
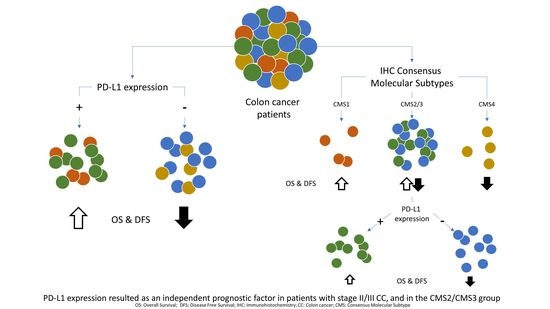
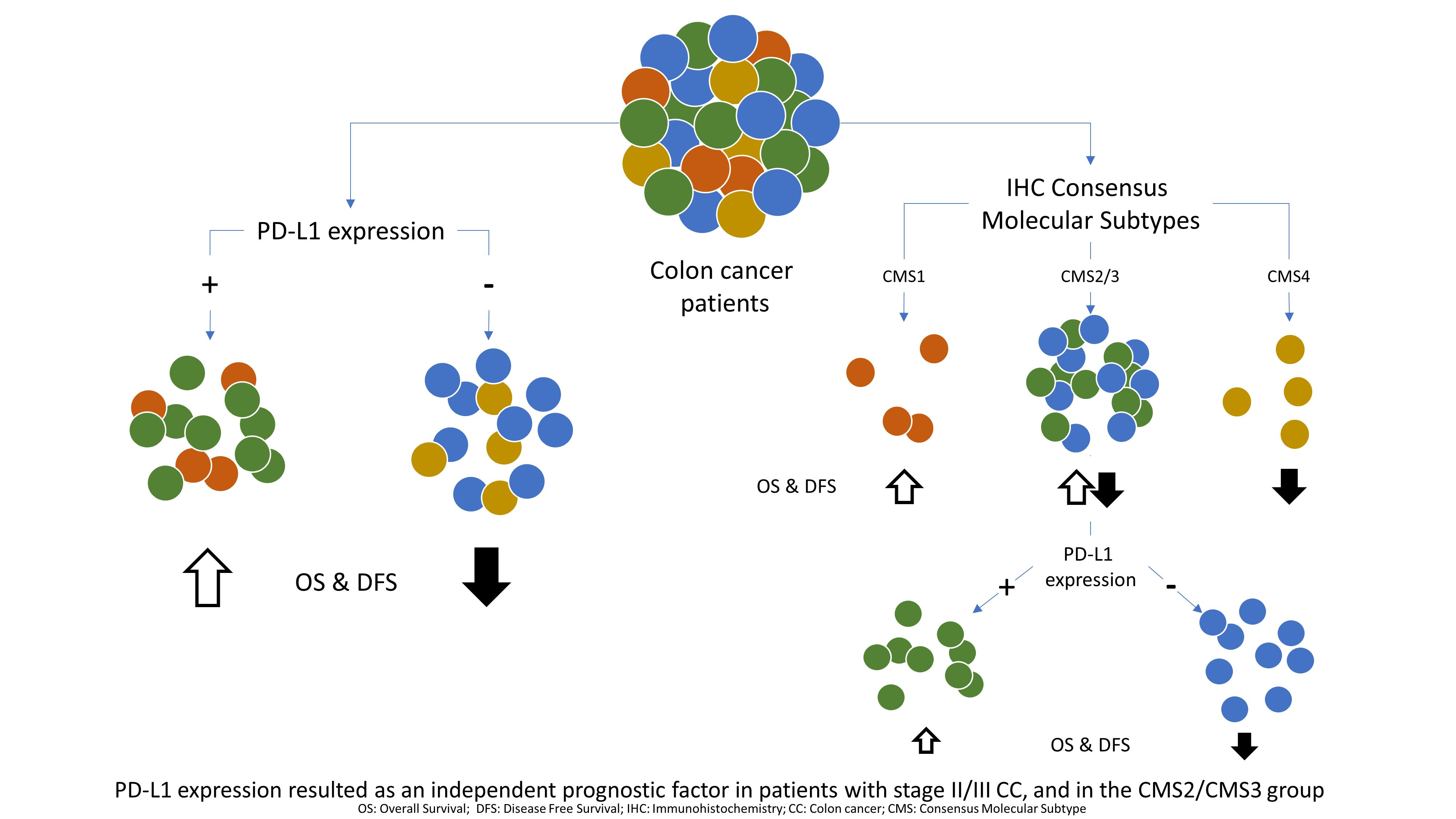
PD-L1 as a Prognostic Factor in Early-Stage Colon Carcinoma within the Immunohistochemical Molecular Subtype Classification

 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Pathological Study
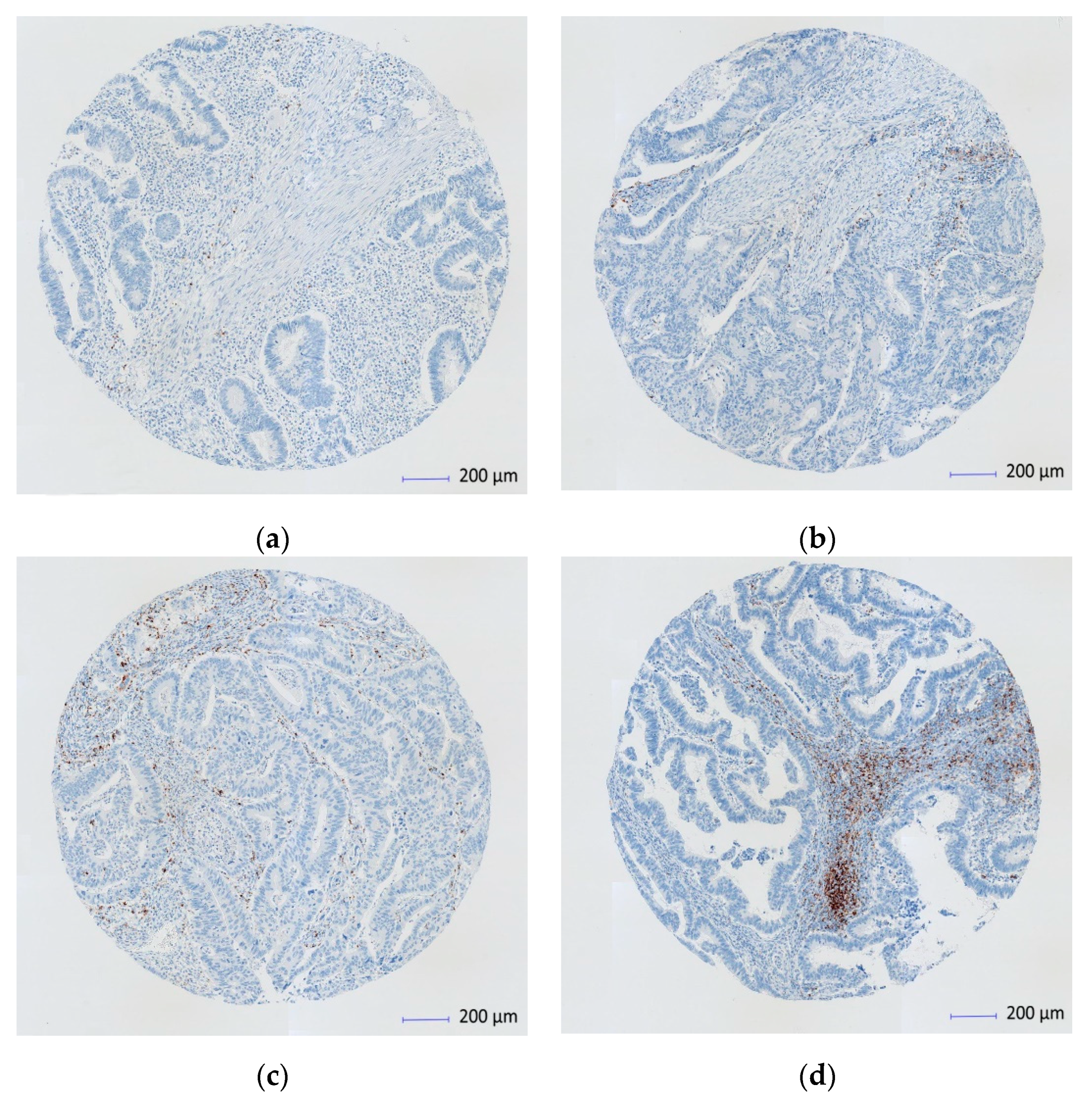
2.3. Immunohistochemical Analysis
2.4. IHC Scoring and Evaluation
2.5. Statistical Analysis
3. Results
3.1. Comparative Analysis
3.2. Univariate Analysis
3.3. Multivariate Analysis
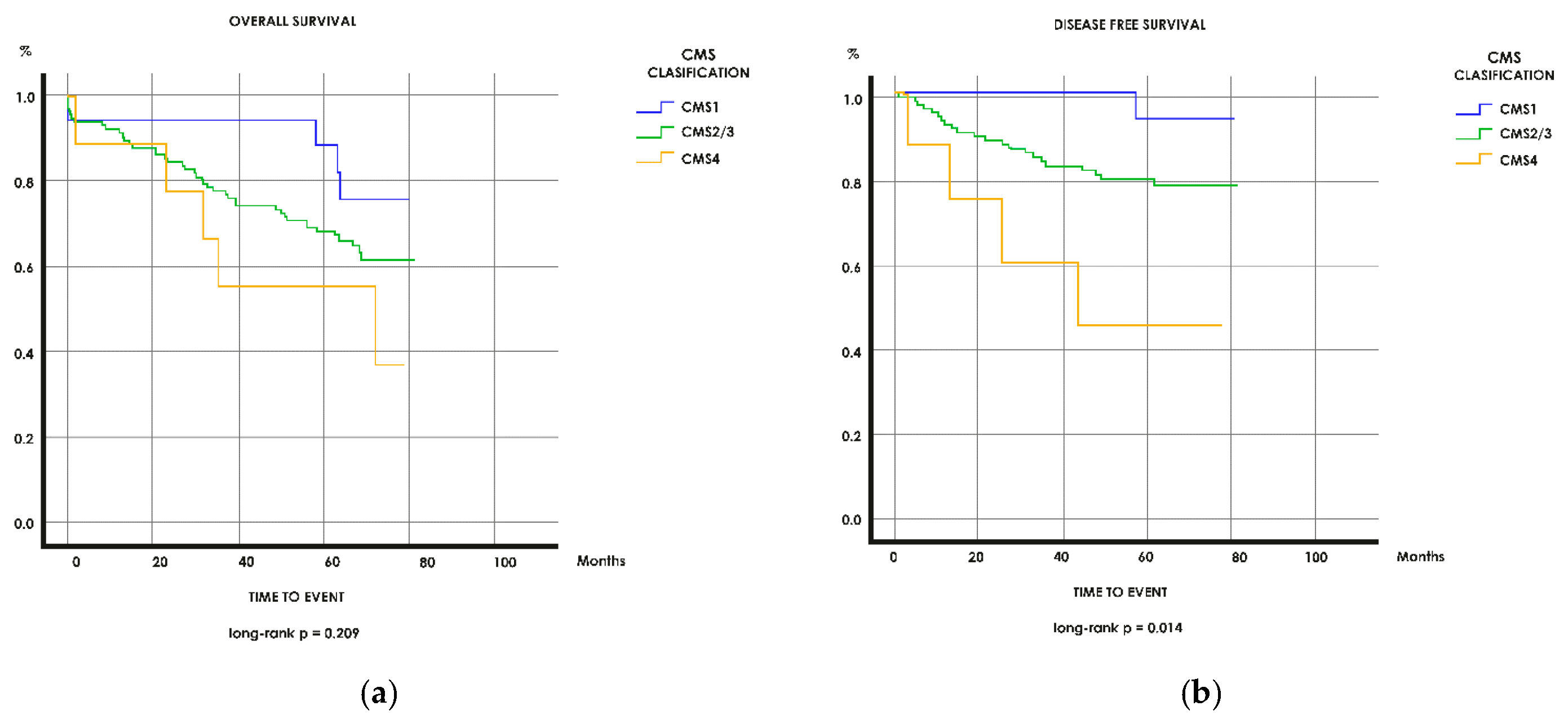
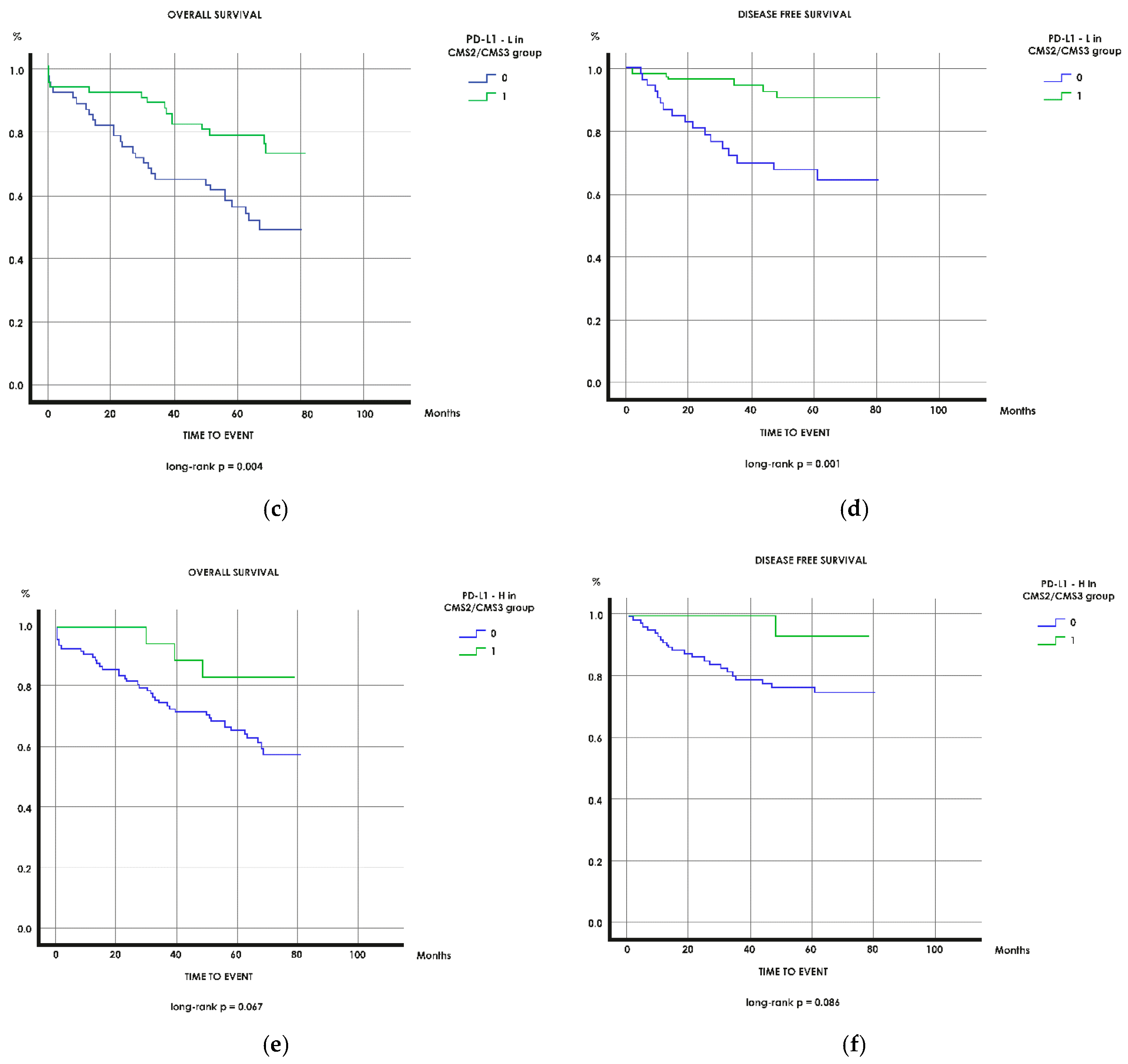
3.4. Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Puccini, A.; Berger, M.D.; Zhang, W.; Lenz, H.-J. What We Know About Stage II and III Colon Cancer: It’s Still Not Enough. Target. Oncol. 2017, 12, 265–275. [Google Scholar] [CrossRef]
- Guinney, J.; Dienstmann, R.; Wang, X.; de Reyniès, A.; Schlicker, A.; Soneson, C.; Marisa, L.; Roepman, P.; Nyamundanda, G.; Angelino, P.; et al. The consensus molecular subtypes of colorectal cancer. Nat. Med. 2015, 21, 1350–1356. [Google Scholar] [CrossRef] [PubMed]
- Trinh, A.; Trumpi, K.; De Sousa, F.; Wang, X.; de Jong, J.H.; Fessler, E.; Kuppen, P.; Reimers, M.; Swets, M.; Koopman, M.; et al. Practical and Robust Identification of Molecular Subtypes in Colorectal Cancer by Immunohistochemistry. Clin Cancer Res. 2017, 23, 387–398. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.; Eiholm, S.; Kirkeby, L.; Espersen, M.; Jess, P.; Gögenür, I.; Troelsen, J.; Espersen, M.L.M. CDX2 downregulation is associated with poor differentiation and MMR deficiency in colon cancer. Exp. Mol. Pathol. 2016, 100, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Pilati, C.; Taieb, J.; Balogoun, R.; Marisa, L.; De Reyniès, A.; Laurent-Puig, P. CDX2 prognostic value in stage II/III resected colon cancer is related to CMS classification. Ann. Oncol. 2017, 28, 1032–1035. [Google Scholar] [CrossRef] [PubMed]
- Soll, C.; Riener, M.-O.; Oberkofler, C.E.; Hellerbrand, C.; Wild, P.J.; DeOliveira, M.L.; Clavien, P.A. Expression of Serotonin Receptors in Human Hepatocellular Cancer. Clin. Cancer Res. 2012, 1, 5902–5910. [Google Scholar] [CrossRef] [PubMed]
- Henriksen, R.; Dizeyi, N.; Abrahamsson, P.-A. Expression of Serotonin Receptors 5-HT1A.; 5-HT1B.; 5-HT2B and 5-HT4 in Ovary and in Ovarian Tumours. Anticancer Res. 2012, 32, 1361–1366. [Google Scholar]
- Xu, Y.; Wang, K.; Yu, Q. FRMD6 inhibits human glioblastoma growth and progression by negatively regulating activity of receptor tyrosine kinases. Oncotarget 2016, 25, 70080–70091. [Google Scholar] [CrossRef][Green Version]
- Angus, L.; Moleirinho, S.; Herron, L.; Sinha, A.; Zhang, X.; Niestrata, M.; Dholakia, K.; Prystowsky, M.B.; Harvey, K.F.; Reynolds, P.; et al. Willin/FRMD6 expression activates the Hippo signaling pathway kinases in mammals and antagonizes oncogenic YAP. Oncogene 2011, 31, 238–250. [Google Scholar] [CrossRef]
- Zhang, P.; Wei, Y.; Wang, L.; Debeb, B.G.; Yuan, Y.; Zhang, J.; Yuan, J.; Wang, M.; Chen, D.; Sun, Y.; et al. ATM-mediated stabilization of ZEB1 promotes DNA damage response and radioresistance through CHK1. Nat. Cell Biol. 2014, 16, 864–875. [Google Scholar] [CrossRef]
- Zhang, P.; Sun, Y.; Ma, L. ZEB1: At the crossroads of epithelial-mesenchymal transition, metastasis and therapy resistance. Cell Cycle 2015, 14, 481–487. [Google Scholar] [CrossRef]
- Zhang, B.Y.; Jones, J.C.; Briggler, A.M.; Hubbard, J.M.; Kipp, B.R.; Sargent, D.J.; Dixon, J.; Grothey, A. Lack of Caudal-Type Homeobox Transcription Factor 2 Expression as a Prognostic Biomarker in Metastatic Colorectal Cancer. Clin. Colorectal Cancer 2017, 16, 124–128. [Google Scholar] [CrossRef]
- Gatalica, Z.; Vranic, S.; Xiu, J.; Swensen, J.; Reddy, S. High microsatellite instability (MSI-H) colorectal carcinoma: A brief review of predictive biomarkers in the era of personalized medicine. Fam. Cancer 2016, 15, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Vilar, E.; Gruber, S.B. Microsatellite instability in colorectal cancer—The stable evidence. Nat. Rev. Clin. Oncol. 2010, 7, 153–162. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology. Colon Cancer Version 4.2019 [Internet]. National Comprehensive Cancer Network. 2019. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed on 14 July 2020).
- Argilés, G.; Tabernero, J.; Labianca, R.; Hochhauser, D.; Salazar, R.; Iveson, T.; Laurent-Puig, P.; Quirke, P.; Yoshino, T.; Taieb, J.; et al. Localised colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1291–1305. [Google Scholar] [CrossRef]
- Andre, T.; Shiu, K.-K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.J.A.; Smith, M.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab versus chemotherapy for microsatellite instability-high/mismatch repair deficient metastatic colorectal cancer: The phase 3 KEYNOTE-177 Study. J. Clin. Oncol. 2020, 20 (Suppl. 18), LBA4. [Google Scholar] [CrossRef]
- Dienstmann, R.; Vermeulen, L.; Guinney, J.; Kopetz, S.; Tejpar, S.; Tabernero, J. Consensus molecular subtypes and the evolution of precision medicine in colorectal cancer. Nat. Rev. Cancer 2017, 17, 79–92. [Google Scholar] [CrossRef]
- De Sousa, E.; Melo, F.; Wang, X.; Jansen, M.; Fessler, E.; Trinh, A.; de Rooij, L.P.M.H.; Jong, H.; de Boer, O.; van Leersum, R.; et al. Poor-prognosis colon cancer is defined by a molecularly distinct subtype and develops from serrated precursor lesions. Nat. Med. 2013, 19, 614–618. [Google Scholar] [CrossRef]
- Roepman, P.; Schlicker, A.; Tabernero, J.; Majewski, I.; Tian, S.; Moreno, V.; Snel, M.H.; Chresta, C.M.; Rosenberg, R.; Nitsche, U.; et al. Colorectal cancer intrinsic subtypes predict chemotherapy benefit, deficient mismatch repair and epithelial-to-mesenchymal transition. Int. J. Cancer 2014, 134, 552–562. [Google Scholar] [CrossRef]
- Song, N.; Pogue-Geile, K.L.; Gavin, P.G.; Yothers, G.; Kim, S.R.; Johnson, N.L.; Lipchik, C.; Allegra, C.; Petrelli, J.; O’Connell, M.; et al. Clinical Outcome From Oxaliplatin Treatment in Stage II/III Colon Cancer According to Intrinsic Subtypes: Secondary Analysis of NSABP C-07/NRG Oncology Randomized Clinical Trial. JAMA Oncol 2016, 1, 1162. [Google Scholar] [CrossRef]
- Fontana, E.; Eason, K.; Cervantes, A.; Salazar, R.; Sadanandam, A. Context matters—consensus molecular subtypes of colorectal cancer as biomarkers for clinical trials. Ann. Oncol. 2019, 30, 520–527. [Google Scholar] [CrossRef]
- Sharpe, A.H.; Pauken, K.E. The diverse functions of the PD1 inhibitory pathway. Nat. Rev. Immunol. 2018, 18, 153–167. [Google Scholar] [CrossRef]
- Oliveira, A.F.; Bretes, L.; Furtado, I. Review of PD-1/PD-L1 Inhibitors in Metastatic dMMR/MSI-H Colorectal Cancer. Front. Oncol. 2019, 14, 396. [Google Scholar] [CrossRef]
- Rosenbaum, M.W.; Bledsoe, J.R.; Morales-Oyarvide, V.; Huynh, T.G.; Mino-Kenudson, M. PD-L1 expression in colorectal cancer is associated with microsatellite instability, BRAF mutation, medullary morphology and cytotoxic tumor-infiltrating lymphocytes. Mod. Pathol. 2016, 29, 1104–1112. [Google Scholar] [CrossRef]
- Ruan, Z.; Liang, M.; Lai, M.; Shang, L.; Deng, X.; Su, X. KYA1797K down-regulates PD-L1 in colon cancer stem cells to block immune evasion by suppressing the β-catenin/STT3 signaling pathway. Int. Immunopharmacol. 2020, 78, 106003. [Google Scholar] [CrossRef]
- Shen, Z.; Gu, L.; Mao, D.; Chen, M.; Jin, R. Clinicopathological and prognostic significance of PD-L1 expression in colorectal cancer: A systematic review and meta-analysis. World J. Surg. Oncol. 2019, 17, 1–9. [Google Scholar] [CrossRef]
- Wyss, J.; Dislich, B.; Koelzer, V.H.; Galván, J.A.; Dawson, H.; Hädrich, M.; Inderbitzin, D.; Lugli, A.; Zlobec, I.; Berger, M.D. Stromal PD-1/PD-L1 Expression Predicts Outcome in Colon Cancer Patients. Clin. Color. Cancer 2019, 18, e20–e38. [Google Scholar] [CrossRef]
- Droeser, R.A.; Hirt, C.; Viehl, C.T.; Frey, D.M.; Nebiker, C.; Huber, X.; Zlobecc, I.; Eppenberger-Castorid, S.; Tzankovd, A.; Rosso, R.; et al. Clinical impact of programmed cell death ligand 1 expression in colorectal cancer. Eur. J. Cancer 2013, 49, 2233–2242. [Google Scholar] [CrossRef]
- Song, M.; Chen, D.; Lu, B.; Wang, C.; Zhang, J.; Huang, L.; Wang, X.; Timmons, C.L.; Hu, J.; Liu, B.; et al. PTEN Loss Increases PD-L1 Protein Expression and Affects the Correlation between PD-L1 Expression and Clinical Parameters in Colorectal Cancer. PLoS ONE 2013, 8, e65821. [Google Scholar] [CrossRef]
- Mettu, N.B.; Twohy, E.; Ou, F.-S.; Halfdanarson, T.R.; Lenz, H.J.; Breakstone, R.; Boland, P.M.; Crysler, O.; Wu, C.; Grothey, A.; et al. BACCI: A phase II randomized, double-blind, multicenter, placebo-controlled study of capecitabine (C) bevacizumab (B) plus atezolizumab (A) or placebo (P) in refractory metastatic colorectal cancer (mCRC): An ACCRU network study. Ann. Oncol. 2019, 30, 203. [Google Scholar] [CrossRef]
- Li, Y.; He, M.; Zhou, Y.; Yang, C.; Wei, S.; Bian, X.; Christopher, O.; Xie, L. The Prognostic and Clinicopathological Roles of PD-L1 Expression in Colorectal Cancer: A Systematic Review and Meta-Analysis. Front. Pharm. 2019, 10, 139. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.U.; Jeong, W.K.; Baek, S.K.; Kim, N.K.; Hwang, I. Prognostic impact of programmed cell death ligand 1 expression on long-term oncologic outcomes in colorectal cancer. Oncol. Lett. 2018, 16, 5214–5222. [Google Scholar] [CrossRef]
- Lee, M.S.; Menter, D.G.; Kopetz, S. Right Versus Left Colon Cancer Biology: Integrating the Consensus Molecular Subtypes. J. Natl. Compr. Canc. Netw. 2017, 15, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; Wiley-Blackwell: Hoboken, NJ, USA, 2011; p. 336. [Google Scholar]
- Hoorn, S.; Trinh, A.; de Jong, J.; Koens, L.; Vermeulen, L. Classification of Colorectal Cancer in Molecular Subtypes by Immunohistochemistry. In Colorectal Cancer; Beaulieu, J.-F., Ed.; Humana Press: New York, NY, USA, 2018; pp. 179–191. [Google Scholar]
- Liu, S.; Gönen, M.; Stadler, Z.K.; Weiser, M.R.; Hechtman, J.F.; Vakiani, E.; Wang, T.; Vyas, M.; Joneja, U.; Al-Bayati, M.; et al. Cellular localization of PD-L1 expression in mismatch-repair-deficient and proficient colorectal carcinomas. Mod. Pathol. 2019, 32, 110–121. [Google Scholar] [CrossRef]
- Berger, M.D.; Yang, D.; Sunakawa, Y.; Zhang, W.; Ning, Y.; Matsusaka, S.; Okazaki, S.; Miyamoto, Y.; Suenaga, M.; Schirripa, M.; et al. Impact of sex, age, and ethnicity/race on the survival of patients with rectal cancer in the United States from 1988 to 2012. Oncotarget 2016, 7, 53668–53678. [Google Scholar] [CrossRef] [PubMed]
- Salem, M.E.; Yin, J.; Weinberg, B.A.; Renfro, L.A.; Pederson, L.D.; Maughan, T.S.; Adams, R.A.; Van Custem, E.; Falcone, A.; Tebbutt, N.C.; et al. Clinicopathological differences and survival outcomes with first-line therapy in patients with left-sided colon cancer and rectal cancer: Pooled analysis of 2879 patients from AGITG (MAX), COIN.; FOCUS2, OPUS.; CRYSTAL and COIN-B trials in the ARCAD database. Eur. J. Cancer 2018, 103, 205–213. [Google Scholar]
- Tamas, K.; Walenkamp, A.M.E.; de Vries, E.G.E.; van Vugt, M.A.T.M.; Beets-Tan, R.G.; van Etten, B.; de Groota, J.A.; Hospersa, G.A.P. Rectal and colon cancer: Not just a different anatomic site. Cancer Treat. Rev. 2015, 41, 671–679. [Google Scholar] [CrossRef]
- Tominaga, T.; Akiyoshi, T.; Yamamoto, N.; Taguchi, S.; Mori, S.; Nagasaki, T.; Fukunaga, Y.; Ueno, M. Clinical significance of soluble programmed cell death-1 and soluble programmed cell death-ligand 1 in patients with locally advanced rectal cancer treated with neoadjuvant chemoradiotherapy. PLoS ONE 2019, 26, e0212978. [Google Scholar] [CrossRef]
- Shao, L.; Peng, Q.; Du, K.; He, J.; Dong, Y.; Lin, X.; Li, J.; Wu, J. Tumor cell PD-L1 predicts poor local control for rectal cancer patients following neoadjuvant radiotherapy. Cancer Manag. Res. 2017, 9, 249–258. [Google Scholar] [CrossRef]
- Llosa, N.J.; Cruise, M.; Tam, A.; Wicks, E.C.; Hechenbleikner, E.M.; Taube, J.M.; Blosser, R.L.; Fan, H.; Wang, H.; Luber, B.S.; et al. The Vigorous Immune Microenvironment of Microsatellite Instable Colon Cancer Is Balanced by Multiple Counter-Inhibitory Checkpoints. Cancer Discov. 2015, 5, 43–51. [Google Scholar] [CrossRef]
- Marginean, E.C.; Melosky, B. Is There a Role for Programmed Death Ligand-1 Testing and Immunotherapy in Colorectal Cancer With Microsatellite Instability? Part II—The Challenge of Programmed Death Ligand-1 Testing and Its Role in Microsatellite Instability-High Colorectal Cancer. Arch. Pathol. Lab. Med. 2018, 1, 26–34. [Google Scholar] [CrossRef]
- Elfishawy, M.; Abd-ELaziz, S.A.; Hegazy, A.; El-Yasergy, D.F. Immunohistochemical Expression of Programmed Death Ligand-1 (PDL-1) in Colorectal carcinoma and Its Correlation with Stromal Tumor Infiltrating Lymphocytes. Asian Pac. J. Cancer Prev. 2020, 21, 225–232. [Google Scholar] [CrossRef] [PubMed]
- El Jabbour, T.; Ross, J.S.; Sheehan, C.; Affolter, K.; Geiersbach, K.B.; Boguniewicz, A.; Ainechi, S.; Bronner, M.P.; Jones, D.M.; Lee, H. PD-L1 protein expression in tumour cells and immune cells in mismatch repair protein-deficient and -proficient colorectal cancer: The foundation study using the SP142 antibody and whole section immunohistochemistry. J. Clin. Pathol. 2018, 71, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Park, H.E.; Cho, N.-Y.; Lee, H.S.; Kang, G.H. Characterisation of PD-L1-positive subsets of microsatellite-unstable colorectal cancers. Br. J. Cancer 2016, 115, 490–496. [Google Scholar] [CrossRef]
- Masugi, Y.; Nishihara, R.; Mingyang, S.; Mima, K.; Da Silva, A.; Shi, Y.; Inamura, K.; Cao, Y.; Song, M.; Nowak, J.A.; et al. Tumour CD274 (PD-L1) expression and T cells in colorectal cancer. Gut 2017, 66, 1463–1473. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, D.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef]
- Tang, Y.; Zhang, P.; Wang, Y.; Wang, J.; Su, M.; Wang, Y.; Zhou, L.; Xiong, W.; Zeng, Z.; Zhou, Y.; et al. The Biogenesis, Biology, and Clinical Significance of Exosomal PD-L1 in Cancer. Front. Immunol. 2020, 11, 604. [Google Scholar] [CrossRef]
- Fehrenbacher, L.; Spira, A.; Ballinger, M.; Kowanetz, M.; Vansteenkiste, J.; Mazieres, J.; Park, K.; Smith, D.; Artal-Cortes, A.; Lewanski, C.; et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): A multicentre, open-label, phase 2 randomised controlled trial. Lancet 2016, 387, 1837–1846. [Google Scholar] [CrossRef]
- Rittmeyer, A.; Barlesi, F.; Waterkamp, D.; Park, K.; Ciardiello, F.; von Pawel, J.; Gadgeel, S.M.; Hida, T.; Kowalski, D.M.; Dols, M.C.; et al. Atezolizumab versus docetaxel in patients with previously treated non-small-cell lung cancer (OAK): A phase 3, open-label, multicentre randomised controlled trial. Lancet 2017, 389, 255–265. [Google Scholar] [CrossRef]
- Schmid, P.; Adams, S.; Rugo, H.S.; Schneeweiss, A.; Barrios, C.H.; Iwata, H.; Diéras, V.; Hegg, R.; Im, S.A.; Shaw Wright, G.; et al. Atezolizumab and Nab-Paclitaxel in Advanced Triple-Negative Breast Cancer. N. Engl. J. Med. 2018, 379, 2108–2121. [Google Scholar] [CrossRef] [PubMed]
- Eckstein, M.; Erben, P.; Kriegmair, M.C.; Worst, T.S.; Weiß, C.-A.; Wirtz, R.M.; Wach, S.; Stoehr, R.; Sikic, D.; Geppert, C.I.; et al. Performance of the Food and Drug Administration/EMA-approved programmed cell death ligand-1 assays in urothelial carcinoma with emphasis on therapy stratification for first-line use of atezolizumab and pembrolizumab. Eur. J. Cancer 2019, 106, 234–243. [Google Scholar] [CrossRef]
- Shi, Q.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Sougklakos, I.; Kerr, R.; Labianca, R.; Meyerhardt, J.A.; et al. Prospective pooled analysis of six phase III trials investigating duration of adjuvant (adjuv) oxaliplatin-based therapy (3 vs. 6 months) for patients (pts) with stage III colon cancer (CC): The IDEA (International Duration Evaluation of Adjuvant chemotherapy) collaboration. J. Clin. Oncol. 2017, 35 (Suppl. 18), LBA1. [Google Scholar]
- Zhu, J.; Chen, L.; Zou, L.; Yang, P.; Wu, R.; Mao, Y.; Zhou, H.; Li, R.; Wang, K.; Wang, W.; et al. MiR-20b, -21, and -130b inhibit PTEN expression resulting in B7-H1 over-expression in advanced colorectal cancer. Hum. Immunol. 2014, 75, 348–353. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.H.; Cavalcanti, M.S.; Segal, N.H.; Hechtman, J.F.; Weiser, M.R.; Smith, J.J.; Garcia-Aguilar, J.; Sadot, E.; Ntiamoah, P.; Markowitz, A.J.; et al. Patterns and prognostic relevance of PD-1 and PD-L1 expression in colorectal carcinoma. Mod. Pathol. 2016, 29, 1433–1442. [Google Scholar] [CrossRef]
- Shan, T.; Chen, S.; Wu, T.; Yang, Y.; Li, S.; Chen, X. PD-L1 expression in colon cancer and its relationship with clinical prognosis. Int. J. Clinc. Exp. Pathol. 2019, 12, 1764–1769. [Google Scholar]
- Ni, X.; Sun, X.; Wang, D.; Chen, Y.; Zhang, Y.; Li, W.; Wang, L.; Suo, J. The clinicopathological and prognostic value of programmed death-ligand 1 in colorectal cancer: A meta-analysis. Clin. Transl. Oncol. 2019, 21, 674–686. [Google Scholar] [CrossRef]
- Zhou, K.I.; Peterson, B.; Serritella, A.; Thomas, J.; Reizine, N.; Moya, S.; Tan, C.; Wang, Y.; Catenacci, D.V.T. Spatial and Temporal Heterogeneity of PD-L1 Expression and Tumor Mutational Burden in Gastroesophageal Adenocarcinoma at Baseline Diagnosis and after Chemotherapy. Clin. Cancer Res. 2020, 26, 6453–6463. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, K.; Iwatsuki, M.; Ajani, J.A.; Baba, H. Programmed death ligand-1 expression in gastrointestinal cancer: Clinical significance and future challenges. Ann. Gastroenterol. Surg. 2020, 4, 369–378. [Google Scholar] [CrossRef]
- Shklovskaya, E.; Rizos, H. Spatial and Temporal Changes in PD-L1 Expression in Cancer: The Role of Genetic Drivers, Tumor Microenvironment and Resistance to Therapy. Int. J. Mol. Sci. 2020, 21, 7139. [Google Scholar] [CrossRef]
- Chen, B.J.; Dashnamoorthy, R.; Galera, P.; Makarenko, V.; Chang, H.; Ghosh, S.; Evens, A.M. The immune checkpoint molecules PD-1, PD-L1, TIM-3 and LAG-3 in diffuse large B-cell lymphoma. Oncotarget 2019, 10, 2030–2040. [Google Scholar] [CrossRef]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef] [PubMed]
- Jung, D.H.; Park, H.J.; Jang, H.H.; Kim, S.-H.; Jung, Y.; Lee, W.-S. Clinical Impact of PD-L1 Expression for Survival in Curatively Resected Colon Cancer. Cancer Investig. 2020, 38, 406–414. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-Y.; Chiang, S.-F.; Ke, T.-W.; Chen, T.-W.; You, Y.-S.; Chen, W.T.-L.; Chao, K.S.C. Clinical significance of programmed death 1 ligand-1 (CD274/PD-L1) and intra-tumoral CD8+ T-cell infiltration in stage II–III colorectal cancer. Sci. Rep. 2018, 8, 15658. [Google Scholar] [CrossRef]
- Chakrabarti, S.; Peterson, C.Y.; Sriram, D.; Mahipal, A. Early stage colon cancer: Current treatment standards, evolving paradigms, and future directions. World J. Gastrointest. Oncol. 2020, 12, 808–832. [Google Scholar] [CrossRef] [PubMed]
- Zhao, T.; Li, C.; Wu, Y.; Li, B.; Zhang, B. Prognostic value of PD-L1 expression in tumor infiltrating immune cells in cancers: A meta-analysis. PLoS ONE 2017, 12, e0176822. [Google Scholar] [CrossRef]
- Yang, L.; Xue, R.; Pan, C. Prognostic and clinicopathological value of PD-L1 in colorectal cancer: A systematic review and meta-analysis. Oncotargets 2019, 12, 3671–3682. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Liu, Z.; Fisher, K.W.; Ren, F.; Lv, J.; Davidson, D.D.; Baldridge, L.A.; Du, X.; Cheng, L. Prognostic value of programmed death ligand 1, p53, and Ki-67 in patients with advanced-stage colorectal cancer. Hum. Pathol. 2018, 71, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Yaghoubi, N.; Soltani, A.; Ghazvini, K.; Hassanian, S.M.; Hashemy, S.I. PD-1/ PD-L1 blockade as a novel treatment for colorectal cancer. Biomed. Pharm. 2019, 110, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Overman, M.J.; McDermott, R.; Leach, J.L.; Lonardi, S.; Lenz, H.-J.; Morse, M.; Desai, J.; Hill, A.; Axelson, M.; Moss, R.; et al. Nivolumab in patients with metastatic DNA mismatch repair-deficient or microsatellite instability-high colorectal cancer (CheckMate 142): An open-label, multicentre, phase 2 study. Lancet Oncol. 2017, 18, 1182–1191. [Google Scholar] [CrossRef]
- Kluger, H.M.; Zito, C.R.; Turcu, G.; Baine, M.K.; Zhang, H.; Adeniran, A.; Szonl, M.; Rimm, D.L.; Kluger, Y.; Chen, L.; et al. PD-L1 Studies Across Tumor Types, Its Differential Expression and Predictive Value in Patients Treated with Immune Checkpoint Inhibitors. Clin. Cancer Res. 2017, 23, 4270–4279. [Google Scholar] [CrossRef]
- Müller, M.F.; Ibrahim, A.E.K.; Arends, M.J. Molecular pathological classification of colorectal cancer. Virchows Arch. 2016, 469, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Iveson, T.; Sobrero, A.F.; Yoshino, T.; Sougklakos, I.; Ou, F.-S.; Meyers, J.P.; Shi, Q.; Saunders, M.P.; Labianca, R.; Yamanaka, T.; et al. Prospective pooled analysis of four randomized trials investigating duration of adjuvant oxaliplatin-based therapy (3 vs 6 months) for patients with high-risk stage II colorectal cancer. J. Clin. Oncol. 2019, 37 (Suppl. 15), 3501. [Google Scholar] [CrossRef]
- Tournigand, C.; André, T.; Bonnetain, F.; Chibaudel, B.; Lledo, G.; Hickish, T.; Tabernero, J.; Boni, C.; Bachet, J.-B.; Teixeira, L.; et al. Adjuvant Therapy With Fluorouracil and Oxaliplatin in Stage II and Elderly Patients (between ages 70 and 75 years) With Colon Cancer: Subgroup Analyses of the Multicenter International Study of Oxaliplatin, Fluorouracil, and Leucovorin in the Adjuvant Treatment of Colon Cancer Trial. J. Clin. Oncol. 2012, 30, 3353–3360. [Google Scholar] [PubMed]
- Grothey, A.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Souglakos, J.; Shi, Q.; Kerr, R.; Labianca, R.; et al. Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. N. Engl. J. Med. 2018, 378, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- André, T.; De Gramont, A.A.; Vernerey, D.; Chibaudel, B.B.; Bonnetain, F.; Tijeras-Raballand, A.A.; Scriva, A.A.; Hickish, T.T.; Tabernero, J.; Van Laethem, J.L.; et al. Adjuvant Fluorouracil, Leucovorin, and Oxaliplatin in Stage II to III Colon Cancer: Updated 10-Year Survival and Outcomes According to BRAF Mutation and Mismatch Repair Status of the MOSAIC Study. J. Clin. Oncol. 2015, 33, 4176–4187. [Google Scholar] [CrossRef] [PubMed]
- Sargent, D.J.; Marsoni, S.; Monges, G.; Thibodeau, S.N.; Labianca, R.; Hamilton, S.R.; French, A.J.; Kabat, B.; Foster, N.R.; Torri, V.; et al. Defective Mismatch Repair As a Predictive Marker for Lack of Efficacy of Fluorouracil-Based Adjuvant Therapy in Colon Cancer. J. Clin. Oncol. 2010, 28, 3219–3226. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N (%) n = 144 | ||
|---|---|---|---|
| Age (years) * | 72.2 (9.6) | ||
| Range | 48–93 | ||
| Gender | |||
| Female | 46 (31.9) | ||
| Male | 98 (68.1) | ||
| Localization | |||
| Right | 79 (54.9) | ||
| Left | 65 (45.1) | ||
| Differentiation grade | |||
| <50% | 26 (18.1) | ||
| ≥50% | 118 (81.9) | ||
| Lymph node ratio | |||
| Mean * (SD) | 6.7 (12.1) | ||
| Median (Q1–Q3) | 0.0 (0–9.3) | ||
| Histologic type | |||
| Colloid | 18 (12.5) | ||
| Adenocarcinoma | 125 (86.8) | ||
| Signet ring cell carcinoma | 1 (0.7) | ||
| TNM Stage | |||
| II | 80 (55.6) | ||
| III | 64 (44.4) | ||
| Lymphatic vascular invasion | |||
| Negative | 108 (75.0) | ||
| Positive | 36 (25.0) | ||
| Blood vessel invasion | |||
| Negative | 102 (70.8) | ||
| Positive | 42 (29.2) | ||
| Perineural invasion | |||
| Negative | 112 (77.8) | ||
| Positive | 32 (22.2) | ||
| Variable | N (%) n = 144 | ||
|---|---|---|---|
| MMR status | |||
| pMMR | 126 (87.5) | ||
| dMMR | 18 (12.5) | ||
| IHC BRAF (V600 mutation) * | |||
| Negative | 125 (89.3) | ||
| Positive | 15 (10.7) | ||
| CMS classification | |||
| CMS1 | 18 (12.5) | ||
| CMS2/CMS3 | 117 (81.3) | ||
| CMS4 | 9 (6.3) | ||
| IHC PD-L1 expression | |||
| Negative | 64 (44.4) | ||
| ≥1–<5% | 51 (35.4) | ||
| ≥5%, >50% | 29 (20.1) | ||
| Variable | MMR pMMR n (%) dMMR n (%) | p | CMS1 n (%) | CMS2/CMS3 n (%) | CMS4 n (%) | p | PD-L1–L Neg (%) Pos (%) | p | PD-L1–H Neg (%) Pos (%) | p | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | Mean (SD) | 72.2 (9.5) | 72.3 (10.6) | 72.6 (9.2) | 66.0 (11.2) | 72.7 (10.4) | 71.8 (9.6) | ||||
| 72.3 (10.6) | 0.948 1 | 0.134 1 | 71.8 (9.0) | 0.583 3 | 73.9 (9.4) | 0.296 3 | |||||
| Gender | Men | 86 (68.3) | 12 (66.7) | 79 (67.5) | 7 (77.8) | 41 (64.1) | 77 (67.0) | ||||
| 12 (66.7) | 57 (71.3) | 21 (72.4) | |||||||||
| Women | 40 (31.7) | 6 (33.3) | 38 (32.5) | 2 (22.2) | 23 (35.9) | 38 (33.0) | |||||
| 6 (33.3) | 0.893 2 | 0.884 4 | 23 (28.7) | 0.358 2 | 8 (27.6) | 0.573 2 | |||||
| Localization | Right | 63 (50.0) | 16 (88.9) | 57 (48.7) | 6 (66.7) | 29 (45.3) | 61 (53.0) | ||||
| 16 (88.9) | 50 (62.5) | 18 (62.1) | |||||||||
| Left | 63 (50.0) | 2 (11.1) | 60 (51.3) | 3 (33.3) | 35 (54.7) | 54 (47.0) | |||||
| 2 (11.1) | 0.0022 | 0.0034 | 30 (37.5) | 0.0392 | 11 (37.9) | 0.412 2 | |||||
| TNM Stage | II | 68 (54.0) | 12 (66.7) | 67 (57.3) | 1 (11.1) | 30 (46.9) | 58 (50.4) | ||||
| 12 (66.7) | 50 (53.1) | 22 (75.9) | |||||||||
| III | 58 (46.0) | 6 (33.3) | 50 (42.7) | 8 (88.9) | 34 (62.5) | 57 (49.6) | |||||
| 6 (33.3) | 0.310 2 | 0.0164 | 30 (37.5) | 0.061 2 | 7 (24.1) | 0.0142 | |||||
| Lymphatic vascular invasion | No | 92 (73.0) | 16 (88.9) | 87 (74.4) | 5 (55.6) | 47 (73.4) | 83 (72.2) | ||||
| 16 (55.9) | 61 (76.3) | 25 (86.2) | |||||||||
| Yes | 34 (27.0) | 2 (11.1) | 30 (25.6) | 4 (44.4) | 17 (26.6) | 32 (27.8) | |||||
| 2 (11.1) | 0.243 4 | 0.169 4 | 19 (23.8) | 0.699 2 | 4 (13.8) | 0.119 2 | |||||
| Blood vessel invasion | No | 88 (69.8) | 14 (77.8) | 90 (68.4) | 8 (88.9) | 40 (62.5) | 79 (68.7) | ||||
| 14 (77.8) | 62 (77.5) | 23 (79.3) | |||||||||
| Yes | 38 (30.2) | 4 (22.2) | 37 (31.6) | 1 (11.1) | 24 (37.5) | 36 (31.3) | |||||
| 4 (22.2) | 0.488 2 | 0.373 4 | 18 (22.5) | 0.0492 | 6 (20.7) | 0.261 2 | |||||
| Perineural invasion | No | 96 (76.2) | 16 (88.9) | 91 (77.8) | 5 (55.6) | 47 (73.4) | 85 (73.9) | ||||
| 16 (88.9) | 65 (81.3) | 27 (93.1) | |||||||||
| Yes | 30 (23.8) | 2 (11.1) | 26 (22.2) | 4 (44.4) | 17 (26.6) | 30 (26.1) | |||||
| 2 (11.1) | 0.363 4 | 0.146 4 | 15 (18.8) | 0.262 2 | 2 (6.9) | 0.026 2 | |||||
| BRAF IHC * | Wild | 118 (94.4) | 7 (46.7) | 109 (94.0) | 9 (100) | 56 (90.3) | 105 (93.8) | ||||
| 7 (46.7) | 69 (88.5) | 20 (71.4) | |||||||||
| Mutant | 7 (5.6) | 8 (53.3) | 7 (6.0) | 0 (0.0) | 6 (9.7) | 7 (6.2) | |||||
| 8 (53.3) | <0.001 4 | <0.0014 | 9 (11.5) | 0.724 2 | 8 (28.6) | 0.0022 | |||||
| MMR status | pMMR | - | 0 (0.0) | 117 (100) | 9 (100) | 60 (93.8) | 107 (93.0) | ||||
| 66 (82.5) | 19 (65.5) | ||||||||||
| dMMR | - | 18 (100) | 0 (0.0) | 0 (0.0) | 4 (6.3) | 8 (7.0) | |||||
| - | <0.0014 | 14 (17.5) | 0.0432 | 10 (34.5) | 0.0012 | ||||||
| PD-L1–L | Neg | 60 (47.6) | 4 (22.2) | 58 (49.6) | 2 (22.2) | - | - | ||||
| 4 (22.2) | |||||||||||
| Pos | 66 (52.4) | 14 (77.8) | 59 (50.4) | 7 (77.8) | - | - | |||||
| 14 (77.8) | 0.0432 | 0.038 4 | - | - | |||||||
| PD-L1–H | Neg | 107 (84.9) | 8 (44.4) | 99 (84.6) | 8 (88.9) | - | - | ||||
| 8 (44.4) | |||||||||||
| Pos | 19 (15.1) | 10 (55.6) | 18 (15.4) | 1 (11.1) | - | - | |||||
| 10 (55.6) | <0.001 4 | <0.001 4 | - | - |
| Variable (Reference) | Hazard Ratio | 95% CI | p Value |
|---|---|---|---|
| Age (Mean) | 1.09 | 1.04–1.14 | <0.001 |
| Gender (Male/Female) | 0.96 | 0.46–2.00 | 0.913 |
| Localization (Right/Left) | 0.78 | 0.39–1.55 | 0.479 |
| Stage (II/III) | 1.51 | 0.76–2.99 | 0.242 |
| Lymphatic vascular invasion | 0.88 | 0.40–1.96 | 0.763 |
| Blood vessel invasion | 1.81 | 0.86–3.78 | 0.114 |
| Perineural invasion | 2.20 | 0.99–4.90 | 0.050 |
| BRAF IHC * (wt/mutant) | 0.25 | 0.05–1.14 | 0.056 |
| MMR status (p/d) | 0.48 | 0.15–1.54 | 0.211 |
| CMS1–CMS2/CMS3 | 1.96 | 0.61–6.34 | |
| CMSCMS1–CMS4 | 4.38 | 0.78–24.5 | 0.224 |
| PD-L1–L | 0.40 | 0.20–0.81 | 0.010 |
| PD-L1–H | 0.41 | 0.15–1.07 | 0.064 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azcue, P.; Encío, I.; Guerrero Setas, D.; Suarez Alecha, J.; Galbete, A.; Mercado, M.; Vera, R.; Gomez-Dorronsoro, M.L. PD-L1 as a Prognostic Factor in Early-Stage Colon Carcinoma within the Immunohistochemical Molecular Subtype Classification. Cancers 2021, 13, 1943. https://doi.org/10.3390/cancers13081943
Azcue P, Encío I, Guerrero Setas D, Suarez Alecha J, Galbete A, Mercado M, Vera R, Gomez-Dorronsoro ML. PD-L1 as a Prognostic Factor in Early-Stage Colon Carcinoma within the Immunohistochemical Molecular Subtype Classification. Cancers. 2021; 13(8):1943. https://doi.org/10.3390/cancers13081943
Chicago/Turabian StyleAzcue, Pablo, Ignacio Encío, David Guerrero Setas, Javier Suarez Alecha, Arkaitz Galbete, María Mercado, Ruth Vera, and Maria Luisa Gomez-Dorronsoro. 2021. "PD-L1 as a Prognostic Factor in Early-Stage Colon Carcinoma within the Immunohistochemical Molecular Subtype Classification" Cancers 13, no. 8: 1943. https://doi.org/10.3390/cancers13081943
APA StyleAzcue, P., Encío, I., Guerrero Setas, D., Suarez Alecha, J., Galbete, A., Mercado, M., Vera, R., & Gomez-Dorronsoro, M. L. (2021). PD-L1 as a Prognostic Factor in Early-Stage Colon Carcinoma within the Immunohistochemical Molecular Subtype Classification. Cancers, 13(8), 1943. https://doi.org/10.3390/cancers13081943