
Neuroendocrine Neoplasms of the Female Genitourinary Tract: A Comprehensive Overview

 , , , ,
, , , ,
Abstract
Simple Summary
Abstract
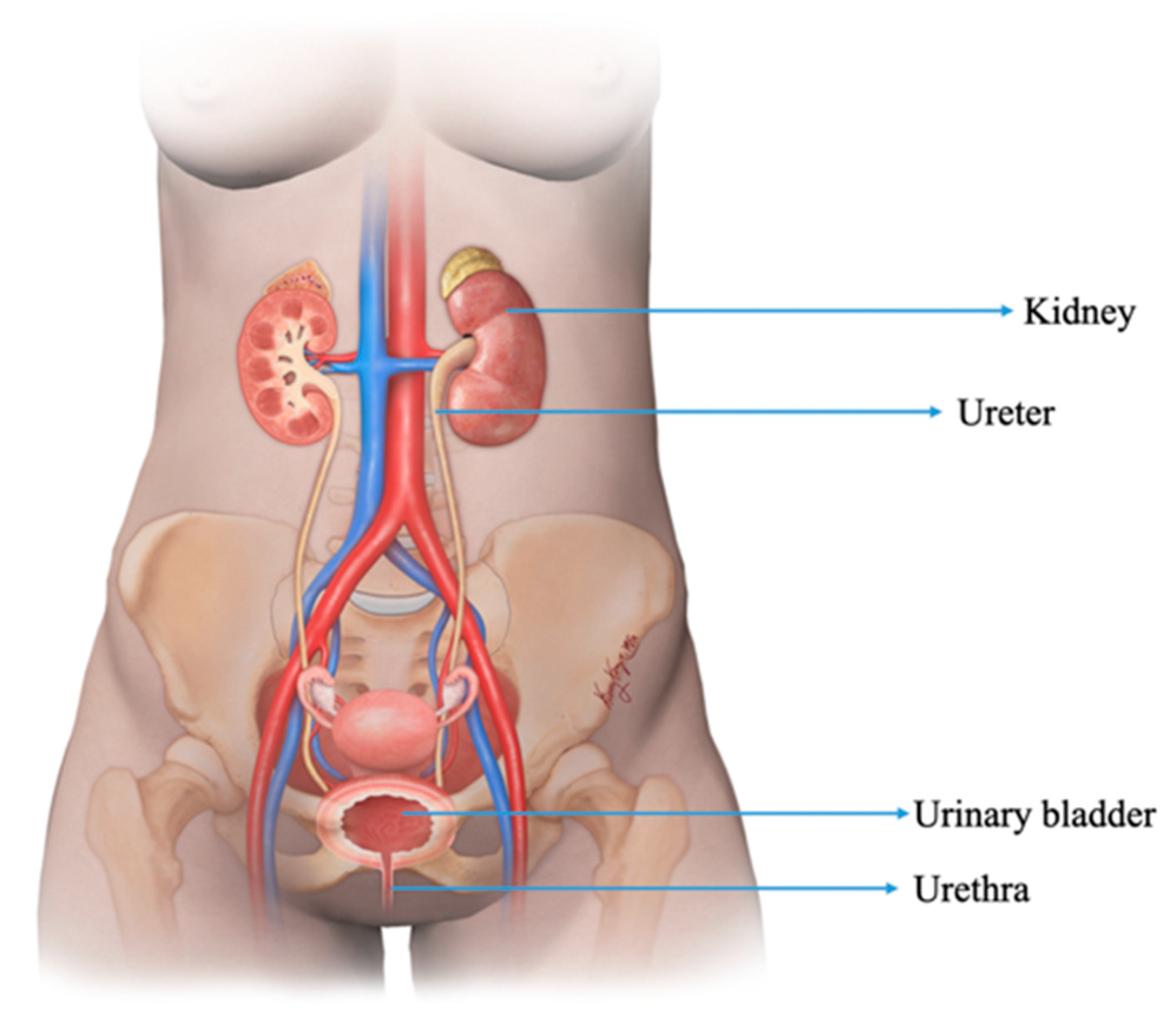
1. Introduction
2. Renal NENs
2.1. Epidemiology, Presentation, and Pathogenesis
2.2. Pathogenesis
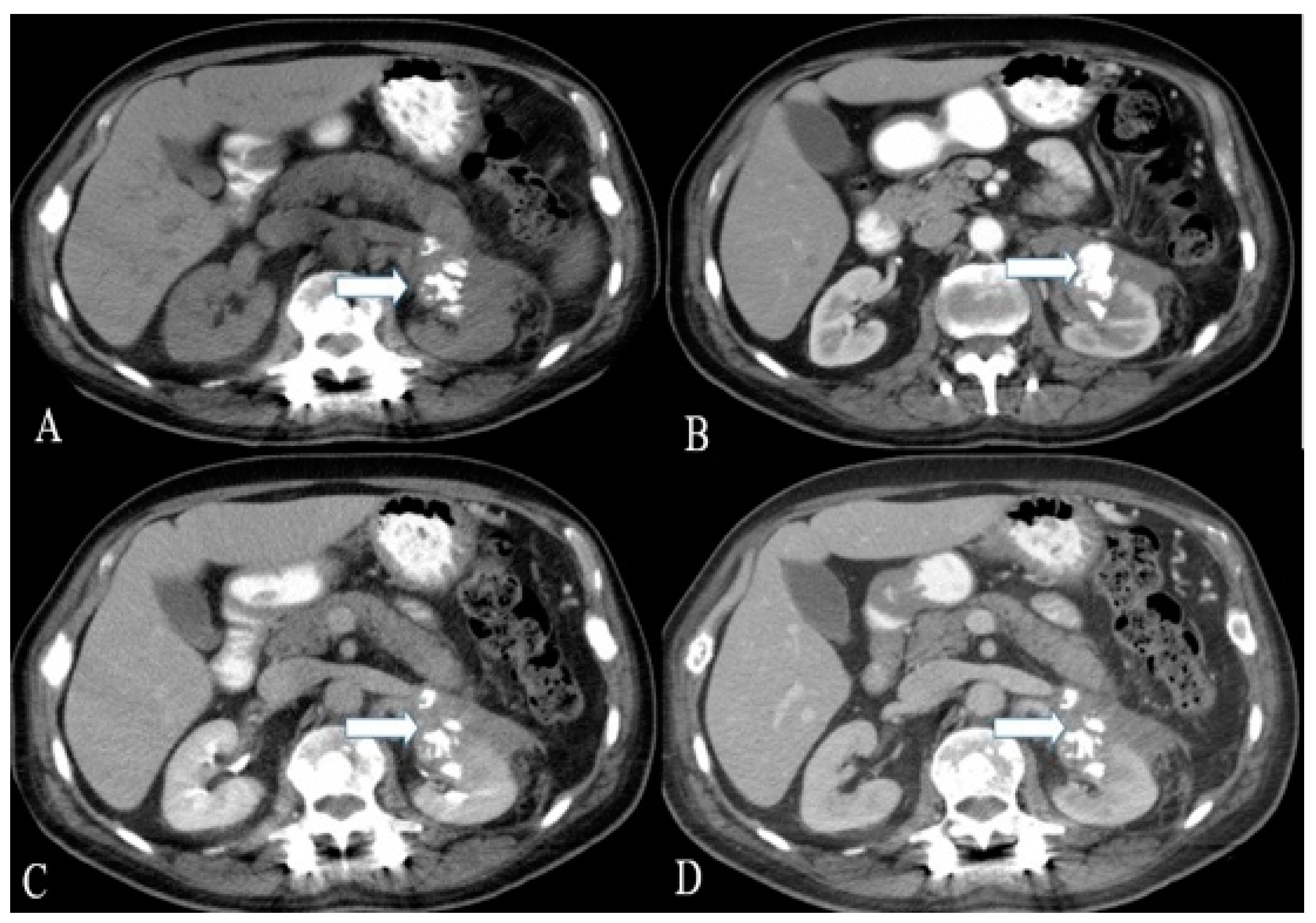
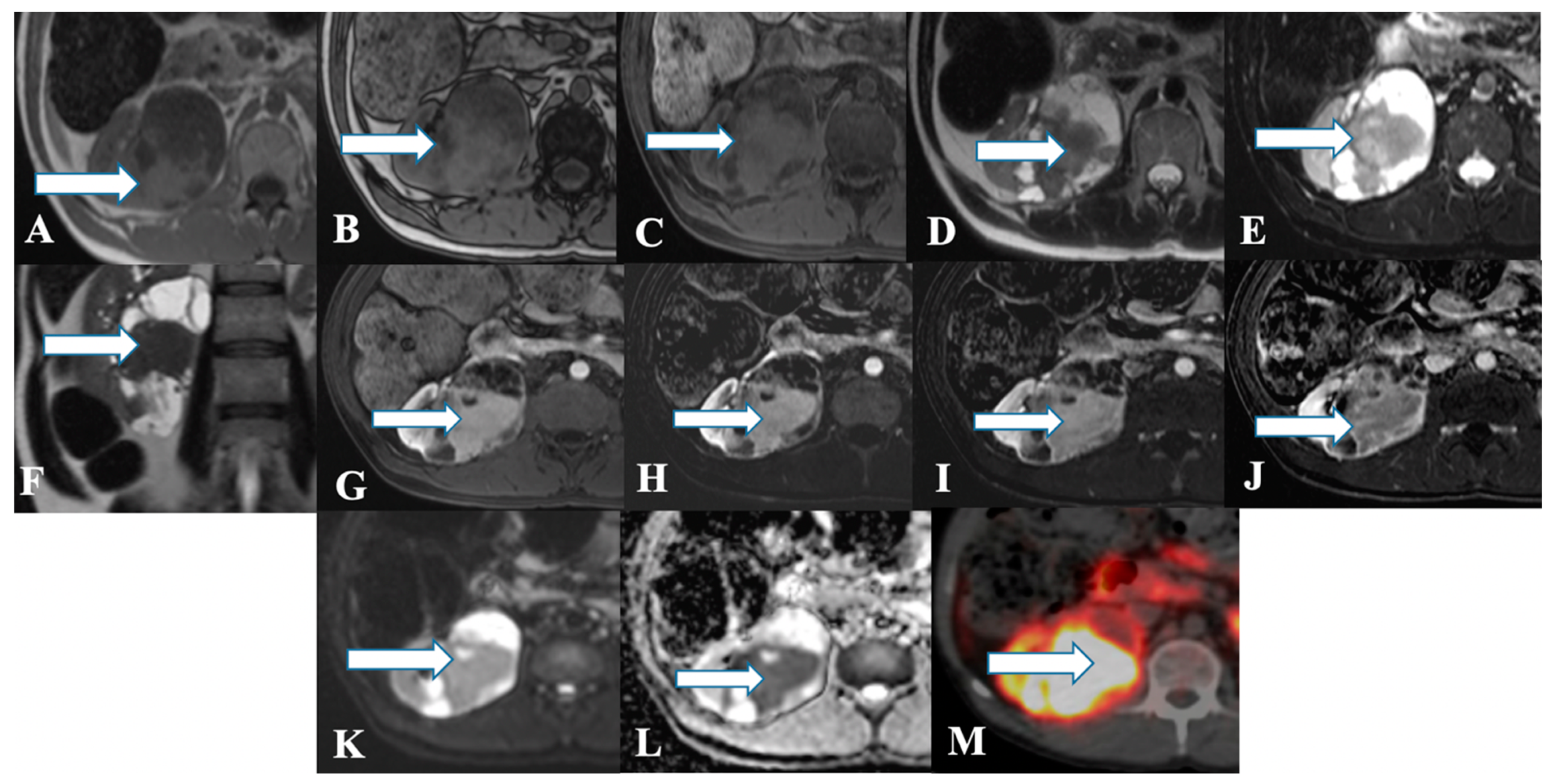
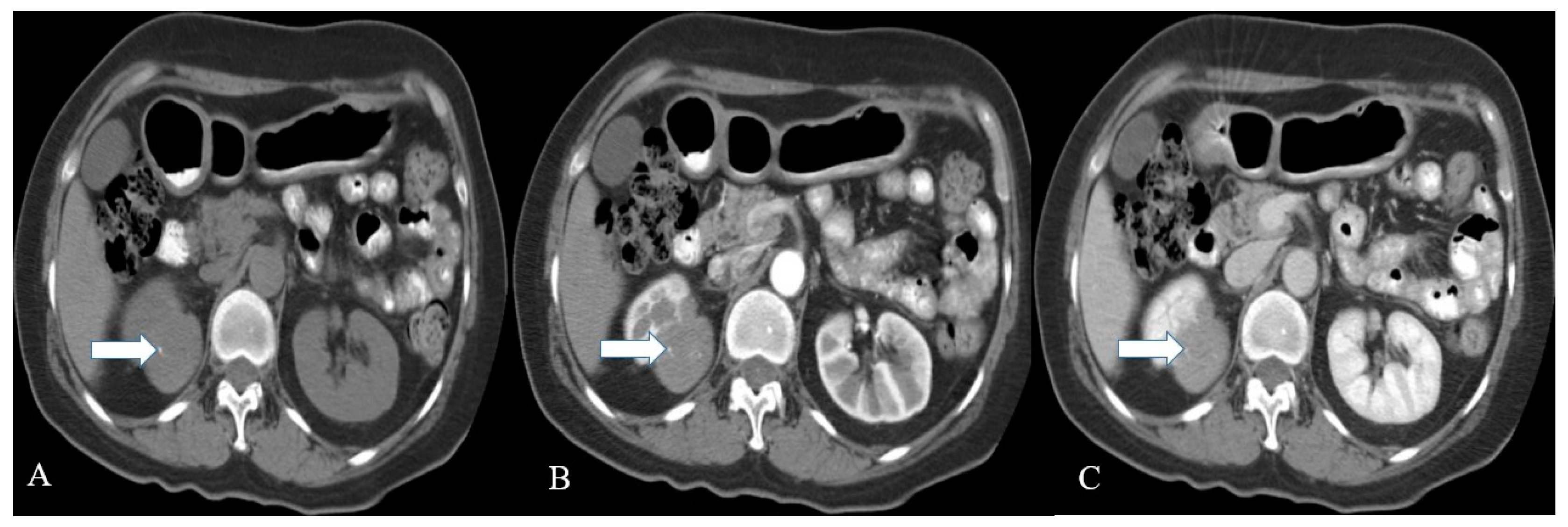
2.3. Imaging
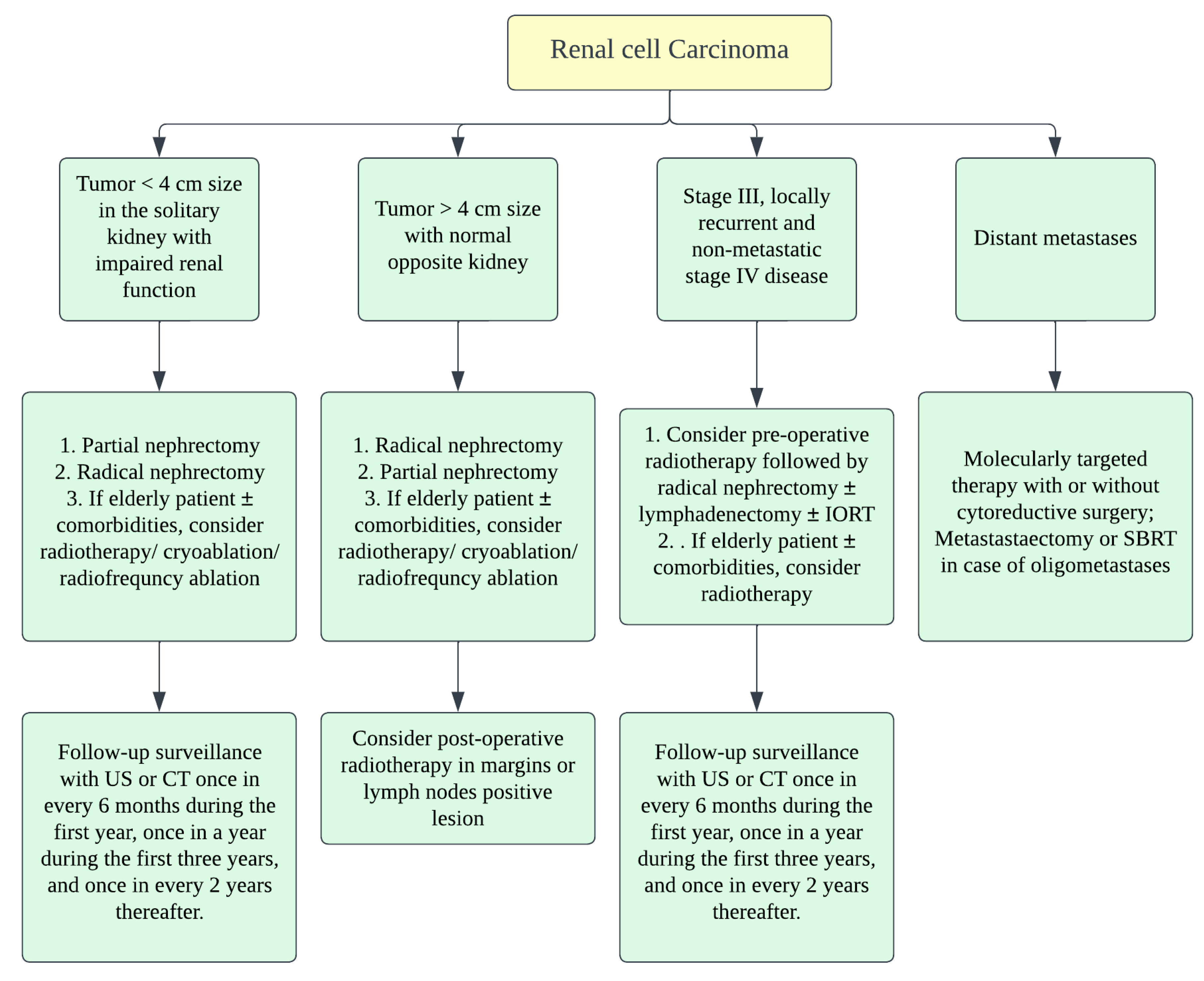
2.4. Prognosis and Management
3. Urinary Bladder NENs
3.1. Epidemiology, Presentation, and Pathogenesis
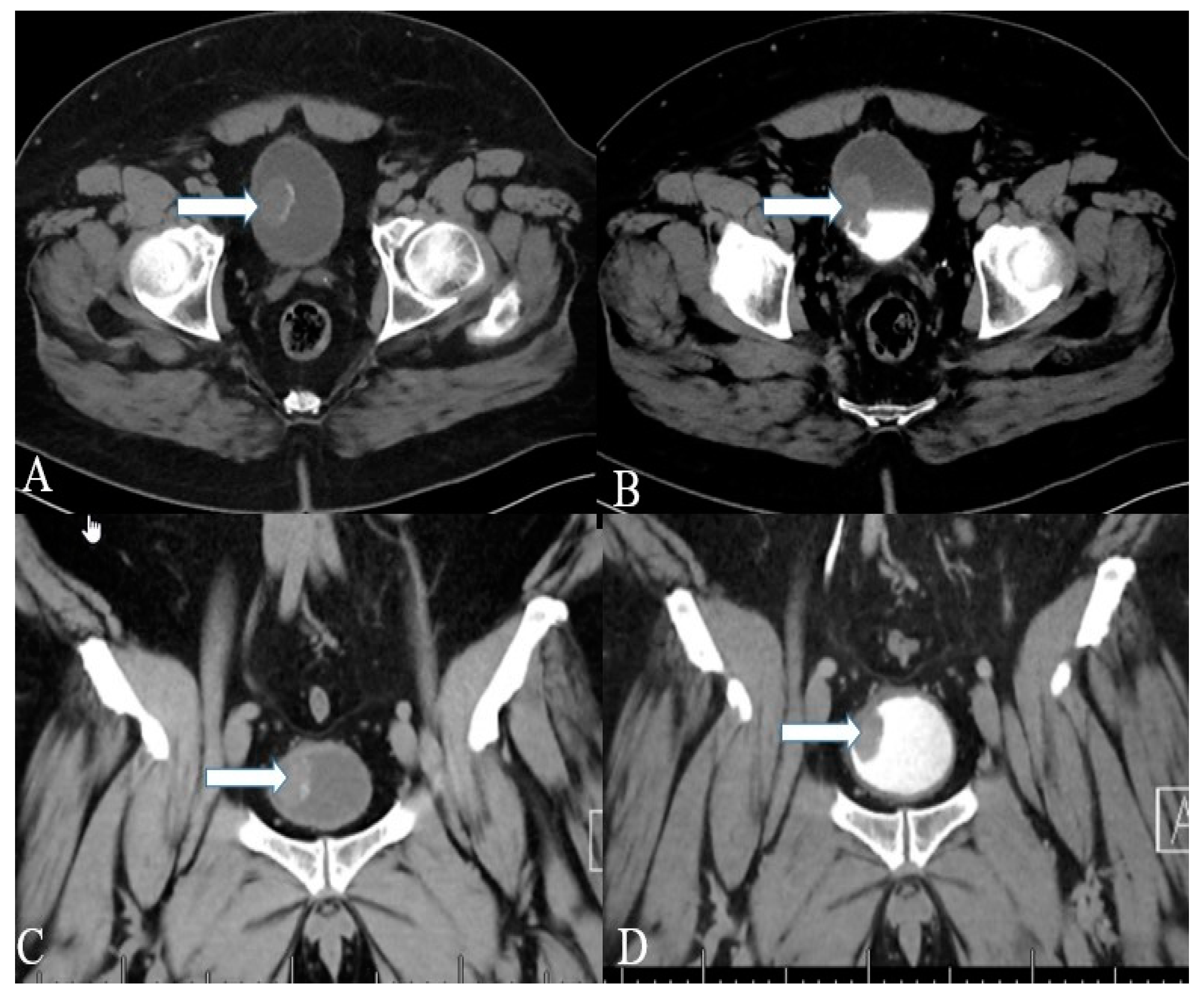
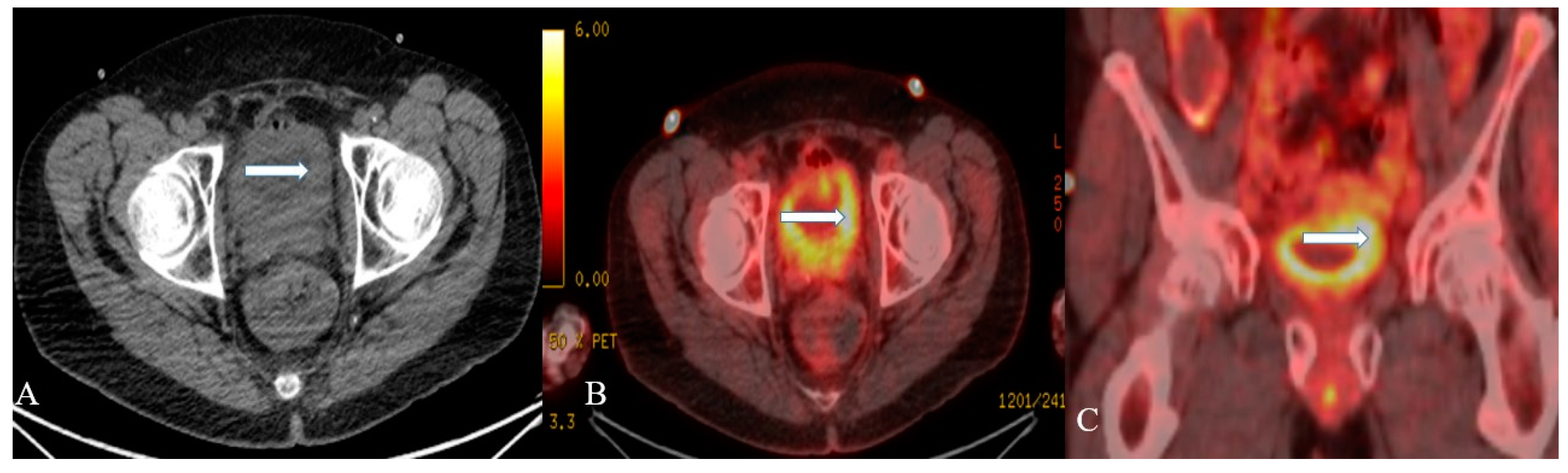
3.2. Imaging
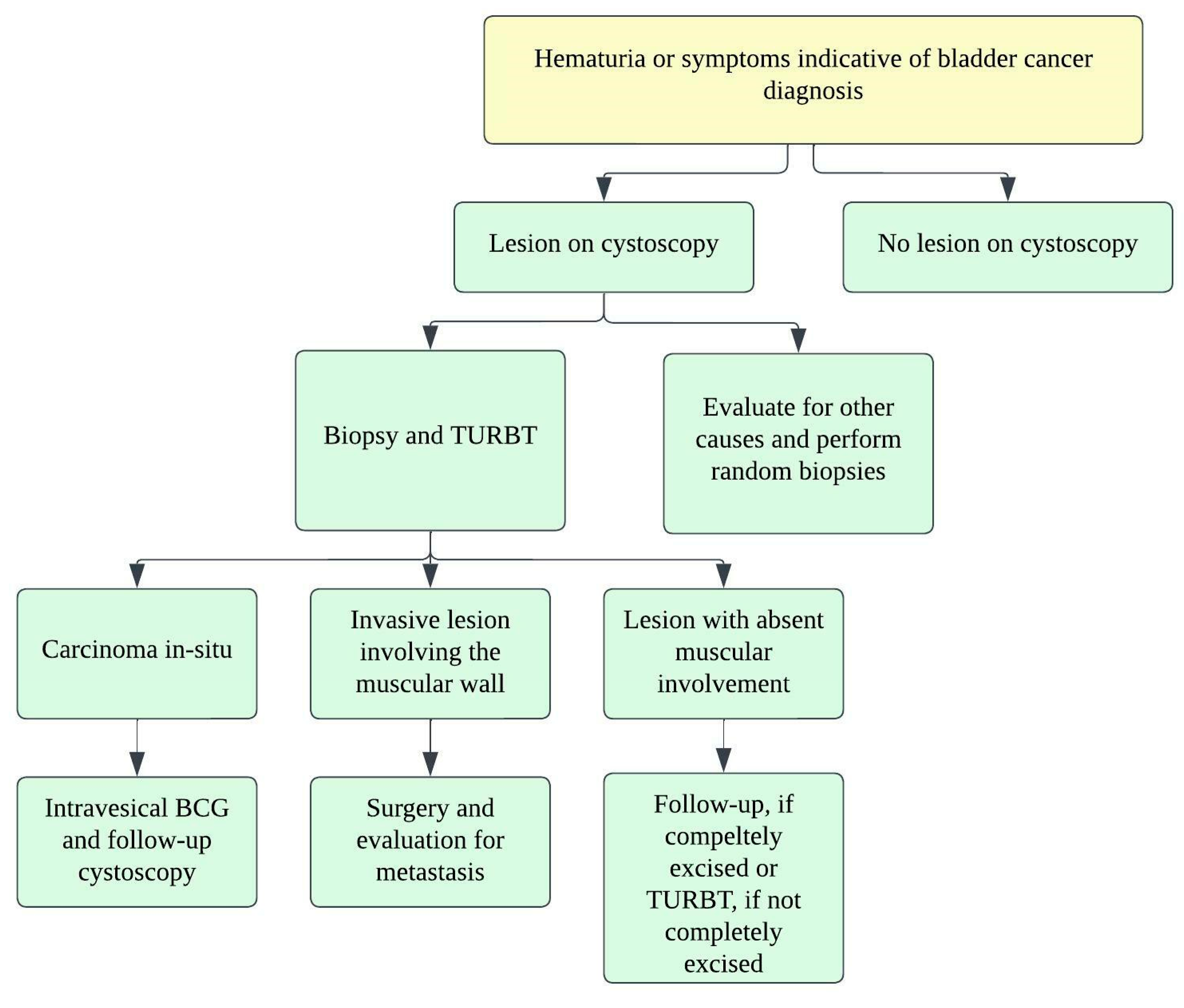
3.3. Prognosis and Management
4. Ureteral NENs
4.1. Epidemiology, Presentation, and Pathogenesis
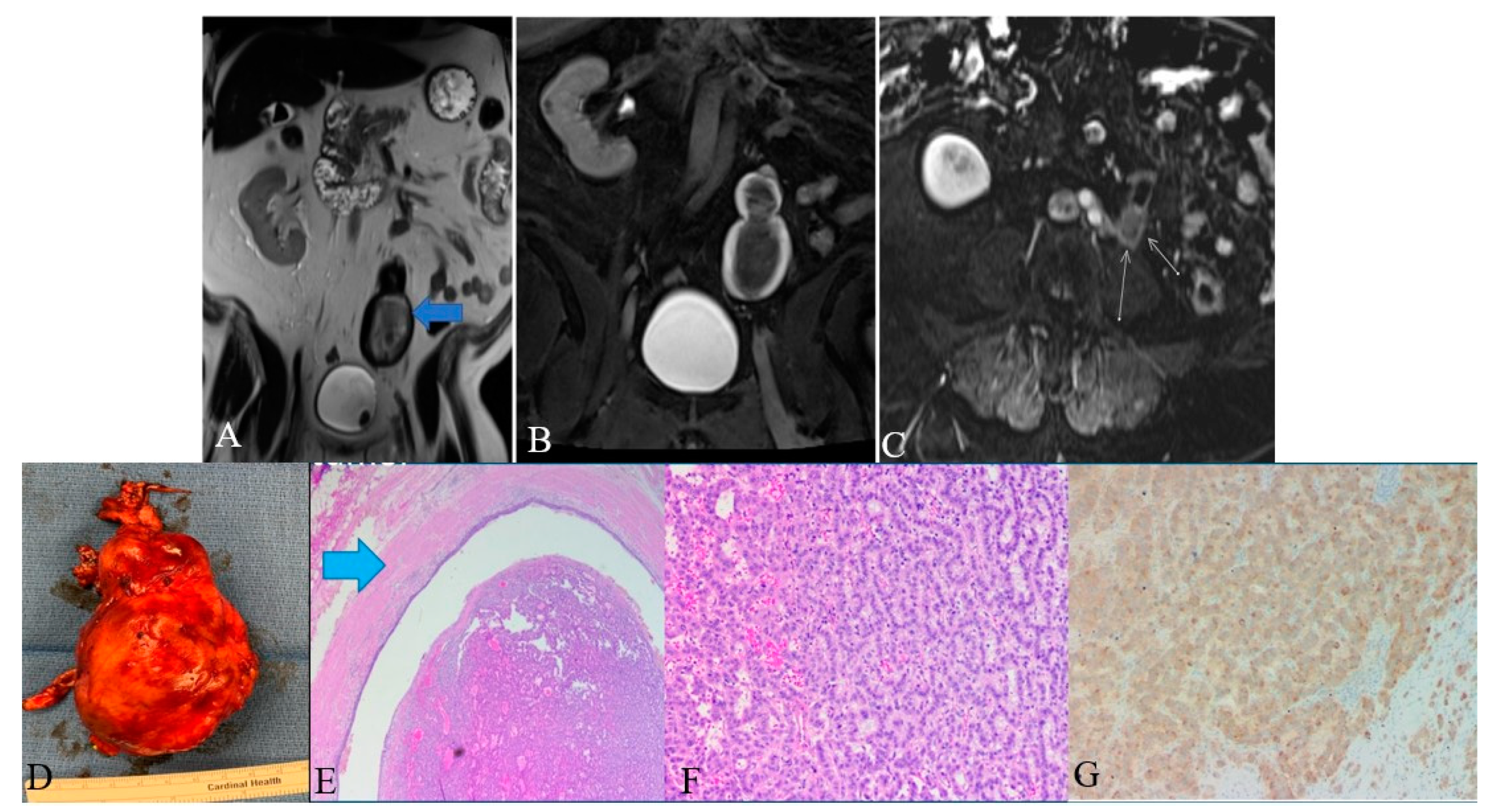
4.2. Imaging
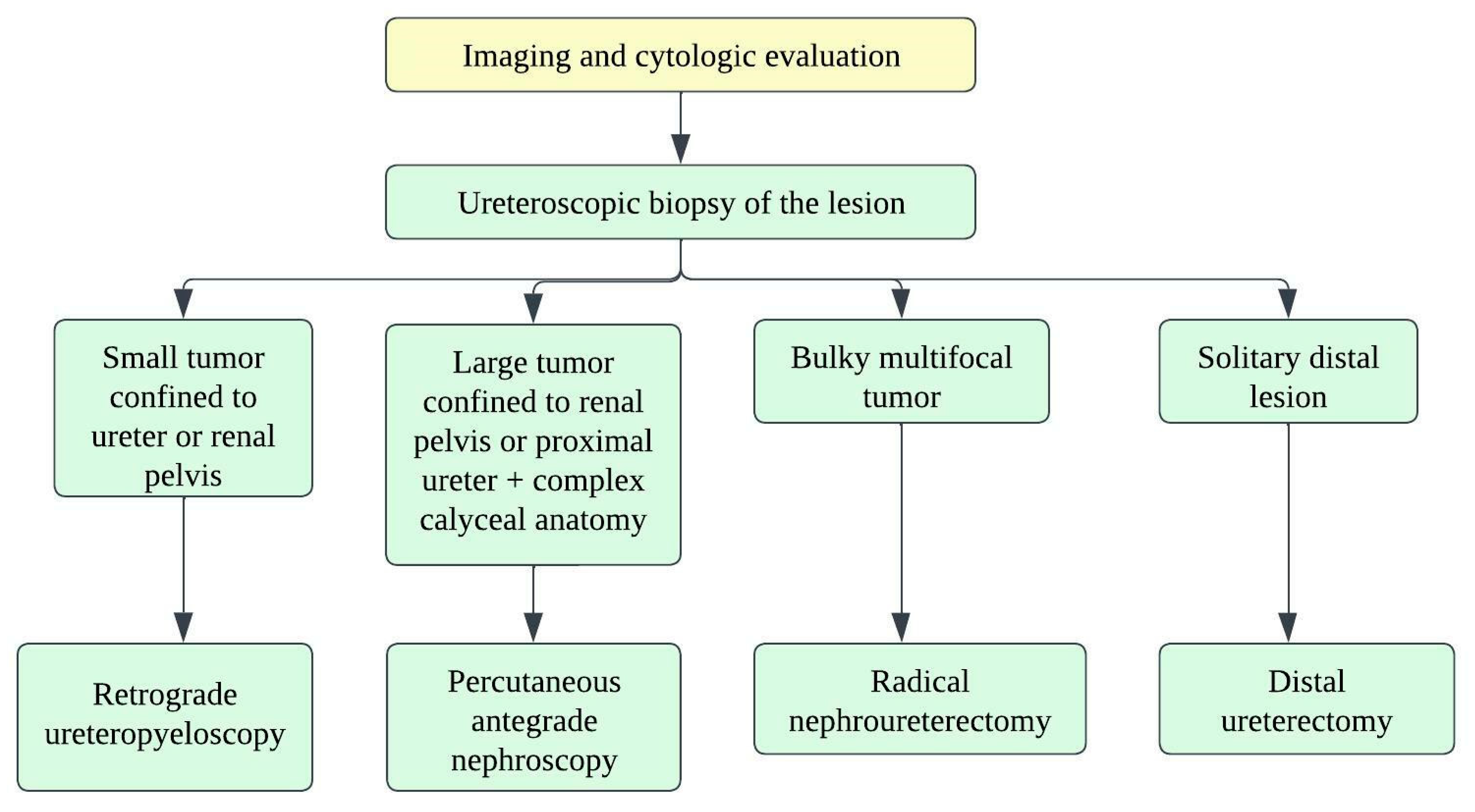
4.3. Prognosis and Management
5. Urethral NENs
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Wang, H.; Ma, C.; Wu, J.; Zhao, F.; Zou, Y.; Zhang, W.; Jiang, Y. Clinicopathologic features of the ureteral neuroendocrine tumors. Pathol. Res. Pract. 2020, 216, 152788. [Google Scholar] [CrossRef] [PubMed]
- Farci, F.; Manassero, F.; Baldesi, R.; Bartolucci, A.; Boldrini, L.; Selli, C.; Faviana, P. Primary small cell carcinoma of the ureter: Case report and review of the literature. Medicine 2018, 97, e11113. [Google Scholar] [CrossRef]
- Yi, Z.; Liu, R.; Hu, J.; He, T.; Wang, Z.; Li, Y.; Zu, X. Clinicopathologic Features and Survival Outcomes for Primary Renal Neuroendocrine Neoplasms. Clin. Genitourin. Cancer 2021, 19, 155–161. [Google Scholar] [CrossRef]
- Moch, H.; Cubilla, A.L.; Humphrey, P.A.; Reuter, V.E.; Ulbright, T.M. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur. Urol. 2016, 70, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Resnick, M.E.; Unterberger, H.; McLoughlin, P.T. Renal carcinoid producing the carcinoid syndrome. Med. Times 1966, 94, 895–896. [Google Scholar] [PubMed]
- Murali, R.; Kneale, K.; Lalak, N.; Delprado, W. Carcinoid tumors of the urinary tract and prostate. Arch. Pathol. Lab. Med. 2006, 130, 1693–1706. [Google Scholar] [CrossRef]
- Hansel, D.E.; Epstein, J.I.; Berbescu, E.; Fine, S.W.; Young, R.H.; Cheville, J.C. Renal carcinoid tumor: A clinicopathologic study of 21 cases. Am. J. Surg. Pathol. 2007, 31, 1539–1544. [Google Scholar] [CrossRef]
- Armah, H.B.; Parwani, A.V.; Perepletchikov, A.M. Synchronous primary carcinoid tumor and primary adenocarcinoma arising within mature cystic teratoma of horseshoe kidney: A unique case report and review of the literature. Diagn. Pathol. 2009, 4, 17. [Google Scholar] [CrossRef]
- Romero, F.R.; Rais-Bahrami, S.; Permpongkosol, S.; Fine, S.W.; Kohanim, S.; Jarrett, T.W. Primary carcinoid tumors of the kidney. J. Urol. 2006, 176, 2359–2366. [Google Scholar] [CrossRef]
- Raslan, W.F.; Ro, J.Y.; Ordonez, N.G.; Amin, M.B.; Troncoso, P.; Sella, A.; Ayala, A.G. Primary carcinoid of the kidney. Immunohistochemical and ultrastructural studies of five patients. Cancer 1993, 72, 2660–2666. [Google Scholar] [CrossRef]
- Moulopoulos, A.; DuBrow, R.; David, C.; Dimopoulos, M.A. Primary renal carcinoid: Computed tomography, ultrasound, and angiographic findings. J. Comput. Assist. Tomogr. 1991, 15, 323–325. [Google Scholar] [CrossRef] [PubMed]
- Katabathina, V.S.; Vikram, R.; Olaoya, A.; Paspulati, R.M.; Nicolas, M.M.; Rao, P.; Zaheer, A.; Prasad, S.R. Neuroendocrine neoplasms of the genitourinary tract in adults: Cross-sectional imaging spectrum. Abdom. Radiol. 2017, 42, 1472–1484. [Google Scholar] [CrossRef] [PubMed]
- Posfai, B.; Kuthi, L.; Varga, L.; Laczo, I.; Revesz, J.; Kranicz, R.; Maraz, A. The Colorful Palette of Neuroendocrine Neoplasms in the Genitourinary Tract. Anticancer Res. 2018, 38, 3243–3254. [Google Scholar] [CrossRef] [PubMed]
- Lane, B.R.; Chery, F.; Jour, G.; Sercia, L.; Magi-Galluzzi, C.; Novick, A.C.; Zhou, M. Renal neuroendocrine tumours: A clinicopathological study. BJU Int. 2007, 100, 1030–1035. [Google Scholar] [CrossRef]
- González-Lois, C.; Madero, S.; Redondo, P.; Alonso, I.; Salas, A.; Montalbán, M.A. Small cell carcinoma of the kidney: A case report and review of the literature. Arch. Pathol. Lab. Med. 2001, 125, 796–798. [Google Scholar] [CrossRef]
- Akkaya, B.K.; Mustafa, U.; Esin, O.; Turker, K.; Gulten, K. Primary small cell carcinoma of the kidney. Urol. Oncol. Semin. Orig. Investig. 2003, 21, 11–13. [Google Scholar] [CrossRef]
- Si, Q.; Dancer, J.; Stanton, M.L.; Tamboli, P.; Ro, J.Y.; Czerniak, B.A.; Shen, S.S.; Guo, C.C. Small cell carcinoma of the kidney: A clinicopathologic study of 14 cases. Hum. Pathol. 2011, 42, 1792–1798. [Google Scholar] [CrossRef]
- Nguyen, A.H.; O’Leary, M.P.; De Andrade, J.P.; Ituarte, P.H.G.; Kessler, J.; Li, D.; Singh, G.; Chang, S. Natural History of Renal Neuroendocrine Neoplasms: A NET by Any Other Name? Front. Endocrinol. 2020, 11, 624251. [Google Scholar] [CrossRef]
- Ratnagiri, R.; Singh, S.S.; Majhi, U. Large-cell neuroendocrine carcinoma of the kidney: Clinicopathologic features. Indian J. Urol. IJU J. Urol. Soc. India 2009, 25, 274. [Google Scholar] [CrossRef]
- Dundr, P.; Pešl, M.; Povýšil, C.; Bauerová, L.; Soukup, V. Primary large cell neuroendocrine carcinoma of the kidney. Pathol. Oncol. Res. 2010, 16, 139–142. [Google Scholar] [CrossRef]
- Palumbo, C.; Talso, M.; Dell’Orto, P.G.; Cozzi, G.; De Lorenzis, E.; Conti, A.; Maggioni, M.; Cesare Rocco, B.M.; Maggioni, A.; Rocco, F. Primary large cell neuroendocrine carcinoma of the renal pelvis: A case report. Urol. J. 2014, 81, 57–59. [Google Scholar] [CrossRef] [PubMed]
- Wann, C.; John, N.T.; Kumar, R.M. Primary renal large cell neuroendocrine carcinoma in a young man. J. Clin. Diagn. Res. JCDR 2014, 8, ND08. [Google Scholar] [CrossRef] [PubMed]
- Shimbori, M.; Osaka, K.; Kawahara, T.; Kasahara, R.; Kawabata, S.; Makiyama, K.; Kondo, K.; Nakaigawa, N.; Yamanaka, S.; Yao, M. Large cell neuroendocrine carcinoma of the kidney with cardiac metastasis: A case report. J. Med. Case Rep. 2017, 11, 297. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Sanguedolce, F.; Calo, B.; Chirico, M.; Tortorella, S.; Carrieri, G.; Cormio, L. Urinary Tract Large Cell Neuroendocrine Carcinoma: Diagnostic, Prognostic and Therapeutic Issues. Anticancer Res. 2020, 40, 2439–2447. [Google Scholar] [CrossRef]
- Yi, C.; Han, L.; Yang, R.; Yu, J. Paraganglioma of the renal pelvis: A case report and review of literature. Tumori 2017, 103, e47–e49. [Google Scholar] [CrossRef]
- Lamb, L.; Shaban, W. Primary renal carcinoid tumor: A radiologic review. Radiol. Case Rep. 2014, 9, 923. [Google Scholar] [CrossRef]
- Mazzucchelli, R.; Morichetti, D.; Lopez-Beltran, A.; Cheng, L.; Scarpelli, M.; Kirkali, Z.; Montironi, R. Neuroendocrine tumours of the urinary system and male genital organs: Clinical significance. BJU Int. 2009, 103, 1464–1470. [Google Scholar] [CrossRef]
- Shehabeldin, A.N.; Ro, J.Y. Neuroendocrine tumors of genitourinary tract: Recent advances. Ann. Diagn. Pathol. 2019, 42, 48–58. [Google Scholar] [CrossRef]
- Bahar, B.; Pambuccian, S.E.; Gupta, G.N.; Barkan, G.A. Renal paraganglioma: Report of a case managed by robotic assisted laparoscopic partial nephrectomy and review of the literature. Case Rep. Urol. 2014, 2014, 527592. [Google Scholar] [CrossRef]
- Fishbein, L.; Del Rivero, J.; Else, T.; Howe, J.R.; Asa, S.L.; Cohen, D.L.; Dahia, P.L.; Fraker, D.L.; Goodman, K.A.; Hope, T.A. The North American Neuroendocrine Tumor Society Consensus Guidelines for Surveillance and Management of Metastatic and/or Unresectable Pheochromocytoma and Paraganglioma. Pancreas 2021, 50, 469–493. [Google Scholar] [CrossRef]
- Kuroda, N.; Imamura, Y.; Hamashima, T.; Ohe, C.; Mikami, S.; Nagashima, Y.; Inoue, K.; Perez-Montiel, D.; Petersson, F.; Michal, M.; et al. Review of small cell carcinoma of the kidney with focus on clinical and pathobiological aspects. Pol. J. Pathol. 2014, 65, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Agoff, S.N.; Lamps, L.W.; Philip, A.T.; Amin, M.B.; Schmidt, R.A.; True, L.D.; Folpe, A.L. Thyroid transcription factor-1 is expressed in extrapulmonary small cell carcinomas but not in other extrapulmonary neuroendocrine tumors. Mod. Pathol. 2000, 13, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, T.; Seber, S.; Yavuzer, D.; Gumus, M.; Turhal, N.S. Primary renal carcinoid: Treatment and prognosis. Crit. Rev. Oncol. Hematol. 2013, 87, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, B.; Truong, L.D.; Saleh, G.; Sirbasku, D.M.; Slawin, K.M. Horseshoe kidney is associated with an increased relative risk of primary renal carcinoid tumor. J. Urol. 1997, 157, 2059–2066. [Google Scholar] [CrossRef]
- Takeshima, Y.; Inai, K.; Yoneda, K. Primary carcinoid tumor of the kidney with special reference to its histogenesis. Pathol. Int. 1996, 46, 894–900. [Google Scholar] [CrossRef]
- Shibata, R.; Okita, H.; Shimoda, M.; Asakura, H.; Murai, M.; Sakamoto, M.; Hata, J. Primary carcinoid tumor in a polycystic kidney. Pathol. Int. 2003, 53, 317–322. [Google Scholar] [CrossRef]
- De Hoog, J.P.; Murray, S.; Chou, W. Horseshoe kidney and primary renal carcinoid tumour: A case report of a rare entity. Grand Rounds 2010, 10, 46–51. [Google Scholar]
- Litwinowicz, R.; Szpor, J.; Januś, G.; Worek, M.; Okoń, K. Primary carcinoid tumour in horseshoe kidney. Pol. J. Pathol. 2011, 62, 72–74. [Google Scholar]
- Jeung, J.A.; Cao, D.; Selli, B.W.; Clapp, W.L.; Oliai, B.R.; Parwani, A.V.; Allan, R.W. Primary renal carcinoid tumors: Clinicopathologic features of 9 cases with emphasis on novel immunohistochemical findings. Hum. Pathol. 2011, 42, 1554–1561. [Google Scholar] [CrossRef]
- Wang, X.; Wang, F.; Liang, Y.; Chen, W. Primary small cell carcinoma after renal transplant: A case report. Medicine 2018, 97, e12592. [Google Scholar] [CrossRef]
- El-Naggar, A.K.; Troncoso, P.; Ordonez, N.G. Primary renal carcinoid tumor with molecular abnormality characteristic of conventional renal cell neoplasms. Diagn. Mol. Pathol. Am. J. Surg. Pathol. Part B 1995, 4, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Gruber, L.M.; Erickson, D.; Babovic-Vuksanovic, D.; Thompson, G.B.; Young, W.F., Jr.; Bancos, I. Pheochromocytoma and paraganglioma in patients with neurofibromatosis type 1. Clin. Endocrinol. 2017, 86, 141–149. [Google Scholar] [CrossRef] [PubMed]
- Van Der Tuin, K.; Mensenkamp, A.R.; Tops, C.M.; Corssmit, E.P.; Dinjens, W.N.; Van De Horst-schrivers, A.N.; Jansen, J.C.; De Jong, M.M.; Kunst, H.P.; Kusters, B. Clinical aspects of SDHA-related pheochromocytoma and paraganglioma: A nationwide study. J. Clin. Endocrinol. Metab. 2018, 103, 438–445. [Google Scholar] [CrossRef] [PubMed]
- McKeown, D.K.; Nguyen, G.-K.; Rudrick, B.; Johnson, M.A. Carcinoid of the kidney: Radiologic findings. Am. J. Roentgenol. 1988, 150, 143–144. [Google Scholar] [CrossRef]
- Karaosmanoğlu, A.D.; Onur, M.R.; Shirkhoda, A.; Ozmen, M.; Hahn, P.F. Unusual Malignant Solid Neoplasms of the Kidney: Cross-Sectional Imaging Findings. Korean J. Radiol. 2015, 16, 853–859. [Google Scholar] [CrossRef] [PubMed]
- Fine, S.W. Neuroendocrine lesions of the genitourinary tract. Adv. Anat. Pathol. 2007, 14, 286–296. [Google Scholar] [CrossRef]
- Shurtleff, B.T.; Shvarts, O.; Rajfer, J. Carcinoid tumor of the kidney: Case report and review of the literature. Rev. Urol. 2005, 7, 229. [Google Scholar]
- Van Oostenbrugge, T.J.; Fütterer, J.J.; Mulders, P.F. Diagnostic imaging for solid renal tumors: A pictorial review. Kidney Cancer 2018, 2, 79–93. [Google Scholar] [CrossRef]
- Lenders, J.W.; Duh, Q.-Y.; Eisenhofer, G.; Gimenez-Roqueplo, A.-P.; Grebe, S.K.; Murad, M.H.; Naruse, M.; Pacak, K.; Young, W.F., Jr. Pheochromocytoma and paraganglioma: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2014, 99, 1915–1942. [Google Scholar] [CrossRef]
- Else, T.; Greenberg, S.; Fishbein, L. Hereditary Paraganglioma-Pheochromocytoma Syndromes. In GeneReviews((R)); Adam, M.P., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Rajiah, P.; Sinha, R.; Cuevas, C.; Dubinsky, T.J.; Bush, W.H., Jr.; Kolokythas, O. Imaging of uncommon retroperitoneal masses. Radiographics 2011, 31, 949–976. [Google Scholar] [CrossRef]
- Dromain, C.; de Baere, T.; Baudin, E.; Galline, J.; Ducreux, M.; Boige, V.; Duvillard, P.; Laplanche, A.; Caillet, H.; Lasser, P. MR imaging of hepatic metastases caused by neuroendocrine tumors: Comparing four techniques. Am. J. Roentgenol. 2003, 180, 121–128. [Google Scholar] [CrossRef] [PubMed]
- Timmers, H.J.; Chen, C.C.; Carrasquillo, J.A.; Whatley, M.; Ling, A.; Havekes, B.; Eisenhofer, G.; Martiniova, L.; Adams, K.T.; Pacak, K. Comparison of 18F-fluoro-L-DOPA, 18F-fluoro-deoxyglucose, and 18F-fluorodopamine PET and 123I-MIBG scintigraphy in the localization of pheochromocytoma and paraganglioma. J. Clin. Endocrinol. Metab. 2009, 94, 4757–4767. [Google Scholar] [CrossRef] [PubMed]
- Timmers, H.J.; Chen, C.C.; Carrasquillo, J.A.; Whatley, M.; Ling, A.; Eisenhofer, G.; King, K.S.; Rao, J.U.; Wesley, R.A.; Adams, K.T. Staging and functional characterization of pheochromocytoma and paraganglioma by 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography. J. Natl. Cancer Inst. 2012, 104, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Hou, G.; Zhu, Z.; Huo, L.; Cheng, W.; Li, F. The value of multiparameter (18)F-FDG PET/CT imaging in differentiating retroperitoneal paragangliomas from unicentric Castleman disease. Sci. Rep. 2020, 10, 12887. [Google Scholar] [CrossRef]
- Lee, K.Y.; Oh, Y.W.; Noh, H.J.; Lee, Y.J.; Yong, H.S.; Kang, E.Y.; Kim, K.A.; Lee, N.J. Extraadrenal paragangliomas of the body: Imaging features. AJR Am. J. Roentgenol. 2006, 187, 492–504. [Google Scholar] [CrossRef]
- Taïeb, D.; Pacak, K. Molecular imaging and theranostic approaches in pheochromocytoma and paraganglioma. Cell Tissue Res. 2018, 372, 393–401. [Google Scholar] [CrossRef]
- Katabathina, V.S.; Rajebi, H.; Chen, M.; Restrepo, C.S.; Salman, U.; Vikram, R.; Menias, C.O.; Prasad, S.R. Genetics and imaging of pheochromocytomas and paragangliomas: Current update. Abdom. Radiol. 2020, 45, 928–944. [Google Scholar] [CrossRef]
- Castinetti, F.; Kroiss, A.; Kumar, R.; Pacak, K.; Taieb, D. 15 YEARS OF PARAGANGLIOMA: Imaging and imaging-based treatment of pheochromocytoma and paraganglioma. Endocr. Relat. Cancer 2015, 22, T135-145. [Google Scholar] [CrossRef]
- Omiyale, A.O.; Venyo, A.K. Primary carcinoid tumour of the kidney: A review of the literature. Adv. Urol. 2013, 2013, 579396. [Google Scholar] [CrossRef]
- McGarrah, P.W.; Westin, G.F.M.; Hobday, T.J.; Scales, J.A.; Ingimarsson, J.P.; Leibovich, B.C.; Halfdanarson, T.R. Renal Neuroendocrine Neoplasms: A Single-center Experience. Clin. Genitourin. Cancer 2020, 18, e343–e349. [Google Scholar] [CrossRef]
- Zhang, Q.; Ming, J.; Zhang, S.; Qiu, X. Primary micro neuroendocrine tumor arising in a horseshoe kidney with cyst: Report of a case and review of literature. Diagn. Pathol. 2012, 7, 126. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, J.E.; Albersheim, J.A.; Sathianathen, N.J.; Murugan, P.; Weight, C.J. Five new cases of primary renal carcinoid tumor: Case reports and literature review. Pathol. Oncol. Res. 2020, 26, 341–346. [Google Scholar] [CrossRef] [PubMed]
- Kouba, E.; Cheng, L. Neuroendocrine Tumors of the Urinary Bladder According to the 2016 World Health Organization Classification: Molecular and Clinical Characteristics. Endocr. Pathol. 2016, 27, 188–199. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Pan, C.X.; Yang, X.J.; Lopez-Beltran, A.; MacLennan, G.T.; Lin, H.; Kuzel, T.M.; Papavero, V.; Tretiakova, M.; Nigro, K.; et al. Small cell carcinoma of the urinary bladder: A clinicopathologic analysis of 64 patients. Cancer 2004, 101, 957–962. [Google Scholar] [CrossRef]
- Qayoom, S.; Chakrabarti, D.; Khan, F.; Goel, M.M. Primary small cell carcinoma of the urinary bladder. BMJ Case Rep. 2019, 12. [Google Scholar] [CrossRef]
- Reyes, C.V.; Soneru, I. Small cell carcinoma of the urinary bladder with hypercalcemia. Cancer 1985, 56, 2530–2533. [Google Scholar] [CrossRef]
- Sehgal, S.S.; Wein, A.J.; Bing, Z.; Malkowicz, S.B.; Guzzo, T.J. Neuroendocrine tumor of the bladder. Rev. Urol. 2010, 12, e197. [Google Scholar]
- Chen, Y.-b.; Epstein, J.I. Primary carcinoid tumors of the urinary bladder and prostatic urethra: A clinicopathologic study of 6 cases. Am. J. Surg. Pathol. 2011, 35, 442–446. [Google Scholar] [CrossRef]
- Holmang, S.; Borghede, G.; Johansson, S.L. Primary small cell carcinoma of the bladder: A report of 25 cases. J. Urol. 1995, 153, 1820–1822. [Google Scholar] [CrossRef]
- Amin, M.B. Histological variants of urothelial carcinoma: Diagnostic, therapeutic and prognostic implications. Mod. Pathol. 2009, 22, S96–S118. [Google Scholar] [CrossRef]
- Watson, G.A.; Ahmed, Y.; Picardo, S.; Chew, S.; Cobbe, S.; Mahony, C.; Crotty, J.; Wallis, F.; Shelly, M.J.; Kiely, P. Unusual sites of high-grade neuroendocrine carcinomas: A case series and review of the literature. Am. J. Case Rep. 2018, 19, 710. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Sol, Y.; Lee, S.W.; Jeh, S.U.; Hwa, J.S.; Hyun, J.S.; Chung, K.H.; Seo, D.H.; Yang, J.W.; Song, D.H.; et al. Primary large-cell neuroendocrine carcinoma of the upper ureter: A case report. Medicine 2019, 98, e15613. [Google Scholar] [CrossRef] [PubMed]
- Oshiro, H.; Odagaki, Y.; Iobe, H.; Ozu, C.; Takizawa, I.; Nagai, T.; Matsubayashi, J.; Inagaki, A.; Miyake, S.; Nagao, T. Primary large cell neuroendocrine carcinoma of the ureter. Int. J. Clin. Exp. Pathol. 2013, 6, 729. [Google Scholar] [PubMed]
- Hanji, A.M.; Rohan, V.S.; Patel, J.J.; Tankshali, R.A. Pheochromocytoma of the urinary bladder: A rare cause of severe hypertension. Saudi J. Kidney Dis. Transplant. 2012, 23, 813. [Google Scholar]
- Dahm, P.; Gschwend, J.E. Malignant non-urothelial neoplasms of the urinary bladder: A review. Eur. Urol. 2003, 44, 672–681. [Google Scholar] [CrossRef]
- Zimmerman, I.J.; Biron, R.E.; MacMahon, H.E. Pheochromocytoma of the urinary bladder. N. Engl. J. Med. 1953, 249, 25–26. [Google Scholar] [CrossRef]
- Dwethi, G.; Vikas, C.; Ramesh, T. Urinary bladder paraganglioma. Appl. Radiol. 2019, 48, 48A–48C. [Google Scholar] [CrossRef]
- Alberti, C. Urology pertinent neuroendocrine tumors: Focusing on renal pelvis, bladder, prostate located sympathetic functional paragangliomas. G. Chir. 2016, 37, 55. [Google Scholar] [CrossRef]
- Yadav, R.; Das, A.K.; Kumar, R. Malignant non-functional paraganglioma of the bladder presenting with azotemia. Int. Urol. Nephrol. 2007, 39, 449–451. [Google Scholar] [CrossRef]
- Sheps, S.G.; Jiang, N.S.; Klee, G.G.; van Heerden, J.A. Recent developments in the diagnosis and treatment of pheochromocytoma. Mayo Clin Proc 1990, 65, 88–95. [Google Scholar] [CrossRef]
- Eble, J.N. Classification of tumours: Pathology and genetics of tumours of the urinary system and male genital organs. World Health Organ. Classif. Tumours 2004, 255–257. [Google Scholar]
- Cheng, L.; Jones, T.D.; McCarthy, R.P.; Eble, J.N.; Wang, M.; MacLennan, G.T.; Lopez-Beltran, A.; Yang, X.J.; Koch, M.O.; Zhang, S.; et al. Molecular genetic evidence for a common clonal origin of urinary bladder small cell carcinoma and coexisting urothelial carcinoma. Am. J. Pathol. 2005, 166, 1533–1539. [Google Scholar] [CrossRef]
- Abrahams, N.; Moran, C.; Reyes, A.; Siefker-Radtke, A.; Ayala, A. Small cell carcinoma of the bladder: A contemporary clinicopathological study of 51 cases. Histopathology 2005, 46, 57–63. [Google Scholar] [CrossRef]
- Akamatsu, S.; Kanamaru, S.; Ishihara, M.; Sano, T.; Soeda, A.; Hashimoto, K. Primary large cell neuroendocrine carcinoma of the urinary bladder. Int. J. Urol. 2008, 15, 1080–1083. [Google Scholar] [CrossRef]
- Wong-You–Cheong, J.J.; Woodward, P.J.; Manning, M.A.; Sesterhenn, I.A. Neoplasms of the urinary bladder: Radiologic-pathologic correlation. Radiographics 2006, 26, 553–580. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.C.; Kim, K.H.; Jung, S. Small cell carcinoma of the urinary bladder: CT and MR imaging findings. Korean J. Radiol. 2003, 4, 130–135. [Google Scholar] [CrossRef]
- Asbury, W., Jr.; Hatcher, P.; Gould, H.; Reeves, W.; Wilson, D. Bladder pheochromocytoma with ring calcification. Abdom. Imaging 1996, 21, 275–277. [Google Scholar]
- Jalil, N.D.; Pattou, F.N.; Combemale, F.; Chapuis, Y.; Henry, J.F.; Peix, J.L.; Proye, C.A. Effectiveness and limits of preoperative imaging studies for the localisation of pheochromocytomas and paragangliomas: A review of 282 cases. French Association of Surgery (AFC), and The French Association of Endocrine Surgeons (AFCE). Eur. J. Surg. 1998, 164, 23–28. [Google Scholar] [CrossRef]
- Hwang, J.J.; Uchio, E.M.; Patel, S.V.; Linehan, W.M.; Walther, M.M.; Pacak, K. Diagnostic localization of malignant bladder pheochromocytoma using 6-18F fluorodopamine positron emission tomography. J. Urol. 2003, 169, 274–275. [Google Scholar] [CrossRef]
- Halefoglu, A.M.; Miroglu, C.; Uysal, V.; Mahmutoglu, A. Malignant paraganglioma of the urinary bladder. Eur. J. Radiol. Extra 2006, 58, 53–58. [Google Scholar] [CrossRef]
- Dhillon, J. Neuroendocrine Tumors of the Urinary Bladder and Molecular Features. In Neuroendocrine Tumors: Review of Pathology, Molecular and Therapeutic Advances; Nasir, A., Coppola, D., Eds.; Springer: New York, NY, USA, 2016; pp. 359–367. [Google Scholar]
- Zhao, X.; Flynn, E.A. Small cell carcinoma of the urinary bladder: A rare, aggressive neuroendocrine malignancy. Arch. Pathol. Lab. Med. 2012, 136, 1451–1459. [Google Scholar] [CrossRef] [PubMed]
- Erdem, G.U.; Özdemir, N.Y.; Demirci, N.S.; Şahin, S.; Bozkaya, Y.; Zengin, N. Small cell carcinoma of the urinary bladder: Changing trends in the current literature. Curr. Med. Res. Opin. 2016, 32, 1013–1021. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.D.; Kernek, K.M.; Yang, X.J.; Lopez-Beltran, A.; MacLennan, G.T.; Eble, J.N.; Lin, H.; Pan, C.-X.; Tretiakova, M.; Baldridge, L.A. Thyroid transcription factor 1 expression in small cell carcinoma of the urinary bladder: An immunohistochemical profile of 44 cases. Hum. Pathol. 2005, 36, 718–723. [Google Scholar] [CrossRef]
- Cheuk, W.; Kwan, M.Y.; Suster, S.; Chan, J.K. Immunostaining for thyroid transcription factor 1 and cytokeratin 20 aids the distinction of small cell carcinoma from Merkel cell carcinoma, but not pulmonary from extrapulmonary small cell carcinomas. Arch. Pathol. Lab. Med. 2001, 125, 228–231. [Google Scholar] [CrossRef]
- Kairi-Vassilatou, E.; Argeitis, J.; Nika, H.; Grapsa, D.; Smyrniotis, V.; Kondi-Pafiti, A. Malignant paraganglioma of the urinary bladder in a 44-year-old female: Clinicopathological and immunohistochemical study of a rare entity and literature review. Eur. J. Gynaecol. Oncol. 2007, 28, 149–151. [Google Scholar] [PubMed]
- Choong, N.W.; Quevedo, J.F.; Kaur, J.S. Small cell carcinoma of the urinary bladder: The Mayo Clinic experience. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2005, 103, 1172–1178. [Google Scholar] [CrossRef]
- Kempasiddaiah, G.M.; Thimmaiah, R.; Gurappa, M. A rare case of early pregnancy with paraganglioma of urinary bladder. Int. J. Curr. Res. Rev. 2014, 6, 15–20. [Google Scholar]
- Magers, M.J.; Lopez-Beltran, A.; Montironi, R.; Williamson, S.R.; Kaimakliotis, H.Z.; Cheng, L. Staging of bladder cancer. Histopathology 2019, 74, 112–134. [Google Scholar] [CrossRef]
- Mirmomen, S.M.; Shinagare, A.B.; Williams, K.E.; Silverman, S.G.; Malayeri, A.A. Preoperative imaging for locoregional staging of bladder cancer. Abdom. Radiol. 2019, 44, 3843–3857. [Google Scholar] [CrossRef]
- Qing, D.; Peng, L.; Cen, F.; Huang, X.; Wei, Q.; Lu, H. Hyperprogression After Immunotherapy for Primary Small Cell Neuroendocrine Carcinoma of the Ureter: A Case Report. Front. Oncol. 2021, 11, 696422. [Google Scholar] [CrossRef]
- Rupert, V.; Clifton, M.M.; Fulmer, B.R.; Mori, R.L.; Williams, H.; Park, A. Primary small cell carcinoma of the upper urinary tract: A case report. Urol. Case Rep. 2019, 27, 100995. [Google Scholar] [CrossRef] [PubMed]
- Fetissof, F.; Dubois, M.; Lanson, Y.; Jobard, P. Endocrine cells in renal pelvis and ureter, an immunohistochemical analysis. J. Urol. 1986, 135, 420–421. [Google Scholar] [CrossRef]
- Harada, K.; Sato, Y.; Ikeda, H.; Hsu, M.; Igarashi, S.; Nakanuma, Y. Notch1-Hes1 signalling axis in the tumourigenesis of biliary neuroendocrine tumours. J. Clin. Pathol. 2013, 66, 386–391. [Google Scholar] [CrossRef]
- Zhong, W.; Lin, R.; Zhang, L.; Jin, C.; Li, X.; He, Q.; Gong, K.; He, Z.; Zhou, L. Clinicopathologic characteristics, therapy and outcomes of patients with primary ureteral small cell carcinoma: A case series and systematic review of the literature. OncoTargets Ther. 2017, 10, 4105. [Google Scholar] [CrossRef] [PubMed]
- Xu, S.; Xu, L.; Cao, P.; Yao, S.; Wu, T.; Hu, X.; Chen, H.; Gu, J.; Che, X. Collision Carcinoma Involving Small Cell Neuroendocrine Carcinoma and Squamous Cell Carcinoma of the Ureter: A Case Report and Review of the Literature. Front. Oncol. 2021, 11, 663119. [Google Scholar] [CrossRef]
- Ouzzane, A.; Ghoneim, T.P.; Udo, K.; Verhasselt-Crinquette, M.; Puech, P.; Betrouni, N.; Rouprêt, M.; Villers, A.; Leroy, X.; Colin, P. Small cell carcinoma of the upper urinary tract (UUT-SCC): Report of a rare entity and systematic review of the literature. Cancer Treat. Rev. 2011, 37, 366–372. [Google Scholar] [CrossRef]
- Acosta, A.M.; Kajdacsy-Balla, A. Primary Neuroendocrine Tumors of the Ureter: A Short Review. Arch. Pathol. Lab. Med. 2016, 140, 714–717. [Google Scholar] [CrossRef]
- Banerji, J.S.; Korula, A.; Panicker, J.B. Multicentric small cell neuroendocrine neoplasm of the renal pelvis and ureter with concomitant focal high-grade urothelial carcinoma of the ureter: A case report. Indian J. Urol. IJU J. Urol. Soc. India 2008, 24, 571. [Google Scholar] [CrossRef]
- Ping, J.H.; Chen, Z.X.; Jiong, Q.; Han, Y.Q.; Nong, X. Small cell neuroendocrine carcinoma of the ureter: A case report and literature review. Oncol. Lett. 2014, 7, 728–730. [Google Scholar] [CrossRef]
- Yang, J.; Zhao, Z.; Ni, J.; Dong, W.; Wang, N.; Wang, B. Urography and CT features of primary small cell carcinoma of the ureter: A case report. Iran. J. Radiol. 2013, 10, 160. [Google Scholar] [CrossRef]
- Hensley, P.J.; Bhalodi, A.A.; Gupta, S. Primary Upper Urinary Tract Small Cell Carcinoma: A Case Series and Literature Review. J. Endourol. Case Rep. 2017, 3, 165–168. [Google Scholar] [CrossRef] [PubMed]
- Acosta, A.M.; Hamedani, F.S.; Meeks, J.J.; Wu, S. Primary ureteral thyroid transcription factor 1–positive small cell neuroendocrine carcinoma: Case report and review of the literature. Int. J. Surg. Pathol. 2015, 23, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.J.; Holmäng, S.; Johansson, S.L.; Lele, S.M. Small cell carcinoma of the renal pelvis and ureter: Clinicopathologic and immunohistochemical features. Arch. Pathol. Lab. Med. 2011, 135, 1565–1569. [Google Scholar] [CrossRef] [PubMed]
- DiPietro, M.; Zeman, R.K.; Keohane, M.; Rosenfield, A.T. Oat cell carcinoma metastatic to ureter. Urology 1983, 22, 419–420. [Google Scholar] [CrossRef]
- Zhu, J.; Feng, Y.; Fan, M.; He, X.; Wang, L. Primary small cell neuroendocrine carcinoma combined with squamous carcinoma of the ureter after renal transplantation: A rare case report. Int. J. Clin. Exp. Pathol. 2019, 12, 1357. [Google Scholar]
- Essenfeld, H.; Manivel, J.C.; Benedetto, P.; Albores-Saavedra, J. Small cell carcinoma of the renal pelvis: A clinicopathological, morphological and immunohistochemical study of 2 cases. J. Urol. 1990, 144, 344–347. [Google Scholar] [CrossRef]
- Sato, R.; Ishikawa, T.; Imagawa, M.; Yonemasu, H.; Narimatsu, T.; Murakami, K. Primary small cell carcinoma of the ureter with hydronephrosis: A case report. Urol. Case Rep. 2020, 29, 101099. [Google Scholar] [CrossRef]
- Sood, A.; Williamson, S.R.; Leavitt, D.A. Neuroendocrine Tumor of the Ureter: A Zebra among Horses. J. Endourol. Case Rep. 2016, 2, 204–208. [Google Scholar] [CrossRef]
- Yao, J.L.; Madeb, R.; Bourne, P.; Lei, J.; Yang, X.; Tickoo, S.; Liu, Z.; Tan, D.; Cheng, L.; Hatem, F. Small cell carcinoma of the prostate: An immunohistochemical study. Am. J. Surg. Pathol. 2006, 30, 705–712. [Google Scholar] [CrossRef]
- Terada, T. Primary small cell carcinoma of the ureter: A case report involving immunohistochemical and molecular genetic analyses of KIT and PDGFRA genes. Pathology 2010, 42, 101–102. [Google Scholar] [CrossRef]
- Arora, H.C.; Fascelli, M.; Zhang, J.H.; Isharwal, S.; Campbell, S.C. Kidney, Ureteral, and Bladder Cancer: A Primer for the Internist. Med. Clin. N. Am. 2018, 102, 231–249. [Google Scholar] [CrossRef] [PubMed]
- Yoo, K.H.; Kim, G.Y.; Kim, T.G.; Min, G.E.; Lee, H.L. Primary small cell neuroendocrine carcinoma of the female urethra. Pathol. Int. 2009, 59, 601–603. [Google Scholar] [CrossRef] [PubMed]
- Rudloff, U.; Amukele, S.A.; Moldwin, R.; Qiao, X.; Morgenstern, N. Small cell carcinoma arising from the proximal urethra. Int. J. Urol. 2004, 11, 674–677. [Google Scholar] [CrossRef] [PubMed]
- Kanagarajah, P.; Ayyathurai, R.; Saleem, U.; Manoharan, M. Small cell carcinoma arising from the bulbar urethra: A case report and literature review. Urol. Int. 2012, 88, 477–479. [Google Scholar] [CrossRef]
- Mackey, J.R.; Au, H.-J.; Hugh, J.; Venner, P. Genitourinary small cell carcinoma: Determination of clinical and therapeutic factors associated with survival. J. Urol. 1998, 159, 1624–1629. [Google Scholar] [CrossRef]
- Iczkowski, K.; Shanks, J.; Allsbrook, W.; Lopez-Beltran, A.; Pantazis, C.; Collins, T.; Wetherington, R.; Bostwick, D. Small cell carcinoma of urinary bladder is differentiated from urothelial carcinoma by chromogranin expression, absence of CD44 variant 6 expression, a unique pattern of cytokeratin expression, and more intense γ-enolase expression. Histopathology 1999, 35, 150–156. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Renal Carcinoids | Renal Small-Cell NEC | Renal Large-Cell NEC | Renal Paraganglioma | |
|---|---|---|---|---|
| Cellular arrangements | Trabecular/gyriform, glandular, insular, solid or mixed patterns | Sheets, nests, trabeculae | Solid nesting growth pattern | |
| Cellular characteristics | Round or polygonal cells with granular cytoplasm. | Poorly differentiated small round to fusiform cells; scanty stroma and cytoplasm | Large cells with abundant cytoplasm | Round to oval cells (Zellballen); sometimes spindle-shaped elongated cells; abundant granular cytoplasm; |
| Nuclei | Round nucleus with finely stippled ribbon-like chromatin; inconspicuous nucleoli | Hyperchromatic nuclei; Nuclear molding; stippled/dispersed chromatin; inconspicuous nucleoli | Pleomorphic nuclei with vesicular chromatin; Prominent nucleoli | Variant nuclei with regular uniform chromatin or hyperchromasia |
| Additional features | Calcifications (25% of cases); Absence of frequent mitosis; Low Ki-67 proliferation index | Extensive tumor necrosis; perivascular DNA deposition (Azzopardi phenomenon); Brisk mitoses; Calcifications can be seen. | High mitotic rate (>10/10 per HPF); Large necrotic areas | Highly vascular intervening stroma; Low mitotic index and necrosis |
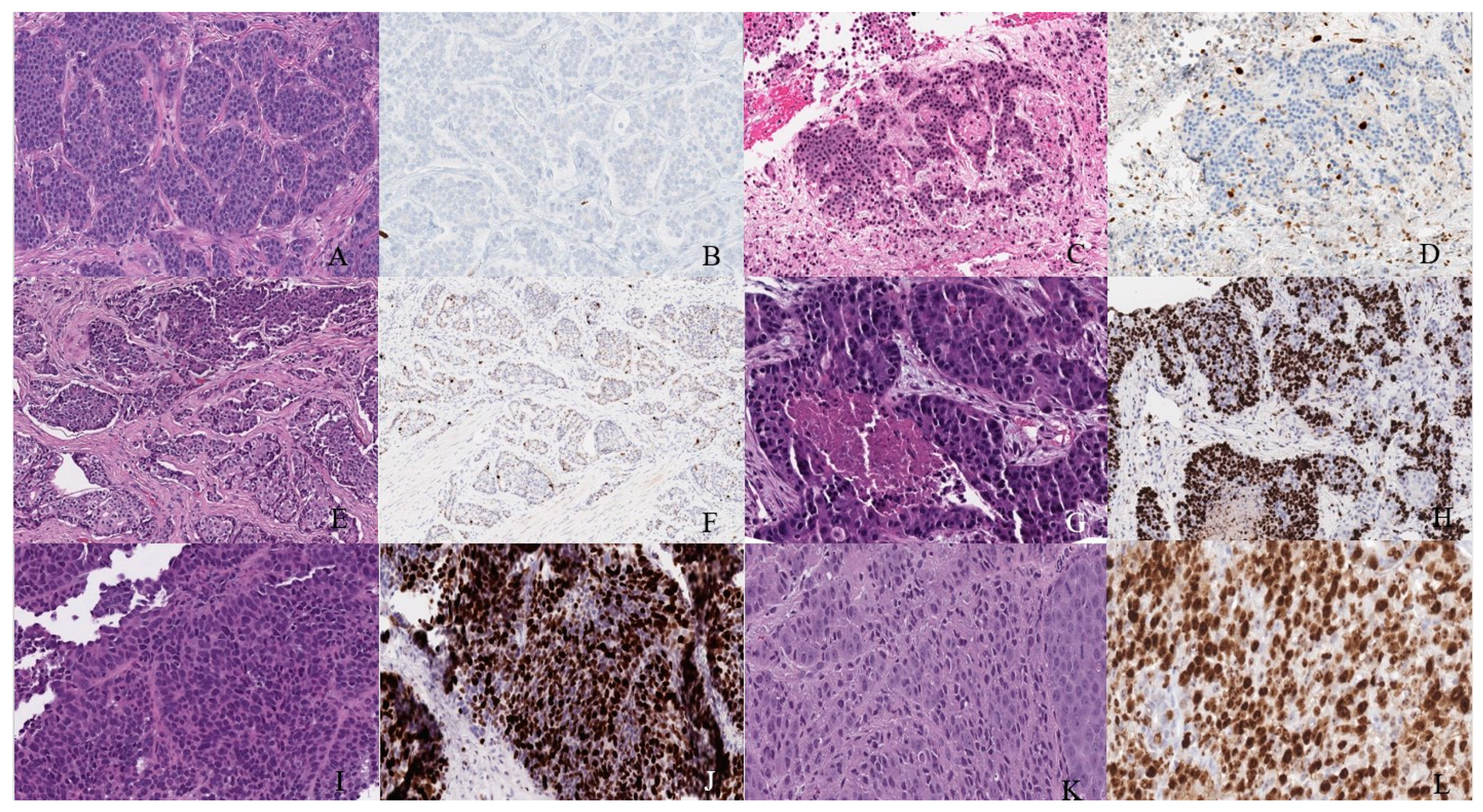
| Immunohistochemistry | Positive for cytokeratin, chromogranin, synaptophysin, gremileus and neuron-specific enolase | Dot-like cytokeratin staining in the cytoplasm; Variable positivity for chromogranin A, synaptophysin, CD56 and NSE; A few cases reported positive staining for TTF-1 [17,31,32] | Diffusely and strongly positive for synaptophysin | Positive for INSM1, synaptophysin and chromogranin; Negative for keratins; Positive tyrosine hydroxylase and nuclear GATS3; scattered S100-sustentacular cells |
| Renal Lesion | CT | MRI |
|---|---|---|
| Clear Cell carcinoma | Heterogeneous mass due to necrotic, cystic and hemorrhagic areas; Strong contrast enhancement in corticomedullary and contrast wash out during nephrographic phases | Hyper vascular lesion; Hyperintense on T2WI and hypo- to isointense on T1WI; Heterogeneous avid enhancement than the rest of RCC types on contrast administration; Microscopic fat in 60% of cases; CSI: >25% signal loss on opposed phase relative to in-phase imaging due to fat content; Tumor pseudo capsule: hypointense rim on T1WI and T2WI. |
| Chromophobe carcinoma | Homogeneous to heterogeneous mass | Well circumscribed homogeneous tumors; Iso- to hypointense lesion son T2WI; The lesion enhances greater than papillary but lesser than clear cell renal carcinoma; Central stellate scar in 30–40% of cases; Spoke-wheel enhancement can be observed; Segmental enhancement inversion may be noticed; Calcifications in 38% of cases. |
| Papillary carcinoma | Tumors < 3 cm: homogeneous; Tumors ≥ 4 cm: Heterogeneous due to necrosis; Subtle contrast enhancement than ccRCC; Absent enhancement can be observed in 25% of patients; | Well-circumscribed homogeneous mass; Usually <3 cm; Mass: hypointense on T2WI which enhance progressively with contrast administration; CSI: signal loss on in-phase relative to opposed phase imaging due to hemosiderin deposition; Fibrous capsule: hypointense on T1WI & T2WI; |
| Renal NET | Heterogeneous solid tumor with cystic component as well; Minimal enhancement on contrast administration; Octreotide scintigraphy: High affinity for somatostatin in 87% of patients. | Heterogeneous signal intensity on T1 and T2WI with areas of high signal intensity on T1WI due to hemorrhage; The mass enhances with contrast administration |
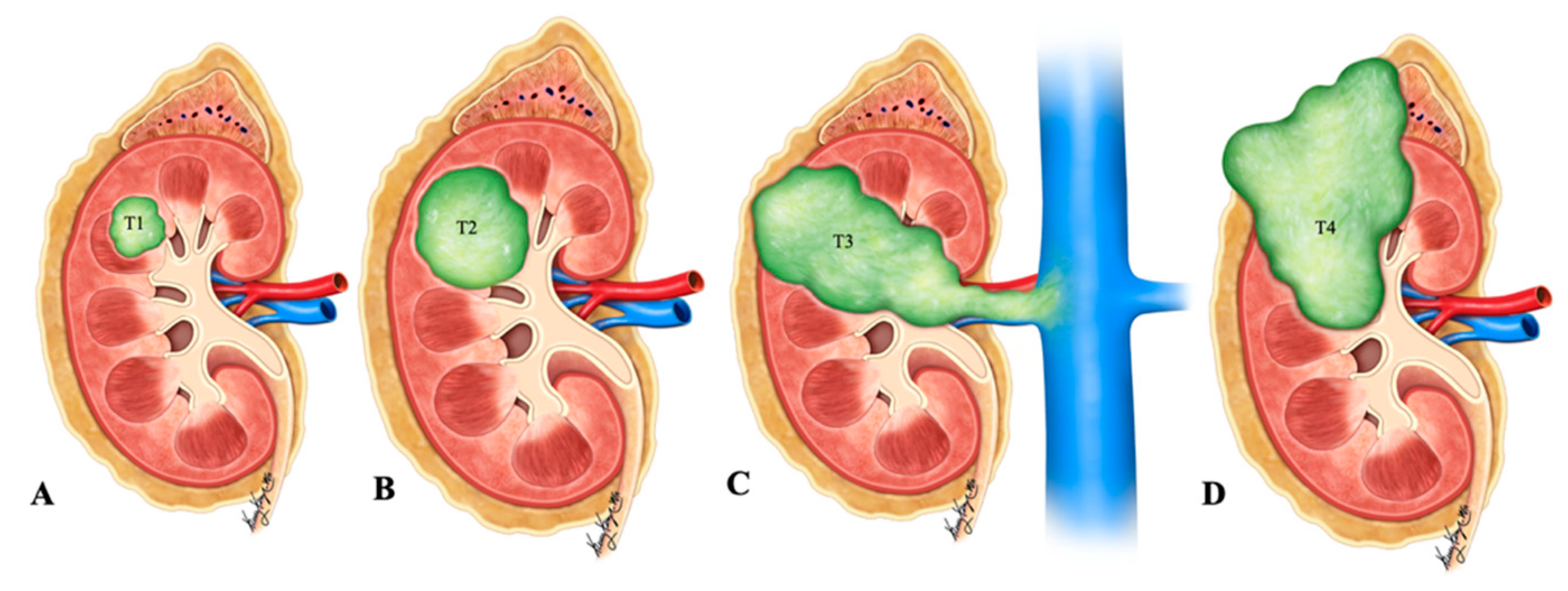
| Stage | TNM Category | Description |
|---|---|---|
| I | T1 N0 M0 | T1–Tumor limited to kidney & ≤7 cm in greatest dimension N0–No lymph node involvement M0–No distant metastasis |
| II | T2 N0 M0 | T2–Tumor limited to kidney & >7 cm in greatest dimension |
| III | T3 N0 M0 | T3–Tumor extending into the major vein or into the tissue around kidney; but not growing into adrenal gland or beyond Gerota’s fascia |
| T1-3 N1 M0 | N1–Tumor spread to regional lymph nodes | |
| IV | T4 Any N M0 | T4–Tumor beyond Gerota’s fascia and may be growing into adrenal gland on the top of kidney |
| Any T Any N M1 | M1–Distant lymph nodes and/or other organs. |
| Stage | TNM Category | Description |
|---|---|---|
| I | T1 N0 M0 | T1–Pheochromocytoma < 5 cm in greatest dimension; No extra-adrenal invasion; N0–no lymph node metastases; M0–No distant metastases |
| II | T2 N0 M0 | T2–Pheochromocytoma ≥ 5 cm, sympathetic paraganglioma of any size; no extra-adrenal invasion |
| III | T1 N1 M0 | N1–Lymph node metastases |
| III | T2 N1 M0 | |
| III | T3 N0 M0 | T3–Tumor of any size with surround tissue invasion (liver, spleen, pancreas and kidneys) |
| III | T3 N1 M0 | |
| IV | Any T Any N M1 | M1–distant metastases; M1a–Distant metastases to only bone; M1b–Distant metastases to only lymph nodes/liver/lung; M1c–Distant metastases to bone plus multiple other sites |
| Histological Features | Well-Differentiated NET | Small-Cell NEC | Large-Cell NEC | Paraganglioma |
|---|---|---|---|---|
| Cellular arrangements | Anastomosing cords; Glandular; Cribriform structures | Diffuse sheets; Nests | Sheets; Solid nests; Trabeculae; Rosettes | Nests; Diffuse growth; Pseudo rosettes |
| Cellular characteristics | Intermediate cuboidal/columnar monomorphic cells with moderate to abundant cytoplasm and eosinophilic granules | Small/intermediate fusiform cells with scant cytoplasm | Large polygonal cells with abundant cytoplasm | Large polygonal cells with moderate cytoplasm |
| Nuclei | Small round to oval nuclei with finely stippled chromatin and inconspicuous nucleolus | Small round to oval nuclei with finely granular chromatin, molding and crush artifact; Inconspicuous salt and pepper nucleolus | Large oval nuclei with coarse, granular, vesicular chromatin and prominent nucleolus | Medium round to oval nuclei with smudged, hyperchromatic chromatin and prominent nucleolus |
| Additional findings | Infrequent mitotic activity and absent necrosis | High mitotic activity and foci of necrosis; Lymphovascular invasion | Very high mitotic activity and large areas of necrosis | Rare mitotic activity and necrosis |
| Stage | TNM Category | Description |
|---|---|---|
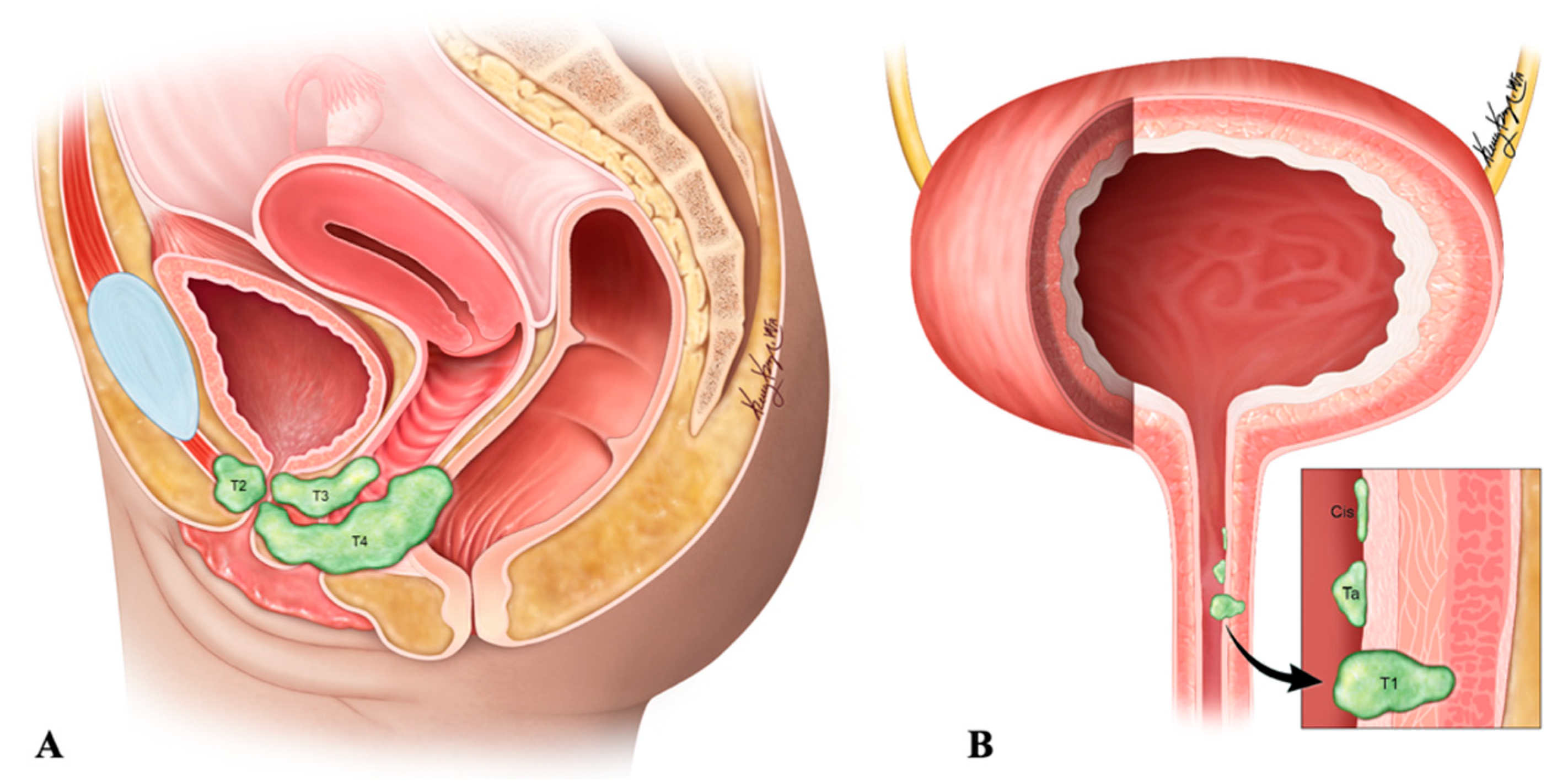
| 0a | Ta N0 M0 | Non-invasive papillary carcinoma; No lymph node involvement; No distant metastasis |
| 0is | Tis N0 M0 | Carcinoma in-situ (“Flat-tumor”) |
| I | T1 N0 M0 | Tumor invasion into subepithelial connective tissue (lamina propria) |
| II | T2a N0 M0 | Tumor invasion into superficial muscularis propria (inner half of detrusor muscle) |
| T2b N0 M0 | Tumor invasion into deep muscularis propria (outer half of detrusor muscle) | |
| IIIA | T3a N0 M0 | Microscopic invasion of peri-vesical tissue |
| T3b N0 M0 | Macroscopic invasion of peri-vesical tissue (extravesical mass) | |
| T4a N0 M0 | Tumor invades any of: prostatic stroma, seminal vesicles, uterus, vagina | |
| T1-4a N1 M0 | Single regional lymph node involvement: peri-vesical, obturator, internal and external iliac, or sacral lymph nodes | |
| IIIB | T1-4a N2 or N3 M0 | N2–Multiple regional lymph node involvement; N3–Common iliac lymph node involvement |
| IVA | T4b Any N M0 | T4b–Tumor invasion into pelvic or abdominal wall |
| Any T Any N M1a | M1a–Distant metastases to lymph nodes beyond common iliac arteries | |
| IVB | Any T Any N M1b | M1b–Distant metastases to sites such as bones, liver or lungs |
| Features | Small-Cell NEC |
|---|---|
| Gross | Well-defined firm-greyish mass protruding into the ureteral lumen; hemorrhagic areas |
| Histology | |
| Cellular arrangement | Solid sheets; rosette; nests |
| Cellular characteristics | Small to medium sized cells with scant cytoplasm and granular chromatin |
| Additional features | Frequent necrotic areas, mitosis and vascular invasion |
| Immunohistochemistry | |
| Neuroendocrine stains | Chromogranin A, synaptophysin, CD56, neuron-specific enolase |
| Epithelial stains | Cytokeratin-7, epithelial membrane antigen, and pan-cytokeratin |
| Differential stains | Uroplakin III-negative (positive in umbrella cells of urothelium and transitional cell carcinoma) |
| Differential Diagnosis | Distinguishing Feature |
|---|---|
| Carcinoid tumors | Small cells with low-grade nuclear atypia; low mitotic activity (usually <2/HPF); low Ki-67 index |
| Small-cell carcinoma | Small cells (usually less than the diameter of the three small lymphocytes) with scant cytoplasm; fine granular chromatin; absent or inconspicuous nuclei; high miotic activity (≥11/HPF with a median of 80/HPF); frequent large areas of necrosis |
| High-grade urothelial carcinoma | Poorly differentiated cells with centrally located nuclei and thick, rough nuclear membranes; Identifiable nucleoli; Irregular chromatin; Positive immunohistochemistry for uroplakin (57–81% of cases) and negative or neuroendocrine markers; |
| Primary or metastatic adenocarcinoma | Diffuse glandular morphology; negative neuroendocrine markers on immunohistochemical analyses |
| Stage | TNM Staging | Description |
|---|---|---|
| 0 | Ta N0 M0 | Non-invasive papillary tumor |
| Tis N0 M0 | Carcinoma in-situ | |
| I | T1 N0 M0 | Tumor invasion into sb-epithelial connective tissue through lamina propria |
| II | T2 N0 M0 | Tumor invasion into muscularis propria |
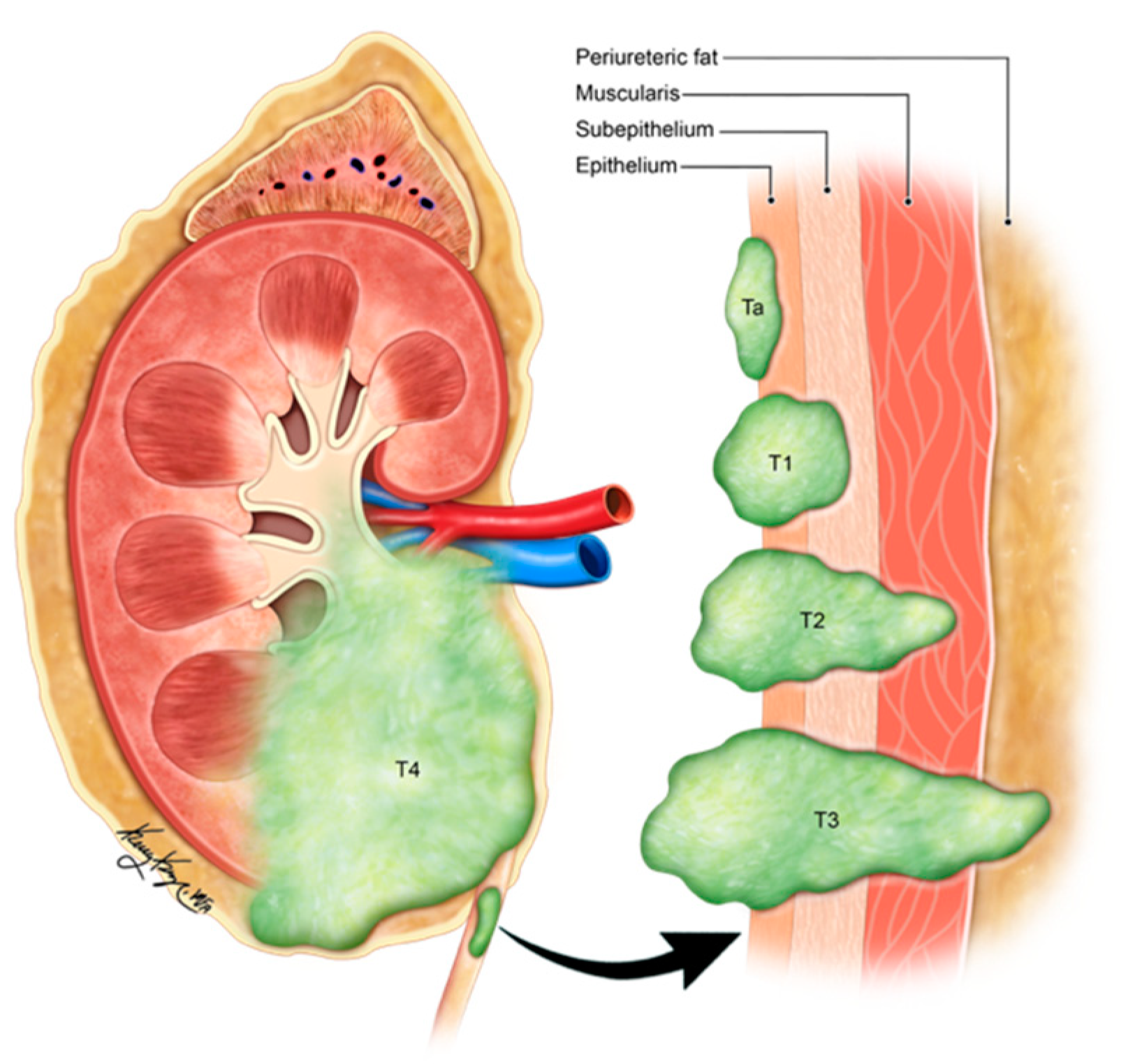
| III | T3 N0 M0 | Tumor invasion into periureteric fat beyond muscularis propria |
| T4 N0 M0 | Tumor invades adjacent organs or through the kidney into the perinephric fat | |
| IV | T4 Any N Any M | N1-metastasis in a single lymph node ≤ 2 cm in greatest dimension N2-Metastasis in a single lymph node > 2 cm; or multiple lymph node involvement N3-Metastasis in a lymph node, more than 5 cm in greatest dimension M1-Distant metastasis |
| Any T N1-3 Any M |
| Differential Diagnosis | Characteristic of Urethral NEN That Helps in Distinguishment |
|---|---|
| Lymphoma | Positive immunohistochemistry with LCA antigen |
| Transitional cell carcinoma | Positive p63 and CD44v6 (80% specific) |
| Carcinoid tumor | Abundant eosinophilic cytoplasm and regular nuclei |
| Primary neuroectodermal tumor | Larger cell bodies with spread out cytoplasm in dendritic processes |
| Metastatic small-cell carcinoma | Positive TTF-1 and presence of primary site on chest CT |
| Merkel cell carcinoma | Penile or scrotal skin involvement and presence of punctate paranuclear cytokeratin staining; positive CK20 |
| Stage | TNM Category | Description | |
|---|---|---|---|
| 0a | Ta N0 M0 | Ta-Non-invasive papillary, polypoid, or verrucous carcinoma; N0-No lymph node involvement; M0-No distant metastases | Proximal: Partial or complete urethrectomy Distal: Urethra-sparing surgery/urethrectomy/radiotherapy |
| 0is | Tis N0 M0 | Tis-Carcinoma in-situ | Proximal: Partial or complete urethrectomy Distal: Urethra-sparing surgery/urethrectomy/radiotherapy |
| I | T1 N0 M0 | T1-Tumor invasion into subepithelial connective tissue | Proximal: Partial or complete urethrectomy Distal: Urethra-sparing surgery/urethrectomy/radiotherapy |
| II | T2 N0 M0 | T2-Tumor invasion into corpus spongiosum/prostate or peri-urethral muscles | Proximal: Partial or complete urethrectomy ± neoadjuvant chemotherapy Distal: Urethra-sparing surgery/urethrectomy/radiotherapy |
| III | T1 N1 M0 | N1-Single lymph node involvement ≤ 2 cm in greatest dimension | Inductive chemotherapy + consolidative surgery; chemoradiotherapy |
| T2 N1 M0 | Inductive chemotherapy + consolidative surgery; chemoradiotherapy | ||
| T3 N0 M0 | T3-Tumor invasion into corpus cavernosum, beyond prostate capsule, anterior vagina and bladder neck | Neoadjuvant chemotherapy + surgery; Surgery + adjuvant radiotherapy | |
| T3 N1 M0 | Inductive chemotherapy + consolidative surgery; chemoradiotherapy | ||
| IV | T4 N0 M0 | T4-Tumor invasion into adjacent organs (e.g., Bladder) | Neoadjuvant chemotherapy + surgery; Surgery + adjuvant radiotherapy |
| T4 N1 M0 | Inductive chemotherapy + consolidative surgery; chemoradiotherapy | ||
| Any T N2 M0 | N2-Single lymph node > 2 cm but ≤5 cm or multiple lymph node involvement (≤5 cm) | Inductive chemotherapy + consolidative surgery; chemoradiotherapy | |
| Any T Any N M1 | M1-Distant metastases | Systemic therapy |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Virarkar, M.; Vulasala, S.S.; Gopireddy, D.; Morani, A.C.; Daoud, T.; Waters, R.; Bhosale, P. Neuroendocrine Neoplasms of the Female Genitourinary Tract: A Comprehensive Overview. Cancers 2022, 14, 3218. https://doi.org/10.3390/cancers14133218
Virarkar M, Vulasala SS, Gopireddy D, Morani AC, Daoud T, Waters R, Bhosale P. Neuroendocrine Neoplasms of the Female Genitourinary Tract: A Comprehensive Overview. Cancers. 2022; 14(13):3218. https://doi.org/10.3390/cancers14133218
Chicago/Turabian StyleVirarkar, Mayur, Sai Swarupa Vulasala, Dheeraj Gopireddy, Ajaykumar C. Morani, Taher Daoud, Rebecca Waters, and Priya Bhosale. 2022. "Neuroendocrine Neoplasms of the Female Genitourinary Tract: A Comprehensive Overview" Cancers 14, no. 13: 3218. https://doi.org/10.3390/cancers14133218
APA StyleVirarkar, M., Vulasala, S. S., Gopireddy, D., Morani, A. C., Daoud, T., Waters, R., & Bhosale, P. (2022). Neuroendocrine Neoplasms of the Female Genitourinary Tract: A Comprehensive Overview. Cancers, 14(13), 3218. https://doi.org/10.3390/cancers14133218