
Effectiveness of Geriatric Assessment-Driven Interventions on Survival and Functional and Nutritional Status in Older Patients with Head and Neck Cancer: A Randomized Controlled Trial (EGeSOR)

 ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Experimental Design
2.2. Setting
2.3. Participants
2.4. Intervention
2.5. Outcomes
2.6. Collected Data
2.7. Sample Size
2.8. Randomization
2.9. Statistical Analysis
3. Results
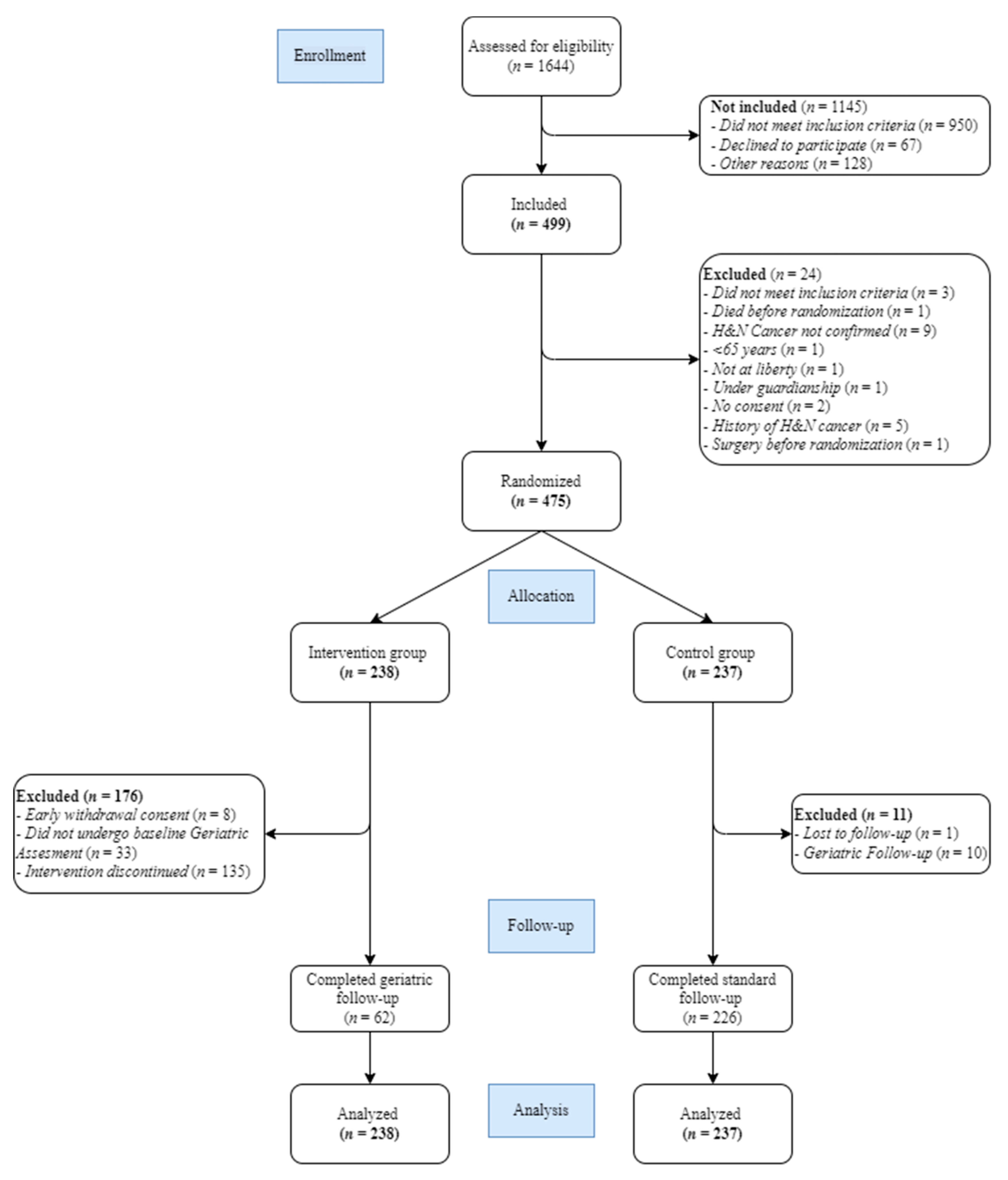
3.1. Description of the Population
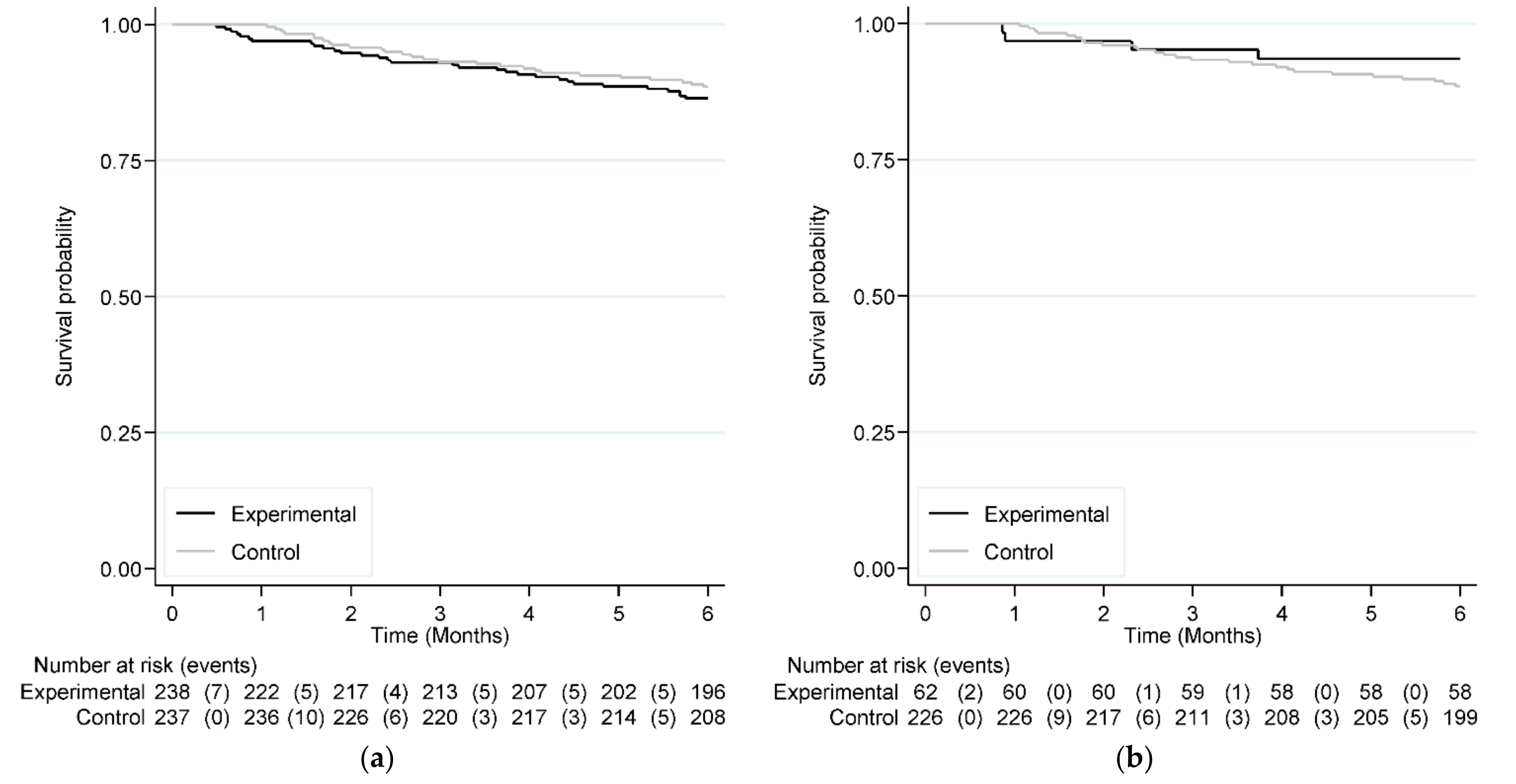
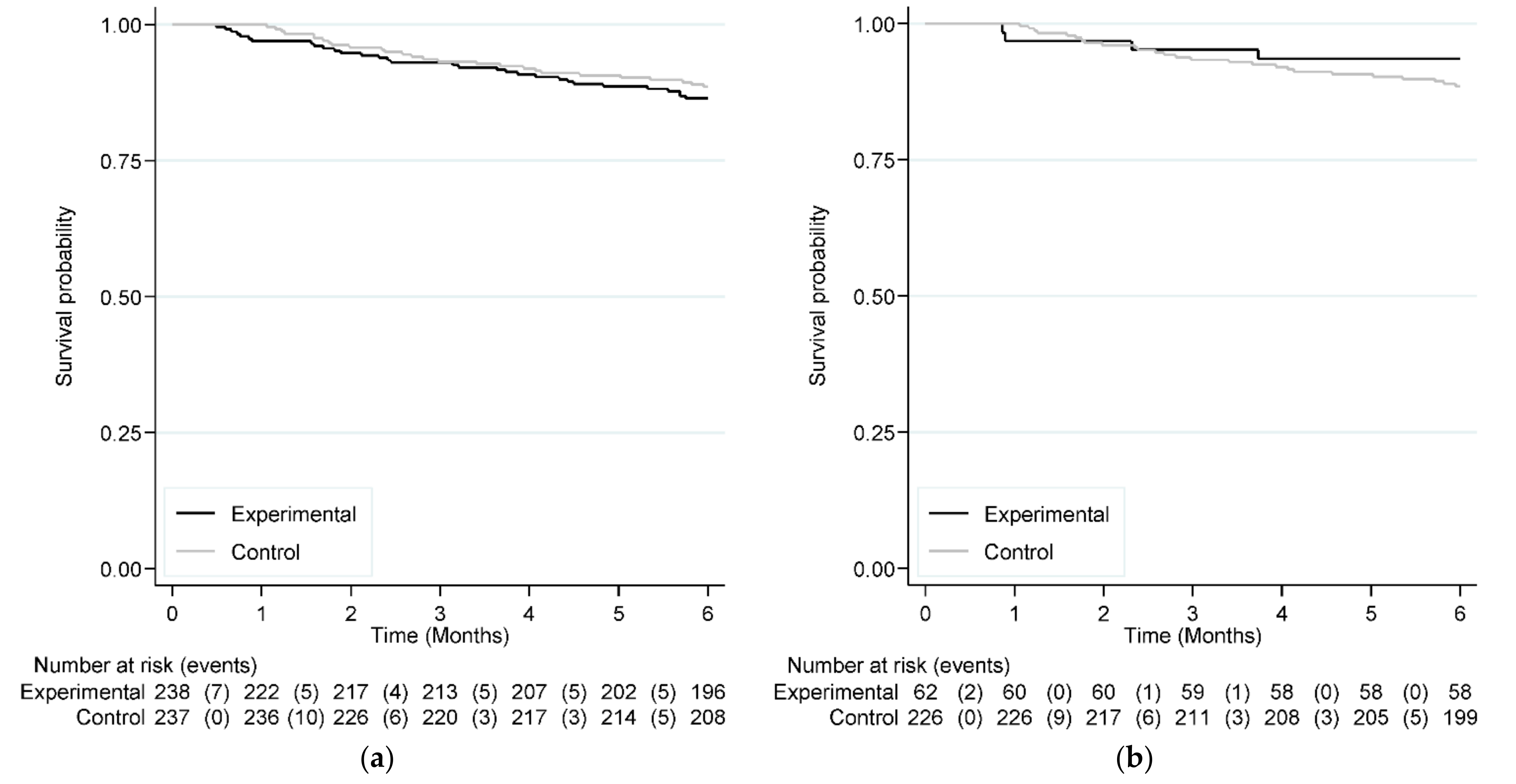
3.2. Efficacy Analysis for the Primary Outcome
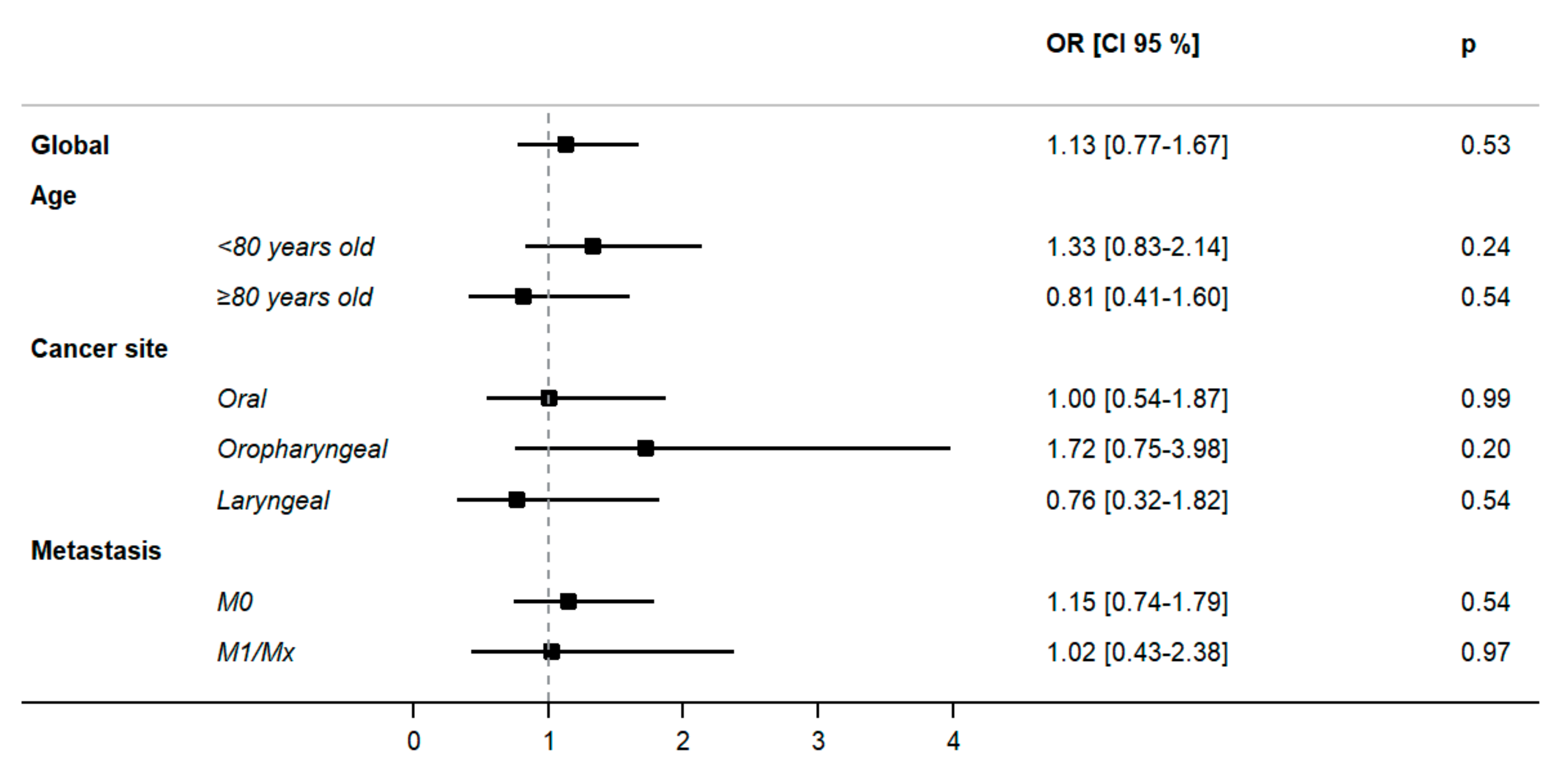
3.3. Subgroup Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Huang, S.H.; O’Sullivan, B.; Waldron, J.; Lockwood, G.; Bayley, A.; Kim, J.; Cummings, B.; Dawson, L.A.; Hope, A.; Cho, J.; et al. Patterns of care in elderly head-and-neck cancer radiation oncology patients: A single-center cohort study. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Guigay, J. Things are changing for head and neck squamous cell carcinomas. Curr. Opin. Oncol. 2019, 31, 121. [Google Scholar] [CrossRef] [PubMed]
- Canoui-Poitrine, F.; Lievre, A.; Dayde, F.; Lopez-Trabada-Ataz, D.; Baumgaertner, I.; Dubreuil, O.; Brunetti, F.; Coriat, R.; Maley, K.; Pernot, S.; et al. Inclusion of Older Patients with Cancer in Clinical Trials: The SAGE Prospective Multicenter Cohort Survey. Oncologist 2019, 24, e1351–e1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervenka, B.P.; Rao, S.; Bewley, A.F. Head and Neck Cancer and the Elderly Patient. Otolaryngol. Clin. N. Am. 2018, 51, 741–751. [Google Scholar] [CrossRef]
- Le Saux, O.; Falandry, C.; Gan, H.K.; You, B.; Freyer, G.; Peron, J. Inclusion of elderly patients in oncology clinical trials. Ann. Oncol. 2016, 27, 1799–1804. [Google Scholar] [CrossRef] [PubMed]
- Puts, M.T.; Santos, B.; Hardt, J.; Monette, J.; Girre, V.; Atenafu, E.G.; Springall, E.; Alibhai, S.M. An update on a systematic review of the use of geriatric assessment for older adults in oncology. Ann. Oncol. 2014, 25, 307–315. [Google Scholar] [CrossRef]
- Noor, A.; Gibb, C.; Boase, S.; Hodge, J.C.; Krishnan, S.; Foreman, A. Frailty in geriatric head and neck cancer: A contemporary review. Laryngoscope 2018, 128, E416–E424. [Google Scholar] [CrossRef]
- Ferrat, E.; Paillaud, E.; Laurent, M.; Le Thuaut, A.; Caillet, P.; Tournigand, C.; Lagrange, J.L.; Canoui-Poitrine, F.; Bastuji-Garin, S.; Group, E.S. Predictors of 1-Year Mortality in a Prospective Cohort of Elderly Patients With Cancer. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 1148–1155. [Google Scholar] [CrossRef]
- Kwon, M.; Kim, S.A.; Roh, J.L.; Lee, S.W.; Kim, S.B.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. An Introduction to a Head and Neck Cancer-Specific Frailty Index and Its Clinical Implications in Elderly Patients: A Prospective Observational Study Focusing on Respiratory and Swallowing Functions. Oncologist 2016, 21, 1091–1098. [Google Scholar] [CrossRef] [Green Version]
- Boulahssass, R.; Gonfrier, S.; Ferrero, J.M.; Sanchez, M.; Mari, V.; Moranne, O.; Rambaud, C.; Auben, F.; Hannoun Levi, J.M.; Bereder, J.M.; et al. Predicting early death in older adults with cancer. Eur. J. Cancer 2018, 100, 65–74. [Google Scholar] [CrossRef]
- Bras, L.; Driessen, D.; de Vries, J.; Festen, S.; van der Laan, B.; van Leeuwen, B.L.; de Bock, G.H.; Halmos, G.B. Patients with head and neck cancer: Are they frailer than patients with other solid malignancies? Eur. J. Cancer Care 2020, 29, e13170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology consensus on geriatric assessment in older patients with cancer. J. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallis, A.G.; Wedding, U.; Lacombe, D.; Soubeyran, P.; Wildiers, H. Questionnaires and instruments for a multidimensional assessment of the older cancer patient: What clinicians need to know? Eur. J. Cancer 2010, 46, 1019–1025. [Google Scholar] [CrossRef]
- Rubenstein, L.Z.; Stuck, A.E.; Siu, A.L.; Wieland, D. Impacts of geriatric evaluation and management programs on defined outcomes: Overview of the evidence. J. Am. Geriatr. Soc. 1991, 39, 8S–16S, discussion 17S–18S. [Google Scholar] [CrossRef]
- Ellis, G.; Gardner, M.; Tsiachristas, A.; Langhorne, P.; Burke, O.; Harwood, R.H.; Conroy, S.P.; Kircher, T.; Somme, D.; Saltvedt, I.; et al. Comprehensive geriatric assessment for older adults admitted to hospital. Cochrane Database Syst. Rev. 2017, 9, Cd006211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lund, C.M.; Vistisen, K.K.; Olsen, A.P.; Bardal, P.; Schultz, M.; Dolin, T.G.; Rønholt, F.; Johansen, J.S.; Nielsen, D.L. The effect of geriatric intervention in frail older patients receiving chemotherapy for colorectal cancer: A randomised trial (GERICO). Br. J. Cancer 2021, 124, 1949–1958. [Google Scholar] [CrossRef] [PubMed]
- Mohile, S.G.; Mohamed, M.R.; Xu, H.; Culakova, E.; Loh, K.P.; Magnuson, A.; Flannery, M.A.; Obrecht, S.; Gilmore, N.; Ramsdale, E.; et al. Evaluation of geriatric assessment and management on the toxic effects of cancer treatment (GAP70+): A cluster-randomised study. Lancet 2021, 398, 1894–1904. [Google Scholar] [CrossRef]
- Li, D.; Sun, C.L.; Kim, H.; Soto-Perez-de-Celis, E.; Chung, V.; Koczywas, M.; Fakih, M.; Chao, J.; Cabrera Chien, L.; Charles, K.; et al. Geriatric Assessment-Driven Intervention (GAIN) on Chemotherapy-Related Toxic Effects in Older Adults With Cancer: A Randomized Clinical Trial. JAMA Oncol. 2021, 7, e214158. [Google Scholar] [CrossRef]
- Boysen, M.; Lövdal, O.; Tausjö, J.; Winther, F. The value of follow-up in patients treated for squamous cell carcinoma of the head and neck. Eur. J. Cancer 1992, 28, 426–430. [Google Scholar] [CrossRef]
- Blanchard, D.; Barry, B.; De Raucourt, D.; Choussy, O.; Dessard-Diana, B.; Hans, S.; Lafarge, D. Actualisation de la recommandation: Suivi post-thérapeutique des carcinomes épidermoïdes des voies aérodigestives supérieures de l’adulte: Recherche des métastases et des localisations métachrones œsophagiennes et bron. Ann. Fr. D’oto-Rhino-Laryngol. Pathol. Cervico-Faciale 2015, 132, 204–209. [Google Scholar] [CrossRef]
- Brugel, L.; Laurent, M.; Caillet, P.; Radenne, A.; Durand-Zaleski, I.; Martin, M.; Baron, M.; de Kermadec, H.; Bastuji-Garin, S.; Canoui-Poitrine, F.; et al. Impact of comprehensive geriatric assessment on survival, function, and nutritional status in elderly patients with head and neck cancer: Protocol for a multicentre randomised controlled trial (EGeSOR). BMC Cancer 2014, 14, 427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morice, V. RandoWeb, an online randomization tool for clinical trials. Comput. Methods Programs Biomed. 2012, 107, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Schulz, K.F.; Altman, D.G.; Moher, D. CONSORT 2010 Statement: Updated guidelines for reporting parallel group randomised trials. BMC Med. 2010, 8, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rao, A.V.; Hsieh, F.; Feussner, J.R.; Cohen, H.J. Geriatric evaluation and management units in the care of the frail elderly cancer patient. J. Gerontol. A Biol. Sci. Med. Sci. 2005, 60, 798–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ommundsen, N.; Wyller, T.B.; Nesbakken, A.; Bakka, A.O.; Jordhøy, M.S.; Skovlund, E.; Rostoft, S. Preoperative geriatric assessment and tailored interventions in frail older patients with colorectal cancer: A randomized controlled trial. Colorectal Dis. 2018, 20, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Magnuson, A.; Lemelman, T.; Pandya, C.; Goodman, M.; Noel, M.; Tejani, M.; Doughtery, D.; Dale, W.; Hurria, A.; Janelsins, M.; et al. Geriatric assessment with management intervention in older adults with cancer: A randomized pilot study. Support Care Cancer 2018, 26, 605–613. [Google Scholar] [CrossRef] [Green Version]
- Williams, G.R.; Weaver, K.E.; Lesser, G.J.; Dressler, E.; Winkfield, K.M.; Neuman, H.B.; Kazak, A.E.; Carlos, R.; Gansauer, L.J.; Kamen, C.S.; et al. Capacity to Provide Geriatric Specialty Care for Older Adults in Community Oncology Practices. Oncologist 2020, 25, 1032–1038. [Google Scholar] [CrossRef]
- McCorkle, R.; Strumpf, N.E.; Nuamah, I.F.; Adler, D.C.; Cooley, M.E.; Jepson, C.; Lusk, E.J.; Torosian, M. A specialized home care intervention improves survival among older post-surgical cancer patients. J. Am. Geriatr. Soc. 2000, 48, 1707–1713. [Google Scholar] [CrossRef]
- Li, D.; Sun, C.-L.; Kim, H.; Chung, V.; Koczywas, M.; Fakih, M.; Chao, J.; Chien, L.; Charles, K.; Hughes, S.F.D.S.; et al. Geriatric assessment-driven intervention (GAIN) on chemotherapy toxicity in older adults with cancer: A randomized controlled trial. J. Clin. Oncol. 2020, 38, 12010. [Google Scholar] [CrossRef]
- Soubeyran, P.; Terret, C.; Bellera, C.; Bonnetain, F.; Jean, O.S.; Galvin, A.; Chakiba, C.; Zwolakowski, M.D.; Mathoulin-Pélissier, S.; Rainfray, M. Role of geriatric intervention in the treatment of older patients with cancer: Rationale and design of a phase III multicenter trial. BMC Cancer 2016, 16, 932. [Google Scholar] [CrossRef] [Green Version]
- Puts, M.T.E.; Hsu, T.; Mariano, C.; Monette, J.; Brennenstuhl, S.; Pitters, E.; Ray, J.; Wan-Chow-Wah, D.; Kozlowski, N.; Krzyzanowska, M.; et al. Clinical and Cost-effectiveness of a Comprehensive geriatric assessment and management for Canadian elders with Cancer-the 5C study: A study protocol for a randomised controlled phase III trial. BMJ Open 2019, 9, e024485. [Google Scholar] [CrossRef] [PubMed]
- Deschodt, M.; Flamaing, J.; Haentjens, P.; Boonen, S.; Milisen, K. Impact of geriatric consultation teams on clinical outcome in acute hospitals: A systematic review and meta-analysis. BMC Med. 2013, 11, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hempenius, L.; Slaets, J.P.; van Asselt, D.; de Bock, G.H.; Wiggers, T.; van Leeuwen, B.L. Outcomes of a Geriatric Liaison Intervention to Prevent the Development of Postoperative Delirium in Frail Elderly Cancer Patients: Report on a Multicentre, Randomized, Controlled Trial. PLoS ONE 2013, 8, e64834. [Google Scholar] [CrossRef] [Green Version]
- Kenis, C.; Bron, D.; Libert, Y.; Decoster, L.; Van Puyvelde, K.; Scalliet, P.; Cornette, P.; Pepersack, T.; Luce, S.; Langenaeken, C.; et al. Relevance of a systematic geriatric screening and assessment in older patients with cancer: Results of a prospective multicentric study. Ann. Oncol. 2013, 24, 1306–1312. [Google Scholar] [CrossRef] [PubMed]
- Van Grootven, B.; McNicoll, L.; Mendelson, D.A.; Friedman, S.M.; Fagard, K.; Milisen, K.; Flamaing, J.; Deschodt, M. Quality indicators for in-hospital geriatric co-management programmes: A systematic literature review and international Delphi study. BMJ Open 2018, 8, e020617. [Google Scholar] [CrossRef] [PubMed]
- Shahrokni, A.; Tin, A.L.; Sarraf, S.; Alexander, K.; Sun, S.; Kim, S.J.; McMillan, S.; Yulico, H.; Amirnia, F.; Downey, R.J.; et al. Association of Geriatric Comanagement and 90-Day Postoperative Mortality Among Patients Aged 75 Years and Older With Cancer. JAMA Netw. Open 2020, 3, e209265. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Experimental Arm n = 238 | Control Arm n = 237 | ||
|---|---|---|---|
| Characteristics, n(%) otherwise indicated | |||
| Age in years, median [Q1–Q3] | 75.2 [70.3–82.2] | 75.6 [70.6–81.7] | |
| Age groups | [65–70] | 57 (23.9) | 51 (21.5) |
| [70–75] | 59 (24.8) | 64 (27.0) | |
| [75–80] | 44 (18.5) | 48 (20.2) | |
| [80–85] | 42 (17.6) | 40 (16.9) | |
| [85–90] | 21 (8.8) | 24 (10.1) | |
| ≥90 | 15 (6.3) | 10 (4.2) | |
| Female gender | 78 (32.8) | 67 (28.3) | |
| Living alone at home (n = 227/232) | 80 (35.2) | 79 (34.1) | |
| Clinical characteristics | |||
| Weight loss † (n = 57/63) | 28 (49.1) | 27 (42.9) | |
| BMI groups | Malnutrition | 39 (16.4) | 33 (13.9) |
| Normal weight | 90 (37.8) | 105 (44.3) | |
| Overweight | 75 (31.5) | 71 (30.0) | |
| Obese | 34 (14.3) | 28 (11.8) | |
| ADL score ≤5.5 (n = 233/236) | 28 (12.0) | 24 (10.2) | |
| Performance status (n = 233/236) | 0 | 140 (60.1) | 149 (63.1) |
| 1 | 71 (30.5) | 69 (29.3) | |
| 2 | 13 (5.6) | 9 (3.8) | |
| 3, 4 | 9 (3.8) | 9 (3.8) | |
| G8 score * ≤14 (n = 183/186) | 109 (59.6) | 120 (64.5) | |
| Comorbidities | Hypertension (n = 230/236) | 134 (58.3) | 146 (61.9) |
| COPD (n = 116/128) | 35 (30.2) | 41 (32.0) | |
| Cardiac arrhythmia (atrial fibrillation) (n = 116/128) | 29 (25.0) | 33 (25.8) | |
| Diabetes (n = 229/236) | 47 (20.5) | 40 (17.0) | |
| PAOD (n = 116/128) | 22 (19.0) | 24 (18.8) | |
| Heart failure (n = 229/236) | 28 (12.2) | 13 (5.5) | |
| Stroke (n = 116/128) | 11 (9.5) | 16 (12.5) | |
| Renal failure (n = 228/236) | 14 (6.1) | 17 (7.2) | |
| Dementia (n = 116/128) | 5 (4.3) | 4 (3.1) | |
| Liver failure (n = 116/128) | 5 (4.3) | 6 (4.7) | |
| Smoking status (n = 229/233) | Active | 50 (21.8) | 48 (20.6) |
| Ex-smoker | 120 (52.4) | 116 (49.8) | |
| Non-smoker | 59 (25.8) | 69 (29.6) | |
| Pack-Years (PY), median [Q1–Q3] (n = 136/132) | 40 [30–55] | 40 [25–57.5] | |
| Alcohol consumption (n = 222/224) | 85 (38.3) | 84 (37.5) | |
| Beer consumption (n = 85/84) | 5 (5.9) | 15 (17.9) | |
| Wine consumption (n = 85/84) | 51 (60.0) | 40 (47.6) | |
| Strong alcohol consumption (n = 85/84) | 9 (10.6) | 14 (16.7) | |
| Baseline symptoms | Dysphagia (n = 227/234) | 44 (19.4) | 53 (22.7) |
| Dysphonia (n = 227/233) | 57 (25.1) | 63 (27.0) | |
| Swallowing disorders (n = 226/232) | 9 (4.0) | 10 (4.3) | |
| Trismus (n = 226/233) | 2 (0.9) | 7 (3.0) | |
| Oncologic characteristics | |||
| Cancer site (n = 232/230) | Oral | 101 (43.5) | 102 (44.4) |
| Oropharyngeal | 53 (22.9) | 50 (21.7) | |
| Laryngeal | 58 (25.0) | 57 (24.8) | |
| Hypopharyngeal | 20 (8.6) | 21 (9.1) | |
| T stage | Tis/T1 | 59 (24.8) | 52 (21.9) |
| T2 | 67 (28.1) | 76 (32.1) | |
| T3 | 53 (22.3) | 47 (19.8) | |
| T4a/T4b/Tx | 59 (24.8) | 62 (26.2) | |
| N stage | N0 | 134 (56.3) | 128 (54.0) |
| N1 | 37 (15.6) | 42 (17.7) | |
| N2a | 16 (6.7) | 17 (7.2) | |
| N2b | 29 (12.2) | 23 (9.7) | |
| N2c | 12 (5.0) | 20 (8.4) | |
| N3 | 10 (4.2) | 7 (3.0) | |
| Metastases (n = 226/233) | M0 | 180 (79.7) | 184 (79.0) |
| M1/Mx | 46 (20.3) | 49 (21.0) | |
| Place of GA (n = 196) | |
|---|---|
| Geriatric day hospital | 5 (2.5) |
| Consultation | 135 (68.9) |
| Hospitalization | 56 (28.6) |
| Functional status | |
| IADL score <8 (n = 193) | 78 (40.4) |
| Mobility | |
| Outside walking with help (walking stick, medical walker, human help) (n = 196) | 32 (16.3) |
| Falls during the last 6 months (n = 197) | 23 (11.7) |
| Timed get-up-and-go test >20 s (n = 170) | 21 (12.4) |
| One-leg standing test <5 s (n = 141) | 59 (41.8) |
| General condition | |
| Asthenia (n = 195) * | 103 (52.8) |
| Comorbidity | |
| Total CIRS-G score, median [Q1–Q3] (n = 175) | 6 [3-9] |
| Nutrional status | |
| MNA score (n = 181) | |
| <17 | 20 (11.0) |
| [17–24] | 60 (33.2) |
| ≥24 | 101 (55.8) |
| Cognition and depression | |
| MMSE score <24 (n = 170) | 31 (18.2) |
| Felt depressed (n = 196) | 47 (24.0) |
| GA-driven interventions (n = 174) | |
| Unnecessary | 65 (37.4) |
| Suggested/Prescribed by geriatrician | 109 (62.6) |
| Social support (human or financial) (n = 174) | |
| Unnecessary | 128 (73.6) |
| Suggested/Prescribed by geriatrician | 46 (26.4) |
| Nursing care (n = 169) | |
| Unnecessary | 148 (87.6) |
| Suggested/Prescribed by geriatrician | 21 (12.4) |
| Physical therapy (n = 171) | |
| Unnecessary | 133 (77.8) |
| Suggested/Prescribed by geriatrician | 38 (22.2) |
| Nutritional support (dietitian visits or nutritional supplements) (n = 171) | |
| Unnecessary | 87 (50.9) |
| Suggested/Prescribed by geriatrician | 84 (49.1) |
| Medication review (n = 171) | |
| Unnecessary | 146 (85.4) |
| Suggested/Prescribed by geriatrician | 25 (14.6) |
| Memory consultation (n = 171) | |
| Unnecessary | 159 (93.0) |
| Suggested/Prescribed by geriatrician | 12 (7.0) |
| Psychological support (psychologist or psychiatrist) (n = 174) | |
| Unnecessary | 149 (85.6) |
| Suggested/Prescribed by geriatrician | 25 (14.4) |
| Experimental Arm n = 238 | Control Arm n = 237 | p | |
|---|---|---|---|
| Intent-to-treat analysis | |||
| Primary endpoint (death, weight loss a and decrease in ADL score b) with multiple imputation | 98 (41.0) | 90 (38.0) | 0.53 * |
| Death ‡ | 31 (13.0) | 27 (11.4) | 0.48 ** |
| Weight loss a | 69 (29.0) | 65 (27.4) | 0.73 * |
| Decrease in ADL score b | 9 (3.8) | 13 (5.5) | 0.35 * |
| Primary endpoint (death, weight loss a and decrease in ADL score b) on complete data case (n = 194/196) | 82 (42.3) | 76 (38.8) | 0.48 *** |
| Death | 31 (13.0) | 27 (11.4) | 0.48 ** |
| Weight loss a (n = 166/172) | 48 (28.9) | 44 (25.6) | 0.49 *** |
| Decrease in ADL score b (n = 179/183) | 6 (3.4) | 10 (5.5) | 0.33 *** |
| Per-protocol analysis | |||
| Primary endpoint (death, weight loss a and decrease in ADL score b) with multiple imputations (n = 62/226) | 19 (30.6) | 86 (38.1) | 0.35 * |
| Death ‡ | 4 (6.5) | 26 (11.5) | 0.27 ** |
| Weight loss a | 16 (25.8) | 62 (27.4) | 0.79 * |
| Decrease in ADL score b | 2 (3.2) | 13 (5.8) | 0.55 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Paillaud, E.; Brugel, L.; Bertolus, C.; Baron, M.; Bequignon, E.; Caillet, P.; Schouman, T.; Lacau Saint Guily, J.; Périé, S.; Bouvard, E.; et al. Effectiveness of Geriatric Assessment-Driven Interventions on Survival and Functional and Nutritional Status in Older Patients with Head and Neck Cancer: A Randomized Controlled Trial (EGeSOR). Cancers 2022, 14, 3290. https://doi.org/10.3390/cancers14133290
Paillaud E, Brugel L, Bertolus C, Baron M, Bequignon E, Caillet P, Schouman T, Lacau Saint Guily J, Périé S, Bouvard E, et al. Effectiveness of Geriatric Assessment-Driven Interventions on Survival and Functional and Nutritional Status in Older Patients with Head and Neck Cancer: A Randomized Controlled Trial (EGeSOR). Cancers. 2022; 14(13):3290. https://doi.org/10.3390/cancers14133290
Chicago/Turabian StylePaillaud, Elena, Lydia Brugel, Chloe Bertolus, Melany Baron, Emilie Bequignon, Philippe Caillet, Thomas Schouman, Jean Lacau Saint Guily, Sophie Périé, Eric Bouvard, and et al. 2022. "Effectiveness of Geriatric Assessment-Driven Interventions on Survival and Functional and Nutritional Status in Older Patients with Head and Neck Cancer: A Randomized Controlled Trial (EGeSOR)" Cancers 14, no. 13: 3290. https://doi.org/10.3390/cancers14133290
APA StylePaillaud, E., Brugel, L., Bertolus, C., Baron, M., Bequignon, E., Caillet, P., Schouman, T., Lacau Saint Guily, J., Périé, S., Bouvard, E., Laurent, M., Salvan, D., Chaumette, L., de Decker, L., Piot, B., Barry, B., Raynaud-Simon, A., Sauvaget, E., Bach, C., ... Canouï-Poitrine, F. (2022). Effectiveness of Geriatric Assessment-Driven Interventions on Survival and Functional and Nutritional Status in Older Patients with Head and Neck Cancer: A Randomized Controlled Trial (EGeSOR). Cancers, 14(13), 3290. https://doi.org/10.3390/cancers14133290