
Management and Outcomes in Anal Canal Adenocarcinomas—A Systematic Review



Abstract
:Simple Summary
Abstract
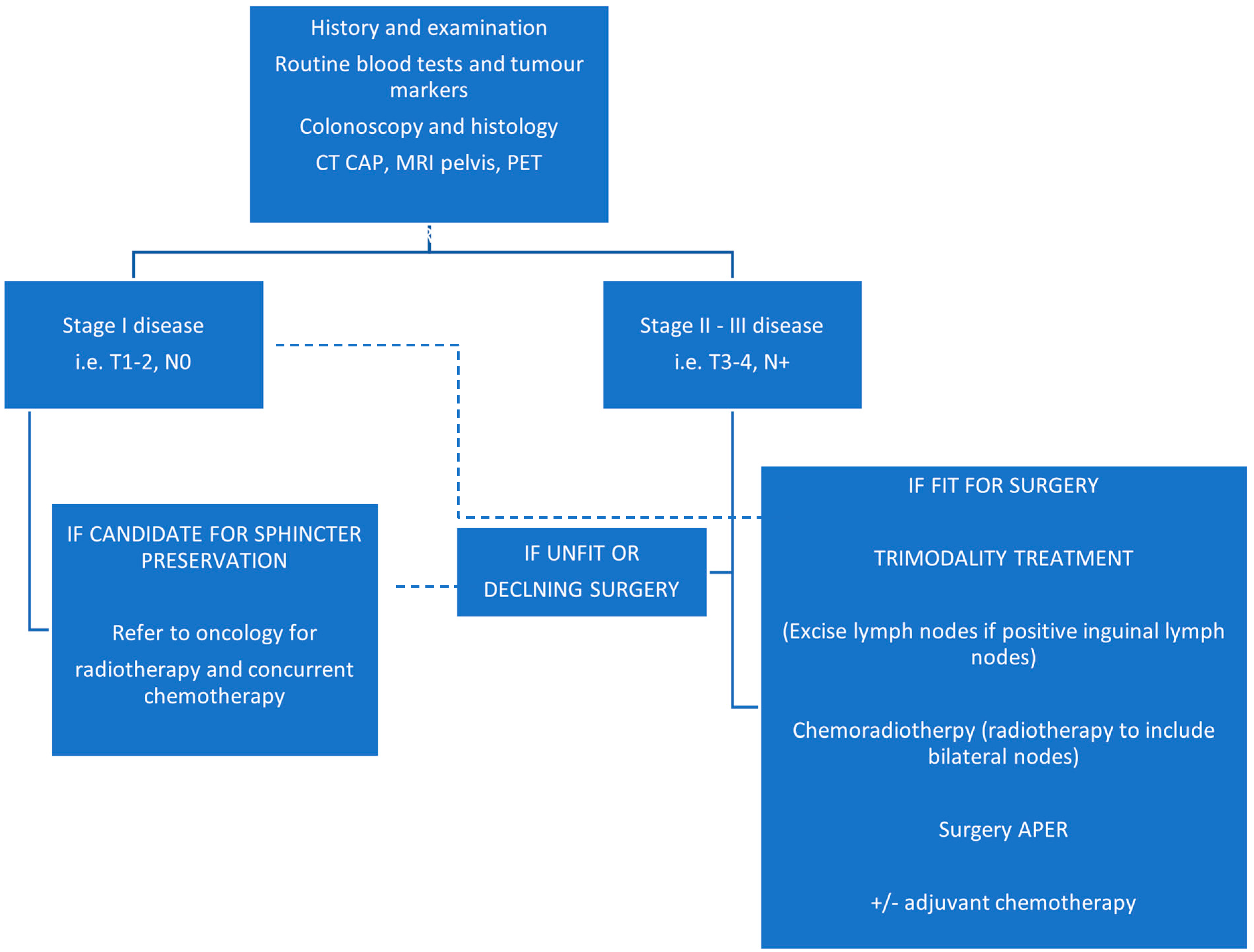
1. Introduction
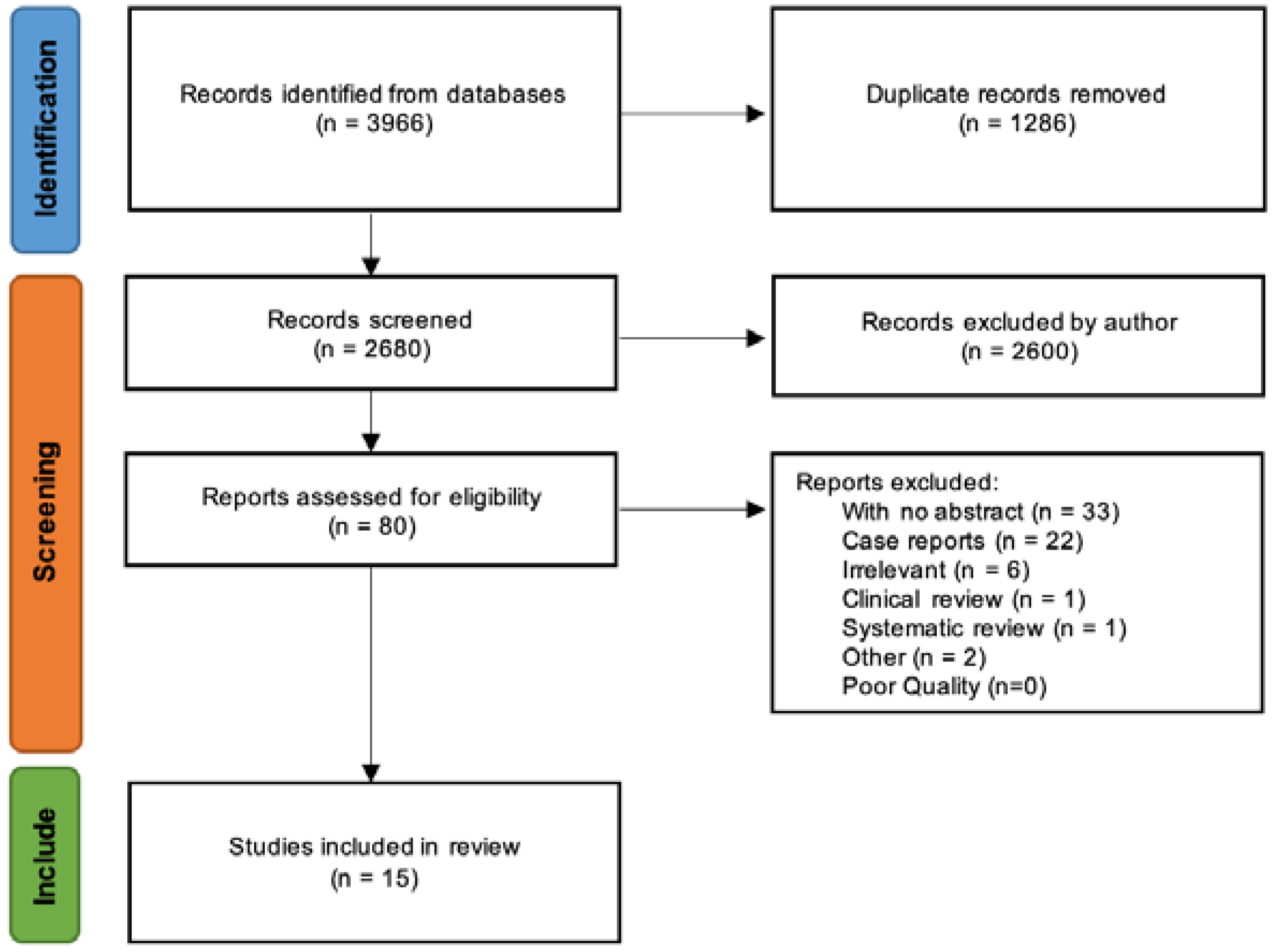
2. Materials and Methods
2.1. Eligibility Criteria, Sources and Search Strategy
2.2. Selection and Data Collection Process
3. Results
3.1. Surgery Only (S)
3.2. Surgery and Postoperative CRT (S + CRT)
3.3. Primary CRT (CRT)
3.4. Neoadjuvant CRT and Surgery (CRT + S)
3.5. Management of Anal Adenocarcinoma in Crohn’s Disease
4. Discussion
4.1. General Interpretation of Results
4.2. Limitations of Evidence and Review Processes Used
4.3. Implications of Results for Practice, Policy, and Future Research
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- Date range used (5 years, 10 years): 2011 to date
- Limits used (gender, article/study type, etc.): English language
- Search terms and notes (full search strategy for database searches below):
- Search terms used
- adenocarcinoma OR adenocarcinomata OR adenocarcin * OR AC
- anus OR anal OR anal canal OR dentate line OR “dentate line” OR pectinate line OR “pectinate line”
- anal adenocarcinoma OR anal adenocarcinomata
- anal canal adenocarcinoma OR anal canal adenocarcinomata
- anus adenocarcinoma OR anus adenocarcinomata
- (anal ADJ3 adenocarcin*) OR (anus ADJ3 adenocarcin*)
- dentate line adenocarcinoma OR “dentate line adenocarcinoma” OR dentate line adenocarcinomata OR “dentate line adenocarcinomata”
- pectinate line adenocarcinoma OR “pectinate line adenocarcinoma” OR pectinate line adenocarcinomata OR “pectinate line adenocarcinomata”
- (dentate line ADJ3 adenocarcin *) OR (pectinate line ADJ3 adenocarcin *)
- radiotherapy OR radiation therapy OR RT OR RTx OR XRT
- chemotherapy OR chemo OR CTX OR CTx OR anticancer drugs OR anti-cancer drugs OR anti cancer drugs
- chemoradiotherapy OR radiochemotherapy OR chemoradiation OR RCT OR RCTx OR RT-CT
- neoadjuvant therapy
- abdominoperineal resection OR abdominoperineal excision OR Abdomino-Perineal Resection OR Abdomino-Perineal Excision OR AP resection OR AP excision OR APR OR APER OR Abdomino-Perineal Rectum Excision OR Abdominoperineal Rectum Excision
- (“abdominoperineal resection” ADJ3 rectum) OR (“abdominoperineal excision” ADJ3 rectum)
- MEDLINE
- ○
- Case Reports
- ○
- Classical Article
- ○
- Clinical Study
- ○
- Clinical Trial (phase i to iv)
- ○
- Comparative Study
- ○
- Controlled Clinical Trial
- ○
- Corrected And Republished Article
- ○
- Evaluation Studies
- ○
- Introductory Journal Article
- ○
- Journal Article
- ○
- Meta-analysis
- ○
- Multicenter Study
- ○
- Observational Study
- ○
- Pragmatic Clinical Trial
- ○
- Randomised Control Trial
- ○
- Review
- ○
- Technical Report
- ○
- Twin Study
- ○
- Validation Studies
- EMBASE
- ○
- Article
- ○
- Journal
- ○
- Letter
- ○
- Report
- ○
- Review
- EMCARE
- ○
- Article
- ○
- Letter
- ○
- Reports
- ○
- Review
- CINAHL
- ○
- Case Study
- ○
- Clinical Trial
- ○
- Corrected Article
- ○
- Journal Article
- ○
- Letter
- ○
- Meta Analysis
- ○
- Meta Synthesis
- ○
- Randomised Control Trial
- ○
- Research
- ○
- Review
- ○
- Systematic Review
Appendix B

{kind=link}
{kind=link}
| From Anwar 2013 | Main Conclusions | |
|---|---|---|
| 1 | Jensen et al. [31] | AA is associated with poor survival |
| 2 | Abel et al. [32] | APR for local control needed in most patients |
| 3 | Basik et al. (1995) [33] | Improved survival through early diagnosis and radical surgery |
| 4 | Joon et al. (1999) [24] | CRT preferred for early cancers and APR reserved for salvage surgery |
| 5 | Wolff and Peiffert [34] | Gold standard for treatment should stay as APR |
| 6 | Belkacémi et al. (2003) [26] | Recommend CRT for early cancers and APR for salvage surgery |
| 7 | Longo et al. [35] | APR followed by CRT is optimal treatment |
| 8 | Anthony et al. [36] | Combination of neoadjuvant CRT and APR is optimal treatment |
| 9 | Klas et al. [37] | Tumours larger than 5 cm should be managed with surgery and CRT, smaller with S alone. |
| 10 | Beal et al. (2003) [30] | APR and CRT combination is a reasonable approach to treatment |
| 11 | Papagikos et al. (2003) [29] | Neoadjuvant CRT and APR combination, +/− adjuvant CT is the optimal treatment regimen |
| 12 | Li et al. [38] | APR and postoperative CRT is suggested |
| 13 | Chang et al. (2009) [25] | APR with neoadjuvant CRT is the most sensible management |
| 14 | Devon et al. [39] | Recommend multimodality therapy |
| 15 | Iesalnieks et al. [27] | For patients with CD and chronic perianal fistulae, cancer surveillance is essential |
| 16 | Wong et al. [40] | Recommend S alone, with postoperative CRT for certain patients |
References
- Types of Anal Cancer. Available online: https://www.cancerresearchuk.org/about-cancer/anal-cancer/stages-types/types (accessed on 17 December 2021).
- Annal Cancer Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/anal-cancer (accessed on 17 December 2021).
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Freedman-Cass, D.A. Anal Carcinoma, Version 2.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2018, 16, 852–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anwar, S.; Welbourn, H.; Hill, J.; Sebag-Montefiore, D. Adenocarcinoma of the anal canal—A systematic review. Colorectal. Dis. 2013, 15, 1481–1488. [Google Scholar] [CrossRef]
- PRISMA Flow Diagram. Available online: http://prisma-statement.org/prismastatement/flowdiagram.aspx (accessed on 30 April 2022).
- Lukovic, J.; Kim, J.J.; Krzyzanowska, M.; Chadi, S.A.; Taniguchi, C.M.; Hosni, A. Anal Adenocarcinoma: A Rare Malignancy in Need of Multidisciplinary Management. JCO Oncol. Pract. 2020, 16, 635–640. [Google Scholar] [CrossRef]
- Ogawa, H.; Haneda, S.; Shibata, C.; Miura, K.; Nagao, M.; Ohnuma, S.; Unno, M. Adenocarcinoma associated with perianal fistulas in Crohn’s disease. Anticancer Res. 2013, 33, 685–689. [Google Scholar]
- Peiffert, D.; Tournier-Rangeard, L.; Gérard, J.P.; Lemanski, C.; François, E.; Giovannini, M.; Ducreux, M. Induction chemotherapy and dose intensification of the radiation boost in locally advanced anal canal carcinoma: Final analysis of the randomized UNICANCER ACCORD 03 trial. J. Clin. Oncol. 2012, 30, 1941–1948. [Google Scholar] [CrossRef] [PubMed]
- Bertelson, N.; Blumetti, J.; Cintron, J.; Harrison, J.; Chaudhry, V.; Abcarian, H. Anal Adenocarcinoma: Outcomes in an Uncommon Malignancy. Am. Surg. 2015, 81, 1114–1117. [Google Scholar] [CrossRef] [PubMed]
- Franklin, R.A.; Giri, S.; Valasareddy, P.; Lands, L.T.; Martin, M.G. Comparative Survival of Patients With Anal Adenocarcinoma, Squamous Cell Carcinoma of the Anus, and Rectal Adenocarcinoma. Clin. Colorectal. Cancer 2016, 15, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Su, Z.; Guo, Z.W.; Mao, Y.P.; Tang, J.; Lan, X.W.; Xie, F.Y.; Li, Q. Anal adenocarcinoma requires prophylactic inguinal nodal treatment: Results from a single Chinese institution. J. Cancer 2017, 8, 1097–1102. [Google Scholar] [CrossRef] [PubMed]
- McKenna, N.P.; Bergquist, J.R.; Habermann, E.B.; Chua, H.K.; Kelley, S.R.; Mathis, K.L. Surgery and chemotherapy are associated with improved overall survival in anal adenocarcinoma: Results of a national cohort study. Int. J. Colorectal. Dis. 2019, 34, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Leong, F.Q.H.; Chan, D.K.H.; Tan, K.K. Anal Adenocarcinoma Can Masquerade as Chronic Anal Fistula in Asians. Ann. Coloproctol. 2019, 35, 47–49. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Fu, J.; Chen, X.; Cai, C.; Ruan, H.; Du, J. What factors are associated with the poor prognosis of anal adenocarcinoma compared with low-lying rectal adenocarcinoma based on a population analysis: A propensity score matching study. PLoS ONE 2019, 14, e0219937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, G.D.; Haque, W.; Butler, E.B.; Teh, B.S. Survival Outcomes and Patterns of Management for Anal Adenocarcinoma. Ann. Surg. Oncol. 2019, 26, 1351–1357. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Shinde, A.; Fakih, M.; Sentovich, S.; Melstrom, K.; Nelson, R.; Amini, A. Impact of Surgical Resection on Survival Outcomes After Chemoradiotherapy in Anal Adenocarcinoma. J. Natl. Compr. Cancer Netw. JNCCN 2019, 17, 1203–1210. [Google Scholar] [CrossRef]
- Malakhov, N.; Kavi, A.M.; Lee, A.; Adedoyin, P.; Sheth, N.; Lederman, A.J.; Schreiber, D. Patterns of Care and Comparison of Outcomes Between Primary Anal Squamous Cell Carcinoma and Anal Adenocarcinoma. Dis. Colon Rectum 2019, 62, 1448–1457. [Google Scholar] [CrossRef]
- Wegner, R.E.; White, R.J.; Hasan, S.; Raj, M.; Monga, D.; Finley, G.; McCormick, J. Anal adenocarcinoma: Treatment outcomes and trends in a rare disease entity. Cancer Med. 2019, 8, 3855–3863. [Google Scholar] [CrossRef]
- Park, H. Survival Outcomes After Initial Treatment for Anal Adenocarcinoma: A Population-Based Cohort Study. Clin. Colorectal. Cancer 2020, 19, e75–e82. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, H.; Haneda, S.; Shibata, C.; Miura, K.; Nagao, M.; Ohnuma, S.; Unno, M. Clinicopathologic Features and Outcome of Adenocarcinoma of the Anal Canal: A Population-Based Study. Int. J. Surg. Oncol. 2020, 2020, 5139236. [Google Scholar]
- Yasuhara, M.; Beppu, N.; Uchino, M.; Ikeuchi, H.; Matsuda, I.; Hirota, S.; Tomita, N. Adverse Oncologic Outcomes of Adenocarcinoma of the Anal Canal in Patients With Crohn’s Disease. Dis. Colon Rectum 2021, 64, 409–419. [Google Scholar] [CrossRef]
- Chatani, P.D.; Dominguez, D.A.; Aversa, J.G.; Davis, J.L.; Hernandez, J.M.; Lai, L.L.; Blakely, A.M. Local excision and chemoradiation for clinical node-negative anal adenocarcinoma. Surg. Oncol. 2021, 37, 101551. [Google Scholar] [CrossRef] [PubMed]
- Plot Digitizer. Available online: https://automeris.io/WebPlotDigitizer/ (accessed on 13 February 2022).
- Joon, D.L.; Chao, M.W.; Ngan, S.Y.; Joon, M.L.; Guiney, M.J. Primary adenocarcinoma of the anus: A retrospective analysis. Int. J. Radiat. Oncol. Biol. Phys. 1999, 45, 1199–1205. [Google Scholar] [CrossRef]
- Chang, G.J.; Gonzalez, R.J.; Skibber, J.M.; Eng, C.; Das, P.; Rodriguez-Bigas, M.A. A twenty-year experience with adenocarcinoma of the anal canal. Dis. Colon Rectum 2009, 52, 1375–1380. [Google Scholar] [CrossRef]
- Belkacémi, Y.; Berger, C.; Poortmans, P.; Piel, G.; Zouhair, A.; Méric, J.-B.; Nguyen, T.-D.; Krengli, M.; Behrensmeier, F.; Allal, A.; et al. Management of primary anal canal adenocarcinoma: A large retrospective study from the Rare Cancer Network. Int. J. Radiat. Oncol. Biol. Phys. 2003, 56, 1274–1283. [Google Scholar] [CrossRef]
- Iesalnieks, I.; Gaertner, W.B.; Glaβ, H.; Strauch, U.; Hipp, M.; Agha, A.; Schlitt, H.J. Fistula-associated anal adenocarcinoma in Crohn’s disease. Inflamm. Bowel Dis. 2010, 16, 1643–1648. [Google Scholar] [CrossRef]
- Kounalakis, N.; Artinyan, A.; Smith, D.; Mojica-Manoso, P.; Paz, B.; Lai, L.L. Abdominal perineal resection improves survival for nonmetastatic adenocarcinoma of the anal canal. Ann. Surg. Oncol. 2009, 16, 1310–1315. [Google Scholar] [CrossRef] [PubMed]
- Papagikos, M.; Crane, C.H.; Skibber, J.; Janjan, N.A.; Feig, B.; Rodriguez-Bigas, M.A.; Hung, A.; Wolff, R.A.; Delclos, W.; Lin, E.; et al. Chemoradiation for adenocarcinoma of the anus. Int. J. Radiat. Oncol. Biol. Phys. 2003, 55, 669–678. [Google Scholar] [CrossRef]
- Beal, K.P.; Wong, D.; Guillem, J.G.; Paty, P.B.; Saltz, L.L.; Wagman, R.; Minsky, B.D. Primary adenocarcinoma of the anus treated with combined modality therapy. Dis. Colon Rectum 2003, 46, 1320–1324. [Google Scholar] [CrossRef] [PubMed]
- Jensen, S.L.; Shokouh-Amiri, M.H.; Hagen, K.; Harling, H.; Nielsen, O.V. Adenocarcinoma of the anal ducts. A series of 21 cases. Dis. Colon. Rectum 1988, 31, 268–272. [Google Scholar] [CrossRef]
- Abel, M.E.; Chiu, Y.S.Y.; Russell, T.R.; Volpe, P.A. Adenocarcinoma of the anal glands: Results of a survey. Dis. Colon. Rectum 1993, 36, 383–387. [Google Scholar] [CrossRef] [PubMed]
- Basik, M.; Rodriguez-Bigas, M.A.; Penetrante, R.; Petrelli, N.J. Prognosis and recurrence patterns of anal adenocarcinoma. Am. J. Surg. 1995, 169, 233–237. [Google Scholar] [CrossRef]
- Wolff, P.; Peiffert, D. In regard to Joon et al. IJROBP 1999;45:1199–1205. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 1517. [Google Scholar] [CrossRef]
- Longo, W.E.; Vernava, A.M.; Wade, T.P.; Coplin, M.A.; Virgo, K.S.; Johnson, F.E. Rare anal canal cancers in the U.S. veteran: Patterns of disease and results of treatment. Am. Surg. 1995, 61, 495–500. [Google Scholar] [PubMed]
- Anthony, T.; Simmang, C.; Lee, E.L.; Turnage, R.H. Perinal mucinous adenocarcinoma. J. Surg. Oncol. 1997, 64, 218–221. [Google Scholar] [CrossRef]
- Klas, J.V.; Rothenberger, D.A.; Wong, W.D.; Madoff, R.D. Malignant tumors of the anal canal: The spectrum of disease, treatment, and outcomes. Cancer 1999, 85, 1686–1693. [Google Scholar] [CrossRef]
- Li, L.R.; Wan, D.S.; Pan, Z.Z.; Pan, Z.Z.; Zhou, Z.W.; Chen, G.; Wu, X.J.; Lu, Z.H.; Ding, P.R. Clinical features and treatment of 49 patients with anal canal adenocarcinoma. Chin. J. Gastrointest. Surg. 2006, 9, 402–404. [Google Scholar]
- Devon, K.M.; Brown, C.J.; Burnstein, M.; McLeod, R.S. Cancer of the anus complicating perianal Crohn’s disease. Dis. Colon. Rectum 2009, 52, 211–216. [Google Scholar] [CrossRef]
- Wong, M.T.C.; Lim, J.F.; Eu, K.W. Anal canal malignancies: A review in an Asian population. Singap. Med. J. 2011, 52, 9–14. [Google Scholar]
| 5-Year Overall Survival by Treatment (%) | ||||||
|---|---|---|---|---|---|---|
| S Only | CRT + S | S + CRT | CRT Only | RT or CT Only | ||
| 1 | Peiffert 2012 [8] | - | - | - | 75.0 (CFS) | - |
| 2 | Bertelson 2015 [9] | - | - | - | - | - |
| 3 | Franklin 2016 [10] | - | - | - | - | - |
| 4 | Su 2017 [11] | - | - | - | - | - |
| 5 | McKenna 2019 [12] | - | - | - | - | - |
| 6 | Leong 2019 [13] | - | - | - | - | - |
| 7 | Wang 2019 [14] | - | - | - | - | - |
| 8 | Lewis 2019 [15] | - | - | - | - | - |
| 9 | Li 2019 [16] | - | 61.1 | - | 39.8 | - |
| 10 | Malakhov 2019 [17] | 57.6 | 64.6 | 51.7 | 39.2 | - |
| 11 | Wegner 2019 [18] | 69.1 | 64.1 | 67.3 | 42.0 | - |
| 12 | Park 2020 [19] | 77.7 (CSS) | 80.3 | 65.8 | 63.9 | 35.7 |
| 13 | Gogna 2020 [20] | - | - | - | - | - |
| 14 | Yasuhara 2021 [21] | - | - | - | - | - |
| 15 | Chatani 2021 [22] | - | - | - | - | - |
| Study | N | N with Fistulas (F) or Crohn’s (CD) | Age (Median) | Intervention (s) | Median Follow-Up (Months) | Recurrence (N) | Median OS (Months) | OS (%) | Quality Scale (NOS) |
|---|---|---|---|---|---|---|---|---|---|
| Peiffert (2012) [8] | 307 | n/a | 58.8 (mean) | CRT/ CRT + ICT | 50 | R = 88/307 LR = 68/88. DM =20/88 | n/a | 75% at 5 years (CRT) 76.5% at 5 years (CRT + ICT) | 8 |
| Bertelson (2015) [9] | 18 | F = 3, CD = 2 | 53 (mean) | S Only (APR)/ S (APR) + CRT/ CRT/ CT Only | 25, 17, 8 | LR = 4, DM = 10 | 24, 17 | n/a | 6 |
| Franklin (2016) [10] | 462 | n/a | 69 | No treatments compared | n/a | n/a | 33 | 30.2% at 5 years | 7 |
| Su (2017) [11] | 126 | n/a | 55.5 | S Only/ S + CRT/ CRT/ Palliative | 30 | LR = 36 DM = 25 | n/a | 43.4% at 5 years | 7 |
| McKenna (2019) [12] | 2117 | n/a | n/a | S/ CT/ RT/ Combinations | n/a | n/a | 65 | n/a | 8 |
| Leong (2019) [13] | 5 | 5 | 64 | CRT + S/ S + CRT/ CRT | n/a | LR = n/a, DM = 3/5 | 10.5 | n/a | 6 |
| Wang (2019) [14] | 136 | n/a | 60 | S (APR) only/ S + RT/ S + CT/ S + CRT | 44 | n/a | n/a | n/a | 8 |
| Lewis (2019) [15] | 1183 | 0 | n/a | CRT/ CRT + S (APR) | 150 | n/a | 72.5 | 55.9% at 5 years | 6 |
| Li (2019) [16] | 1747 | n/a | n/a | CRT Only/ CRT + S(APR) | 41.1 | n/a | n/a | 61.1% at 5 years (CRT + S) 39.8% at 5 years (CRT only) | 8 |
| Malakhov (2019) [17] | 1193 | n/a | 66 | S Only/ CRT + S/ S + CRT/ CRT | 47.6 | n/a | n/a | 48.4% at 5 years | 7 |
| Wegner (2019) [18] | 1729 | n/a | 65 | S Only/ CRT + S/ S + CRT/ CRT | 55 | n/a | 69, 92, 83, 45 | 55% at 5 years | 8 |
| Park (2020) [19] | 393 | n/a | 65 | S Only/ CRT + S/ S + CRT/ CRT/ RT or CT | 29 | n/a | n/a | 72.9% at 3 years (CSS) | 6 |
| Gogna (2020) [20] | 2090 | n/a | 68.12 | CRT/ CRT + S | n/a | n/a | n/a | 39.6% at 5 years | 6 |
| Yasuhara (2021) [21] | 102 | CD = 34 | 56 | S only/ S + CRT | 54.9 | LR = 26, DM = 25 | n/a | 91% at 5 years (CA) 85.7% at 5 years (NCA) | 6 |
| Chatani (2021) [22] | 359 | n/a | 65, 62 | S + CRT/ CRT + S (LE or APR) | n/a | n/a | 85.8, 65.3 | n/a | 6 |
| From This Study | Main Conclusions | |
|---|---|---|
| 1 | Peiffert et al. (2012) [8] | No advantage for induction chemotherapy (ICT) or HD radiation boost use |
| 2 | Bertelson et al. (2015) [9] | For stage II AA patients CRT followed by APR is the treatment choice, with curative resection offering no significant long-term DFS outcomes |
| 3 | Franklin et al. (2016) [10] | Consider more aggressive therapy since AA has worse prognosis than SCCA and RA |
| 4 | Su et al. (2017) [11] | Prophylactic inguinal nodal treatment necessary for AA patients, even if negative ILNs |
| 5 | McKenna et al. (2019) [12] | Increased mortality associated with non-surgical management thus AA patients need MDT evaluation and surgery referral |
| 6 | Leong et al. (2019) [13] | Treatment of choice is multimodal with neoadjuvant CRT followed by APR (CRT + S) |
| 7 | Wang et al. (2019) [14] | AA has worse prognosis than RA and T staging criteria for anal carcinoma may not be valid for AA |
| 8 | Lewis et al. (2019) [15] | Trimodality therapy offers better survival outcomes than CRT alone, specifically CRT followed by APR within 6 months |
| 9 | Li et al. (2019) [16] | CRT followed by surgery (CRT + S) associated with significant OS benefit |
| 10 | Malakhov et al. (2019) [17] | AA tends to be treated like rectal cancer using neoadjuvant CRT and a more aggressive approach necessary with surgery, particularly APR, being important |
| 11 | Wegner et al. (2019) [18] | Improved OS by incorporating surgery in AA management compared to CRT alone |
| 12 | Park (2020) [19] | CRT given preoperatively with surgical resection might maximise OS outcomes |
| 13 | Gogna et al. (2020) [20] | Survival outcomes significantly improved with surgery |
| 14 | Yasuhara et al. (2021) [21] | Outcomes Crohn’s disease-associated patients with larger sized AA tumours are significantly poorer. Improved outcomes of CRT + S compared to S only. |
| 15 | Chatani et al. (2021) [22] | No overall survival difference between local excision or APR in combination with CRT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Taliadoros, V.; Rafique, H.; Rasheed, S.; Tekkis, P.; Kontovounisios, C. Management and Outcomes in Anal Canal Adenocarcinomas—A Systematic Review. Cancers 2022, 14, 3738. https://doi.org/10.3390/cancers14153738
Taliadoros V, Rafique H, Rasheed S, Tekkis P, Kontovounisios C. Management and Outcomes in Anal Canal Adenocarcinomas—A Systematic Review. Cancers. 2022; 14(15):3738. https://doi.org/10.3390/cancers14153738
Chicago/Turabian StyleTaliadoros, Vasilis, Henna Rafique, Shahnawaz Rasheed, Paris Tekkis, and Christos Kontovounisios. 2022. "Management and Outcomes in Anal Canal Adenocarcinomas—A Systematic Review" Cancers 14, no. 15: 3738. https://doi.org/10.3390/cancers14153738
APA StyleTaliadoros, V., Rafique, H., Rasheed, S., Tekkis, P., & Kontovounisios, C. (2022). Management and Outcomes in Anal Canal Adenocarcinomas—A Systematic Review. Cancers, 14(15), 3738. https://doi.org/10.3390/cancers14153738