
SARS-CoV-2 Neutralizing Antibodies Kinetics Postvaccination in Cancer Patients under Treatment with Immune Checkpoint Inhibition

 ,
,  , ,
, ,  , , ,
, , ,  ,
,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Neutralizing Antibodies Detection
2.3. Outcomes
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chan, J.F.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- OurWorld in Data. Available online: https://ourworldindata.org/coronavirus-data (accessed on 26 April 2022).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Shang, J.; Ye, G.; Shi, K.; Wan, Y.; Luo, C.; Aihara, H.; Geng, Q.; Auerbach, A.; Li, F. Structural basis of receptor recognition by SARS-CoV-2. Nature 2020, 581, 221–224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef]
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Pérez Marc, G.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and Efficacy of NVX-CoV2373 COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef]
- Falsey, A.R.; Sobieszczyk, M.E.; Hirsch, I.; Sproule, S.; Robb, M.L.; Corey, L.; Neuzil, K.M.; Hahn, W.; Hunt, J.; Mulligan, M.J.; et al. Phase 3 Safety and Efficacy of AZD1222 (ChAdOx1 nCoV-19) COVID-19 Vaccine. N. Engl. J. Med. 2021, 385, 2348–2360. [Google Scholar] [CrossRef]
- Sadoff, J.; Gray, G.; Vandebosch, A.; Cárdenas, V.; Shukarev, G.; Grinsztejn, B.; Goepfert, P.A.; Truyers, C.; Fennema, H.; Spiessens, B.; et al. Safety and Efficacy of Single-Dose Ad26.COV2.S Vaccine against COVID-19. N. Engl. J. Med. 2021, 384, 2187–2201. [Google Scholar] [CrossRef]
- Trougakos, I.P.; Stamatelopoulos, K.; Terpos, E.; Tsitsilonis, O.E.; Aivalioti, E.; Paraskevis, D.; Kastritis, E.; Pavlakis, G.N.; Dimopoulos, M.A. Insights to SARS-CoV-2 life cycle, pathophysiology, and rationalized treatments that target COVID-19 clinical complications. J. Biomed. Sci. 2021, 28, 9. [Google Scholar] [CrossRef]
- Wang, Q.; Berger, N.A.; Xu, R. Analyses of Risk, Racial Disparity, and Outcomes Among US Patients with Cancer and COVID-19 Infection. JAMA Oncol. 2021, 7, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, H.; Mikami, T.; Chopra, N.; Yamada, T.; Chernyavsky, S.; Rizk, D.; Cruz, C. Do patients with cancer have a poorer prognosis of COVID-19? An experience in New York City. Ann. Oncol. 2020, 31, 1088–1089. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Banerjee, S.; Cervantes, A.; Garassino, M.C.; Garrido, P.; Girard, N.; Haanen, J.; Jordan, K.; Lordick, F.; Machiels, J.P.; et al. Managing cancer patients during the COVID-19 pandemic: An ESMO multidisciplinary expert consensus. Ann. Oncol. 2020, 31, 1320–1335. [Google Scholar] [CrossRef] [PubMed]
- Liontos, M.; Kastritis, E.; Markellos, C.; Migkou, M.; Eleftherakis-Papaiakovou, E.; Koutsoukos, K.; Gavriatopoulou, M.; Zagouri, F.; Psaltopoulou, T.; Terpos, E.; et al. Continuing Cancer Therapy through the Pandemic While Protecting Our Patients: Results of the Implementation of Preventive Strategies in a Referral Oncology Unit. Cancers 2021, 13, 763. [Google Scholar] [CrossRef]
- CDC. Available online: https://www.cdc.gov/cancer/survivors/staying-well-during-covid-19.htm (accessed on 26 April 2022).
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef]
- Clinicaltrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT04743388 (accessed on 26 April 2022).
- Terpos, E.; Zagouri, F.; Liontos, M.; Sklirou, A.D.; Koutsoukos, K.; Markellos, C.; Briasoulis, A.; Papanagnou, E.D.; Trougakos, I.P.; Dimopoulos, M.A. Low titers of SARS-CoV-2 neutralizing antibodies after first vaccination dose in cancer patients receiving checkpoint inhibitors. J. Hematol. Oncol. 2021, 14, 86. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck RWJr Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; Swanson, K.A.; et al. Safety and Immunogenicity of Two RNA-Based COVID-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Trougakos, I.P.; Terpos, E.; Zirou, C.; Sklirou, A.D.; Apostolakou, F.; Gumeni, S.; Charitaki, I.; Papanagnou, E.D.; Bagratuni, T.; Liacos, C.I.; et al. Comparative kinetics of SARS-CoV-2 anti-spike protein RBD IgGs and neutralizing antibodies in convalescent and naïve recipients of the BNT162b2 mRNA vaccine versus COVID-19 patients. BMC Med. 2021, 19, 208. [Google Scholar] [CrossRef]
- Worldometer. Available online: https://www.worldometers.info/coronavirus (accessed on 26 April 2022).
- OurWorld in Data. Available online: https://ourworldindata.org/covid-vaccinations (accessed on 27 April 2022).
- Vivarelli, S.; Falzone, L.; Grillo, C.M.; Scandurra, G.; Torino, F.; Libra, M. Cancer Management during COVID-19 Pandemic: Is Immune Checkpoint Inhibitors-Based Immunotherapy Harmful or Beneficial? Cancers 2020, 12, 2237. [Google Scholar] [CrossRef]
- Nelli, F.; Fabbri, A.; Onorato, A.; Giannarelli, D.; Silvestri, M.A.; Pessina, G.; Giron Berrios, J.R.; Virtuoso, A.; Marrucci, E.; Schirripa, M.; et al. Six month immunogenicity of COVID-19 mRNA-BNT162b2 vaccine in actively treated cancer patients: Updated results of the Vax-On study. Ann. Oncol. 2022, 33, 352–354. [Google Scholar] [CrossRef]
- Ligumsky, H.; Dor, H.; Etan, T.; Golomb, I.; Nikolaevski-Berlin, A.; Greenberg, I.; Halperin, T.; Angel, Y.; Henig, O.; Spitzer, A.; et al. Immunogenicity and safety of BNT162b2 mRNA vaccine booster in actively treated patients with cancer. Lancet Oncol. 2022, 23, 193–195. [Google Scholar] [CrossRef]
- Waldhorn, I.; Holland, R.; Goshen-Lago, T.; Shirman, Y.; Szwarcwort-Cohen, M.; Reiner-Benaim, A.; Shachor-Meyouhas, Y.; Hussein, K.; Fahoum, L.; Peer, A.; et al. Six-Month Efficacy and Toxicity Profile of BNT162b2 Vaccine in Cancer Patients with Solid Tumors. Cancer Discov. 2021, 11, 2430–2435. [Google Scholar] [CrossRef] [PubMed]
- Massarweh, A.; Eliakim-Raz, N.; Stemmer, A.; Levy-Barda, A.; Yust-Katz, S.; Zer, A.; Benouaich-Amiel, A.; Ben-Zvi, H.; Moskovits, N.; Brenner, B.; et al. Evaluation of Seropositivity Following BNT162b2 Messenger RNA Vaccination for SARS-CoV-2 in Patients Undergoing Treatment for Cancer. JAMA Oncol. 2021, 7, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Kastritis, E.; Terpos, E.; Evangelakou, Z.; Theodorakakou, F.; Fotiou, D.; Manola, M.S.; Gianniou, D.D.; Bagratuni, T.; Kanellias, N.; Migkou, M.; et al. Kinetics of anti-SARS-CoV-2 neutralizing antibodies development after BNT162b2 vaccination in patients with amyloidosis and the impact of therapy. Am. J. Hematol. 2022, 97, E27–E31. [Google Scholar] [CrossRef]
- Terpos, E.; Gavriatopoulou, M.; Ntanasis-Stathopoulos, I.; Briasoulis, A.; Gumeni, S.; Malandrakis, P.; Papanagnou, E.D.; Migkou, M.; Kanellias, N.; Kastritis, E.; et al. Booster BNT162b2 optimizes SARS-CoV-2 humoral response in patients with myeloma: The negative effect of anti-BCMA therapy. Blood 2022, 139, 1409–1412. [Google Scholar] [CrossRef]
- Lee, A.R.Y.B.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of COVID-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Clinical severity of, and effectiveness of mRNA vaccines against, COVID-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: Prospective observational study. BMJ 2022, 376, e069761. [Google Scholar] [CrossRef]
- Abu-Raddad, L.J.; Chemaitelly, H.; Ayoub, H.H.; AlMukdad, S.; Yassine, H.M.; Al-Khatib, H.A.; Smatti, M.K.; Tang, P.; Hasan, M.R.; Coyle, P.; et al. Effect of mRNA Vaccine Boosters against SARS-CoV-2 Omicron Infection in Qatar. N. Engl. J. Med. 2022, 386, 1804–1816. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a Fourth Dose of COVID-19 mRNA Vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef]
- Bar-On, Y.M.; Goldberg, Y.; Mandel, M.; Bodenheimer, O.; Amir, O.; Freedman, L.; Alroy-Preis, S.; Ash, N.; Huppert, A.; Milo, R. Protection by a Fourth Dose of BNT162b2 against Omicron in Israel. N. Engl. J. Med. 2022, 386, 1712–1720. [Google Scholar] [CrossRef] [PubMed]
- Arbel, R.; Sergienko, R.; Friger, M.; Peretz, A.; Beckenstein, T.; Yaron, S.; Netzer, D.; Hammerman, A. Effectiveness of a second BNT162b2 booster vaccine against hospitalization and death from COVID-19 in adults aged over 60 years. Nat. Med. 2022. [Google Scholar] [CrossRef] [PubMed]
- Bloomberg. Available online: https://www.bloomberg.com/news/articles/2022-01-11/repeat-booster-shots-risk-overloading-immune-system-ema-says (accessed on 26 April 2022).
- Notarte, K.I.; Ver, A.T.; Velasco, J.V.; Pastrana, A.; Catahay, J.A.; Salvagno, G.L.; Yap, E.P.H.; Martinez-Sobrido, L.; BTorrelles, J.; Lippi, G.; et al. Effects of age, sex, serostatus, and underlying comorbidities on humoral response post-SARS-CoV-2 Pfizer-BioNTech mRNA vaccination: A systematic review. Crit. Rev. Clin. Lab. Sci. 2022, 28, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Nichetti, F.; Bini, M.; Ambrosini, M.; Ottini, A.; Rametta, A.; Leporati, R.; Polastri, D.; Pircher, C.; Dotti, K.; Ferrari, L.; et al. COVID-19 risk for patients undergoing anticancer treatment at the outpatient clinic of the National Cancer Institute of Milan: The COVINT study. ESMO Open 2020, 5 (Suppl. S3), e000883. [Google Scholar] [CrossRef] [PubMed]
- Angelis, V.; Tippu, Z.; Joshi, K.; Reis, S.; Gronthoud, F.; Fribbens, C.; Okines, A.; Stanway, S.; Cottier, E.; McGrath, S.; et al. Defining the true impact of coronavirus disease 2019 in the at-risk population of patients with cancer. Eur. J. Cancer 2020, 136, 99–106. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Total Population; Median (IQR) |
|---|---|
| Age | 68.04 (62–77) |
| BMI | 26.89 (24–29) |
| Sex | |
| Male | 52 (61.18%) |
| Female | 33 (38.82%) |
| Type of Cancer | |
| Urothelial/bladder cancer | 22 (25.89%) |
| Renal cancer | 21 (24.71%) |
| Lung cancer | 20 (23.53%) |
| Endometrial cancer | 5 (5.88%) |
| Pancreatic cancer | 2 (2.35%) |
| Other | 15 (17.65%) |
| Type of Therapy | |
| Anti-PD-1 | 66 (77.65%) |
| Anti-PD-L1 | 11 (12.94%) |
| I/O combo | 8 (9.41%) |
| Comorbidities | |
| Yes | 64 (75.29%) |
| None | 13 (15.29%) |
| Missing | 8 (9.41%) |
| Type of Vaccine | |
| BNT162b2 | 61 (71.76%) |
| AZD1222 | 17 (20%) |
| mRNA-1273 | 7 (8.24%) |
| COVID-19 Infection | |
| Yes | 3 (3.53%) |
| No | 78 (91.76%) |
| Missing | 4 (4.71%) |
| Vaccine-Related Adverse Events | |
| Pain at injection site | 27 (31.76%) |
| Fatigue | 17 (20%) |
| Fever | 7 (8.24%) |
| None | 36 (42.35%) |
| Other or missing | 14 (16.47%) |
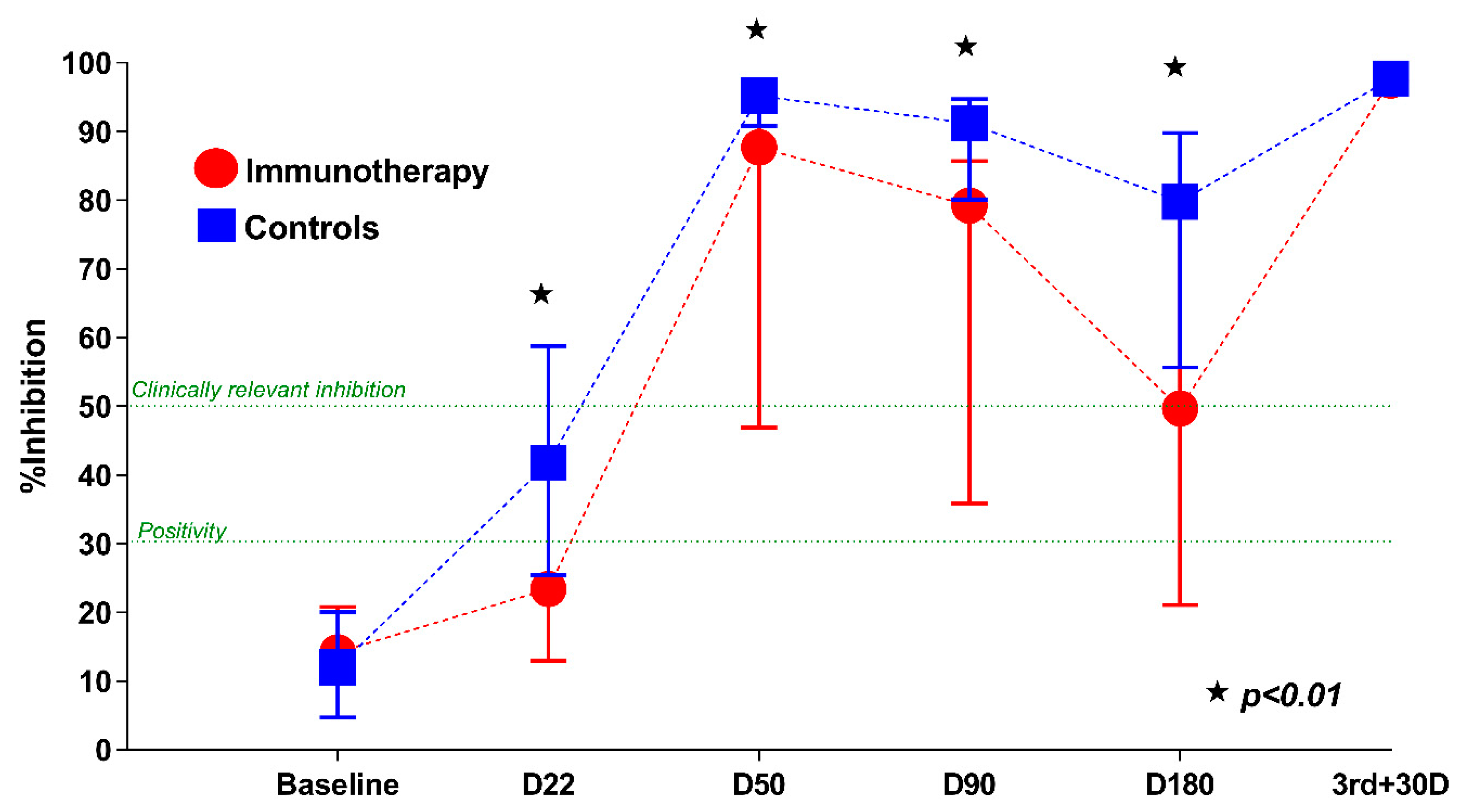
| Timepoint | Mean NAb Titers ± Standard Deviation | Median NAb Titers (IQR) |
|---|---|---|
| Baseline (D1) | 15.8 ± 9.4 | 14.2 (10.7–20.8) |
| Prior to 2nd dose (D22) | 29.1 ± 24.7 | 23.4 (13–39.8) |
| 1 month after 2nd dose (D50) | 70.7 ± 31.8 | 87.1 (46.9–95.9) |
| 3 months after 2nd dose (D90) | 61.3 ± 28.9 | 70.2 (35.9–85.7) |
| 6 months after 2nd dose (D180) | 48.4 ± 28.2 | 49.7 (21.1–78.8) |
| 1 month after 3rd dose (3rd + 30D) | 96.6 ± 2.1 | 97.5 (96.5–97.9) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Terpos, E.; Liontos, M.; Fiste, O.; Zagouri, F.; Briasoulis, A.; Sklirou, A.D.; Markellos, C.; Skafida, E.; Papatheodoridi, A.; Andrikopoulou, A.; et al. SARS-CoV-2 Neutralizing Antibodies Kinetics Postvaccination in Cancer Patients under Treatment with Immune Checkpoint Inhibition. Cancers 2022, 14, 2796. https://doi.org/10.3390/cancers14112796
Terpos E, Liontos M, Fiste O, Zagouri F, Briasoulis A, Sklirou AD, Markellos C, Skafida E, Papatheodoridi A, Andrikopoulou A, et al. SARS-CoV-2 Neutralizing Antibodies Kinetics Postvaccination in Cancer Patients under Treatment with Immune Checkpoint Inhibition. Cancers. 2022; 14(11):2796. https://doi.org/10.3390/cancers14112796
Chicago/Turabian StyleTerpos, Evangelos, Michalis Liontos, Oraianthi Fiste, Flora Zagouri, Alexandros Briasoulis, Aimilia D. Sklirou, Christos Markellos, Efthymia Skafida, Alkistis Papatheodoridi, Angeliki Andrikopoulou, and et al. 2022. "SARS-CoV-2 Neutralizing Antibodies Kinetics Postvaccination in Cancer Patients under Treatment with Immune Checkpoint Inhibition" Cancers 14, no. 11: 2796. https://doi.org/10.3390/cancers14112796
APA StyleTerpos, E., Liontos, M., Fiste, O., Zagouri, F., Briasoulis, A., Sklirou, A. D., Markellos, C., Skafida, E., Papatheodoridi, A., Andrikopoulou, A., Koutsoukos, K., Kaparelou, M., Iconomidou, V. A., Trougakos, I. P., & Dimopoulos, M.-A. (2022). SARS-CoV-2 Neutralizing Antibodies Kinetics Postvaccination in Cancer Patients under Treatment with Immune Checkpoint Inhibition. Cancers, 14(11), 2796. https://doi.org/10.3390/cancers14112796