
The High Proportion of Discordant EGFR Mutations among Multiple Lung Tumors

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Selection and Clinicopathologic Review
2.2. EGFR Analysis
2.3. Sample Preparation and DNA Extraction for NGS
2.4. Library Preparation and Sequencing
2.5. Data Analysis
2.6. Assay Validation
2.7. Statistical Analysis
3. Results
3.1. Case Selection and Clinical Parameters
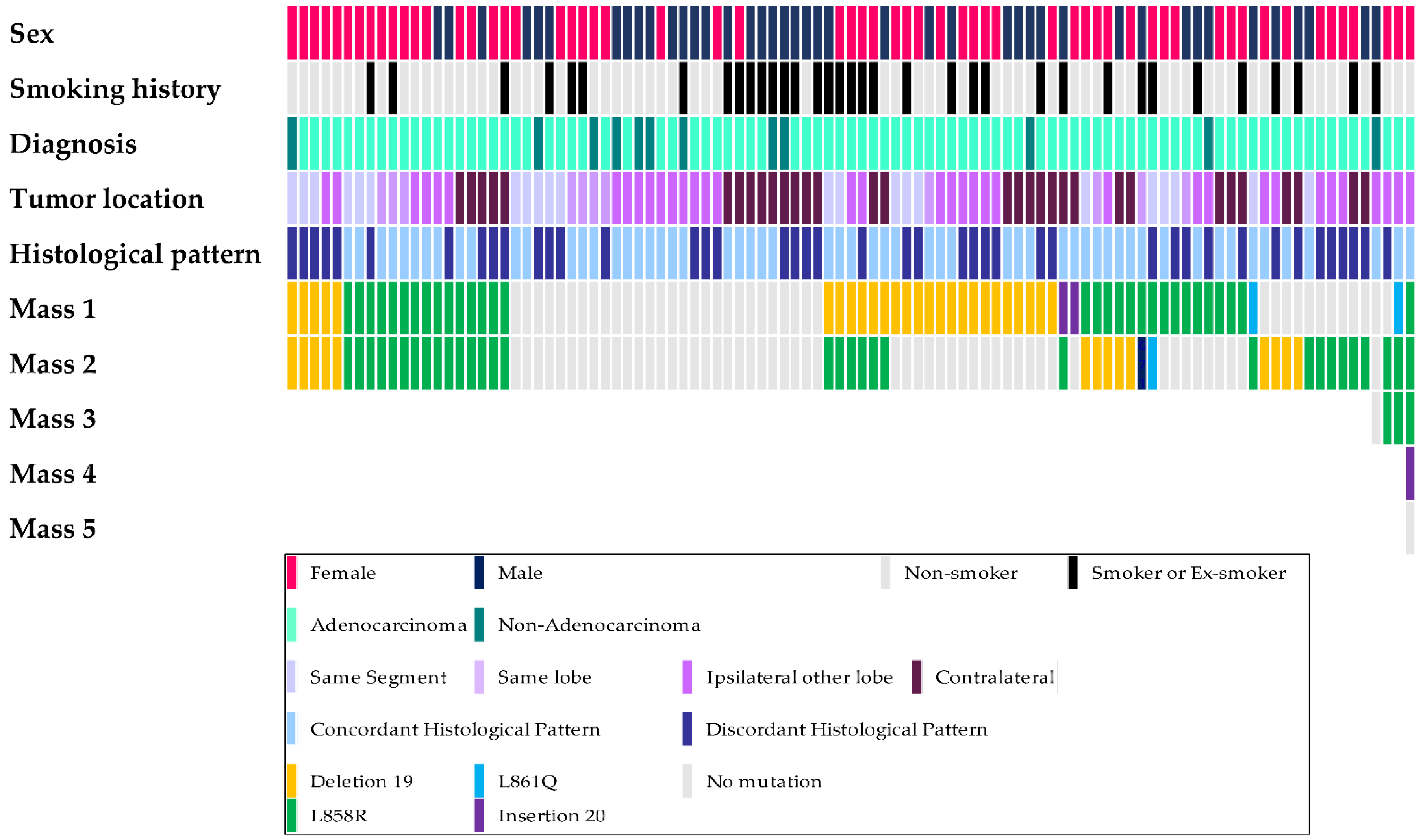
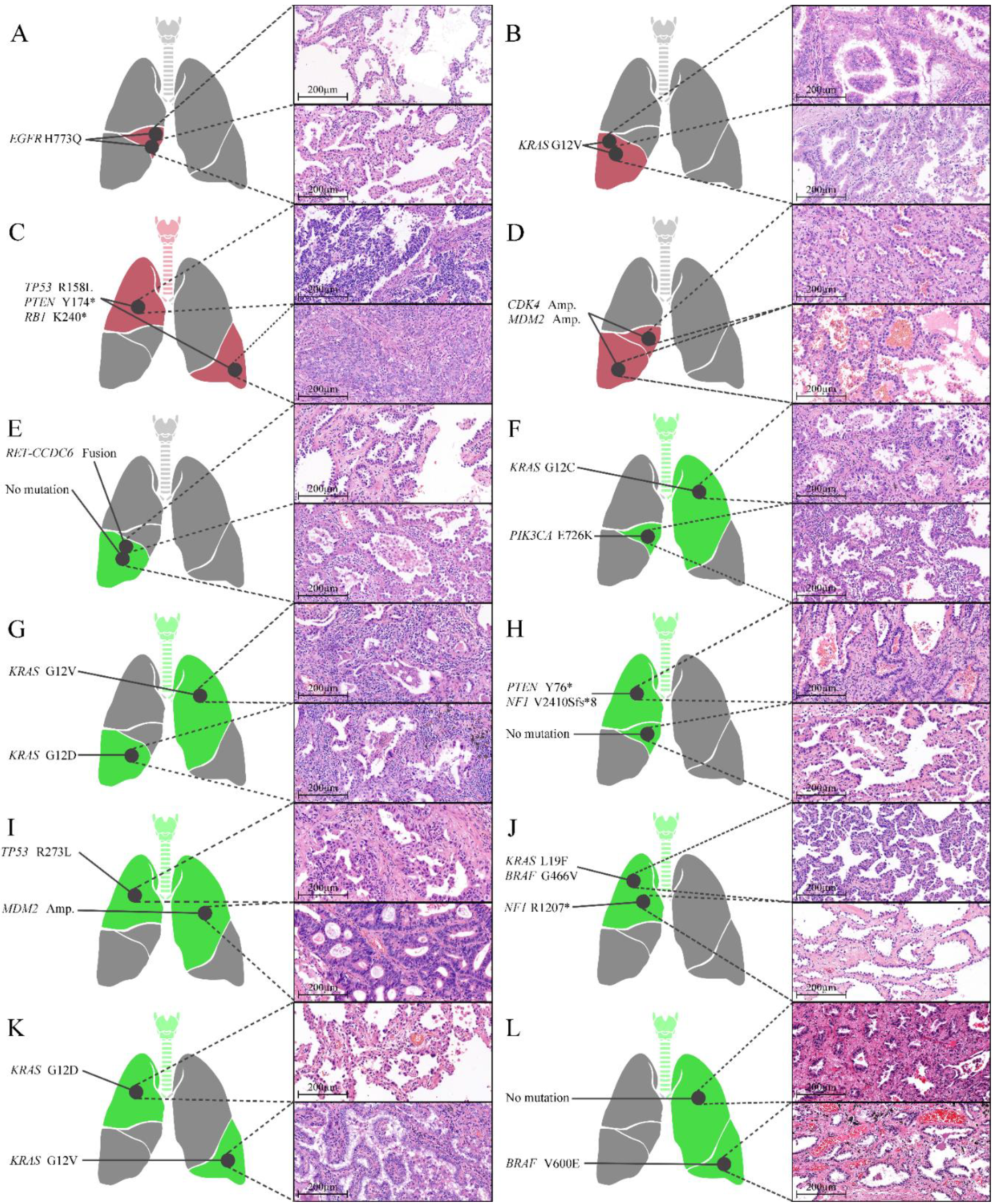
3.2. EGFR Mutation Status of Tumors
3.3. Concordance of EGFR Mutation Status
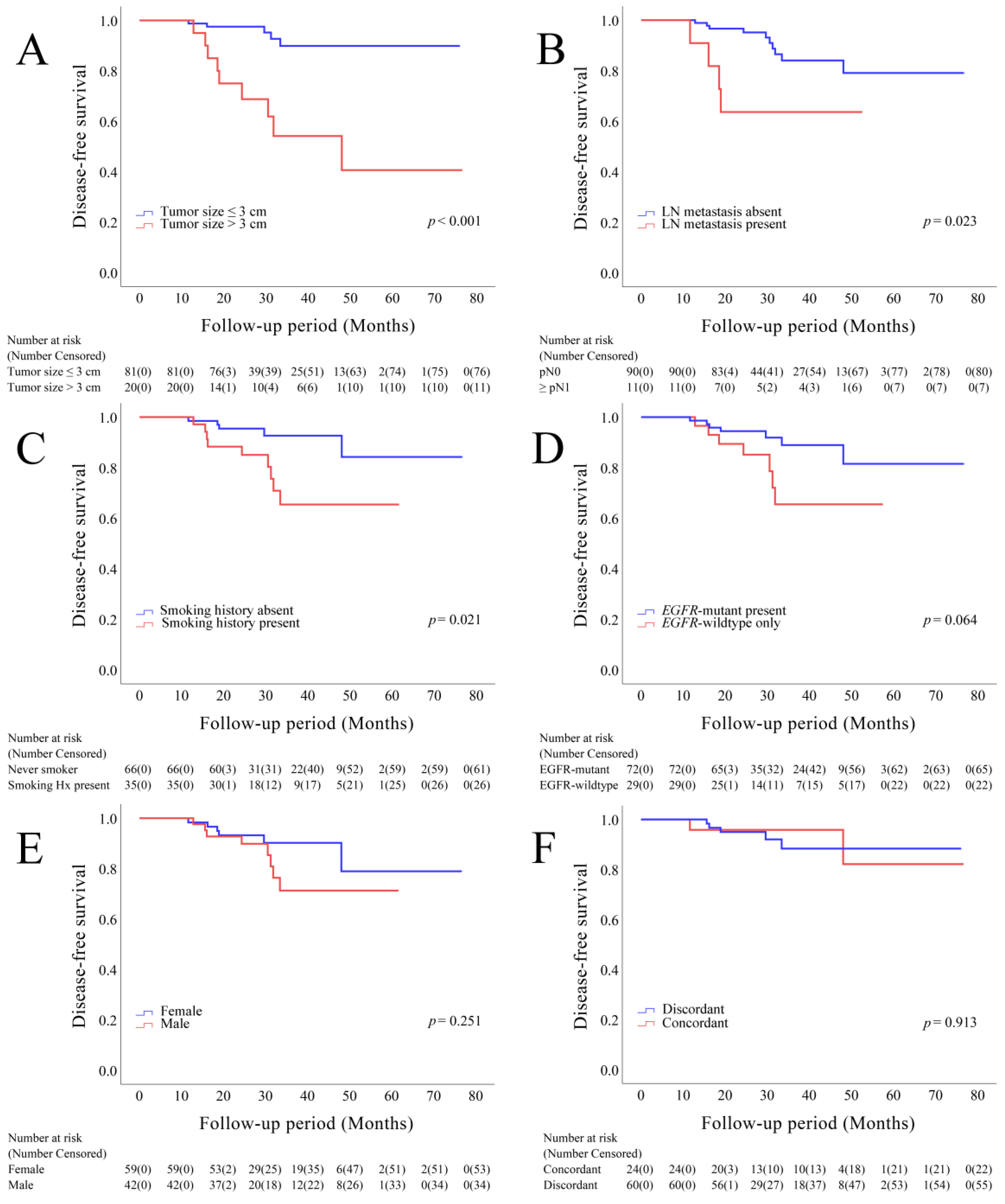
3.4. Survival Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Nakata, M.; Sawada, S.; Yamashita, M.; Saeki, H.; Kurita, A.; Takashima, S.; Tanemoto, K. Surgical treatments for multiple primary adenocarcinoma of the lung. Ann. Thorac. Surg. 2004, 78, 1194–1199. [Google Scholar] [CrossRef] [PubMed]
- Rostad, H.; Strand, T.E.; Naalsund, A.; Norstein, J. Resected synchronous primary malignant lung tumors: A population-based study. Ann. Thorac. Surg. 2008, 85, 204–209. [Google Scholar] [CrossRef] [PubMed]
- Pommier, R.F.; Vetto, J.T.; Lee, J.T.; Johnston, K.M. Synchronous non-small cell lung cancers. Am. J. Surg. 1996, 171, 521–524. [Google Scholar] [CrossRef]
- Chang, Y.-L.; Wu, C.-T.; Lee, Y.-C. Surgical treatment of synchronous multiple primary lung cancers: Experience of 92 patients. J. Thorac. Cardiovasc. Surg. 2007, 134, 630–637. [Google Scholar] [CrossRef] [PubMed]
- Slaughter, D.P.; Southwick, H.W.; Smejkal, W. Field cancerization in oral stratified squamous epithelium; clinical implications of multicentric origin. Cancer 1953, 6, 963–968. [Google Scholar] [CrossRef]
- Kitamura, H.; Kameda, Y.; Ito, T.; Hayashi, H. Atypical adenomatous hyperplasia of the lung. Implications for the pathogenesis of peripheral lung adenocarcinoma. Am. J. Clin. Pathol. 1999, 111, 610–622. [Google Scholar] [CrossRef]
- Tang, X.; Shigematsu, H.; Bekele, B.N.; Roth, J.A.; Minna, J.D.; Hong, W.K.; Gazdar, A.F.; Wistuba, I.I. EGFR tyrosine kinase domain mutations are detected in histologically normal respiratory epithelium in lung cancer patients. Cancer Res. 2005, 65, 7568–7572. [Google Scholar] [CrossRef]
- Ikeda, K.; Nomori, H.; Ohba, Y.; Shibata, H.; Mori, T.; Honda, Y.; Iyama, K.; Kobayashi, T. Epidermal growth factor receptor mutations in multicentric lung adenocarcinomas and atypical adenomatous hyperplasias. J. Thorac. Oncol. 2008, 3, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Martini, N.; Melamed, M.R. Multiple primary lung cancers. J. Thorac. Cardiovasc. Surg. 1975, 70, 606–612. [Google Scholar] [CrossRef]
- Alberts, W.M. Diagnosis and management of lung cancer executive summary: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 2007, 132, 1S–19S. [Google Scholar] [CrossRef] [PubMed]
- Shen, K.R.; Meyers, B.F.; Larner, J.M.; Jones, D.R. Special treatment issues in lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest 2007, 132, 290S–305S. [Google Scholar] [CrossRef] [PubMed]
- Girard, N.; Deshpande, C.; Lau, C.; Finley, D.; Rusch, V.; Pao, W.; Travis, W.D. Comprehensive histologic assessment helps to differentiate multiple lung primary nonsmall cell carcinomas from metastases. Am. J. Surg. Pathol. 2009, 33, 1752–1764. [Google Scholar] [CrossRef]
- Zheng, R.; Shen, Q.; Mardekian, S.; Solomides, C.; Wang, Z.-X.; Evans III, N.R. Molecular profiling of key driver genes improves staging accuracy in multifocal non–small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2020, 160, e71–e79. [Google Scholar] [CrossRef]
- Mansuet-Lupo, A.; Barritault, M.; Alifano, M.; Janet-Vendroux, A.; Zarmaev, M.; Biton, J.; Velut, Y.; Le Hay, C.; Cremer, I.; Regnard, J.F.; et al. Proposal for a Combined Histomolecular Algorithm to Distinguish Multiple Primary Adenocarcinomas from Intrapulmonary Metastasis in Patients with Multiple Lung Tumors. J. Thorac. Oncol. 2019, 14, 844–856. [Google Scholar] [CrossRef]
- Liu, C.; Liu, C.; Zou, X.; Shao, L.; Sun, Y.; Guo, Y. Next-generation sequencing facilitates differentiating between multiple primary lung cancer and intrapulmonary metastasis: A case series. Diagn. Pathol. 2021, 16, 21. [Google Scholar] [CrossRef]
- Wang, H.; Hou, J.; Zhang, G.; Zhang, M.; Li, P.; Yan, X.; Ma, Z. Clinical characteristics and prognostic analysis of multiple primary malignant neoplasms in patients with lung cancer. Cancer Gene Ther. 2019, 26, 419–426. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Nakayama, H.; Ito, H.; Yokose, T.; Tsuboi, M.; Nishii, T.; Masuda, M. Surgical Treatment for Synchronous Primary Lung Adenocarcinomas. Ann. Thorac. Surg. 2014, 98, 1983–1988. [Google Scholar] [CrossRef]
- Midha, A.; Dearden, S.; McCormack, R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: A systematic review and global map by ethnicity (mutMapII). Am. J. Cancer Res. 2015, 5, 2892–2911. [Google Scholar]
- Dearden, S.; Stevens, J.; Wu, Y.L.; Blowers, D. Mutation incidence and coincidence in non small-cell lung cancer: Meta-analyses by ethnicity and histology (mutMap). Ann. Oncol. 2013, 24, 2371–2376. [Google Scholar] [CrossRef] [PubMed]
- Kosaka, T.; Yatabe, Y.; Endoh, H.; Kuwano, H.; Takahashi, T.; Mitsudomi, T. Mutations of the epidermal growth factor receptor gene in lung cancer: Biological and clinical implications. Cancer Res. 2004, 64, 8919–8923. [Google Scholar] [CrossRef] [PubMed]
- Shigematsu, H.; Lin, L.; Takahashi, T.; Nomura, M.; Suzuki, M.; Wistuba, I.I.; Fong, K.M.; Lee, H.; Toyooka, S.; Shimizu, N.; et al. Clinical and biological features associated with epidermal growth factor receptor gene mutations in lung cancers. J. Natl. Cancer Inst. 2005, 97, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.Y.; Choi, S.-J.; Cho, J.H.; Choi, H.J.; Lee, J.; Jung, K.; Irwin, D.; Liu, X.; Lira, M.E.; Mao, M.; et al. Lung cancer in never-smoker Asian females is driven by oncogenic mutations, most often involving EGFR. Oncotarget 2015, 6, 5465–5474. [Google Scholar] [CrossRef] [PubMed]
- Tseng, C.H.; Chen, K.C.; Hsu, K.H.; Tseng, J.S.; Ho, C.C.; Hsia, T.C.; Su, K.Y.; Wu, M.F.; Chiu, K.L.; Liu, C.M.; et al. EGFR mutation and lobar location of lung adenocarcinoma. Carcinogenesis 2016, 37, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Sun, Y.; Pan, Y.; Li, C.; Shen, L.; Li, Y.; Luo, X.; Ye, T.; Wang, R.; Hu, H.; et al. Frequency of driver mutations in lung adenocarcinoma from female never-smokers varies with histologic subtypes and age at diagnosis. Clin. Cancer Res. 2012, 18, 1947–1953. [Google Scholar] [CrossRef]
- Yoshida, Y.; Shibata, T.; Kokubu, A.; Tsuta, K.; Matsuno, Y.; Kanai, Y.; Asamura, H.; Tsuchiya, R.; Hirohashi, S. Mutations of the epidermal growth factor receptor gene in atypical adenomatous hyperplasia and bronchioloalveolar carcinoma of the lung. Lung Cancer 2005, 50, 1–8. [Google Scholar] [CrossRef]
- Gazdar, A.F.; Minna, J.D. Multifocal lung cancers—Clonality vs field cancerization and does it matter? J. Natl. Cancer Inst. 2009, 101, 541–543. [Google Scholar] [CrossRef]
- Strong, M.S.; Incze, J.; Vaughan, C.W. Field cancerization in the aerodigestive tract--its etiology, manifestation, and significance. J. Otolaryngol. 1984, 13, 1–6. [Google Scholar]
- Sun, S.; Schiller, J.H.; Gazdar, A.F. Lung cancer in never smokers—A different disease. Nat. Rev. Cancer 2007, 7, 778–790. [Google Scholar] [CrossRef]
- Park, J.Y.; Jang, S.H. Epidemiology of Lung Cancer in Korea: Recent Trends. Tuberc. Respir. Dis. 2016, 79, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-C.; Won, Y.-J. The Development of the Korean Lung Cancer Registry (KALC-R). Tuberc. Respir. Dis. 2019, 82, 91–93. [Google Scholar] [CrossRef]
- Kang, H.; Park, C.-W.; Kim, W.; Song, S.-Y.; Na, K.-J.; Jeong, J.U.; Yoon, M.S.; Ahn, S.-J.; Choi, Y.-D.; Choi, C.; et al. Never-Smoker Lung Cancer Is Increasing. J. Lung Cancer 2012, 11, 89–93. [Google Scholar] [CrossRef][Green Version]
- Kerpel-Fronius, A.; Tammemägi, M.; Cavic, M.; Henschke, C.; Jiang, L.; Kazerooni, E.; Lee, C.T.; Ventura, L.; Yang, D.; Lam, S.; et al. Screening for Lung Cancer in Individuals Who Never Smoked: An International Association for the Study of Lung Cancer Early Detection and Screening Committee Report. J. Thorac. Oncol. 2022, 17, 56–66. [Google Scholar] [CrossRef]
- Zhou, F.; Zhou, C. Lung cancer in never smokers-the East Asian experience. Transl. Lung Cancer Res. 2018, 7, 450–463. [Google Scholar] [CrossRef]
- Sun, Y.; Ren, Y.; Fang, Z.; Li, C.; Fang, R.; Gao, B.; Han, X.; Tian, W.; Pao, W.; Chen, H.; et al. Lung adenocarcinoma from East Asian never-smokers is a disease largely defined by targetable oncogenic mutant kinases. J. Clin. Oncol. 2010, 28, 4616–4620. [Google Scholar] [CrossRef]
- Li, S.; Choi, Y.L.; Gong, Z.; Liu, X.; Lira, M.; Kan, Z.; Oh, E.; Wang, J.; Ting, J.C.; Ye, X.; et al. Comprehensive Characterization of Oncogenic Drivers in Asian Lung Adenocarcinoma. J. Thorac. Oncol. 2016, 11, 2129–2140. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. The AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017; pp. 431–456. [Google Scholar]
- Sun, P.L.; Seol, H.; Lee, H.J.; Yoo, S.B.; Kim, H.; Xu, X.; Jheon, S.; Lee, C.T.; Lee, J.S.; Chung, J.H. High incidence of EGFR mutations in Korean men smokers with no intratumoral heterogeneity of lung adenocarcinomas: Correlation with histologic subtypes, EGFR/TTF-1 expressions, and clinical features. J. Thorac. Oncol. 2012, 7, 323–330. [Google Scholar] [CrossRef]
- De Alava, E.; Pareja, M.J.; Carcedo, D.; Arrabal, N.; García, J.-F.; Bernabé-Caro, R. Cost-effectiveness analysis of molecular diagnosis by next-generation sequencing versus sequential single testing in metastatic non-small cell lung cancer patients from a south Spanish hospital perspective. Expert Rev. Pharmacoecon. Outcomes Res. 2022, 1–10. [Google Scholar] [CrossRef]
- Christofyllakis, K.; Bittenbring, J.T.; Thurner, L.; Ahlgrimm, M.; Stilgenbauer, S.; Bewarder, M.; Kaddu-Mulindwa, D. Cost-effectiveness of precision cancer medicine-current challenges in the use of next generation sequencing for comprehensive tumour genomic profiling and the role of clinical utility frameworks. Mol. Clin. Oncol. 2022, 16, 21. [Google Scholar] [CrossRef]
- Chen, R.L.; Sun, L.L.; Cao, Y.; Chen, H.R.; Zhou, J.X.; Gu, C.Y.; Zhang, Y.; Wang, S.Y.; Hou, W.; Lin, L.Z. Adjuvant EGFR-TKIs for Patients With Resected EGFR-Mutant Non-Small Cell Lung Cancer: A Meta-Analysis of 1283 Patients. Front. Oncol. 2021, 11, 629394. [Google Scholar] [CrossRef]
- Cheng, H.; Li, X.J.; Wang, X.J.; Chen, Z.W.; Wang, R.Q.; Zhong, H.C.; Wu, T.C.; Cao, Q.D. A meta-analysis of adjuvant EGFR-TKIs for patients with resected non-small cell lung cancer. Lung Cancer 2019, 137, 7–13. [Google Scholar] [CrossRef]
- Cheng, B.; Li, C.; Zhao, Y.; Li, J.; Xiong, S.; Liang, H.; Liu, Z.; Zeng, W.; Liang, W.; He, J. The impact of postoperative EGFR-TKIs treatment on residual GGO lesions after resection for lung cancer. Signal Transduct. Target. Ther. 2021, 6, 73. [Google Scholar] [CrossRef]
- Fenizia, F.; De Luca, A.; Pasquale, R.; Sacco, A.; Forgione, L.; Lambiase, M.; Iannaccone, A.; Chicchinelli, N.; Franco, R.; Rossi, A. EGFR mutations in lung cancer: From tissue testing to liquid biopsy. Future Oncol. 2015, 11, 1611–1623. [Google Scholar] [CrossRef]
- Lee, H.; Han, J.; Choi, Y.L. Real-World Analysis of the EGFR Mutation Test in Tissue and Plasma Samples from Non-Small Cell Lung Cancer. Diagnostics 2021, 11, 1695. [Google Scholar] [CrossRef]
- Liang, X.; Zhang, W.; Li, J.; Zhu, J.; Shao, J.; Wang, J.; Wu, H.; Dai, J.; Li, J.; Xu, J.; et al. Clinical implications of ctDNA for EGFR-TKIs as first-line treatment in NSCLC. J. Cancer. Res. Clin. Oncol. 2022. [Google Scholar] [CrossRef]
- Szpechcinski, A.; Bryl, M.; Wojcik, P.; Czyzewicz, G.; Wojda, E.; Rudzinski, P.; Duk, K.; Moes-Sosnowska, J.; Maszkowska-Kopij, K.; Langfort, R.; et al. Detection of EGFR mutations in liquid biopsy samples using allele-specific quantitative PCR: A comparative real-world evaluation of two popular diagnostic systems. Adv. Med. Sci. 2021, 66, 336–342. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Number of Patients (%) |
|---|---|
| Age (years; mean ± SD) | 65.89 ± 8.30 |
| <65 | 46 (45.6) |
| ≥65 | 55 (54.5) |
| Sex | |
| Male | 42 (41.6) |
| Female | 59 (58.4) |
| Tumor location | |
| Unilateral side, single lobe | 33 (32.7) |
| Same segment | 22 (21.8) |
| Multiple segments | 11 (10.9) |
| Unilateral side, multiple lobes | 33 (32.7) |
| Bilateral side | 35 (34.6) |
| Number of masses | |
| 2 | 97 (96.0) |
| 3 | 3 (2.9) |
| 5 | 1 (0.1) |
| Largest tumor size | |
| ≤3 cm | 81 (80.2) |
| >3 cm | 20 (19.8) |
| Lymph node metastasis | |
| Absent | 90 (89.1) |
| Present | 11 (10.9) |
| Synchronous vs. Metachronous | |
| Synchronous | 92 (91.1) |
| Metachronous | 9 (8.9) |
| Smoking history | |
| Absent | 66 (65.3) |
| Present | 35 (34.7) |
| Present smoking status | |
| Never-smoker | 66 (65.3) |
| Ex-smoker | 20 (19.8) |
| Current smoker | 15 (14.9) |
| Patient status | |
| Alive | 97 (96.0) |
| Dead | 4 (4.0) |
| Parameters | EGFR-Mutant (n = 72) | p-Value | EGFR-Wildtype (n = 29) | p-Value * | |
|---|---|---|---|---|---|
| EGFR- Mutant/Wildtype (n = 36) | EGFR- Mutant/Mutant (n = 36) | ||||
| Sex | |||||
| Male | 13 (36.1) | 9 (25.0) | 0.306 | 20 (69.0) | <0.001 |
| Female | 23 (63.9) | 27 (75.0) | 9 (31.0) | ||
| Age (years; mean ± SD) | 64.50 ± 7.54 | 65.58 ± 8.30 | 0.564 | 68.00 ± 9.04 | 0.130 |
| <65 | 19 (52.8) | 16 (44.4) | 0.479 | 11 (37.9) | 0.652 |
| ≥65 | 17 (47.2) | 20 (55.6) | 18 (62.1) | ||
| Smoking history | |||||
| Absent | 28 (77.8) | 30 (83.3) | 0.551 | 8 (27.6) | <0.001 |
| Present | 8 (22.2) | 6 (16.7) | 21 (72.4) | ||
| Smoking duration (pack–years) † | 22.13 ± 12.36 | 13.00 ± 14.57 | 0.245 | 37.81 ± 12.78 | <0.001 |
| Present smoking status | |||||
| Never-smoker | 28 (77.8) | 30 (83.3) | - | 8 (27.6) | <0.001 |
| Ex-smoker | 5 (13.9) | 5 (13.9) | 10 (34.5) | ||
| Current smoker | 3 (8.3) | 1 (2.8) | 11 (37.9) | ||
| Parameter | Same (n = 20) | Different (n = 16) | p-Value |
|---|---|---|---|
| Sex | 0.146 | ||
| Male | 3 (15.0) | 6 (37.5) | |
| Female | 17 (85.0) | 10 (62.5) | |
| Age (years) | 0.940 | ||
| <65 | 9 (45.0) | 7 (43.8) | |
| ≥65 | 11 (55.0) | 9 (56.3) | |
| History of smoking | |||
| No | 18 (90.0) | 12 (75.0) | |
| Yes | 2 (10.0) | 4 (25.0) | 0.374 |
| Present smoking status | |||
| Never-smoker | 18 (90.0) | 12 (75.0) | |
| Ex-smoker | 2 (10.0) | 3 (18.8) | |
| Current smoker | 0 (0.0) | 1 (6.3) | 0.175 |
| Largest tumor size | 0.455 | ||
| ≤3 cm | 16 (80.0) | 14 (87.5) | |
| >3 cm | 4 (20.0) | 2 (12.5) | |
| Lymph node metastasis | 0.053 | ||
| Absent | 15 (75.0) | 16 (100.0) | |
| Present | 5 (25.0) | 0 (0.0) | |
| Tumor location | |||
| Unilateral side, same lobe | 9 (45.0) | 7 (43.8) | 0.762 |
| Same segment | 6 (30.0) | 5 (31.3) | |
| Different segment | 3 (15.0) | 2 (12.5) | |
| Unilateral side, different lobe | 6 (30.0) | 3 (18.8) | |
| Bilateral side | 5 (25.0) | 6 (37.5) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, H.; Park, J.H.; Han, J.; Shim, Y.M.; Kim, J.; Choi, Y.S.; Kim, H.K.; Cho, J.H.; Choi, Y.-L.; Kim, W.-S. The High Proportion of Discordant EGFR Mutations among Multiple Lung Tumors. Cancers 2022, 14, 3011. https://doi.org/10.3390/cancers14123011
Lee H, Park JH, Han J, Shim YM, Kim J, Choi YS, Kim HK, Cho JH, Choi Y-L, Kim W-S. The High Proportion of Discordant EGFR Mutations among Multiple Lung Tumors. Cancers. 2022; 14(12):3011. https://doi.org/10.3390/cancers14123011
Chicago/Turabian StyleLee, Hyunwoo, Jin Hee Park, Joungho Han, Young Mog Shim, Jhingook Kim, Yong Soo Choi, Hong Kwan Kim, Jong Ho Cho, Yoon-La Choi, and Wan-Seop Kim. 2022. "The High Proportion of Discordant EGFR Mutations among Multiple Lung Tumors" Cancers 14, no. 12: 3011. https://doi.org/10.3390/cancers14123011
APA StyleLee, H., Park, J. H., Han, J., Shim, Y. M., Kim, J., Choi, Y. S., Kim, H. K., Cho, J. H., Choi, Y.-L., & Kim, W.-S. (2022). The High Proportion of Discordant EGFR Mutations among Multiple Lung Tumors. Cancers, 14(12), 3011. https://doi.org/10.3390/cancers14123011