
NF2 Alteration/22q Loss Is Associated with Recurrence in WHO Grade 1 Sphenoid Wing Meningiomas

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Cohort
2.2. Data Collection
2.3. DNA Extraction and Sanger Sequencing
2.4. Multiplex Ligation-Dependent Probe Amplification (MLPA)
2.5. Statistical Analysis
3. Results
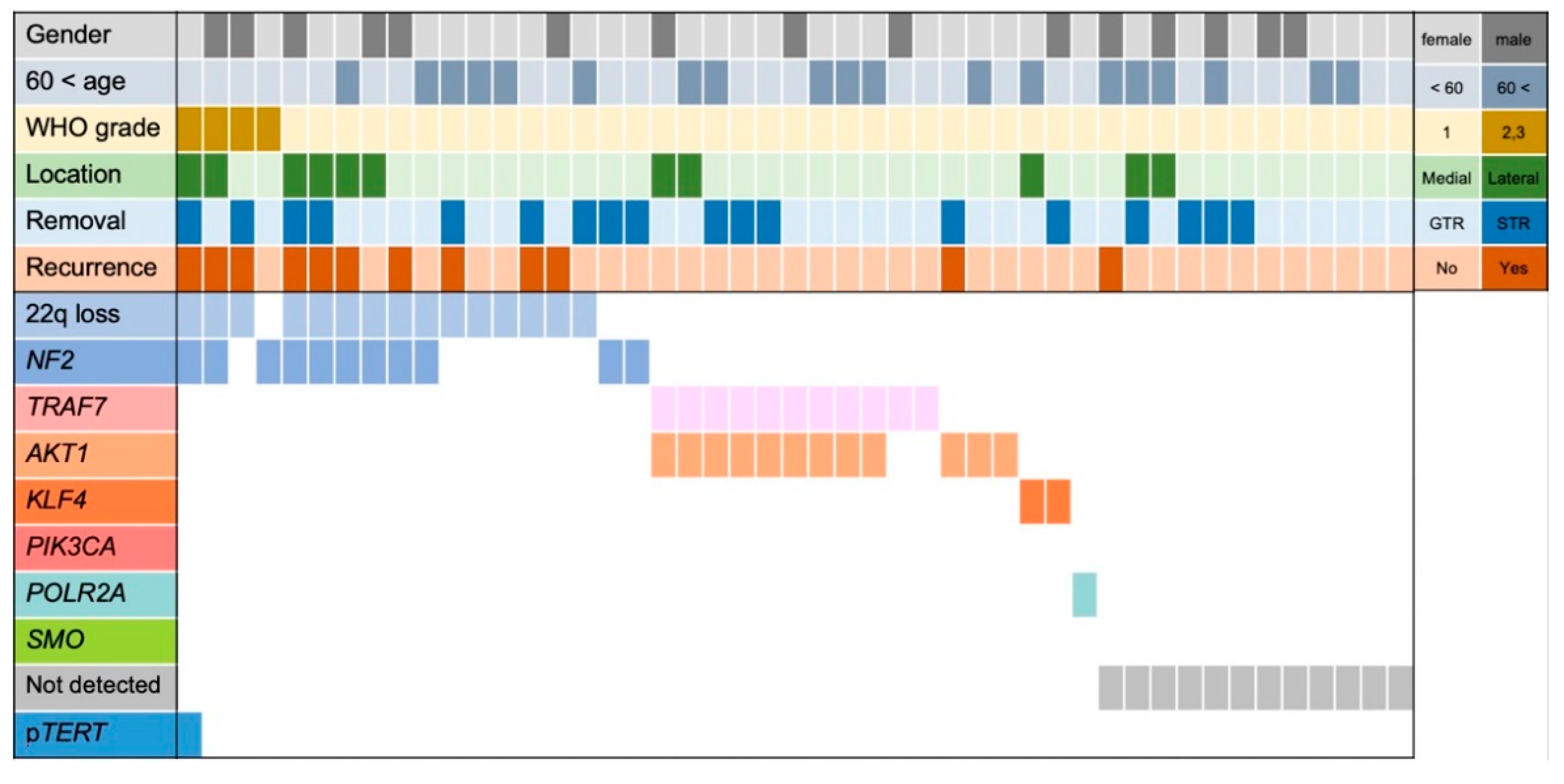
3.1. Tumor Characteristics of This Cohort
3.2. Tumor Characteristics of WHO Grade 1 Meningiomas
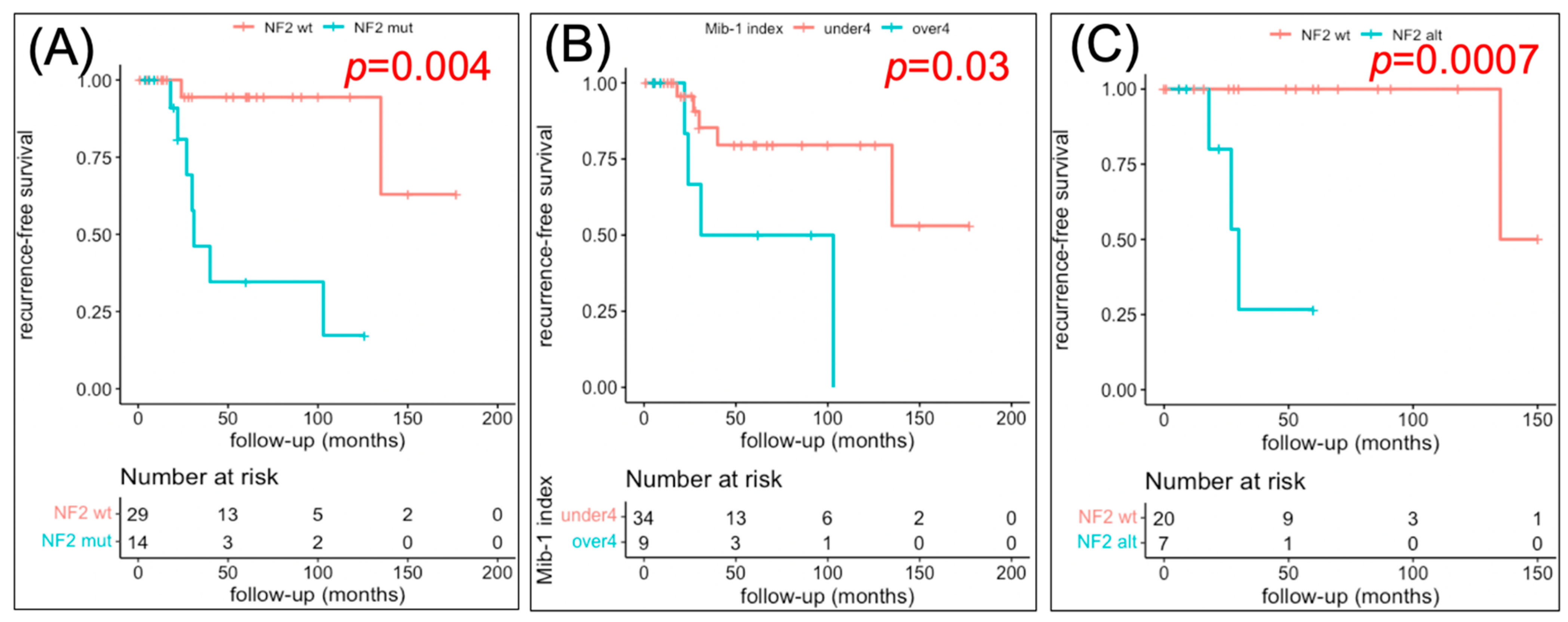
3.3. Factors Related to RFS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Güdük, M.; Özduman, K.; Pamir, M.N. Sphenoid Wing Meningiomas: Surgical Outcomes in a Series of 141 Cases and Proposal of a Scoring System Predicting Extent of Resection. World Neurosurg. 2019, 125, e48–e59. [Google Scholar] [CrossRef] [PubMed]
- Al-Mefty, O. Clinoidal meningiomas. J. Neurosurg. 1990, 73, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Mirimanoff, R.O.; Dosoretz, D.E.; Linggood, R.M.; Ojemann, R.G.; Martuza, R.L. Meningioma: Analysis of recurrence and progression following neurosurgical resection. J. Neurosurg. 1985, 62, 18–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonnal, J.; Thibaut, A.; Brotchi, J.; Born, J. Invading meningiomas of the sphenoid ridge. J. Neurosurg. 1980, 53, 587–599. [Google Scholar] [CrossRef] [Green Version]
- Mathiesen, T.; Lindquist, C.; Kihlström, L.; Karlsson, B. Recurrence of Cranial Base Meningiomas. Neurosurgery 1996, 39, 2–9. [Google Scholar] [CrossRef]
- Nakamura, M.; Roser, F.; Jacobs, C.; Vorkapic, P.; Samii, M. Medial Sphenoid Wing Meningiomas: Clinical Outcome and Recurrence Rate. Neurosurgery 2006, 58, 626–639. [Google Scholar] [CrossRef]
- Kros, J.; de Greve, K.; van Tilborg, A.; Hop, W.; Pieterman, H.; Avezaat, C.; Lekanne Dit Deprez, R.; Zwarthoff, E. NF2 status of meningiomas is associated with tumour localization and histology. J. Pathol. 2001, 194, 367–372. [Google Scholar] [CrossRef]
- Riemenschneider, M.J.; Perry, A.; Reifenberger, G. Histological classification and molecular genetics of meningiomas. Lancet Neurol. 2006, 5, 1045–1054. [Google Scholar] [CrossRef]
- Zang, K.D.; Singer, H. Chromosomal Constitution of Meningiomas. Nature 1967, 216, 84–85. [Google Scholar] [CrossRef]
- Suppiah, S.; Nassiri, F.; Bi, W.L.; Dunn, I.F.; Hanemann, C.O.; Horbinski, C.M.; Hashizume, R.; James, C.D.; Mawrin, C.; Noushmehr, H.; et al. Molecular and translational advances in meningiomas. Neuro-Oncology 2019, 21, i4–i17. [Google Scholar] [CrossRef]
- Clark, V.E.; Erson-Omay, E.Z.; Serin, A.; Yin, J.; Cotney, J.; Özduman, K.; Avşar, T.; Li, J.; Murray, P.B.; Henegariu, O.; et al. Genomic Analysis of Non- NF2 Meningiomas Reveals Mutations in TRAF7, KLF4, AKT1, and SMO. Science 2013, 339, 1077–1080. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reuss, D.E.; Piro, R.M.; Jones, D.T.; Simon, M.; Ketter, R.; Kool, M.; Becker, A.; Sahm, F.; Pusch, S.; Meyer, J.; et al. Secretory meningiomas are defined by combined KLF4 K409Q and TRAF7 mutations. Acta Neuropathol. 2013, 125, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Clark, V.E.; Harmanci, A.S.; Bai, H.; Youngblood, M.W.; Lee, T.I.; Baranoski, J.F.; Ercan-Sencicek, A.G.; Abraham, B.J.; Weintraub, A.S.; Hnisz, D.; et al. Recurrent somatic mutations in POLR2A define a distinct subset of meningiomas. Nat. Genet. 2016, 48, 1253–1259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, J.C.-S.; Chung, N.Y.F.; Chan, N.H.L.; Poon, W.S.; Thomas, T.; Ng, H.-K. Rare mutation of PIK3CA in meningiomas. Acta Neuropathol. 2006, 111, 284–285. [Google Scholar] [CrossRef] [PubMed]
- Sahm, F.; Schrimpf, D.; Olar, A.; Koelsche, C.; Reuss, D.; Bissel, J.; Kratz, A.; Capper, D.; Schefzyk, S.; Hielscher, T.; et al. TERT Promoter Mutations and Risk of Recurrence in Meningioma. J. Natl. Cancer Inst. 2016, 108, djv377. [Google Scholar] [CrossRef]
- WHO Classification of Tumours Editorial Board. World Health Organization Classification of Tumours of the Central Nervous System, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2021. [Google Scholar]
- Sahm, F.; Schrimpf, D.; Stichel, D.; Jones, D.T.W.; Hielscher, T.; Schefzyk, S.; Okonechnikov, K.; Koelsche, C.; Reuss, D.E.; Capper, D.; et al. DNA methylation-based classification and grading system for meningioma: A multicentre, retrospective analysis. Lancet Oncol. 2017, 18, 682–694. [Google Scholar] [CrossRef] [Green Version]
- Nassiri, F.; Liu, J.; Patil, V.; Mamatjan, Y.; Wang, J.Z.; Hugh-White, R.; Macklin, A.M.; Khan, S.; Singh, O.; Karimi, S.; et al. A clinically applicable integrative molecular classification of meningiomas. Nature 2021, 597, 119–125. [Google Scholar] [CrossRef]
- Maas, S. Integrated molecular-morphologic meningiomas classification: A multicenter retrospective analysis, retrospectively and prospetively validated. J. Clin. Oncol. 2021, 39, 3839–3852. [Google Scholar] [CrossRef]
- Nassiri, F.; Mamatjan, Y.; Suppiah, S.; Badhiwala, J.H.; Mansouri, S.; Karimi, S.; Saarela, O.; Poisson, L.M.; Gepfner-Tuma, I.; Schittenhelm, J.; et al. DNA methylation profiling to predict recurrence risk in meningioma: Development and validation of a nomogram to optimize clinical management. Neuro-Oncology 2019, 21, 901–910. [Google Scholar] [CrossRef] [Green Version]
- Paramasivam, N.; Hübschmann, D.; Toprak, U.H.; Ishaque, N.; Neidert, M.; Schrimpf, D.; Stichel, D.; Reuss, D.; Sievers, P.; Reinhardt, A.; et al. Mutational patterns and regulatory networks in epigenetic subgroups of meningioma. Acta Neuropathol. 2019, 138, 295–308. [Google Scholar] [CrossRef]
- Youngblood, M.W.; Miyagishima, D.F.; Jin, L.; Gupte, T.; Li, C.; Duran, D.; Montejo, J.D.; Zhao, A.; Sheth, A.; Tyrtova, E.; et al. Associations of meningioma molecular subgroup and tumor recurrence. Neuro-Oncology 2021, 23, 783–794. [Google Scholar] [CrossRef] [PubMed]
- Cushing, H.W.; Eisenhardt, L. Meningiomas: Their Classification, Regional Behavior Life History, and Surgical End Results; Hafner Publishing Company: New York, NY, USA, 1938; pp. 298–341. [Google Scholar]
- Jin, L.; Youngblood, M.W.; Gupte, T.P.; Vetsa, S.; Nadar, A.; Barak, T.; Yalcin, K.; Aguilera, S.M.; Mishra-Gorur, K.; Blondin, N.A.; et al. Type of bony involvement predicts genomic subgroup in sphenoid wing meningiomas. J. Neuro-Oncol. 2021, 154, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Simpson, D. The Recurrence of Intracranial Meningiomas after Surgical Treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro-Oncology 2021, 23, 1231–1251. [Google Scholar] [CrossRef] [PubMed]
- Oya, S.; Kawai, K.; Nakatomi, H.; Saito, N. Significance of Simpson grading system in modern meningioma surgery: Integration of the grade with MIB-1 labeling index as a key to predict the recurrence of WHO Grade I meningiomas. J. Neurosurg. 2012, 117, 121–128. [Google Scholar] [CrossRef] [Green Version]
- Okano, A.; Miyawaki, S.; Hongo, H.; Dofuku, S.; Teranishi, Y.; Mitsui, J.; Tanaka, M.; Shin, M.; Nakatomi, H.; Saito, N. Associations of pathological diagnosis and genetic abnormalities in meningiomas with the embryological origins of the meninges. Sci. Rep. 2021, 11, 6987. [Google Scholar] [CrossRef]
- Korkolopoulou, P.; Levidou, G.; Trigka, E.-A.; Prekete, N.; Karlou, M.; Thymara, I.; Sakellariou, S.; Fragkou, P.; Isaiadis, D.; Pavlopoulos, P.; et al. A comprehensive immunohistochemical and molecular approach to the PI3K/AKT/mTOR (phosphoinositide 3-kinase/v-akt murine thymoma viral oncogene/mammalian target of rapamycin) pathway in bladder urothelial carcinoma. Br. J. Urol. 2012, 110, E1237–E1248. [Google Scholar] [CrossRef] [Green Version]
- El-Habr, E.; Levidou, G.; Trigka, E.-A.; Sakalidou, J.; Piperi, C.; Chatziandreou, I.; Spyropoulou, A.; Soldatos, R.; Tomara, G.; Petraki, K.; et al. Complex interactions between the components of the PI3K/AKT/mTOR pathway, and with components of MAPK, JAK/STAT and Notch-1 pathways, indicate their involvement in meningioma development. Virchows Arch. 2014, 465, 473–485. [Google Scholar] [CrossRef]
- Chen, H.; Xue, L.; Wang, H.; Wang, Z.; Wu, H. Differential NF2 Gene Status in Sporadic Vestibular Schwannomas and its Prognostic Impact on Tumour Growth Patterns. Sci. Rep. 2017, 7, 5470. [Google Scholar] [CrossRef] [Green Version]
- Domingues, P.H.; Sousa, P.; Otero, A.; Gonçalves, J.M.; Ruiz, L.; De Oliveira, C.; Lopes, M.C.; Orfao, A.; Tabernero, M.D. Proposal for a new risk stratification classification for meningioma based on patient age, WHO tumor grade, size, localization, and karyotype. Neuro-Oncology 2014, 16, 735–747. [Google Scholar] [CrossRef] [Green Version]
- González-Tablas, M.; Prieto, C.; Arandia, D.; Jara-Acevedo, M.; Otero, Á.; Pascual, D.; Ruíz, L.; Álvarez-Twose, I.; García-Montero, A.C.; Orfao, A. Whole-Exome Sequencing Reveals Recurrent but Heterogeneous Mutational Profiles in Sporadic WHO Grade 1 Meningiomas. Front. Oncol. 2021, 11, 740782. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.J.; Wan, Y.W.; Al-Ouran, R.; Revelli, J.P.; Cardenas, M.F.; Oneissi, M.; Xi, L.; Jalali, A.; Magnotti, J.F.; Muzny, D.M.; et al. Molecular profiling predicts meningioma recurrence and reveals loss of DREAM complex repression in aggressive tumors. Proc. Natl. Acad. Sci. USA 2019, 116, 21715–21726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanson, M.; Kalamarides, M. Epigenetics: A new tool for meningioma management? Lancet Oncol. 2017, 18, 569–570. [Google Scholar] [CrossRef]
- Blume, C. Integrated phspho-proteogenomic and single-cell transcriptomic analysis of menigiomas establishes robust subtyping and reveals subtype-specific immune invasion. bioRxiv 2021. [Google Scholar] [CrossRef]
- Choudhury, A.; Magill, S.T.; Eaton, C.D.; Prager, B.C.; Chen, W.C.; Cady, M.A.; Seo, K.; Lucas, C.-H.G.; Casey-Clyde, T.J.; Vasudevan, H.N.; et al. Meningioma DNA methylation groups identify biologic drivers and therapeutic vulnerabilities. Nat Genet. 2022, 54, 649–659. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Variables | WHO Grade 1–3 (47) | WHO Grade 1 (43) | WHO Grade 2/3 (4) |
|---|---|---|---|
| General | |||
| Age (years) | 57 (49–64) | 57 (50–65.5) | 50.5 (48.5–53) |
| Male | 15 (31.9%) | 13 (30.2%) | 2 (50%)) |
| Recurrence | 12 (25.5%) | 9 (20.9%) | 3 (75%) |
| Follow-up months | 27 (12–61.5) | 28 (13–64) | 16 (8.3–26.5) |
| Clinical symptoms | |||
| Eye field symptom | 22 (46.8%) | 19 (44.2%) | 3 (75%) |
| Vision loss | 14 (29.8%) | 12 (27.9%) | 2 (50%) |
| Oculomotor dysfunction | 4 (8.5%) | 3 (7.0%) | 1 (25%) |
| Radiological features | |||
| Medial | 36 (76.6%) | 34 (79.1%) | 2 (50%) |
| Bone invasion | 7 (14.9%) | 4 (9.3%) | 3 (75%) |
| Hyperostosis | 10 (21.3%) | 8 (18.6%) | 2 (50%) |
| Brain edema | 17 (36.2%) | 14 (32.6%) | 3 (75%) |
| CS invasion | 8 (17.0%) | 6 (14.0%) | 2 (50%) |
| Irregular shape | 12 (25.5%) | 9 (20.9%) | 3 (75%) |
| Volume (cm3) | 14.0 (6.0–33.1) | 11.7 (5.8–28.5) | 79.7 (42.8–125.6) |
| Histological analysis | |||
| MIB-1 LI ≧ 4 | 11 (23.4%) | 9 (20.9%) | 2 (50%) |
| Genetic analysis | |||
| NF2 alt./22q loss | 18 (38.3%) | 14 (32.6%) | 4 (100%) |
| Surgery | |||
| GTR | 29 (61.7%) | 27 (62.8%) | 2 (50%) |
| Variables | All (43) | NF2 alt./22q Loss (14) | NF2/22q wt. (29) | p Value |
|---|---|---|---|---|
| General | ||||
| Age (years) | 57 (50–65.5) | 57 (47.8–63.8) | 58 (51–67) | 0.64 |
| Male | 13 (30.2%) | 4 (28.6%)) | 9 (31.0%) | 0.87 |
| Recurrence | 9 (20.9%) | 7 (50%) | 2 (6.9%) | 0.0026 |
| Follow-up months | 30 (14.5–70) | 25 (18.5–37.8) | 30 (13–70) | 0.30 |
| Clinical symptom | ||||
| Eye field symptom | 19 (44.2%) | 7 (50.0%) | 12 (41.4%) | 0.59 |
| Vision loss | 12 (27.9%) | 4 (28.6%) | 8 (27.6%) | 0.95 |
| Oculomotor dysfunction | 3 (7.0%) | 3 (14.3%) | 0 (0%) | 0.030 |
| Radiological features | ||||
| Medial | 34 (79.1%) | 10 (71.4%) | 24 (82.8%) | 0.39 |
| Bone invasion | 4 (9.3%) | 4 (28.6%) | 0 (0%) | 0.008 |
| Hyperostosis | 8 (18.6%) | 4 (28.6%) | 4 (13.8%) | 0.24 |
| Brain edema | 14 (32.6%) | 3 (21.4%) | 11 (37.9%) | 0.28 |
| CS invasion | 6 (14.0%) | 1 (7.1%) | 5 (17.2%) | 0.37 |
| Irregular shape | 9 (20.9%) | 4 (28.6%) | 5 (17.2%) | 0.39 |
| Volume (cm3) | 11.7 (5.8–28.5) | 10.2 (5.2–52.6) | 11.7 (6.9–24.0) | 0.21 |
| Histological analysis | ||||
| MIB-1 LI ≧ 4 | 9 (20.9%) | 4 (28.6%) | 5 (17.2%) | 0.39 |
| Surgery | ||||
| GTR | 27 (62.8%) | 7 (50%) | 20 (69.0%) | 0.23 |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | HR | 95% CI | p Value | |
| NF2/22q loss | 16.8 | 2.1–137.0 | 0.009 | 13.1 | 1.5–111 | 0.019 |
| MIB-1 LI ≥ 4 | 4.2 | 1.05–16.9 | 0.04 | 2.2 | 0.5–9.3 | 0.28 |
| Lateral | 2.3 | 0.5–9.5 | 0.27 | |||
| Male | 2.2 | 0.6–8.8 | 0.25 | |||
| Age < 60 | 2.3 | 0.6–9.5 | 0.23 | 1.6 | 0.4–6.6 | 0.53 |
| STR | 2.0 | 0.5–7.5 | 0.31 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sakai, Y.; Miyawaki, S.; Teranishi, Y.; Okano, A.; Ohara, K.; Hongo, H.; Ishigami, D.; Shimada, D.; Mitsui, J.; Nakatomi, H.; et al. NF2 Alteration/22q Loss Is Associated with Recurrence in WHO Grade 1 Sphenoid Wing Meningiomas. Cancers 2022, 14, 3183. https://doi.org/10.3390/cancers14133183
Sakai Y, Miyawaki S, Teranishi Y, Okano A, Ohara K, Hongo H, Ishigami D, Shimada D, Mitsui J, Nakatomi H, et al. NF2 Alteration/22q Loss Is Associated with Recurrence in WHO Grade 1 Sphenoid Wing Meningiomas. Cancers. 2022; 14(13):3183. https://doi.org/10.3390/cancers14133183
Chicago/Turabian StyleSakai, Yu, Satoru Miyawaki, Yu Teranishi, Atsushi Okano, Kenta Ohara, Hiroki Hongo, Daiichiro Ishigami, Daisuke Shimada, Jun Mitsui, Hirofumi Nakatomi, and et al. 2022. "NF2 Alteration/22q Loss Is Associated with Recurrence in WHO Grade 1 Sphenoid Wing Meningiomas" Cancers 14, no. 13: 3183. https://doi.org/10.3390/cancers14133183
APA StyleSakai, Y., Miyawaki, S., Teranishi, Y., Okano, A., Ohara, K., Hongo, H., Ishigami, D., Shimada, D., Mitsui, J., Nakatomi, H., & Saito, N. (2022). NF2 Alteration/22q Loss Is Associated with Recurrence in WHO Grade 1 Sphenoid Wing Meningiomas. Cancers, 14(13), 3183. https://doi.org/10.3390/cancers14133183