1. Introduction
On 31 December 2019, the World Health Organization (WHO) was informed about the first “cases of pneumonia of unknown etiology” (later identified as the SARS-CoV-2 (COVID-19)). The virus was confirmed to have reached Europe on 24 January 2020, when the first COVID-19 case was identified in France. On 30 January 2020, the virus was identified in Italy, followed by a wave of massive infections in the north of Italy, putting its healthcare system on the edge of breaking. Two weeks later, a similar situation was observed in France, with an unprecedented swell of patients’ hospitalization, ICU beds saturation, and medical staff shortage, leading to a total lockdown between 17 March 2020 and 11 May 2020.
The way in which to manage cancer patients and pursue oncological practice in this context was of high challenge. In China, due to the complexity of the situation, it was decided to postpone postoperative chemotherapy, to withhold chemotherapy when concomitantly prescribed with radiation, and to reduce chemotherapy doses in older and/or frail patients. In France, the first guidelines to ensure patient protection and make oncology departments “sanctuaries” free of COVID-19 were released on 25 March 2020 [
1]. The recommendations were largely based on the Chinese experience, but also on worrisome data from Italy.
Here, we present how these guidelines were implemented at the “Institut de Cancérologie des Hospices de Lyon” (IC-HCL), a French hospital overload with COVID-19 patients during the peak of the pandemic (March–May 2020). The measures put in place to protect patients and caregivers are described in a narrative summary as well as how these measures have impacted the IC-HCL activities in terms of treatment sessions, consultations, surgical procedures, and multidisciplinary team meetings (MDTMs). The number of patients with solid cancer hospitalized for COVID-19 during this period was also collected as their characteristics in terms of cancer type, stage, and co-morbidities.
2. Materials and Methods
Period of reference: Spring 2020 corresponds to the 3 month period of the first wave of the COVID-19 pandemic in France: March 2020 to May 2020. Winter 2019–2020 corresponds to the 3 month period from December 2019 to February 2020. Spring 2019 corresponds to the 3 month period from March 2019 to May 2019. Data were collected for spring 2020, winter 2019–2020, and spring 2019. Here, we defined winter 2019-2020 (the three months immediately before COVID-19 pandemic) as our period of reference, compared to spring 2020. Comparison between spring 2020 and spring 2019 activities are provided in some cases for complementary information.
Data were collected for solid tumor cancer patients only.
Strategies put in place to avoid cross-contamination between patients and caregivers, and treatment adjustments: Ten heads of oncology departments from different specialties (pulmonology, digestive, medical oncology and gynecology, dermatology, neuro-oncology) were asked to fill an electronic questionnaire concerning the measures taken in spring 2020 to counter the COVID-19 epidemic within the hospital.
Treatment dispensations: Data were collected from the 4 oncological treatment platforms of the IC-HCL. Collected data included IV systemic therapies (chemotherapies, immunotherapies, etc.). Radiotherapies were not included in this dataset (impossibility for radiotherapists to provide these data for the concerned periods).
MDTMs: The number of patient files discussed per month were collected from the 17 MDTMs (10 specialties) that are run weekly at the IC-HCL.
Consultations: The number of physical and teleconsultations (phone) per week were provided by the medical information department. Aside from the medical oncology department, in the other departments, it was not possible to distinguish oncological from non-oncological consultations.
Surgical procedures: Data were collected for the head and neck and thoracic surgery departments. For gynecology procedures, data were extrapolated from Lamblin et al. [
2]. Data from other specialties were not available for technical reasons (impossibility to distinguish cancer-related surgeries from others). The number of HCL operating rooms that remained opened during spring 2020 was extracted from an article by Philouze et al. [
3].
Clinical trials: The status of HCL-sponsored trials during spring 2020 (opened or closed) was provided by the HCL research department. Monthly trial enrolment rate for cancer trials (HCL-sponsored trials and external sponsored trials) were provided by the IC-HCL clinical research assistants from each specialty.
Patients: The number of patients hospitalized for COVID-19 during spring 2020 was provided by the medical information department. Among them, a retrospective study (NCT04910633) was conducted on patients with an “active” solid cancer (i.e., patients who were following an oncological treatment). The following data were collected: sex, age, cancer type, cancer stage, type of anti-cancer treatment, nature of comorbidities (3 maximum), vital status, COVID-19 severity (based on chest X-ray damage (low ≤ 25%, medium: between 25 and 50%, high > 50%) and for those who died, causality between COVID-19 status and death.
3. Results
3.1. Strategies Put in Place to Avoid Cross-Contamination between Patients and Caregivers
In early March 2020, the following measures were put in place in oncology departments: phone calls prior to patient hospital visit, in order to verify the absence of COVID-19 symptoms; request for patient to come alone; assignment of dedicated caregivers to screen COVID-19 symptoms using questionnaires and measuring patient’s temperature; reorganization of waiting rooms to respect social distancing; mandatory hand sanitization and protective face masks for both patients and professionals; installation of curtains and screens to avoid cross-contamination between roommates for double rooms; set-up of a dedicated space organized for patients with severe COVID-19 symptoms (low blood oxygen, important coughing, difficulty breathing, etc.) prior to hospitalization; and maintaining of doors being closed for patients that were requested to not circulate outside their room.
3.2. Treatment Adjustments
The reported treatment adjustments made at the IC-HCL were as follows: switch from IV to oral therapy whenever possible (5FU was replaced by capecitabine; prescription of temporary hormone therapy for HER-positive breast cancer patients); modification of the administration schedule to reduce the frequency of treatment administration (pembrolizumab 200 mg every three weeks was replaced by pembrolizumab 400 mg every 6 weeks; nivolumab 240 mg every two weeks was replaced by nivolumab 480mg every month; weekly 80 mg/m2 paclitaxel was replaced by 175 mg/m2 paclitaxel with granulocyte colony-stimulating factor (G-CSF) every 3 weeks; cancelation of 1/2 trastuzumab/cetuximab administration for patients having received maintenance treatment for several months/year(s)); switch of the type of the molecule to reduce the duration of the hospitalization (cisplatin was replaced by carboplatin whenever possible); and generalization of G-CSF prescription—even in patients with low-risk of febrile neutropenia.
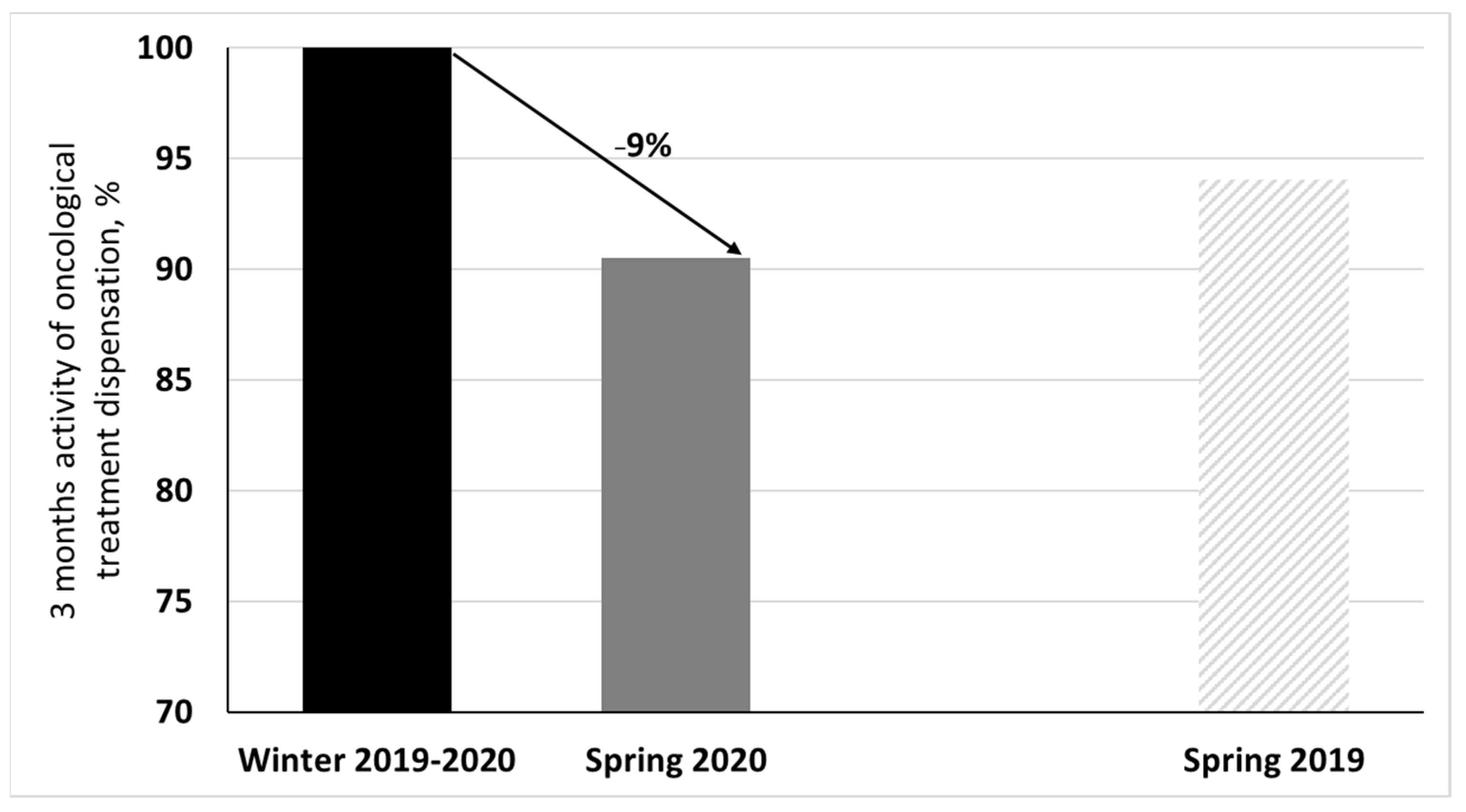
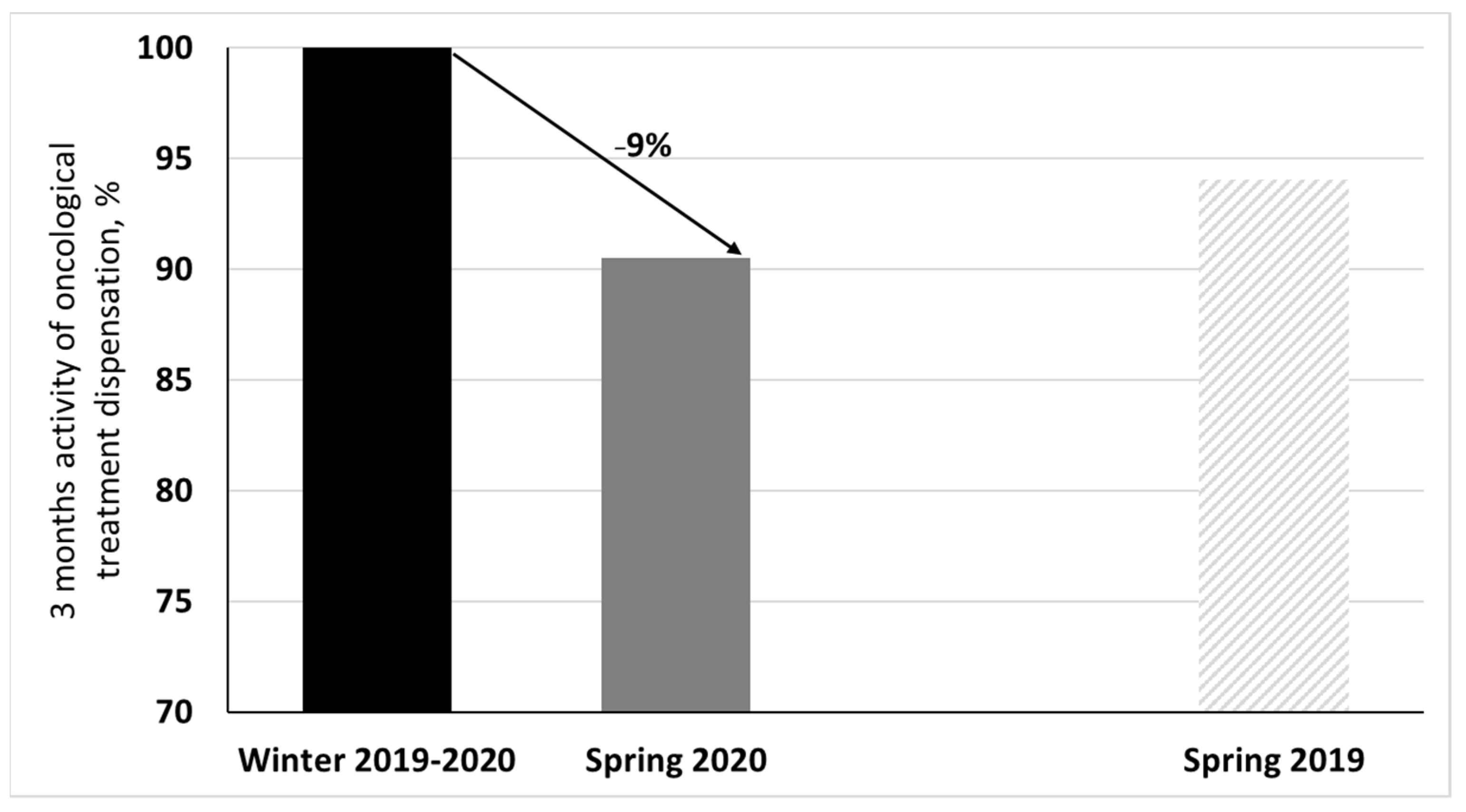
3.3. Treatment Dispensations
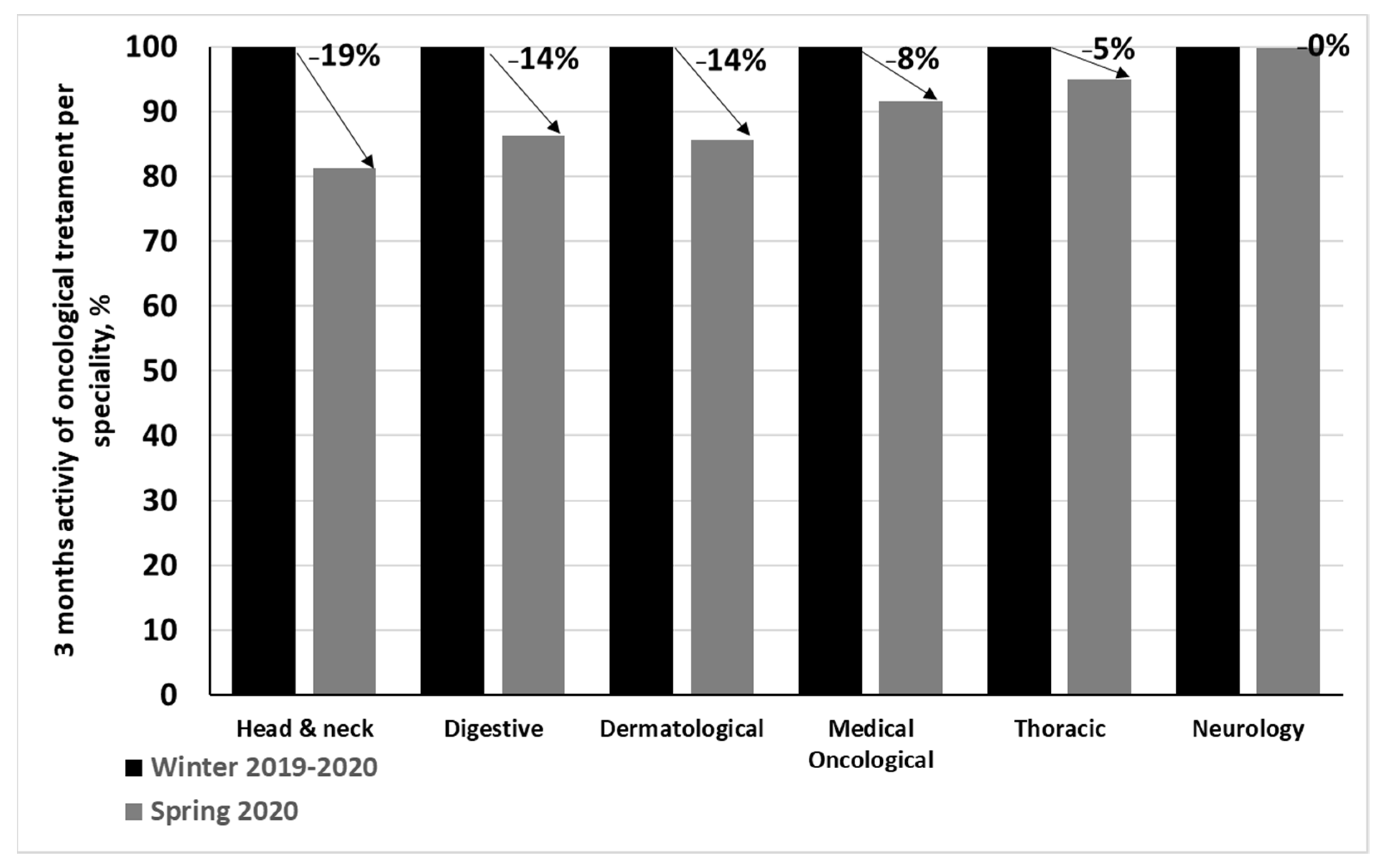
A total of 6960 oncological treatment sessions were conducted during spring 2019—they were 7400 during winter 2019–2020 and 6699 during spring 2020. The decrease of activity between spring 2020 and the period of reference (winter 2019–2020) was 9% (
Figure 1).
The most impacted specialties were head and neck (−19%), digestive (−14%), and dermatology (−14%). Medical oncology and thoracic activities were respectively impacted by −8%, and −5%. Neurology was not impacted (0%;
Figure 2).
3.4. Multidisciplinary Team Meetings (MDTMs)
In total, there was a decrease of 17% of MDTM activity. The most impacted specialties were dermatology (31%), urology (31%), thyroid (28%), gynecology (27%), and medical oncology (24%), followed by digestive (18%), neurology (18%), thoracic (15%), and endocrine tumors (12%). The least impacted specialty was head and neck (7%;
Table 1).
3.5. Consultations
Teleconsultations represented 0% of all consultations in January (0/1221), 0% in February 2020 (0/1148), 29% in March (407/1381), 42% in April (430/1035), and 24% in May (217/919).
3.6. Surgical Procedures for Cancer Treatment
A total of 173 head and neck surgeries were conducted during spring 2019—they were 203 during winter 2019–2020 and 158 during spring 2020. The decrease of activity between spring 2020 and the period of reference (winter 2019–2020) was 22%.
For thoracic surgeries, the decrease of activity was 18% (
Table 2).
Criteria to postpone surgery were decided by each department depending on operating room and staff availability of each IC-HCL site and the patient’s specific condition.
During spring 2020, 3 surgeries were postponed/cancelled for head and neck cancers (161 planned versus 158 performed) and 19 for thoracic cancers (209 planned versus 190 performed). Moreover, among the 115 gynecological surgical procedures planned, 40 (34.8%) were postponed, 7 (6.1%) were cancelled, and 9 (7.8%) had been modified in comparison with the initial surgery strategy [
2]. In total, the number of operating rooms was reduced from 20 to 5 as they were gradually reassigned to new COVID-19 intensive care units [
3].
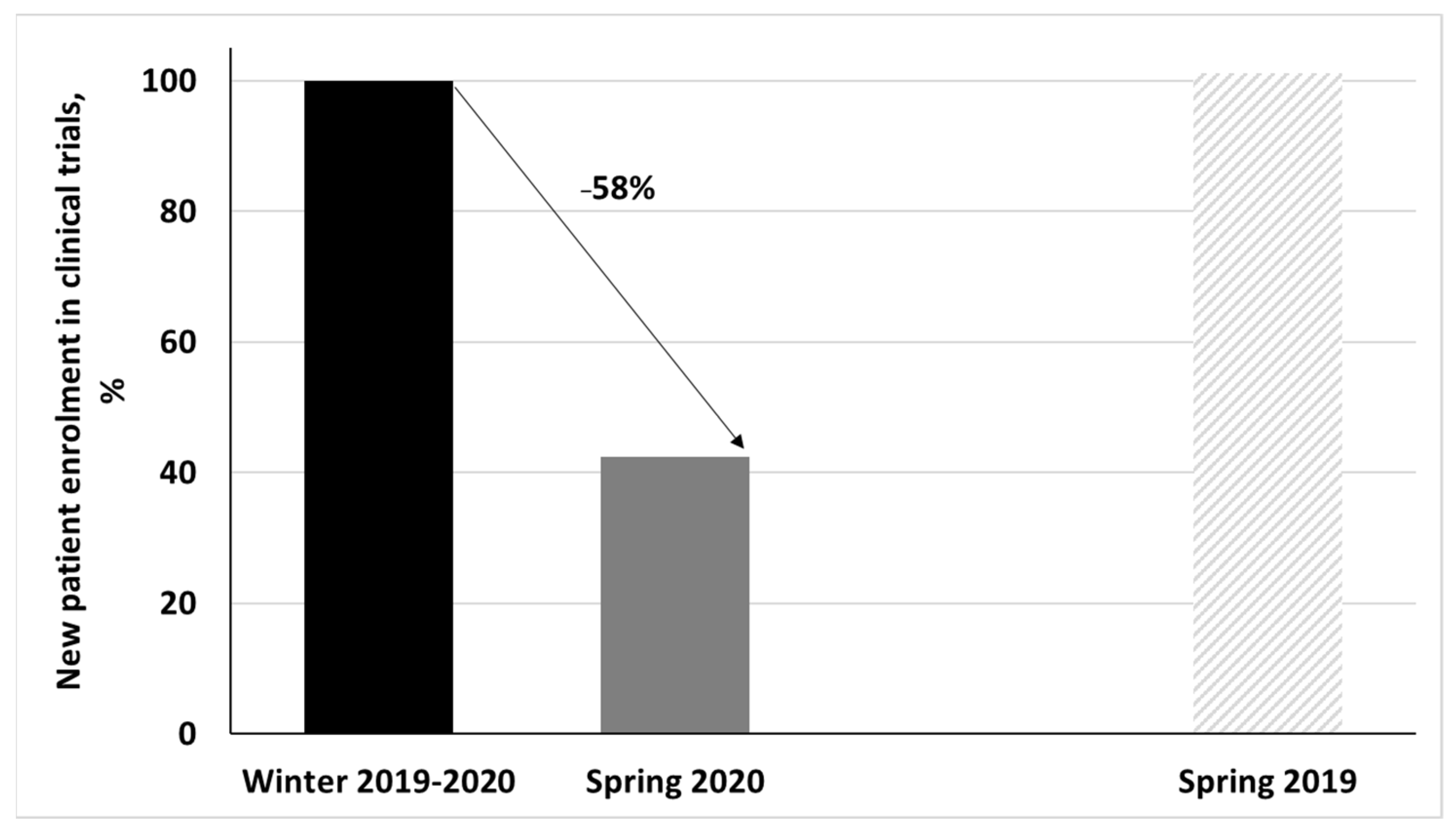
3.7. Clinical Trials
They were 244 HCL-sponsored clinical trials opened to inclusion during winter 2019–2020 (29/224 being dedicated to cancer patients). In total, 224/244 (91%) were suspended at the beginning of March 2020. Among the 20 trials that remained opened, 11 were cancer trials.
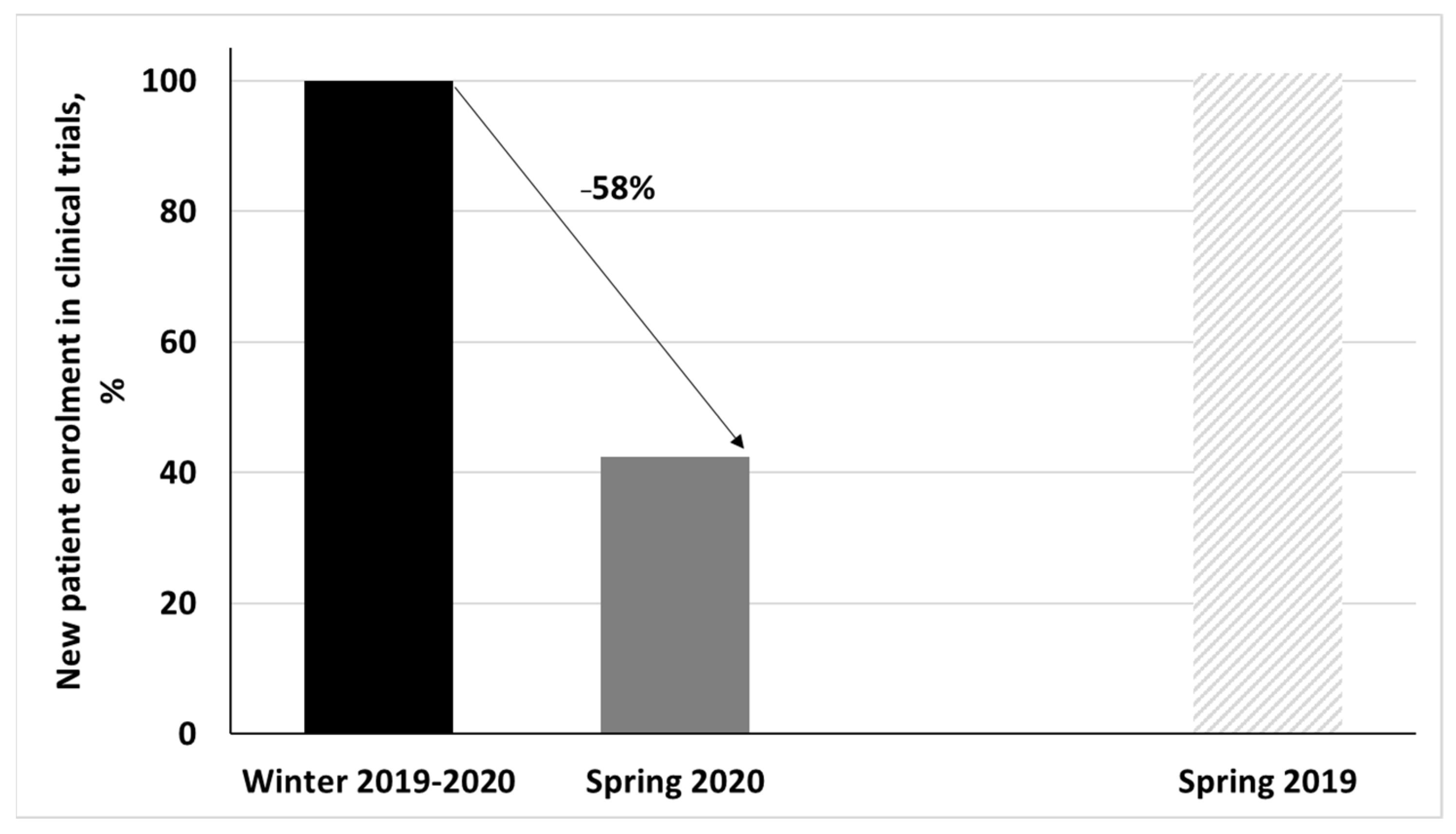
During spring 2020, 39 patients were included in cancer trials (HCL-sponsored trial and external sponsored trials) compared to 92 during winter 2019–2020 and 93 during spring 2019. The inclusion rate decrease was 58% compared to the period of reference (
Figure 3).
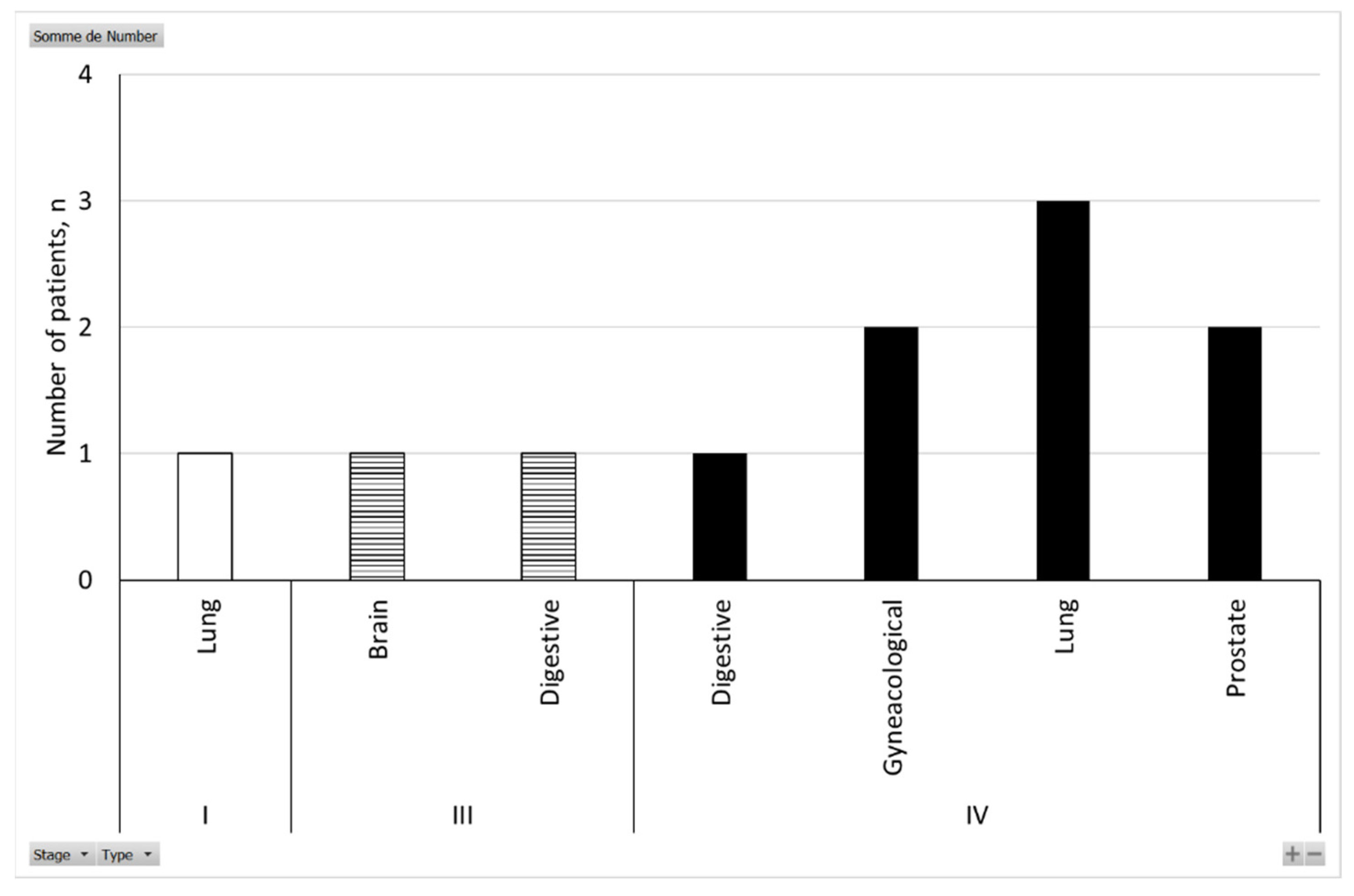
3.8. Patients
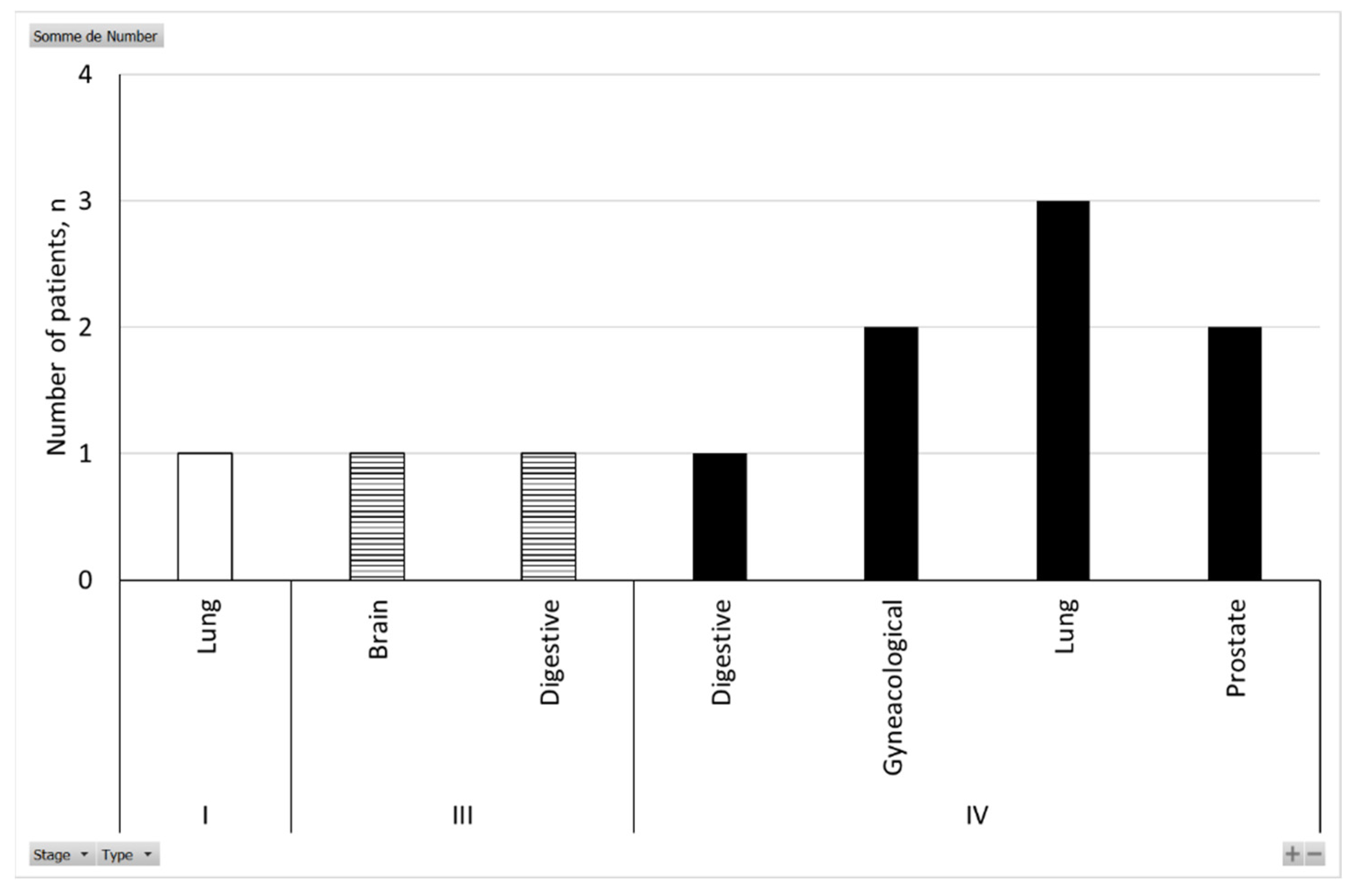
A total of 1781 patients were hospitalized at the HCL for COVID-19 during spring 2020; 333 died (18.7%). Our retrospective study identified 43 patients that were following an oncological treatment for solid cancer during this period; 51% died (22/43). Half of the deaths were linked to COVID-19 (11/22), and the other half to cancer progression (11/22). For the deaths linked to COVID-19, 82% of patients were above 70 years old (9/11) and 73% were stage IV (8/11;
Figure 4). Lung cancer was the most represented cancer type, with 36% of patients (4/11;
Figure 4). All patients were suffering from at least one comorbidity, with hypertension being the most representative (73%; 8/11), followed by diabetes (45%; 5/11) and vascular disorders (36%; 4/11).
4. Discussion
When the COVID-19 pandemic outbreak reached Europe, oncological learned societies quickly released guidelines to ensure patient protection [
1,
4,
5,
6,
7,
8,
9,
10,
11,
12,
13,
14,
15,
16,
17,
18]. Recommendations were made to minimize patient presence at the hospital; it was recommended to prefer online consultations, to use oral instead of intravenous drugs, to interspace drugs and irradiation scheduling, and to allow temporary breaks in the treatment of advanced-line patients with chronic diseases. The authors also suggested to prioritize hospital visits based on curative intent, age, life-expectancy, earlier line of treatment, severity of symptoms, and palliative care need. The results of the present study indicate that the adjustments made at the IC-HCL are totally in line with these recommendations. These have, however, not greatly impacted the activity of the IC-HCL in terms of the number treatment dispensations.
It would be of interest to compare the effect of the approach used in the IC-HCL to that of other centers in Europe, but, to the best of our knowledge, similar data have yet to be published.
IV treatment administrations schedules were not greatly modified, and patients continued to come to the hospital to receive their treatment. However, medical consultations were mostly switched to teleconsultations, especially during the highest peak of the pandemic in April 2020. This avoided changes in the therapeutic plan of patients that is reported to lead to high level of anxiety, distress, and fear [
19]. Unlike IV treatments, cancer surgery was differently impacted by COVID-19 depending on specialty. Indeed, thoracic and head and neck operations were not greatly impacted by the COVID-19 epidemic, while half of the gynecological surgeries were cancelled because of the COVID-19 outbreak [
2]. This surgical triage was perhaps not optimal as it is now proven that a 12 week surgery delay results in overall survival being decreased for breast cancer patients [
20].
Accordingly, the number of patients’ files discussed at the MDTMs did not decrease significantly for head and neck and thoracic specialties compared to gynecological specialties. Data concerning the other specialties are needed in order to confirm this result.
It is of note that clinical research was the most impacted activity in our institution, as almost all HCL-sponsored trials were suspended. This is concordant with the report by Upadhaya et al. who found that only 20% of the research institutions in the United States and 14% of the research institutions in Europe continued to enroll patients at their usual rate during the first wave of the COVID-19 pandemic period [
21].
Regarding the link between COVID-19 and the mortality of cancer patients, the results of the present small study are in concordance with the current understanding that adverse COVID-19 outcomes are principally driven by advanced stage, age, and the presence of other non-cancer comorbidities and that the risk to develop severe or critical symptoms of COVID-19 is correlated with factors co-occurring in cancer patients and not to the cancer condition per se [
22,
23,
24,
25,
26]. The results of the present study also correlate with the findings that lung cancer seems to be an important risk factor for COVID-19 severity, certainly due to factors related to underlying pulmonary condition, as well as lower acceptance rate in critical care [
27,
28]. Our study has important limitations (small size sample, observational results only, no control cases, first wave patients not affected by new variants) that, however, restrict these conclusions.
5. Conclusions
While a number of routines and treatment regimens were changed, there was no major decline in numbers of treatments conducted at the IC-HCL during the first wave of the COVID-19 pandemic that hit France between March and May 2020, except for clinical trials and some surgery acts. For the next waves, it would be of interest to maintain the research activity to prevent drug discovery attrition and patients access to new treatments. The modification of surgical triage guidelines for future COVID-19 waves should also be implemented for certain specialties to limit patients’ loss of chance.
Author Contributions
Conceptualization, G.F.; methodology, G.F. and A.-S.B.; formal analysis, C.S.; investigation, A.-S.B., C.S., A.B., S.C. (Stéphanie Cartalat), M.C. (Marion Chauvenet) and M.C. (Marc Colombel), S.D., T.D., M.D. (Marie Darrason) and M.D. (Michael Duruisseaux), G.D., M.G., O.G., P.P., F.T. and T.W.; writing—original draft preparation, A.-S.B. and C.S.; writing—review and editing, A.-S.B., S.C. (Sara Calattini) and all authors; supervision, G.F. and B.Y. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
An authorization to the LUH research data ethics committee was requested to conduct this retrospective study. A short protocol was written to describe the nature of the data to be collected, the primary and secondary objectives of the study, the methodology to access and preserve data, the persons in charge of data collection and analysis, etc. The study was conducted according to the guidelines of the Declaration of Helsinki and approved by LUH research data ethic committee (protocol 253, approved 28/04/2021. Conformité MR004 n°21_5253 and avis CSE n°21_253). In parallel, the study was registered on clinicaltrial. gov (NCT04910633) (3 June 2021).
Informed Consent Statement
Patients were informed that LUH could take the opportunity to re- use their medical data for COVID-19 research purposes unless an opposition was clearly provided. Patients that had raised an opposition were removed from our panel of studied patients (non-inclusion criteria).
Data Availability Statement
The data presented in this study are available on request from the corresponding authors. The data are not publicly available due to the necessity to make every effort to maintain patients non identifiable according to European law.
Acknowledgments
We would like to thank clinical research assistants, coordinators, and nurses who participated to the providing of data regarding clinical trials, MTDM numbers, and chemodaycare session figures.
Conflicts of Interest
The authors declare no conflict of interest.
References
- You, B.; Ravaud, A.; Canivet, A.; Ganem, G.; Giraud, P.; Guimbaud, R.; Kaluzinski, L.; Krakowski, I.; Mayeur, D.; Grellety, T.; et al. The official French guidelines to protect patients with cancer against SARS-CoV-2 infection. Lancet Oncol. 2020, 21, 619–621. [Google Scholar] [CrossRef] [Green Version]
- Lamblin, G.; Golfier, F.; Peron, J.; Moret, S.; Chene, G.; Nohuz, E.; Lebon, M.; Dubernard, G.; Cortet, M. Impact de la pandémie de Covid-19 sur les modifications thérapeutiques des patientes atteintes de cancers gynécologiques. Gynécologie Obs. Fertil. Sénologie 2020, 48, 777–783. [Google Scholar] [CrossRef] [PubMed]
- Philouze, P.; Cortet, M.; Quattrone, D.; Céruse, P.; Aubrun, F.; Dubernard, G.; Mabrut, J.Y.; Delignette, M.C.; Mohkam, K. Surgical activity during the Covid-19 pandemic: Results for 112 patients in a French tertiary care center, a quality improvement study. Int. J. Surg. 2020, 80, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Grellety, T.; Ravaud, A.; Canivet, A.; Ganem, G.; Giraud, P.; Guimbaud, R.; Kaluzinski, L.; Krakowski, I.; Mayeur, D.; Lotz, J.P.; et al. SARS-CoV-2/COVID 19 Infection and Solid Cancers: Synthesis of Recommendations for Health Professionals. Bull. Cancer 2020, 107, 400–402. [Google Scholar] [CrossRef] [PubMed]
- Giraud, P.; Monpetit, E.; Dieudonne, A. Epidémie de COVID-19 : Recommandations à l’usage des professionnels de l’Oncologie Radiothérapie. Cancer Radiother. 2020, 24, 87. [Google Scholar] [CrossRef] [PubMed]
- Penel, N.; Bonvalot, S.; Minard, V.; Orbach, D.; Gouin, F.; Corradini, N.; Brahmi, M.; Marec-Berard, P.; Briand, S.; Gaspar, N.; et al. Options thérapeutiques de prise en charge des sarcomes durant la pandémie COVID-19 : Propositions du groupe sarcome français. Bull. Cancer 2020, 107, 398–399. [Google Scholar] [CrossRef] [PubMed]
- Daste, A.; Guigay, J.; Borel, C.; Saâda-Bouzid, E.; Huguet, C.; Florence, L.T.; Biau, J.; Sire, C.; Baujat, B.; Cupissol, D.; et al. Recommandations d’experts Concernant la Prise en Charge des Patients Atteints de Cancer des VADS Pendant la Pandémie de COVID-19. Mise à jour du 26 mars 2020. ONCORIF 2020. Available online: https://www.oncorif.fr/wp-content/uploads/2020/03/COVID-19-ORL-Unicancer.pdf (accessed on 5 November 2021).
- Thureau, S.; Faivre, J.C.; Assaker, R.; Biver, E.; Confavreux, C.B.; Debiais, F.; Duterque-Coquillaud, M.; Giammarile, F.; Heymann, D.; Lecouvet, F.E.; et al. Adapting palliative radiation therapy for bone metastases during the Covid-19 pandemic: GEMO position paper. J. Bone Oncol. 2020, 22, 100291. [Google Scholar] [CrossRef] [PubMed]
- ASCO Special Report: A Guide to Cancer Care Delivery during the COVID-19 Pandemic. ASCO 2020. Available online: https://www.asco.org/sites/new-www.asco.org/files/content-files/2020-ASCO-Guide-Cancer-COVID19.pdf (accessed on 5 November 2021).
- Albrand, G.; Paricio, T.; Bengrine-Lefevre, L.; Boulahssas, R.; Bourcy, V.; Carola, É.; Corre, R.; Cudenne, T.; De Decker, L.; Dorval, E.; et al. COVID-19: Position de la SOFOG. SOFOG 2020. Available online: file:///C:/Users/MDPI/AppData/Local/Temp/COVID%2019%20-%20position%20de%20la%20SOFOG%20-%20SOFOG.pdf (accessed on 5 November 2021).
- Gligorov, J.; Bachelot, T.; Pierga, J.Y.; Antoine, E.C.; Balleyguier, C.; Barranger, E.; Belkacemi, Y.; Bonnefoi, H.; Bidard, F.C.; Ceugnart, L.; et al. COVID-19 and people followed for breast cancer: French guidelines for clinical practice of Nice-St Paul de Vence, in collaboration with the Collège Nationale des Gynécologues et Obstétriciens Français (CNGOF), the Société d’Imagerie de la Femme (SIFEM), the Société Française de Chirurgie Oncologique (SFCO), the Société Française de Sénologie et Pathologie Mammaire (SFSPM) and the French Breast Cancer Intergroup-UNICANCER (UCBG). Bull. Cancer 2020, 107, 528–537. [Google Scholar] [CrossRef] [PubMed]
- Di Fiore, F.; Sefrioui, D.; Gangloff, A.; Schwarz, L.; Tuech, J.; Phelip, J.; Lepage, C.; Aparicio, T.; Manfredi, S.; Lievre, A.; et al. Propositions Alternatives de Prise en Charge des Cancers Digestifs en Fonction de la Situation épidémique au COVID 19, Selon les Données de la Littérature et de L’expérience Chinoise. FFCD 2020. Available online: https://www.ffcd.fr/DOC/NEWSLETTER/COVID%20ONCODIG.pdf (accessed on 5 November 2021).
- Audigier-ValetteJ, C.; Bennouna, J.; Besse, B.; Cadranel, J.; Cortot, A.; Couraud, S.; Duruisseaux, M.; Girard, N.; Greillier, E.G.-L.L.; Mazières, J.; et al. Propositions de Prise en Charge des Patients Dans le Contexte de la Pandémie COVID-19Rédaction : Groupe D’experts Groupe D’Oncologie SPLF (Société de Pneumologie de Langue Française) et IFCT (Intergroupe Francophone de Cancérologie Thoracique) à la Date du 18 Mars 2020. SPLF 2020. Available online: https://splf.fr/wp-content/uploads/2020/03/COVID-FINALE-GOLF2020-03-19.pdf (accessed on 5 November 2021).
- Le Board du GINECO; Ray-Coquard, I.; Hardy-Bessard, A.C.; Lortholary, A.; Selle, F.; Pautier, P.; Leary, A.; Gladieff, L.; Kurtz, J.E.; Freyer, G.; et al. GINECO et le COVID19. GINECO 2020. Available online: https://sfc.asso.fr/wp-content/uploads/2020/03/Le-GINECO-et-le-COVID19final.pdf (accessed on 5 November 2021).
- Mejean, A.; Rouprêt, M.; Rozet, F.; Bensalah, K.; Murez, T.; Game, X.; Rebillard, X.; Mallet, R.; Faix, A.; Mongiat-Artus, P.; et al. Recommendations CCAFU on the Management of Cancers of the Urogenital System during an Epidemic with Coronavirus COVID-19. Prog. Urol. 2020, 30, 221–231. [Google Scholar] [CrossRef] [PubMed]
- Choquet, S.; Delmer, A.; Garçon, L.; Hunault, M.; Lamy, T.; Maloisel, F.; Maynadié, M.; Michallet, A.-S.; Raffoux, E.; Truchan-Graczyk, M. COVID-19 et Prise en Charge des Malades D’hématologie Propositions de la Société Française D’Hématologie (SFH). 17 Mars 2020. SFH 2020. Available online: https://sfh.hematologie.net/sites/sfh.hematologie.net/files/medias/documents/covid-19_propostion_sfh_17-03-2020_0.pdf (accessed on 5 November 2021).
- Classe, J.-M.; Dolivet, G.; Evrard, S.; Ferron, G.; Lécuru, F.; Leufflen, L.; Rivoire, M.; Sgarbura, O. Recommandations de la Société française de Chirurgie Oncologique (SFCO) Pour L’organisation de la Chirurgie Oncologique Durant l’épidémie de COVID-19. Bull. Cancer 2020, 107, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Alcantara, M.; Blay, J.-Y.; Dalle, S.; Damotte, D.; Delord, J.-P.; Depil, S.; Dreno, B.; Galon, J.; Gomez-Roca, C.; Houot, R.; et al. Recommandations de la societe française d’immunotherapie des cancers (fitc) et du groupe d’immuno-oncologie d’unicancer (GIO)concernant le traitement par immunotherapie de patients atteints de cancer dans le contexte d’épidémie de coronavirus SARS-COV. FITC 2020. Available online: https://www.fitcancer.fr/wp-content/uploads/2020/03/20200325_Recommandations-coronavirus.pdf (accessed on 5 November 2021).
- Gregucci, F.; Caliandro, M.; Surgo, A.; Carbonara, R.; Bonaparte, I.; Fiorentino, A. Cancer patients in Covid-19 era: Swimming against the tide. Radiother. Oncol. 2020, 149, 109–110. [Google Scholar] [CrossRef] [PubMed]
- Johnson, B.A.; Waddimba, A.C.; Ogola, G.O.; Fleshman, J.W.; Preskitt, J.T. A systematic review and meta-analysis of surgery delays and survival in breast, lung and colon cancers: Implication for surgical triage during the COVID-19 pandemic. Am. J. Surg. 2021, 222. [Google Scholar] [CrossRef] [PubMed]
- Upadhaya, S.; Xin Yu, J.; Oliva, C.; Hooton, M.; Hodge, J.; Hubbard-Lucey, V.M. Impact of COVID-19 on oncology clinical trials. Nat. Rev. Drug Dis. 2020, 19, 376–377. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.Y.W.; Cazier, J.B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.T.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.Y.; Desai, A.; de Lima Lopes, G.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Vivarelli, S.; Falzone, L.; Grillo, C.M.; Scandurra, G.; Torino, F.; Libra, M. Cancer Management during COVID-19 Pandemic: Is Immune Checkpoint Inhibitors-Based Immunotherapy Harmful or Beneficial? Cancers 2020, 12, 2237. [Google Scholar] [CrossRef] [PubMed]
- Jee, J.; Foote, M.B.; Lumish, M.; Stonestrom, A.J.; Wills, B.; Narendra, V.; Avutu, V.; Murciano-Goroff, Y.R.; Chan, J.E.; Derkach, A.; et al. Chemotherapy and COVID-19 Outcomes in Patients with Cancer. J. Clin. Oncol. 2020, 38, 3538–3546. [Google Scholar] [CrossRef] [PubMed]
- Péron, J.; Dagonneau, T.; Conrad, A.; Pineau, F.; Calattini, S.; Freyer, G.; Perol, D.; Sajous, C.; Heiblig, M. Covid-19 presentation and outcomes among cancer patients: A matched case-control study. Cancers 2021, 13, 5283. [Google Scholar] [CrossRef] [PubMed]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020, 21, 914–922. [Google Scholar] [CrossRef]
- Passaro, A.; Bestvina, C.; Velez Velez, M.; Garassino, M.C.; Garon, E.; Peters, S. Severity of COVID-19 in patients with lung cancer: Evidence and challenges. J. Immunother. Cancer 2021, 9, 2266. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}