
Tumor-Treating Fields in Glioblastomas: Past, Present, and Future

 ,
,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Mechanisms of Action Underlying the Effects of TTFields
2.1. Electromagnetism and the Impact of Electric Intensity and Frequency
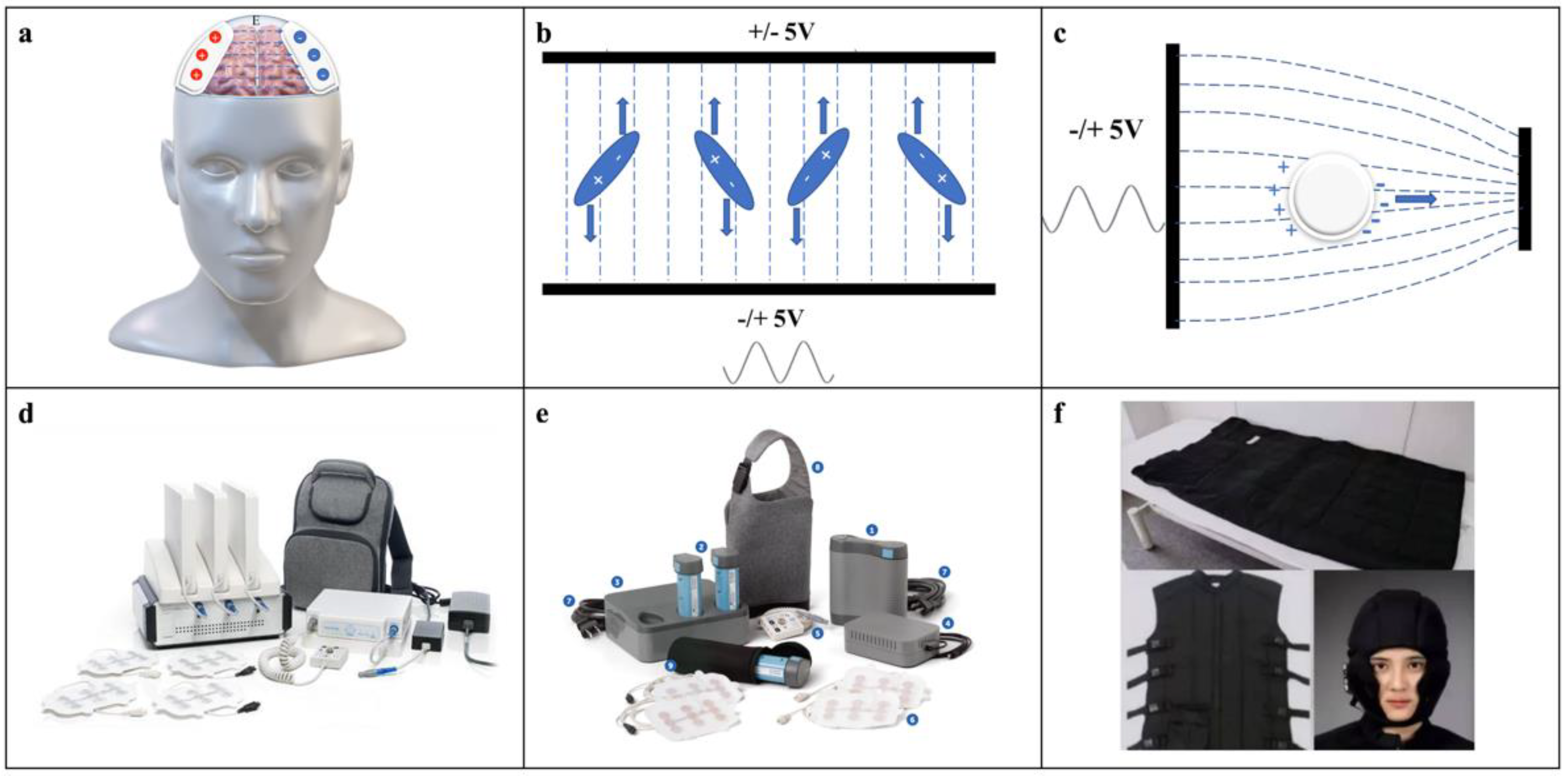
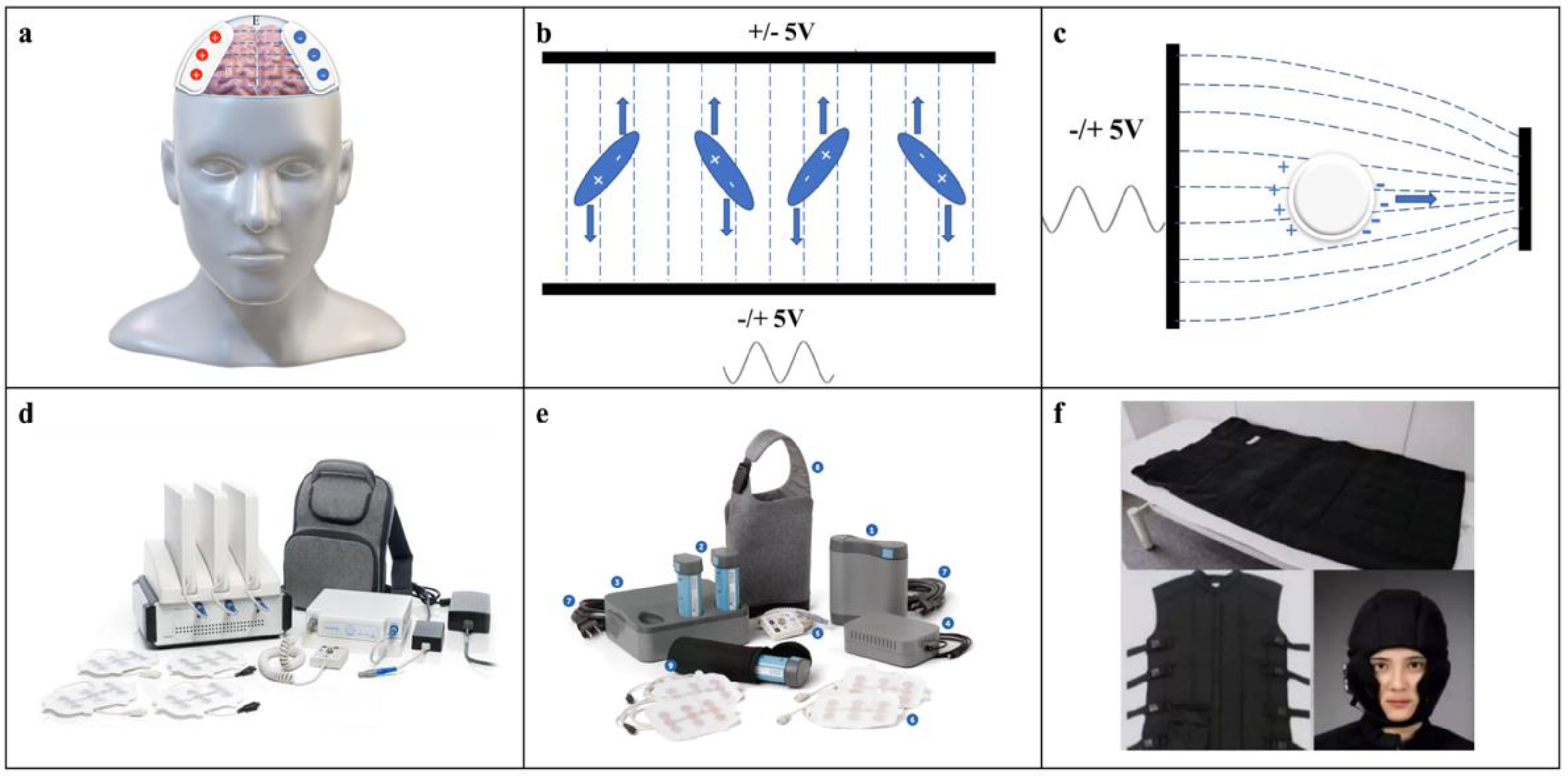
2.1.1. Electromagnetism of TTFields
2.1.2. Impact of Electric Intensity and Frequency on the Efficacy of TTFields
2.2. Biological Effects of TTFields on GBM Cells
2.2.1. Mitosis and Cell Cycle
2.2.2. Cell Autophagy
2.2.3. DNA Damage Repair and Replication
2.2.4. Cell Migration and Metastasis
2.2.5. Cell Metabolism
2.2.6. Integrity of the Cell Membrane and the Blood–Brain Barrier (BBB)
2.3. Biological Effects of TTFields on the Tumor Microenvironment (TME)
3. Clinical Studies of TTFields Treatment on GBMs
3.1. TTFields Apparatus Applied in the Clinic
3.2. Initial Trials of TTFields Applied in Human GBM Patients

{kind=link}
{kind=link}
| Study | Year | Phase | Arms | Patients | Tumor Type | Treatment Protocol | mOS | mPFS | Systemic AEs | Skin Toxicity |
|---|---|---|---|---|---|---|---|---|---|---|
| EF-14 | 2017 [4] | 3 | 2 | 695 | ndGBM | Arm1 (n = 466): TTFields plus maintenance temozolomide chemotherapy after tumor resection or biopsy and concomitant radiochemotherapy | 20.9 months | 6.7 months | 48% | 52% |
| Arm2 (n = 229): temozolomide alone after tumor resection or biopsy and concomitant radiochemotherapy | 16.0 months | 4.0 months | 44% | 0% | ||||||
| EF-14 | 2015 [5] | 3 | 2 | 315 | ndGBM | Arm1 (n = 210): TTFields plus maintenance temozolomide chemotherapy after tumor resection or biopsy and concomitant radiochemotherapy | 20.5 months | 7.1 months | 44% | 43% |
| Arm2 (n = 105): temozolomide alone after tumor resection or biopsy and concomitant radiochemotherapy | 15.6 months | 4.0 months | 44% | 0% | ||||||
| EF-11 | 2012 [16] | 3 | 2 | 237 | rGBM | Arm1 (n = 120): TTFields alone | 6.6 months | 2.2 months | 0% | 16% |
| Arm2 (n = 117): chemotherapy (physician’s best choice) | 6.0 months | 2.1 months | 16% | 0% | ||||||
| EF-07 | 2009 [85] | 1 | 1 | 10 | ndGBM | TTFields combined with maintenance temozolomide after surgery and radiation therapy | >39 months | 155 weeks | 0% | 100% |
| EF-07 | 2007 [26] | 1 | 1 | 10 | rGBM | Continuous TTFields after adjuvant temozolomide and brain surgery and/or radiotherapy for the primary tumor | 62.2 weeks | 26.1 weeks | 0% | 90% |
| EF-02 | 2008 [83] | 1 | 1 | 1 | rGBM | Continuous TTFields treatment for at least 4 weeks after heavily pretreatment with several lines of therapy | Not available | Not available | 0% | Not available |
3.3. Clinical Efficacy of TTFields in rGBM Patients
3.4. Clinical Efficacy of TTFields in ndGBMs
3.5. Combination Therapy with TTFields
3.5.1. TTFields Combined with Chemotherapy
3.5.2. TTFields Combined with Radiotherapy
3.5.3. TTFields Combined with Targeted Therapy
3.5.4. TTFields Combined with Immunotherapy
3.5.5. TTFields Combined with Other Treatment Modalities
3.5.6. Use of TTFields in Pediatric GBM Patients
3.6. Identification of Distinct Response to TTFields Treatment
3.7. Safety/Adverse Events
3.8. Health-Related Quality of Life
3.9. Real-World Cost-Effectiveness
4. Ongoing Trials of TTFields Use in GBM Patients
5. Conclusions and Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Ostrom, Q.T.; Cioffi, G.; Waite, K.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS statistical report: Primary brain and other central nervous system tumors diagnosed in the United States in 2014–2018. Neuro-Oncol. 2021, 23, iii1–iii105. [Google Scholar] [CrossRef]
- Stupp, R.; Hegi, M.E.; Mason, W.P.; van den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Stupp, R.; Mason, W.P.; van den Bent, M.J.; Weller, M.; Fisher, B.; Taphoorn, M.J.; Belanger, K.; Brandes, A.A.; Marosi, C.; Bogdahn, U.; et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N. Engl. J. Med. 2005, 352, 987–996. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Taillibert, S.; Kanner, A.; Read, W.; Steinberg, D.; Lhermitte, B.; Toms, S.; Idbaih, A.; Ahluwalia, M.S.; Fink, K.; et al. Effect of Tumor-Treating Fields Plus Maintenance Temozolomide vs Maintenance Temozolomide Alone on Survival in Patients With Glioblastoma: A Randomized Clinical Trial. JAMA 2017, 318, 2306–2316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stupp, R.; Taillibert, S.; Kanner, A.A.; Kesari, S.; Steinberg, D.M.; Toms, S.A.; Taylor, L.P.; Lieberman, F.; Silvani, A.; Fink, K.L.; et al. Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: A randomized clinical trial. JAMA 2015, 314, 2535–2543. [Google Scholar] [CrossRef]
- Chen, F.; Wendl, M.C.; Wyczalkowski, M.A.; Bailey, M.H.; Li, Y.; Ding, L. Moving pan-cancer studies from basic research toward the clinic. Nat. Cancer 2021, 2, 879–890. [Google Scholar] [CrossRef]
- Voloshin, T.; Schneiderman, R.S.; Volodin, A.; Shamir, R.R.; Kaynan, N.; Zeevi, E.; Koren, L.; Klein-Goldberg, A.; Paz, R.; Giladi, M.; et al. Tumor treating fields (TTFields) hinder cancer cell motility through regulation of microtubule and acting dynamics. Cancers 2020, 12, 3016. [Google Scholar] [CrossRef] [PubMed]
- Voloshin, T.; Kaynan, N.; Davidi, S.; Porat, Y.; Shteingauz, A.; Schneiderman, R.S.; Zeevi, E.; Munster, M.; Blat, R.; Tempel Brami, C.; et al. Tumor-treating fields (TTFields) induce immunogenic cell death resulting in enhanced antitumor efficacy when combined with anti-PD-1 therapy. Cancer Immunol. Immunother. 2020, 69, 1191–1204. [Google Scholar] [CrossRef] [Green Version]
- Lassman, A.B.; Joanta-Gomez, A.E.; Pan, P.C.; Wick, W. Current usage of tumor treating fields for glioblastoma. Neurooncol. Adv. 2020, 2, vdaa069. [Google Scholar] [CrossRef]
- Kissling, C.; Di Santo, S. Tumor treating fields-behind and beyond inhibiting the cancer cell cycle. CNS Neurol. Disord. Drug Targets 2020, 19, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.H.; Jo, Y.; Sai, S.; Park, M.J.; Kim, J.Y.; Kim, J.S.; Lee, Y.J.; Cho, J.M.; Kwak, S.Y.; Baek, J.H.; et al. Tumor-treating fields induce autophagy by blocking the Akt2/miR29b axis in glioblastoma cells. Oncogene 2019, 38, 6630–6646. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.H.; Song, H.S.; Yoo, S.H.; Yoon, M. Tumor treating fields inhibit glioblastoma cell migration, invasion and angiogenesis. Oncotarget 2016, 7, 65125–65136. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.; Le, S.B.; Hutchinson, T.E.; Calinescu, A.A.; Sebastian, M.; Jin, D.; Liu, T.; Ghiaseddin, A.; Rahman, M.; Tran, D.D. Tumor treating fields dually activate STING and AIM2 inflammasomes to induce adjuvant immunity in glioblastoma. J. Clin. Investig. 2022, 132, e149258. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, J.; Zhou, H.; Xiang, R. Primary Cilia-Related Pathways Moderate the Development and Therapy Resistance of Glioblastoma. Front. Oncol. 2021, 11, 718995. [Google Scholar] [CrossRef]
- Shi, P.; Tian, J.; Ulm, B.S.; Mallinger, J.C.; Khoshbouei, H.; Deleyrolle, L.P.; Sarkisian, M.R. Tumor Treating Fields Suppression of Ciliogenesis Enhances Temozolomide Toxicity. Front. Oncol. 2022, 12, 837589. [Google Scholar] [CrossRef] [PubMed]
- Stupp, R.; Wong, E.T.; Kanner, A.A.; Steinberg, D.; Engelhard, H.; Heidecke, V.; Kirson, E.D.; Taillibert, S.; Liebermann, F.; Dbaly, V.; et al. NovoTTF-100A versus physician’s choice chemotherapy in recurrent glioblastoma: A randomised phase III trial of a novel treatment modality. Eur. J. Cancer 2012, 48, 2192–2202. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mun, E.J.; Babiker, H.M.; Weinberg, U.; Kirson, E.D.; Von Hoff, D.D. Tumor-Treating Fields: A Fourth Modality in Cancer Treatment. Clin. Cancer Res. 2018, 24, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Palti, Y. Stimulation of muscles and nerves by means of externally applied electrodes. Bull. Res. Counc. Isr. Sect. E Exp. Med. 1962, 10, 54–56. [Google Scholar]
- Palti, Y. Stimulation of internal organs by means of externally applied electrodes. J. Appl. Physiol. 1966, 21, 1619–1623. [Google Scholar] [CrossRef] [PubMed]
- Rotshenker, S.; Palti, Y. Changes in fraction of current penetrating an axon as a function of duration of stimulating pulse. J. Theor. Biol. 1973, 41, 401–407. [Google Scholar] [CrossRef]
- Bostock, H. The strength-duration relationship for excitation of myelinated nerve: Computed dependence on membrane parameters. J. Physiol. 1983, 341, 59–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehrenberg, B.; Farkas, D.L.; Fluhler, E.N.; Lojewska, Z.; Loew, L.M. Membrane potential induced by external electric field pulses can be followed with a potentiometric dye. Biophys. J. 1987, 51, 833–837. [Google Scholar] [CrossRef] [Green Version]
- Siems, L.L.; Kosman, A.J.; Osborne, S.L. A comparative study of short wave and microwave diathermy on blood flow; the role of the somatic and sympathetic nerves in the vascular response to deep tissue heating. Arch. Phys. Med. Rehabil. 1948, 29, 759–764. [Google Scholar] [PubMed]
- Yang, W.J.; Wang, J.H. Shortwave and microwave diathermy for deep-tissue heating. Med. Biol. Eng. Comput. 1979, 17, 518–524. [Google Scholar] [CrossRef]
- Kirson, E.D.; Gurvich, Z.; Schneiderman, R.; Dekel, E.; Itzhaki, A.; Wasserman, Y.; Schatzberger, R.; Palti, Y. Disruption of cancer cell replication by alternating electric fields. Cancer Res. 2004, 64, 3288–3295. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirson, E.D.; Dbaly, V.; Tovarys, F.; Vymazal, J.; Soustiel, J.F.; Itzhaki, A.; Mordechovich, D.; Steinberg-Shapira, S.; Gurvich, Z.; Schneiderman, R.; et al. Alternating electric fields arrest cell proliferation in animal tumor models and human brain tumors. Proc. Natl. Acad. Sci. USA 2007, 104, 10152–10157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silginer, M.; Weller, M.; Stupp, R.; Roth, P. Biological activity of tumor-treating fields in preclinical glioma models. Cell Death Dis. 2017, 8, e2753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korshoej, A.R.; Hansen, F.L.; Thielscher, A.; von Oettingen, G.B.; Sorensen, J.C.H. Impact of tumor position, conductivity distribution and tissue homogeneity on the distribution of tumor treating fields in a human brain: A computer modeling study. PLoS ONE 2017, 12, e0179214. [Google Scholar] [CrossRef] [Green Version]
- Ballo, M.T.; Urman, N.; Lavy-Shahaf, G.; Grewal, J.; Bomzon, Z.; Toms, S. Correlation of Tumor Treating Fields Dosimetry to Survival Outcomes in Newly Diagnosed Glioblastoma: A Large-Scale Numerical Simulation-Based Analysis of Data from the Phase 3 EF-14 Randomized Trial. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 1106–1113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turner, S.G.; Gergel, T.; Wu, H.; Lacroix, M.; Toms, S.A. The effect of field strength on glioblastoma multiforme response in patients treated with the NovoTTF™-100A system. World J. Surg. Oncol. 2014, 12, 162. [Google Scholar] [CrossRef] [Green Version]
- Glas, M.; Ballo, M.T.; Bomzon, Z.; Urman, N.; Levi, S.; Lavy-Shahaf, G.; Jeyapalan, S.; Sio, T.T.; DeRose, P.M.; Misch, M.; et al. The Impact of Tumor Treating Fields on Glioblastoma Progression Patterns. Int. J. Radiat. Oncol. Biol. Phys. 2022, 112, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Korshoej, A.R.; Lukacova, S.; Lassen-Ramshad, Y.; Rahbek, C.; Severinsen, K.E.; Guldberg, T.L.; Mikic, N.; Jensen, M.H.; Cortnum, S.O.S.; von Oettingen, G.; et al. OptimalTTF-1: Enhancing tumor treating fields therapy with skull remodeling surgery. A clinical phase I trial in adult recurrent glioblastoma. Neurooncol. Adv. 2020, 2, vdaa121. [Google Scholar] [CrossRef] [PubMed]
- Korshoej, A.R.; Mikic, N.; Hansen, F.L.; Saturnino, G.B.; Thielscher, A.; Bomzon, Z. Enhancing Tumor Treating Fields Therapy with Skull-Remodeling Surgery. The Role of Finite Element Methods in Surgery Planning. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. 2019, 2019, 6995–6997. [Google Scholar] [PubMed]
- Branter, J.; Estevez-Cebrero, M.; Diksin, M.; Griffin, M.; Castellanos-Uribe, M.; May, S.; Rahman, R.; Grundy, R.; Basu, S.; Smith, S. Genome-wide expression and anti-proliferative effects of electric field therapy on pediatric and adult brain tumors. Int. J. Mol. Sci. 2022, 23, 1982. [Google Scholar] [CrossRef] [PubMed]
- Ahmadi-Zeidabadi, M.; Akbarnejad, Z.; Esmaeeli, M.; Masoumi-Ardakani, Y.; Mohammadipoor-Ghasemabad, L.; Eskandary, H. Impact of extremely low-frequency electromagnetic field (100 Hz, 100 G) exposure on human glioblastoma U87 cells during Temozolomide administration. Electromagn. Biol. Med. 2019, 38, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Akbarnejad, Z.; Eskandary, H.; Dini, L.; Vergallo, C.; Nematollahi-Mahani, S.N.; Farsinejad, A.; Abadi, M.F.S.; Ahmadi, M. Cytotoxicity of temozolomide on human glioblastoma cells is enhanced by the concomitant exposure to an extremely low-frequency electromagnetic field (100 Hz, 100 G). Biomed. Pharmacother. 2017, 92, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Giladi, M.; Schneiderman, R.S.; Voloshin, T.; Porat, Y.; Munster, M.; Blat, R.; Sherbo, S.; Bomzon, Z.; Urman, N.; Itzhaki, A.; et al. Mitotic spindle disruption by alternating electric fields leads to improper chromosome segregation and mitotic catastrophe in cancer cells. Sci. Rep. 2015, 5, 18046. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Yang, F.; Rubinsky, B. A Theoretical Study on the Biophysical Mechanisms by Which Tumor Treating Fields Affect Tumor Cells During Mitosis. IEEE Trans. Biomed. Eng. 2020, 67, 2594–2602. [Google Scholar] [CrossRef]
- Gera, N.; Yang, A.; Holtzman, T.S.; Lee, S.X.; Wong, E.T.; Swanson, K.D. Tumor treating fields perturb the localization of septins and cause aberrant mitotic exit. PLoS ONE 2015, 10, e0125269. [Google Scholar] [CrossRef] [Green Version]
- Jo, Y.; Kim, E.H.; Sai, S.; Kim, J.S.; Cho, J.M.; Kim, H.; Baek, J.H.; Kim, J.Y.; Hwang, S.G.; Yoon, M. Functional biological activity of sorafenib as a tumor-treating field sensitizer for glioblastoma therapy. Int. J. Mol. Sci. 2018, 19, 3684. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Yang, F.; Rubinsky, B. A Correlation Between Electric Fields That Target the Cell Membrane Potential and Dividing HeLa Cancer Cell Growth Inhibition. IEEE Trans. Biomed. Eng. 2021, 68, 1951–1956. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.M.M.; Towers, C.G.; Thorburn, A. Targeting autophagy in cancer. Nat. Rev. Cancer 2017, 17, 528–542. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.C.; Williams, B.R.; Siegel, J.J.; Amon, A. Identification of aneuploidy-selective antiproliferation compounds. Cell 2011, 144, 499–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stingele, S.; Stoehr, G.; Peplowska, K.; Cox, J.; Mann, M.; Storchova, Z. Global analysis of genome, transcriptome and proteome reveals the response to aneuploidy in human cells. Mol. Syst. Biol. 2012, 8, 608. [Google Scholar] [CrossRef] [PubMed]
- Shteingauz, A.; Porat, Y.; Voloshin, T.; Schneiderman, R.S.; Munster, M.; Zeevi, E.; Kaynan, N.; Gotlib, K.; Giladi, M.; Kirson, E.D.; et al. AMPK-dependent autophagy upregulation serves as a survival mechanism in response to Tumor Treating Fields (TTFields). Cell Death Dis. 2018, 9, 1074. [Google Scholar] [CrossRef] [Green Version]
- Giladi, M.; Munster, M.; Schneiderman, R.S.; Voloshin, T.; Porat, Y.; Blat, R.; Zielinska-Chomej, K.; Haag, P.; Bomzon, Z.; Kirson, E.D.; et al. Tumor treating fields (TTFields) delay DNA damage repair following radiation treatment of glioma cells. Radiat. Oncol. 2017, 12, 206. [Google Scholar] [CrossRef] [Green Version]
- Roy, R.; Chun, J.; Powell, S.N. BRCA1 and BRCA2: Different roles in a common pathway of genome protection. Nat. Rev. Cancer 2011, 12, 68–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karanam, N.K.; Srinivasan, K.; Ding, L.; Sishc, B.; Saha, D.; Story, M.D. Tumor-treating fields elicit a conditional vulnerability to ionizing radiation via the downregulation of BRCA1 signaling and reduced DNA double-strand break repair capacity in non-small cell lung cancer cell lines. Cell Death Dis. 2017, 8, e2711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karanam, N.K.; Ding, L.; Aroumougame, A.; Story, M.D. Tumor treating fields cause replication stress and interfere with DNA replication fork maintenance: Implications for cancer therapy. Transl. Res. 2020, 217, 33–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.J.; Cho, J.M.; Sai, S.; Oh, J.Y.; Park, J.A.; Oh, S.J.; Park, M.; Kwon, J.; Shin, U.S.; Beak, J.H.; et al. 5-fluorouracil as a tumor-treating field-sensitizer in colon cancer therapy. Cancers 2019, 11, 1999. [Google Scholar] [CrossRef] [Green Version]
- Wang, M.; Zhang, C.; Wang, X.; Yu, H.; Zhang, H.; Xu, J.; Zhao, J.; Jiang, X. Tumor-treating fields (TTFields)-based cocktail therapy: A novel blueprint for glioblastoma treatment. Am. J. Cancer Res. 2021, 11, 1069–1086. [Google Scholar]
- Lazaridis, L.; Schafer, N.; Teuber-Hanselmann, S.; Blau, T.; Schmidt, T.; Oster, C.; Weller, J.; Tzaridis, T.; Pierscianek, D.; Keyvani, K.; et al. Tumour Treating Fields (TTFields) in combination with lomustine and temozolomide in patients with newly diagnosed glioblastoma. J. Cancer Res. Clin. Oncol. 2020, 146, 787–792. [Google Scholar] [CrossRef]
- Giladi, M.; Weinberg, U.; Schneiderman, R.S.; Porat, Y.; Munster, M.; Voloshin, T.; Blatt, R.; Cahal, S.; Itzhaki, A.; Onn, A.; et al. Alternating electric fields (tumor-treating fields therapy) can improve chemotherapy treatment efficacy in non-small cell lung cancer both in vitro and in vivo. Semin. Oncol. 2014, 41, S35–S41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jo, Y.; Oh, G.; Gi, Y.; Sung, H.; Joo, E.B.; Lee, S.; Yoon, M. Tumor treating fields (TTF) treatment enhances radiation-induced apoptosis in pancreatic cancer cells. Int. J. Radiat. Biol. 2020, 96, 1528–1533. [Google Scholar] [CrossRef] [PubMed]
- Schneiderman, R.S.; Shmueli, E.; Kirson, E.D.; Palti, Y. TTFields alone and in combination with chemotherapeutic agents effectively reduce the viability of MDR cell sub-lines that over-express ABC transporters. BMC Cancer 2010, 10, 229. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.S.; Cho, J.M.; Kim, H.; Jeong, Y.K.; Kim, J.K.; Kim, E.H. Tumor treating fields can effectively overcome trastuzumab resistant breast cancer multiplication. Am. J. Cancer Res. 2021, 11, 3935–3945. [Google Scholar]
- Weller, M.; Wick, W.; Aldape, K.; Brada, M.; Berger, M.; Pfister, S.M.; Nishikawa, R.; Rosenthal, M.; Wen, P.Y.; Stupp, R.; et al. Glioma. Nat. Rev. Dis. Primers 2015, 1, 15017. [Google Scholar] [CrossRef]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- Kirson, E.D.; Giladi, M.; Gurvich, Z.; Itzhaki, A.; Mordechovich, D.; Schneiderman, R.S.; Wasserman, Y.; Ryffel, B.; Goldsher, D.; Palti, Y. Alternating electric fields (TTFields) inhibit metastatic spread of solid tumors to the lungs. Clin. Exp. Metastasis 2009, 26, 633–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oh, J.Y.; Lee, Y.J.; Kim, E.H. Tumor-Treating Fields Inhibit the Metastatic Potential of Osteosarcoma Cells. Technol. Cancer Res. Treat. 2020, 19, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Sarkisian, M.R.; Siebzehnrubl, D.; Hoang-Minh, L.; Deleyrolle, L.; Silver, D.J.; Siebzehnrubl, F.A.; Guadiana, S.M.; Srivinasan, G.; Semple-Rowland, S.; Harrison, J.K.; et al. Detection of primary cilia in human glioblastoma. J. Neurooncol. 2014, 117, 15–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishimura, Y.; Kasahara, K.; Shiromizu, T.; Watanabe, M.; Inagaki, M. Primary Cilia as Signaling Hubs in Health and Disease. Adv. Sci. 2019, 6, 1801138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanahan, D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022, 12, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Pavlova, N.N.; Zhu, J.; Thompson, C.B. The hallmarks of cancer metabolism: Still emerging. Cell Metab. 2022, 34, 355–377. [Google Scholar] [CrossRef] [PubMed]
- Patel, C.B.; Beinat, C.; Xie, Y.; Chang, E.; Gambhir, S.S. Tumor treating fields (TTFields) impairs aberrant glycolysis in glioblastoma as evaluated by [(18)F]DASA-23, a non-invasive probe of pyruvate kinase M2 (PKM2) expression. Neoplasia 2021, 23, 58–67. [Google Scholar] [CrossRef]
- Dayton, T.L.; Jacks, T.; Vander Heiden, M.G. PKM2, cancer metabolism, and the road ahead. EMBO Rep. 2016, 17, 1721–1730. [Google Scholar] [CrossRef] [Green Version]
- Chang, E.; Patel, C.B.; Pohling, C.; Young, C.; Song, J.; Flores, T.A.; Zeng, Y.; Joubert, L.M.; Arami, H.; Natarajan, A.; et al. Tumor treating fields increases membrane permeability in glioblastoma cells. Cell Death Discov. 2018, 4, 113. [Google Scholar] [CrossRef]
- Hong, P.; Kudulaiti, N.; Wu, S.; Nie, J.; Zhuang, D. Tumor treating fields: A comprehensive overview of the underlying molecular mechanism. Expert Rev. Mol. Diagn. 2022, 22, 19–28. [Google Scholar] [CrossRef]
- Yamada, S.; Muragaki, Y.; Maruyama, T.; Komori, T.; Okada, Y. Role of neurochemical navigation with 5-aminolevulinic acid during intraoperative MRI-guided resection of intracranial malignant gliomas. Clin. Neurol. Neurosurg. 2015, 130, 134–139. [Google Scholar] [CrossRef] [Green Version]
- Hadjipanayis, C.G.; Widhalm, G.; Stummer, W. What is the Surgical Benefit of Utilizing 5-Aminolevulinic Acid for Fluorescence-Guided Surgery of Malignant Gliomas? Neurosurgery 2015, 77, 663–673. [Google Scholar] [CrossRef] [Green Version]
- Sharabi, S.; Bresler, Y.; Ravid, O.; Shemesh, C.; Atrakchi, D.; Schnaider-Beeri, M.; Gosselet, F.; Dehouck, L.; Last, D.; Guez, D.; et al. Transient blood-brain barrier disruption is induced by low pulsed electrical fields in vitro: An analysis of permeability and trans-endothelial electric resistivity. Drug Deliv. 2019, 26, 459–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, K.; Zhang, K.; Xu, S.; Wang, X.; Zhou, Y.; Zhou, Y.; Gao, P.; Lin, J.; Ding, G.; Guo, G. EMP-induced BBB-disruption enhances drug delivery to glioma and increases treatment efficacy in rats. Bioelectromagnetics 2018, 39, 60–67. [Google Scholar] [CrossRef] [PubMed]
- Chang, E.; Pohling, C.; Beygui, N.; Patel, C.B.; Rosenberg, J.; Ha, D.H.; Gambhir, S.S. Synergistic inhibition of glioma cell proliferation by Withaferin A and tumor treating fields. J. Neurooncol. 2017, 134, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Neuhaus, E.; Zirjacks, L.; Ganser, K.; Klumpp, L.; Schuler, U.; Zips, D.; Eckert, F.; Huber, S.M. Alternating Electric Fields (TTFields) Activate Cav1.2 Channels in Human Glioblastoma Cells. Cancers 2019, 11, 110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pei, Z.; Lee, K.C.; Khan, A.; Erisnor, G.; Wang, H.Y. Pathway analysis of glutamate-mediated, calcium-related signaling in glioma progression. Biochem. Pharmacol. 2020, 176, 113814. [Google Scholar] [CrossRef] [PubMed]
- Grabowski, M.M.; Sankey, E.W.; Ryan, K.J.; Chongsathidkiet, P.; Lorrey, S.J.; Wilkinson, D.S.; Fecci, P.E. Immune suppression in gliomas. J. Neurooncol. 2021, 151, 3–12. [Google Scholar] [CrossRef]
- Park, J.I.; Song, K.H.; Jung, S.Y.; Ahn, J.; Hwang, S.G.; Kim, J.; Kim, E.H.; Song, J.Y. Tumor-Treating Fields Induce RAW264.7 Macrophage Activation Via NK-kappaB/MAPK Signaling Pathways. Technol. Cancer. Res Treat. 2019, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Simchony, H.; Diamant, D.; Ram, Z.; Volovitz, I. Evaluation of the Compatibility of Electric Tumor Treating Fields with Key Anti-tumoral T-Cell Functions. Isr. Med. Assoc. J. 2019, 21, 503. [Google Scholar]
- Diamant, G.; Goldman, H.S.; Plotnitsky, L.G.; Roitman, M.; Shiloach, T.; Globerson-Levin, A.; Eshhar, Z.; Haim, O.; Pencovich, N.; Grossman, R.; et al. T cells retain pivotal antitumoral functions under tumor-treating electric fields. J. Immunol. 2021, 207, 709–719. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Liu, R.; Liu, J.; Tang, J. Growth inhibition of malignant melanoma by intermediate frequency alternating electric fields, and the underlying mechanisms. J. Int. Med. Res. 2012, 40, 85–94. [Google Scholar] [CrossRef] [Green Version]
- Trusheim, J.; Dunbar, E.; Battiste, J.; Iwamoto, F.; Mohile, N.; Damek, D.; Bota, D.A.; Connelly, J. A state-of-the-art review and guidelines for tumor treating fields treatment planning and patient follow-up in glioblastoma. CNS Oncol. 2017, 6, 29–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palmer, J.D.; Bhamidipati, D.; Mehta, M.; Williams, N.L.; Dicker, A.P.; Werner-Wasik, M.; Shi, W. Treatment recommendations for elderly patients with newly diagnosed glioblastoma lack worldwide consensus. J. Neurooncol. 2018, 140, 421–426. [Google Scholar] [CrossRef]
- Salzberg, M.; Kirson, E.; Palti, Y.; Rochlitz, C. A pilot study with very low-intensity, intermediate-frequency electric fields in patients with locally advanced and/or metastatic solid tumors. Onkologie 2008, 31, 362–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rulseh, A.M.; Keller, J.; Klener, J.; Sroubek, J.; Dbaly, V.; Syrucek, M.; Tovarys, F.; Vymazal, J. Long-term survival of patients suffering from glioblastoma multiforme treated with tumor-treating fields. World J. Surg. Oncol. 2012, 10, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirson, E.D.; Schneiderman, R.S.; Dbaly, V.; Tovarys, F.; Vymazal, J.; Itzhaki, A.; Mordechovich, D.; Gurvich, Z.; Shmueli, E.; Goldsher, D.; et al. Chemotherapeutic treatment efficacy and sensitivity are increased by adjuvant alternating electric fields (TTFields). BMC Med. Phys. 2009, 9, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Xin, Q.; Kang, J.M. Bevacizumab for recurrent glioblastoma: A systematic review and meta-analysis. Eur. Rev. Med. Pharmacol Sci 2021, 25, 6480–6491. [Google Scholar] [PubMed]
- Toms, S.A.; Kim, C.Y.; Nicholas, G.; Ram, Z. Increased compliance with tumor treating fields therapy is prognostic for improved survival in the treatment of glioblastoma: A subgroup analysis of the EF-14 phase III trial. J. Neurooncol. 2019, 141, 467–473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hombach-Klonisch, S.; Mehrpour, M.; Shojaei, S.; Harlos, C.; Pitz, M.; Hamai, A.; Siemianowicz, K.; Likus, W.; Wiechec, E.; Toyota, B.D.; et al. Glioblastoma and chemoresistance to alkylating agents: Involvement of apoptosis, autophagy, and unfolded protein response. Pharmacol. Ther. 2018, 184, 13–41. [Google Scholar] [CrossRef] [PubMed]
- Da Ros, M.; De Gregorio, V.; Iorio, A.L.; Giunti, L.; Guidi, M.; de Martino, M.; Genitori, L.; Sardi, I. Glioblastoma chemoresistance: The double play by microenvironment and blood-brain barrier. Int. J. Mol. Sci. 2018, 19, 2879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, C.Y.; Paek, S.H.; Nam, D.H.; Chang, J.H.; Hong, Y.K.; Kim, J.H.; Kim, O.L.; Kim, S.H. Tumor treating fields plus temozolomide for newly diagnosed glioblastoma: A sub-group analysis of Korean patients in the EF-14 phase 3 trial. J. Neurooncol. 2020, 146, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Herrlinger, U.; Tzaridis, T.; Mack, F.; Steinbach, J.P.; Schlegel, U.; Sabel, M.; Hau, P.; Kortmann, R.D.; Krex, D.; Grauer, O.; et al. Lomustine-temozolomide combination therapy versus standard temozolomide therapy in patients with newly diagnosed glioblastoma with methylated MGMT promoter (CeTeG/NOA-09): A randomised, open-label, phase 3 trial. Lancet 2019, 393, 678–688. [Google Scholar] [CrossRef]
- Kim, E.H.; Kim, Y.H.; Song, H.S.; Jeong, Y.K.; Lee, J.Y.; Sung, J.; Yoo, S.H.; Yoon, M. Biological effect of an alternating electric field on cell proliferation and synergistic antimitotic effect in combination with ionizing radiation. Oncotarget 2016, 7, 62267–62279. [Google Scholar] [CrossRef] [Green Version]
- Lee, W.S.; Seo, S.J.; Chung, H.K.; Park, J.W.; Kim, J.K.; Kim, E.H. Tumor-treating fields as a proton beam-sensitizer for glioblastoma therapy. Am. J. Cancer Res. 2021, 11, 4582–4594. [Google Scholar] [PubMed]
- Bokstein, F.; Blumenthal, D.; Limon, D.; Harosh, C.B.; Ram, Z.; Grossman, R. Concurrent tumor treating fields (TTFields) and radiation therapy for newly diagnosed glioblastoma: A prospective safety and feasibility study. Front. Oncol. 2020, 10, 411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stein, M.; Dohmen, H.; Wolk, B.; Eberle, F.; Kolodziej, M.; Acker, T.; Uhl, E.; Jensen, A. Case Report of Complete Radiological Response of a Thalamic Glioblastoma After Treatment With Proton Therapy Followed by Temozolomide and Tumor-Treating Fields. Front. Oncol. 2020, 10, 477. [Google Scholar] [CrossRef] [Green Version]
- Miller, R.; Song, A.; Ali, A.; Niazi, M.; Bar-Ad, V.; Martinez, N.; Glass, J.; Alnahhas, I.; Andrews, D.; Judy, K.; et al. Scalp-Sparing Radiation With Concurrent Temozolomide and Tumor Treating Fields (SPARE) for Patients With Newly Diagnosed Glioblastoma. Front. Oncol. 2022, 12, 896246. [Google Scholar] [CrossRef] [PubMed]
- Lu, G.; Rao, M.; Zhu, P.; Liang, B.; El-Nazer, R.T.; Fonkem, E.; Bhattacharjee, M.B.; Zhu, J.J. Triple-drug Therapy With Bevacizumab, Irinotecan, and Temozolomide Plus Tumor Treating Fields for Recurrent Glioblastoma: A Retrospective Study. Front. Neurol. 2019, 10, 42. [Google Scholar] [CrossRef] [Green Version]
- Wong, E.T.; Lok, E.; Swanson, K.D. Clinical benefit in recurrent glioblastoma from adjuvant NovoTTF-100A and TCCC after temozolomide and bevacizumab failure: A preliminary observation. Cancer Med. 2015, 4, 383–391. [Google Scholar] [CrossRef]
- Elzinga, G.; Wong, E.T. Resolution of cystic enhancement to add-on tumor treating electric fields for recurrent glioblastoma after incomplete response to bevacizumab. Case Rep. Neurol. 2014, 6, 109–115. [Google Scholar] [CrossRef]
- Ansstas, G.; Tran, D.D. Treatment with Tumor-Treating Fields Therapy and Pulse Dose Bevacizumab in Patients with Bevacizumab-Refractory Recurrent Glioblastoma: A Case Series. Case Rep. Neurol. 2016, 8, 1–9. [Google Scholar] [CrossRef]
- Meletath, S.K.; Pavlick, D.; Brennan, T.; Hamilton, R.; Chmielecki, J.; Elvin, J.A.; Palma, N.; Ross, J.S.; Miller, V.A.; Stephens, P.J.; et al. Personalized Treatment for a Patient With a BRAF V600E Mutation Using Dabrafenib and a Tumor Treatment Fields Device in a High-Grade Glioma Arising From Ganglioglioma. J. Natl. Compr. Canc. Netw. 2016, 14, 1345–1350. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.Y.; Jo, Y.; Oh, H.K.; Kim, E.H. Sorafenib increases tumor treating fields-induced cell death in glioblastoma by inhibiting STAT3. Am. J. Cancer Res. 2020, 10, 3475–3486. [Google Scholar] [PubMed]
- Kessler, A.F.; Frombling, G.E.; Gross, F.; Hahn, M.; Dzokou, W.; Ernestus, R.I.; Lohr, M.; Hagemann, C. Effects of tumor treating fields (TTFields) on glioblastoma cells are augmented by mitotic checkpoint inhibition. Cell Death Discov. 2018, 4, 12. [Google Scholar] [CrossRef] [Green Version]
- Wang, E.J.; Chen, J.S.; Jain, S.; Morshed, R.A.; Haddad, A.F.; Gill, S.; Beniwal, A.S.; Aghi, M.K. Immunotherapy resistance in glioblastoma. Front. Genet. 2021, 12, 750675. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Liu, P.; Xing, H.; Wen, X.; Wang, Y.; Hu, C.; Li, L.; Ma, W. Skull modulated strategies to intensify tumor treating fields on brain tumor: A finite element study. Biomech. Model. Mechanobiol. 2022, 21, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y.; Han, Y.I.; Lee, E.; Seo, J.; Oh, G.; Sung, H.; Gi, Y.; Kim, H.; Park, S.; Yoon, M. The combination of tumor treating fields and hyperthermia has synergistic therapeutic effects in glioblastoma cells by downregulating STAT3. Am. J. Cancer Res. 2022, 12, 1423–1432. [Google Scholar] [PubMed]
- Green, A.L.; Mulcahy Levy, J.M.; Vibhakar, R.; Hemenway, M.; Madden, J.; Foreman, N.; Dorris, K. Tumor treating fields in pediatric high-grade glioma. Child’s Nerv. Syst. 2017, 33, 1043–1045. [Google Scholar] [CrossRef]
- Gott, H.; Kiez, S.; Dohmen, H.; Kolodziej, M.; Stein, M. Tumor treating fields therapy is feasible and safe in a 3-year-old patient with diffuse midline glioma H3K27M-a case report. Child’s Nerv. Syst. 2022. [Google Scholar] [CrossRef] [PubMed]
- Dono, A.; Mitra, S.; Shah, M.; Takayasu, T.; Zhu, J.J.; Tandon, N.; Patel, C.B.; Esquenazi, Y.; Ballester, L.Y. PTEN mutations predict benefit from tumor treating fields (TTFields) therapy in patients with recurrent glioblastoma. J. Neurooncol. 2021, 153, 153–160. [Google Scholar] [CrossRef]
- Pandey, M.; Xiu, J.; Mittal, S.; Zeng, J.; Saul, M.; Kesari, S.; Azadi, A.; Newton, H.; Deniz, K.; Ladner, K. Molecular alterations associated with improved outcome in patients with glioblastoma treated with Tumor-Treating Fields. Neurooncol. Adv. 2022, 4, vdaa069. [Google Scholar] [CrossRef]
- Mohan, S.; Chawla, S.; Wang, S.; Verma, G.; Skolnik, A.; Brem, S.; Peters, K.B.; Poptani, H. Assessment of early response to tumor-treating fields in newly diagnosed glioblastoma using physiologic and metabolic MRI: Initial experience. CNS Oncol. 2016, 5, 137–144. [Google Scholar] [CrossRef]
- Bosnyak, E.; Barger, G.R.; Michelhaugh, S.K.; Robinette, N.L.; Amit-Yousif, A.; Mittal, S.; Juhasz, C. Amino Acid PET Imaging of the Early Metabolic Response During Tumor-Treating Fields (TTFields) Therapy in Recurrent Glioblastoma. Clin. Nucl. Med. 2018, 43, 176–179. [Google Scholar] [CrossRef]
- Lacouture, M.E.; Anadkat, M.J.; Ballo, M.T.; Iwamoto, F.; Jeyapalan, S.A.; La Rocca, R.V.; Schwartz, M.; Serventi, J.N.; Glas, M. Prevention and Management of Dermatologic Adverse Events Associated With Tumor Treating Fields in Patients With Glioblastoma. Front. Oncol. 2020, 10, 1045. [Google Scholar] [CrossRef] [PubMed]
- Lacouture, M.E.; Davis, M.E.; Elzinga, G.; Butowski, N.; Tran, D.; Villano, J.L.; DiMeglio, L.; Davies, A.M.; Wong, E.T. Characterization and management of dermatologic adverse events with the NovoTTF-100A System, a novel anti-mitotic electric field device for the treatment of recurrent glioblastoma. Semin. Oncol. 2014, 41, S1–S14. [Google Scholar] [CrossRef] [Green Version]
- Mrugala, M.M.; Engelhard, H.H.; Dinh Tran, D.; Kew, Y.; Cavaliere, R.; Villano, J.L.; Annenelie Bota, D.; Rudnick, J.; Love Sumrall, A.; Zhu, J.J.; et al. Clinical practice experience with NovoTTF-100A system for glioblastoma: The patient registry dataset (PRiDe). Semin. Oncol. 2014, 41, S4–S13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cruickshank, C.N. The microanatomy of the epidermis in relation to trauma. J. Tissue Viability 2006, 16, 16–19. [Google Scholar] [CrossRef]
- Cowley, K.; Vanoosthuyze, K. Insights into shaving and its impact on skin. Br. J. Dermatol. 2012, 166, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Wolf, R.; Orion, E.; Ruocco, E.; Baroni, A.; Ruocco, V. Contact dermatitis: Facts and controversies. Clin. Dermatol. 2013, 31, 467–478. [Google Scholar] [CrossRef]
- Voegeli, D. Moisture-associated skin damage: An overview for community nurses. Br. J. Community Nurs. 2013, 18, 6–12. [Google Scholar] [CrossRef]
- Lukas, R.V.; Ratermann, K.L.; Wong, E.T.; Villano, J.L. Skin toxicities associated with tumor treating fields: Case based review. J. Neurooncol. 2017, 135, 593–599. [Google Scholar] [CrossRef]
- Oberheim-Bush, N.A.; Shi, W.; McDermott, M.W.; Grote, A.; Stindl, J.; Lustgarten, L. The safety profile of Tumor Treating Fields (TTFields) therapy in glioblastoma patients with ventriculoperitoneal shunts. J. Neuroonco.l 2022, 158, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Shukla, G.; Peng, C.; Lockamy, V.; Liu, H.; Shi, W. Dosimetric Impact of a Tumor Treating Fields Device for Glioblastoma Patients Undergoing Simultaneous Radiation Therapy. Front. Oncol. 2018, 8, 51. [Google Scholar] [CrossRef] [Green Version]
- Taphoorn, M.J.B.; Dirven, L.; Kanner, A.A.; Lavy-Shahaf, G.; Weinberg, U.; Taillibert, S.; Toms, S.A.; Honnorat, J.; Chen, T.C.; Sroubek, J.; et al. Influence of Treatment With Tumor-Treating Fields on Health-Related Quality of Life of Patients With Newly Diagnosed Glioblastoma: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2018, 4, 495–504. [Google Scholar] [CrossRef]
- Palmer, J.D.; Chavez, G.; Furnback, W.; Chuang, P.Y.; Wang, B.; Proescholdt, C.; Tang, C.H. Health-Related Quality of Life for Patients Receiving Tumor Treating Fields for Glioblastoma. Front. Oncol. 2021, 11, 772261. [Google Scholar] [CrossRef]
- Halasz, L.M.; Mitin, T. Tumor-Treating Fields: Answering the Concern About Quality of Life. JAMA Oncol. 2018, 4, 504–505. [Google Scholar] [CrossRef]
- Bernard-Arnoux, F.; Lamure, M.; Ducray, F.; Aulagner, G.; Honnorat, J.; Armoiry, X. The cost-effectiveness of tumor-treating fields therapy in patients with newly diagnosed glioblastoma. Neuro. Oncol. 2016, 18, 1129–1136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connock, M.; Auguste, P.; Dussart, C.; Guyotat, J.; Armoiry, X. Cost-effectiveness of tumor-treating fields added to maintenance temozolomide in patients with glioblastoma: An updated evaluation using a partitioned survival model. J. Neurooncol. 2019, 143, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Lamers, L.M.; Stupp, R.; van den Bent, M.J.; Al, M.J.; Gorlia, T.; Wasserfallen, J.B.; Mittmann, N.; Jin Seung, S.; Crott, R.; Uyl-de Groot, C.A.; et al. Cost-effectiveness of temozolomide for the treatment of newly diagnosed glioblastoma multiforme: A report from the EORTC 26981/22981 NCI-C CE3 Intergroup Study. Cancer 2008, 112, 1337–1344. [Google Scholar] [CrossRef] [PubMed]
- Guzauskas, G.F.; Pollom, E.L.; Stieber, V.W.; Wang, B.C.M.; Garrison, L.P., Jr. Tumor treating fields and maintenance temozolomide for newly-diagnosed glioblastoma: A cost-effectiveness study. J. Med. Econ. 2019, 22, 1006–1013. [Google Scholar] [CrossRef]
- Wang, Z.; Ren, Y.; Du, F.; Sun, Y.; Jiang, W. Tumor treating fields combined with a poly (adenosine diphosphate-ribose) polymerase inhibitor during radiotherapy for rapidly progressing IDH-wildtype diffuse astrocytoma: A case report. J. Int. Med. Res. 2021, 49, 1–7. [Google Scholar] [CrossRef]
- Chari, A.; Vogl, D.T.; Gavriatopoulou, M.; Nooka, A.K.; Yee, A.J.; Huff, C.A.; Moreau, P.; Dingli, D.; Cole, C.; Lonial, S.; et al. Oral Selinexor-Dexamethasone for Triple-Class Refractory Multiple Myeloma. N. Engl. J. Med. 2019, 381, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Ghiaseddin, A.P.; Shin, D.; Melnick, K.; Tran, D.D. Tumor Treating Fields in the Management of Patients with Malignant Gliomas. Curr. Treat. Options Oncol. 2020, 21, 76. [Google Scholar] [CrossRef] [PubMed]

| Study Identifier | Status | Arms | Sample Size | Tumor Type | Intervention/Treatment | OS | PFS | AE | QoL | Others | Duration |
|---|---|---|---|---|---|---|---|---|---|---|---|
| NCT03501134 (ACTION) | Completed | 1 | 20 | ndGBM | TTFields | √ | 24w-MET-h/wk, 24w-sleep quality, 24w-mood state, 24w-functional capacity, 8/16/24w-average daily number of steps | 3 years | |||
| NCT03033992 | Recruiting | 1 | 25 | rGBM | TTFields | √ | ORR, EFS | 4 years | |||
| NCT03642080 | Recruiting | 1 | 48 | ndGBM, rGBM | TTFields | √ | 5 years | ||||
| NCT05086497 | Not yet recruiting | 2 | 155 | ndGBM, rGBM | TTFields + conventional/advanced MR imaging array mapping layout | √ | √ | 4 years | |||
| NCT05030298 | Not yet recruiting | 2 | 40 | ndGBM | TTFields + RT + TMZ + radiosurgery | √ | √ | √ | Toxicity | 3 years | |
| NCT02903069 | Completed | Multi | 66 | ndGBM | MRZ + TMZ ± RT ± TTFields | √ | √ | √ | MTD, drug serum concentrations | 5 years | |
| NCT04223999 (OptimalTTF-2) | Recruiting | 2 | 70 | rGBM | Skull-remodeling surgery ± TTFields | √ | √ | √ | √ | ORR, KPS | 4 years |
| NCT04218019 (GERAS) | Suspended | 2 | 68 | ndGBM | Early/late TTFields | √ | √ | √ | SCTR | 2 years | |
| NCT03223103 | Active, not recruiting | 1 | 13 | ndGBM | Poly-ICLC + TTFields + peptides | √ | √ | DLT, ORR | 5 years | ||
| NCT04469075 | Recruiting | 1 | 58 | ndGBM | Clindamycin phosphate + triamcinolone acetonide | √ | Grade 2 or higher skin toxicity | 3 years | |||
| NCT04474353 | Recruiting | 1 | 12 | ndGBM | TTFields + TMZ + SRS + gadolinium | √ | √ | DLT | 3 years | ||
| NCT04689087 | Recruiting | 1 | 40 | rGBM | TTFields + BPC | √ | √ | √ | 2 years | ||
| NCT04471844 (EF-32) | Recruiting | 2 | 950 | ndGBM | TTFields + TMZ + RT | √ | √ | √ | √ | ORR | 6 years |
| NCT04221503 | Recruiting | 2 | 30 | rGBM | Surgery + TTFields + niraparib | √ | √ | √ | Disease control, ORR | 6 years | |
| NCT03258021 (TIGER) | Active, not recruiting | 1 | 710 | ndGBM | TTFields | √ | √ | √ | √ | Compliance, reason for refusing TTFields | 4 years |
| NCT04671459 (TaRRGET) | Recruiting | 1 | 40 | rGBM | TTFields + SRS | √ | √ | Radiation necrosis range, steroid needs, ORR, patterns of failure | 3 years | ||
| NCT02893137 | Completed | 1 | 15 | ndGBM, rGBM | Craniectomy + TTFields | √ | √ | √ | √ | ORR | 3 years |
| NCT04717739 | Not yet recruiting | 1 | 500 | ndGBM, rGBM | TTFields | √ | √ | Compliance, sleep quality, neurocognitive functioning | 2 years | ||
| NCT04421378 | Recruiting | Multi | 474 | ndGBM, rGBM | Selinexor ± TTFields ± TMZ ± RT ± lomustine ± bevacizumab | √ | √ | √ | Phase 1a: maximum tolerated dose, recommended phase 2 dose; Phase 1a/1b: TTP, drug serum concentrations; Phase 2: ORR | 3 years | |
| NCT04757662 | Active, not recruiting | 1 | 18 | ndGBM | Tadalafil + TMZ + TTFields | √ | √ | √ | MDSC change, severe lymphopenia, HDI | 2 years | |
| NCT00916409 | Completed | 2 | 700 | ndGBM | TMZ ± TTFields | √ | √ | 8 years | |||
| NCT04492163 (EF-33) | Recruiting | 2 | 24 | rGBM | TTFields | √ | √ | √ | ORR | 2 years | |
| NCT01954576 | Terminated | 1 | 21 | rGBM | TTFields | √ | √ | ORR, genetic signature of response | 8 years | ||
| NCT03194971 | Recruiting | 2 | 20 | ndGBM, rGBM | TTFields | States of mitotically cells | 7 years | ||||
| NCT03405792 (2-THE-TOP) | Active, not recruiting | 1 | 31 | ndGBM | TMZ + TTFields + pembrolizumab | √ | √ | Toxicity and tolerability, immune reaction by pembrolizumab | 5 years |
| Positive Characteristics | Negative Characteristics |
|---|---|
| Mechanisms of action | Mechanisms of action |
| Disturbing mitosis and cell cycle | Still imperfectly unelucidated |
| Delaying DNA damage repair process | |
| Enhancing cell autophagy | Clinical efficacy |
| Inhibiting cell metabolism and angiogenesis | Phase 3 trials on combination therapy are needed |
| Limiting cancer cell migration and metastasis | |
| Increasing the permeability of cancer cell membrane and blood–brain barrier | Acceptance of the use of TTFields in the real world |
| Strengthening intratumoral immunity by turning the “cold” TME into “hot” | Very low (<12% to <16%) |
| Clinical efficacy | |
| Prolonged OS and PFS in ndGBM patients | Safety/adverse events |
| Prolonged OS and PFS in rGBM patients | Dermatologic events, mostly mild to moderate |
| Additional survival benefit when combined with other treatment modalities | |
| Quality of life | Real-world cost-effectiveness |
| No significant differences after adding TTFields to the standard protocol | Above the willingness-to-pay threshold |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guo, X.; Yang, X.; Wu, J.; Yang, H.; Li, Y.; Li, J.; Liu, Q.; Wu, C.; Xing, H.; Liu, P.; et al. Tumor-Treating Fields in Glioblastomas: Past, Present, and Future. Cancers 2022, 14, 3669. https://doi.org/10.3390/cancers14153669
Guo X, Yang X, Wu J, Yang H, Li Y, Li J, Liu Q, Wu C, Xing H, Liu P, et al. Tumor-Treating Fields in Glioblastomas: Past, Present, and Future. Cancers. 2022; 14(15):3669. https://doi.org/10.3390/cancers14153669
Chicago/Turabian StyleGuo, Xiaopeng, Xin Yang, Jiaming Wu, Huiyu Yang, Yilin Li, Junlin Li, Qianshu Liu, Chen Wu, Hao Xing, Penghao Liu, and et al. 2022. "Tumor-Treating Fields in Glioblastomas: Past, Present, and Future" Cancers 14, no. 15: 3669. https://doi.org/10.3390/cancers14153669
APA StyleGuo, X., Yang, X., Wu, J., Yang, H., Li, Y., Li, J., Liu, Q., Wu, C., Xing, H., Liu, P., Wang, Y., Hu, C., & Ma, W. (2022). Tumor-Treating Fields in Glioblastomas: Past, Present, and Future. Cancers, 14(15), 3669. https://doi.org/10.3390/cancers14153669