
Occupational Factors and Socioeconomic Differences in Breast Cancer Risk and Stage at Diagnosis in Swiss Working Women

 , ,
, ,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Follow-Up
2.2. Outcome Definition
2.3. Independent Variables Considered
2.4. Potential Confounders
2.5. Statistical Analyses
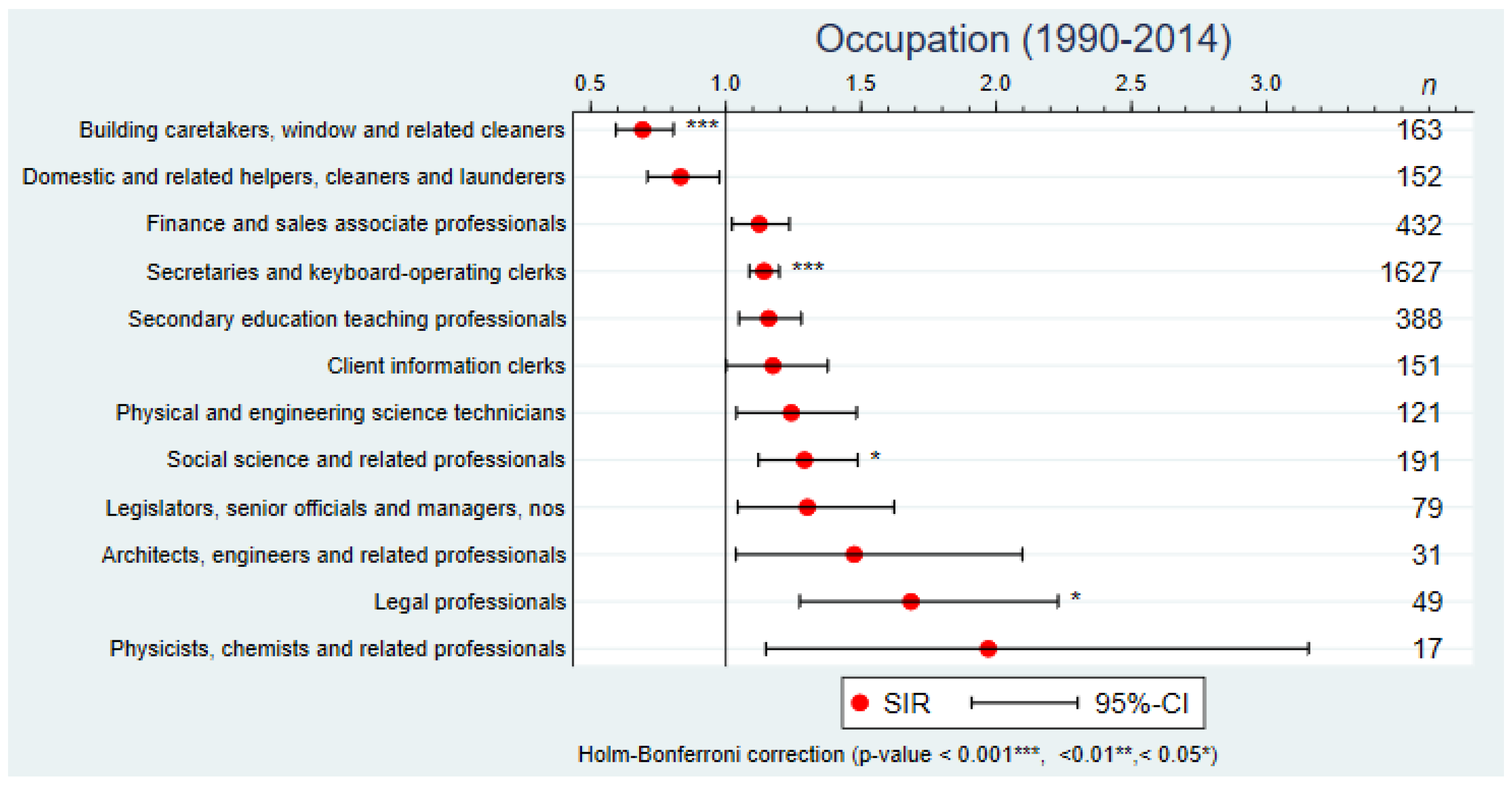
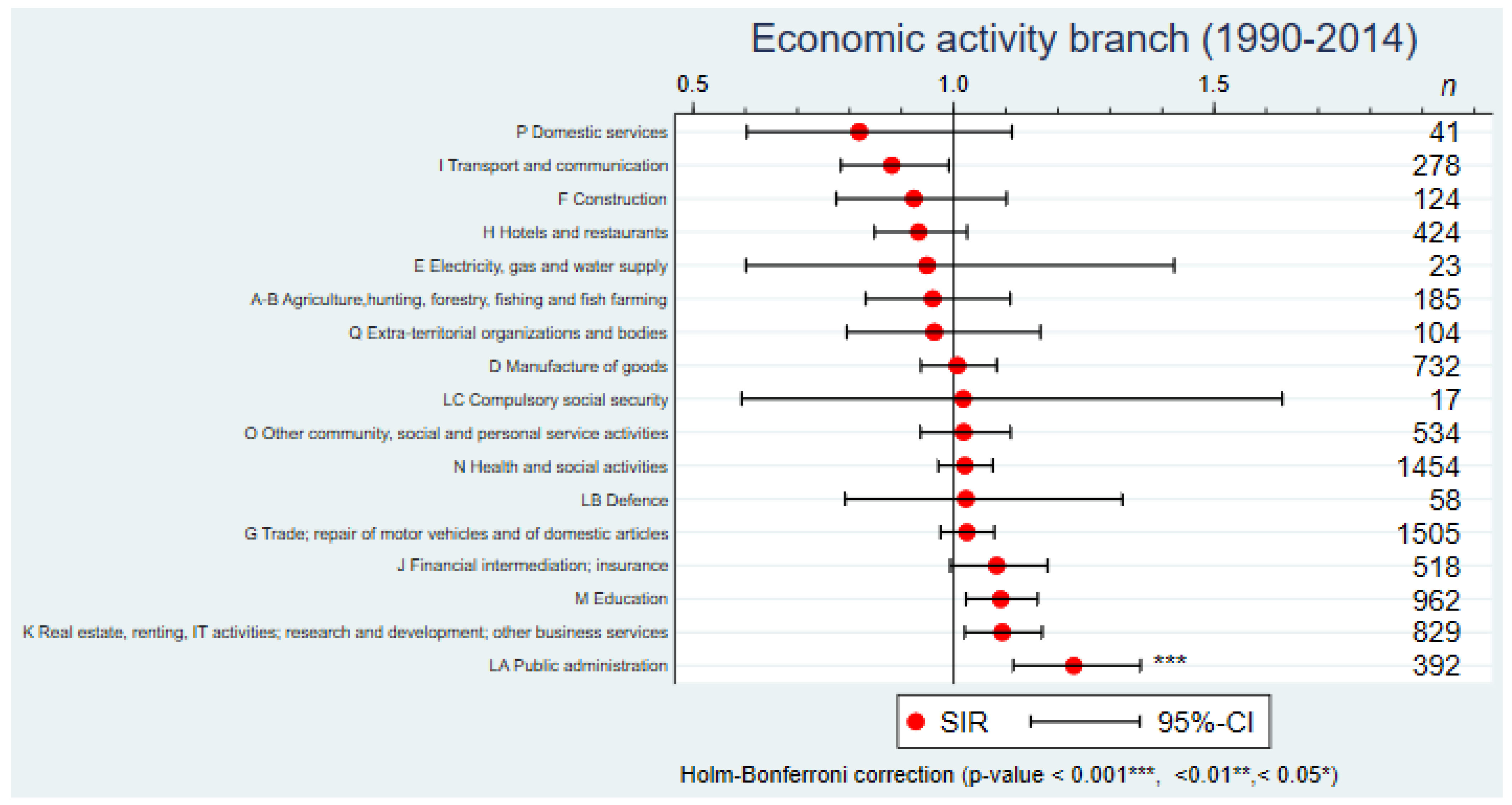
2.5.1. Standardized Incidence Ratios (SIRs)
2.5.2. Modelling BC Incidence Rates
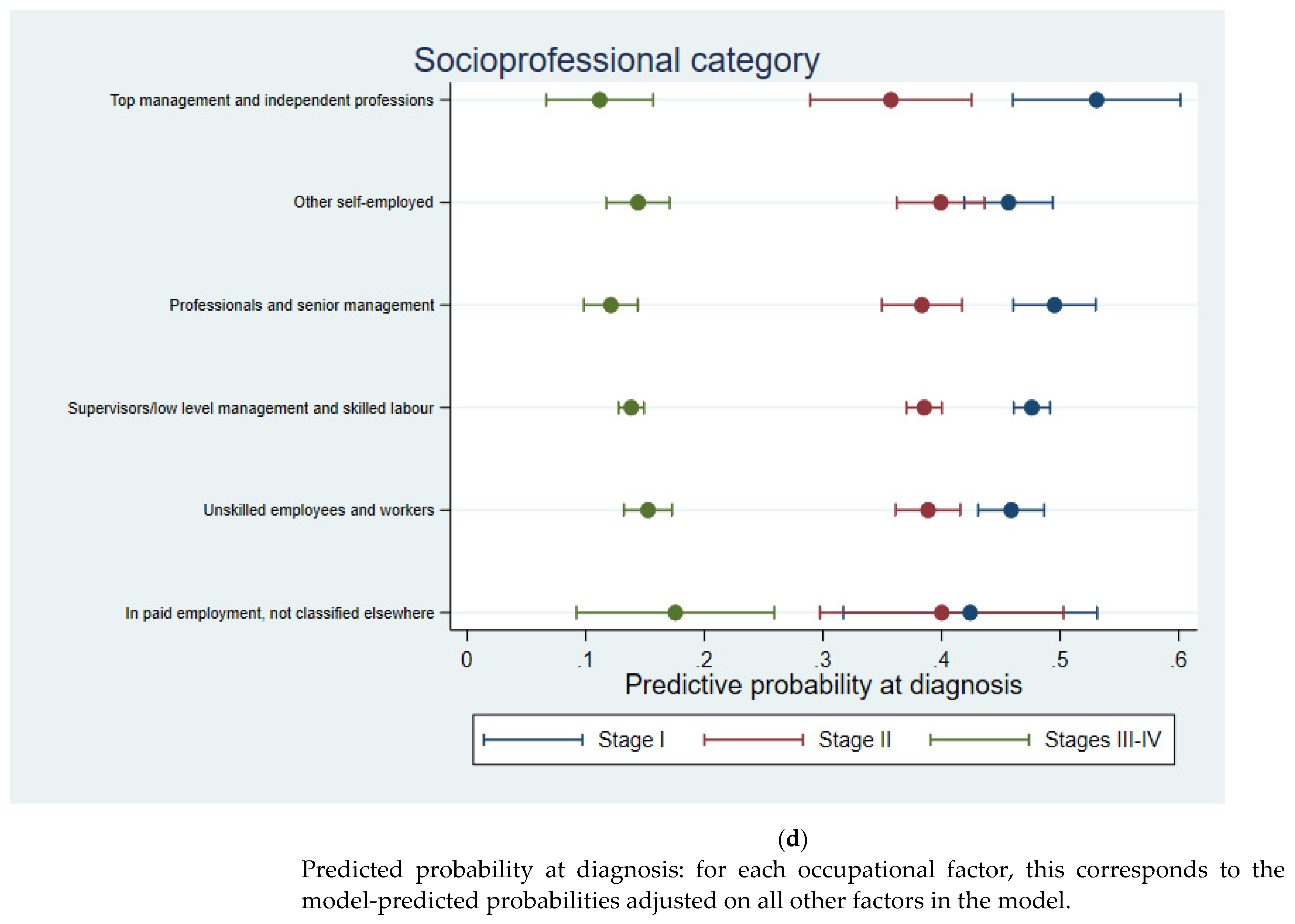
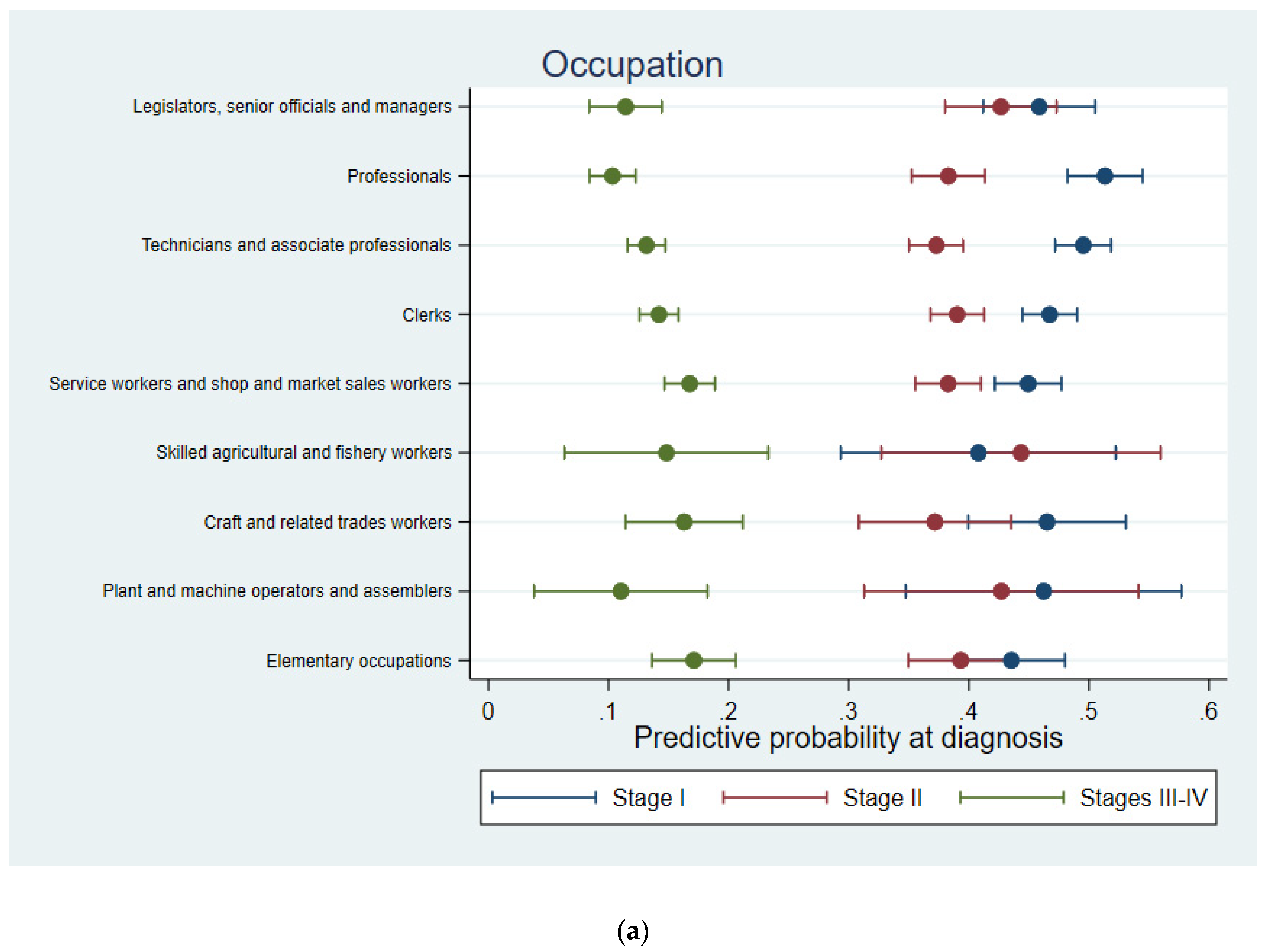
2.5.3. Modelling Stage at Diagnosis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Federal Statistical Office; National Agency for Cancer Registration; Childhood Cancer Registry. Le Cancer en Suisse, Rapport 2021—Etat des Lieux et Évolutions; Federal Statistical Office: Neuchâtel, Switzerland, 2021; p. 148.
- Tamimi, R.M.; Spiegelman, D.; Smith-Warner, S.A.; Wang, M.; Pazaris, M.; Willett, W.C.; Eliassen, A.H.; Hunter, D.J. Population attributable risk of modifiable and nonmodifiable breast cancer risk factors in postmenopausal breast cancer. Am. J. Epidemiol. 2016, 184, 884–893. [Google Scholar] [CrossRef] [Green Version]
- Lukasiewicz, S.; Czeczelewski, M.; Forma, A.; Baj, J.; Sitarz, R.; Stanislawek, A. Breast cancer-epidemiology, risk factors, classification, prognostic markers, and current treatment strategies-an updated review. Cancers 2021, 13, 4287. [Google Scholar] [CrossRef]
- Preston, D.L.; Kitahara, C.M.; Freedman, D.M.; Sigurdson, A.J.; Simon, S.L.; Little, M.P.; Cahoon, E.K.; Rajaraman, P.; Miller, J.S.; Alexander, B.H.; et al. Breast cancer risk and protracted low-to-moderate dose occupational radiation exposure in the US Radiologic Technologists Cohort, 1983–2008. Br. J. Cancer 2016, 115, 1105–1112. [Google Scholar] [CrossRef] [Green Version]
- Weiderpass, E.; Pukkala, E.; Kauppinen, T.; Mutanen, P.; Paakkulainen, H.; Vasama-Neuvonen, K.; Boffetta, P.; Partanen, T. Breast cancer and occupational exposures in women in Finland. Am. J. Ind. Med. 1999, 36, 48–53. [Google Scholar] [CrossRef]
- Schernhammer, E.S.; Laden, F.; Speizer, F.E.; Willett, W.C.; Hunter, D.J.; Kawachi, I.; Colditz, G.A. Rotating night shifts and risk of breast cancer in women participating in the nurses’ health study. J. Natl. Cancer Inst. 2001, 93, 1563–1568. [Google Scholar] [CrossRef] [Green Version]
- Grundy, A.; Richardson, H.; Burstyn, I.; Lohrisch, C.; SenGupta, S.K.; Lai, A.S.; Lee, D.; Spinelli, J.J.; Aronson, K.J. Increased risk of breast cancer associated with long-term shift work in Canada. Occup. Environ. Med. 2013, 70, 831–838. [Google Scholar] [CrossRef] [Green Version]
- Li, W.; Ray, R.M.; Thomas, D.B.; Davis, S.; Yost, M.; Breslow, N.; Gao, D.L.; Fitzgibbons, E.D.; Camp, J.E.; Wong, E.; et al. Shift work and breast cancer among women textile workers in Shanghai, China. Cancer Causes Control 2015, 26, 143–150. [Google Scholar] [CrossRef] [Green Version]
- Travis, R.C.; Balkwill, A.; Fensom, G.K.; Appleby, P.N.; Reeves, G.K.; Wang, X.S.; Roddam, A.W.; Gathani, T.; Peto, R.; Green, J.; et al. Night Shift Work and Breast Cancer Incidence: Three Prospective Studies and Meta-analysis of Published Studies. J. Natl. Cancer Inst. 2016, 108, djw169. [Google Scholar] [CrossRef]
- Cordina-Duverger, E.; Menegaux, F.; Popa, A.; Rabstein, S.; Harth, V.; Pesch, B.; Bruning, T.; Fritschi, L.; Glass, D.C.; Heyworth, J.S.; et al. Night shift work and breast cancer: A pooled analysis of population-based case-control studies with complete work history. Eur. J. Epidemiol. 2018, 33, 369–379. [Google Scholar] [CrossRef]
- Feller, A.; Schmidlin, K.; Bordoni, A.; Bouchardy, C.; Bulliard, J.L.; Camey, B.; Konzelmann, I.; Maspoli, M.; Wanner, M.; Clough-Gorr, K.M.; et al. Socioeconomic and demographic disparities in breast cancer stage at presentation and survival: A Swiss population-based study. Int. J. Cancer 2017, 141, 1529–1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lundqvist, A.; Andersson, E.; Ahlberg, I.; Nilbert, M.; Gerdtham, U. Socioeconomic inequalities in breast cancer incidence and mortality in Europe-a systematic review and meta-analysis. Eur. J. Public Health 2016, 26, 804–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.; Zhang, J.; Huang, R.; Feng, W.L.; Kong, Y.N.; Xu, F.; Zhao, L.; Song, Q.K.; Li, J.; Zhang, B.N.; et al. Influence of occupation and education level on breast cancer stage at diagnosis, and treatment options in China: A nationwide, multicenter 10-year epidemiological study. Medicine 2017, 96, e6641. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Luo, L.; McLafferty, S. Healthcare access, socioeconomic factors and late-stage cancer diagnosis: An exploratory spatial analysis and public policy implication. Int. J. Public Policy 2010, 5, 237–258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renaud, A. Methodology Report—Coverage Estimation for the Swiss Population Census 2000; Federal Statistical Office: Neuchâtel, Switzerland, 2004; p. 153.
- Spoerri, A.; Zwahlen, M.; Egger, M.; Bopp, M. The Swiss National Cohort: A unique database for national and international researchers. Int. J. Public Health 2010, 55, 239–242. [Google Scholar] [CrossRef] [Green Version]
- Working Group Report. International rules for multiple primary cancers (ICD-0 third edition). Eur. J. Cancer Prev. 2005, 14, 307–308. [Google Scholar] [CrossRef]
- Sobin, L.; Gospodarowicz, M.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; Wiley-Blackwell: Chichester, United Kingdom, 2009. [Google Scholar]
- Milner, A.; Spittal, M.J.; Pirkis, J.; LaMontagne, A.D. Suicide by occupation: Systematic review and meta-analysis. Br. J. Psychiatry 2013, 203, 409–416. [Google Scholar] [CrossRef]
- Guseva Canu, I.; Bovio, N.; Mediouni, Z.; Bochud, M.; Wild, P.; Swiss National, C. Suicide mortality follow-up of the Swiss National Cohort (1990–2014): Sex-specific risk estimates by occupational socio-economic group in working-age population. Soc. Psychiatry Psychiatr. Epidemiol. 2019, 54, 1483–1495. [Google Scholar] [CrossRef]
- Federal Statistical Office. Catégories Socioprofessionnelles (CSP) 2010—Opérationnalisation des CSP dans le Système des Variables-Clés SHAPE dès 2010; Federal Statistical Office: Neuchâtel, Switzerland, 2017.
- Bulliard, J.-L.; Brändle, K.; Fracheboud, J.; Zwahlen, M. Breast Cancer Screening Programmes in Switzerland, 2010–2018; Unisanté: Lausanne, Switzerland, 2021; p. 23. [Google Scholar]
- Smith, D.; Thomson, K.; Bambra, C.; Todd, A. The breast cancer paradox: A systematic review of the association between area-level deprivation and breast cancer screening uptake in Europe. Cancer Epidemiol. 2019, 60, 77–85. [Google Scholar] [CrossRef]
- Jack, R.H.; Moller, H.; Robson, T.; Davies, E.A. Breast cancer screening uptake among women from different ethnic groups in London: A population-based cohort study. BMJ Open 2014, 4, e005586. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Han, M.; Chen, Z.; Tang, Y.; Ma, J.; Zhang, Z.; Liu, Z.; Zhang, N.; Xi, C.; Liu, J.; et al. Does marital status correlate with the female breast cancer risk? A systematic review and meta-analysis of observational studies. PLoS ONE 2020, 15, e0229899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panczak, R.; Galobardes, B.; Voorpostel, M.; Spoerri, A.; Zwahlen, M.; Egger, M.; Swiss National, C.; Swiss Household, P. A Swiss neighbourhood index of socioeconomic position: Development and association with mortality. J. Epidemiol. Community Health 2012, 66, 1129–1136. [Google Scholar] [CrossRef] [PubMed]
- Holm, S. A simple sequentially rejective multiple test procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Villeneuve, S.; Fevotte, J.; Anger, A.; Truong, T.; Lamkarkach, F.; Gaye, O.; Kerbrat, P.; Arveux, P.; Miglianico, L.; Imbernon, E.; et al. Breast cancer risk by occupation and industry: Analysis of the CECILE study, a population-based case-control study in France. Am. J. Ind. Med. 2011, 54, 499–509. [Google Scholar] [CrossRef] [PubMed]
- Khalis, M.; El Rhazi, K.; Fort, E.; Chajes, V.; Charaka, H.; Huybrechts, I.; Moskal, A.; Biessy, C.; Romieu, I.; Abbass, F.; et al. Occupation and risk of female breast cancer: A case-control study in Morocco. Am. J. Ind. Med. 2019, 62, 838–846. [Google Scholar] [CrossRef]
- Rodgers, K.M.; Udesky, J.O.; Rudel, R.A.; Brody, J.G. Environmental chemicals and breast cancer: An updated review of epidemiological literature informed by biological mechanisms. Environ. Res. 2018, 160, 152–182. [Google Scholar] [CrossRef]
- Ekenga, C.C.; Parks, C.G.; Sandler, D.P. Chemical exposures in the workplace and breast cancer risk: A prospective cohort study. Int. J. Cancer 2015, 137, 1765–1774. [Google Scholar] [CrossRef] [Green Version]
- Videnros, C.; Selander, J.; Wiebert, P.; Albin, M.; Plato, N.; Borgquist, S.; Manjer, J.; Gustavsson, P. Investigating the risk of breast cancer among women exposed to chemicals: A nested case-control study using improved exposure estimates. Int. Arch. Occup. Environ. Health 2020, 93, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, J.E.; Strandberg-Larsen, K.; Andersson, M.; Hansen, J. Breast cancer among Danish women occupationally exposed to diesel exhaust and polycyclic aromatic hydrocarbons, 1964–2016. Scand. J. Work Environ. Health 2021, 47, 154–162. [Google Scholar] [CrossRef]
- Bulliard, J.-L.; De Landtsheer, J.-P.; Levi, F. Reattendance in the Swiss mammography screening pilot programme. J. Med. Screen. 2004, 11, 59–64. [Google Scholar] [CrossRef] [Green Version]
- Cullati, S.; von Arx, M.; Courvoisier, D.S.; Sandoval, J.L.; Manor, O.; Burton-Jeangros, C.; Bouchardy, C.; Guessous, I. Organised population-based programmes and change in socioeconomic inequalities in mammography screening: A 1992–2012 nationwide quasi-experimental study. Prev. Med. 2018, 116, 19–26. [Google Scholar] [CrossRef] [PubMed]
- John, E.M.; Phipps, A.I.; Hines, L.M.; Koo, J.; Ingles, S.A.; Baumgartner, K.B.; Slattery, M.L.; Wu, A.H. Menstrual and reproductive characteristics and breast cancer risk by hormone receptor status and ethnicity: The Breast Cancer Etiology in Minorities study. Int. J. Cancer 2020, 147, 1808–1822. [Google Scholar] [CrossRef] [PubMed]
- Aoki, R.F.; Uong, S.P.; Gomez, S.L.; Alexeeff, S.E.; Caan, B.J.; Kushi, L.H.; Torres, J.M.; Guan, A.; Canchola, A.J.; Morey, B.N.; et al. Individual- and neighborhood-level socioeconomic status and risk of aggressive breast cancer subtypes in a pooled cohort of women from Kaiser Permanente Northern California. Cancer 2021, 127, 4602–4612. [Google Scholar] [CrossRef] [PubMed]
- Kresovich, J.K.; Erdal, S.; Chen, H.Y.; Gann, P.H.; Argos, M.; Rauscher, G.H. Metallic air pollutants and breast cancer heterogeneity. Environ. Res. 2019, 177, 108639. [Google Scholar] [CrossRef] [PubMed]
- Linnenbringer, E.; Gehlert, S.; Geronimus, A.T. Black-White disparities in breast cancer subtype: The intersection of socially patterned stress and genetic expression. AIMS Public Health 2017, 4, 526–556. [Google Scholar] [CrossRef]
- Trewin, C.B.; Hjerkind, K.V.; Johansson, A.L.V.; Strand, B.H.; Kiserud, C.E.; Ursin, G. Socioeconomic inequalities in stage-specific breast cancer incidence: A nationwide registry study of 1.1 million young women in Norway, 2000–2015. Acta Oncol. 2020, 59, 1284–1290. [Google Scholar] [CrossRef]
- Lorez, M.; Bordoni, A.; Bouchardy, C.; Bulliard, J.L.; Camey, B.; Dehler, S.; Frick, H.; Konzelmann, I.; Maspoli, M.; Mousavi, S.M.; et al. Evaluation of completeness of case ascertainment in Swiss cancer registration. Eur. J. Cancer Prev. 2017, 26, S139–S146. [Google Scholar] [CrossRef]
- Plys, E.; Bovio, N.; Arveux, P.; Bergeron, Y.; Bulliard, J.L.; Elia, N.; Fournier, E.; Konzelmann, I.; Maspoli, M.; Aylward, E.R.; et al. Research on occupational diseases in the absence of occupational data: A mixed-method study among cancer registries of Western Switzerland. Swiss Med. Wkly. 2022, 152, w30127. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n ** | (%) | n of Breast Cancers | (%) |
|---|---|---|---|---|
| Total | 381,873 | (100) | 8818 | (100) |
| Time at risk (in 100,000 person-years) | 56.08 | |||
| Period | ||||
| 1990–1994 | 274,696 | (23) | 1409 | (16) |
| 1995–1999 | 263,795 | (22) | 2023 | (23) |
| 2000–2004 | 224,828 | (19) | 1600 | (18) |
| 2005–2009 | 219,306 | (18) | 2042 | (23) |
| 2010–2014 | 214,185 | (18) | 1744 | (20) |
| Age group | ||||
| Below 50 | 322,654 | (59) | 2843 | (32) |
| Between 50 and 70 | 203,688 | (37) | 5658 | (64) |
| Over 70 | 24,643 | (4) | 317 | (4) |
| Nationality | ||||
| Swiss | 279,425 | (72) | 7120 | (81) |
| Non-Swiss | 106,152 | (28) | 1698 | (19) |
| Canton of residence | ||||
| Geneva | 113,083 | (29) | 2883 | (33) |
| Neuchâtel | 44,393 | (11) | 954 | (11) |
| Vaud | 169,979 | (44) | 3827 | (43) |
| Wallis | 59,868 | (15) | 1154 | (13) |
| Socioprofessional category | ||||
| Top management and independent professions | 7450 | (2) | 232 | (3) |
| Other self-employed | 27,485 | (7) | 823 | (9) |
| Professionals and senior management | 35,542 | (9) | 926 | (11) |
| Supervisors/low level management and skilled labour | 234,051 | (56) | 5003 | (57) |
| Unskilled employees and workers | 100,259 | (24) | 1711 | (19) |
| In paid employment, not classified elsewhere | 12,689 | (3) | 123 | (1) |
| Skill level required for the occupation | ||||
| Lowest skill level | 54,831 | (13) | 707 | (8) |
| Second lowest skill level | 206,451 | (49) | 4281 | (49) |
| Second highest skill level | 97,576 | (23) | 2124 | (24) |
| Highest skill level | 65,869 | (16) | 1706 | (19) |
| Marital status | ||||
| Single | 137,586 | (33) | 1679 | (19) |
| Married | 216,093 | (53) | 5368 | (61) |
| Widowed | 11,011 | (3) | 388 | (4) |
| Divorced | 46,686 | (11) | 1383 | (16) |
| Age at the start of follow-up (mean) | 36.68 | |||
| Age at the end of follow-up (mean) | 51.36 | |||
| Follow-up duration in years (mean) | 14.69 | |||
| Occupational Variables | Nb Cases | Person-Years (in 100,000) | Models 1 * RR [95%CI] | Models 2 ** RR [95%CI] | Models 3 *** RR [95%CI] | |||
|---|---|---|---|---|---|---|---|---|
| Occupation a | p < 0.001 | p < 0.001 | p < 0.001 | |||||
| 1. Legislators, senior officials and managers | 524 | 2.78 | 1.00 | Ref. | 1.00 | Ref. | 1.00 | Ref. |
| 2. Professionals | 1182 | 6.09 | 1.04 | [0.93,1.17] | 1.13 | [1.00,1.26] | 1.14 | [1.01,1.27] |
| 3. Technicians and associate professionals | 2124 | 13.37 | 0.90 | [0.81,1.00] | 1.00 | [0.90,1.11] | 1.01 | [0.91,1.12] |
| 4. Clerks | 2283 | 14.18 | 0.98 | [0.88,1.09] | 1.06 | [0.95,1.18] | 1.06 | [0.95,1.18] |
| 5. Service workers and shop and market sales workers | 1529 | 10.83 | 0.82 | [0.74,0.92] | 0.92 | [0.82,1.03] | 0.93 | [0.83,1.03] |
| 6. Skilled agricultural and fishery workers | 101 | 0.71 | 0.75 | [0.59,0.96] | 0.82 | [0.64,1.05] | 0.82 | [0.64,1.05] |
| 7. Craft and related trades workers | 275 | 1.71 | 0.84 | [0.71,0.99] | 0.90 | [0.77,1.06] | 0.92 | [0.78,1.08] |
| 8. Plant and machine operators and assemblers | 93 | 0.60 | 0.80 | [0.63,1.01] | 0.82 | [0.64,1.04] | 0.83 | [0.65,1.05] |
| 9. Elementary occupations | 707 | 5.80 | 0.80 | [0.71,0.91] | 0.77 | [0.68,0.88] | 0.78 | [0.68,0.88] |
| Socioprofessional category | p < 0.001 | p < 0.001 | p < 0.001 | |||||
| Top management and independent professions | 232 | 0.98 | 1.00 | Ref. | 1.00 | Ref. | 1.00 | Ref. |
| Other self-employed | 823 | 3.68 | 1.01 | [0.86,1.18] | 0.97 | [0.82,1.14] | 0.96 | [0.82,1.12] |
| Professionals and senior management | 926 | 4.83 | 0.84 | [0.71,0.98] | 0.96 | [0.82,1.12] | 0.97 | [0.83,1.14] |
| Supervisors/low level management and skilled labour | 5003 | 33.31 | 0.73 | [0.63,0.84] | 0.87 | [0.75,1.01] | 0.89 | [0.77,1.02] |
| Unskilled employees and workers | 1711 | 12.02 | 0.71 | [0.61,0.82] | 0.75 | [0.64,0.87] | 0.77 | [0.66,0.89] |
| In paid employment, not classified elsewhere | 123 | 1.25 | 0.67 | [0.52,0.87] | 0.67 | [0.52,0.87] | 0.70 | [0.54,0.90] |
| Skill level required for the occupation | p < 0.001 | p < 0.001 | p < 0.001 | |||||
| Lowest skill level | 707 | 5.80 | 1.00 | Ref. | 1.00 | Ref. | 1.00 | Ref. |
| 2nd lowest skill level | 4281 | 28.03 | 1.12 | [1.02,1.23] | 1.27 | [1.15,1.39] | 1.26 | [1.15,1.39] |
| 2nd highest skill level | 2124 | 13.37 | 1.12 | [1.01,1.24] | 1.30 | [1.17,1.43] | 1.29 | [1.16,1.43] |
| Highest skill level | 1706 | 8.88 | 1.28 | [1.16,1.42] | 1.40 | [1.27,1.56] | 1.39 | [1.25,1.54] |
| Economic activity branch b | p < 0.001 | p < 0.001 | p < 0.001 | |||||
| Unknown | 636 | 3.35 | 1.09 | [0.98,1.21] | 1.05 | [0.94,1.16] | 1.06 | [0.95,1.17] |
| A–B Agriculture, hunting, forestry, fishing and fish farming | 185 | 1.03 | 1.00 | [0.84,1.19] | 0.97 | [0.81,1.15] | 0.94 | [0.79,1.12] |
| C Mining and quarrying | 2 | 0.01 | 0.71 | [0.16,3.07] | 0.76 | [0.18,3.28] | 0.76 | [0.18,3.28] |
| D Manufacture of goods | 732 | 4.99 | 0.90 | [0.81,1.00] | 0.94 | [0.85,1.04] | 0.95 | [0.85,1.05] |
| E Electricity, gas and water supply | 23 | 0.16 | 0.77 | [0.49,1.19] | 0.82 | [0.53,1.28] | 0.82 | [0.53,1.28] |
| F Construction | 124 | 0.84 | 0.79 | [0.64,0.97] | 0.79 | [0.64,0.97] | 0.78 | [0.64,0.97] |
| G Trade; repair of motor vehicles and of domestic articles | 1505 | 9.84 | 0.93 | [0.85,1.01] | 0.95 | [0.87,1.03] | 0.95 | [0.88,1.04] |
| H Hotels and restaurants | 424 | 3.37 | 0.78 | [0.69,0.88] | 0.84 | [0.74,0.94] | 0.85 | [0.76,0.97] |
| I Transport and communication | 278 | 2.39 | 0.68 | [0.59,0.79] | 0.74 | [0.65,0.86] | 0.75 | [0.65,0.86] |
| J Financial intermediation; insurance | 518 | 3.69 | 0.92 | [0.82,1.03] | 0.97 | [0.86,1.09] | 0.98 | [0.88,1.10] |
| K Real estate, renting, IT activities; research and development; other business services | 829 | 5.39 | 0.91 | [0.83,1.00] | 0.96 | [0.87,1.06] | 0.98 | [0.89,1.08] |
| LA Public administration | 392 | 1.95 | 1.19 | [1.04,1.35] | 1.11 | [0.98,1.27] | 1.09 | [0.96,1.24] |
| LB Defence | 58 | 0.32 | 0.92 | [0.70,1.22] | 0.99 | [0.75,1.30] | 0.97 | [0.74,1.29] |
| LC Compulsory social security | 17 | 0.09 | 0.91 | [0.55,1.51] | 0.94 | [0.57,1.56] | 0.94 | [0.57,1.55] |
| M Education | 962 | 5.25 | 1.12 | [1.02,1.23] | 1.05 | [0.95,1.15] | 1.04 | [0.94,1.14] |
| N Health and social activities | 1454 | 9.07 | 1.00 | Ref. | 1.00 | Ref. | 1.00 | Ref. |
| O Other community, social and personal service activities | 534 | 3.40 | 0.90 | [0.81,1.01] | 0.90 | [0.80,1.00] | 0.91 | [0.81,1.01] |
| P Domestic services | 41 | 0.37 | 0.84 | [0.57,1.23] | 0.71 | [0.49,1.03] | 0.73 | [0.50,1.06] |
| Q Extra-territorial organizations and bodies | 104 | 0.57 | 1.22 | [0.97,1.53] | 0.89 | [0.70,1.11] | 0.94 | [0.75,1.18] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bulliard, J.-L.; Bovio, N.; Arveux, P.; Bergeron, Y.; Chiolero, A.; Fournier, E.; Germann, S.; Konzelmann, I.; Maspoli, M.; Rapiti, E.; et al. Occupational Factors and Socioeconomic Differences in Breast Cancer Risk and Stage at Diagnosis in Swiss Working Women. Cancers 2022, 14, 3713. https://doi.org/10.3390/cancers14153713
Bulliard J-L, Bovio N, Arveux P, Bergeron Y, Chiolero A, Fournier E, Germann S, Konzelmann I, Maspoli M, Rapiti E, et al. Occupational Factors and Socioeconomic Differences in Breast Cancer Risk and Stage at Diagnosis in Swiss Working Women. Cancers. 2022; 14(15):3713. https://doi.org/10.3390/cancers14153713
Chicago/Turabian StyleBulliard, Jean-Luc, Nicolas Bovio, Patrick Arveux, Yvan Bergeron, Arnaud Chiolero, Evelyne Fournier, Simon Germann, Isabelle Konzelmann, Manuela Maspoli, Elisabetta Rapiti, and et al. 2022. "Occupational Factors and Socioeconomic Differences in Breast Cancer Risk and Stage at Diagnosis in Swiss Working Women" Cancers 14, no. 15: 3713. https://doi.org/10.3390/cancers14153713
APA StyleBulliard, J.-L., Bovio, N., Arveux, P., Bergeron, Y., Chiolero, A., Fournier, E., Germann, S., Konzelmann, I., Maspoli, M., Rapiti, E., & Canu, I. G. (2022). Occupational Factors and Socioeconomic Differences in Breast Cancer Risk and Stage at Diagnosis in Swiss Working Women. Cancers, 14(15), 3713. https://doi.org/10.3390/cancers14153713