
Long-Term Outcomes and Evaluation of Hepatocellular Carcinoma Recurrence after Hepatitis C Virus Eradication by Direct-Acting Antiviral Treatment: All Kagawa Liver Disease Group (AKLDG) Study

 , , ,
, , ,  , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patients’ Characteristics
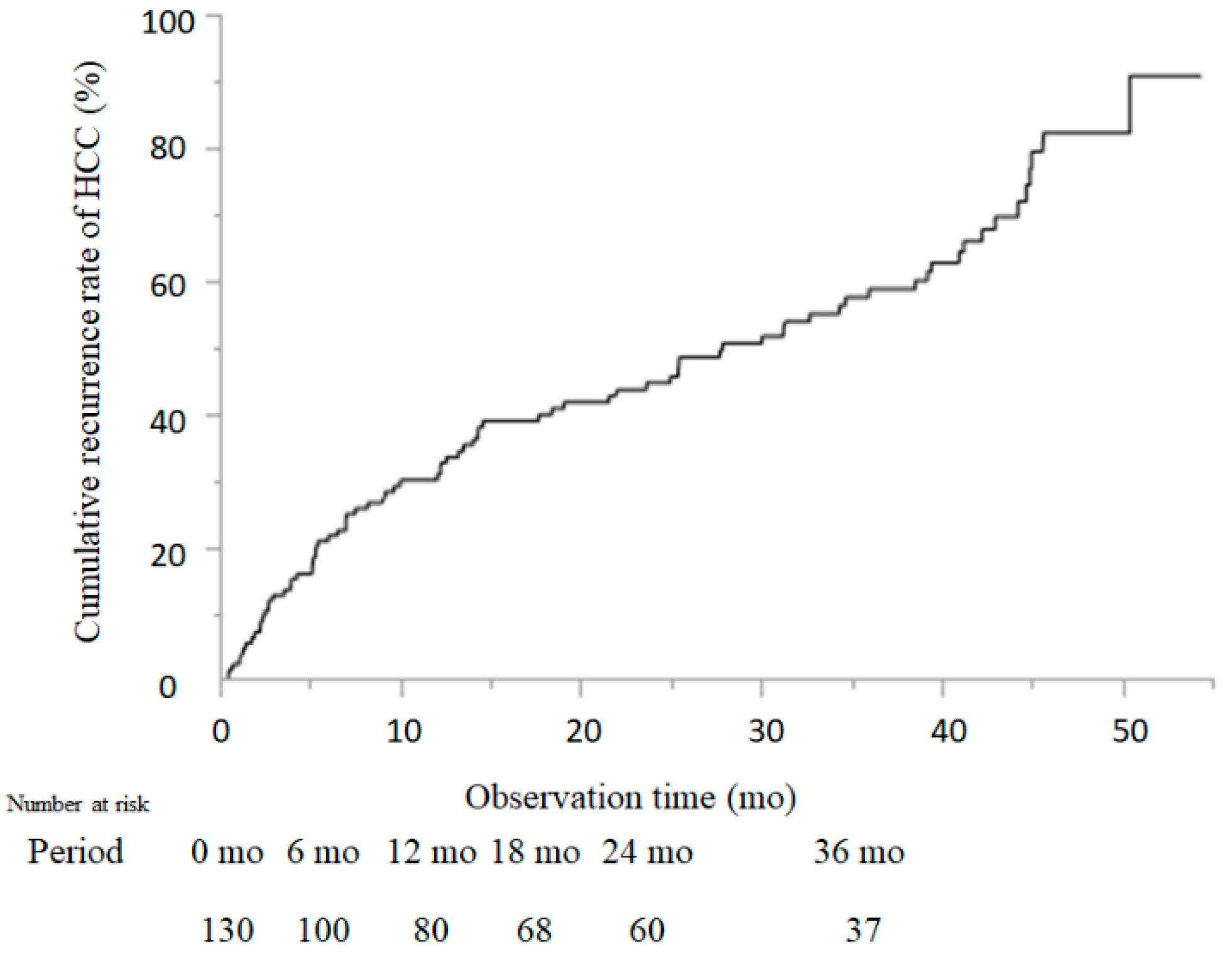
2.2. Cumulative Recurrence Rate of HCC
2.3. Comparison of Patient Characteristics between Cases with and without HCC-R
2.4. Risk Factors for HCC-R after DAA Treatment
2.5. Receiver Operating Characteristic Analysis and Diagnostic Value
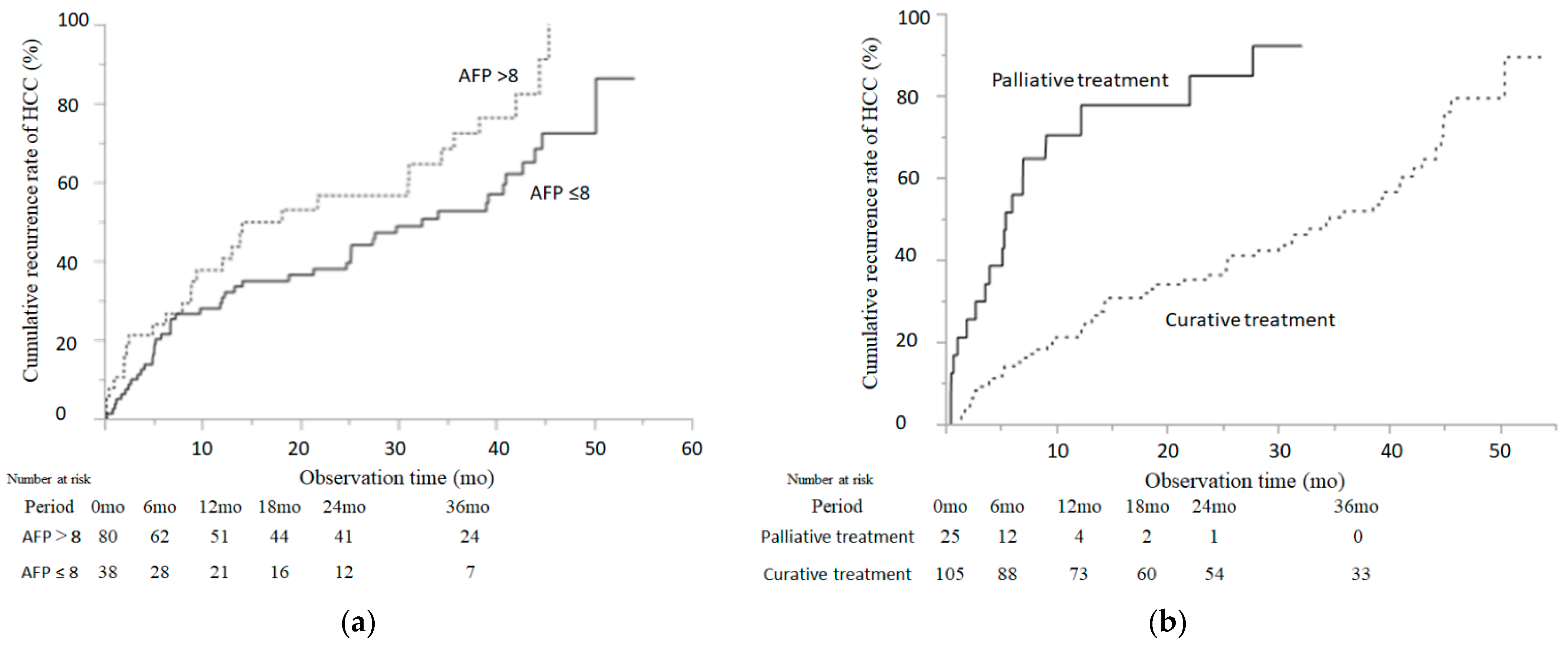
2.6. Cumulative Incidence of HCC-R According to the Serum AFP Level (AFP) at SVR12 and Palliative Treatment
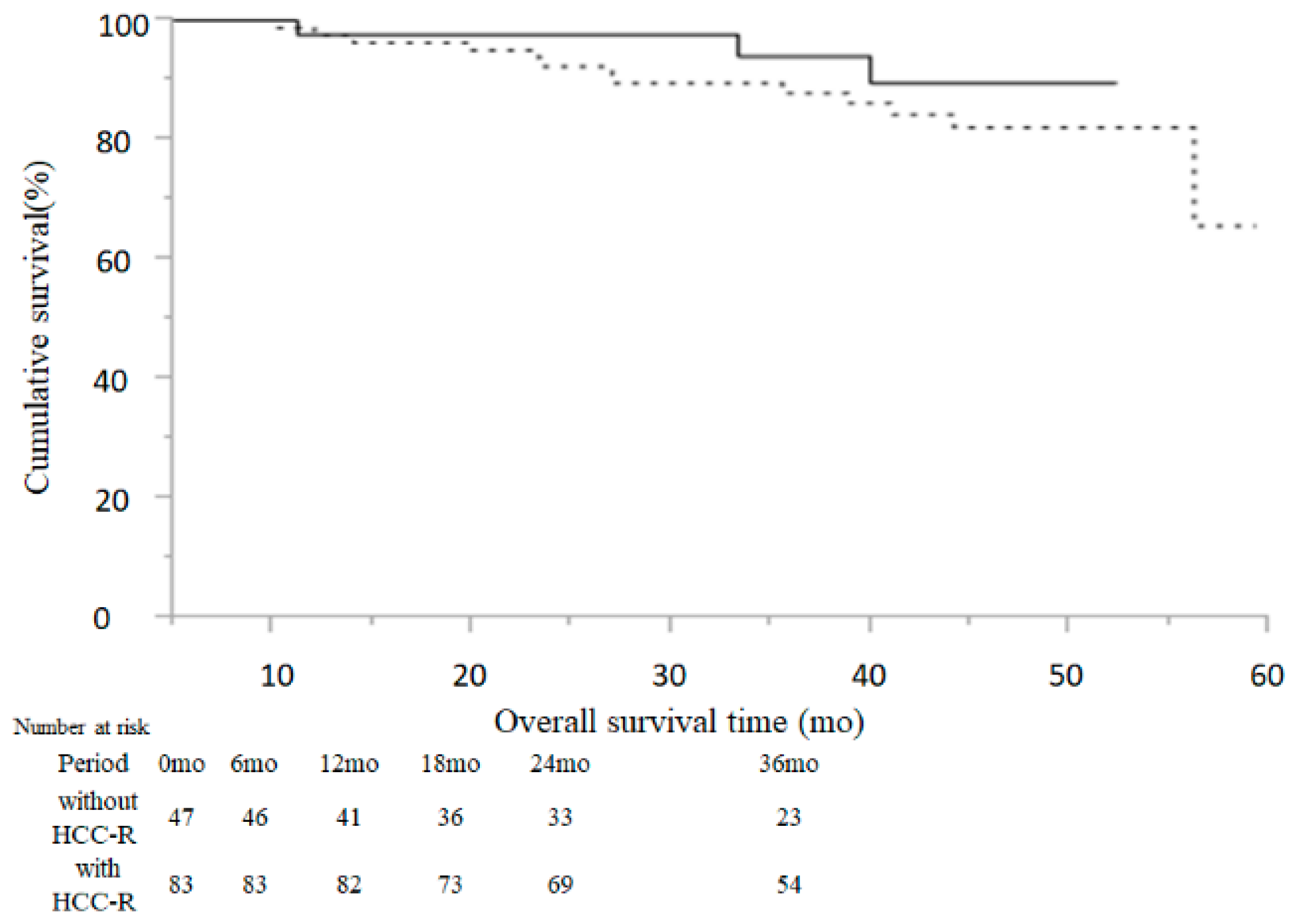
2.7. Comparison of Overall Survival Time between Cases without and with HCC-R
2.8. Relative Changes in HCC Status and Serological Data at Baseline and at HCC-R after DAA Treatment
3. Discussion
4. Materials and Methods
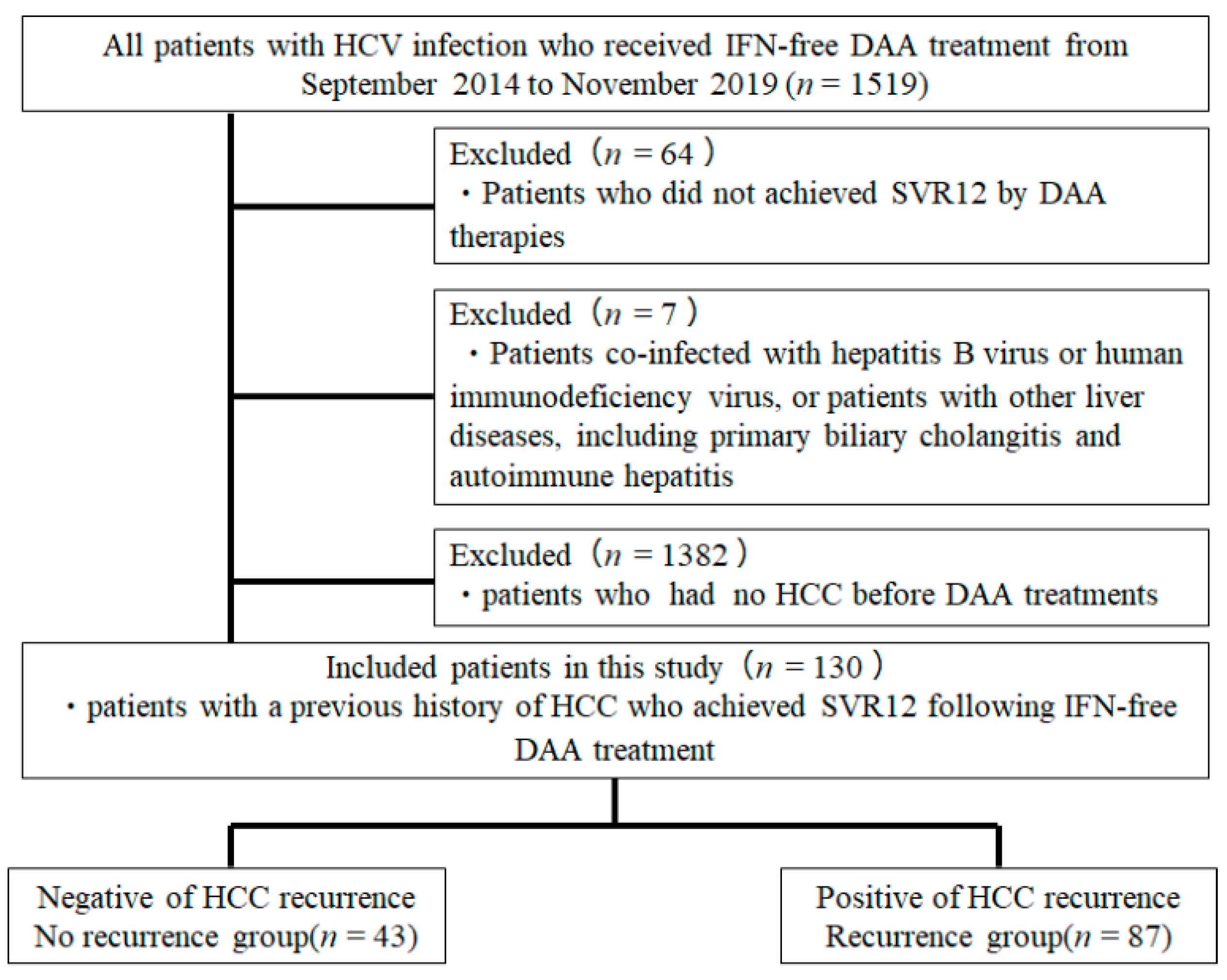
4.1. Patients
4.2. HCC Surveillance after DAA Treatment
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Villanueva, A. Hepatocellular Carcinoma. N. Engl. J. Med. 2019, 380, 1450–1462. [Google Scholar] [CrossRef]
- Lauer, G.M.; Walker, B.D. Hepatitis C virus infection. N. Engl. J. Med. 2001, 345, 41–52. [Google Scholar] [CrossRef]
- Fried, M.W.; Shiffman, M.L.; Reddy, K.R.; Smith, C.; Marinos, G.; Goncales, F.L., Jr.; Haussinger, D.; Diago, M.; Carosi, G.; Dhumeaux, D.; et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N. Engl. J. Med. 2002, 347, 975–982. [Google Scholar] [CrossRef]
- Hadziyannis, S.J.; Sette, H., Jr.; Morgan, T.R.; Balan, V.; Diago, M.; Marcellin, P.; Ramadori, G.; Bodenheimer, H., Jr.; Bernstein, D.; Rizzetto, M.; et al. Peginterferon-alpha2a and ribavirin combination therapy in chronic hepatitis C: A randomized study of treatment duration and ribavirin dose. Ann. Intern. Med. 2004, 140, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Manns, M.P.; McHutchison, J.G.; Gordon, S.C.; Rustgi, V.K.; Shiffman, M.; Reindollar, R.; Goodman, Z.D.; Koury, K.; Ling, M.; Albrecht, J.K. Peginterferon alfa-2b plus ribavirin compared with interferon alfa-2b plus ribavirin for initial treatment of chronic hepatitis C: A randomised trial. Lancet 2001, 358, 958–965. [Google Scholar] [CrossRef]
- Fried, M.W. Side effects of therapy of hepatitis C and their management. Hepatology 2002, 36, S237–S244. [Google Scholar] [CrossRef]
- Omata, M.; Nishiguchi, S.; Ueno, Y.; Mochizuki, H.; Izumi, N.; Ikeda, F.; Toyoda, H.; Yokosuka, O.; Nirei, K.; Genda, T.; et al. Sofosbuvir plus ribavirin in Japanese patients with chronic genotype 2 HCV infection: An open-label, phase 3 trial. J. Viral. Hepat. 2014, 21, 762–768. [Google Scholar] [CrossRef]
- Ogawa, E.; Furusyo, N.; Nomura, H.; Dohmen, K.; Higashi, N.; Takahashi, K.; Kawano, A.; Azuma, K.; Satoh, T.; Nakamuta, M.; et al. NS5A resistance-associated variants undermine the effectiveness of ledipasvir and sofosbuvir for cirrhotic patients infected with HCV genotype 1b. J. Gastroenterol. 2017, 52, 845–854. [Google Scholar] [CrossRef]
- Poordad, F.; Felizarta, F.; Asatryan, A.; Sulkowski, M.S.; Reindollar, R.W.; Landis, C.S.; Gordon, S.C.; Flamm, S.L.; Fried, M.W.; Bernstein, D.E.; et al. Glecaprevir and pibrentasvir for 12 weeks for hepatitis C virus genotype 1 infection and prior direct-acting antiviral treatment. Hepatology 2017, 66, 389–397. [Google Scholar] [CrossRef]
- Toyoda, H.; Kumada, T.; Tada, T.; Shimada, N.; Takaguchi, K.; Senoh, T.; Tsuji, K.; Tachi, Y.; Hiraoka, A.; Ishikawa, T.; et al. Efficacy and tolerability of an IFN-free regimen with DCV/ASV for elderly patients infected with HCV genotype 1B. J. Hepatol. 2017, 66, 521–527. [Google Scholar] [CrossRef]
- Toyoda, H.; Chayama, K.; Suzuki, F.; Sato, K.; Atarashi, T.; Watanabe, T.; Atsukawa, M.; Naganuma, A.; Notsumata, K.; Osaki, Y.; et al. Efficacy and safety of glecaprevir/pibrentasvir in Japanese patients with chronic genotype 2 hepatitis C virus infection. Hepatology 2017. [Google Scholar] [CrossRef]
- Suda, G.; Kurosaki, M.; Itakura, J.; Izumi, N.; Uchida, Y.; Mochida, S.; Hasebe, C.; Abe, M.; Haga, H.; Ueno, Y.; et al. Safety and efficacy of elbasvir and grazoprevir in Japanese hemodialysis patients with genotype 1b hepatitis C virus infection. J. Gastroenterol. 2018. [Google Scholar] [CrossRef]
- Poon, R.T. Prevention of recurrence after resection of hepatocellular carcinoma: A daunting challenge. Hepatology 2011, 54, 757–759. [Google Scholar] [CrossRef] [PubMed]
- Asahina, Y.; Tsuchiya, K.; Nishimura, T.; Muraoka, M.; Suzuki, Y.; Tamaki, N.; Yasui, Y.; Hosokawa, T.; Ueda, K.; Nakanishi, H.; et al. alpha-fetoprotein levels after interferon therapy and risk of hepatocarcinogenesis in chronic hepatitis C. Hepatology 2013, 58, 1253–1262. [Google Scholar] [CrossRef]
- Hirakawa, M.; Ikeda, K.; Arase, Y.; Kawamura, Y.; Yatsuji, H.; Hosaka, T.; Sezaki, H.; Akuta, N.; Kobayashi, M.; Saitoh, S.; et al. Hepatocarcinogenesis following HCV RNA eradication by interferon in chronic hepatitis patients. Intern. Med. 2008, 47, 1637–1643. [Google Scholar] [CrossRef][Green Version]
- Nagata, H.; Nakagawa, M.; Asahina, Y.; Sato, A.; Asano, Y.; Tsunoda, T.; Miyoshi, M.; Kaneko, S.; Otani, S.; Kawai-Kitahata, F.; et al. Effect of interferon-based and -free therapy on early occurrence and recurrence of hepatocellular carcinoma in chronic hepatitis C. J. Hepatol. 2017, 67, 933–939. [Google Scholar] [CrossRef]
- Abdelaziz, A.O.; Nabil, M.M.; Abdelmaksoud, A.H.; Shousha, H.I.; Cordie, A.A.; Hassan, E.M.; Omran, D.A.; Leithy, R.; Elbaz, T.M. De-novo versus recurrent hepatocellular carcinoma following direct-acting antiviral therapy for hepatitis C virus. Eur. J. Gastroenterol. Hepatol. 2018, 30, 39–43. [Google Scholar] [CrossRef]
- Alberti, A.; Piovesan, S. Increased incidence of liver cancer after successful DAA treatment of chronic hepatitis C: Fact or fiction? Liver Int. 2017, 37, 802–808. [Google Scholar] [CrossRef]
- Conti, F.; Buonfiglioli, F.; Scuteri, A.; Crespi, C.; Bolondi, L.; Caraceni, P.; Foschi, F.G.; Lenzi, M.; Mazzella, G.; Verucchi, G.; et al. Early occurrence and recurrence of hepatocellular carcinoma in HCV-related cirrhosis treated with direct-acting antivirals. J. Hepatol. 2016, 65, 727–733. [Google Scholar] [CrossRef]
- Reig, M.; Mariño, Z.; Perelló, C.; Iñarrairaegui, M.; Ribeiro, A.; Lens, S.; Díaz, A.; Vilana, R.; Darnell, A.; Varela, M.; et al. Unexpected high rate of early tumor recurrence in patients with HCV-related HCC undergoing interferon-free therapy. J. Hepatol. 2016, 65, 719–726. [Google Scholar] [CrossRef]
- Lack of evidence of an effect of direct-acting antivirals on the recurrence of hepatocellular carcinoma: Data from three ANRS cohorts. J. Hepatol. 2016, 65, 734–740. [CrossRef] [PubMed]
- Nagaoki, Y.; Imamura, M.; Nishida, Y.; Daijo, K.; Teraoka, Y.; Honda, F.; Nakamura, Y.; Morio, K.; Fujino, H.; Nakahara, T.; et al. The impact of interferon-free direct-acting antivirals on clinical outcome after curative treatment for hepatitis C virus-associated hepatocellular carcinoma: Comparison with interferon-based therapy. J. Med. Virol. 2019, 91, 650–658. [Google Scholar] [CrossRef]
- George, P.M.; Badiger, R.; Alazawi, W.; Foster, G.R.; Mitchell, J.A. Pharmacology and therapeutic potential of interferons. Pharmacol. Ther. 2012, 135, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Ferrantini, M.; Capone, I.; Belardelli, F. Interferon-alpha and cancer: Mechanisms of action and new perspectives of clinical use. Biochimie 2007, 89, 884–893. [Google Scholar] [CrossRef]
- Kanda, T.; Lau, G.K.K.; Wei, L.; Moriyama, M.; Yu, M.L.; Chuang, W.L.; Ibrahim, A.; Lesmana, C.R.A.; Sollano, J.; Kumar, M.; et al. APASL HCV guidelines of virus-eradicated patients by DAA on how to monitor HCC occurrence and HBV reactivation. Hepatol. Int. 2019, 13, 649–661. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, K.; Kawamura, Y.; Kobayashi, M.; Kominami, Y.; Fujiyama, S.; Sezaki, H.; Hosaka, T.; Akuta, N.; Saitoh, S.; Suzuki, F.; et al. Direct-Acting Antivirals Decreased Tumor Recurrence After Initial Treatment of Hepatitis C Virus-Related Hepatocellular Carcinoma. Dig. Dis. Sci. 2017, 62, 2932–2942. [Google Scholar] [CrossRef]
- Mashiba, T.; Joko, K.; Kurosaki, M.; Ochi, H.; Osaki, Y.; Kojima, Y.; Nakata, R.; Goto, T.; Takehiro, A.; Kimura, H.; et al. Does interferon-free direct-acting antiviral therapy for hepatitis C after curative treatment for hepatocellular carcinoma lead to unexpected recurrences of HCC? A multicenter study by the Japanese Red Cross Hospital Liver Study Group. PLoS ONE 2018, 13, e0194704. [Google Scholar] [CrossRef]
- Cabibbo, G.; Petta, S.; Calvaruso, V.; Cacciola, I.; Cannavò, M.R.; Madonia, S.; Distefano, M.; Larocca, L.; Prestileo, T.; Tinè, F.; et al. Is early recurrence of hepatocellular carcinoma in HCV cirrhotic patients affected by treatment with direct-acting antivirals? A prospective multicentre study. Aliment. Pharmacol. Ther. 2017, 46, 688–695. [Google Scholar] [CrossRef]
- Gao, X.; Zhan, M.; Wang, L.; Ding, Y.; Niu, J. Timing of DAA Initiation After Curative Treatment and Its Relationship with the Recurrence of HCV-Related HCC. J. Hepatocell. Carcinoma 2020, 7, 347–360. [Google Scholar] [CrossRef]
- Toyoda, H.; Tada, T.; Takaguchi, K.; Senoh, T.; Shimada, N.; Hiraoka, A.; Michitaka, K.; Ishikawa, T.; Kumada, T. Differences in background characteristics of patients with chronic hepatitis C who achieved sustained virologic response with interferon-free versus interferon-based therapy and the risk of developing hepatocellular carcinoma after eradication of hepatitis C virus in Japan. J. Viral. Hepat. 2017, 24, 472–476. [Google Scholar] [CrossRef]
- Watanabe, T.; Tokumoto, Y.; Joko, K.; Michitaka, K.; Horiike, N.; Tanaka, Y.; Tada, F.; Kisaka, Y.; Nakanishi, S.; Yamauchi, K.; et al. Predictors of hepatocellular carcinoma occurrence after direct-acting antiviral therapy in patients with hepatitis C virus infection. Hepatol. Res. 2019, 49, 136–146. [Google Scholar] [CrossRef]
- Tani, J.; Morishita, A.; Sakamoto, T.; Takuma, K.; Nakahara, M.; Fujita, K.; Oura, K.; Tadokoro, T.; Mimura, S.; Nomura, T.; et al. Simple scoring system for prediction of hepatocellular carcinoma occurrence after hepatitis C virus eradication by direct-acting antiviral treatment: All Kagawa Liver Disease Group Study. Oncol. Lett. 2020, 19, 2205–2212. [Google Scholar] [CrossRef] [PubMed]
- Waziry, R.; Hajarizadeh, B.; Grebely, J.; Amin, J.; Law, M.; Danta, M.; George, J.; Dore, G.J. Hepatocellular carcinoma risk following direct-acting antiviral HCV therapy: A systematic review, meta-analyses, and meta-regression. J. Hepatol. 2017, 67, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Minami, T.; Tateishi, R.; Nakagomi, R.; Fujiwara, N.; Sato, M.; Enooku, K.; Nakagawa, H.; Asaoka, Y.; Kondo, Y.; Shiina, S.; et al. The impact of direct-acting antivirals on early tumor recurrence after radiofrequency ablation in hepatitis C-related hepatocellular carcinoma. J. Hepatol. 2016, 65, 1272–1273. [Google Scholar] [CrossRef]
- Ikeda, M.; Arai, Y.; Park, S.J.; Takeuchi, Y.; Anai, H.; Kim, J.K.; Inaba, Y.; Aramaki, T.; Kwon, S.H.; Yamamoto, S.; et al. Prospective study of transcatheter arterial chemoembolization for unresectable hepatocellular carcinoma: An Asian cooperative study between Japan and Korea. J. Vasc. Interv. Radiol. 2013, 24, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Song, T.Q.; Zhang, T.; Wu, Q.; Kong, D.L.; Li, Q.; Sun, H.C. Adjuvant interferon for early or late recurrence of hepatocellular carcinoma and mortality from hepatocellular carcinoma following curative treatment: A meta-analysis with comparison of different types of hepatitis. Mol. Clin. Oncol. 2014, 2, 1125–1134. [Google Scholar] [CrossRef] [PubMed]
- Bucci, L.; Garuti, F.; Lenzi, B.; Pecorelli, A.; Farinati, F.; Giannini, E.G.; Granito, A.; Ciccarese, F.; Rapaccini, G.L.; Di Marco, M.; et al. The evolutionary scenario of hepatocellular carcinoma in Italy: An update. Liver Int. 2017, 37, 259–270. [Google Scholar] [CrossRef] [PubMed]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef]
- Atsukawa, M.; Tsubota, A.; Kondo, C.; Toyoda, H.; Nakamuta, M.; Takaguchi, K.; Watanabe, T.; Hiraoka, A.; Uojima, H.; Ishikawa, T.; et al. Real-World Clinical Application of 12-Week Sofosbuvir/Velpatasvir Treatment for Decompensated Cirrhotic Patients with Genotype 1 and 2: A Prospective, Multicenter Study. Infect. Dis. Ther. 2020, 9, 851–866. [Google Scholar] [CrossRef] [PubMed]
- Granito, A.; Bolondi, L. Non-transplant therapies for patients with hepatocellular carcinoma and Child-Pugh-Turcotte class B cirrhosis. Lancet Oncol. 2017, 18, e101–e112. [Google Scholar] [CrossRef]
- Kudo, M.; Chung, H.; Osaki, Y. Prognostic staging system for hepatocellular carcinoma (CLIP score): Its value and limitations, and a proposal for a new staging system, the Japan Integrated Staging Score (JIS score). J. Gastroenterol. 2003, 38, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.C.; Hung, C.H.; Lu, S.N.; Wang, J.H.; Lee, C.M.; Chen, C.H.; Yen, M.F.; Lin, S.C.; Yen, Y.H.; Tsai, M.C.; et al. A novel predictive score for hepatocellular carcinoma development in patients with chronic hepatitis C after sustained response to pegylated interferon and ribavirin combination therapy. J. Antimicrob. Chemother. 2012, 67, 2766–2772. [Google Scholar] [CrossRef] [PubMed]
- Cabibbo, G.; Petta, S.; Barbàra, M.; Missale, G.; Virdone, R.; Caturelli, E.; Piscaglia, F.; Morisco, F.; Colecchia, A.; Farinati, F.; et al. A meta-analysis of single HCV-untreated arm of studies evaluating outcomes after curative treatments of HCV-related hepatocellular carcinoma. Liver Int. 2017, 37, 1157–1166. [Google Scholar] [CrossRef]
- Lee, M.H.; Yang, H.I.; Lu, S.N.; Jen, C.L.; You, S.L.; Wang, L.Y.; Wang, C.H.; Chen, W.J.; Chen, C.J. Chronic hepatitis C virus infection increases mortality from hepatic and extrahepatic diseases: A community-based long-term prospective study. J. Infect. Dis. 2012, 206, 469–477. [Google Scholar] [CrossRef]
- Bruix, J.; Sherman, M. Management of hepatocellular carcinoma. Hepatology 2005, 42, 1208–1236. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Kitano, M.; Sakurai, T.; Nishida, N. General Rules for the Clinical and Pathological Study of Primary Liver Cancer, Nationwide Follow-Up Survey and Clinical Practice Guidelines: The Outstanding Achievements of the Liver Cancer Study Group of Japan. Dig. Dis. 2015, 33, 765–770. [Google Scholar] [CrossRef]
- Hung, C.H.; Lu, S.N.; Wang, J.H.; Lee, C.M.; Chen, T.M.; Tung, H.D.; Chen, C.H.; Huang, W.S.; Changchien, C.S. Correlation between ultrasonographic and pathologic diagnoses of hepatitis B and C virus-related cirrhosis. J. Gastroenterol. 2003, 38, 153–157. [Google Scholar] [CrossRef]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, M.S.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef]
- Lin, Z.H.; Xin, Y.N.; Dong, Q.J.; Wang, Q.; Jiang, X.J.; Zhan, S.H.; Sun, Y.; Xuan, S.Y. Performance of the aspartate aminotransferase-to-platelet ratio index for the staging of hepatitis C-related fibrosis: An updated meta-analysis. Hepatology 2011, 53, 726–736. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the ALBI grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sex (Male/Female) | 83 (63.8)/47 (36.2) |
| Age (years) | 75.5 (60–81) |
| CH/LC | 44 (33.8)/86 (66.2) |
| HCV genotype (1/2 or 3) | 98 (75.4)/32 (34.6) |
| Body mass index (kg/m2) | 22.9 (20.2–24.9) |
| Diabetes mellitus (no/yes) | 96 (73.8)/34 (26.2) |
| Treatment history of IFN (no/yes) | 97 (74.6)/33 (25.4) |
| DAA therapy | |
| ASV +DCV, n (%) | 22 (16.9) |
| SOF + LDV, n (%) | 53 (40.8) |
| SOF + RBV, n (%) | 28 (21.5) |
| ERB + GZR, n (%) | 8 (6.2) |
| OBV + PTV + r, n (%) | 9 (6.9) |
| GLE + PIB, n (%) | 10 (7.7) |
| Number of HCC lesions | 1 (1–2) |
| Size of main tumor lesion (mm) | 18 (15–26) |
| Total number of treatments (times) | 1 (1–2) |
| Final treatment method for HCC before DAA therapy | |
| Hepatectomy, n (%) | 23 (17.7) |
| RFA, n (%) | 82 (63.1) |
| TACE, n (%) | 22 (16.9) |
| MTA, n (%) | 3 (1.2) |
| AST (IU/L) | 51(36–65.75) |
| ALT (IU/L) | 39.5 (26–50.75) |
| Total bilirubin (mg/dL) | 0.8 (0.6–1.1) |
| Albumin (g/dL) | 3.7 (3.4–3.9) |
| Hemoglobin (g/dL) | 12.5 (11.5–13.7) |
| White blood cell count (/μL) | 3860 (3100–5010) |
| Platelet count (×104/μL) | 10.0 (7.775–13.7) |
| AFP (ng/mL) | 8.7 (4.2–18) |
| DCP (mAU/mL) | 22 (16.25–33) |
| Total cholesterol (mg/dL) | 149 (131.75–172) |
| FIB4 | 5.88 (3.96–8.58) |
| APRI | 1.62 (1.04–2.61) |
| WFA-M2BP (COI) | 4.14 (1.765–6.85) |
| ALBI Score | −2.48 (−2.73–−2.21) |
| Child–Pugh score (5/6/7) | 89 (68.5)/36 (27.7)/5 (3.8) |
| HCV-RNA (log copies/mL) | 6.0 (5.2–6.4) |
| Factor | Cases without HCC-R (n = 47) | Cases with HCC-R (n = 83) | p-Value |
|---|---|---|---|
| Sex (male/female) | 26 (55.3)/21 (44.7) | 57 (68.7)/26 (31.3) | 0.1298 |
| Age (years) | 75 (69–82) | 76 (67–81) | 0.7972 |
| CH/LC | 15 (31.9)/32 (68.1) | 17 (20.5)/66 (79.5) | 0.1460 |
| HCV genotype (1/2 or 3) | 32 (68.1)/15 (31.9) | 66 (79.5)/17 (20.5) | 0.1503 |
| Body mass index (kg/m2) | 22.3 (19.9–24.9) | 22.8 (20.2–24.9) | 0.3085 |
| Diabetes mellitus (no/yes) | 37 (78.7)/10 (21.3) | 59 (71.1)/24 (28.9) | 0.3410 |
| Treatment history of IFN (no/yes) | 36 (76.6)/11 (23.4) | 22 (26.5)/61 (73.5) | 0.6962 |
| DAA regimen (SOF-based DAA/others) | |||
| 25 (53.2)/22 (46.8) | 56 (67.5)/27 (32.5) | 0.1080 | |
| Interval period between the last treatment for HCC and the DAA initiation (months) | |||
| 10.2 (3.7–38.2) | 5.8 (2.6–16.3) | 0.0288 | |
| Number of HCC lesions | 1(1–2) | 1 (1–2) | 0.6757 |
| Size of main tumor lesion (mm) | 17 (15–21.5) | 18.5 (15–28) | 0.0977 |
| Total number of treatments (range) | 1 (1–2) | 2 (1–2.25) | 0.0058 |
| Final treatment method for HCC before DAA treatment | |||
| Curative treatment for HCC (i.e., resection + RFA)/palliative treatment (i.e., TACE + MTA) | |||
| 43 (91.5)/4 (8.5) | 62 (74.7)/21 (25.3) | 0.0208 | |
| Hepatectomy, n (%) | 11 (23.4) | 12 (14.5) | 0.3192 |
| RFA, n (%) | 32 (68.1) | 50 (60.2) | 0.5182 |
| TACE, n (%) | 3 (6.4) | 19 (22.9) | 0.0227 |
| MTA, n (%) | 1 (2.1) | 2 (2.4) | 0.9181 |
| (A) Baseline characteristics | |||
| AST (IU/L) | 51 (34–67) | 50 (37–66) | 0.2657 |
| ALT (IU/L) | 40 (27–57) | 39 (26–49) | 0.6721 |
| Total bilirubin (mg/dL) | 0.8 (0.6–1.0) | 0.9 (0.7–1.1) | 0.0956 |
| Albumin (g/dL) | 3.7 (3.5–3.9) | 3.6 (3.3–3.925) | 0.8125 |
| Platelet count (×104/μL) | 10.9 (7.8–14.6) | 9.9 (7.65–12.95) | 0.8974 |
| AFP (ng/mL) | 8 (3.5–22) | 10 (4.775–18) | 0.1750 |
| DCP (mAU/mL) | 21.34 (17.5–31.5) | 23 (16–34.5) | 0.2114 |
| Total cholesterol (mg/dL) | 149.5 (132–179.25) | 148 (128–169) | 0.6094 |
| FIB4 | 5.25 (3.37–7.95) | 6.44 (4.19–8.68) | 0.0887 |
| APRI | 1.62 (0.75–2.49) | 1.65 (1.14–2.79) | 0.1709 |
| WFA-M2BP (COI) | 3.00 (1.72–6.7) | 4.27 (1.80–7.51) | 0.5039 |
| ALBI score | −2.44 (−2.21–−2.59) | −2.26 (−1.99–−2.65) | 0.9183 |
| Child–Pugh score (5/6/7) | 31/14/2 | 58/22/3 | 0.8976 |
| HCV-RNA (log copies/mL) | 6 (5.1−6.35) | 6 (5.2−6.5) | 0.3110 |
| (B) Blood test at SVR12 | |||
| AST (IU/L) | 25.5 (22–30) | 27 (23–36) | 0.1629 |
| ALT (IU/L) | 16.5 (11–21.75) | 19 (13–23) | 0.6251 |
| Total bilirubin (mg/dL) | 0.65 (0.5–1.0) | 0.9 (0.6–1.225) | 0.0157 |
| Albumin (g/dL) | 4.0 (3.725–4.3) | 3.9 (3.675–4.2) | 0.1312 |
| Platelet count (×104/μL) | 11.85 (9.7–14.8) | 10.55 (7.975–14.7) | 0.7872 |
| AFP (ng/mL) | 5 (3–7) | 6.2 (3.925–9.625) | 0.0199 |
| DCP (mAU/mL) | 20 (17–29) | 25 (16–45) | 0.2982 |
| Total cholesterol (mg/dL) | 183 (156.5–209.5) | 169.5 (133–193.25) | 0.0151 |
| FIB4 | 4.14 (3.21–5.42) | 4.73 (3.25–6.35) | 0.0970 |
| APRI | 0.73 (0.53–0.96) | 0.90 (0.54–1.37) | 0.0724 |
| WFA-M2BP (COI) | 2.63 (1.56–5.63) | 3.27 (1.58–6.12) | 0.5169 |
| ALBI score | −2.71 (−2.50–−2.98) | −2.61 (−2.30–−2.81) | 0.0322 |
| Child–Pugh score (5/6/7) | 42/5/1 | 72/10/1 | 0.8930 |
| Factor | Category | Multivariate Analysis | ||
|---|---|---|---|---|
| Hazzard Ratio | 95%CI | p-Value | ||
| Interval period between the last treatment for HCC and DAA initiation | ||||
| For every 1 month | 0.999 | 0.992–1.001 | 0.5183 | |
| Total number of treatments | For each time | 1.028 | 0.834–1.229 | 0.7824 |
| Final treatment method for HCC before DAA treatment | ||||
| Curative treatment (i.e., resection + RFA)/ palliative treatment (i.e., TACE + MTA) | Curative versus palliative | 3.974 | 1.924–8.207 | 0.0006 |
| Blood test at SVR12 | ||||
| Total bilirubin | For every 1 mg/dL | 1.051 | 0.550–1.914 | 0.8762 |
| AFP | For every 1 ng/mL | 1.048 | 1.016–1.077 | 0.0047 |
| Total cholesterol | For every 1 mg/dL | 0.996 | 0.987–1.004 | 0.3147 |
| ALBI score | For every 1 | 1.601 | 0.602–4.024 | 0.8930 |
| Factor | At Baseline | At HCC-R after DAA Treatment | p-Value |
|---|---|---|---|
| Number of HCC lesions | 1 (1–2) | 1 (1–2) | 0.2378 |
| Size of main tumor lesion (mm) | 18.5 (15–28) | 15 (12–20) | 0.0138 |
| Barcelona-Clinic Liver Cancer staging classification(0/A/B/C) | 35/22/22/3 | 33/28/18/3 | 0.7581 |
| AST (IU/L) | 50 (37–66) | 26 (23–36) | <0.001 |
| ALT (IU/L) | 39 (26–49) | 16 (14–24) | <0.001 |
| Total bilirubin (mg/dL) | 0.9 (0.7–1.1) | 0.9 (0.6–1.0) | 0.3895 |
| Albumin (g/dL) | 3.6 (3.3–3.925) | 4.1 (3.6–4.3) | <0.001 |
| Platelet count (×104/μL) | 9.9 (7.65–12.95) | 11.4 (9.5–14.7) | 0.0032 |
| AFP (ng/mL) | 10 (4.775–18) | 9 (5–33.25) | 0.0459 |
| DCP (mAU/mL) | 23 (16–34.5) | 36.5 (19.75–139.25) | 0.1709 |
| ALBI score | −2.26 (−2.81–−1.96) | −2.70 (−2.94–−2.28) | <0.001 |
| Child–Pugh score (5/6/7) | 58/22/3 | 72/10/1 | 0.0301 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tani, J.; Senoh, T.; Moriya, A.; Ogawa, C.; Deguchi, A.; Sakamoto, T.; Takuma, K.; Nakahara, M.; Oura, K.; Tadokoro, T.; et al. Long-Term Outcomes and Evaluation of Hepatocellular Carcinoma Recurrence after Hepatitis C Virus Eradication by Direct-Acting Antiviral Treatment: All Kagawa Liver Disease Group (AKLDG) Study. Cancers 2021, 13, 2257. https://doi.org/10.3390/cancers13092257
Tani J, Senoh T, Moriya A, Ogawa C, Deguchi A, Sakamoto T, Takuma K, Nakahara M, Oura K, Tadokoro T, et al. Long-Term Outcomes and Evaluation of Hepatocellular Carcinoma Recurrence after Hepatitis C Virus Eradication by Direct-Acting Antiviral Treatment: All Kagawa Liver Disease Group (AKLDG) Study. Cancers. 2021; 13(9):2257. https://doi.org/10.3390/cancers13092257
Chicago/Turabian StyleTani, Joji, Tomonori Senoh, Akio Moriya, Chikara Ogawa, Akihiro Deguchi, Teppei Sakamoto, Kei Takuma, Mai Nakahara, Kyoko Oura, Tomoko Tadokoro, and et al. 2021. "Long-Term Outcomes and Evaluation of Hepatocellular Carcinoma Recurrence after Hepatitis C Virus Eradication by Direct-Acting Antiviral Treatment: All Kagawa Liver Disease Group (AKLDG) Study" Cancers 13, no. 9: 2257. https://doi.org/10.3390/cancers13092257
APA StyleTani, J., Senoh, T., Moriya, A., Ogawa, C., Deguchi, A., Sakamoto, T., Takuma, K., Nakahara, M., Oura, K., Tadokoro, T., Mimura, S., Fujita, K., Yoneyama, H., Kobara, H., Morishita, A., Himoto, T., Tsutsui, A., Nagano, T., Takaguchi, K., & Masaki, T. (2021). Long-Term Outcomes and Evaluation of Hepatocellular Carcinoma Recurrence after Hepatitis C Virus Eradication by Direct-Acting Antiviral Treatment: All Kagawa Liver Disease Group (AKLDG) Study. Cancers, 13(9), 2257. https://doi.org/10.3390/cancers13092257