
The Clinical Applications of Liquid Biopsies in Pediatric Brain Tumors: A Systematic Literature Review



Abstract
:Simple Summary
Abstract
1. Introduction
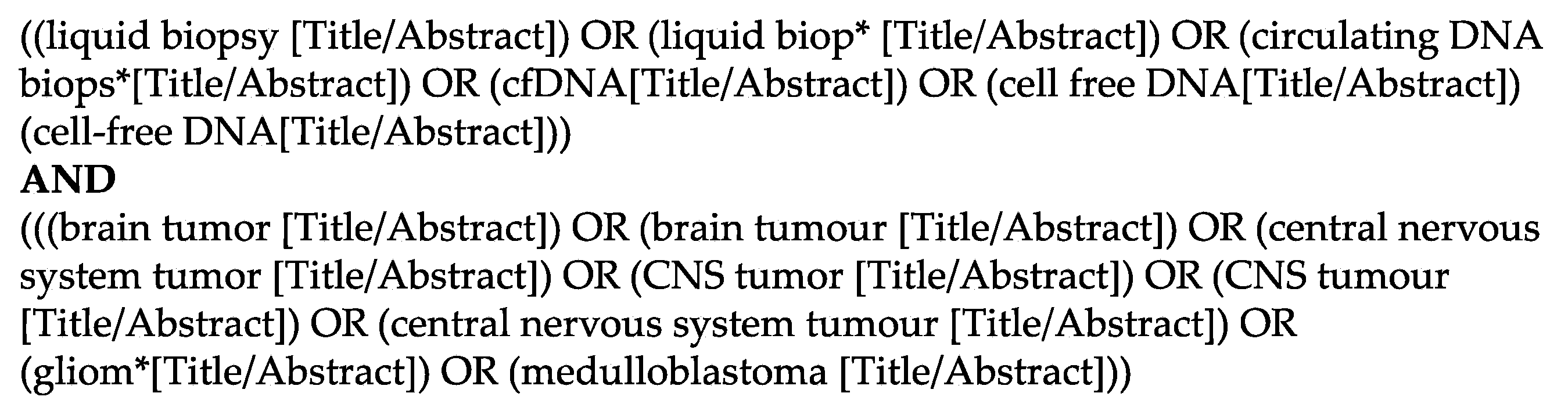
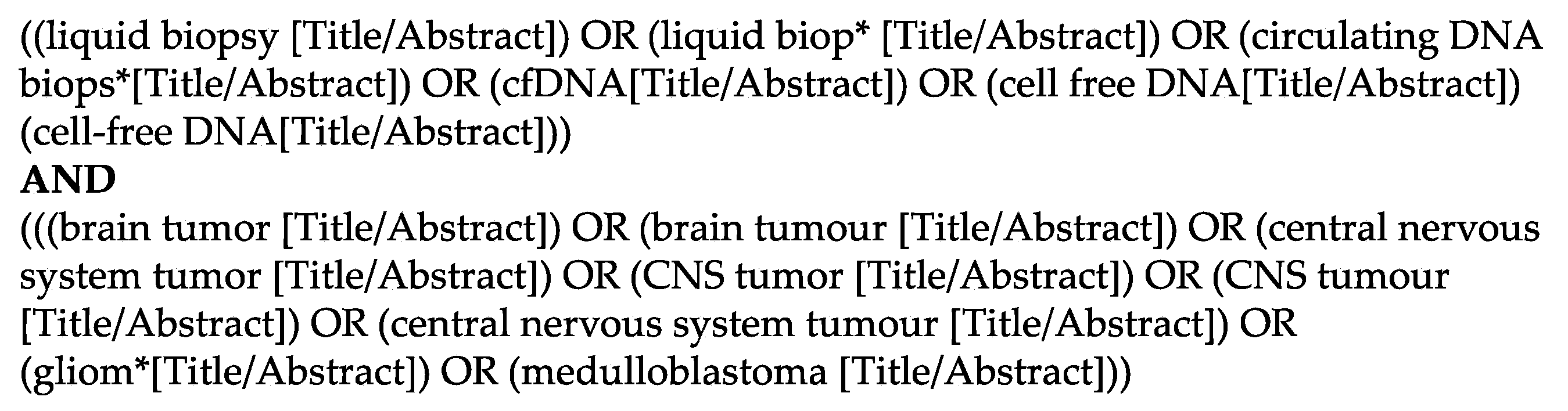
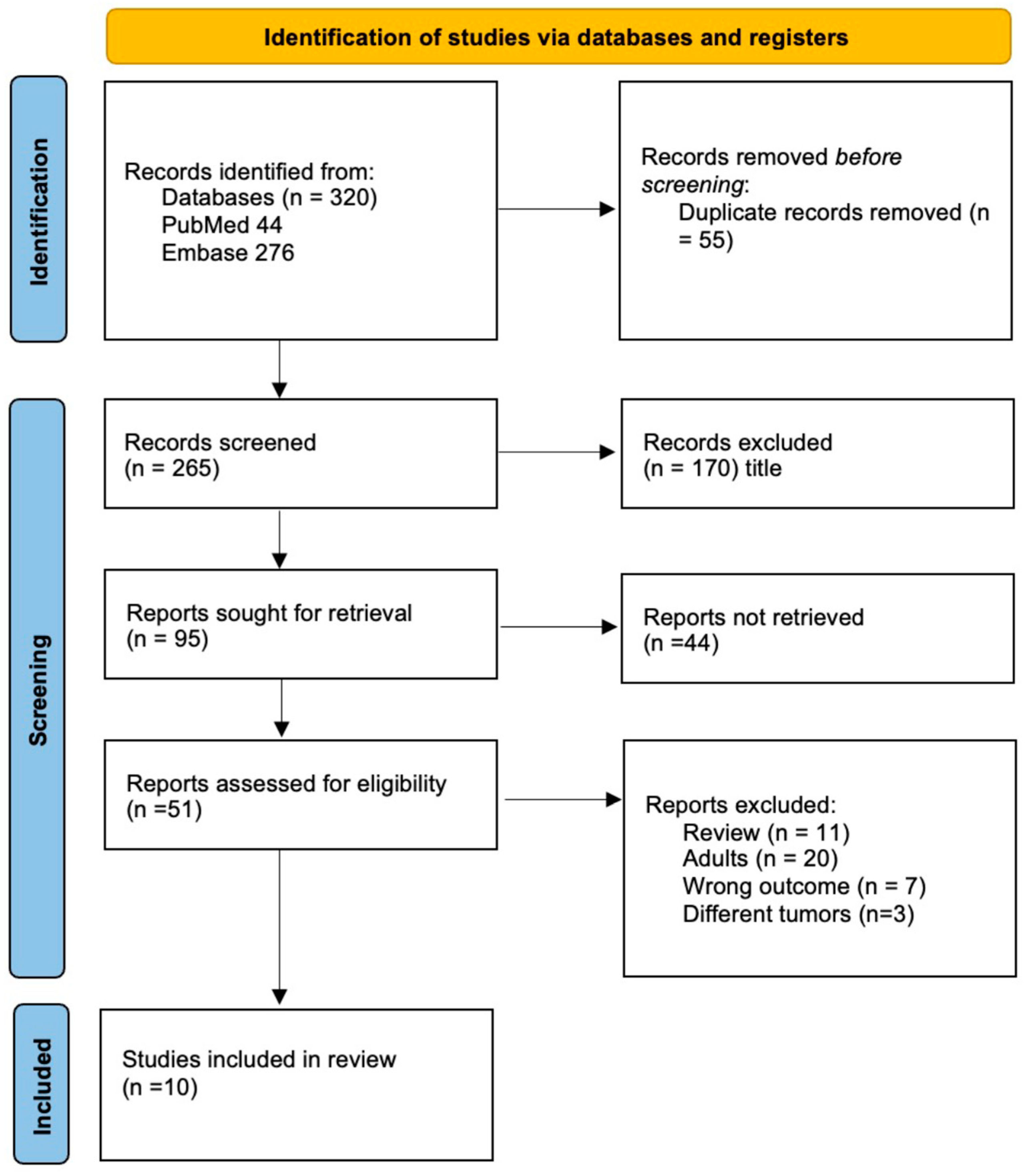
2. Materials and Methods
3. Results
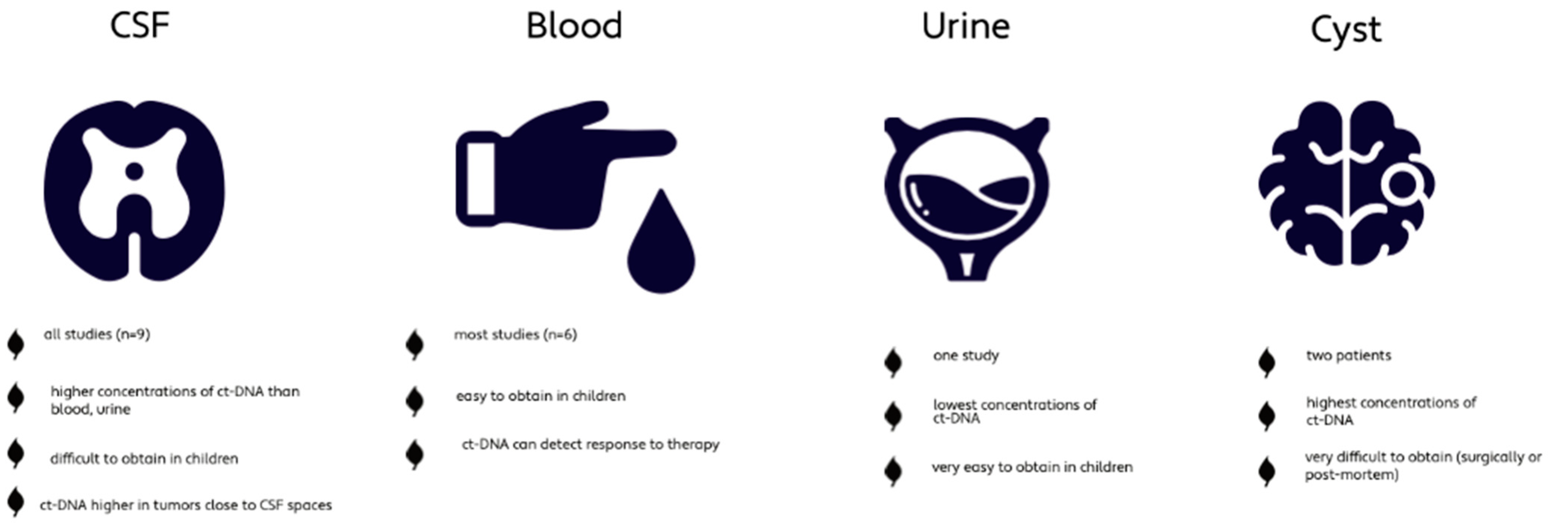
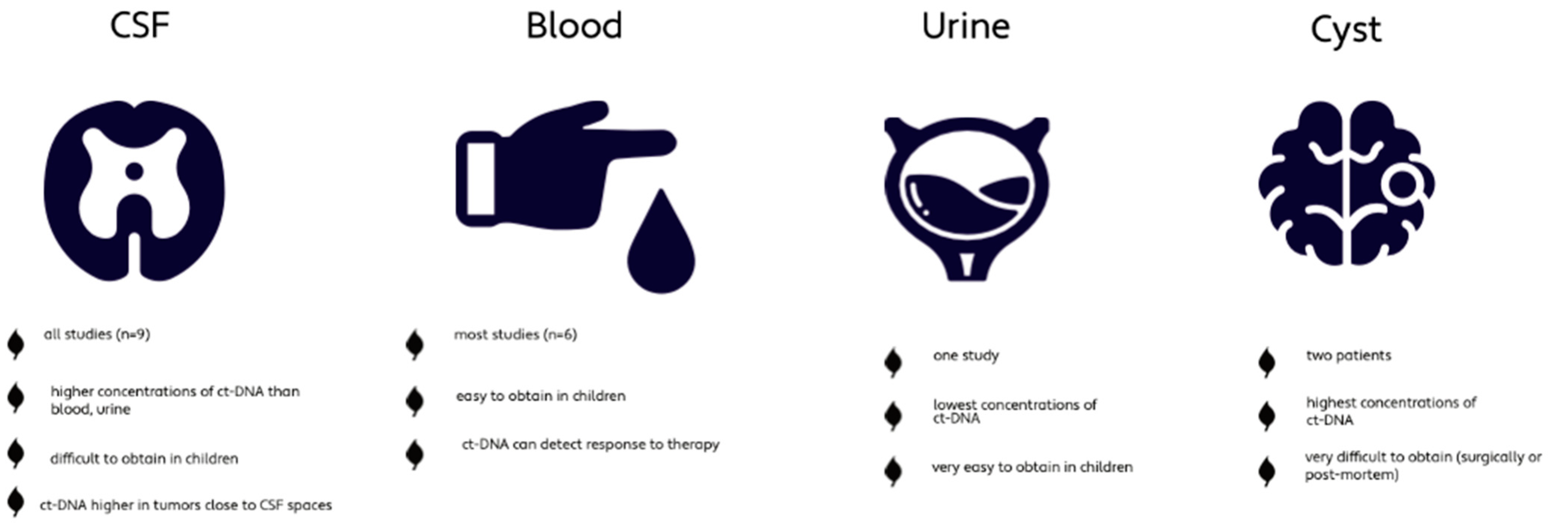
3.1. Analysis of Corporeal Fluids Used
3.2. High-Grade Glioma and Diffuse Midline Glioma
3.3. Medulloblastoma
3.4. Other Pediatric CNS Tumors
4. Discussion
4.1. Tumor Detection and Characterization with Liquid Biopsy
4.2. Disease Monitoring with Liquid Biopsy
4.3. Future Prospective of Liquid Biopsy in PBT
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Truitt, G.; Boscia, A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011–2015. Neuro-Oncol. 2018, 20, iv1–iv86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA A Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Carta, R.; Del Baldo, G.; Miele, E.; Po, A.; Besharat, Z.M.; Nazio, F.; Colafati, G.S.; Piccirilli, E.; Agolini, E.; Rinelli, M.; et al. Cancer Predisposition Syndromes and Medulloblastoma in the Molecular Era. Front. Oncol. 2020, 10, 566822. [Google Scholar] [CrossRef] [PubMed]
- Diwanji, T.P.; Engelman, A.; Snider, J.W.; Mohindra, P. Epidemiology, Diagnosis, and Optimal Management of Glioma in Adolescents and Young Adults. Adolesc. Heal. Med. Ther. 2017, 8, 99–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miklja, Z.; Pasternak, A.; Stallard, S.; Nicolaides, T.; Kline-Nunnally, C.; Cole, B.; Beroukhim, R.; Bandopadhayay, P.; Chi, S.; Ramkissoon, S.H.; et al. Molecular Profiling and Targeted Therapy in Pediatric Gliomas: Review and Consensus Recommendations. Neuro-Oncol. 2019, 21, 968–980. [Google Scholar] [CrossRef]
- Northcott, P.A.; Buchhalter, I.; Morrissy, A.S.; Hovestadt, V.; Weischenfeldt, J.; Ehrenberger, T.; Gröbner, S.; Segura-Wang, M.; Zichner, T.; Rudneva, V.A.; et al. The Whole-Genome Landscape of Medulloblastoma Subtypes. Nature 2017, 547, 311–317. [Google Scholar] [CrossRef] [Green Version]
- Northcott, P.A.; Robinson, G.W.; Kratz, C.P.; Mabbott, D.J.; Pomeroy, S.L.; Clifford, S.C.; Rutkowski, S.; Ellison, D.W.; Malkin, D.; Taylor, M.D.; et al. Medulloblastoma. Nat. Rev. Dis. Primers 2019, 5, 11. [Google Scholar] [CrossRef]
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A Summary. Neuro-Oncol. 2021, 23, 1231–1251. [Google Scholar] [CrossRef]
- Azad, T.D.; Jin, M.C.; Bernhardt, L.J.; Bettegowda, C. Liquid Biopsy for Pediatric Diffuse Midline Glioma: A Review of Circulating Tumor DNA and Cerebrospinal Fluid Tumor DNA. Neurosurg. Focus 2020, 48, E9. [Google Scholar] [CrossRef] [Green Version]
- Bounajem, M.T.; Karsy, M.; Jensen, R.L. Liquid Biopsies for the Diagnosis and Surveillance of Primary Pediatric Central Nervous System Tumors: A Review for Practicing Neurosurgeons. Neurosurg. Focus 2020, 48, E8. [Google Scholar] [CrossRef] [Green Version]
- Bonner, E.R.; Bornhorst, M.; Packer, R.J.; Nazarian, J. Liquid Biopsy for Pediatric Central Nervous System Tumors. Npj Precis. Onc. 2018, 2, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ignatiadis, M.; Lee, M.; Jeffrey, S.S. Circulating Tumor Cells and Circulating Tumor DNA: Challenges and Opportunities on the Path to Clinical Utility. Clin. Cancer Res. 2015, 21, 4786–4800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, A.P.Y.; Smith, K.S.; Kumar, R.; Paul, L.; Bihannic, L.; Lin, T.; Maass, K.K.; Pajtler, K.W.; Chintagumpala, M.; Su, J.M.; et al. Serial Assessment of Measurable Residual Disease in Medulloblastoma Liquid Biopsies. Cancer Cell 2021, 39, 1519–1530.e4. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, E.; Proszek, P.; Pericoli, G.; Temelso, S.; Clarke, M.; Carvalho, D.M.; Mackay, A.; Marshall, L.V.; Carceller, F.; Hargrave, D.; et al. Droplet Digital PCR-Based Detection of Circulating Tumor DNA from Pediatric High Grade and Diffuse Midline Glioma Patients. Neuro-Oncol. Adv. 2021, 3, vdab013. [Google Scholar] [CrossRef]
- Panditharatna, E.; Kilburn, L.B.; Aboian, M.S.; Kambhampati, M.; Gordish-Dressman, H.; Magge, S.N.; Gupta, N.; Myseros, J.S.; Hwang, E.I.; Kline, C.; et al. Clinically Relevant and Minimally Invasive Tumor Surveillance of Pediatric Diffuse Midline Gliomas Using Patient-Derived Liquid Biopsy. Clin. Cancer Res. 2018, 24, 5850–5859. [Google Scholar] [CrossRef] [Green Version]
- Sun, Y.; Li, M.; Ren, S.; Liu, Y.; Zhang, J.; Li, S.; Gao, W.; Gong, X.; Liu, J.; Wang, Y.; et al. Exploring Genetic Alterations in Circulating Tumor DNA from Cerebrospinal Fluid of Pediatric Medulloblastoma. Sci. Rep. 2021, 11, 5638. [Google Scholar] [CrossRef]
- Rayyan—Intelligent Systematic Review. Available online: https://www.rayyan.ai/ (accessed on 16 March 2022).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, n71. [Google Scholar] [CrossRef]
- Pagès, M.; Rotem, D.; Gydush, G.; Reed, S.; Rhoades, J.; Ha, G.; Lo, C.; Fleharty, M.; Duran, M.; Jones, R.; et al. Liquid Biopsy Detection of Genomic Alterations in Pediatric Brain Tumors from Cell-Free DNA in Peripheral Blood, CSF, and Urine. Neuro-Oncol. 2022, noab299. [Google Scholar] [CrossRef]
- Li, D.; Bonner, E.R.; Wierzbicki, K.; Panditharatna, E.; Huang, T.; Lulla, R.; Mueller, S.; Koschmann, C.; Nazarian, J.; Saratsis, A.M. Standardization of the Liquid Biopsy for Pediatric Diffuse Midline Glioma Using DdPCR. Sci. Rep. 2021, 11, 5098. [Google Scholar] [CrossRef]
- Huang, T.Y.; Piunti, A.; Lulla, R.R.; Qi, J.; Horbinski, C.M.; Tomita, T.; James, C.D.; Shilatifard, A.; Saratsis, A.M. Detection of Histone H3 Mutations in Cerebrospinal Fluid-Derived Tumor DNA from Children with Diffuse Midline Glioma. Acta Neuropathol. Commun. 2017, 5, 28. [Google Scholar] [CrossRef]
- Li, J.; Zhao, S.; Lee, M.; Yin, Y.; Li, J.; Zhou, Y.; Ballester, L.Y.; Esquenazi, Y.; Dashwood, R.H.; Davies, P.J.A.; et al. Reliable Tumor Detection by Whole-Genome Methylation Sequencing of Cell-Free DNA in Cerebrospinal Fluid of Pediatric Medulloblastoma. Sci. Adv. 2020, 6, eabb5427. [Google Scholar] [CrossRef] [PubMed]
- Cantor, E.; Wierzbicki, K.; Tarapore, R.S.; Ravi, K.; Thomas, C.; Cartaxo, R.; Nand Yadav, V.; Ravindran, R.; Bruzek, A.K.; Wadden, J.; et al. Serial H3K27M Cell-Free Tumor DNA (Cf-TDNA) Tracking Predicts ONC201 Treatment Response and Progression in Diffuse Midline Glioma. Neuro-Oncol. 2022, noac030. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liu, Y.; Chen, R.; Wang, X.; Wang, Y.; Wei, J.; Zhang, K.; Zhang, C. Electrochemical Biosensing of Circulating MicroRNA-21 in Cerebrospinal Fluid of Medulloblastoma Patients through Target-Induced Redox Signal Amplification. Microchim. Acta 2022, 189, 105. [Google Scholar] [CrossRef] [PubMed]
- Diehl, F.; Schmidt, K.; Choti, M.A.; Romans, K.; Goodman, S.; Li, M.; Thornton, K.; Agrawal, N.; Sokoll, L.; Szabo, S.A.; et al. Circulating Mutant DNA to Assess Tumor Dynamics. Nat. Med. 2008, 14, 985–990. [Google Scholar] [CrossRef]
- Schiavon, G.; Hrebien, S.; Garcia-Murillas, I.; Cutts, R.J.; Pearson, A.; Tarazona, N.; Fenwick, K.; Kozarewa, I.; Lopez-Knowles, E.; Ribas, R.; et al. Analysis of ESR1 Mutation in Circulating Tumor DNA Demonstrates Evolution during Therapy for Metastatic Breast Cancer. Sci. Transl. Med. 2015, 7, 313ra182. [Google Scholar] [CrossRef] [Green Version]
- Sarkaria, J.N.; Hu, L.S.; Parney, I.F.; Pafundi, D.H.; Brinkmann, D.H.; Laack, N.N.; Giannini, C.; Burns, T.C.; Kizilbash, S.H.; Laramy, J.K.; et al. Is the Blood-Brain Barrier Really Disrupted in All Glioblastomas? A Critical Assessment of Existing Clinical Data. Neuro. Oncol. 2018, 20, 184–191. [Google Scholar] [CrossRef]
- Jahr, S.; Hentze, H.; Englisch, S.; Hardt, D.; Fackelmayer, F.O.; Hesch, R.D.; Knippers, R. DNA Fragments in the Blood Plasma of Cancer Patients: Quantitations and Evidence for Their Origin from Apoptotic and Necrotic Cells. Cancer Res. 2001, 61, 1659–1665. [Google Scholar]
- Newman, A.M.; Bratman, S.V.; To, J.; Wynne, J.F.; Eclov, N.C.W.; Modlin, L.A.; Liu, C.L.; Neal, J.W.; Wakelee, H.A.; Merritt, R.E.; et al. An Ultrasensitive Method for Quantitating Circulating Tumor DNA with Broad Patient Coverage. Nat. Med. 2014, 20, 548–554. [Google Scholar] [CrossRef]
- Ramkissoon, S.H.; Bandopadhayay, P.; Hwang, J.; Ramkissoon, L.A.; Greenwald, N.F.; Schumacher, S.E.; O’Rourke, R.; Pinches, N.; Ho, P.; Malkin, H.; et al. Clinical Targeted Exome-Based Sequencing in Combination with Genome-Wide Copy Number Profiling: Precision Medicine Analysis of 203 Pediatric Brain Tumors. NEUONC 2017, 19, now294. [Google Scholar] [CrossRef]
- Wang, Y.; Springer, S.; Zhang, M.; McMahon, K.W.; Kinde, I.; Dobbyn, L.; Ptak, J.; Brem, H.; Chaichana, K.; Gallia, G.L.; et al. Detection of Tumor-Derived DNA in Cerebrospinal Fluid of Patients with Primary Tumors of the Brain and Spinal Cord. Proc. Natl. Acad. Sci. USA 2015, 112, 9704–9709. [Google Scholar] [CrossRef] [Green Version]
- Parsons, D.W.; Li, M.; Zhang, X.; Jones, S.; Leary, R.J.; Lin, J.C.-H.; Boca, S.M.; Carter, H.; Samayoa, J.; Bettegowda, C.; et al. The Genetic Landscape of the Childhood Cancer Medulloblastoma. Science 2011, 331, 435–439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, H.; Zheng, S.; Amini, S.S.; Virk, S.M.; Mikkelsen, T.; Brat, D.J.; Grimsby, J.; Sougnez, C.; Muller, F.; Hu, J.; et al. Whole-Genome and Multisector Exome Sequencing of Primary and Post-Treatment Glioblastoma Reveals Patterns of Tumor Evolution. Genome Res. 2015, 25, 316–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.; Cazzato, E.; Ladewig, E.; Frattini, V.; Rosenbloom, D.I.S.; Zairis, S.; Abate, F.; Liu, Z.; Elliott, O.; Shin, Y.-J.; et al. Clonal Evolution of Glioblastoma under Therapy. Nat. Genet. 2016, 48, 768–776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gajjar, A.; Robinson, G.W.; Smith, K.S.; Lin, T.; Merchant, T.E.; Chintagumpala, M.; Mahajan, A.; Su, J.; Bouffet, E.; Bartels, U.; et al. Outcomes by Clinical and Molecular Features in Children with Medulloblastoma Treated with Risk-Adapted Therapy: Results of an International Phase III Trial (SJMB03). JCO 2021, 39, 822–835. [Google Scholar] [CrossRef] [PubMed]
- Hamisch, C.; Kickingereder, P.; Fischer, M.; Simon, T.; Ruge, M.I. Update on the Diagnostic Value and Safety of Stereotactic Biopsy for Pediatric Brainstem Tumors: A Systematic Review and Meta-Analysis of 735 Cases. J. Neurosurg. Pediatrics 2017, 20, 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koschmann, C.; Wu, Y.-M.; Kumar-Sinha, C.; Lonigro, R.; Vats, P.; Kasaian, K.; Cieslik, M.; Cao, X.; Anderson, B.; Frank, K.; et al. Clinically Integrated Sequencing Alters Therapy in Children and Young Adults With High-Risk Glial Brain Tumors. JCO Precis. Oncol. 2018, 2, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Soleman, J. MRI-Based Diagnosis and Treatment of Pediatric Brain Tumors: Is Tissue Sample Always Needed? Childs Nerv. Syst. 2021, 37, 1449–1459. [Google Scholar] [CrossRef]
- Li, D.; Romanski, K.; Kilgallon, M.; Speck, S.; Bowman, R.; DiPatri, A.; Alden, T.; Tomita, T.; Lam, S.; Saratsis, A.M. Safety of Ventricular Reservoir Sampling in Pediatric Posthemorrhagic Hydrocephalus Patients: Institutional Experience and Review of the Literature. J. Neurosci. Nurs. 2021, 53, 11–17. [Google Scholar] [CrossRef]
- Bin Nafisah, S.; Ahmad, M. Ommaya Reservoir Infection Rate: A 6-Year Retrospective Cohort Study of Ommaya Reservoir in Pediatrics. Childs Nerv. Syst. 2015, 31, 29–36. [Google Scholar] [CrossRef]
- Strauss, S.B.; Meng, A.; Ebani, E.J.; Chiang, G.C. Imaging Glioblastoma Posttreatment: Progression, Pseudoprogression, Pseudoresponse, Radiation Necrosis. Radiol. Clin. N. A. 2019, 57, 1199–1216. [Google Scholar] [CrossRef]
- Soleman, J.; Kozyrev, D.A.; Ben-Sira, L.; Constantini, S.; Roth, J. Management of Incidental Brain Tumors in Children: A Systematic Review. Childs Nerv. Syst. 2020, 36, 1607–1619. [Google Scholar] [CrossRef] [PubMed]
- Kozyrev, D.A.; Soleman, J.; Tsering, D.; Keating, R.F.; Hersh, D.S.; Boop, F.A.; Spennato, P.; Cinalli, G.; Tamburrini, G.; Thomale, U.-W.; et al. Pediatric Thalamic Incidentalomas: An International Retrospective Multicenter Study. J. Neurosurg. Pediatrics 2021, 29, 1–9. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Author and Year of Publication | No of Patients | Analyzed Tumor | Analyzed Corporeal Fluids | Targeted Mutations | Method of Analysis | Results |
|---|---|---|---|---|---|---|
| Pagès et al. 2022 [19] | 258 | CNS tumors (102 LGG, 35 HGG, 27 MB, 5 ATRT, 2 ependymoma, 1 pineoblasotma, 7 others) | CSF, blood, urine | multiple | Ultra-low-pass whole genome sequencing (ULP-WGS) | Low levels of ct-DNA <1%, |
| Li et al. 2021 [20] | 7 | DMG | CSF, blood | H3K27M | Digital droplet PCR (ddPCR) | Reliable detection of H2K27M mutation with liquid biopsy |
| Panditharatna et al. 2018 [15] | 48 | DMG | CSF, blood, cyst fluid | H3K27M | ddPCR | Detection of response to radiotherapy and recurrence in plasma |
| Huang et al. 2017 [21] | 11 | DMG | CSF | H3K27, H3.3G34 | Sanger sequencing for H3F3A and HIST1H3B, and Nested PCR with primers specific to H3F3A | Liquid biopsy successfully detects mutations in DMG |
| Izquierdo et al. 2021 [14] | 33 | DMG and HGG | CSF, blood, cyst fluid | H3K27, H3.3G34, BRAFV600E, G328V, IDH1, TP53, PIK3CA, MYCN | ddPCR | Successful detection of mutations in DMG |
| Cantor et al. 2022 [23] | 28 | DMG H3K27 positive | CSF, Blood | H3K27 | ddPCR | Spike in ct-DNA detects and predicts recurrence prior to imaging, distinguishes between progression and pseudo-progression |
| Liu et al. 2021 [13] | 123 | MB | CSF | CTNNB1, SUFU, KMT2D, CREBBP, KBTBD4, PT53, DDX3X, PTCH1 KDM6A | Low coverage whole genome sequencing (lcWGS) | Ct-DNA higher in metastatic disease, increase with disease progression prior to radiological progression, higher ct-DNA levels in tumors close to CSF system |
| Sun et al. 2021 [16] | 58 | MB | CSF, blood | KMT2D, KMT2C, SMARCA4, BCOR, TP53, PTCH1, EP300, NF1, SETD2, MED12, SPEN | Next-generation sequencing (NGS) | Increase in ct-DNA in disease progression |
| Li et al. 2020 [22] | 4 | MB | CSF | Methylation | Whole-genome bisulfite sequencing (WGBS) and anti–cytosine-5-methylenesulfonate (anti-CMS) immunoprecipitation sequencing (CMS-IP–seq) | Detection of different methylation patterns, tumor-specific methylation pattern changes throughout therapy and indicates response, significant association with PFS |
| Specific Mutations | Detection | Monitoring of Disease | Differentiation Progression vs. Pseudoprogression | |
|---|---|---|---|---|
| High-grade glioma (including DMG) | H3K27, H3.3G34, BRAFV600E, G328V, IDH1, TP53, PIK3CA, MYCN | Reliable detection in CSF (64–96.5%) | Response to radiotherapy (plasma) (83%) and recurrence (plasma/CSF) (60%) measurable recurrence can be detected before radiographic recurrence (50%) | Differentiation between progression/pseudoprogression/ pseudoresponse (2 patients only, 18%) |
| Medulloblastoma | CTNNB1, SUFU, KMT2D/C CREBBP, KBTBD4, PT53, DDX3X, PTCH1 KDM6A SMARCA4, BCOR, EP300, NF1, SETD2, MED12, SPEN | Reliable detection in CSF (26–85%) 62% of cytology negative CSF samples were positive for ct-DNA | Response to treatment detectable progression can be detected before radiographic progression (50%) MRD during therapy correlates with shorter PFS | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greuter, L.; Frank, N.; Guzman, R.; Soleman, J. The Clinical Applications of Liquid Biopsies in Pediatric Brain Tumors: A Systematic Literature Review. Cancers 2022, 14, 2683. https://doi.org/10.3390/cancers14112683
Greuter L, Frank N, Guzman R, Soleman J. The Clinical Applications of Liquid Biopsies in Pediatric Brain Tumors: A Systematic Literature Review. Cancers. 2022; 14(11):2683. https://doi.org/10.3390/cancers14112683
Chicago/Turabian StyleGreuter, Ladina, Nicole Frank, Raphael Guzman, and Jehuda Soleman. 2022. "The Clinical Applications of Liquid Biopsies in Pediatric Brain Tumors: A Systematic Literature Review" Cancers 14, no. 11: 2683. https://doi.org/10.3390/cancers14112683
APA StyleGreuter, L., Frank, N., Guzman, R., & Soleman, J. (2022). The Clinical Applications of Liquid Biopsies in Pediatric Brain Tumors: A Systematic Literature Review. Cancers, 14(11), 2683. https://doi.org/10.3390/cancers14112683