
Immunological Landscape of HER-2 Positive Breast Cancer

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
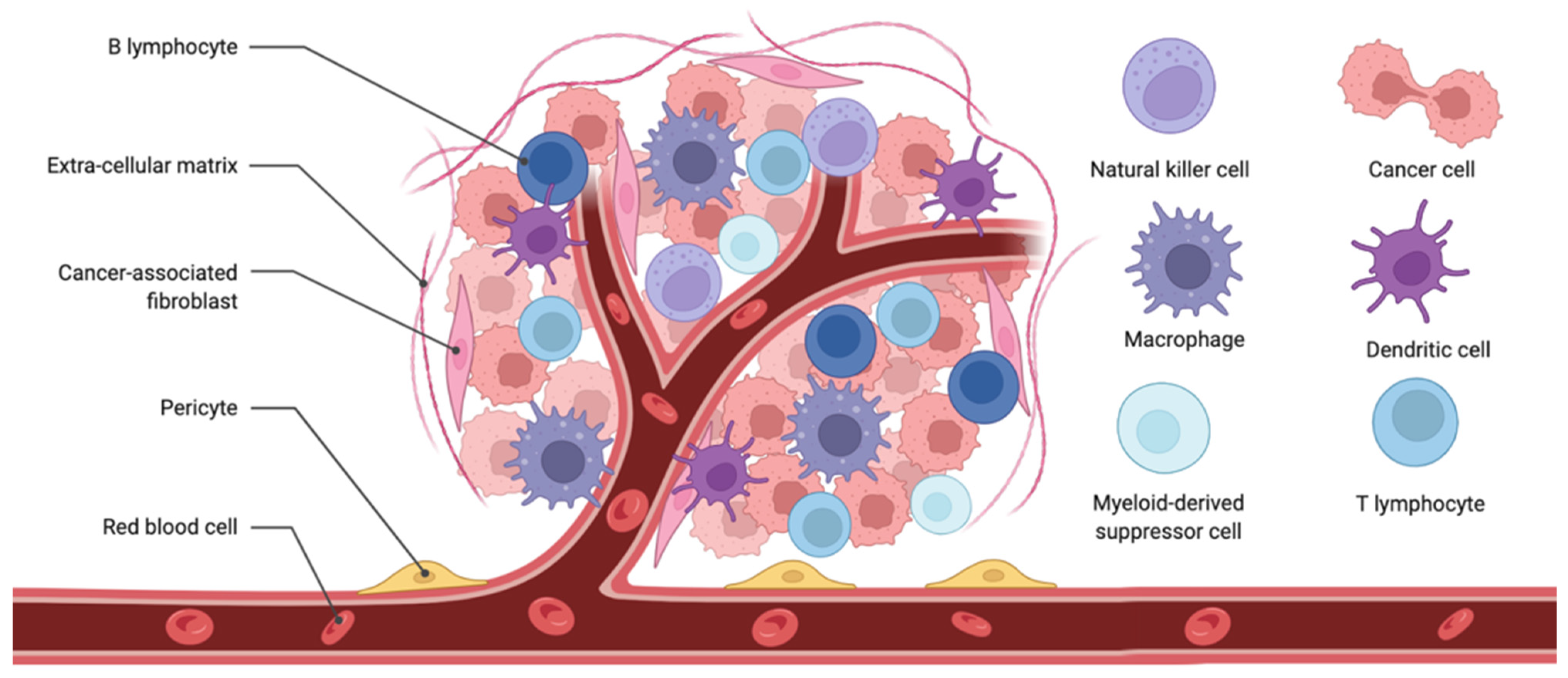
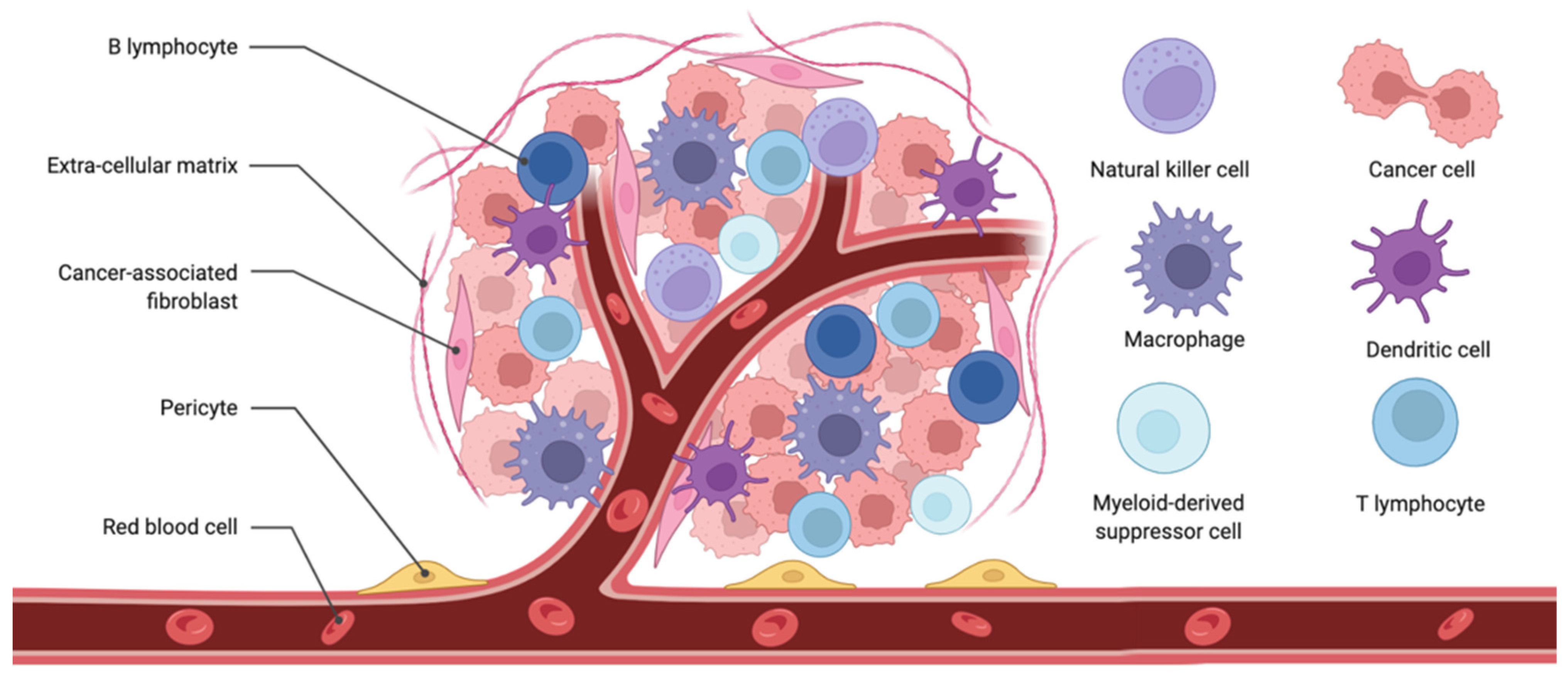
2. Tumour Microenvironment
2.1. Tumour-Infiltrating Lymphocytes
2.2. Tertiary Lymphoid Structures
2.3. Tumour Mutational Burden
2.4. PD-L1 Expression
2.5. Microsatellite Instability
3. Immune-Mediated Effects by HER2- Targeted Therapies
4. Immune Therapies for HER2+ Breast Cancer
4.1. Immune Checkpoint Blockade for HER2+ BC
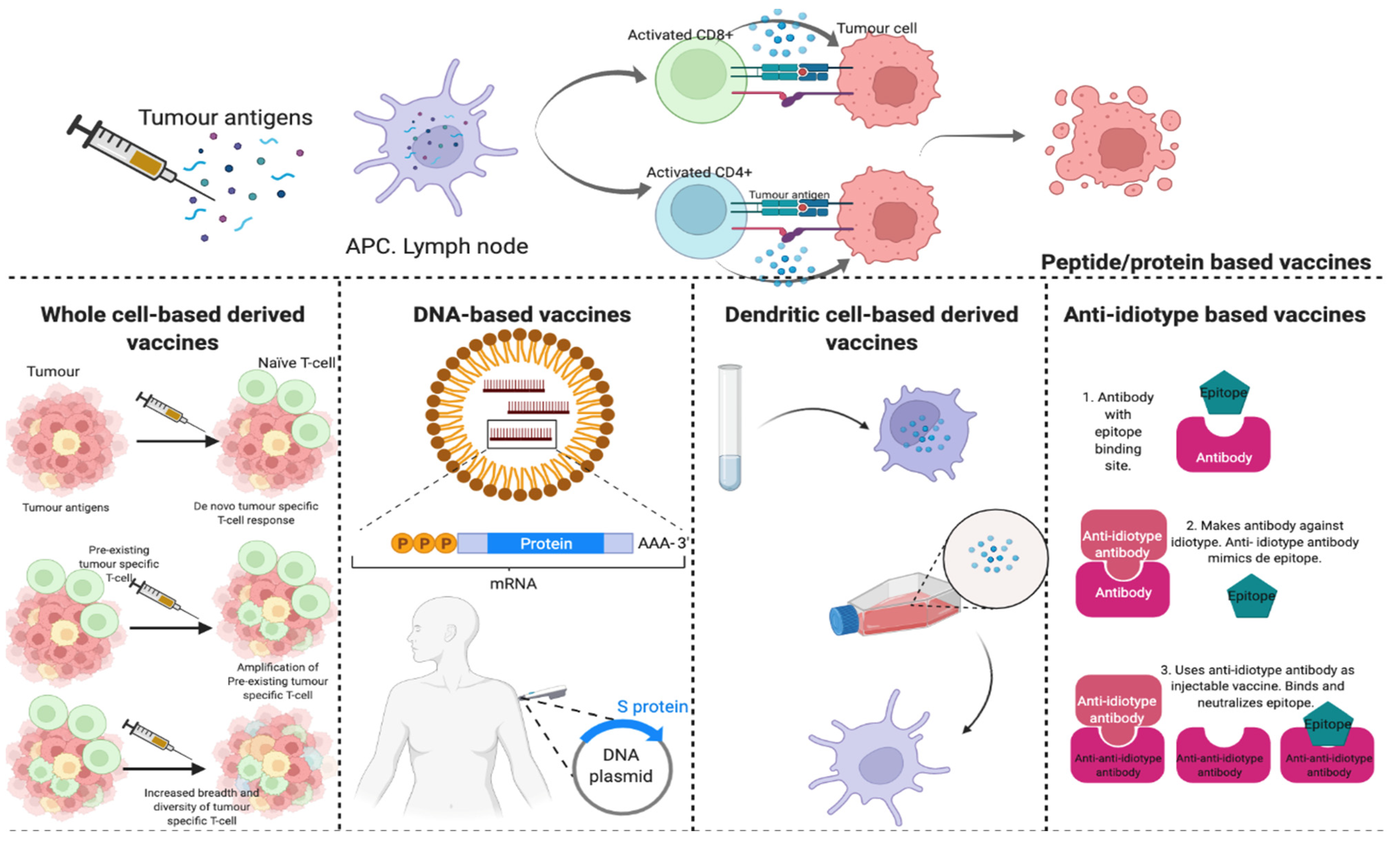
4.2. AntiHER2-Vaccines
4.2.1. HER2-Derived Peptide Vaccines
4.2.2. Protein-Derived Vaccines
4.2.3. Anti-Idiotype Vaccines
4.2.4. DNA-Based Vaccines
4.2.5. Dentritic Cell-Based Vaccines
4.2.6. Whole Cell-Based Derived Vaccines
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Modi, S.; Saura, C.; Yamashita, T.; Park, Y.H.; Kim, S.-B.; Tamura, K.; Andre, F.; Iwata, H.; Ito, Y.; Tsurutani, J.; et al. Trastuzumab Deruxtecan in Previously Treated HER2-Positive Breast Cancer. N. Engl. J. Med. 2020, 382, 610–621. [Google Scholar] [CrossRef]
- Diéras, V.; Miles, D.; Verma, S.; Pegram, M.; Welslau, M.; Baselga, J.; Krop, I.E.; Blackwell, K.; Hoersch, S.; Xu, J.; et al. Trastuzumab emtansine versus capecitabine plus lapatinib in patients with previously treated HER2-positive advanced breast cancer (EMILIA): A descriptive analysis of final overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 732–742. [Google Scholar] [CrossRef]
- Datta, J.; Rosemblit, C.; Berk, E.; Showalter, L.; Namjoshi, P.; Mick, R.; Lee, K.P.; Brod, A.M.; Yang, R.L.; Kelz, R.R.; et al. Progressive loss of anti-HER2 CD4+ T-helper type 1 response in breast tumorigenesis and the potential for immune restoration. OncoImmunology 2015, 4, e1022301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soberino, J.; Racca, F.; Pérez-García, J.; García-Fernández, L.F.; Cortés, J. Immunotherapy for HER2-Positive Breast Cancer: Changing the Paradigm. Curr. Breast Cancer Rep. 2019, 11, 248–258. Available online: https://www.researchgate.net/publication/337232152_Immunotherapy_for_HER2-Positive_Breast_Cancer_Changing_the_Paradigm (accessed on 17 February 2022). [CrossRef]
- Chew, V.; Toh, H.C.; Abastado, J.-P. Immune Microenvironment in Tumor Progression: Characteristics and Challenges for Therapy. J. Oncol. 2012, 2012, 608406. [Google Scholar] [CrossRef] [Green Version]
- De Melo Gagliato, D.; Cortes, J.; Curigliano, G.; Loi, S.; Denkert, C.; Perez-Garcia, J.; Holgado, E. Tumor-infiltrating lymphocytes in Breast Cancer and implications for clinical practice. Biochim. Biophys. Acta-Rev. Cancer 2017, 1868, 527–537. [Google Scholar] [CrossRef]
- Pallerla, S.; Abdul, A.; Comeau, J.; Jois, S. Cancer Vaccines, Treatment of the Future: With Emphasis on HER2-Positive Breast Cancer. Int. J. Mol. Sci. 2021, 22, 779. [Google Scholar] [CrossRef]
- Costa, R.L.B.; Czerniecki, B.J. Clinical development of immunotherapies for HER2+ breast cancer: A review of HER2-directed monoclonal antibodies and beyond. NPJ Breast Cancer 2020, 6, 10. Available online: https://pubmed.ncbi.nlm.nih.gov/32195333/ (accessed on 6 October 2021). [CrossRef] [Green Version]
- Chen, K.; Lu, P.; Beeraka, N.M.; Sukocheva, O.A.; Madhunapantula, S.V.; Liu, J.; Sinelnikov, M.Y.; Nikolenko, V.N.; Bulygin, K.V.; Mikhaleva, L.M.; et al. Mitochondrial mutations and mitoepigenetics: Focus on regulation of oxidative stress-induced responses in breast cancers. Semin. Cancer Biol. 2020, in press. [CrossRef]
- Chen, K.; Zhang, J.; Beeraka, N.M.; Tang, C.; Babayeva, Y.; Sinelnikov, M.Y.; Zhang, X.; Zhang, J.; Liu, J.; Reshetov, I.V.; et al. Advances in prevention and treatment of obesity-driven effects in breast cancers. Front. Oncol. 2022, 2663. [Google Scholar] [CrossRef]
- Anderson, N.M.; Simon, M.C. The tumor microenvironment. Curr. Biol. 2020, 30, R921–R925. Available online: https://pubmed.ncbi.nlm.nih.gov/32810447/ (accessed on 23 February 2022). [CrossRef] [PubMed]
- Ayoub, N.M.; Al-Shami, K.M.; Yaghan, R.J. Immunotherapy for HER2-Positive Breast Cancer: Recent Advances and Combination Therapeutic Approaches. Breast Cancer Targets Ther. 2019, 11, 53–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, S.; Wang, B.; Wang, Z.; He, J.; Ma, X. Common Multiple Primary Cancers Associated With Breast and Gynecologic Cancers and Their Risk Factors, Pathogenesis, Treatment and Prognosis: A Review. Front. Oncol. 2022, 12, 2681. [Google Scholar] [CrossRef]
- Tan, T.J.; Chan, J.J.; Kamis, S.; Dent, R.A. What is the role of immunotherapy in breast cancer? Chin. Clin. Oncol. 2018, 7, 13. [Google Scholar] [CrossRef]
- Wang, M.; Zhao, J.; Zhang, L.; Wei, F.; Lian, Y.; Wu, Y.; Gong, Z.; Zhang, S.; Zhou, J.; Cao, K.; et al. Role of tumor microenvironment in tumorigenesis. J. Cancer 2017, 8, 761–773. Available online: https://pubmed.ncbi.nlm.nih.gov/28382138/ (accessed on 23 February 2022). [CrossRef] [PubMed]
- Triulzi, T.; Forte, L.; Regondi, V.; Di Modica, M.; Ghirelli, C.; Carcangiu, M.L.; Sfondrini, L.; Balsari, A.; Tagliabue, E. HER2 signaling regulates the tumor immune microenvironment and trastuzumab efficacy. OncoImmunology 2018, 8, e1512942. [Google Scholar] [CrossRef] [PubMed]
- Zhai, L.; Spranger, S.; Binder, D.C.; Gritsina, G.; Lauing, K.L.; Giles, F.J.; Wainwright, D.A. Molecular Pathways: Targeting IDO1 and Other Tryptophan Dioxygenases for Cancer Immunotherapy. Clin. Cancer Res. 2015, 21, 5427–5433. Available online: https://pubmed.ncbi.nlm.nih.gov/26519060/ (accessed on 21 December 2021). [CrossRef] [Green Version]
- Soliman, H.; Rawal, B.; Fulp, J.; Lee, J.H.; Lopez, A.; Bui, M.M.; Khalil, F.; Antonia, S.; Yfantis, H.G.; Lee, D.H.; et al. Analysis of indoleamine 2-3 dioxygenase (IDO1) expression in breast cancer tissue by immunohistochemistry. Cancer Immunol. Immunother. 2013, 62, 829–837. [Google Scholar] [CrossRef]
- Le Naour, J.; Galluzzi, L.; Zitvogel, L.; Kroemer, G.; Vacchelli, E. Trial watch: IDO inhibitors in cancer therapy. Oncoimmunology 2020, 9, 1777625. Available online: https://pubmed.ncbi.nlm.nih.gov/32934882/ (accessed on 23 February 2022). [CrossRef]
- A Phase 1 Study of Peptide Vaccination for the Treatment of Patients with Solid Tumors Moderately Expressing HER2/Neu. Available online: https://clinicaltrials.gov/ct2/show/NCT02276300 (accessed on 23 February 2022).
- Kruse, M.; Abraham, J. Breast Cancer. In Immune Checkpoint Inhibitors in Cancer; Ito, F., Ernstoff, M.S., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 157–167. Available online: https://linkinghub.elsevier.com/retrieve/pii/B9780323549486000081 (accessed on 23 February 2022).
- Purmonen, T.T.; Pänkäläinen, E.; Turunen, J.; Asseburg, C.; Martikainen, J.A. Short-course adjuvant trastuzumab therapy in early stage breast cancer in Finland: Cost-effectiveness and value of information analysis based on the 5-year follow-up results of the FinHer Trial. Acta Oncol. 2011, 50, 344–352. Available online: https://pubmed.ncbi.nlm.nih.gov/21299447/ (accessed on 3 March 2022). [CrossRef] [Green Version]
- Loi, S.; Michiels, S.; Salgado, R.; Sirtaine, N.; Jose, V.; Fumagalli, D.; Kellokumpu-Lehtinen, P.-L.; Bono, P.; Kataja, V.; Desmedt, C.; et al. Tumor infiltrating lymphocytes are prognostic in triple negative breast cancer and predictive for trastuzumab benefit in early breast cancer: Results from the FinHER trial. Ann. Oncol. 2014, 25, 1544–1550. Available online: http://www.annalsofoncology.org/article/S0923753419348070/fulltext (accessed on 3 March 2022). [CrossRef] [PubMed]
- Romond, E.H.; Perez, E.A.; Bryant, J.; Suman, V.J.; Geyer, C.E., Jr.; Davidson, N.E.; Tan-Chiu, E.; Martino, S.; Paik, S.; Kaufman, P.A.; et al. Trastuzumab plus Adjuvant Chemotherapy for Operable HER2-Positive Breast Cancer. N. Engl. J. Med. 2005, 353, 1673–1684. Available online: https://www.nejm.org/doi/full/10.1056/nejmoa052122 (accessed on 3 March 2022). [CrossRef] [PubMed] [Green Version]
- Kim, S.-R.; Gavin, P.G.; Pogue-Geile, K.L.; Song, N.; Finnigan, M.; Bandos, H.; Jeong, J.-H.; Rastogi, P.; Romond, E.H.; Fehrenbacher, L.; et al. Abstract 2837: A surrogate gene expression signature of tumor infiltrating lymphocytes (TILs) predicts degree of benefit from trastuzumab added to standard adjuvant chemotherapy in NSABP (NRG) trial B-31 for HER2+ breast cancer. Cancer Res. 2015, 75, 2837. Available online: https://aacrjournals.org/cancerres/article/75/15_Supplement/2837/601684/Abstract-2837-A-surrogate-gene-expression (accessed on 3 March 2022). [CrossRef]
- Perez, E.A.; Thompson, E.A.; Ballman, K.V.; Anderson, S.K.; Asmann, Y.W.; Kalari, K.; Eckel-Passow, J.E.; Dueck, A.C.; Tenner, K.S.; Jen, J.; et al. Genomic Analysis Reveals That Immune Function Genes Are Strongly Linked to Clinical Outcome in the North Central Cancer Treatment Group N9831 Adjuvant Trastuzumab Trial. J. Clin. Oncol. 2015, 33, 701–708. [Google Scholar] [CrossRef] [PubMed]
- Von Minckwitz, G.; Procter, M.; de Azambuja, E.; Zardavas, D.; Benyunes, M.; Viale, G.; Suter, T.; Arahmani, A.; Rouchet, N.; Clark, E.; et al. Adjuvant Pertuzumab and Trastuzumab in Early HER2-Positive Breast Cancer. N. Engl. J. Med. 2017, 377, 122–131. Available online: https://www.nejm.org/doi/full/10.1056/nejmoa1703643 (accessed on 3 March 2022). [CrossRef]
- Krop, I.E.; Paulson, J.; Campbell, C.; Kiermaier, A.C.; Andre, F.; Fumagalli, D.; De Haas, S.; Salgado, R.; Denkert, C.; Loibl, S.; et al. Genomic correlates of response to adjuvant trastuzumab (H) and pertuzumab (P) in HER2+ breast cancer (BC): Biomarker analysis of the APHINITY trial. J. Clin. Oncol. 2019, 37, 1012. [Google Scholar] [CrossRef]
- De Azambuja, E.; Holmes, A.P.; Piccart-Gebhart, M.; Holmes, E.; Di Cosimo, S.; Swaby, R.F.; Untch, M.; Jackisch, C.; Lang, I.; Smith, I.; et al. Lapatinib with trastuzumab for HER2-positive early breast cancer (NeoALTTO): Survival outcomes of a randomised, open-label, multicentre, phase 3 trial and their association with pathological complete response. Lancet Oncol. 2014, 15, 1137–1146. Available online: http://www.thelancet.com/article/S1470204514703201/fulltext (accessed on 3 March 2022). [CrossRef] [Green Version]
- Salgado, R.; Denkert, C.; Campbell, C.; Savas, P.; Nuciforo, P.; Aura, C.; De Azambuja, E.; Eidtmann, H.; Ellis, C.E.; Baselga, J.; et al. Tumor-Infiltrating Lymphocytes and Associations with Pathological Complete Response and Event-Free Survival in HER2-Positive Early-Stage Breast Cancer Treated with Lapatinib and Trastuzumab: A Secondary Analysis of the NeoALTTO Trial. JAMA Oncol. 2015, 1, 448–455. Available online: https://jamanetwork.com/journals/jamaoncology/fullarticle/2279849 (accessed on 3 March 2022). [CrossRef] [PubMed]
- Llombart-Cussac, A.; Cortes, J.; Pare, L.; Galván, P.; Bermejo, B.; Martínez, N.; Vidal, M.; Pernas, S.; López, R.L.; Munoz, M.; et al. HER2-enriched subtype as a predictor of pathological complete response following trastuzumab and lapatinib without chemotherapy in early-stage HER2-positive breast cancer (PAMELA): An open-label, single-group, multicentre, phase 2 trial. Lancet Oncol. 2017, 18, 545–554. Available online: https://pubmed.ncbi.nlm.nih.gov/28238593/ (accessed on 1 March 2022). [CrossRef]
- Nuciforo, P.; Pascual, T.; Cortés, J.; Llombart-Cussac, A.; Fasani, R.; Pare, L.; Oliveira, M.; Galvan, P.; Martínez, N.; Bermejo, B.; et al. A predictive model of pathologic response based on tumor cellularity and tumor-infiltrating lymphocytes (CelTIL) in HER2-positive breast cancer treated with chemo-free dual HER2 blockade. Ann. Oncol. 2017, 29, 170–177. Available online: https://pubmed.ncbi.nlm.nih.gov/29045543/ (accessed on 1 March 2022). [CrossRef]
- Guarneri, V.; Frassoldati, A.; Bottini, A.; Cagossi, K.; Bisagni, G.; Sarti, S.; Ravaioli, A.; Cavanna, L.; Giardina, G.; Musolino, A.; et al. Preoperative chemotherapy plus trastuzumab, lapatinib, or both in human epidermal growth factor receptor 2-positive operable breast cancer: Results of the randomized phase II CHER-LOB study. J. Clin. Oncol. 2012, 30, 1989–1995. Available online: https://pubmed.ncbi.nlm.nih.gov/22493419/ (accessed on 3 March 2022). [CrossRef]
- Dieci, M.V.; Bisagni, G.; Cagossi, K.; Bottini, A.; Sarti, S.; Piacentini, F.; Conte, P.; Guarneri, V. Abstract PD1-1: Tumor infiltrating lymphocytes and correlation with outcome in the Cher-LOB study. Cancer Res. 2015, 75, PD1-1. Available online: https://aacrjournals.org/cancerres/article/75/9_Supplement/PD1-1/607832/Abstract-PD1-1-Tumor-infiltrating-lymphocytes-and (accessed on 3 March 2022). [CrossRef]
- Von Minckwitz, G.; Schneeweiss, A.; Loibl, S.; Salat, C.; Denkert, C.; Rezai, M.; Blohmer, J.U.; Jackisch, C.; Paepke, S.; Gerber, B.; et al. Neoadjuvant carboplatin in patients with triple-negative and HER2-positive early breast cancer (GeparSixto; GBG 66): A randomised phase 2 trial. Lancet Oncol. 2014, 15, 747–756. Available online: https://pubmed.ncbi.nlm.nih.gov/24794243/ (accessed on 3 March 2022).
- Denkert, C.; Von Minckwitz, G.; Brase, J.C.; Sinn, B.V.; Gade, S.; Kronenwett, R.; Pfitzner, B.M.; Salat, C.; Loi, S.; Schmitt, W.; et al. Tumor-Infiltrating Lymphocytes and Response to Neoadjuvant Chemotherapy With or Without Carboplatin in Human Epidermal Growth Factor Receptor 2–Positive and Triple-Negative Primary Breast Cancers. J. Clin. Oncol. 2015, 33, 983–991. [Google Scholar] [CrossRef]
- Gianni, L.; Pienkowski, T.; Im, Y.-H.; Roman, L.; Tseng, L.-M.; Liu, M.-C.; Lluch, A.; Staroslawska, E.; De La Haba-Rodriguez, J.; Im, S.-A.; et al. Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): A randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012, 13, 25–32. Available online: http://www.thelancet.com/article/S1470204511703369/fulltext (accessed on 3 March 2022). [CrossRef]
- Bianchini, G.; Pusztai, L.; Pienkowski, T.; Im, Y.-H.; Bianchi, G.V.; Tseng, L.-M.; Liu, M.-C.; Lluch, A.; Galeota, E.; Magazzù, D.; et al. Immune modulation of pathologic complete response after neoadjuvant HER2-directed therapies in the NeoSphere trial. Ann. Oncol. 2015, 26, 2429–2436. Available online: http://www.annalsofoncology.org/article/S0923753419357266/fulltext (accessed on 3 March 2022). [CrossRef] [PubMed]
- Tokunaga, E.; Masuda, N.; Yamamoto, N.; Iwata, H.; Bando, H.; Aruga, T.; Ohtani, S.; Fujisawa, T.; Takano, T.; Inoue, K.; et al. Long-Term Outcomes of a Randomized Study of Neoadjuvant Induction Dual HER2 Blockade with Trastuzumab and Lapatinib Followed by Weekly Paclitaxel Plus Dual HER2 Blockade for HER2-Positive Primary Breast Cancer (Neo-Lath Study). Cancers 2021, 13, 4008. [Google Scholar] [CrossRef] [PubMed]
- Tokunaga, E.; Masuda, N.; Yamamoto, N.; Iwata, H.; Bando, H.; Aruga, T.; Ohtani, S.; Fujisawa, T.; Takano, T.; Inoue, K.; et al. Analysis of tumor infiltrating lymphocytes in HER2-positive primary breast cancer treated with neoadjuvant lapatinib and trastuzumab: The NeoLath study (JBCRG-16). J. Clin. Oncol. 2016, 34, 599. [Google Scholar] [CrossRef]
- Solinas, C.; Ceppi, M.; Lambertini, M.; Scartozzi, M.; Garaud, S.; Fumagalli, D.; De Azambuja, E.; Salgado, R.; Willard-Gallo, K.; Ignatiadis, M. Tumor infiltrating lymphocytes in HER2-positive breast cancer patients treated with neoadjuvant chemotherapy plus trastuzumab, lapatinib or their combination: A meta-analysis of published randomized clinical trials. Ann. Oncol. 2017, 28, i11. Available online: http://www.annalsofoncology.org/article/S0923753419324652/fulltext (accessed on 3 March 2022). [CrossRef]
- Swain, S.M.; Miles, D.; Kim, S.-B.; Im, Y.-H.; Im, S.-A.; Semiglazov, V.; Ciruelos, E.; Schneeweiss, A.; Loi, S.; Monturus, E.; et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): End-of-study results from a double-blind, randomised, placebo-controlled, phase 3 study. Lancet Oncol. 2020, 21, 519–530. Available online: https://pubmed.ncbi.nlm.nih.gov/32171426/ (accessed on 21 December 2021). [CrossRef]
- Luen, S.J.; Salgado, R.; Fox, S.; Savas, P.; Eng-Wong, J.; Clark, E.; Kiermaier, A.; Swain, S.; Baselga, J.; Michiels, S.; et al. Tumour-infiltrating lymphocytes in advanced HER2-positive breast cancer treated with pertuzumab or placebo in addition to trastuzumab and docetaxel: A retrospective analysis of the CLEOPATRA study. Lancet Oncol. 2016, 18, 52–62. Available online: http://www.thelancet.com/article/S1470204516306313/fulltext (accessed on 4 March 2022). [CrossRef] [Green Version]
- Gelmon, K.A.; Boyle, F.M.; Kaufman, B.; Huntsman, D.G.; Manikhas, A.; Di Leo, A.; Martin, M.; Schwartzberg, L.S.; Lemieux, J.; Aparicio, S.; et al. Lapatinib or Trastuzumab Plus Taxane Therapy for Human Epidermal Growth Factor Receptor 2–Positive Advanced Breast Cancer: Final Results of NCIC CTG MA.31. J. Clin. Oncol. 2015, 33, 1574–1583. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Chen, B.; Burugu, S.; Leung, S.; Gao, N.; Virk, S.; Kos, Z.; Parulekar, W.R.; Shepherd, L.; Gelmon, K.A.; et al. Role of Cytotoxic Tumor-Infiltrating Lymphocytes in Predicting Outcomes in Metastatic HER2-Positive Breast Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2017, 3, e172085. Available online: https://pubmed.ncbi.nlm.nih.gov/28750133/ (accessed on 1 March 2022). [CrossRef]
- Emens, L.A.; Esteva, F.J.; Beresford, M.; Saura, C.; De Laurentiis, M.; Kim, S.-B.; Im, S.-A.; Wang, Y.; Salgado, R.; Mani, A.; et al. Trastuzumab emtansine plus atezolizumab versus trastuzumab emtansine plus placebo in previously treated, HER2-positive advanced breast cancer (KATE2): A phase 2, multicentre, randomised, double-blind trial. Lancet Oncol. 2020, 21, 1283–1295. Available online: http://www.thelancet.com/article/S1470204520304654/fulltext (accessed on 17 February 2022). [CrossRef]
- Loi, S.; Giobbie-Hurder, A.; Gombos, A.; Bachelot, T.; Hui, R.; Curigliano, G.; Campone, M.; Biganzoli, L.; Bonnefoi, H.; Jerusalem, G.; et al. Pembrolizumab plus trastuzumab in trastuzumab-resistant, advanced, HER2-positive breast cancer (PANACEA): A single-arm, multicentre, phase 1b–2 trial. Lancet Oncol. 2019, 20, 371–382. Available online: http://www.thelancet.com/article/S147020451830812X/fulltext (accessed on 12 December 2021). [CrossRef]
- Loi, S.; Michiels, S.; Adams, S.; Loibl, S.; Budczies, J.; Denkert, C.; Salgado, R. The journey of tumor-infiltrating lymphocytes as a biomarker in breast cancer: Clinical utility in an era of checkpoint inhibition. Ann. Oncol. 2021, 32, 1236–1244. Available online: http://www.annalsofoncology.org/article/S0923753421021852/fulltext (accessed on 12 December 2021). [CrossRef]
- Dieci, M.; Conte, P.; Bisagni, G.; Brandes, A.; Frassoldati, A.; Cavanna, L.; Musolino, A.; Giotta, F.; Rimanti, A.; Garrone, O.; et al. Association of tumor-infiltrating lymphocytes with distant disease-free survival in the ShortHER randomized adjuvant trial for patients with early HER2+ breast cancer. Ann. Oncol. 2019, 30, 418–423. Available online: https://pubmed.ncbi.nlm.nih.gov/30657852/ (accessed on 12 December 2021). [CrossRef]
- Loi, S.; Sirtaine, N.; Piette, F.; Salgado, R.; Viale, G.; Van Eenoo, F.; Rouas, G.; Francis, P.; Crown, J.P.; Hitre, E.; et al. Prognostic and Predictive Value of Tumor-Infiltrating Lymphocytes in a Phase III Randomized Adjuvant Breast Cancer Trial in Node-Positive Breast Cancer Comparing the Addition of Docetaxel to Doxorubicin With Doxorubicin-Based Chemotherapy: BIG 02-98. J. Clin. Oncol. 2013, 31, 860–867. Available online: https://pubmed.ncbi.nlm.nih.gov/23341518/ (accessed on 28 December 2021). [CrossRef]
- Sautès-Fridman, C.; Petitprez, F.; Calderaro, J.; Fridman, W.H. Tertiary lymphoid structures in the era of cancer immunotherapy. Nat. Cancer 2019, 19, 307–325. Available online: https://pubmed.ncbi.nlm.nih.gov/31092904/ (accessed on 8 December 2021). [CrossRef]
- Gambardella, V.; Martínez-Ciarpaglini, C.; Fleitas, T.; Cervantes, A. In the literature: October 2021. ESMO Open 2021, 6, 100285. Available online: http://www.esmoopen.com/article/S2059702921002477/fulltext (accessed on 8 December 2021).
- Vanhersecke, L.; Brunet, M.; Guégan, J.-P.; Rey, C.; Bougouin, A.; Cousin, S.; Le Moulec, S.; Besse, B.; Loriot, Y.; Larroquette, M.; et al. Mature tertiary lymphoid structures predict immune checkpoint inhibitor efficacy in solid tumors independently of PD-L1 expression. Nat. Cancer 2021, 2, 794–802. Available online: https://www.nature.com/articles/s43018-021-00232-6 (accessed on 8 December 2021). [CrossRef]
- Prabhakaran, S.; Rizk, V.T.; Ma, Z.; Cheng, C.-H.; Berglund, A.E.; Coppola, D.; Khalil, F.; Mulé, J.J.; Soliman, H.H. Evaluation of invasive breast cancer samples using a 12-chemokine gene expression score: Correlation with clinical outcomes. Breast Cancer Res. 2017, 19, 71. Available online: https://pubmed.ncbi.nlm.nih.gov/28629479/ (accessed on 8 December 2021). [CrossRef] [Green Version]
- Liu, X.; Tsang, J.Y.; Hlaing, T.; Hu, J.; Ni, Y.-B.; Chan, S.K.; Cheung, S.Y.; Tse, G.M. Distinct Tertiary Lymphoid Structure Associations and Their Prognostic Relevance in HER2 Positive and Negative Breast Cancers. Oncologist 2017, 22, 1316–1324. Available online: https://pubmed.ncbi.nlm.nih.gov/28701569/ (accessed on 8 December 2021). [CrossRef] [PubMed] [Green Version]
- Zhang, N.-N.; Qu, F.-J.; Liu, H.; Li, Z.-J.; Zhang, Y.-C.; Han, X.; Zhu, Z.-Y.; Lv, Y. Prognostic impact of tertiary lymphoid structures in breast cancer prognosis: A systematic review and meta-analysis. Cancer Cell Int. 2021, 21, 536. Available online: https://cancerci.biomedcentral.com/articles/10.1186/s12935-021-02242-x (accessed on 8 December 2021). [CrossRef] [PubMed]
- Valero, C.; Lee, M.; Hoen, D.; Wang, J.; Nadeem, Z.; Patel, N.; Postow, M.A.; Shoushtari, A.N.; Plitas, G.; Balachandran, V.P.; et al. The association between tumor mutational burden and prognosis is dependent on treatment context. Nat. Genet. 2021, 53, 11–15. Available online: https://www.nature.com/articles/s41588-020-00752-4 (accessed on 29 September 2021). [CrossRef] [PubMed]
- O’Meara, T.A.; Tolaney, S.M. Tumor mutational burden as a predictor of immunotherapy response in breast cancer. Oncotarget 2021, 12, 394–400. Available online: https://pubmed.ncbi.nlm.nih.gov/33747355/ (accessed on 23 February 2022). [CrossRef]
- Xu, J.; Bao, H.; Wu, X.; Wang, X.; Shao, Y.W.; Sun, T. Elevated tumor mutation burden and immunogenic activity in patients with hormone receptor-negative or human epidermal growth factor receptor 2-positive breast cancer. Oncol. Lett. 2019, 18, 449–455. Available online: https://pubmed.ncbi.nlm.nih.gov/31289516/ (accessed on 5 October 2021). [CrossRef] [Green Version]
- Park, S.E.; Park, K.; Lee, E.; Kim, J.-Y.; Ahn, J.S.; Im, Y.-H.; Lee, C.; Jung, H.; Cho, S.Y.; Park, W.-Y.; et al. Clinical implication of tumor mutational burden in patients with HER2-positive refractory metastatic breast cancer. OncoImmunology 2018, 7, e1466768-23. [Google Scholar] [CrossRef]
- Reck, M.; Rodríguez-Abreu, D.; Robinson, A.G.; Hui, R.; Csőszi, T.; Fülöp, A.; Gottfried, M.; Peled, N.; Tafreshi, A.; Cuffe, S.; et al. Pembrolizumab versus Chemotherapy for PD-L1–Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2016, 375, 1823–1833. Available online: https://www.nejm.org/doi/full/10.1056/nejmoa1606774 (accessed on 21 October 2021). [CrossRef] [Green Version]
- van der Heijden, M.S.; Loriot, Y.; Durán, I.; Ravaud, A.; Retz, M.; Vogelzang, N.J.; Nelson, B.; Wang, J.; Shen, X.; Powles, T. Atezolizumab Versus Chemotherapy in Patients with Platinum-treated Locally Advanced or Metastatic Urothelial Carcinoma: A Long-term Overall Survival and Safety Update from the Phase 3 IMvigor211 Clinical Trial. Eur. Urol. 2021, 80, 7–11. [Google Scholar] [CrossRef]
- Bertucci, F.; Gonçalves, A. Immunotherapy in Breast Cancer: The Emerging Role of PD-1 and PD-L1. Curr. Oncol. Rep. 2017, 19, 64. Available online: https://pubmed.ncbi.nlm.nih.gov/28799073/ (accessed on 21 October 2021). [CrossRef]
- Hou, Y.; Nitta, H.; Wei, L.; Banks, P.M.; Lustberg, M.; Wesolowski, R.; Ramaswamy, B.; Parwani, A.V.; Li, Z. PD-L1 expression and CD8-positive T cells are associated with favorable survival in HER2-positive invasive breast cancer. Breast J. 2018, 24, 911–919. Available online: https://pubmed.ncbi.nlm.nih.gov/30230111/ (accessed on 21 October 2021). [CrossRef]
- Gennari, A.; André, F.; Barrios, C.; Cortés, J.; de Azambuja, E.; DeMichele, A.; Dent, R.; Fenlon, D.; Gligorov, J.; Hurvitz, S.; et al. ESMO Clinical Practice Guideline for the diagnosis, staging and treatment of patients with metastatic breast cancer. Ann. Oncol. 2021, 32, 1475–1495. [Google Scholar] [CrossRef] [PubMed]
- Weis, L.N.; Tolaney, S.M.; Barrios, C.H.; Barroso-Sousa, R. Tissue-agnostic drug approvals: How does this apply to patients with breast cancer? NPJ Breast Cancer 2021, 7, 120. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.S.; Leung, S.C.Y.; Gao, D.; Burugu, S.; Anurag, M.; Ellis, M.J.; Nielsen, T.O. Mismatch repair protein loss in breast cancer: Clinicopathological associations in a large British Columbia cohort. Breast Cancer Res. Treat. 2019, 179, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccart-Gebhart, M.J.; Procter, M.; Leyland-Jones, B.; Goldhirsch, A.; Untch, M.; Smith, I.; Gianni, L.; Baselga, J.; Bell, R.H.; Jackisch, C.; et al. Trastuzumab after Adjuvant Chemotherapy in HER2-Positive Breast Cancer. N. Engl. J. Med. 2005, 353, 1659–1672. Available online: https://www.nejm.org/doi/full/10.1056/nejmoa052306 (accessed on 26 February 2022). [CrossRef] [PubMed] [Green Version]
- Valabrega, G.; Montemurro, F.; Aglietta, M. Trastuzumab: Mechanism of action, resistance and future perspectives in HER2-overexpressing breast cancer. Ann. Oncol. 2007, 18, 977–984. Available online: https://pubmed.ncbi.nlm.nih.gov/17229773/ (accessed on 21 October 2021). [CrossRef] [PubMed]
- Musolino, A.; Naldi, N.; Bortesi, B.; Pezzuolo, D.; Capelletti, M.; Missale, G.; Laccabue, D.; Zerbini, A.; Camisa, R.; Bisagni, G.; et al. Immunoglobulin G fragment C receptor polymorphisms and clinical efficacy of trastuzumab-based therapy in patients with HER-2/neu-positive metastatic breast cancer. J. Clin. Oncol. 2008, 26, 1789–1796. Available online: https://pubmed.ncbi.nlm.nih.gov/18347005/ (accessed on 28 February 2022). [CrossRef] [PubMed]
- Kaifu, T.; Nakamura, A. Polymorphisms of immunoglobulin receptors and the effects on clinical outcome in cancer immunotherapy and other immune diseases: A general review. Int. Immunol. 2017, 29, 319–325. Available online: https://academic.oup.com/intimm/article/29/7/319/4036383 (accessed on 6 October 2021). [CrossRef]
- Shimizu, C.; Mogushi, K.; Morioka, M.S.; Yamamoto, H.; Tamura, K.; Fujiwara, Y.; Tanaka, H. Fc-Gamma receptor polymorphism and gene expression of peripheral blood mononuclear cells in patients with HER2-positive metastatic breast cancer receiving single-agent trastuzumab. Breast Cancer 2015, 23, 624–632. Available online: https://link.springer.com/article/10.1007/s12282-015-0614-y (accessed on 13 October 2021). [CrossRef] [PubMed]
- Roca, L.; Diéras, V.; Roché, H.; Lappartient, E.; Kerbrat, P.; Cany, L.; Chieze, S.; Canon, J.-L.; Spielmann, M.; Penault-Llorca, F.; et al. Correlation of HER2, FCGR2A, and FCGR3A gene polymorphisms with trastuzumab related cardiac toxicity and efficacy in a subgroup of patients from UNICANCER-PACS04 trial. Breast Cancer Res. Treat. 2013, 139, 789–800. Available online: https://link.springer.com/article/10.1007/s10549-013-2587-x (accessed on 13 October 2021). [CrossRef]
- Park, S.; Jiang, Z.; Mortenson, E.D.; Deng, L.; Radkevich-Brown, O.; Yang, X.; Sattar, H.; Wang, Y.; Brown, N.K.; Greene, M.; et al. The therapeutic effect of anti-HER2/neu antibody depends on both innate and adaptive immunity. Cancer Cell 2010, 18, 160–170. Available online: https://pubmed.ncbi.nlm.nih.gov/20708157/ (accessed on 6 October 2021). [CrossRef] [Green Version]
- Takada, K.; Kashiwagi, S.; Goto, W.; Asano, Y.; Takahashi, K.; Takashima, T.; Tomita, S.; Ohsawa, M.; Hirakawa, K.; Ohira, M. Use of the tumor-infiltrating CD8 to FOXP3 lymphocyte ratio in predicting treatment responses to combination therapy with pertuzumab, trastuzumab, and docetaxel for advanced HER2-positive breast cancer. J. Transl. Med. 2018, 16, 86. [Google Scholar] [CrossRef]
- Song, P.N.; Mansur, A.; Dugger, K.J.; Davis, T.R.; Howard, G.; Yankeelov, T.E.; Sorace, A.G. CD4 T-cell immune stimulation of HER2 + breast cancer cells alters response to trastuzumab in vitro. Cancer Cell Int. 2020, 20, 544. Available online: https://cancerci.biomedcentral.com/articles/10.1186/s12935-020-01625-w (accessed on 27 February 2022). [CrossRef] [PubMed]
- Capelan, M.; Pugliano, L.; de Azambuja, E.; Bozovic, I.; Saini, K.S.; Sotiriou, C.; Loi, S.; Piccart-Gebhart, M.J. Pertuzumab: New hope for patients with HER2-positive breast cancer. Ann. Oncol. 2012, 24, 273–282. Available online: https://pubmed.ncbi.nlm.nih.gov/22910839/ (accessed on 28 February 2022). [CrossRef]
- Ishii, K.; Morii, N.; Yamashiro, H. Pertuzumab in the treatment of HER2-positive breast cancer: An evidence-based review of its safety, efficacy, and place in therapy. Core Evid. 2019, 14, 51–70. Available online: https://www.dovepress.com/pertuzumab-in-the-treatment-of-her2-positive-breast-cancer-an-evidence-peer-reviewed-fulltext-article-CE (accessed on 27 February 2022). [CrossRef] [PubMed] [Green Version]
- Mamidi, S.; Cinci, M.; Hasmann, M.; Fehring, V.; Kirschfink, M. Lipoplex mediated silencing of membrane regulators (CD46, CD55 and CD59) enhances complement*dependent anti-tumor activity of trastuzumab and pertuzumab. Mol. Oncol. 2013, 7, 580. [Google Scholar] [CrossRef]
- Nordstrom, J.L.; Gorlatov, S.; Zhang, W.; Yang, Y.; Huang, L.; Burke, S.; Li, H.; Ciccarone, V.; Zhang, T.; Stavenhagen, J.; et al. Anti-tumor activity and toxicokinetics analysis of MGAH22, an anti-HER2 monoclonal antibody with enhanced Fcγ receptor binding properties. Breast Cancer Res. 2011, 13, R123. Available online: https://pubmed.ncbi.nlm.nih.gov/22129105/ (accessed on 19 October 2021). [CrossRef] [PubMed] [Green Version]
- Rugo, H.S.; Im, S.-A.; Wright, G.L.S.; Escriva-De-Romani, S.; Delaurentiis, M.; Cortes, J.; Bahadur, S.W.; Haley, B.B.; Oyola, R.H.; Riseberg, D.A.; et al. SOPHIA primary analysis: A phase 3 (P3) study of margetuximab (M) + chemotherapy (C) versus trastuzumab (T) + C in patients (pts) with HER2+ metastatic (met) breast cancer (MBC) after prior anti-HER2 therapies (Tx). J. Clin. Oncol. 2019, 37, 1000. [Google Scholar] [CrossRef]
- Müller, P.; Kreuzaler, M.; Khan, T.; Thommen, D.S.; Martin, K.; Glatz, K.; Savic, S.; Harbeck, N.; Nitz, U.; Gluz, O.; et al. Trastuzumab emtansine (T-DM1) renders HER2+ breast cancer highly susceptible to CTLA-4/PD-1 blockade. Sci. Transl. Med. 2015, 7, 315ra188. Available online: https://pubmed.ncbi.nlm.nih.gov/26606967/ (accessed on 28 February 2022). [CrossRef]
- Ogitani, Y.; Hagihara, K.; Oitate, M.; Naito, H.; Agatsuma, T. Bystander killing effect of DS -8201a, a novel anti-human epidermal growth factor receptor 2 antibody–drug conjugate, in tumors with human epidermal growth factor receptor 2 heterogeneity. Cancer Sci. 2016, 107, 1039–1046. [Google Scholar] [CrossRef]
- Iwata, T.N.; Sugihara, K.; Wada, T.; Agatsuma, T. A HER2-Targeting Antibody-Drug Conjugate, Trastuzumab Deruxtecan (DS-8201a), Enhances Antitumor Immunity in a Mouse Model. Mol. Cancer Ther. 2018, 17, 1494–1503. Available online: https://pubmed.ncbi.nlm.nih.gov/29703841/ (accessed on 22 October 2021). [CrossRef] [Green Version]
- Iwata, T.N.; Ishii, C.; Ishida, S.; Ogitani, Y.; Wada, T.; Agatsuma, T. [Fam-] trastuzumab deruxtecan (DS-8201a)-induced antitumor immunity is facilitated by the anti-CTLA-4 antibody in a mouse model. PLoS ONE 2019, 14, e0222280. Available online: https://pubmed.ncbi.nlm.nih.gov/31574081/ (accessed on 22 October 2021). [CrossRef] [PubMed] [Green Version]
- Hamilton, E.; Shapiro, C.L.; Petrylak, D.; Boni, V.; Martin, M.; Del Conte, G.; Cortes, J.; Agarwal, L.; Arkenau, H.-T.; Tan, A.R.; et al. Primary analysis from DS8201-A-U105: A 2-part, open label, phase 1b trial assessing trastuzumab deruxtecan (T-DXd) with nivolumab (nivo) in patients (pts) with HER2-expressing advanced breast cancer. Ann. Oncol. 2022, 33, S194–S223. [Google Scholar] [CrossRef]
- Cortés, J.; Kim, S.-B.; Chung, W.-P.; Im, S.-A.; Park, Y.; Hegg, R.; Kim, M.; Tseng, L.-M.; Petry, V.; Chung, C.-F.; et al. LBA1 Trastuzumab deruxtecan (T-DXd) vs trastuzumab emtansine (T-DM1) in patients (Pts) with HER2+ metastatic breast cancer (mBC): Results of the randomized phase III DESTINY-Breast03 study. Ann. Oncol. 2021, 32, S1287–S1288. [Google Scholar] [CrossRef]
- Hamilton, E.P.; Petit, T.; Pistilli, B.; Goncalves, A.; Ferreira, A.A.; Dalenc, F.; Cardoso, F.; Mita, M.M.; Dezentjé, V.O.; Manso, L.; et al. Clinical activity of MCLA-128 (zenocutuzumab), trastuzumab, and vinorelbine in HER2 amplified metastatic breast cancer (MBC) patients (pts) who had progressed on anti-HER2 ADCs. J. Clin. Oncol. 2020, 38, 3093. [Google Scholar] [CrossRef]
- Oberg, H.H.; Kellner, C.; Gonnermann, D.; Sebens, S.; Bauerschlag, D.; Gramatzki, M.; Kabelitz, D.; Peipp, M.; Wesch, D. Tribody [(HER2)2xCD16] Is More Effective Than Trastuzumab in Enhancing γδ T Cell and Natural Killer Cell Cytotoxicity Against HER2-Expressing Cancer Cells. Front. Immunol. 2018, 9, 814. [Google Scholar] [CrossRef]
- Borghaei, H.; Alpaugh, R.K.; Bernardo, P.; Palazzo, I.E.; Dutcher, J.P.; Venkatraj, U.; Wood, W.C.; Goldstein, L.; Weiner, L.M. Induction of adaptive Anti-HER2/neu immune responses in a Phase 1B/2 trial of 2B1 bispecific murine monoclonal antibody in metastatic breast cancer (E3194): A trial coordinated by the Eastern Cooperative Oncology Group. J. Immunother. 2007, 30, 455–467. Available online: https://pubmed.ncbi.nlm.nih.gov/17457220/ (accessed on 4 November 2021). [CrossRef]
- Hashimoto, K.; Modjtahedi, H. CD137 as an Attractive T Cell Co-Stimulatory Target in the TNFRSF for Immuno-Oncology Drug Development. Cancers 2021, 13, 2288. Available online: https://www.mdpi.com/2072-6694/13/10/2288/htm (accessed on 9 November 2021). [CrossRef]
- Ku, G.; Bendell, J.; Tolcher, A.; Hurvitz, S.; Krishnamurthy, A.; El-Khoueiry, A.; Patnaik, A.; Shroff, R.; Noonan, A.; Hahn, N.; et al. 525O A phase I dose escalation study of PRS-343, a HER2/4-1BB bispecific molecule, in patients with HER2-positive malignancies. Ann. Oncol. 2020, 31, S462–S463. Available online: http://www.annalsofoncology.org/article/S0923753420406350/fulltext (accessed on 4 November 2021). [CrossRef]
- PRS-343 in Combination With Atezolizumab in HER2-Positive Solid Tumors-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03650348 (accessed on 4 November 2021).
- A Phase I Study of BTRC4017A in Participants With Locally Advanced or Metastatic HER2-Expressing Cancers-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03448042 (accessed on 9 November 2021).
- Nagai, Y.; Tsuchiya, H.; Runkle, E.A.; Young, P.D.; Ji, M.Q.; Norton, L.; Drebin, J.A.; Zhang, H.; Greene, M.I. Disabling of the erbB Pathway Followed by IFN-γ Modifies Phenotype and Enhances Genotoxic Eradication of Breast Tumors. Cell Rep. 2015, 12, 2049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez-Gracia, J.L.; Hansen, A.R.; Eefsen, R.H.L.; Gomez-Roca, C.A.; Negrier, S.; Pedrazzoli, P.; Lee, J.-L.; Gordoa, T.A.; Rodriguez, C.S.; Mellado, B.; et al. Randomized phase Ib study to evaluate safety, pharmacokinetics and therapeutic activity of simlukafusp α in combination with atezolizumab ± bevacizumab in patients with unresectable advanced/ metastatic renal cell carcinoma (RCC) (NCT03063762). J. Clin. Oncol. 2021, 39, 4556. [Google Scholar] [CrossRef]
- A Study Evaluating Safety, Pharmacokinetics, and Therapeutic Activity of RO6874281 as a Single Agent (Part A) or in Combination With Trastuzumab or Cetuximab (Part B or C)-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT02627274 (accessed on 13 March 2022).
- Basket Study to Evaluate the Therapeutic Activity of Simlukafusp Alfa as a Combination Therapy in Participants With Advanced and/or Metastatic Solid Tumors-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03386721 (accessed on 13 March 2022).
- Maruyama, T.; Mimura, K.; Izawa, S.; Inoue, A.; Shiba, S.; Watanabe, M.; Kawaguchi, Y.; Inoue, M.; Nogata, H.; Inoue, S.; et al. Lapatinib enhances herceptin-mediated antibody-dependent cellular cytotoxicity by up-regulation of cell surface HER2 expression. Anticancer Res. 2011, 31, 2999–3005. [Google Scholar]
- Griguolo, G.; Pascual, T.; Dieci, M.V.; Guarneri, V.; Prat, A. Interaction of host immunity with HER2-targeted treatment and tumor heterogeneity in HER2-positive breast cancer. J. Immunother. Cancer 2019, 7, 90. Available online: https://jitc.biomedcentral.com/articles/10.1186/s40425-019-0548-6 (accessed on 1 March 2022). [CrossRef] [PubMed]
- Scaltriti, M.; Verma, C.; Guzman, M.; Jimenez, J.; Parra, J.L.; Pedersen, K.; Smith, D.J.; Landolfi, S.; Cajal, S.R.Y.; Arribas, J.; et al. Lapatinib, a HER2 tyrosine kinase inhibitor, induces stabilization and accumulation of HER2 and potentiates trastuzumab-dependent cell cytotoxicity. Oncogene 2008, 28, 803–814. Available online: https://pubmed.ncbi.nlm.nih.gov/19060928/ (accessed on 1 March 2022). [CrossRef] [PubMed] [Green Version]
- Hannesdóttir, L.; Tymoszuk, P.; Parajuli, N.; Wasmer, M.-H.; Philipp, S.; Daschil, N.; Datta, S.; Koller, J.-B.; Tripp, C.H.; Stoitzner, P.; et al. Lapatinib and doxorubicin enhance the Stat1-dependent antitumor immune response. Eur. J. Immunol. 2013, 43, 2718–2729. Available online: https://pubmed.ncbi.nlm.nih.gov/23843024/ (accessed on 1 March 2022). [CrossRef] [PubMed] [Green Version]
- Fumagalli, D.; Venet, D.; Ignatiadis, M.; Azim, H.A.; Maetens, M.; Rothé, F.; Salgado, R.; Bradbury, I.; Pusztai, L.; Harbeck, N.; et al. RNA Sequencing to Predict Response to Neoadjuvant Anti-HER2 Therapy: A Secondary Analysis of the NeoALTTO Randomized Clinical Trial. JAMA Oncol. 2017, 3, 227–234. Available online: https://jamanetwork.com/journals/jamaoncology/fullarticle/2554757 (accessed on 1 March 2022). [CrossRef] [PubMed]
- Dieci, M.V.; Prat, A.; Tagliafico, E.; Paré, L.; Ficarra, G.; Bisagni, G.; Piacentini, F.; Generali, D.G.; Conte, P.; Guarneri, V. Integrated evaluation of PAM50 subtypes and immune modulation of pCR in HER2-positive breast cancer patients treated with chemotherapy and HER2-targeted agents in the CherLOB trial. Ann. Oncol. 2016, 27, 1867–1873. Available online: https://pubmed.ncbi.nlm.nih.gov/27484801/ (accessed on 1 March 2022). [CrossRef]
- Canonici, A.; Gijsen, M.; Mullooly, M.; Bennett, R.; Bouguern, N.; Pedersen, K.; O’Brien, N.A.; Roxanis, I.; Li, J.-L.; Bridge, E.; et al. Neratinib overcomes trastuzumab resistance in HER2 amplified breast cancer. Oncotarget 2013, 4, 1592–1605. Available online: https://pubmed.ncbi.nlm.nih.gov/24009064/ (accessed on 1 March 2022). [CrossRef] [Green Version]
- Collins, D.M.; Gately, K.; Hughes, C.; Edwards, C.; Davies, A.; Madden, S.F.; O’Byrne, K.J.; O’Donovan, N.; Crown, J. Tyrosine kinase inhibitors as modulators of trastuzumab-mediated antibody-dependent cell-mediated cytotoxicity in breast cancer cell lines. Cell. Immunol. 2017, 319, 35–42. Available online: https://pubmed.ncbi.nlm.nih.gov/28735814/ (accessed on 1 March 2022). [CrossRef]
- Murthy, R.K.; Loi, S.; Okines, A.; Paplomata, E.; Hamilton, E.; Hurvitz, S.A.; Lin, N.U.; Borges, V.; Abramson, V.; Anders, C.; et al. Tucatinib, Trastuzumab, and Capecitabine for HER2-Positive Metastatic Breast Cancer. N. Engl. J. Med. 2020, 382, 597–609. Available online: https://www.nejm.org/doi/full/10.1056/nejmoa1914609 (accessed on 1 March 2022). [CrossRef]
- Li, R.; Sant, S.; Brown, E.; Caramia, F.; Byrne, A.; Clarke, K.; Neeson, M.; Neeson, P.J.; Darcy, P.K.; Peterson, S.; et al. Abstract PS10-04: Tucatinib favourably modulates the immune microenvironment and synergises with anti-PD1 therapy in a trastuzumab resistant HER2+ murine model. Cancer Res. 2021, 81, PS10-04. Available online: https://aacrjournals.org/cancerres/article/81/4_Supplement/PS10-04/648168/Abstract-PS10-04-Tucatinib-favourably-modulates (accessed on 2 March 2022). [CrossRef]
- Huober, J.; Barrios, C.; Niikura, N.; Jarzab, M.; Chang, Y.-C.; Huggins-Puhalla, S.; Graupner, V.; Eiger, D.; Henschel, V.; Gochitashvili, N.; et al. VP6-2021: IMpassion050: A phase III study of neoadjuvant atezolizumab + pertuzumab + trastuzumab + chemotherapy (neoadj A + PH + CT) in high-risk, HER2-positive early breast cancer (EBC). Ann. Oncol. 2021, 32, 1061–1062. Available online: http://www.annalsofoncology.org/article/S0923753421020251/fulltext (accessed on 16 March 2022). [CrossRef]
- Dirix, L.Y.; Takacs, I.; Jerusalem, G.; Nikolinakos, P.; Arkenau, H.T.; Forero-Torres, A.; Boccia, R.; Lippman, M.E.; Somer, R.; Smakal, M.; et al. Avelumab, an anti-PD-L1 antibody, in patients with locally advanced or metastatic breast cancer: A phase 1b JAVELIN Solid Tumor study. Breast Cancer Res. Treat. 2018, 167, 671–686. Available online: https://pubmed.ncbi.nlm.nih.gov/29063313/ (accessed on 8 December 2021). [CrossRef] [PubMed] [Green Version]
- Chia, S.; Bedard, P.L.; Hilton, J.; Amir, E.; Gelmon, K.; Goodwin, R.; Villa, D.; Cabanero, M.; Tu, D.; Tsao, M.; et al. A Phase Ib Trial of Durvalumab in Combination with Trastuzumab in HER2-Positive Metastatic Breast Cancer (CCTG IND.229). Oncologist 2019, 24, 1439–1445. Available online: https://pubmed.ncbi.nlm.nih.gov/31420468/ (accessed on 18 December 2021). [CrossRef] [Green Version]
- Neoadjuvant Treatment of HER2 Positive Early High-risk and Locally Advanced Breast Cancer-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03595592 (accessed on 14 March 2022).
- Testing the Drug Atezolizumab or Placebo With Usual Therapy in First-Line HER2-Positive Metastatic Breast Cancer-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03199885 (accessed on 14 March 2022).
- The AVIATOR Study: Trastuzumab and Vinorelbine with Avelumab OR Avelumab & Utomilumab in Advanced HER2+ Breast Cancer-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03414658 (accessed on 18 December 2021).
- Atezolizumab + Pertuzumab + Trastuzumab in CNS Mets in BC-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03417544 (accessed on 14 March 2022).
- Datta, J.; Fracol, M.; McMillan, M.T.; Berk, E.; Xu, S.; Goodman, N.; Lewis, D.A.; DeMichele, A.; Czerniecki, B.J. Association of Depressed Anti-HER2 T-Helper Type 1 Response With Recurrence in Patients With Completely Treated HER2-Positive Breast Cancer: Role for Immune Monitoring. JAMA Oncol. 2016, 2, 242–246. Available online: https://pubmed.ncbi.nlm.nih.gov/26719971/ (accessed on 9 November 2021). [CrossRef] [PubMed] [Green Version]
- Costa, R.L.B.; Soliman, H.; Czerniecki, B.J. The clinical development of vaccines for HER2 + breast cancer: Current landscape and future perspectives. Cancer Treat Rev. 2017, 61, 107–115. Available online: https://pubmed.ncbi.nlm.nih.gov/29125981/ (accessed on 9 November 2021). [CrossRef]
- Benavides, L.C.; Gates, J.D.; Carmichael, M.G.; Patel, R.; Holmes, J.P.; Hueman, M.T.; Mittendorf, E.A.; Craig, D.; Stojadinovic, A.; Ponniah, S.; et al. The impact of HER2/neu expression level on response to the E75 vaccine: From U.S. Military Cancer Institute Clinical Trials Group Study I-01 and I-02. Clin. Cancer Res. 2009, 15, 2895–2904. Available online: https://pubmed.ncbi.nlm.nih.gov/19351776/ (accessed on 6 March 2022). [CrossRef] [Green Version]
- Peoples, G.E.; Gurney, J.M.; Hueman, M.T.; Woll, M.M.; Ryan, G.B.; Storrer, C.E.; Fisher, C.; Shriver, C.D.; Ioannides, C.G.; Ponniah, S. Clinical trial results of a HER2/neu (E75) vaccine to prevent recurrence in high-risk breast cancer patients. J. Clin. Oncol. 2005, 23, 7536–7545. Available online: https://pubmed.ncbi.nlm.nih.gov/16157940/ (accessed on 6 March 2022). [CrossRef]
- Mittendorf, E.A.; Lu, B.; Melisko, M.; Hiller, J.P.; Bondarenko, I.; Brunt, A.M.; Sergii, G.; Petrakova, K.; Peoples, G.E. Efficacy and Safety Analysis of Nelipepimut-S Vaccine to Prevent Breast Cancer Recurrence: A Randomized, Multicenter, Phase III Clinical Trial. Clin. Cancer Res. 2019, 25, 4248–4254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clifton, G.T.T.; Hale, D.; Vreeland, T.J.; Hickerson, A.T.; Litton, J.K.; Alatrash, G.; Murthy, R.K.; Qiao, N.; Philips, A.V.; Lukas, J.J.; et al. Results of a Randomized Phase IIb Trial of Nelipepimut-S + Trastuzumab versus Trastuzumab to Prevent Recurrences in Patients with High-Risk HER2 Low-Expressing Breast Cancer. Clin. Cancer Res. 2020, 26, 2515–2523. Available online: https://pubmed.ncbi.nlm.nih.gov/32071118/ (accessed on 14 November 2021). [CrossRef] [Green Version]
- Mittendorf, E.A.; Clifton, G.T.; Holmes, J.P.; Clive, K.S.; Patil, R.; Benavides, L.C.; Gates, J.D.; Sears, A.K.; Stojadinovic, A.; Ponniah, S.; et al. Clinical trial results of the HER-2/neu (E75) vaccine to prevent breast cancer recurrence in high-risk patients: From US Military Cancer Institute Clinical Trials Group Study I-01 and I-02. Cancer 2012, 118, 2594–2602. Available online: https://pubmed.ncbi.nlm.nih.gov/21989902/ (accessed on 6 March 2022). [CrossRef] [Green Version]
- Peoples, G.E.; Holmes, J.P.; Hueman, M.T.; Mittendorf, E.A.; Amin, A.; Khoo, S.; Dehqanzada, Z.A.; Gurney, J.M.; Woll, M.M.; Ryan, G.B.; et al. Combined Clinical Trial Results of a HER2/neu (E75) Vaccine for the Prevention of Recurrence in High-Risk Breast Cancer Patients: U.S. Military Cancer Institute Clinical Trials Group Study I-01 and I-02. Clin. Cancer Res. 2008, 14, 797–803. Available online: https://clincancerres.aacrjournals.org/content/14/3/797 (accessed on 26 December 2021). [CrossRef] [Green Version]
- Patil, R.; Clifton, G.T.; Holmes, J.P.; Amin, A.; Carmichael, M.G.; Gates, J.D.; Benavides, L.H.; Hueman, M.T.; Ponniah, S.; Peoples, G.E. Clinical and immunologic responses of HLA-A3+ breast cancer patients vaccinated with the HER2/neu-derived peptide vaccine, E75, in a phase I/II clinical trial. J. Am. Coll. Surg. 2010, 210, 140–147. Available online: https://pubmed.ncbi.nlm.nih.gov/20113933/ (accessed on 6 March 2022). [CrossRef] [PubMed]
- Mittendorf, E.A.; Ardavanis, A.; Symanowski, J.; Murray, J.L.; Shumway, N.M.; Litton, J.K.; Hale, D.F.; Perez, S.A.; Anastasopoulou, E.A.; Pistamaltzian, N.F.; et al. Primary analysis of a prospective, randomized, single-blinded phase II trial evaluating the HER2 peptide AE37 vaccine in breast cancer patients to prevent recurrence. Ann. Oncol. 2016, 27, 1241–1248. Available online: https://pubmed.ncbi.nlm.nih.gov/27029708/ (accessed on 21 November 2021). [CrossRef] [PubMed]
- Holmes, J.P.; Benavides, L.C.; Gates, J.D.; Carmichael, M.G.; Hueman, M.T.; Mittendorf, E.A.; Amin, A.; Craig, D.; von Hofe, E.; Ponniah, S.; et al. Results of the first phase I clinical trial of the novel II-key hybrid preventive HER-2/neu peptide (AE37) vaccine. J. Clin. Oncol. 2008, 26, 3426–3433. Available online: https://pubmed.ncbi.nlm.nih.gov/18612158/ (accessed on 6 March 2022). [CrossRef] [PubMed]
- Clifton, G.T.; Litton, J.K.; Rn, K.A.; Ponniah, S.; Ibrahim, N.K.; Gall, V.; Alatrash, G.; Peoples, G.E.; Mittendorf, E.A. Results of a Phase Ib Trial of Combination Immunotherapy with a CD8+ T Cell Eliciting Vaccine and Trastuzumab in Breast Cancer Patients. Ann. Surg. Oncol. 2017, 24, 2161–2167. Available online: https://pubmed.ncbi.nlm.nih.gov/28315060/ (accessed on 6 March 2022). [CrossRef]
- Patel, S.S.; McWilliams, D.B.; Patel, M.S.; Fischette, C.T.; Thompson, J.; Daugherty, F.J. Abstract PS10-23: Five year median follow-up data from a prospective, randomized, placebo-controlled, single-blinded, multicenter, phase IIb study evaluating the reduction of recurrences using HER2/neu peptide GP2 + GM-CSF vs. GM-CSF alone after adjuvant trastuzumab in HER2 positive women with operable breast cancer. Cancer Res. 2021, 81, PS10–PS23. Available online: https://aacrjournals.org/cancerres/article/81/4_Supplement/PS10-23/648223/Abstract-PS10-23-Five-year-median-follow-up-data (accessed on 6 March 2022).
- Valdes-Zayas, A.; Gonzalez, Z.; Mulens, V.; Vega, A.M.; Perez, K.; Lorenzo-Luaces, P.; Rubio, M.C.; Estevez, A.; Curbelo, I.; Fernandez, L.E.; et al. Immunologic Response Elicited in Breast Cancer Patients Receiving a NeuGcGM3-based Vaccine as Adjuvant Therapy. J. Immunother. 2017, 40, 289–301. Available online: https://pubmed.ncbi.nlm.nih.gov/28604556/ (accessed on 16 March 2022). [CrossRef]
- Koski, G.K.; Koldovsky, U.; Xu, S.; Mick, R.; Sharma, A.; Fitzpatrick, E.; Weinstein, S.; Nisenbaum, H.; Levine, B.L.; Fox, K.; et al. A novel dendritic cell-based immunization approach for the induction of durable Th1-polarized anti-HER-2/neu responses in women with early breast cancer. J. Immunother. 2012, 35, 54–65. Available online: https://pubmed.ncbi.nlm.nih.gov/22130160/ (accessed on 21 November 2021). [CrossRef] [Green Version]
- Lowenfeld, L.; Mick, R.; Datta, J.; Xu, S.; Fitzpatrick, E.; Fisher, C.S.; Fox, K.R.; DeMichele, A.; Zhang, P.J.; Weinstein, S.P.; et al. Dendritic Cell Vaccination Enhances Immune Responses and Induces Regression of HER2pos DCIS Independent of Route: Results of Randomized Selection Design Trial. Clin. Cancer Res. 2017, 23, 2961–2971. Available online: https://clincancerres.aacrjournals.org/content/23/12/2961 (accessed on 9 November 2021). [CrossRef] [Green Version]
- Higgins, M.; Curigliano, G.; Dieras, V.; Kuemmel, S.; Kunz, G.; Fasching, P.A.; Campone, M.; Bachelot, T.; Krivorotko, P.; Chan, S.; et al. Safety and immunogenicity of neoadjuvant treatment using WT1-immunotherapeutic in combination with standard therapy in patients with WT1-positive Stage II/III breast cancer: A randomized Phase I study. Breast Cancer Res. Treat. 2017, 162, 479–488. Available online: https://pubmed.ncbi.nlm.nih.gov/28176175/ (accessed on 6 March 2022). [CrossRef] [Green Version]
- Czerniecki, B.J.; Koski, G.K.; Koldovsky, U.; Xu, S.; Cohen, P.A.; Mick, R.; Nisenbaum, H.; Pasha, T.; Xu, M.; Fox, K.R.; et al. Targeting HER-2/neu in early breast cancer development using dendritic cells with staged interleukin-12 burst secretion. Cancer Res. 2007, 67, 1842–1852. Available online: https://pubmed.ncbi.nlm.nih.gov/17293384/ (accessed on 6 March 2022). [CrossRef] [PubMed] [Green Version]
- Bekaii-Saab, T.; Wesolowski, R.; Ahn, D.H.; Wu, C.; Mortazavi, A.; Lustberg, M.B.; Ramaswamy, B.; Fowler, J.; Wei, L.; Overholser, J.; et al. Phase I Immunotherapy Trial with Two Chimeric HER-2 B-Cell Peptide Vaccines Emulsified in Montanide ISA 720VG and Nor-MDP Adjuvant in Patients with Advanced Solid Tumors. Clin. Cancer Res. 2019, 25, 3495–3507. Available online: https://pubmed.ncbi.nlm.nih.gov/30804020/ (accessed on 27 December 2021). [CrossRef] [PubMed] [Green Version]
- Wiedermann, U.; Wiltschke, C.; Jasinska, J.; Kundi, M.; Zurbriggen, R.; Garner-Spitzer, E.; Bartsch, R.; Steger, G.; Pehamberger, H.; Scheiner, O.; et al. A virosomal formulated Her-2/neu multi-peptide vaccine induces Her-2/neu-specific immune responses in patients with metastatic breast cancer: A phase I study. Breast Cancer Res. Treat. 2010, 119, 673–683. Available online: https://pubmed.ncbi.nlm.nih.gov/20092022/ (accessed on 27 December 2021). [CrossRef] [PubMed] [Green Version]
- Tiriveedhi, V.; Tucker, N.; Herndon, J.; Li, L.; Sturmoski, M.; Ellis, M.; Ma, C.; Naughton, M.; Lockhart, A.C.; Gao, F.; et al. Safety and Preliminary Evidence of Biologic Efficacy of a Mammaglobin-A DNA Vaccine in Patients with Stable Metastatic Breast Cancer. Clin. Cancer Res. 2014, 20, 5964–5975. Available online: https://pubmed.ncbi.nlm.nih.gov/25451106/ (accessed on 28 December 2021). [CrossRef] [PubMed] [Green Version]
- Park, J.W.; Melisko, M.E.; Esserman, L.J.; Jones, L.A.; Wollan, J.B.; Sims, R. Treatment With Autologous Antigen-Presenting Cells Activated With the HER-2 –Based Antigen Lapuleucel-T: Results of a Phase I Study in Immunologic and Clinical Activity in HER-2-Overexpressing Breast Cancer. J. Clin. Oncol. 2007, 25, 3680–3687. Available online: https://pubmed.ncbi.nlm.nih.gov/17704416/ (accessed on 21 November 2021). [CrossRef] [PubMed]
- Ahlert, T.; Sauerbrei, W.; Bastert, G.; Ruhland, S.; Bartik, B.; Simiantonaki, N.; Schumacher, J.; Häcker, B.; Schumacher, M.; Schirrmacher, V. Tumor-cell number and viability as quality and efficacy parameters of autologous virus-modified cancer vaccines in patients with breast or ovarian cancer. J. Clin. Oncol. 1997, 15, 1354–1366. Available online: https://pubmed.ncbi.nlm.nih.gov/9193327/ (accessed on 14 March 2022). [CrossRef]
- Curigliano, G.; Romieu, G.; Campone, M.; Dorval, T.; Duck, L.; Canon, J.-L.; Roemer-Becuwe, C.; Roselli, M.; Neciosup, S.; Burny, W.; et al. A phase I/II trial of the safety and clinical activity of a HER2-protein based immunotherapeutic for treating women with HER2-positive metastatic breast cancer. Breast Cancer Res. Treat. 2016, 156, 301–310. Available online: https://pubmed.ncbi.nlm.nih.gov/26975189/ (accessed on 21 December 2021). [CrossRef] [PubMed]
- Disis, M.L.; Wallace, D.R.; Gooley, T.A.; Dang, Y.; Slota, M.; Lu, H.; Coveler, A.L.; Childs, J.S.; Higgins, D.M.; Fintak, P.A.; et al. Concurrent trastuzumab and HER2/neu-specific vaccination in patients with metastatic breast cancer. J. Clin. Oncol. 2009, 27, 4685–4692. Available online: https://pubmed.ncbi.nlm.nih.gov/19720923/ (accessed on 7 March 2022). [CrossRef] [Green Version]
- Krasniqi, E.; Barchiesi, G.; Pizzuti, L.; Mazzotta, M.; Venuti, A.; Maugeri-Saccà, M.; Sanguineti, G.; Massimiani, G.; Sergi, D.; Carpano, S.; et al. Immunotherapy in HER2-positive breast cancer: State of the art and future perspectives. J. Hematol. Oncol. 2019, 12, 1–26. Available online: https://jhoonline.biomedcentral.com/articles/10.1186/s13045-019-0798-2 (accessed on 26 December 2021). [CrossRef]
- Dillon, P.M.; Brenin, C.M.; Jr, C.L.S. Evaluating Nelipepimut-S in the Treatment of Breast Cancer: A Short Report on the Emerging Data. Breast Cancer Targets Ther. 2020, 12, 69–75. [Google Scholar] [CrossRef] [Green Version]
- McCarthy, P.M.; Clifton, G.T.; Vreeland, T.J.; Adams, A.M.; O’Shea, A.E.; Peoples, G.E. AE37: A HER2-targeted vaccine for the prevention of breast cancer recurrence. Expert Opin. Investig. Drugs 2020, 30, 5–11. Available online: https://pubmed.ncbi.nlm.nih.gov/33191799/ (accessed on 21 November 2021). [CrossRef]
- Tobias, J.; Battin, C.; Linhares, A.D.S.; Lebens, M.; Baier, K.; Ambroz, K.; Drinić, M.; Högler, S.; Inic-Kanada, A.; Garner-Spitzer, E.; et al. A New Strategy Toward B Cell-Based Cancer Vaccines by Active Immunization With Mimotopes of Immune Checkpoint Inhibitors. Front. Immunol. 2020, 11, 895. [Google Scholar] [CrossRef] [PubMed]
- Tobias, J.; Garner-Spitzer, E.; Drinić, M.; Wiedermann, U. Vaccination against Her-2/neu, with focus on peptide-based vaccines. ESMO Open 2022, 7, 100361. Available online: http://www.esmoopen.com/article/S2059702921003239/fulltext (accessed on 12 March 2022). [CrossRef] [PubMed]
- Nordin, M.L.; Norpi, A.S.M.; Ng, P.Y.; Yusoff, K.; Abu, N.; Lim, K.P.; Azmi, F. HER2/neu-Based Peptide Vaccination-Pulsed with B-Cell Epitope Induced Efficient Prophylactic and Therapeutic Antitumor Activities in TUBO Breast Cancer Mice Model. Cancers 2021, 13, 4958. Available online: https://pubmed.ncbi.nlm.nih.gov/34638441/ (accessed on 27 December 2021). [CrossRef]
- Wiedermann, U.; Davis, A.B.; Zielinski, C.C. Vaccination for the prevention and treatment of breast cancer with special focus on Her-2/neu peptide vaccines. Breast Cancer Res. Treat. 2013, 138, 1–12. Available online: https://pubmed.ncbi.nlm.nih.gov/23340862/ (accessed on 27 December 2021).
- Wiedermann, U.; Garner-Spitzer, E.; Chao, Y.; Maglakelidze, M.; Bulat, I.; Dechaphunkul, A.; Arpornwirat, W.; Charoentum, C.; Yen, C.J.; Yau, T.C.; et al. Clinical and immunologic responses to a B-Cell epitope vaccine in patients with HER2/neu-overexpressing advanced gastric cancer—results from phase Ib trial IMU.ACS.001. Clin. Cancer Res. 2021, 27, 3649–3660. Available online: https://aacrjournals.org/clincancerres/article/27/13/3649/671490/Clinical-and-Immunologic-Responses-to-a-B-Cell (accessed on 12 March 2022).
- Disis, M.L.; Schiffman, K.; Guthrie, K.; Salazar, L.G.; Knutson, K.L.; Goodell, V.; dela Rosa, C.; Cheever, M.A. Effect of dose on immune response in patients vaccinated with an her-2/neu intracellular domain protein–based vaccine. J. Clin. Oncol. 2004, 22, 1916–1925. Available online: https://pubmed.ncbi.nlm.nih.gov/15143085/ (accessed on 27 December 2021). [CrossRef] [PubMed] [Green Version]
- Ladjemi, M.Z.; Chardès, T.; Corgnac, S.; Garambois, V.; Morisseau, S.; Robert, B.; Bascoul-Mollevi, C.; Arsa, I.A.; Jacot, W.; Pouget, J.-P.; et al. Vaccination with human anti-trastuzumab anti-idiotype scFv reverses HER2 immunological tolerance and induces tumor immunity in MMTV.f.huHER2(Fo5) mice. Breast Cancer Res. 2011, 13, R17. Available online: https://breast-cancer-research.biomedcentral.com/articles/10.1186/bcr2826 (accessed on 21 November 2021). [CrossRef]
- Tiriveedhi, V.; Fleming, T.P.; Goedegebuure, P.S.; Naughton, M.; Ma, C.; Lockhart, C.; Gao, F.; Gillanders, W.E.; Mohanakumar, T. Mammaglobin-A cDNA vaccination of breast cancer patients induces antigen-specific cytotoxic CD4+ICOShi T cells. Breast Cancer Res. Treat. 2012, 138, 109–118. Available online: https://pubmed.ncbi.nlm.nih.gov/22678162/ (accessed on 28 December 2021). [CrossRef] [PubMed] [Green Version]
- Garg, A.D.; Vara-Perez, M.; Schaaf, M.; Agostinis, P.; Zitvogel, L.; Kroemer, G.; Galluzzi, L. Trial watch: Dendritic cell-based anticancer immunotherapy. OncoImmunology 2017, 6, e1328341. Available online: https://pubmed.ncbi.nlm.nih.gov/28811970/ (accessed on 21 November 2021). [CrossRef]
- Vaccine Therapy, Trastuzumab, and Vinorelbine in Treating Patients With Locally Recurrent or Metastatic Breast Cancer-Full Text View-ClinicalTrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT00266110 (accessed on 21 November 2021).
- Jiang, X.P.; Yang, D.C.; Elliott, R.L.; Head, J.F. Vaccination with a Mixed Vaccine of Autogenous and Allogeneic Breast Cancer Cells and Tumor Associated Antigens CA15-3, CEA and CA125-Results in Immune and Clinical Responses in Breast Cancer Patients. Cancer Biother. Radiopharm. 2000, 15, 495–505. Available online: https://pubmed.ncbi.nlm.nih.gov/11155821/ (accessed on 21 November 2021). [CrossRef]
- Elliott, R.L.; Head, J.F. Adjuvant breast cancer vaccine improves disease specific survival of breast cancer patients with depressed lymphocyte immunity. Surg. Oncol. 2013, 22, 172–177. Available online: https://pubmed.ncbi.nlm.nih.gov/23791552/ (accessed on 22 November 2021). [CrossRef] [PubMed]
- Perez, E.A.; Romond, E.H.; Suman, V.J.; Jeong, J.; Sledge, G.; Geyer, C.E., Jr.; Martino, S.; Rastogi, P.; Gralow, J.; Swain, S.; et al. Trastuzumab Plus Adjuvant Chemotherapy for Human Epidermal Growth Factor Receptor 2–Positive Breast Cancer: Planned Joint Analysis of Overall Survival From NSABP B-31 and NCCTG N9831. J. Clin. Oncol. 2014, 32, 3744–3752. [Google Scholar] [CrossRef] [PubMed]
- Hamy, A.-S.; Pierga, J.-Y.; Sabaila, A.; Laas, E.; Bonsang-Kitzis, H.; Laurent, C.; Vincent-Salomon, A.; Cottu, P.; Lerebours, F.; Rouzier, R.; et al. Stromal lymphocyte infiltration after neoadjuvant chemotherapy is associated with aggressive residual disease and lower disease-free survival in HER2-positive breast cancer. Ann. Oncol. 2017, 28, 2233–2240. Available online: http://www.annalsofoncology.org/article/S0923753419352561/fulltext (accessed on 19 March 2022). [CrossRef] [PubMed]
- Loi, S.; Adams, S.; Schmid, P.; Cortés, J.; Cescon, D.W.; Winer, E.P.; Toppmeyer, D.L.; Rugo, H.S.; De Laurentiis, M.; Nanda, R.; et al. Relationship between Tumor Infiltrating Lymphocyte (TIL) Levels and Response to Pembrolizumab (Pembro) in Metastatic Triple-Negative Breast Cancer (mTNBC): Results from KEYNOTE-086. In Proceedings of the ESMO Annul Meeting, Madrid, Spain, 8–12 September 2017; Elsevier Inc.: Amsterdam, The Netherlands, 2017. Available online: http://www.annalsofoncology.org/article/S0923753420391055/fulltext (accessed on 25 December 2021).
- Schmid, P.; Cortes, J.; Pusztai, L.; McArthur, H.; Kümmel, S.; Bergh, J.; Denkert, C.; Park, Y.H.; Hui, R.; Harbeck, N.; et al. Pembrolizumab for Early Triple-Negative Breast Cancer. N. Engl. J. Med. 2020, 382, 810–821. Available online: https://pubmed.ncbi.nlm.nih.gov/32101663/ (accessed on 19 March 2021). [CrossRef] [PubMed]
- Hamson, E.J.; Keane, F.M.; Tholen, S.; Schilling, O.; Gorrell, M.D. Understanding fibroblast activation protein (FAP): Substrates, activities, expression and targeting for cancer therapy. Proteom.-Clin. Appl. 2014, 8, 454–463. Available online: https://pubmed.ncbi.nlm.nih.gov/24470260/ (accessed on 25 December 2021). [CrossRef] [PubMed]
- Arab, A.; Yazdian-Robati, R.; Behravan, J. HER2-Positive Breast Cancer Immunotherapy: A Focus on Vaccine Development. Arch. Immunol. Ther. Exp. 2020, 68, 2. Available online: https://pubmed.ncbi.nlm.nih.gov/31915932/ (accessed on 9 November 2021). [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Setting | Conducted Study | Type of Study | Population | Intervention | Primary Endpoint | TILs Assessment |
|---|---|---|---|---|---|---|
| ADJUVANT | FinHER Purmonen et al., 2011 [22,23] | Phase III RCT | 232 early stage, operable BC HER2+ pts | 9 weeks of trastuzumab or no trastuzumab in addition to chemotherapy | DDFS: benefit from adding trastuzumab to adjuvant Cht (HR = 0.32; p = 0.029) | Each 10% increase in TILs was associated with 13% reduction in the DDFS (HR 0.77; 95% CI 0.61–0.98, p = 0.02) |
| NSAPB B-31 Romond et al., 2005 [24,25] | Phase III RCT | 2043 early stage, operable BC HER2+ pts | Adjuvant Cht with or without trastuzumab | DFS: benefit from the addition of trastuzumab to adjuvant Cht (p < 0.001; stratified HR = 0.52); (95% CI, 0.45 to 0.60) | Pts with sTILs were statistically significantly associated with improved DFS (HR = 0.65, (95% CI, 0.49 to 0.86), p = 0.003) | |
| NCCTG Perez et al., 2005 [24,26] | Phase III RCT | 1633 early stage, operable HER2+ pts | Adjuvant Cht with or without trastuzumab | DFS: Decrease in DFS events by 40% (HR, 0.60 (95% CI, 0.53 to 0.68); p < 0.001) | No association between high levels of TILS and benefit from trastuzumab therapy benefit (HR, 1.26 (95% CI, 0.50–3.17); p = 0.63) 1 | |
| APHINITY Von Minckwitz et al., 2017 [27,28] | Phase III RCT | 4805 early stage, operable HER2+ BC pts. | Adjuvant Cht plus 1 year of treatment with trastuzumab Added or not to pertuzumab | 3-year iDFS rate: 94.1% vs. 93.2%.(HR = 0.81 (95% CI, 0.66 to 1.00); p = 0.045) in favor of pertuzumab | Higher levels of TILs associated with increased iDFS in pts treated with dual HER2 blockade. (HR 0.35 (95% CI 0.19–0.65); p = 0.003) | |
| NEOADJUVANT | NEOALTTO De Azambuja et al., 2014 [29,30] | Phase III RCT | 455 early stage HER2+ BC pts | Neodjuvant Trastuzumab, lapatinib, or the combination of both for 6 weeks followed by 12 week taxane + trastuzumab therapy followed by 3 cycles of fluorouracil, epirubicin, and cyclo- phosphamide after surgery | PCR (44% within the combination arm vs. 27% and 20% with trastuzumab and lapatinib, respectively) EFS: No difference between the lapatinib and trastuzumab groups (p = 0.81), nor the combination or trastuzumab groups (p = 0.33) | High TILs at diagnosis 2 was positively related to both pCR (nonlinear) and better EFS (linear) regardless of treatment group 3 |
| PAMELA Llombart-Cussac et al., 2017 [31,32] | Phase II RCT | 151 early stage HER2+ BC pts regardless of hormone receptor | Neoadjuvant lapatinib and trastuzumab for 18 weeks | pCR prediction by HER2-enriched subtypes (41 vs. 10%; p = 0·0004) | TILs at day 15, but not baseline TILs, were significantly associated with pCR | |
| CHER-LOB guarneri et al., 2012 [33,34] | Phase II RCT | 121 early stage HER2+ BC pts | Neoadjuvant chemotherapy plus trastuzumab, lapatinib, or both. | pCR from Cht plus Trastuzumab: 25%; Lapatinib: 27.2%; Trastuzumab + lapatinib: 44% | pCR rates were significantly higher in High TILs group compared to Low-TILs cases (59% vs. 27%, p = 0.011) | |
| GEPARSIXTO von Minckwitz et al., 2015 [35,36] | Phase II RCT | 293 early stage locally advanced triple negative (157 pts) and HER2+ (136 pts) BC | HER2+ cohort: Neoadjuvant trastuzumab plus lapatinib with or without carboplatin | pCR from HER2+ cohort: No differential in pCR between carboplatin and no carboplatin group (45% vs. 50%; p = 0.58) | In HER2+ pts, pCR rates ≥ 75% were observed in LPBC phenotype (p = 0.006) | |
| NEOSPHERE Gianni et al., 2012 [37,38] | Phase II RCT | 417 early stage, operable or locally advanced HER2+ BC pts | Neoadjuvant (A)Trastuzumab plus docetaxel (B) Pertuzumab, trastuzumab plus docetaxel (C) Pertuzumab and trastuzumab (D) pertuzumab plus docetaxel | pCR: 45·8% from group B compared with groups A (29%), C (16%) or D (24%) | Low-TILs group: lowest pCR rate (4.3%) Intermediate-TILs group: 26.9% -LPBC (26.7%) 4 | |
| NeoLath Tokunaga et al., 2021 [39,40] | Phase II RCT | 215 early stage, operable or locally advanced HER2+ BC pts | Neoadjuvant lapatinib and trastuzumab followed by either standard or prolonged course of lapatinib and trastuzumab plus weekly paclitaxel | CpCR- No difference between standard or prolonged course | NRP-1 6 + TILs significantly associated with pCR (OR 1.08; (95% CI, 1.04–1.13); p < 0.0001) | |
| Meta-analysis Solina et al., 2017 [41] | Included trials: CHER-LOB, GeparQuattr, GeparQuinto, Geparsixto, NeoALTTO Total: 1256 pts | Significant association between high pre-treatment TIL levels and pCR rates (OR 2.46; (95% CI, 1.36–4.43); p = 0.003) 5 | ||||
| ADVANCED | CLEOPATRA Swain et al., 2020 [42,43] | Phase III RCT | 808 locally recurrent, unresectable or metastatic previously untreated HER2+ patients | Docetaxel plus trastuzumab with or without pertuzumab as first-line treatment | PFS benefit from adding pertuzumab: 12.4 vs. 18.7 months (HR 0.69; 95% CI, 0.58–0.81) | Each 10% increase in TILs was related to longer OS (HR 0.89 (95% CI, 0.83–0.96); p = 0.0014) No significant association between TILs and PFS (p = 0.063). |
| MA.31 Gelmon et al., 2015 [44,45] | Phase III RCT | 652 locally recurrent, unresectable or metastatic previously untreated HER2+ patients | Taxane plus trastuzumab or lapatinib as first-line treatment | PFS benefit from trastuzumab vs. lapatinib: 11.3 vs. 9 months; (HR 1.37 (95% CI, 1.13–1.65); p = 0.001) | Low levels of pre-existing CD8+ infiltrates were related to better benefit from trastuzumab compared to lapatinib | |
| KATE2 Emens et al., 2020 [46] | Phase II RCT | 330 HER2+ metastatic patients previously treated with trastuzumab and a taxane | T-DM1 with or without Atezolizumab | PFS. No significant benefit from the addition of Atezolizumab (p = 0.33) | Pts with TILs > 5% had non-significant PFS improvement (HR = 0·62; CI, 0.37–1.03) | |
| PANACEA Loi et al., 2019 [47] | Phase Ib/II single-arm trial | 61 HER2+ metastatic patients at progression to trastuzumab-based therapy | Phase II: pembrolizumab plus trastuzumab | ORR in PD-L1 population (15%) | A higher number of TILs was associated with responders/disease control (p = 0.006) |
| Setting | Study | Phase | Population | Intervention | Primary Endpoint | Results |
|---|---|---|---|---|---|---|
| Early stage | IMpassion050 [109] | III | 226 high-risk HER2+ BC | Standard neoadjuvant treatment with or without Atezolizumab | pCR | No significant benefit from the addition of Atezolizumab (p = 1.0) in the ITT population nor in PD-L1+ population |
| Metastatic disease | KATE2 [46] | Phase II RCT | 330 HER2+ metastatic patients previously treated with trastuzumab and a taxane | T-DM1 with or without Atezolizumab | PFS | No significant benefit from the addition of Atezolizumab (p = 0.33) |
| PANACEA [47] | Single arm phase Ib/II trial | 61 HER2+ metastatic patients at progression to trastuzumab-based therapy | Phase II: pembrolizumab plus trastuzumab | ORR in PD-L1+ population | 6 PD-L1-positive patients achieved an objective response (15%, 90% CI 7–29) | |
| JAVELIN Solid Tumour trial [110] | Phase Ib | 168 MBC pts independently of subtype (15.5% HER2+) | Avelumab monotherapy | Confirmed BOR | 3% overall. No HER2+ pts responding to Avelumab 1 | |
| CCTG IND.229 [111] | Phase Ib | 14 HER2+ MBC pts previously treated with CT and anti-HER2 blockade | Durvalumab and trastuzumab | Safety and efficacy | No responses (SD in 29%) | |
| DS8201-A-U105 [83] | Phase Ib | 48 pts (32 HER2+ pts-cohort 1 and 16 HER2 low-cohort 2) 2 | Nivolumab and T-Dxt | confirmed ORR | No significant benefit. ORR: 65.6% (95% CI, 46.8–81.4) for cohort 1 50% (95% CI, 24.7–75.3) for cohort 2. |
| PUBLISHED | ||||||
|---|---|---|---|---|---|---|
| Setting | Author | Drug | Nº pts | Phase | Outcomes | |
| Early | Adjuvant | Benavides et al., 2009 [118] | E75 | 150 | II | Immune response (p = 0.02) DFS (p = 0.4 low expressors; p = 0.7 overexpressors) Mortality (p = 0.08 low expressors LE; p = 0.6 overexpressors) |
| Peoples et al., 2005 [119] | E75 | 53 | I | DFS (p < 0.19) | ||
| Mittendorf et al., 2019 [120] | E75 | 758 | III | DFS (p = 0.07) | ||
| Clifton et al. (2020) [121] | E75 | 275 (HER2 IHC 1+/2+, nonamplified FISH) | IIb | 24-month DFS (p = 0.18) | ||
| Peoples et al., 2008; Mittendorf et al., 2012 [122,123] | E75 | 186 | I/II | Immunological response DFS (p = 0.04 20 months; p = 0.08 24 months) | ||
| Patil et al., 2010 [124] | E75 | 52 | I/II | Immunological response Safety | ||
| Mittendorf et al., 2016 [125] | AE37 | 144 HER2+ (3+/positive FISH) | II | DFS (p = 0.45) Immunological response | ||
| Holmes et al.2008 [126] | AE37 | 15 | I | Immune response | ||
| Mittendorf et al., 2016 [125] | GP2 | 101 | II | DFS (p = 0.43) | ||
| Clifton et al.2017 [127] | GP2 | 17 | I | Immunological response | ||
| Patel et al., 2021 [128] | GP2 | 168 (96 HER2+ 3+ After T; 72 HER2+ 1+/2+) | IIb | DFS: HER 3+: p = 0.03388 HER2 1+/2+: p = 0.41 | ||
| Valdes-Zayas et al., 2017 [129] | Anti-ganglyoside vaccine (NeuGcGM3) | 22 | III | Immunological response | ||
| Neoadjuvant | Koski et al., 2012 [130] | DC-based vaccine | 27 | I | Immunological response | |
| Lowenfeld et al., 2017 [131] | DC-based vaccine | 54 | I | Immunological response -pCR | ||
| Higgins et al., 2017 [132] | Wilms’ tumor 1 immunotherapeutic | 15 | I | Safety Immunological response | ||
| Czerniecki et al., 2007 [133] | DC-based vaccine | 13 | I | Immunological response | ||
| Metastatic | Bekaii-Saab et al., 2019 [134] | Chimeric HER-2 B-cell peptide vaccines + T-cell epitope | 49 (solid tumours) | I | Safety immunogenicity | |
| Wiedermann et al., 2010 [135] | 3 HER2-peptides plus influenza virosome | 10 (HER2+ 1+/2+ FISH negative) | I | Safety immunogenicity | ||
| Tiriveedhi et al., 2014 [136] | Mam-A plasmid DNA | 14 | I | Safety Immunogenicity Efficacy: PFS improvement at 6 months (p = 0.011) | ||
| Park et al., 2007 [137] | DC-based vaccine | 19 | I | Safety Immunogenicity | ||
| Ahlert et al. [138] | ATCV | 121 (of which 27 were MBC) | NR | Immunogenicity Efficacy. NS Survival benefit (p = 0.18) | ||
| Curigliano et al., 2016 [139] | Protein-derived (ECD+ICD + AS15) vaccine: dHER2 | 40 | I/II | Safety Response rate (2/25 PR), prolonged SD in 25% | ||
| Disis et al., 2009 [140] | Protein-derived T-cell vaccine | 22 | I/II | Safety and immunogenicity | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moragon, S.; Hernando, C.; Martinez-Martinez, M.T.; Tapia, M.; Ortega-Morillo, B.; Lluch, A.; Bermejo, B.; Cejalvo, J.M. Immunological Landscape of HER-2 Positive Breast Cancer. Cancers 2022, 14, 3167. https://doi.org/10.3390/cancers14133167
Moragon S, Hernando C, Martinez-Martinez MT, Tapia M, Ortega-Morillo B, Lluch A, Bermejo B, Cejalvo JM. Immunological Landscape of HER-2 Positive Breast Cancer. Cancers. 2022; 14(13):3167. https://doi.org/10.3390/cancers14133167
Chicago/Turabian StyleMoragon, Santiago, Cristina Hernando, Maria Teresa Martinez-Martinez, Marta Tapia, Belen Ortega-Morillo, Ana Lluch, Begoña Bermejo, and Juan Miguel Cejalvo. 2022. "Immunological Landscape of HER-2 Positive Breast Cancer" Cancers 14, no. 13: 3167. https://doi.org/10.3390/cancers14133167
APA StyleMoragon, S., Hernando, C., Martinez-Martinez, M. T., Tapia, M., Ortega-Morillo, B., Lluch, A., Bermejo, B., & Cejalvo, J. M. (2022). Immunological Landscape of HER-2 Positive Breast Cancer. Cancers, 14(13), 3167. https://doi.org/10.3390/cancers14133167