
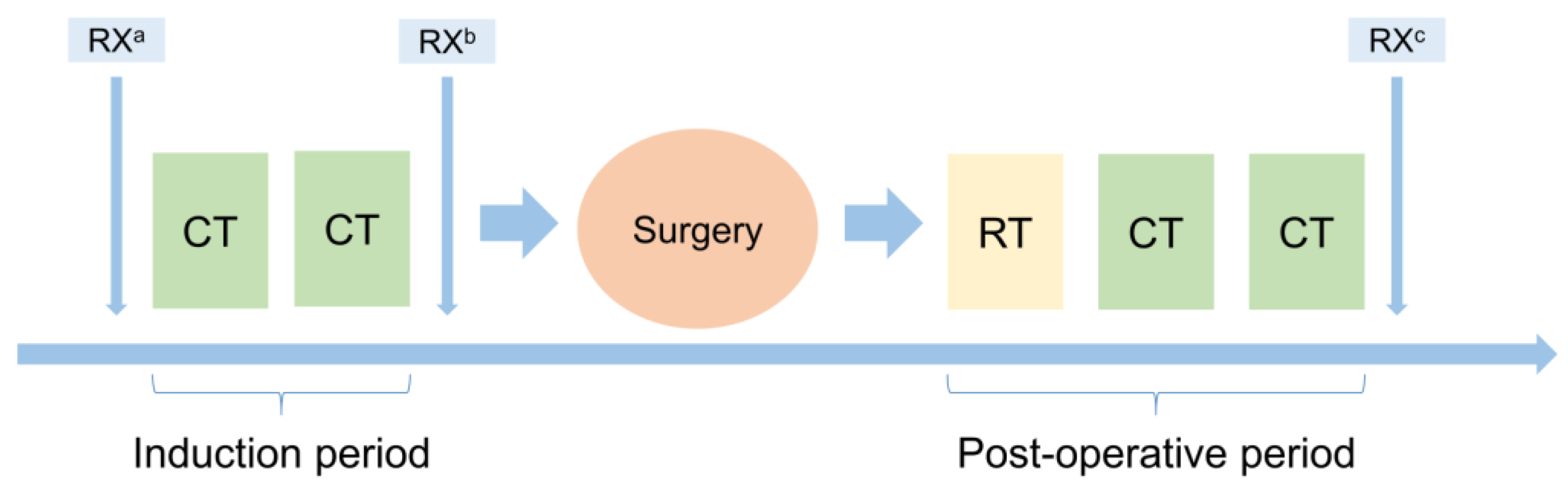
A Trimodality, Four-Step Treatment including Chemotherapy, Pleurectomy/Decortication and Radiotherapy in Early-Stage Malignant Pleural Mesothelioma: A Single-Institution Retrospective Case Series Study


 ,
,  ,
, 

 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients’ Selection and Data Collection
2.2. Objectives
2.3. Statistical Methods
3. Results
3.1. Induction Therapy
3.2. Surgery
3.3. Post-Operative RT
3.4. Post-Operative CT
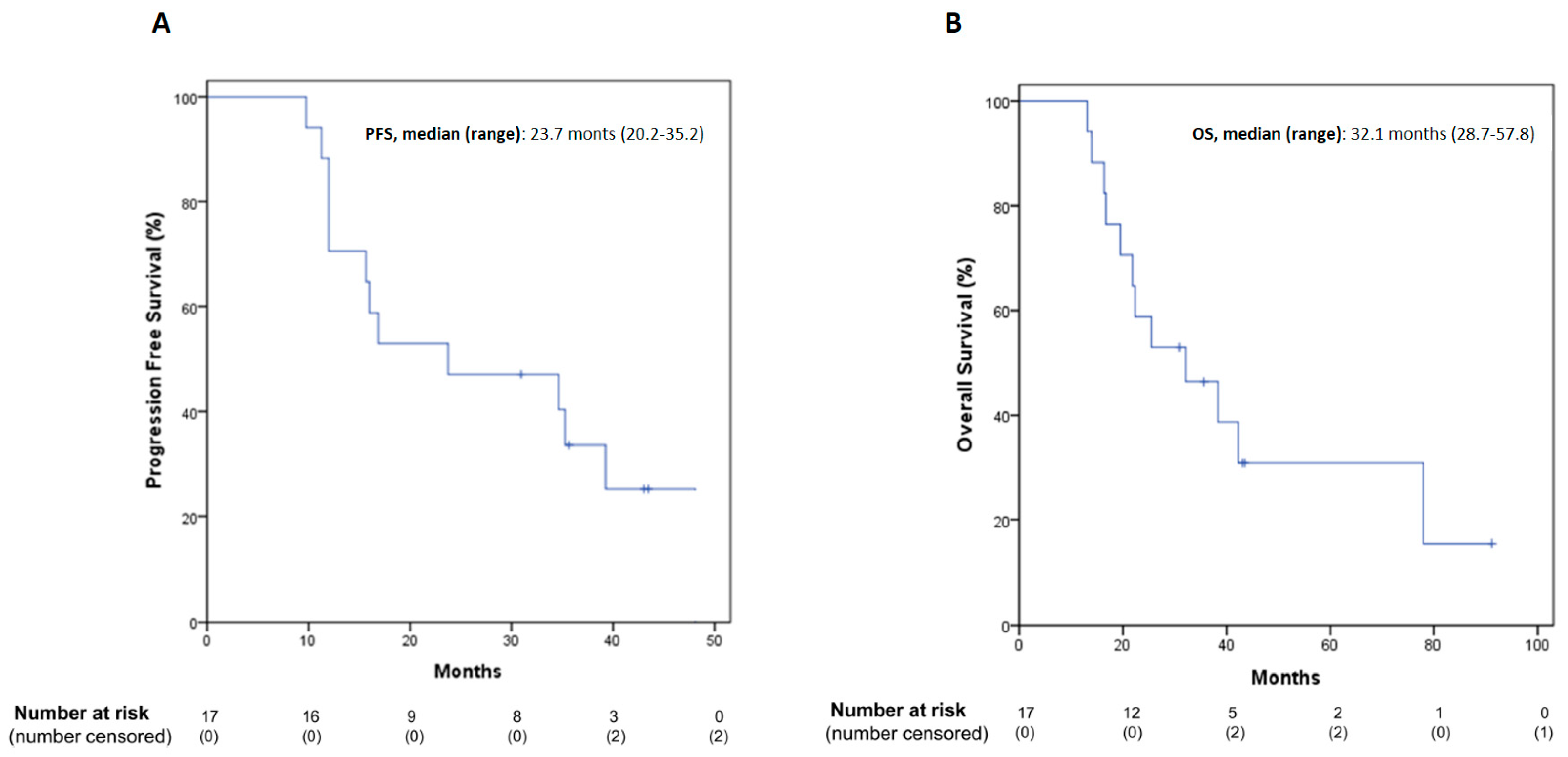
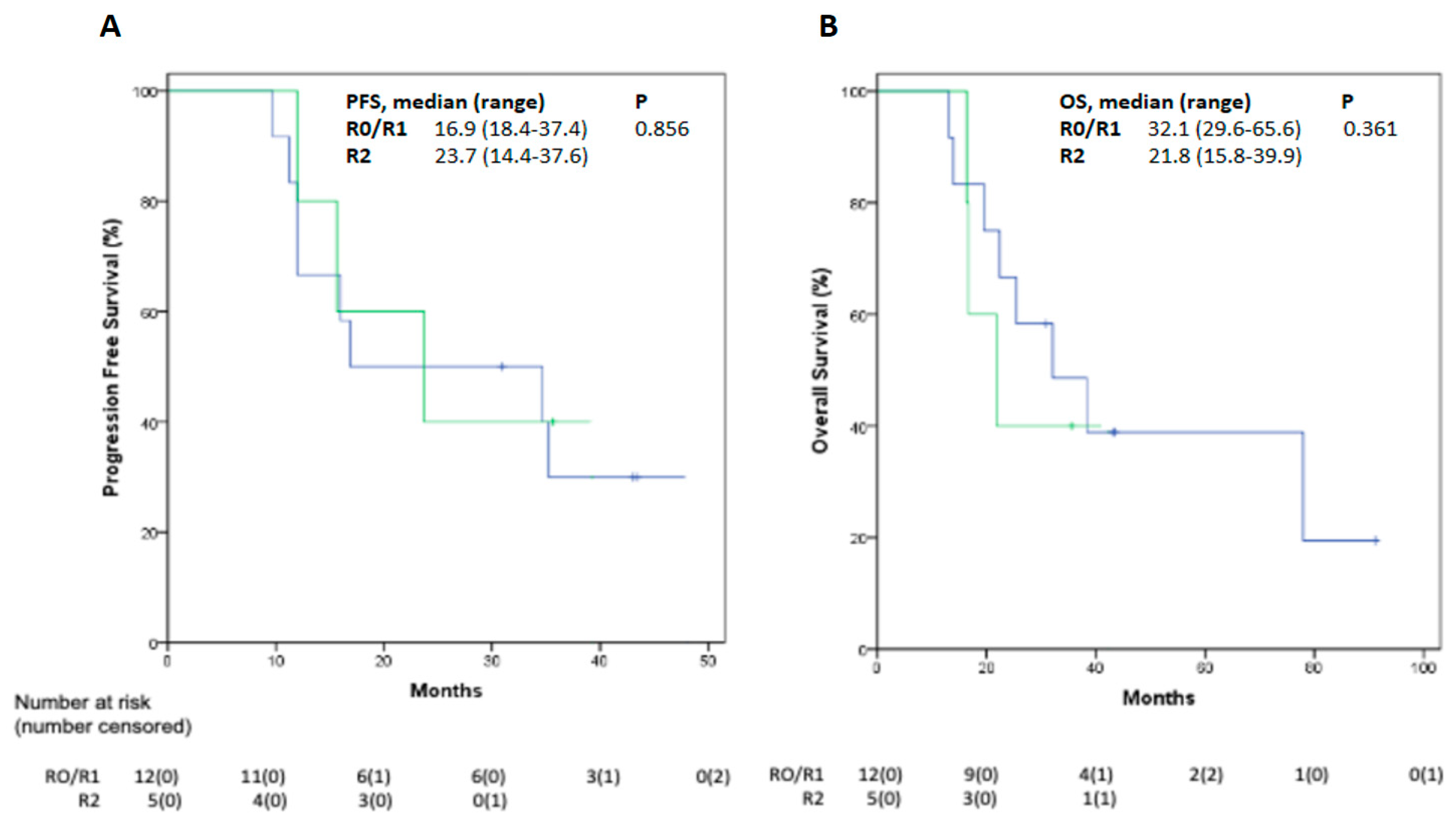
3.5. Follow-Up and Efficacy Outcomes
4. Comment
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tossavainen, A. Global use of asbestos and the incidence of mesothelioma. Int. J. Occup. Environ. Health 2004, 10, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Popat, S.; Baas, P.; Faivre-Finn, C.; Girard, N.; Nicholson, A.G.; Nowak, A.K.; Opitz, I.; Scherpereel, A.; Reck, M.; on behalf of the ESMO Guidelines Committee. Malignant pleural mesothelioma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2021. in press. [Google Scholar] [CrossRef] [PubMed]
- Metintas, M.; Ucgun, I.; Elbek, O.; Erginel, S.; Metintas, S.; Kolsuz, M.; Harmanci, E.; Alatas, F.; Hillerdal, G.; Ozkan, R.; et al. Computed tomography features in malignant pleural mesothelioma and other commonly seen pleural diseases. Eur. J. Radiol. 2002, 41, 1–9. [Google Scholar] [CrossRef]
- Kim, R.Y.; Sterman, D.H.; Haas, A.R. Malignant Mesothelioma: Has Anything Changed? Semin. Respir. Crit. Care Med. 2019, 40, 347–360. [Google Scholar] [CrossRef] [PubMed]
- Zauderer, M.G.; Krug, L.M. The evolution of multimodality therapy for malignant pleural mesothelioma. Curr. Treat. Options Oncol. 2011, 12, 163–172. [Google Scholar] [CrossRef] [Green Version]
- Buduhan, G.; Menon, S.; Aye, R.; Louie, B.; Mehta, V.; Vallières, E. Trimodality therapy for malignant pleural mesothelioma. Ann. Thorac. Surg. 2009, 88, 870–875. [Google Scholar] [CrossRef]
- Viscardi, G.; Di Liello, R.; Morgillo, F. How I treat malignant pleural mesothelioma. ESMO Open 2020, 4, e000669. [Google Scholar] [CrossRef] [Green Version]
- Verma, V.; Ahern, C.A.; Berlind, C.G.; Lindsay, W.D.; Sharma, S.; Shabason, J.; Culligan, M.J.; Grover, S.; Friedberg, J.S.; Simone, C.B. National Cancer Database Report on Pneumonectomy Versus Lung-Sparing Surgery for Malignant Pleural Mesothelioma. J. Thorac. Oncol. 2017, 12, 1704–1714. [Google Scholar] [CrossRef] [Green Version]
- Bovolato, P.; Casadio, C.; Billè, A.; Ardissone, F.; Santambrogio, L.; Ratto, G.B.; Garofalo, G.; Bedini, A.V.; Garassino, M.; Porcu, L.; et al. Does Surgery Improve Survival of Patients with Malignant Pleural Mesothelioma?: A Multicenter Retrospective Analysis of 1365 Consecutive Patients. J. Thorac. Oncol. 2014, 9, 390–396. [Google Scholar] [CrossRef] [Green Version]
- Sugarbaker, D.J.; Jaklitsch, M.T.; Bueno, R.; Richards, W.; Lukanich, J.; Mentzer, S.J.; Colson, Y.; Linden, P.; Chang, M.; Capalbo, L.; et al. Prevention, early detection, and management of complications after 328 consecutive extrapleural pneumonectomies. J. Thorac. Cardiovasc. Surg. 2004, 128, 138–146. [Google Scholar] [CrossRef] [Green Version]
- Bertoglio, P.; Ambrogi, M.C.; Chella, A.; Aprile, V.; Dini, P.; Korasidis, S.; Fanucchi, O.; Mussi, A. Is less also better? A single-institution experience on treatment of early stage Malignant Pleural Mesothelioma. Eur. J. Surg. Oncol. 2017, 43, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Santini, M.; Vicidomini, G. Instrumental diagnosis of mesothelioma: The thoracoscopy. In Mesothelioma from the Bench Side to Clinic; Baldi, A., Ed.; Nova Science Publishers: Hauppauge, NY, USA, 2008; pp. 389–403. ISBN 9781600217890. [Google Scholar]
- Hasegawa, S.; Kondo, N.; Matsumoto, S.; Takuwa, T.; Hashimoto, M.; Kuroda, A.; Nakamichi, T.; Kamikonya, N.; Tsujimura, T.; Nakano, T. Surgical Risk and Survival Associated with Less Invasive Surgery for Malignant Pleural Mesothelioma. Semin. Thorac. Cardiovasc. Surg. 2019, 31, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Lang-Lazdunski, L.; Bille, A.; Papa, S.; Marshall, S.; Lal, R.; Galeone, C.; Landau, D.; Steele, J.; Spicer, J. Pleurectomy/decortication, hyperthermic pleural lavage with povidone-iodine, prophylactic radiotherapy, and systemic chemotherapy in patients with malignant pleural mesothelioma: A 10-year experience. J. Thorac. Cardiovasc. Surg. 2015, 149, 556–558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pass, H.I.; Kranda, K.; Temeck, B.K.; Feuerstein, I.; Steinberg, S.M. Surgically debulked malignant pleural mesothelioma: Results and prognostic factors. Ann. Surg. Oncol. 1997, 4, 215–222. [Google Scholar] [CrossRef] [PubMed]
- Sugarbaker, D.J.; Flores, R.M.; Jaklitsch, M.T.; Richards, W.G.; Strauss, G.M.; Corson, J.M.; DeCamp, M.M.J.; Swanson, S.J.; Bueno, R.; Lukanich, J.M.; et al. Resection margins, extrapleural nodal status, and cell type determine postoperative long-term survival in trimodality therapy of malignant pleural mesothelioma: Results in 183 patients. J. Thorac. Cardiovasc. Surg. 1999, 117, 54–55. [Google Scholar] [CrossRef] [Green Version]
- Treasure, T.; Lang-Lazdunski, L.; Waller, D.; Bliss, J.M.; Tan, C.; Entwisle, J.; Snee, M.; O’Brien, M.; Thomas, G.; Senan, S.; et al. Extra-pleural pneumonectomy versus no extra-pleural pneumonectomy for patients with malignant pleural mesothelioma: Clinical outcomes of the Mesothelioma and Radical Surgery (MARS) randomised feasibility study. Lancet Oncol. 2011, 12, 763–772. [Google Scholar] [CrossRef]
- Bölükbas, S.; Manegold, C.; Eberlein, M.; Bergmann, T.; Fisseler-Eckhoff, A.; Schirren, J. Survival after trimodality therapy for malignant pleural mesothelioma: Radical Pleurectomy, chemotherapy with Cisplatin/Pemetrexed and radiotherapy. Lung Cancer 2011, 71, 75–81. [Google Scholar] [CrossRef]
- Lim, E.; Darlison, L.; Edwards, J.; Elliott, D.; Fennell, D.A.; Popat, S.; Rintoul, R.C.; Waller, D.; Ali, C.; Bille, A.; et al. Mesothelioma and Radical Surgery 2 (MARS 2): Protocol for a multicentre randomised trial comparing (extended) pleurectomy decortication versus no (extended) pleurectomy decortication for patients with malignant pleural mesothelioma. BMJ Open 2020, 10, e038892. [Google Scholar] [CrossRef]
- Rosskamp, M.; Macq, G.; Nackaerts, K.; Praet, M.; Van Eycken, L.; Van Meerbeeck, J.P.; De Schutter, H. Real-life treatment practice for malignant pleural mesothelioma in Belgium. Lung Cancer 2018, 125, 258–264. [Google Scholar] [CrossRef]
- Saddoughi, S.A.; Abdelsattar, Z.M.; Blackmon, S.H. National Trends in the Epidemiology of Malignant Pleural Mesothelioma: A National Cancer Data Base Study. Ann. Thorac. Surg. 2018, 105, 432–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Perrot, M.; Wu, L.; Wu, M.; Cho, B.C.J. Radiotherapy for the treatment of malignant pleural mesothelioma. Lancet Oncol. 2017, 18, e532–e542. [Google Scholar] [CrossRef]
- Dumane, V.; Yorke, E.; Rimner, A.; RosenzweigG, K. SU-E-T-595: Comparison of Volumetric Modulated Arc Therapy (VMAT) and Static Intensity Modulated Radiotherapy (IMRT) for Malignant Pleural Mesothelioma in Patients with Intact Lungs/Post Pleurectomy. Med. Phys. 2012, 39, 3842. [Google Scholar] [CrossRef]
- Raskin, J.; Surmont, V.; Cornelissen, R.; Baas, P.; van Schil, P.E.Y.; van Meerbeeck, J.P. A randomized phase II study of pleurectomy/decortication preceded or followed by (neo-)adjuvant chemotherapy in patients with early stage malignant pleural mesothelioma (EORTC 1205). Transl. Lung Cancer Res. 2018, 7, 593–598. [Google Scholar] [CrossRef]
- Oehl, K.; Vrugt, B.; Wagner, U.; Kirschner, M.B.; Meerang, M.; Weder, W.; Felley-Bosco, E.; Wollscheid, B.; Bankov, K.; Demes, M.C.; et al. Alterations in BAP1 Are Associated with Cisplatin Resistance through Inhibition of Apoptosis in Malignant Pleural Mesothelioma. Clin. Cancer Res. 2021, 27, 2277–2291. [Google Scholar] [CrossRef]
- Hassan, R.; Morrow, B.; Thomas, A.; Walsh, T.; Lee, M.K.; Gulsuner, S.; Gadiraju, M.; Panou, V.; Gao, S.; Mian, I.; et al. Inherited predisposition to malignant mesothelioma and overall survival following platinum chemotherapy. Proc. Natl. Acad. Sci. USA 2019, 116, 9008–9013. [Google Scholar] [CrossRef] [Green Version]
- Fennell, D.A.; King, A.; Mohammed, S.; Branson, A.; Brookes, C.; Darlison, L.; Dawson, A.G.; Gaba, A.; Hutka, M.; Morgan, B.; et al. Rucaparib in patients with BAP1-deficient or BRCA1-deficient mesothelioma (MiST1): An open-label, single-arm, phase 2a clinical trial. Lancet. Respir. Med. 2021, 9, 593–600. [Google Scholar] [CrossRef]
- Gomez, D.R.; Rimner, A.; Simone, C.B.; Cho, B.C.J.; de Perrot, M.; Adjei, A.A.; Bueno, R.; Gill, R.R.; Harpole, D.H.; Hesdorffer, M.; et al. The Use of Radiation Therapy for the Treatment of Malignant Pleural Mesothelioma: Expert Opinion from the National Cancer Institute Thoracic Malignancy Steering Committee, International Association for the Study of Lung Cancer, and Mesothelioma Applied Re. J. Thorac. Oncol. 2019, 14, 1172–1183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenzweig, K.E. Radiation Therapy for Malignant Pleural Mesothelioma. Thorac. Surg. Clin. 2020, 30, 473–480. [Google Scholar] [CrossRef] [PubMed]
- Van Gerwen, M.; Wolf, A.; Liu, B.; Flores, R.; Taioli, E. Short-term outcomes of pleurectomy decortication and extrapleural pneumonectomy in mesothelioma. J. Surg. Oncol. 2018, 118, 1178–1187. [Google Scholar] [CrossRef] [PubMed]
- Euhus, C.J.; Ripley, R.T. The Staging of Malignant Pleural Mesothelioma. Thorac. Surg. Clin. 2020, 30, 425–433. [Google Scholar] [CrossRef]
- Weder, W.; Stahel, R.A.; Bernhard, J.; Bodis, S.; Vogt, P.; Ballabeni, P.; Lardinois, D.; Betticher, D.; Schmid, R.; Stupp, R.; et al. Multicenter trial of neo-adjuvant chemotherapy followed by extrapleural pneumonectomy in malignant pleural mesothelioma. Ann. Oncol. 2007, 18, 1196–1202. [Google Scholar] [CrossRef] [PubMed]
- Cao, C.; Tian, D.H.; Pataky, K.A.; Yan, T.D. Systematic review of pleurectomy in the treatment of malignant pleural mesothelioma. Lung Cancer 2013, 81, 319–327. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Age, Median (Range) | 66 (58–73) |
| Age category, n (%) | |
| <70 | 15 (88.2) |
| ≥70 | 2 (11.8) |
| Sex, n (%) | |
| Male | 12 (70.6) |
| Female | 5 (29.4) |
| ECOG PS, n (%) | |
| 0 | 5 (29.4) |
| 1 | 10 (58.8) |
| 2 | 2 (11.8) |
| Smoking status, n (%) | |
| Current/former | 15 (88.2) |
| Never | 2 (11.8) |
| Asbestos exposure, n (%) | |
| Yes | 12 (70.6) |
| No | 5 (29.4) |
| Clinical stage, n (%) | |
| I | 14 (82.4) |
| II | 3 (17.6) |
| Histology, n (%) | |
| Epithelioid | 15 (88.2) |
| Sarcomatoid | 0 (0) |
| Biphasic | 2 (11.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vicidomini, G.; Della Corte, C.M.; Noro, A.; Di Liello, R.; Cappabianca, S.; Fiorelli, A.; Nardone, V.; Messina, G.; Viscardi, G.; Sangiovanni, A.; et al. A Trimodality, Four-Step Treatment including Chemotherapy, Pleurectomy/Decortication and Radiotherapy in Early-Stage Malignant Pleural Mesothelioma: A Single-Institution Retrospective Case Series Study. Cancers 2022, 14, 142. https://doi.org/10.3390/cancers14010142
Vicidomini G, Della Corte CM, Noro A, Di Liello R, Cappabianca S, Fiorelli A, Nardone V, Messina G, Viscardi G, Sangiovanni A, et al. A Trimodality, Four-Step Treatment including Chemotherapy, Pleurectomy/Decortication and Radiotherapy in Early-Stage Malignant Pleural Mesothelioma: A Single-Institution Retrospective Case Series Study. Cancers. 2022; 14(1):142. https://doi.org/10.3390/cancers14010142
Chicago/Turabian StyleVicidomini, Giovanni, Carminia Maria Della Corte, Antonio Noro, Raimondo Di Liello, Salvatore Cappabianca, Alfonso Fiorelli, Valerio Nardone, Gaetana Messina, Giuseppe Viscardi, Angelo Sangiovanni, and et al. 2022. "A Trimodality, Four-Step Treatment including Chemotherapy, Pleurectomy/Decortication and Radiotherapy in Early-Stage Malignant Pleural Mesothelioma: A Single-Institution Retrospective Case Series Study" Cancers 14, no. 1: 142. https://doi.org/10.3390/cancers14010142
APA StyleVicidomini, G., Della Corte, C. M., Noro, A., Di Liello, R., Cappabianca, S., Fiorelli, A., Nardone, V., Messina, G., Viscardi, G., Sangiovanni, A., Monti, R., Accardo, M., Morgillo, F., Ciardiello, F., Franco, R., & Santini, M. (2022). A Trimodality, Four-Step Treatment including Chemotherapy, Pleurectomy/Decortication and Radiotherapy in Early-Stage Malignant Pleural Mesothelioma: A Single-Institution Retrospective Case Series Study. Cancers, 14(1), 142. https://doi.org/10.3390/cancers14010142