
Prognostic Gene Expression-Based Signature in Clear-Cell Renal Cell Carcinoma

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
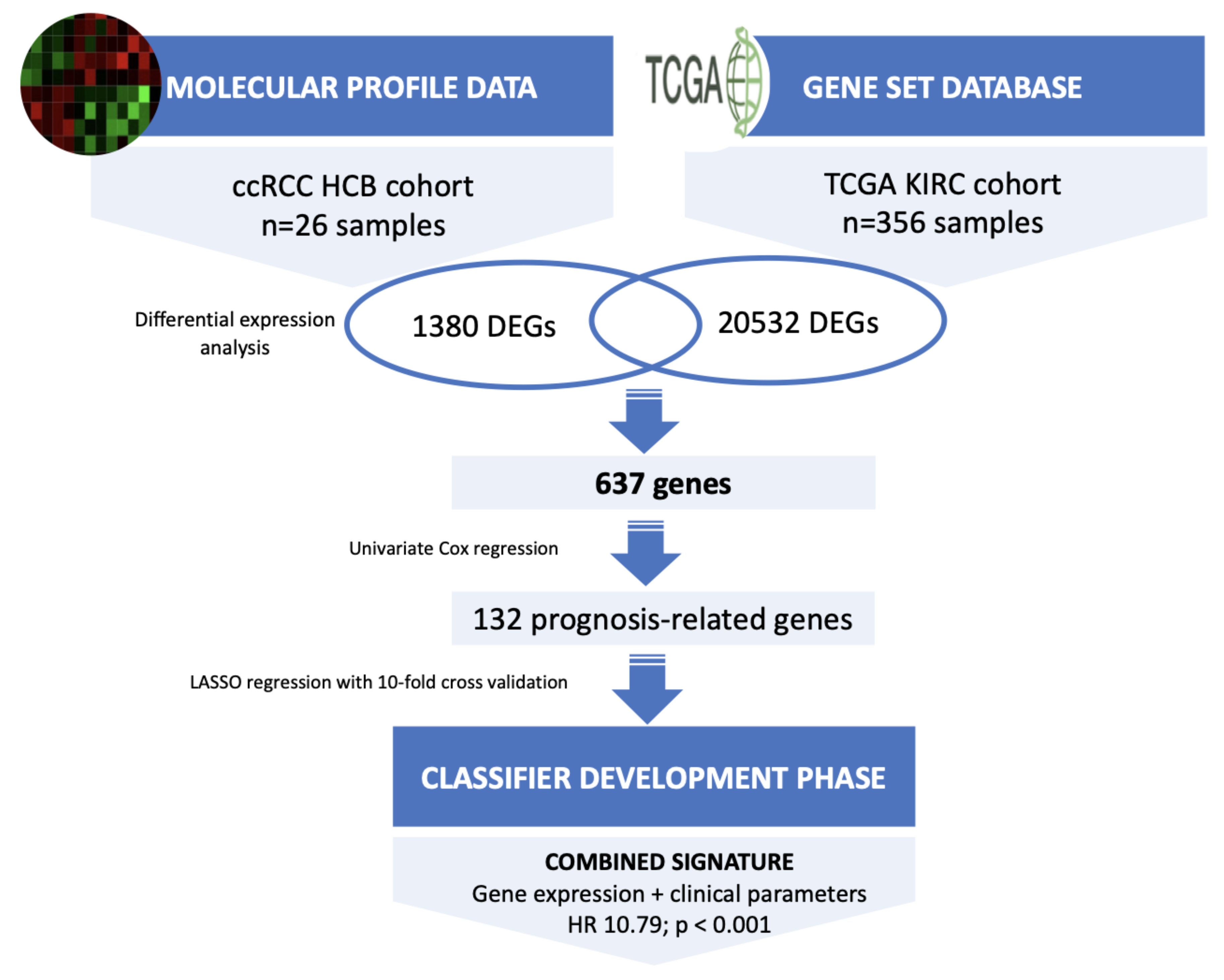
2.1. Patients, Datasets Sources and Study Design
2.2. Tissue Specimens and RNA Isolation
2.3. Molecular Profiling by RNA Sequencing
2.4. Selection and Verification of Prognosis-Related Genes
2.5. Development of a Gene Expression-Based Signature
2.6. Pathway Enrichment Analysis
3. Results
3.1. Clinical Features of the Cohort
3.2. Molecular Profiling of ccRCC Samples
3.3. Identification of Prognosis-Related Genes in an External Data Set
3.4. Development of a Prognostic Signature
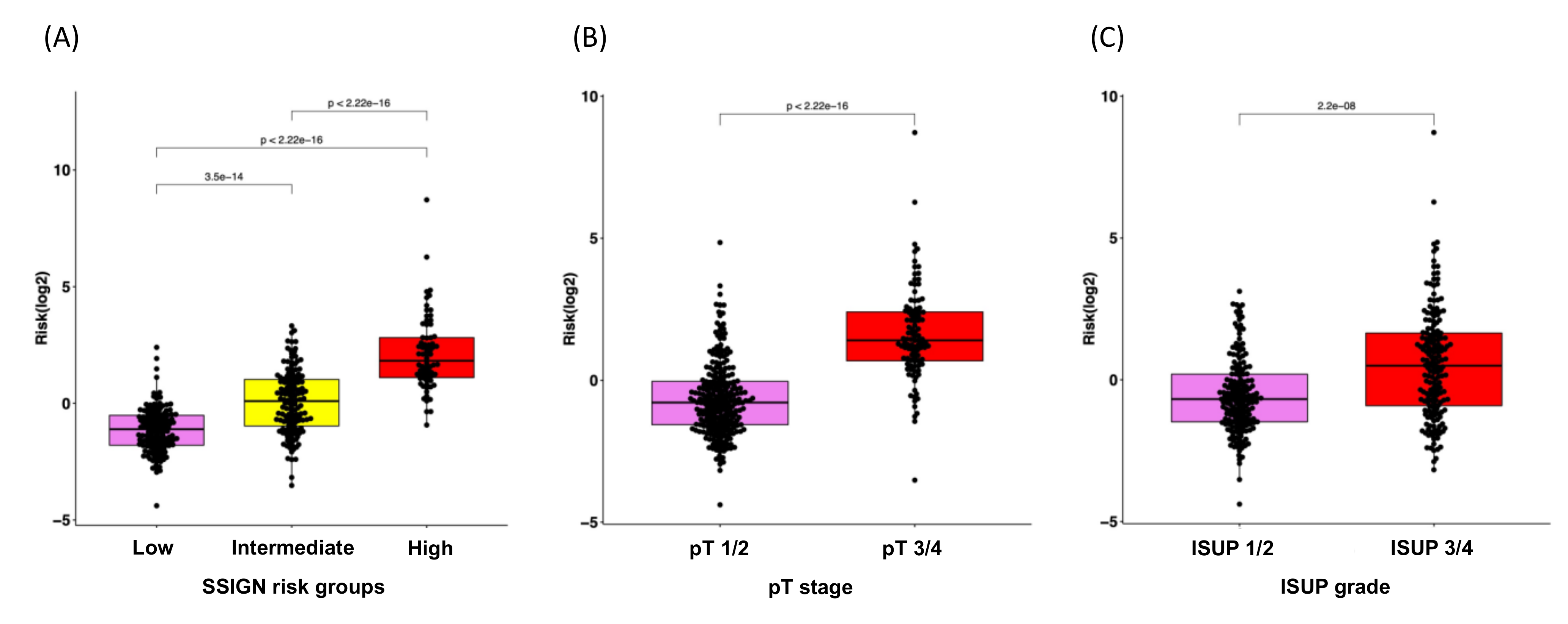
3.5. Correlation Analysis of the RS with Clinical Characteristics for Disease Progression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ljungberg, B.; Albiges, L.; Bensalah, K.; Bex, A.; Giles, R.H.; Hora, M.; Kuczyk, M.A.; Lam, T.; Marconi, L.; Canfield, S.; et al. EAU Guidelines. Edn. presented at the EAU Annual Congress Amsterdam 2020. Eur. Urol. 2020, 67, 913–924. [Google Scholar] [CrossRef] [PubMed]
- Klatte, T.; Rossi, S.H.; Stewart, G.D. Prognostic factors and prognostic models for renal cell carcinoma: A literature review. World J. Urol. 2018, 36, 1943–1952. [Google Scholar] [CrossRef] [PubMed]
- Padala, S.A.; Barsouk, A.; Thandra, K.C.; Saginala, K.; Mohammed, A.; Vakiti, A.; Rawla, P.; Barsouk, A. Epidemiology of Renal Cell Carcinoma. World J. Oncol. 2020, 11, 79. [Google Scholar] [CrossRef]
- Motzer, R.J.; Haas, N.B.; Donskov, F.; Gross-Goupil, M.; Varlamov, S.; Kopyltsov, E.; Lee, J.L.; Melichar, B.; Rini, B.I.; Choueiri, T.K.; et al. Randomized phase III trial of adjuvant pazopanib versus placebo after nephrectomy in patients with localized or locally advanced renal cell carcinoma. J. Clin. Oncol. 2017, 35, 3916–3923. [Google Scholar] [CrossRef]
- Haas, N.B.; Manola, J.; Uzzo, R.G.; Flaherty, K.T.; Wood, C.G.; Kane, C.; Jewett, M.; Dutcher, J.P.; Atkins, M.B.; Pins, M.; et al. Adjuvant sunitinib or sorafenib for high-risk, non-metastatic renal-cell carcinoma (ECOG-ACRIN E2805): A double-blind, placebo-controlled, randomised, phase 3 trial. Lancet 2016, 387, 2008–2016. [Google Scholar] [CrossRef] [Green Version]
- Zhao, H.; Cao, Y.; Wang, Y.; Zhang, L.; Chen, C.; Wang, Y.; Lu, X.; Liu, S.; Yan, F. Dynamic prognostic model for kidney renal clear cell carcinoma (KIRC) patients by combining clinical and genetic information. Sci. Rep. 2018, 8, 17613. [Google Scholar] [CrossRef]
- Rini, B.; Goddard, A.; Knezevic, D.; Maddala, T.; Zhou, M.; Aydin, H.; Campbell, S.; Elson, P.; Koscielny, S.; Lopatin, M.; et al. A 16-gene assay to predict recurrence after surgery in localised renal cell carcinoma: Development and validation studies. Lancet Oncol. 2015, 16, 676–685. [Google Scholar] [CrossRef]
- Brooks, S.A.; Brannon, A.R.; Parker, J.S.; Fisher, J.C.; Sen, O.; Kattan, M.W.; Hakimi, A.A.; Hsieh, J.J.; Choueiri, T.K.; Tamboli, P.; et al. ClearCode34: A prognostic risk predictor for localized clear cell renal cell carcinoma. Eur. Urol. 2014, 66, 77–84. [Google Scholar] [CrossRef] [Green Version]
- Xing, Q.; Zeng, T.; Liu, S.; Cheng, H.; Ma, L.; Wang, Y. A novel 10 glycolysis-related genes signature could predict overall survival for clear cell renal cell carcinoma. BMC Cancer 2021, 21, 381. [Google Scholar] [CrossRef]
- FireBrowse. Available online: http://firebrowse.org/ (accessed on 8 October 2021).
- Liu, J.; Lichtenberg, T.; Hoadley, K.A.; Poisson, L.M.; Lazar, A.J.; Cherniack, A.D.; Kovatich, A.J.; Benz, C.C.; Levine, D.A.; Lee, A.V.; et al. An Integrated TCGA Pan-Cancer Clinical Data Resource to Drive High-Quality Survival Outcome Analytics. Cell 2018, 173, 400–416.e11. [Google Scholar] [CrossRef] [Green Version]
- Babraham Bioinformatics—Trim Galore! Available online: https://www.bioinformatics.babraham.ac.uk/projects/trim_galore/ (accessed on 15 May 2019).
- Dobin, A.; Davis, C.A.; Schlesinger, F.; Drenkow, J.; Zaleski, C.; Jha, S.; Batut, P.; Chaisson, M.; Gingeras, T.R. STAR: Ultrafast universal RNA-seq aligner. Bioinformatics 2013, 29, 15–21. [Google Scholar] [CrossRef]
- Ritchie, M.E.; Phipson, B.; Wu, D.; Hu, Y.; Law, C.W.; Shi, W.; Smyth, G.K. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015, 43, e47. [Google Scholar] [CrossRef]
- Kanehisa, M.; Goto, S. KEGG: Kyoto Encyclopedia of Genes and Genomes. Nucleic Acids Res. 2000, 28, 27–30. [Google Scholar] [CrossRef]
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A Software Environment for Integrated Models of Biomolecular Interaction Networks. Genome Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef]
- Merico, D.; Isserlin, R.; Stueker, O.; Emili, A.; Bader, G.D. Enrichment map: A network-based method for gene-set enrichment visualization and interpretation. PLoS ONE 2010, 5, e13984. [Google Scholar] [CrossRef]
- Reimand, J.; Isserlin, R.; Voisin, V.; Kucera, M.; Tannus-Lopes, C.; Rostamianfar, A.; Wadi, L.; Meyer, M.; Wong, J.; Xu, C.; et al. Pathway enrichment analysis and visualization of omics data using g:Profiler, GSEA, Cytoscape and EnrichmentMap. Nat. Protoc. 2019, 14, 482–517. [Google Scholar] [CrossRef]
- Kucera, M.; Isserlin, R.; Arkhangorodsky, A.; Bader, G.D. AutoAnnotate: A Cytoscape app for summarizing networks with semantic annotations. F1000Research 2016, 5, 1717. [Google Scholar] [CrossRef]
- Boulesteix, A.L.; De Bin, R.; Jiang, X.; Fuchs, M. IPF-LASSO: Integrative L1-Penalized Regression with Penalty Factors for Prediction Based on Multi-Omics Data. Comput. Math. Methods Med. 2017, 2017, 7691937. [Google Scholar] [CrossRef] [Green Version]
- Frank, I.; Blute, M.L.; Cheville, J.C.; Lohse, C.M.; Weaver, A.L.; Zincke, H. An outcome prediction model for patients with clear cell renal cell carcinoma treated with radical nephrectomy based on tumor stage, size, grade and necrosis: The SSIGN score. J. Urol. 2002, 168, 2395–2400. [Google Scholar] [CrossRef]
- Choueiri, T.K.; Tomczak, P.; Park, S.H.; Venugopal, B.; Ferguson, T.; Chang, Y.-H.; Hajek, J.; Symeonides, S.N.; Lee, J.L.; Sarwar, N.; et al. Adjuvant Pembrolizumab after Nephrectomy in Renal-Cell Carcinoma. N. Engl. J. Med. 2021, 385, 683–694. [Google Scholar] [CrossRef]
- Ravaud, A.; Motzer, R.J.; Pandha, H.S.; George, D.J.; Pantuck, A.J.; Patel, A.; Chang, Y.-H.; Escudier, B.; Donskov, F.; Magheli, A.; et al. Adjuvant Sunitinib in High-Risk Renal-Cell Carcinoma after Nephrectomy. N. Engl. J. Med. 2016, 375, 2246–2254. [Google Scholar] [CrossRef]
- Malone, E.R.; Oliva, M.; Sabatini, P.J.B.; Stockley, T.L.; Siu, L.L. Molecular profiling for precision cancer therapies. Genome Med. 2020, 12, 8. [Google Scholar] [CrossRef] [Green Version]
- Dimitrieva, S.; Schlapbach, R.; Rehrauer, H. Prognostic value of cross-omics screening for kidney clear cell renal cancer survival. Biol. Direct 2016, 11, 68. [Google Scholar] [CrossRef] [Green Version]
- Li, P.; Conley, A.; Zhang, H.; Kim, H.L. Whole-Transcriptome profiling of formalin-fixed, paraffin-embedded renal cell carcinoma by RNA-seq. BMC Genomics 2014, 15, 1087. [Google Scholar] [CrossRef] [Green Version]
- Goeman, J.J. L1 Penalized Estimation in the Cox Proportional Hazards Model. Biometrical J. 2010, 52, 70–84. [Google Scholar] [CrossRef]
- Dai, J.; Lu, Y.; Wang, J.; Yang, L.; Han, Y.; Wang, Y.; Yan, D.; Ruan, Q.; Wang, S. A four-gene signature predicts survival in clear-cell renal-cell carcinoma. Oncotarget 2016, 7, 82712–82726. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.; Luo, Y.; Wang, G.; Qian, K.; Qian, G.; Wu, C.L.; Dan, H.C.; Wang, X.; Xiao, Y. Prognostic value of a gene signature in clear cell renal cell carcinoma. J. Cell. Physiol. 2019, 234, 10324–10335. [Google Scholar] [CrossRef]
- Li, F.; Hu, W.; Zhang, W.; Li, G.; Guo, Y. A 17-Gene Signature Predicted Prognosis in Renal Cell Carcinoma. Dis. Markers 2020, 2020, 8352809. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Lin, E.; Zhuang, H.; Xie, L.; Feng, X.; Liu, J.; Yu, Y. Construction of a novel gene-based model for prognosis prediction of clear cell renal cell carcinoma. Cancer Cell Int. 2020, 20, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Uhlen, M.; Zhang, C.; Lee, S.; Sjöstedt, E.; Fagerberg, L.; Bidkhori, G.; Benfeitas, R.; Arif, M.; Liu, Z.; Edfors, F.; et al. A pathology atlas of the human cancer transcriptome. Science 2017, 357, eaan2507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, M.; Wang, H.; Chen, H.; Han, Y. SMARCD3 is a potential prognostic marker and therapeutic target in CAFs. Aging 2020, 12, 20835–20861. [Google Scholar] [CrossRef] [PubMed]
- Wei, R.; Liu, H.; Li, C.; Guan, X.; Zhao, Z.; Ma, C.; Wang, X.; Jiang, Z. Computational identification of 29 colon and rectal cancer-associated signatures and their applications in constructing cancer classification and prognostic models. Front. Genet. 2020, 11, 740. [Google Scholar] [CrossRef]
- Zuo, Y.; Xu, X.; Chen, M.; Qi, L. The oncogenic role of the cerebral endothelial cell adhesion molecule (CERCAM) in bladder cancer cells in vitro and in vivo. Cancer Med. 2021, 10, 4437–4450. [Google Scholar] [CrossRef]
- Roldán, F.L.; Lozano, J.J.; Ingelmo-Torres, M.; Carrasco, R.; Díaz, E.; Ramirez-Backhaus, M.; Rubio, J.; Reig, O.; Alcaraz, A.; Mengual, L.; et al. Clinicopathological and Molecular Prognostic Classifier for Intermediate/High-Risk Clear Cell Renal Cell Carcinoma. Cancers 2021, 13, 6338. [Google Scholar] [CrossRef]
- Lundin, L.; Larsson, H.; Kreuger, J.; Kanda, S.; Lindahl, U.; Salmivirta, M.; Claesson-Welsh, L. Selectively desulfated heparin inhibits fibroblast growth factor-induced mitogenicity and angiogenesis. J. Biol. Chem. 2000, 275, 24653–24660. [Google Scholar] [CrossRef] [Green Version]
- Chen, E.; Stringer, S.E.; Rusch, M.A.; Selleck, S.B.; Ekker, S.C. A unique role for 6-O sulfation modification in zebrafish vascular development. Dev. Biol. 2005, 284, 364–376. [Google Scholar] [CrossRef]
- Hellerbrand, C.; Amann, T.; Schlegel, J.; Wild, P.; Bataille, F.; Spruss, T.; Hartmann, A.; Bosserhoff, A.K. The novel gene MIA2 acts as a tumour suppressor in hepatocellular carcinoma. Gut 2008, 57, 243–251. [Google Scholar] [CrossRef] [Green Version]
- Sasahira, T.; Kirita, T.; Nishiguchi, Y.; Kurihara, M.; Nakashima, C.; Bosserhoff, A.K.; Kuniyasu, H. A comprehensive expression analysis of the MIA gene family in malignancies: MIA gene family members are novel, useful markers of esophageal, lung, and cervical squamous cell carcinoma. Oncotarget 2016, 7, 31137–31152. [Google Scholar] [CrossRef] [Green Version]
- Expression of MIA2 in cancer—Summary—The Human Protein Atlas. Available online: https://www.proteinatlas.org/ENSG00000150527-MIA2/pathology (accessed on 12 May 2022).
- Ma, Q.; Wu, K.; Li, H.; Li, H.; Zhu, Y.; Hu, G.; Hu, L.; Kong, X. ONECUT2 overexpression promotes RAS-driven lung adenocarcinoma progression. Sci. Rep. 2019, 9, 20021. [Google Scholar] [CrossRef]
- Wu, Y.; Jiang, G.; Zhang, N.; Liu, S.; Lin, X.; Perschon, C.; Zheng, S.L.; Ding, Q.; Wang, X.; Na, R.; et al. HOXA9, PCDH17, POU4F2, and ONECUT2 as a Urinary Biomarker Combination for the Detection of Bladder Cancer in Chinese Patients with Hematuria. Eur. Urol. Focus 2020, 6, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.; Wu, B.; Yu, Y.; Zhu, W.; Zhang, S.; Zhang, Y.; Guo, J.; Deng, N. Blockade of ONECUT2 expression in ovarian cancer inhibited tumor cell proliferation, migration, invasion and angiogenesis. Cancer Sci. 2018, 109, 2221. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Ci, X.; Ahmed, M.; Hua, J.T.; Soares, F.; Lin, D.; Puca, L.; Vosoughi, A.; Xue, H.; Li, E.; et al. ONECUT2 is a driver of neuroendocrine prostate cancer. Nat. Commun. 2019, 10, 278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, L.; Hu, F.; Shen, S.; Xiao, H.; Li, G.; Wang, M.S.; Mei, J. Knockdown of SOX12 expression inhibits the proliferation and metastasis of lung cancer cells. Am. J. Transl. Res. 2017, 9, 4003. [Google Scholar]
- Gu, W.; Wang, B.; Wan, F.; Wu, J.; Lu, X.; Wang, H.; Zhu, Y.; Zhang, H.; Shi, G.; Dai, B.; et al. SOX2 and SOX12 are predictive of prognosis in patients with clear cell renal cell carcinoma. Oncol. Lett. 2018, 15, 4564–4570. [Google Scholar] [CrossRef]
- Huang, W.; Chen, Z.; Shang, X.; Tian, D.; Wang, D.; Wu, K.; Fan, D.; Xia, L. Sox12, a direct target of FoxQ1, promotes hepatocellular carcinoma metastasis through up-regulating Twist1 and FGFBP1. Hepatology 2015, 61, 1920–1933. [Google Scholar] [CrossRef]
- Gao, Y.; Li, L.; Hou, L.; Niu, B.; Ru, X.; Zhang, D. SOX12 promotes the growth of multiple myeloma cells by enhancing Wnt/β-catenin signaling. Exp. Cell Res. 2020, 388, 111814. [Google Scholar] [CrossRef]
- Ghatalia, P.; Gordetsky, J.; Kuo, F.; Dulaimi, E.; Cai, K.Q.; Devarajan, K.; Bae, S.; Naik, G.; Chan, T.A.; Uzzo, R.; et al. Prognostic impact of immune gene expression signature and tumor infiltrating immune cells in localized clear cell renal cell carcinoma. J. Immunother. Cancer 2019, 7, 139. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| KERRYPNX | Discovery Phase Hospital Clinic Barcelona (n = 26) | Validation Phase TCGA Cohort (n = 356) |
|---|---|---|
| Gender | ||
| Male | 18 (69.2) | 231 (64.9) |
| Female | 8 (30.8) | 125 (35.1) |
| Age at diagnosis (year) | 59 (34–81) | 60 (29–90) |
| Pathological tumor size (cm) | 5.5 (1.9–17.5) | 5.1 (1.0–25) |
| ISUP | ||
| ISUP 1 | 3 (11.5) | 4 (1.1) |
| ISUP 2 | 12 (46.2) | 173 (48.6) |
| ISUP 3 | 6 (23.1) | 145 (40.7) |
| ISUP 4 | 5 (19.2) | 34 (9.6) |
| Tumor stage | ||
| pT1 | 15 (57.7) | 211 (59.3) |
| pT2 | 5 (19.2) | 41 (11.5) |
| pT3 | 5 (19.2) | 102 (28.7) |
| pT4 | 1 (3.8) | 2 (0.6) |
| N stage | ||
| N0/x | 24 (92.3) | 346 (97.2) |
| N1 | 2 (7.7) | 10 (2.8) |
| Necrosis | 10 (38.5) | 144 (40.4) |
| SSIGN score * | ||
| Low risk | 12 (46.2) | 143 (40.2) |
| Intermediate risk | 8 (30.7) | 141 (39.6) |
| High risk | 6 (23.1) | 72 (20.2) |
| Progression-Free Survival | Cancer-Specific Survival | |||||
|---|---|---|---|---|---|---|
| p | 95% CI | HR | p | 95% CI | HR | |
| CERCAM | <0.001 | 1.387–3.807 | 2.298 | <0.001 | 1.036–1.075 | 1.055 |
| HS6ST2 | <0.001 | 1.164–3.106 | 1.902 | 0.034 | 1.043–2.866 | 1.729 |
| MIA2 | <0.001 | 0.222–0.632 | 0.375 | <0.001 | 0.825–0.935 | 0.878 |
| ONECUT2 | 0.015 | 1.111–2.952 | 1.811 | <0.001 | 2.443–5.942 | 3.810 |
| SOX12 | 0.001 | 1.354–3.748 | 2.252 | <0.001 | 1.177–1.488 | 1.323 |
| TMEM132A | <0.001 | 1.526–4.288 | 2.558 | <0.001 | 1.070–1.156 | 1.112 |
| pT Stage | <0.001 | 1.775–3.024 | 2.317 | <0.001 | 2.547–9.940 | 5.032 |
| Tumor size | <0.001 | 1.154–1.273 | 1.212 | <0.001 | 1.125–1.271 | 1.195 |
| ISUP | <0.001 | 1.568–3.158 | 2.225 | 0.001 | 1.628–7.845 | 3.574 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roldán, F.L.; Izquierdo, L.; Ingelmo-Torres, M.; Lozano, J.J.; Carrasco, R.; Cuñado, A.; Reig, O.; Mengual, L.; Alcaraz, A. Prognostic Gene Expression-Based Signature in Clear-Cell Renal Cell Carcinoma. Cancers 2022, 14, 3754. https://doi.org/10.3390/cancers14153754
Roldán FL, Izquierdo L, Ingelmo-Torres M, Lozano JJ, Carrasco R, Cuñado A, Reig O, Mengual L, Alcaraz A. Prognostic Gene Expression-Based Signature in Clear-Cell Renal Cell Carcinoma. Cancers. 2022; 14(15):3754. https://doi.org/10.3390/cancers14153754
Chicago/Turabian StyleRoldán, Fiorella L., Laura Izquierdo, Mercedes Ingelmo-Torres, Juan José Lozano, Raquel Carrasco, Alexandra Cuñado, Oscar Reig, Lourdes Mengual, and Antonio Alcaraz. 2022. "Prognostic Gene Expression-Based Signature in Clear-Cell Renal Cell Carcinoma" Cancers 14, no. 15: 3754. https://doi.org/10.3390/cancers14153754
APA StyleRoldán, F. L., Izquierdo, L., Ingelmo-Torres, M., Lozano, J. J., Carrasco, R., Cuñado, A., Reig, O., Mengual, L., & Alcaraz, A. (2022). Prognostic Gene Expression-Based Signature in Clear-Cell Renal Cell Carcinoma. Cancers, 14(15), 3754. https://doi.org/10.3390/cancers14153754