
Comparative Analysis of PSA Density and an MRI-Based Predictive Model to Improve the Selection of Candidates for Prostate Biopsy

 , , , , , , ,
, , , , , , ,  and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design, Setting and Participants
2.2. Intervention
2.3. MRI Technique and Evaluation
2.4. Prostate Biopsy Procedure
2.5. Pathologic Analysis and csPCa Definition
2.6. Endpoint Measurements
2.7. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
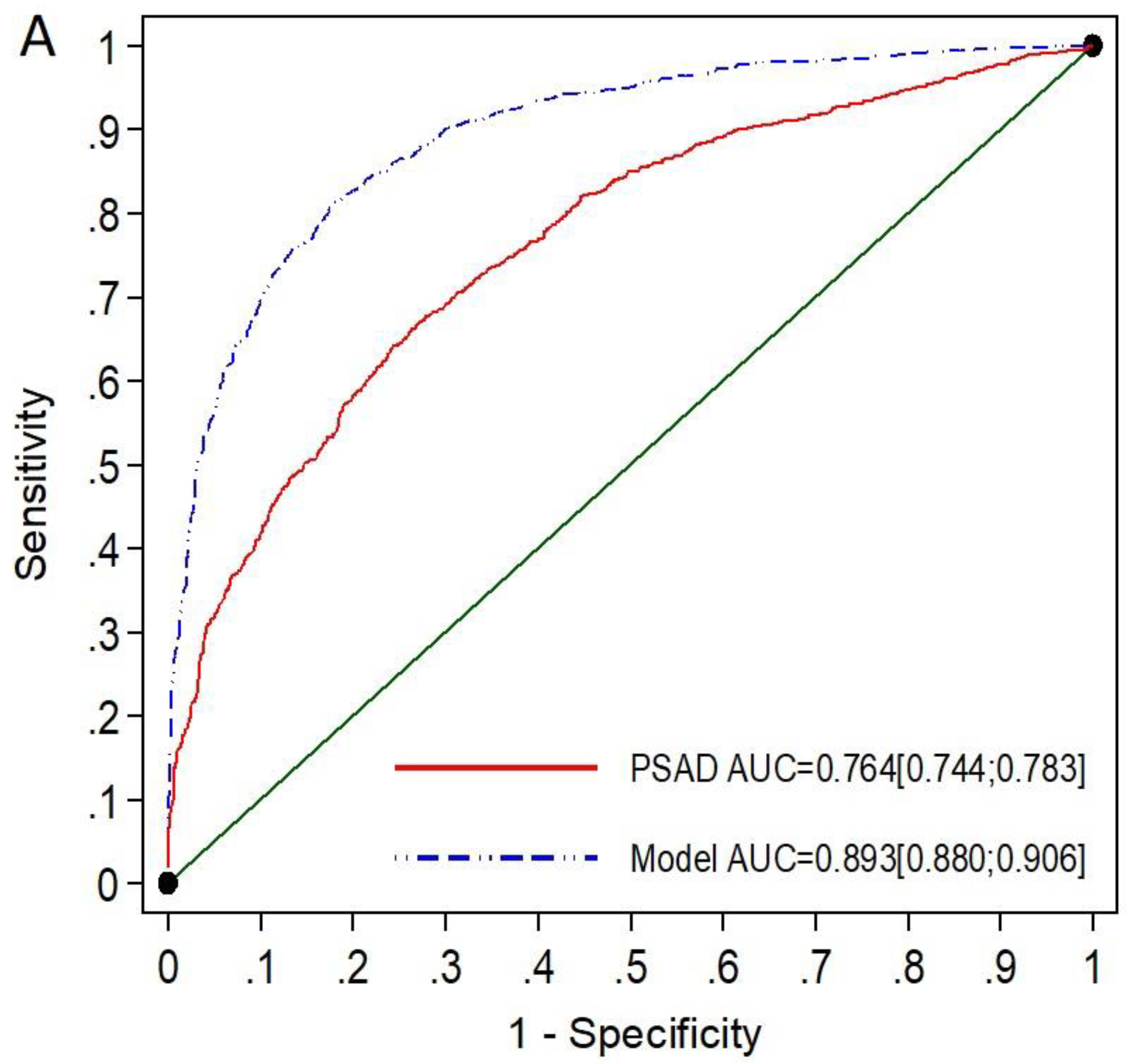
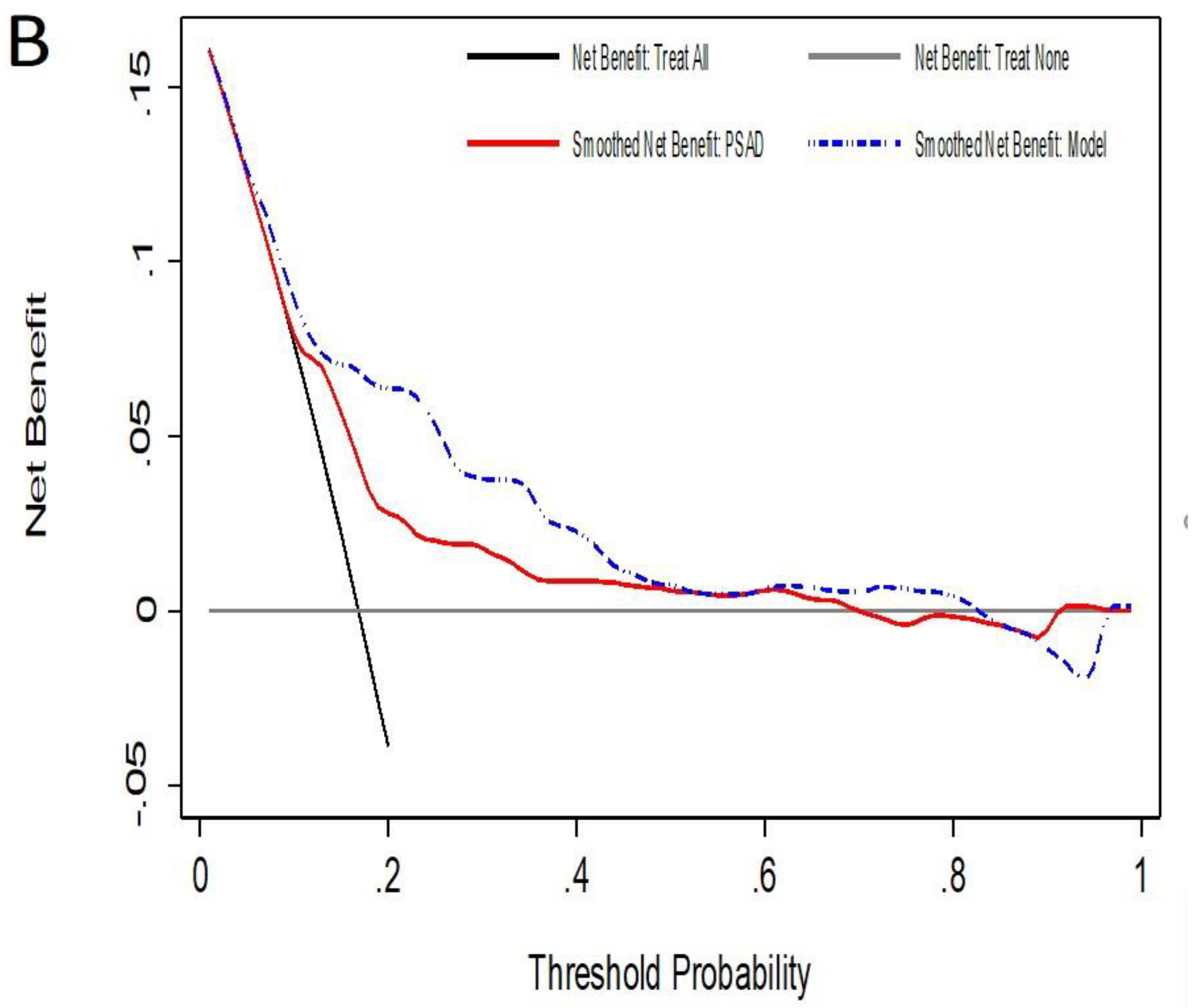
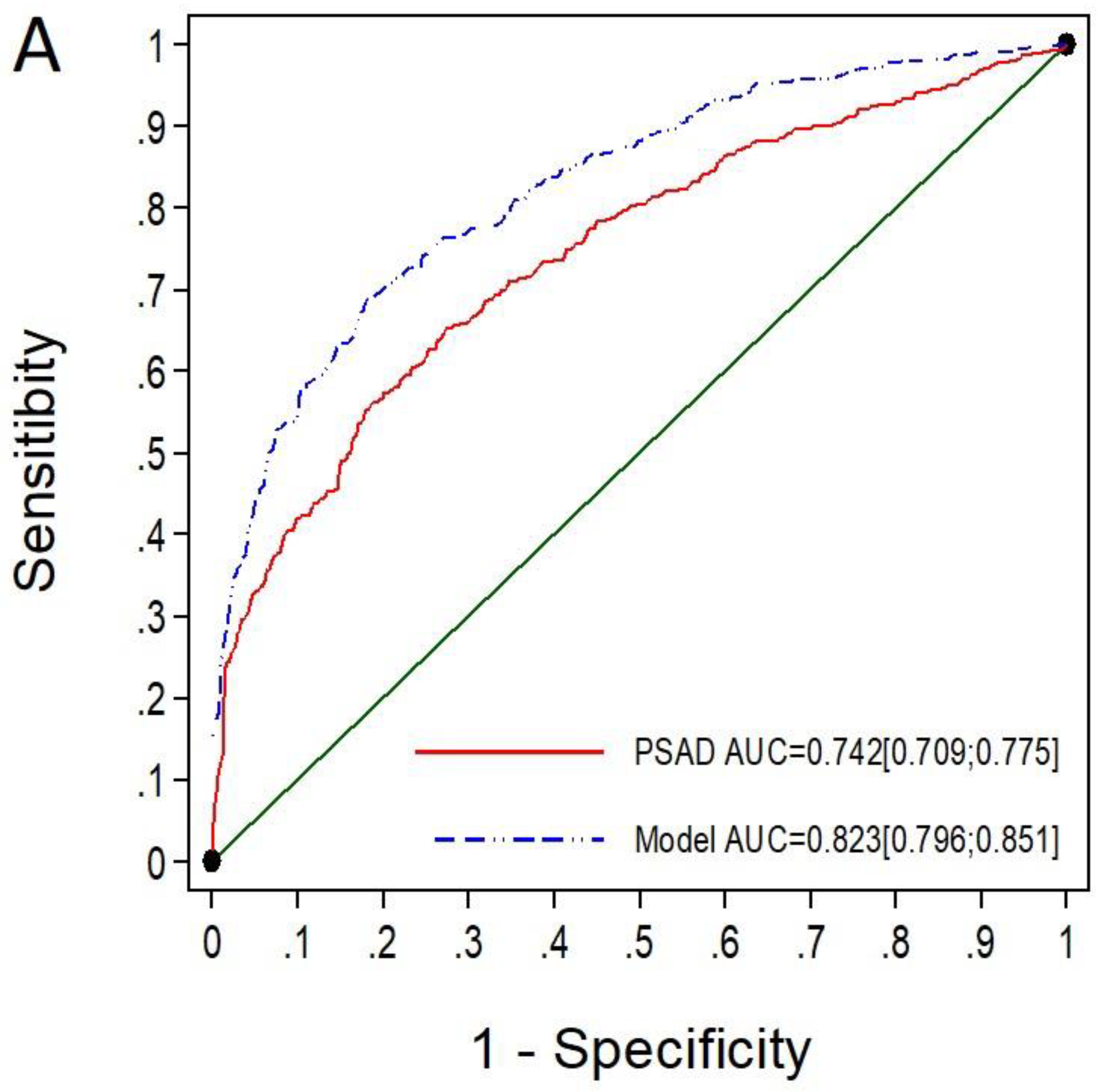
3.2. Performance of mPSAD and MRI-PMbdex in the Entire Population
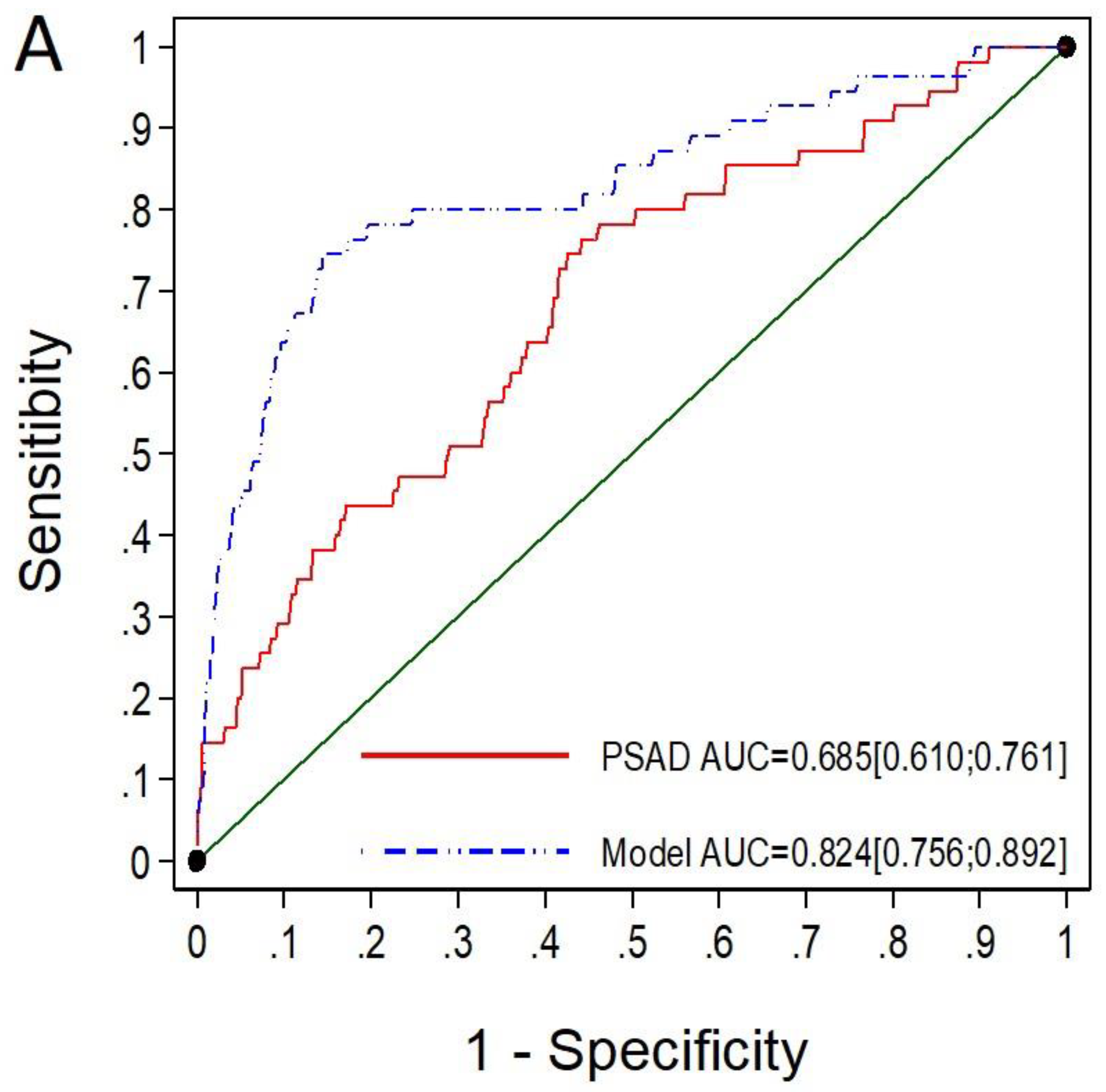
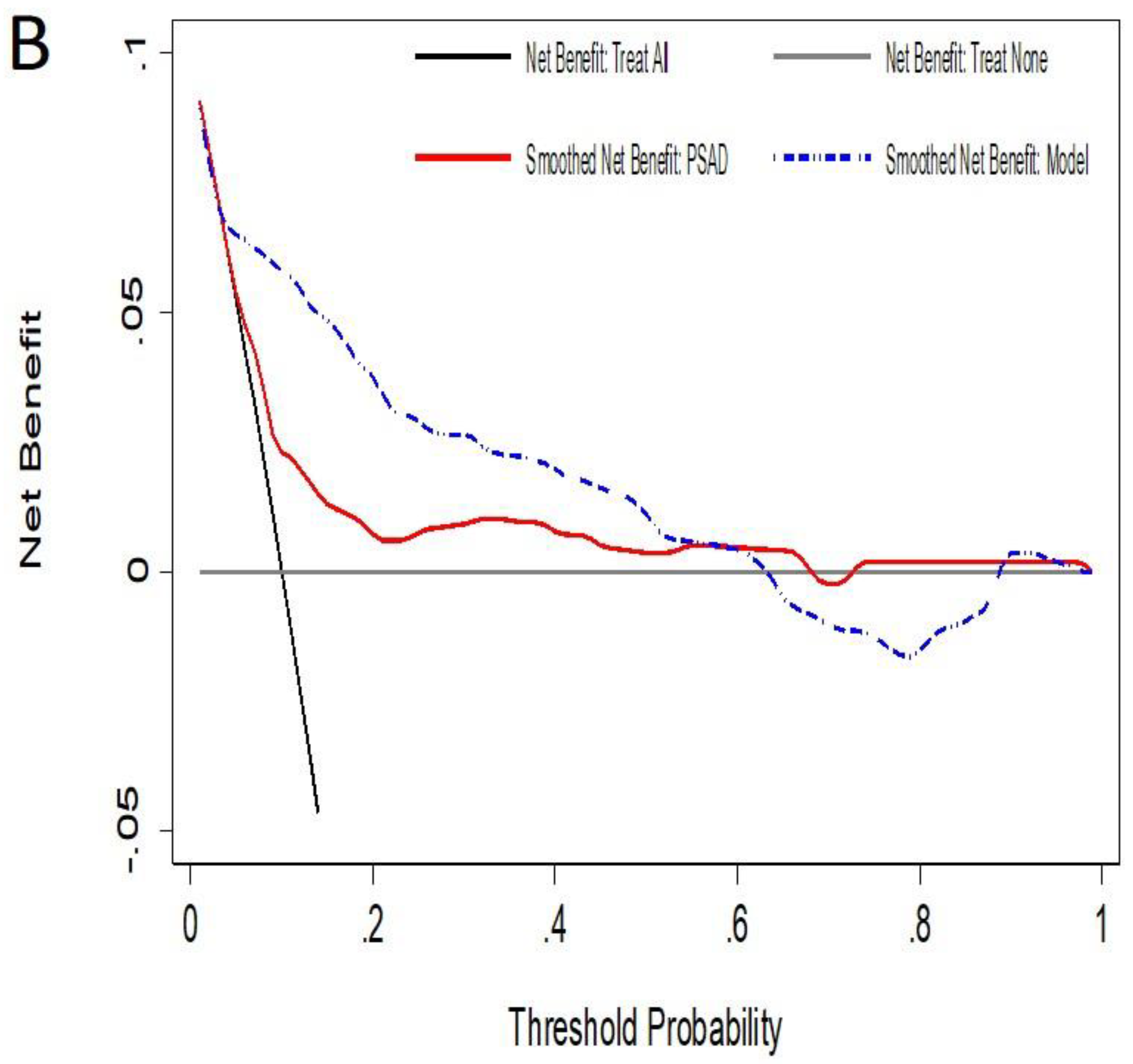
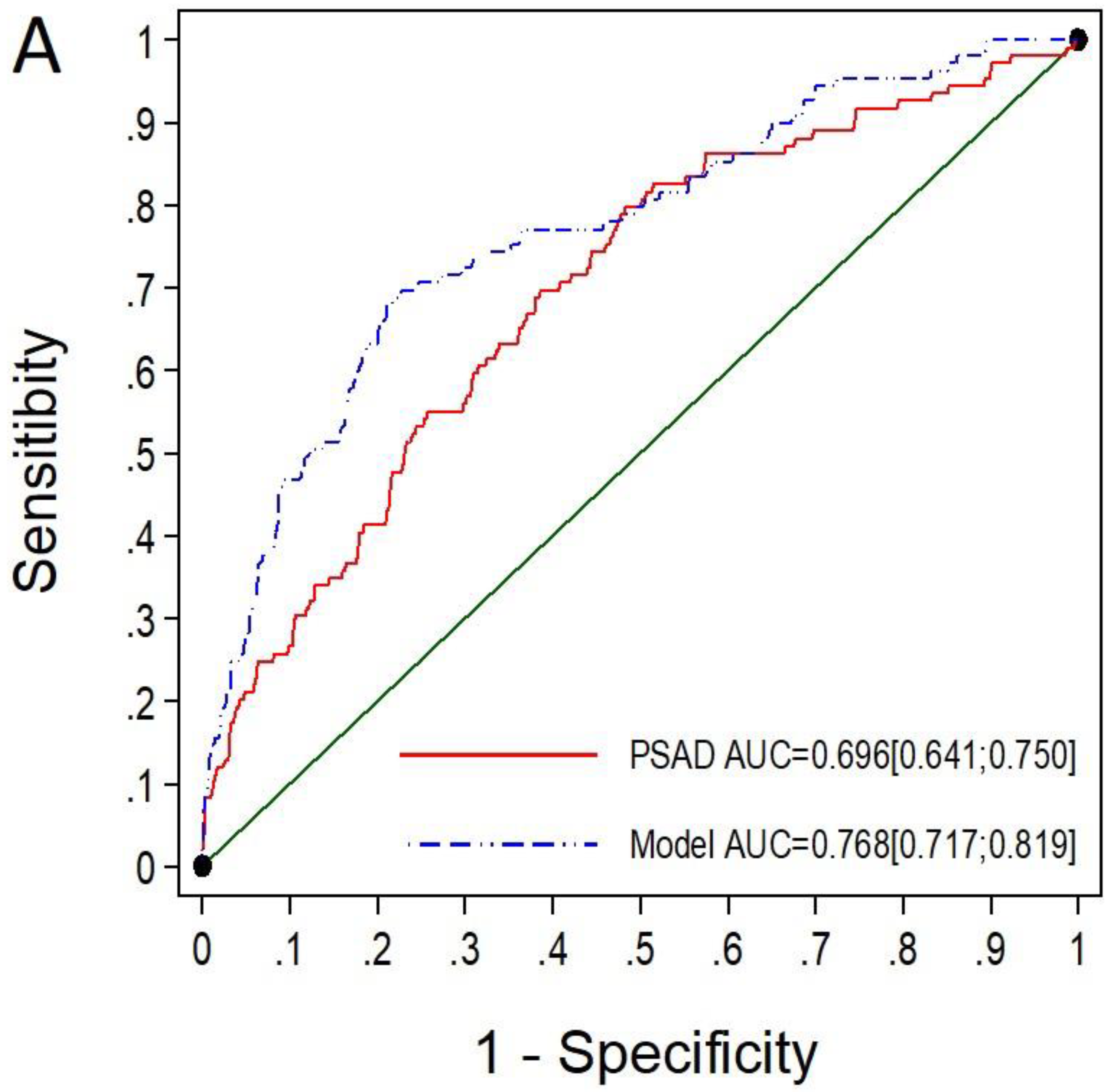
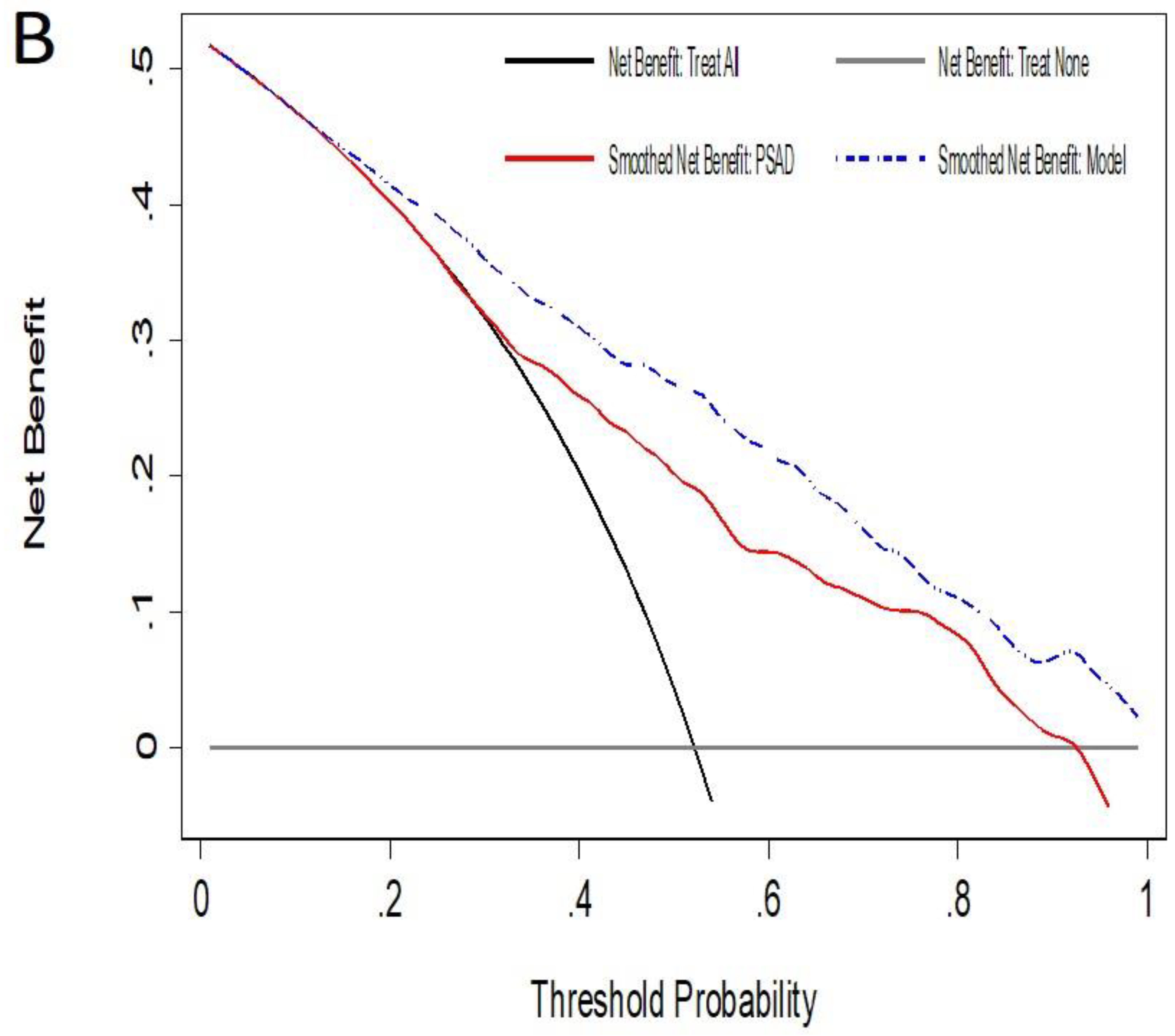
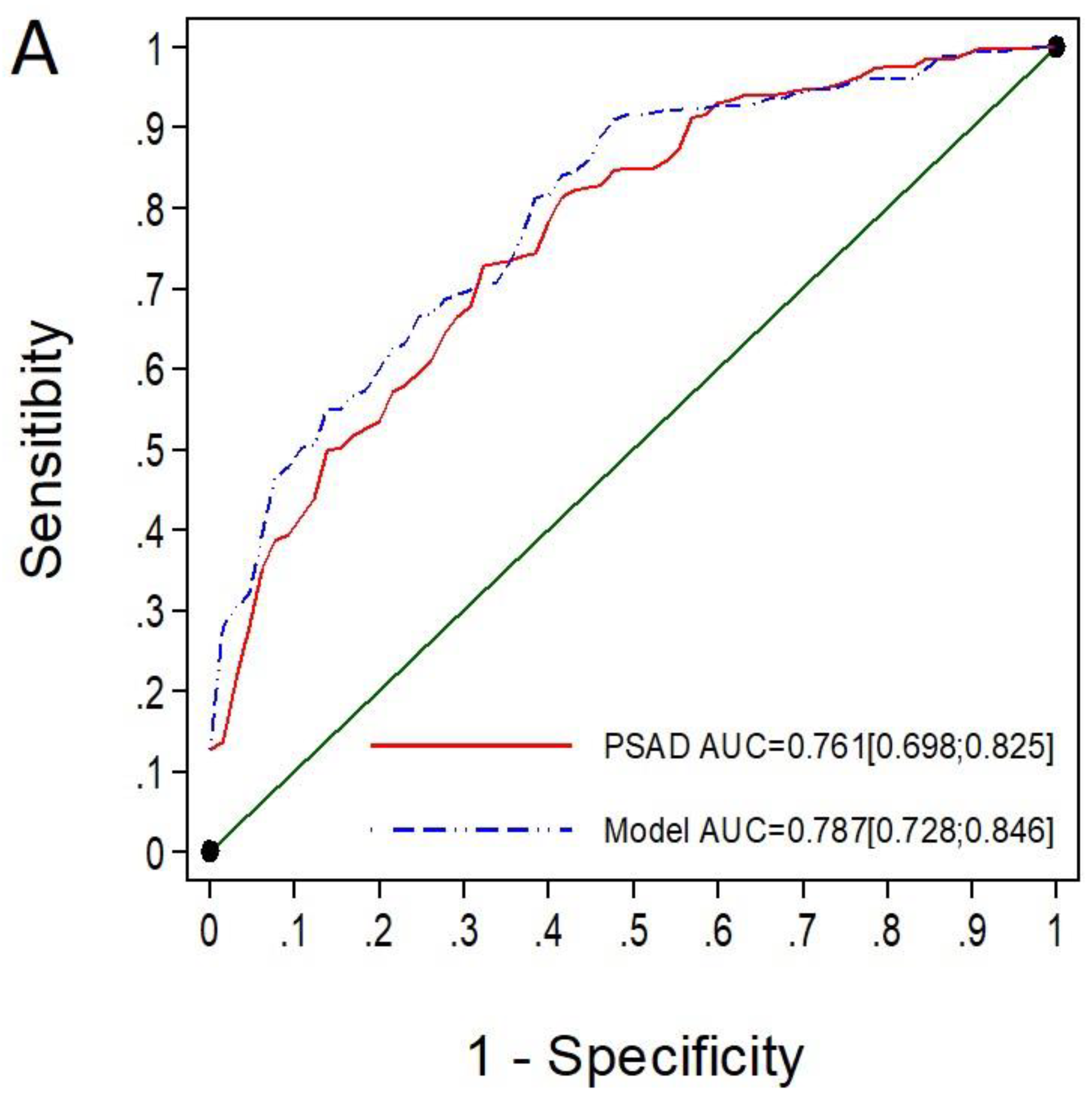
3.3. Performance of mPSAD and MRI-PMbdex According to the PI-RADS Categories
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
Acronyms and Abbreviations
| CI | confidence interval |
| csPCa | clinically significant PCa |
| DRE | digital rectal examination |
| GG | grade group |
| iPCa | insignificant PCa |
| IQR | interquartile range |
| mPSAD | MRI associated PSAD |
| MRI | magnetic resonance imaging |
| PCa | prostate cancer |
| PI-RADS | prostate imaging-report and data system |
| PSA | prostate-specific antigen |
| PSAD | PSA density |
| PM | predictive model |
| PMbdex | developed and externally validated Barcelona PM |
| RC | risk calculator |
| TRUS | transrectal ultrasound |
References
- Hugosson, J.; Roobol, M.J.; Månsson, M.; Tammela, T.L.J.; Zappa, M.; Nelen, V.; Kwiatkowski, M.; Lujan, M.; Carlsson, S.V.; Talala, K.M.; et al. A 16-yr Follow-up of the European Randomized study of Screening for Prostate Cancer. Eur. Urol. 2019, 7, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Chou, R.; Croswell, J.M.; Dana, T.; Bougatsos, C.; Blazina, I.; Fu, R.; Gleitsmann, K.; Koenig, H.C.; Lam, C.; Maltz, A.; et al. Screening for prostate cancer: A review of the evidence for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2011, 155, 762–771. [Google Scholar] [CrossRef] [PubMed]
- Drazer, M.W.; Huo, D.; Eggener, S.E. National Prostate Cancer Screening Rates After the 2012 US Preventive Services Task Force Recommendation Discouraging Prostate-Specific Antigen-Based Screening. J. Clin. Oncol. 2015, 33, 2416–2423. [Google Scholar] [CrossRef] [PubMed]
- Fenton, J.J.; Weyrich, M.S.; Durbin, S.; Liu, Y.; Bang, H.; Melnikow, J. Prostate-Specific Antigen-Based Screening for Prostate Cancer: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2018, 319, 1914–1931. [Google Scholar] [CrossRef]
- US PSTF; Grossman, D.C.; Curry, S.J.; Owens, D.K.; Bibbins-Domingo, K.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Ebell, M.; Epling, J.W.; et al. Screening for Prostate Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 319, 1901–1913. [Google Scholar] [CrossRef]
- Van Poppel, H.; Hogenhout, R.; Albers, P.; van den Bergh, R.C.N.; Barentsz, J.O.; Roobol, M.J. A European Model for an Organised Risk-stratified Early Detection Programme for Prostate Cancer. Eur. Urol. Oncol. 2021, 80, 703–711. [Google Scholar] [CrossRef]
- Mottet, N.; van den Bergh, R.C.N.; Briesrs, E.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2021, 79, 243–262. [Google Scholar] [CrossRef]
- Schoots, I.G. MRI in early prostate cancer detection: How to manage indeterminate or equivocal PI-RADS 3 lesions. Transl. Androl. Urol. 2018, 7, 770–782. [Google Scholar] [CrossRef]
- Maggi, M.; Panebianco, V.; Mosca, A.; Salciccia, S.; Gentilucci, A.; Di Pierro, G.; Busetto, G.M.; Barchetti, G.; Campa, R.; Sperduti, I.; et al. Prostate Imaging Reporting and Data System 3 Category Cases at Multiparametric Magnetic Resonance for Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. Focus. 2020, 6, 463–478. [Google Scholar] [CrossRef]
- Moldovan, P.C.; Van den Broeck, T.; Sylvester, R.; Marconi, L.; Bellmunt, J.; van den Bergh, R.C.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; Fossati, N.; et al. What Is the Negative Predictive Value of Multiparametric Magnetic Resonance Imaging in Excluding Prostate Cancer at Biopsy? A Systematic Review and Meta-analysis from the European Association of Urology Prostate Cancer Guidelines Panel. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef]
- Sathianathen, N.J.; Omer, A.; Harriss, E.; Davies, L.; Kasivisvanathan, V.; Punwani, S.; Moore, C.M.; Kastner, C.; Barrett, T.; Van Den Bergh, R.C.; et al. Negative Predictive Value of Multiparametric Magnetic Resonance Imaging in the Detection of Clinically Significant Prostate Cancer in the Prostate Imaging Reporting and Data System Era: A Systematic Review and Meta-Analysis. Eur Urol. 2020, 78, 402–414. [Google Scholar] [CrossRef] [PubMed]
- Wagaskar, V.G.; Levy, M.; Ratnani, P.; Moody, K.; Garcia, M.; Pedraza, A.M.; Parekh, S.; Pandav, K.; Shukla, B.; Prasad, S.; et al. Clinical Utility of Negative Multiparametric Magnetic Resonance Imaging in the Diagnosis of Prostate Cancer and Clinically Significant Prostate Cancer. Eur. Urol. Open Sci. 2021, 28, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Kasivisvanathan, V.; Stabile, A.; Neves, J.; Giganti, F.; Valerio, M.; Shanmugabavan, Y.; Clement, K.; Sarkar, D.; Philippou, Y.; Thurtle, D.; et al. Magnetic Resonance Imaging-targeted Biopsy Versus Systematic Biopsy in the Detection of Prostate Cancer: A Systematic Review and Meta-analysis. Eur. Urol. 2019, 76, 284–303. [Google Scholar] [CrossRef] [PubMed]
- Drost, F.H.; Osses, D.; Nieboer, D.; Bangma, C.H.; Steyerberg, E.W.; Roobol, M.J.; Schoots, I.G. Prostate Magnetic Resonance Imaging, with or without Magnetic Resonance Imaging-Targeted Biopsy, and Systematic Biopsy for Detecting Prostate Cancer: A Cochrane Systematic Review and Meta-Analysis. Eur. Urol. 2020, 77, 78–94. [Google Scholar] [CrossRef]
- Mazzone, E.; Stabile, A.; Pellegrino, F.; Basile, G.; Cignoli, D.; Cirulli, G.O.; Sorce, G.; Barletta, F.; Scuderi, S.; Bravi, C.A.; et al. Positive Predictive Value of Prostate Imaging Reporting and Data System Version 2 for the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. Oncol. 2021, 4, 697–713. [Google Scholar] [CrossRef]
- Osses, D.F.; Roobol, M.J.; Schoots, I.G. Prediction Medicine: Biomarkers, Risk Calculators and Magnetic Resonance Imaging as Risk Stratification Tools in Prostate Cancer Diagnosis. Int. J. Mol. Sci. 2020, 20, 1637. [Google Scholar] [CrossRef]
- Benson, M.C.; Whang, I.S.; Pantuck, A.; Ring, K.; Kaplan, S.A.; Olsson, C.A.; Cooner, W.H. Prostate specific antigen density: A means of distinguishing benign prostatic hypertrophy and prostate cancer. J. Urol. 1992, 147, 815–816. [Google Scholar] [CrossRef]
- Dianat, S.S.; Rancier, R.R.M.; Bonekamp, D.; Carter, H.B.; Macura, K.J. Prostate volumetric assessment by magnetic resonance imaging and transrectal ultrasound: Impact of variation in calculated prostate-specific antigen density on patient eligibility for active surveillance program. J. Comput. Assist. Tomogr. 2013, 37, 589–595. [Google Scholar] [CrossRef]
- Boesen, L.; Nørgaard, N.; Løgager, V.; Balslev, I.; Bisbjerg, R.; Thestrup, K.C.; Jakobsen, H.; Thomsen, H.S. Prebiopsy Biparametric Magnetic Resonance Imaging Combined with Prostate-specific Antigen Density in Detecting and Ruling out Gleason 7–10 Prostate Cancer in Biopsy-naïve Men. Eur. Urol. Oncol. 2019, 2, 311–319. [Google Scholar] [CrossRef]
- Morote, J.; Celma, A.; Planas, J. Re: Lars Boesen, Nis Nørgaard, Vibeke Løgager, et al. Prebiopsy Biparametric Magnetic Resonance Imaging Combined with Prostate-specific Antigen Density in Detecting and Ruling out Gleason 7–10 Prostate Cancer in Biopsy-naïve Men. Eur. Urol. Oncol. 2020, 3, 392–393. [Google Scholar] [CrossRef]
- Morote, J.; Celma, A.; Diaz, F.; Regis, L.; Roche, S.; Mast, R.; Semidey, M.E.; de Torres, I.M.; Planas, J.; Trilla, E. Prostatic-specific antigen density behavior according to multiparametric magnetic resonance imaging result. Urol. Oncol. 2020, 38, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Görtz, M.; Radtke, J.P.; Hatiboglu, G.; Schütz, V.; Tosev, G.; Güttlein, M.; Leichsenring, J.; Stenzinger, A.; Bonekamp, D.; Schlemmer, H.P.; et al. The Value of Prostate-specific Antigen Density for Prostate Imaging-Reporting and Data System 3 Lesions on Multiparametric Magnetic Resonance Imaging: A Strategy to Avoid Unnecessary Prostate Biopsies. Eur. Urol. Focus 2021, 7, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.K.; Li, J.; Das, S.K.; Xiong, Y.; Yang, C.B.; Peng, T. Developing a nomogram based on multiparametric magnetic resonance imaging for forecasting high-grade prostate cancer to reduce unnecessary biopsies within the prostate-specific antigen gray zone. BMC Med. Imaging 2017, 17, 11. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.H.; Weaver, J.K.; Shetty, A.S.; Vetter, J.M.; Andriole, G.L.; Strope, S.A. Magnetic Resonance Imaging Provides Added Value to the Prostate Cancer Prevention Trial Risk Calculator for Patients with Estimated Risk of High-Grade Prostate Cancer Less Than or Equal to 10. Urology 2017, 102, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.M.; Liyanage, S.H.; Wulaningsih, W.; Wolfe, K.; Carr, T.; Younis, C.; Van Hemelrijck, M.; Popert, R.; Acher, P. Toward an MRI-based nomogram for the prediction of transperineal prostate biopsy outcome: A physician and patient decision tool. Urol. Oncol. 2017, 35, 664–668. [Google Scholar] [CrossRef]
- Mehralivand, S.; Shih, J.H.; Rais-Bahrami, S.; Oto, A.; Bednarova, S.; Nix, J.W.; Thomas, J.V.; Gordetsky, J.B.; Gaur, S.; Harmon, S.A.; et al. A Magnetic Resonance Imaging-Based Prediction Model for Prostate Biopsy Risk Stratification. JAMA Oncol. 2018, 4, 678–685. [Google Scholar] [CrossRef]
- Truong, M.; Wang, B.; Gordetsky, J.B.; Nix, J.W.; Frye, T.P.; Messing, E.M.; Thomas, J.V.; Feng, C.; Rais-Bahrami, S. Multi-institutional nomogram predicting benign prostate pathology on magnetic resonance/ultrasound fusion biopsy in men with a prior negative 12-core systematic biopsy. Cancer 2018, 124, 278–285. [Google Scholar] [CrossRef]
- Huang, C.; Song, G.; Wang, H.; Li, J.; Chen, Y.; Fan, Y.; Fang, D.; Xiong, G.; Xin, Z.; Zhou, L. MultiParametric Magnetic Resonance Imaging-Based Nomogram for Predicting Prostate Cancer and Clinically Significant Prostate Cancer in Men Undergoing Repeat Prostate Biopsy. Biomed. Res. Int. 2018, 2018, 6368309. [Google Scholar] [CrossRef]
- Bjurlin, M.A.; Rosenkrantz, A.B.; Sarkar, S.; Lepor, H.; Huang, W.C.; Huang, R.; Venkataraman, R.; Taneja, S.S. Prediction of Prostate Cancer Risk Among Men Undergoing Combined MRI-targeted and Systematic Biopsy Using Novel Pre-biopsy Nomograms That Incorporate MRI Findings. Urology 2018, 112, 112–120. [Google Scholar] [CrossRef]
- Grönberg, H.; Eklund, M.; Picker, W.; Aly, M.; Jäderling, F.; Adolfsson, J.; Landquist, M.; Haug, E.S.; Ström, P.; Carlsson, S.; et al. Prostate Cancer Diagnostics Using a Combination of the Stockholm3 Blood Test and Multiparametric Magnetic Resonance Imaging. Eur. Urol. 2018, 74, 722–778. [Google Scholar] [CrossRef]
- Liu, C.; Liu, S.L.; Wang, Z.X.; Yu, K.; Feng, C.X.; Ke, Z.; Wang, L.; Zeng, X.Y. Using the prostate imaging reporting and data system version 2 (PI-RIDS v2) to detect prostate cancer can prevent unnecessary biopsies and invasive treatment. Asian J. Androl. 2018, 20, 459–464. [Google Scholar] [PubMed]
- Borque-Fernando, A.; Esteban, L.M.; Celma, A.; Roche, S.; Planas, J.; Regis, L.; de Torres, I.; Semidey, M.E.; Trilla, E.; Morote, J. How to implement magnetic resonance imaging before prostate biopsy in clinical practice: Nomograms for saving biopsies. World J. Urol. 2019, 38, 1481–1491. [Google Scholar] [CrossRef] [PubMed]
- Bjurlin, M.A.; Renson, A.; Rais-Bahrami, S.; Truong, M.; Rosenkrantz, A.B.; Huang, R.; Taneja, S.S. Predicting Benign Prostate Pathology on Magnetic Resonance Imaging/Ultrasound Fusion Biopsy in Men with a Prior Negative 12-core Systematic Biopsy: External Validation of a Prognostic Nomogram. Eur. Urol. Focus. 2019, 5, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Alberts, A.R.; Roobol, M.J.; Verbeek, J.F.M.; Schoots, I.G.; Chiu, P.K.; Osses, D.F.; Tijsterman, J.D.; Beerlage, H.P.; Mannaerts, C.K.; ScAhimmöller, L.; et al. Prediction of High-grade Prostate Cancer Following Multiparametric Magnetic Resonance Imaging: Improving the Rotterdam European Randomized Study of Screening for Prostate Cancer Risk Calculators. Eur. Urol. 2019, 75, 310–318. [Google Scholar] [CrossRef]
- He, B.M.; Shi, Z.K.; Li, H.S.; Lin, H.Z.; Yang, Q.S.; Lu, J.P.; Sun, Y.H.; Wang, H.F. A Novel Prediction Tool Based on Multiparametric Magnetic Resonance Imaging to Determine the Biopsy Strategy for Clinically Significant Prostate Cancer in Patients with PSA Levels Less than 50 ng/mL. Ann. Surg. Oncol. 2020, 27, 1284–1295. [Google Scholar] [CrossRef]
- Noh, T.I.; Hyun, C.W.; Kang, H.E.; Jin, H.J.; Tae, J.H.; Shim, J.S.; Kang, S.G.; Sung, D.J.; Cheon, J.; Lee, J.G.; et al. A Predictive Model Based on Bi-parametric Magnetic Resonance Imaging and Clinical Parameters for Clinically Significant Prostate Cancer in the Korean Population. Cancer Res. Treat. 2021, 53, 1148–1855. [Google Scholar] [CrossRef]
- Schoots, I.G.; Roobol, M.J. Multivariate risk prediction tools including MRI for individualized biopsy decision in prostate cancer diagnosis: Current status and future directions. World J. Urol. 2020, 38, 517–529. [Google Scholar] [CrossRef]
- Morote, J.; Borque-Fernando, A.; Triquell, M.; Celma, A.; Regis, L.; Abascal, J.M.; Sola, C.; Servian, P.; Escobar, M.; Mast, R.; et al. The Barcelona Predictive Model of Clinically Significant Prostate Cancer. Cancers 2022, 14, 1589. [Google Scholar] [CrossRef]
- Remmers, S.; Kasivisvanathan, V.; Verbeek, J.F.M.; Moore, C.M.; Roobol, M.J. ERSPC RSGPRECISIONIG. Reducing Biopsies and Magnetic Resonance Imaging Scans during the Diagnostic Pathway of Prostate Cancer: Applying the Rotterdam Prostate Cancer Risk Calculator to the PRECISION Trial Data. Eur. Urol. Open Sci. 2022, 36, 1–8. [Google Scholar] [CrossRef]
- Vickers, A.J.; Russo, G.; Lilja, H.; Evans, C.; Schalken, J.A.; Klein, E.; Eggener, S. How Should Molecular Markers and Magnetic Resonance Imaging Be Used in the Early Detection of Prostate Cancer. Eur. Urol. Oncol. 2021, 5, 135–137. [Google Scholar] [CrossRef]
- Punnen, S.; Freedland, S.J.; Polascik, T.J.; Loeb, S.; Risk, M.C.; Savage, S.; Mathur, S.C.; Uchio, E.; Dong, Y.; Silberstein, J.L. A Multi-Institutional Prospective Trial Confirms Noninvasive Blood Test Maintains Predictive Value in African American Men. J. Urol. 2018, 199, 1459–1463. [Google Scholar] [CrossRef] [PubMed]
- Punnen, S.; Nahar, B.; Soodana-Prakash, N.; Koru-Sengui, T.; Stoyanova, R.; Pollack, A.; Gonzalgo, M.L.; Ritch, C.R.; Parekh, J. Optimizing patient’s selection for prostate biopsy: A single institution experience with multi-parametric MRI and the 4Kscore test for the detection of aggressive prostate cance. PLoS ONE 2018, 13, e0201384. [Google Scholar] [CrossRef] [PubMed]
- Marzouk, K.; Ehdaie, B.; Vertosick, E.; Zappala, S.; Vickers, A. Developing an effective strategy to improve the detection of significant prostate cancer by combining the 4Kscore and multiparametric MRI. Urol. Oncol. 2019, 37, 672–677. [Google Scholar] [CrossRef] [PubMed]
- Falagario, U.G.; Martini, A.; Wajswol, E.; Treacy, P.J.; Ratnani, P.; Jambor, I.; Anastos, H.; Lewis, S.; Haines, K.; Cormio, L.; et al. Avoiding Unnecessary Magnetic Resonance Imaging (MRI) and Biopsies: Negative and Positive Predictive Value of MRI According to Prostate-specific Antigen Density, 4Kscore and Risk Calculators. Eur. Urol. Oncol. 2020, 3, 700–704. [Google Scholar] [CrossRef] [PubMed]
- Wagaskar, V.G.; Sobotka, S.; Ratnani, P.; Young, J.; Lantz, A.; Pareckh, S.; Falagario, U.G.; Li, L.; Lewis, S.; Punnen, S.; et al. A 4K score/MRI-based nomogram for predicting prostate cancer, clinically significant prostate cancer, and unfavorable prostate cancer. Cancer Rep. 2021, 4, e1357. [Google Scholar] [CrossRef]
- Porpiglia, F.; Russo, F.; Manfredi, M.; Mele, F.; Fiori, C.; Bollito, E.; Papotti, M.; Molineris, I.; Passera, R.; Regge, D. The roles of multiparametric MRI, PCA3 and PHI: Which is the best predictor of prostate cancer after a negative biopsy? Results of a prospective study. J. Urol. 2014, 192, 60–66. [Google Scholar] [CrossRef]
- Gnanapragasam, V.J.; Burling, K.; George, A.; Stearn, S.; Warren, A.; Barrett, T.; Koo, B.; Gallagher, F.A.; Doble, A.; Kastner, C.; et al. The Prostate Health Index adds predictive value to multi-parametric MRI in detecting significant prostate cancers in a repeat biopsy population. Sci. Rep. 2016, 6, 35364. [Google Scholar] [CrossRef]
- Fan, Y.H.; Pan, P.H.; Cheng, W.M.; Wang, H.K.; Shen, S.H.; Liu, H.T.; Cheng, H.M.; Chen, W.R.; Huang, T.H.; Wei, T.C.; et al. The Prostate Health Index aids multi-parametric MRI in diagnosing significant prostate cancer. Sci. Rep. 2021, 11, 1286. [Google Scholar] [CrossRef]
- Hendriks, R.J.; van der Leest, M.M.G.; Dijkstra, S.; Barentsz, J.O.; Van Criekinge, W.; Hulsbergen-van de Kaa, C.A.; Schalken, J.A.; Mulders, P.F.A.; van Oort, I.M. A urinary biomarker-based risk score correlates with multiparametric MRI for prostate cancer detection. Prostate 2017, 77, 1401–1407. [Google Scholar] [CrossRef]
- Hendriks, R.J.; van der Leest, M.M.G.; Israël, B.; Hannink, G.; YantiSetiasti, A.; Cornel, E.B.; Hulsbergen-van de Kaa, C.A.; Klaver, O.S.; Sedelaar, J.P.M.; Van Criekinge, W.; et al. Clinical use of the SelectMDx urinary-biomarker test with or without mpMRI in prostate cancer diagnosis: A prospective, multicenter study in biopsy-naïve men. Prostate Cancer Prostatic Dis. 2021, 24, 1110–1119. [Google Scholar] [CrossRef]
- Maggi, M.; Del Giudice, F.; Falagario, U.G.; Cocci, A.; Russo, G.I.; Di Mauro, M.; Sepe, G.S.; Galasso, F.; Leonardi, R.; Iacona, A.; et al. SelectMDx and Multiparametric Magnetic Resonance Imaging of the Prostate for Men Undergoing Primary Prostate Biopsy: A Prospective Assessment in a Multi-Institutional Study. Cancers 2021, 13, 2047. [Google Scholar] [CrossRef] [PubMed]
- Morote, J.; Campistol, M.; Regis, L.; Celma, A.; de Torres, I.; Semidey, M.E.; Roche, S.; Mast, R.; Santamaria, A.; Planas, J.; et al. Who with suspected prostate cancer can benefit from Proclarix after multiparametric magnetic resonance imaging. Int. J. Biol. Markers 2022, 3936155221081537. [Google Scholar] [CrossRef] [PubMed]
- Morote, J.; Campistol, M.; Celma, A.; Regis, L.; de Torres, I.; Semidey, M.E.; Roche, S.; Mast, R.; Santamaría, A.; Planas, J.; et al. The Efficacy of Proclarix to Select Appropriate Candidates for Magnetic Resonance Imaging and Derived Prostate Biopsies in Men with Suspected Prostate Cancer. World J. Mens Health 2022, 40, 270–279. [Google Scholar] [CrossRef] [PubMed]
- Barentsz, J.O.; Richenberg, J.; Clements, R.; Choyke, P.; Verma, S.; Villeirs, G.; Rouviere, O.; Logager, V.; Futterer, J.J. ESUR prostate MR guidelines 2012. Eur. Radiol. 2012, 22, 746–757. [Google Scholar] [CrossRef]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; et al. PI-RADS Prostate Imaging—Reporting and Data System: 2015, Version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef]
- Schoots, I.G.; Roobol, M.J.; Nieboer, D.; Bangma, C.H.; Steyerberg, E.W.; Hunink, M.G. Magnetic resonance imaging-targeted biopsy may enhance the diagnostic accuracy of significant prostate cancer detection compared to standard transrectal ultrasound-guided biopsy: A systematic review and meta-analysis. Eur. Urol. 2015, 68, 438–450. [Google Scholar] [CrossRef]
- Epstein, J.I.; Egevad, L.; Amin, M.B.; Delahunt, B.; Srigley, J.R.; Humphrey, P.A.; Grading, C. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am. J. Surg. Pathol. 2016, 40, 244–252. [Google Scholar] [CrossRef]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Statistics SOTNCI-EORTCWGOCD. REporting recommendations for tumour MARKer prognostic studies (REMARK). Br. J. Cancer 2005, 93, 387–391. [Google Scholar] [CrossRef]
- Bossuyt, P.M.; Reitsma, J.B.; Bruns, D.E.; Korevaar, D.A. STARD 2015: An updated list of essential items for reporting diagnostic accuracy studies. BMJ 2015, 351, h5527. [Google Scholar] [CrossRef]
- Creelman, C.D.; Donaldson, W. ROC curves for discrimination of linear extent. J. Exp. Psychol. 1968, 77, 514–516. [Google Scholar] [CrossRef]
- DeLong, E.R.; DeLong DMClarke-Pearson, D.L. Comparing the areas under two or more correlated receiver operating characteristic curves: A nonparametric approach. Biometrics 1988, 44, 837–845. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J.; Elkin, E.B. Decision curve analysis: A novel method for evaluating prediction models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Benson, M.C.; Whang, I.S.; Olsson, C.A.; McMahon, D.J.; Cooner, W.H. The use of prostate specific antigen density to enhance the predictive value of intermediate levels of serum prostate specific antigen. J. Urol. 1992, 147, 817–821. [Google Scholar] [CrossRef]
- Catalona, W.J.; Richie, J.P.; deKernion, J.B.; Ahmann, F.R.; Ratliff, T.L.; Dalkin, B.L.; Kavoussi, L.R.; MacFarlane, M.T.; Southwick, P.C. Comparison of prostate specific antigen concentration versus prostate specific antigen density in the early detection of prostate cancer: Receiver operating characteristic curves. J. Urol. 1994, 152, 2031–2036. [Google Scholar] [CrossRef]
- Yamashiro, J.R.; de Riese, W.T.W. Any Correlation Between Prostate Volume and Incidence of Prostate Cancer: A Review of Reported Data for the Last Thirty Years. Res. Rep. Urol. 2021, 13, 749–757. [Google Scholar] [CrossRef]
- Bangma, C.H.; Niemer, A.Q.; Grobbee, D.E.; Schröder, F.H. Transrectal ultrasonic volumetry of the prostate: In vivo comparison of different methods. Prostate 1996, 28, 107–110. [Google Scholar] [CrossRef]
- Thon, W.F.; Gadban, F.; Truss, M.C.; Kuczyk, M.; Hartmann, U.; Jonas, U. Prostate-specific antigen density a reliable parameter for the detection of prostate cancer. World J. Urol. 1996, 14, 53–58. [Google Scholar] [CrossRef]
- Keetch, D.W.; McMurtry, J.M.; Smith, D.S.; Andriole, G.L.; Catalona, W.J. Prostate specific antigen density versus prostate specific antigen slope as predictors of prostate cancer in men with initially negative prostatic biopsies. J. Urol. 1996, 156, 428–431. [Google Scholar] [CrossRef]
- Morote, J.; Raventós, C.X.; Lorente, J.A.; Lopez-Pacios, M.A.; Encabo, G.; de Torres, I.; Andreu, J. Comparison of percent free prostate specific antigen and prostate specific antigen density as methods to enhance prostate specific antigen specificity in early prostate cancer detection in men with normal rectal examination and prostate specific antigen between 4.1 and 10 ng/mL. J. Urol. 1997, 158, 502–504. [Google Scholar]
- Loeb, S.; Roehl, K.A.; Thaxton, C.S.; Catalona, W.J. Combined prostate-specific antigen density and biopsy features to predict “clinically insignificant” prostate cancer. Urology 2008, 72, 143–147. [Google Scholar] [CrossRef]
- Roobol, M.J.; Schröder, F.H.; Hugosson, J.; Jones, J.S.; Kattan, M.W.; Klein, E.A.; Hamdy, F.; Neal, D.; Donovan, J.; Parekh, D.J.; et al. Importance of prostate volume in the European Randomised Study of Screening for Prostate Cancer (ERSPC) risk calculators: Results from the prostate biopsy collaborative group. World J. Urol. 2012, 30, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Roobol, M.J.; van Vugt, H.A.; Loeb, S.; Zhu, X.; Bul, M.; Bangma, C.H.; van Leenders, A.G.; Steyerberg, E.W.; Schröder, F.H. Prediction of prostate cancer risk: The role of prostate volume and digital rectal examination in the ERSPC risk calculators. Eur. Urol. 2012, 61, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Christie, D.R.H.; Sharpley, C.F. How Accurately Can Prostate Gland Imaging Measure the Prostate Gland Volume? Results of a Systematic Review. Prostate Cancer 2019, 2019, 6932572. [Google Scholar] [CrossRef] [PubMed]
- Jeong, C.W.; Park, H.K.; Hong, S.K.; Byun, S.S.; Lee, H.J.; Lee, S.E. Comparison of prostate volume measured by transrectal ultrasonography and MRI with the actual prostate volume measured after radical prostatectomy. Urol. Int. 2008, 81, 179–185. [Google Scholar] [CrossRef] [PubMed]
- Boesen, L.; Thomsen, F.B.; Nørgaard, N.; Løgager, V.; Balslev, I.; Bisbjerg, R.; Thomsen, H.S.; Jakobsen, H. A predictive model based on biparametric magnetic resonance imaging and clinical parameters for improved risk assessment and selection of biopsy-naïve men for prostate biopsies. Prostate Cancer Prostatic Dis. 2019, 2, 311–319. [Google Scholar] [CrossRef] [PubMed]
- Fang, D.; Zhao, C.; Ren, D.; Yu, W.; Wang, R.; Wang, H.; Li, X.; Yin, W.; Yu, X.; Yang, K.; et al. Could Magnetic Resonance Imaging Help to Identify the Presence of Prostate Cancer Before Initial Biopsy? The Development of Nomogram Predicting the Outcomes of Prostate Biopsy in the Chinese Population. Ann. Surg. Oncol. 2016, 23, 4284–4292. [Google Scholar] [CrossRef] [PubMed]
- Radtke, J.P.; Wiesenfarth, M.; Kesch, C.; Freitag, M.T.; Alt, C.D.; Celik, K.; Distler, F.; Roth, W.; Wieczorek, K.; Stock, C.; et al. Combined Clinical Parameters and Multiparametric Magnetic Resonance Imaging for Advanced Risk Modeling of Prostate Cancer-Patient-tailored Risk Stratification Can Reduce Unnecessary Biopsies. Eur. Urol. 2017, 72, 888–896. [Google Scholar] [CrossRef]
- Van Leeuwen, P.J.; Hayen, A.; Thompson, J.E.; James, E.; Moses, D.; Shnier, R.; Böhm, M.; Abuodha, M.; Haynes, A.M.; Ting, F.; et al. A multiparametric magnetic resonance imaging-based risk model to determine the risk of significant prostate cancer prior to biopsy. BJU Int. 2017, 120, 774–781. [Google Scholar] [CrossRef]
- Chen, R.; Verbeek, J.F.M.; Yang, Y.; Song, Z.; Sun, Y.; Roobol, M.J. Comparing the prediction of prostate biopsy outcome using the Chinese Prostate Cancer Consortium (CPCC) Risk Calculator and the Asian adapted Rotterdam European Randomized Study of Screening for Prostate Cancer (ERSPC) Risk Calculator in Chinese and European men. World J. Urol. 2021, 39, 73–80. [Google Scholar]
- Schoots, I.G.; Padhani, A.R.; Rouvière, O.; Barentsz, J.O.; Richenberg, J. Risk-adapted biopsy decision based on prostate magnetic resonance imaging and prostate-specific antigen density for enhanced biopsy avoidance in first prostate cancer diagnostic evaluation. BJU Int. 2021, 127, 175–178. [Google Scholar] [CrossRef]
- Morote, J.; Planas, J.; Trilla, E. Re: Magdalena Görtz, Jan Philipp Radtke, Gencay Hatiboglu, et al. The Value of Prostate-specific Antigen Density for Prostate Imaging-Reporting and Data System 3 Lesions on Multiparametric Magnetic Resonance Imaging: A Strategy to Avoid Un-necessary Prostate Biopsies. Eur Urol Focus 2021; 7: 325-31. Eur. Urol. Focus 2022, S2405–S4569. [Google Scholar] [CrossRef]
- Washino, S.; Okochi, T.; Saito, K.; Konishi, T.; Hirai, M.; Kobayashi, Y.; Miyagawa, T. Combination of prostate imaging reporting and data system (PI-RADS) score and prostate-specific antigen (PSA) density predicts biopsy outcome in prostate biopsy naïve patients. BJU Int. 2017, 119, 225–233. [Google Scholar] [CrossRef] [PubMed]
- Jue, J.S.; Barboza, M.P.; Prakash, N.S.; Venkatramani, V.; Sinha, V.R.; Pavan, N.; Nahar, B.; Kanabur, P.; Ahdoot, M.; Dong, Y.; et al. Re-examining Prostate-specific Antigen (PSA) Density: Defining the Optimal PSA Range and Patients for Using PSA Density to Predict Prostate Cancer Using Extended Template Biopsy. Urology 2017, 105, 123–128. [Google Scholar] [CrossRef]
- Hansen, N.L.; Barrett, T.; Koo, B.; Doble, A.; Gnanapragasam, V.; Warren, A.; Kastner, C.; Bratt, O. The influence of prostate-specific antigen density on positive and negative predictive values of multiparametric magnetic resonance imaging to detect Gleason score 7-10 prostate cancer in a repeat biopsy setting. BJU Int. 2017, 119, 724–730. [Google Scholar] [CrossRef] [PubMed]
- Distler, F.A.; Radtke, J.P.; Bonekamp, D.; Kesch, C.; Schlemmer, H.-P.; Wieczorek, K.; Kirchner, M.; Pahernik, S.; Hohenfellner, M.; Hadaschik, B.A. The Value of PSA Density in Combination with PI-RADS™ for the Accuracy of Prostate Cancer Prediction. J. Urol. 2017, 198, 575–582. [Google Scholar] [CrossRef]
- Kotb, A.F.; Spaner, S.; Crump, T.; Hyndman, M.E. The role of mpMRI and PSA density in patients with an initial negative prostatic biopsy. World J. Urol. 2018, 36, 2021–2025. [Google Scholar] [CrossRef]
- Stevens, E.; Truong, M.; Bullen, J.A.; Ward, R.D.; Purysko ASKlein, E.A. Clinical utility of PSAD combined with PI-RADS category for the detection of clinically significant prostate cancer. Urol. Oncol. 2020, 38, 846–849. [Google Scholar] [CrossRef]
- Ryoo, H.; Kang, M.Y.; Sung, H.H.; Chang Jeong, B.; Seo, S.I.; Jeon, S.S.; Lee, H.M.; Jeon, H.G. Detection of prostate cancer using prostate imaging reporting and data system score and prostate-specific antigen density in biopsy-naive and prior biopsy-negative patients. Prostate Int. 2020, 8, 25–29. [Google Scholar] [CrossRef]
- Yusim, I.; Krenawi, M.; Mazor, E.; Novack, V.; Mabjeesh, N.J. The use of prostate specific antigen density to predict clinically significant prostate cancer. Sci. Rep. 2020, 10, 20015. [Google Scholar] [CrossRef]
- Yu, J.; Boo, Y.; Kang, M.; Sung, H.H.; Jeong, B.C.; Seo, S.; Jeon, S.S.; Lee, H.; Jeon, H.G. Can Prostate-Specific Antigen Density Be an Index to Distinguish Patients Who Can Omit Repeat Prostate Biopsy in Patients with Negative Magnetic Resonance Imaging. Cancer Manag. Res. 2021, 13, 5467–5475. [Google Scholar] [CrossRef]
- Falagario, U.G.; Jambor, I.; Lantz, A.; Ettala, O.; Stabile, A.; Taimen, P.; Aronen, H.J.; Knaapila, J.; Perez, I.M.; Gandaglia, G.; et al. Combined Use of Prostate-specific Antigen Density and Magnetic Resonance Imaging for Prostate Biopsy Decision Planning: A Retrospective Multi-institutional Study Using the Prostate Magnetic Resonance Imaging Outcome Database (PROMOD). Eur. Urol. Oncol. 2021, 4, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Girometti, R.; Giannarini, G.; Panebianco, V.; Maresca, S.; Cereser, L.; De Martino, M.; Pizzolitto, S.; Pecoraro, M.; Ficarra, V.; Zuiani, C.; et al. Comparison of different thresholds of PSA density for risk stratification of PI-RADSv2.1 categories on prostate MRI. Br. J. Radiol. 2021, 95, 20210886. [Google Scholar] [CrossRef] [PubMed]
- Tafuri, A.; Iwata, A.; Shakir, A.; Iwata, T.; Gupta, C.; Sali, A.; Sugano, D.; Mahdi, A.S.; Cacciamani, G.E.; Kaneko, M.; et al. Systematic Biopsy of the Prostate can Be Omitted in Men with PI-RADS™ 5 and Prostate Specific Antigen Density Greater than 15. J. Urol. 2021, 206, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.B.; Wei, C.G.; Zhang, Y.Y.; Pan, P.; Dai, G.C.; Tu, J.; Shen, J.K. The Role of PSA Density among PI-RADS v2.1 Categories to Avoid an Unnecessary Transition Zone Biopsy in Patients with PSA 4–20 ng/mL. Biomed. Res. Int. 2021, 2021 , 3995789. [Google Scholar] [CrossRef]
- Haroon, M.; Sathiadoss, P.; Breau, R.H.; Cagiannos, I.; Flood, T.; Lavallee, L.T.; Morash, C.; Shieda, N. Proportion of clinically significant prostate cancer diagnosed by systematic template biopsy after negative pre-biopsy multiparametric magnetic resonance imaging and predictive value of prostate-specific antigen density. Can. Urol. Assoc. J. 2022, 16, 178–180. [Google Scholar] [CrossRef]
- Woźnicki, P.; Westhoff, N.; Huber, T.; Riffel, P.; Froelich, M.F.; Gresser, E.; von Hardenberg, J.; Mühlberg, A.; Michel, M.S.; Schoenberg, S.O.; et al. Multiparametric MRI for Prostate Cancer Characterization: Combined Use of Radiomics Model with PI-RADS and Clinical Parameters. Cancers 2020, 12, 1767. [Google Scholar] [CrossRef]
- Ferro, M.; de Cobelli, O.; Vartolomei, M.D.; Lucarelli, G.; Crocetto, F.; Barone, B.; Sciarra, A.; Del Giudice, F.; Muto, M.; Maggi, M.; et al. Prostate Cancer Radiogenomics—From Imaging to Molecular Characterization. Int. J. Mol. Sci. 2021, 22, 9971. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Measurement |
|---|---|
| Number of cases | 2432 |
| Median age, years (IQR) | 68 (62–73) |
| Median total PSA, ng/mL (IQR) | 6.5 (4.7–10.0) |
| Abnormal DRE, n (%) | 612 (25.2) |
| Median prostate volume, ml (IQR) | 55 (40–77) |
| Median PSA density, ng/mL2 (IQR) | 0.12 (0.08–0.20) |
| Repeat biopsy, n (%) | 681 (28.0) |
| Family history of PCa, n (%) | 161 (6.6%) |
| PI-RADS, n (%) | |
| 1–2 | 550 (22.6) |
| 3 | 645 (26.5) |
| 4 | 841 (34.6) |
| 5 | 396 (16.3) |
| Overall PCa detection, n (%) | 1214 (49.9) |
| csPCa detection, n (%) | 934 (38.4) |
| iPCa detection, n (%) | 280 (11.5) |
| Characteristic | PI-RADS 1 | p Value | PI-RADS 2 | p Value | PI-RADS 3 | p Value | PI-RADS 4 | p Value | PI-RADS 5 |
|---|---|---|---|---|---|---|---|---|---|
| Number of cases | 427 | - | 123 | - | 645 | - | 841 | - | 396 |
| Median age, years (IQR) | 66 (60–72) | =0.633 | 66 (60–71) | =0.901 | 66 (60–71) | <0.001 | 69 (63–74) | <0.001 | 72 (66–76) |
| Median total PSA, ng/mL (IQR) | 6.2 (4.5–8.7) | =0.323 | 5.8 (4.4–8.4) | =0.644 | 6.0 (4.4–8.4) | <0.001 | 6.6 (4.8–9.5) | <0.001 | 9.4 (5.8–18.0) |
| Abnormal DRE, n (%) | 59 (13.8) | =0.818 | 18 (14.6) | =0.497 | 80 (12.4) | <0.001 | 216 (25.7) | <0.001 | 239 (60.4) |
| Median PV, mL (IQR) | 63 (43–90) | =0.666 | 60 (45–84) | =0.833 | 63 (45–82) | <0.001 | 50 (37–74) | <0.001 | 46 (35–60) |
| Median PSAD, ng/mL2 (IQR) | 0.10 (0.07–0.15) | =0.960 | 0.11 (0.07–0.15) | =0.797 | 0.10 (0.07–0.15) | <0.001 | 0.13 (0.08–0.20) | <0.001 | 0.21 (0.13–0.37) |
| Repeat biopsy, n (%) | 83 (19.4) | <0.001 | 42 (34.1) | =0.631 | 206 (31.9) | =0.860 | 271 (32.3) | <0.001 | 78 (19.7) |
| Family history of PCa, n (%) | 20 (4.7) | =0.649 | 7 (5.7) | =0.733 | 42 (6.5) | =0.702 | 59 (7.0) | =0.410 | 33 (8.3) |
| Overall PCa detection, n (%) | 97 (22.7) | =0.574 | 25 (20.3) | =0.028 | 194 (30.5) | <0.001 | 548 (65.2) | <0.001 | 350 (88.4) |
| csPCa detection, n (%) | 42 (9.8) | =0.865 | 13 (10.6) | =0.081 | 109 (16.9) | <0.001 | 439 (52.2) | <0.001 | 331 (83.6) |
| iPCa detection, n (%) | 55 (12.9) | =0.351 | 12 (9.8) | =0.295 | 85 (13.2) | =0.902 | 109 (13.0) | <0.001 | 19 (4.8) |
| Parameter | mPSAD | MRI-PMbdex |
|---|---|---|
| Sensitivity | 887/934 (95.0) | 887/934 (95.0) |
| Specificity | 294/2091 (19.6) | 765/1498 (51.1) |
| Negative predictive value | 294/341 (86.2) | 765/812 (94.2) |
| Positive predictive value | 887/2091 (42.4) | 887/1620 (54.8) |
| Accuracy | 1181/2432 (48.6) | 1652/2432 (67.9) |
| Avoided biopsies | 341/2432 (14.0) | 812/2432 (33.4) |
| Missed csPCa | 47/934 (5%) | 47/934 (5%) |
| Odds ratios (95% CI) | 4.61 (3.35–6.35) | 19.70 (14.44–26.86) |
| p Value | <0.001 | <0.001 |
| GG 2 | 25 | 25 |
| GG 3 | 13 | 22 |
| GG 4 | 8 | 0 |
| GG 5 | 1 | 0 |
| Parameter | mPSAD | MRI-PMbdex |
|---|---|---|
| Sensitivity | 50/55 (90.9) | 37/55 (67.3) |
| Specificity | 106/495 (21.4) | 434/495 (87.7) |
| Negative predictive value | 106/111 (95.5) | 434/452 (96.0) |
| Positive predictive value | 50/439 (11.4) | 37/98 (67.3) |
| Accuracy | 156/550 (28.4) | 471/550 (85.6) |
| Avoided biopsies | 111/550 (20.2) | 452/550 (82.2) |
| Missed csPCa | 5/55 (9.1) | 18/55 (32.7) |
| Odds ratio (95% CI) | 2.27 (1.06–7.00) | 14.62 (7.84–27, 29) |
| p Value | =0.033 | <0.001 |
| GG 2 | 4 | 13 |
| GG 3 | 1 | 5 |
| GG 4 | 0 | 0 |
| GG 5 | 0 | 0 |
| Parameter | mPSAD | MRI-PMbdex |
|---|---|---|
| Sensitivity | 101/109 (92.7) | 86/109 (78.9) |
| Specificity | 110/536 (20.5) | 279/536 (52.1) |
| Negative predictive value | 110/118 (93.2) | 279/302 (92.4) |
| Positive predictive value | 101/527 (19.2) | 86/343 (25.1) |
| Accuracy | 211/645 (32.5) | 365/645 (56.6) |
| Avoided biopsies | 118/645 (18.3) | 302/645 (46.8) |
| Missed csPCa | 8/109 (7.3) | 23/109 (21.1) |
| Odds Ratio (95% CI) | 3.26 (1.54–6.90) | 4.06 (2.49–6.63) |
| p Value | <0.001 | <0.001 |
| GG 2 | 5 | 12 |
| GG 3 | 2 | 11 |
| GG 4 | 1 | 0 |
| GG 5 | 0 | 0 |
| Parameter | mPSAD | MRI-PMbdex |
|---|---|---|
| Sensitivity | 414/439 (94.3) | 433/439 (98.6) |
| Specificity | 65/402 (16.2) | 42/402 (12.2) |
| Negative predictive value | 65/90 (72.2) | 49/55 (89.1) |
| Positive predictive value | 414/751 (55.1) | 433/786 (55.1) |
| Accuracy | 479/841 (57.0) | 482/841 (57.3) |
| Avoided biopsies | 90/841 (10.7) | 55/841 (6.5) |
| Missed csPCa | 25/439 (5.7) | 6/439 (1.4) |
| Odds Ratio (95% CI) | 3.19 (1.97–5.18) | 10.02 (4.24–23.66) |
| p Value | <0.001 | <0.001 |
| GG 2 | 12 | 1 |
| GG 3 | 8 | 5 |
| GG 4 | 5 | 0 |
| GG 5 | 0 | 0 |
| Parameter | mPSAD | MRI-PMbdex |
|---|---|---|
| Sensitivity | 322/331 (97.3) | 331/331 (100) |
| Specificity | 13/65 (20.0) | 3/65 (4.6) |
| Negative predictive value | 13/22 (59.1) | 3/3 (100) |
| Positive predictive value | 322/374 (86.1) | 331/393 (84.2) |
| Accuracy | 335/396 (84.6) | 334/396 (84.3) |
| Avoided biopsies | 22/396 (5.6) | 3/396 (0.8) |
| Missed csPCa | 9/331 (2.7) | 0/331 (0) |
| Odds Ratio (95% CI) | 8.94 (3.63–21.98) | - |
| p Value | <0.001 | =0.004 |
| GG 2 | 2 | 0 |
| GG 3 | 3 | 0 |
| GG 4 | 3 | 0 |
| GG 5 | 1 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morote, J.; Borque-Fernando, A.; Triquell, M.; Celma, A.; Regis, L.; Mast, R.; de Torres, I.M.; Semidey, M.E.; Abascal, J.M.; Servian, P.; et al. Comparative Analysis of PSA Density and an MRI-Based Predictive Model to Improve the Selection of Candidates for Prostate Biopsy. Cancers 2022, 14, 2374. https://doi.org/10.3390/cancers14102374
Morote J, Borque-Fernando A, Triquell M, Celma A, Regis L, Mast R, de Torres IM, Semidey ME, Abascal JM, Servian P, et al. Comparative Analysis of PSA Density and an MRI-Based Predictive Model to Improve the Selection of Candidates for Prostate Biopsy. Cancers. 2022; 14(10):2374. https://doi.org/10.3390/cancers14102374
Chicago/Turabian StyleMorote, Juan, Angel Borque-Fernando, Marina Triquell, Anna Celma, Lucas Regis, Richard Mast, Inés M. de Torres, María E. Semidey, José M. Abascal, Pol Servian, and et al. 2022. "Comparative Analysis of PSA Density and an MRI-Based Predictive Model to Improve the Selection of Candidates for Prostate Biopsy" Cancers 14, no. 10: 2374. https://doi.org/10.3390/cancers14102374
APA StyleMorote, J., Borque-Fernando, A., Triquell, M., Celma, A., Regis, L., Mast, R., de Torres, I. M., Semidey, M. E., Abascal, J. M., Servian, P., Santamaría, A., Planas, J., Esteban, L. M., & Trilla, E. (2022). Comparative Analysis of PSA Density and an MRI-Based Predictive Model to Improve the Selection of Candidates for Prostate Biopsy. Cancers, 14(10), 2374. https://doi.org/10.3390/cancers14102374