
| Mao 2015 [76] | Not described | 0 | 19 | 46.3 | 73.7 | 10.5 | 15.8 | 78.9 | - |
| Mc Conechy 2015 [77] | Frozen tissue | 0 | 38 | 24.2 | 50 | 5.3 | 10.5 | 55.3 | - |
| Stewart 2015 [78] | FFPE | 0 | 13 | 59.1 | 76.9 | 15.4 | 30.8 | 84.7 | - |
| Watkins 2016 [79] | FFPE | 1 | 27 | 21.6 | 88.9 | 3.7 | 14.8 | 44.4 | 25.9 |
| Pocrnich 2016 [80] | Not described | 1 | 8 | 44.4 | 75 | 12.5 | 12.5 | 75 | - |
| Lin 2016 [81] | Not described | 1 | 17 | 22.3 | 82.3 | 17.6 | 17.6 | 82.3 | 64.7 |
| Mills 2016 [82] | Not described | 1 | 66 | 31.4 | 65.2 | 18.2 | 31.8 | 71.2 | - |
| Ramalingam 2016 [83] | FFPE | 0 | 18 | 51.4 | 94.4 | 5.6 | 5.6 | 94.4 | - |
| Shikama 2016 [84] | FFPE | 1 | 62 | 28 | 62.9 | 14.5 | 38.7 | 67.7 | - |
| Kato 2016 [85] | FFPE | 1 | 8 | 2.2 | - | - | - | - | - |
| Okoye 2016 [86] | FFPE | 0 | 40 | 9.7 | - | - | - | - | 75 |
| Russo 2017 [87] | FFPE + healthy tissue | 0 | 3 | 50 | 66.7 | 33.3 | 33.3 | 66.7 | - |
| Bregar 2017 [88] | FFPE | 0 | 13 | 18.5 | - | 0 | 0 | - | - |
| Pelletier 2017 [89] | Not described | 0 | 34 | 26.8 | 67.6 | 8.8 | 14.7 | 85.3 | - |
| Stelloo 2017 [90] | FFPE | 0 | 169 | 24.3 | 85.2 | 5.9 | 13.6 | 89.9 | - |
| Dillon 2017 [91] | FFPE | 1 | 60 | 26 | 85 | 3.3 | 3.3 | 85 | 81.2 |
| Tangjitgamol 2017 [92] | FFPE | 0 | 212 | 55.1 | 60.4 | 29.7 | 70.3 | 62.3 | - |
| Zakhour 2017 [93] | FFPE | 1 | 6 | 7.1 | 33.3 | 50 | 66.7 | 33.3 | - |
| Najdawi 2017 [94] | FFPE | 1 | 36 | 29 | 86.7 | 13.9 | 26.7 | 93.3 | - |
| Sloan 2017 [95] | FFPE | 1 | 38 | 56.7 | - | - | - | - | 15.8 |
| Watkins 2017 [96] | FFPE | 1 | 48 | 19.8 | 81.3 | 8.3 | 14.6 | 85.4 | - |
| Chen 2017 [97] | FFPE | 0 | 30 | 10.3 | - | - | - | - | - |
| Kobel 2017 [98] | FFPE | 0 | 6 | 37.5 | 50 | 33.3 | 50 | 33.3 | - |
| Pina 2018 [99] | Not described | 1 | 242 | 27.1 | 78.9 | 21.1 | 21.1 | 78.9 | 69 |
| Adar 2018 [100] | Not described | 1 | 107 | 22.1 | 80.3 | 19.6 | 19.6 | 15.4 | 70 |
| Chapel 2018 [101] | FFPE | 1 | 30 | 30.3 | 86.7 | 10 | 10 | 90 | - |
| Bosse 2018 [102] | Not described | 0 | 136 | 36.2 | - | - | - | - | - |
| Saita 2018 [103] | Not described | 1 | 13 | - | 46.2 | 23.1 | 30.8 | - | - |
| Espinosa 2018 [104] | FFPE | 0 | 2 | 50 | 100 | 0 | 0 | 100 | - |
| Li 2018 [105] | FFPE | 0 | 162 | 23.1 | 80.2 | 19.8 | 19.8 | 80.2 | - |
| Doghri 2019 [106] | FFPE | 0 | 10 | 22.2 | 80 | 10 | 10 | 80 | - |
| Hashmi 2019 [107] | FFPE | 1 | 56 | 44.4 | 92.9 | 17.9 | 35.7 | 89.3 | - |
| Saeki 2019 [108] | FFPE + healthy tissue | 0 | 18 | 18.4 | 77.8 | 22.2 | 44.4 | 83.3 | - |
| Zannoni 2019 [109] | FFPE | 0 | 15 | 33.3 | 0 | 46.7 | 73.3 | 26.7 | - |
| Abdufatah 2019 [110] | Not described | 0 | 20 | 40 | 5 | 10 | 80 | 80 | - |
| Chapel 2019 [111] | FFPE | 1 | 17 | 100 | 94.1 | 5.9 | 5.9 | 94.1 | - |
| Kahn 2019 [112] | Not described | 1 | 1672 | 28.3 | 69.3 | - | - | - | 53.9 |
| Ryan 2019 [113] | Not described | 1 | 2563 | 24.5 | 17.5 | 3 | 3 | 2 | 37.6 |
| Wu 2019 [114] | FFPE | 1 | 50 | 100 | 63 | 10 | 24 | 72 | - |
| Saijo 2019 [115] | FFPE | 0 | 6 | 10.5 | - | - | - | - | - |
| Sarode 2019 [116] | FFPE | 1 | 45 | 9.3 | - | - | - | - | 26.7 |
| Sari 2019 [117] | FFPE | 0 | 22 | 30 | 68.2 | 9 | 13.6 | 68.2 | - |
| Lucas 2019 [118] | FFPE | 1 | 63 | - | 54 | 19 | 42.9 | 55.6 | - |
| Baniak 2019 [119] | FFPE | 0 | 0 | - | - | - | - | - | - |
| Backes 2019 [120] | Not described | 0 | 64 | 32.5 | - | - | - | - | - |
| Dong 2019 [121] | FFPE | 0 | 63 | 24 | - | - | - | - | - |
| Gan 2019 [122] | FFPE | 1 | 91 | 27.2 | 87.9 | 12.1 | 12.1 | 87.9 | 69.2 |
| He 2019 [123] | Not described | 1 | 2 | 3.3 | - | ||||
| Ryan 2020 [124] | FFPE + healthy tissue | 1 | 132 | 26 | 75.8 | 9.1 | 18.9 | 75.8 | 62.9 |
| Rosa 2020 [125] | FFPE | 1 | 80 | 33.1 | 51.3 | 12.5 | 22.5 | 43.8 | 48.8 |
| Beinse 2020 [126] | FFPE | 0 | 35 | 29.7 | - | - | 17 | 83 | - |
| Timmerman 2020 [127] | Not described | 1 | 33 | 31 | 81.8 | 3 | 15.2 | 6.1 | 79 |
| Missaoui 2020 [128] | FFPE | 1 | 1 | 3.7 | 100 | - | - | 100 | 100 |
| Dasgupta 2020 [129] | Not described | 1 | 4 | - | 100 | - | - | 100 | - |
| Kolehmainen 2020 [130] | FFPE | 0 | 287 | 47.5 | - | - | - | - | - |
| León-Castillo 2020 [131] | FFPE | 0 | 137 | 33.4 | - | - | - | - | - |
| Rekhi 2020 [132] | FFPE | 0 | 50 | - | 66 | 28 | 28 | 66 | - |
| Kim 2020 [133] | FFPE | 0 | 5 | 9.6 | - | - | - | - | - |
| Pasanen 2020 [134] | FFPE + tumor cells | 0 | 191 | 37.3 | - | - | - | - | - |
| Jin 2020 [135] | Not described | 0 | 1 | 5 | - | - | - | - | - |
| Rowe 2020 [136] | FFPE | 1 | 43 | - | - | - | - | - | 46.5 |
| Stinton 2021 [137] | Not described | 1 | - | - | - | - | - | - | - |
| Pecriaux 2021 [138] | FFPE | 1 | 9 | 60 | 100 | 0 | 0 | 88.9 | - |
| Tjalsma 2021 [139] | Not described | 1 | 41 | 23 | 14 | 9 | 9 | 14 | 14 |
| Joehlin-Price 2021 [140] | FFPE | 1 | 35 | 36.8 | 77.1 | 11.4 | 25.9 | 77.1 | 20 |
| Yamamoto 2021 [141] | FFPE | 1 | 68 | 17.2 | 77.9 | 16.2 | 17.6 | 79.4 | 75 |
| Reference | Technique | MLH1 Promoter Methylation (%) |
|---|---|---|
| Simpkins 1999 [19] | PCR + bisulfite conversion | 14.3 |
| Horowitz 2002 [143] | PCR + bisulfite conversion | - |
| Strazzullo 2003 [144] | PCR | - |
| Buttin 2004 [33] | PCR + bisulfite conversion | 70 |
| Macdonald 2004 [32] | Not described | 69 |
| Soliman 2005 [34] | PCR + bisulfite conversion | - |
| Irving 2005 [26] | PCR | 83.3 |
| Kanaya 2005 [145] | PCR + bisulfite conversion | - |
| Ollikainen 2005 [36] | PCR | - |
| Westin 2008 [47] | PCR | 16.7 |
| Nam Yoon 2008 [40] | PCR | 14 |
| Zighelboim 2009 [146] | Pyrosequencing and/or combined bisulfite restriction analysis | |
| Koyamatsu 2010 [147] | Not described | - |
| Walsh 2010 [42] | PCR + bisulfite conversion | - |
| Cossio 2010 [52] | Methylation-specific multiplex ligation-dependent probe amplification | |
| Leenen 2012 [55] | Methylation-specific multiplex ligation-dependent probe amplification | 73.8 |
| Egoavil 2013 [57] | Methylation-specific multiplex ligation-dependent probe amplification | 55.7 |
| Bosse 2013 [58] | PCR + bisulfite conversion | 88.9 |
| Moline 2013 [59] | PCR | 55.9 |
| Batte 2014 [148] | Not described | - |
| Bruegl 2014 [149] | PCR | - |
| Buchanan 2014 [69] | PCR + bisulfite conversion | |
| Goodfellow 2015 [71] | Pyrosequencing and/or combined bisulfite restriction analysis | 70.3 |
| Stelloo 2015 [75] | PCR | 47.4 |
| McConechy 2015 [77] | PCR | - |
| Goverde 2016 [150] | Not described | - |
| Watkins 2016 [79] | PCR | 25.9 |
| Lin 2016 [81] | PCR | 64.7 |
| Mills 2016 [82] | PCR | - |
| Ramalingam 2016 [83] | PCR | - |
| Shikama 2016 [84] | PCR + bisulfite conversion | - |
| Kato 2016 [85] | Methylation-specific multiplex ligation-dependent probe amplification | - |
| Okoye 2016 [86] | PCR + bisulfite conversion | 75 |
| Bruegl 2017 [151] | PCR | - |
| Zeimet 2017 [152] | Not described | - |
| Stelloo 2017 [90] | PCR | - |
| Dillon 2017 [91] | PCR | 81.2 |
| Najdawi 2017 [94] | PCR | - |
| Sloan 2017 [95] | PCR | 15.8 |
| Watkins 2017 [96] | PCR + bisulfite conversion | - |
| Adar 2018 [100] | PCR + bisulfite conversion | 70 |
| Pina 2018 [99] | Not described | 69 |
| Kahn 2019 [112] | Not described | 53.9 |
| Ryan 2019 [113] | Not described | 37.6 |
| Sarode 2019 [116] | Not described | 26.7 |
| Gan 2019 [122] | PCR | 69.2 |
| Ryan 2020 [124] | NGS for germline mutation | 62.9 |
| Rosa 2020 [125] | PCR + bisulfite conversion + NGS for germline mutation | 48.8 |
| Timmerman 2020 [127] | NGS for germline mutation | 79 |
| Missaoui 2020 [128] | PCR + bisulfite conversion | 100 |
| Dasgupta 2020 [129] | Methylation-specific multiplex ligation-dependent probe amplification | - |
| Ren 2020 [46] | PCR + bisulfite conversion | 33.3 |
| Rowe 2020 [136] | PCR | 46.5 |
| Stinton 2021 [137] | Not described | - |
| Tjalsma 2021 [139] | Not described | 14 |
| Joehlin-Price 2021 [140] | Not described | 20 |
| Yamamoto 2021 [141] | PCR | 75 |
| Reference | EC Total (n) | Type of Tissue | MMRd (n) | * RFS or Recurrence MMRd | * RFS or Recurrence MMRp | ** OS or Deaths MMRd | ** OS or DeathsMMRp | Prognosis Conclusion |
|---|---|---|---|---|---|---|---|---|
| Parc 2000 [153] | 62 | Fresh + normal tissue | 21 | - | - | - | - | Not significant |
| Ju 2006 [154] | 50 | FFPE | 12 | - | - | - | - | Not significant |
| Choi 2008 [155] | 39 | FFPE | 8 | - | - | - | - | Not significant |
| Shih 2011 [54] | 56 | FFPE | 9 | 5 year: 71.1%, 95% CI (53.1–89.1%) | 5 year: 97.6%, 95% CI (95.2–100%) | 5 year: 71.1%, 95% CI (53.1–89.1%) | 5 year: 100% | MMRd was associated with worse RFS and OS compared with MMRp |
| Peiro 2013 [20] | 260 | FFPE | 33 | - | - | - | - | Not significant |
| Ruiz 2014 [63] | 212 | FFPE | 64 | - | - | - | - | Not significant |
| Stelloo 2015 [75] | 216 | FFPE | 19 | 5 year: 95% | 5 year: 93% POL-E, 52% no specific molecular profile 42% p53 | - | - | MMRd was associated with a better RFS compared with MMRp |
| Mao 2015 [76] | 41 | Not described | 16 | - | - | - | - | Not significant |
| Tangjitgamol 2017 [92] | 385 | FFPE | 212 | 5 year: 67.0%, 95% CI (49.7–79.5%) advanced stage | 5 year: 40.0%, 95% CI (25.5–54.1%) advanced stage | 5 year: 66.5%, 95% CI (49.2–79.1) advanced stage | 5 year: 45.5%, 95% CI (30.2–59.5) advanced stage | MMRd was associated with better RFS and OS in advanced stage compared with MMRp in advanced stage |
| Pina 2018 [99] | 892 | Not described | 242 | Recurrence: 10% | Recurrence: 42% | Deaths: 13.1% | Deaths: 36.1% | MMRd was associated with better RFS and OS compared with MMRp |
| Bosse 2018 [102] | 381 | Not described | 136 | HR = 0.61, 95% CI (0.37–1.00) compared with no specific molecular profile | HR = 0.23, 95% CI (0.07–0.77) POLE compared with no specific molecular profile | HR = 0.84, 95% CI (0.57–1.25) compared with no specific molecular profile | HR = 0.56, 95% CI (0.27–1.15) POLE compared with no specific molecular profile | MMRd was associated with better RFS and OS compared with MMRp |
| Backes 2019 [120] | 197 | Not described | 64 | 5 year: 66%, 95% CI (45–79%) | 5 year: 89%, 95% CI (76–94%) | 5 year: 74% | 5 year: 86% | MMRd was associated with worse RFS and OS compared with MMRp |
| Beinse 2020 [126] | 159 | FFPE | 35 | - | - | - | - | Intermediate |
| Kolin 2020 [158] | 96 | FFPE | 34 | 36 months | 9 months | - | - | MMRd was associated with better RFS compared with MMRp |
| León-Castillo 2020 [131] | 423 | FFPE | 137 | 5 year: 71.7% | 5 year: 98% POL-E, 48% p53 | 5 year: 81.3% | 5 year: 98% POLE, 53% p53 | Intermediate |
| Kim 2020 [133] | 52 | FFPE | 5 | - | - | - | - | Not significant |
| Joehlin-Price 2021 [140] | 95 | FFPE | 35 | - | - | - | - | Not significant |
| Yamamoto 2021 [141] | 395 | FFPE | 68 | - | - | - | - | Not significant |
| Reference | Type of Tissue | MMRd (n) | MMRd (%) | PDL-1 |
|---|---|---|---|---|
| Jones 2020 [161] | Not described | 203 | 33 | PDL-1 was more frequent in MMRd tumors |
| Bregar 2017 [88] | FFPE | 13 | 33 | PDL-1 was present in 62% of MMRd tumors and high-grade tumors vs. 46% in MMRp tumors |
| Sloan 2017 [95] | FFPE | 38 | 56.7 | 100% MMRd tumors demonstrated PDL-1 expression in peritumoral immune compartment |
| Rowe 2020 [136] | FFPE | 43 | 69.4 | 60.4% MMRd tumors showed positive tumoral PDL-1 vs. 5.3% MMRp |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Favier, A.; Varinot, J.; Uzan, C.; Duval, A.; Brocheriou, I.; Canlorbe, G. The Role of Immunohistochemistry Markers in Endometrial Cancer with Mismatch Repair Deficiency: A Systematic Review. Cancers 2022, 14, 3783. https://doi.org/10.3390/cancers14153783
Favier A, Varinot J, Uzan C, Duval A, Brocheriou I, Canlorbe G. The Role of Immunohistochemistry Markers in Endometrial Cancer with Mismatch Repair Deficiency: A Systematic Review. Cancers. 2022; 14(15):3783. https://doi.org/10.3390/cancers14153783
Chicago/Turabian StyleFavier, Amelia, Justine Varinot, Catherine Uzan, Alex Duval, Isabelle Brocheriou, and Geoffroy Canlorbe. 2022. "The Role of Immunohistochemistry Markers in Endometrial Cancer with Mismatch Repair Deficiency: A Systematic Review" Cancers 14, no. 15: 3783. https://doi.org/10.3390/cancers14153783
APA StyleFavier, A., Varinot, J., Uzan, C., Duval, A., Brocheriou, I., & Canlorbe, G. (2022). The Role of Immunohistochemistry Markers in Endometrial Cancer with Mismatch Repair Deficiency: A Systematic Review. Cancers, 14(15), 3783. https://doi.org/10.3390/cancers14153783