
De Novo Carcinoma after Solid Organ Transplantation to Give Insight into Carcinogenesis in General—A Systematic Review and Meta-Analysis

 , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy and Study Selection
2.2. Data Collection and Interpretation
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
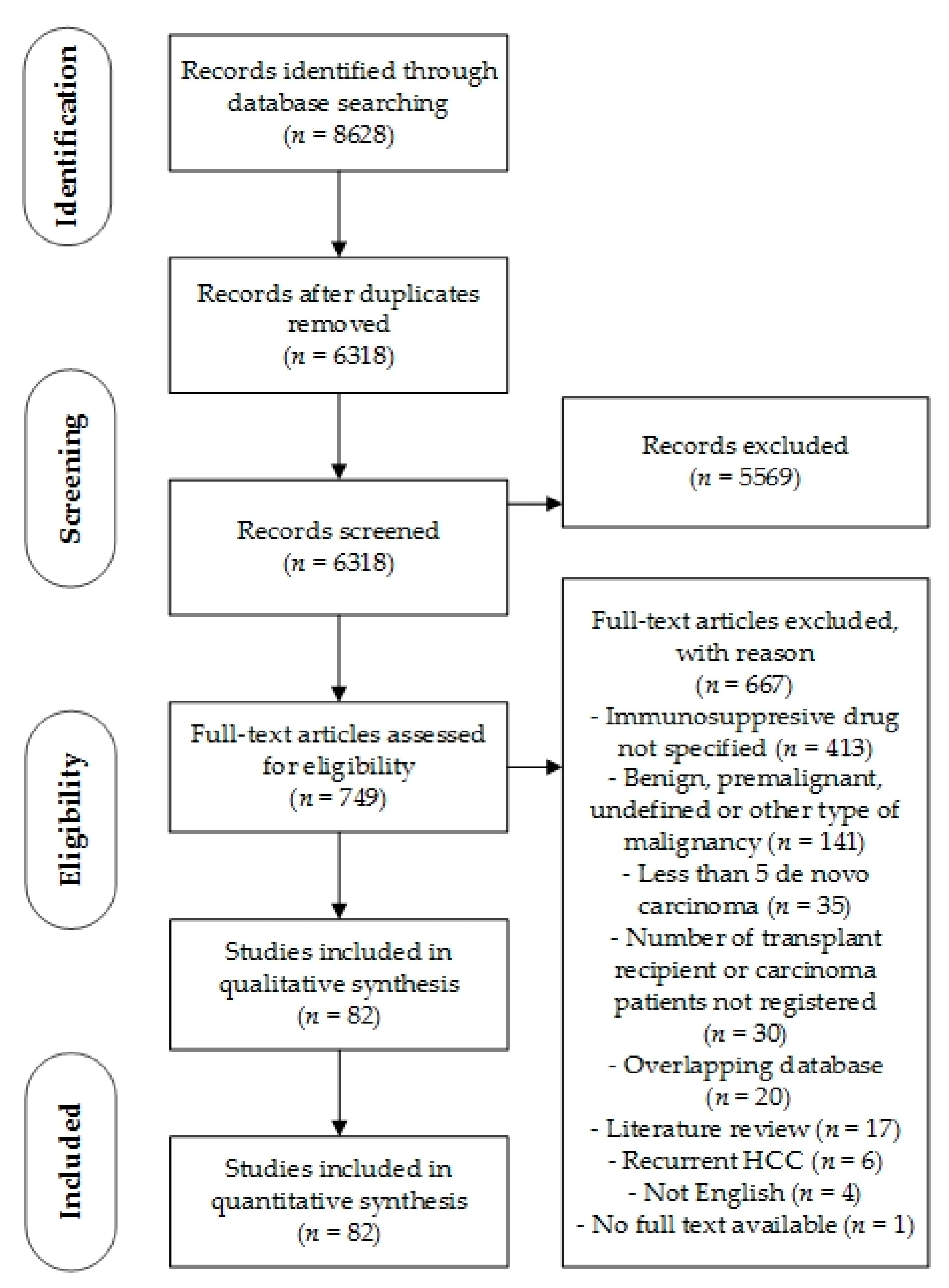
3.1. Study Selection
3.2. Study Characteristics
3.3. Quality Assessment
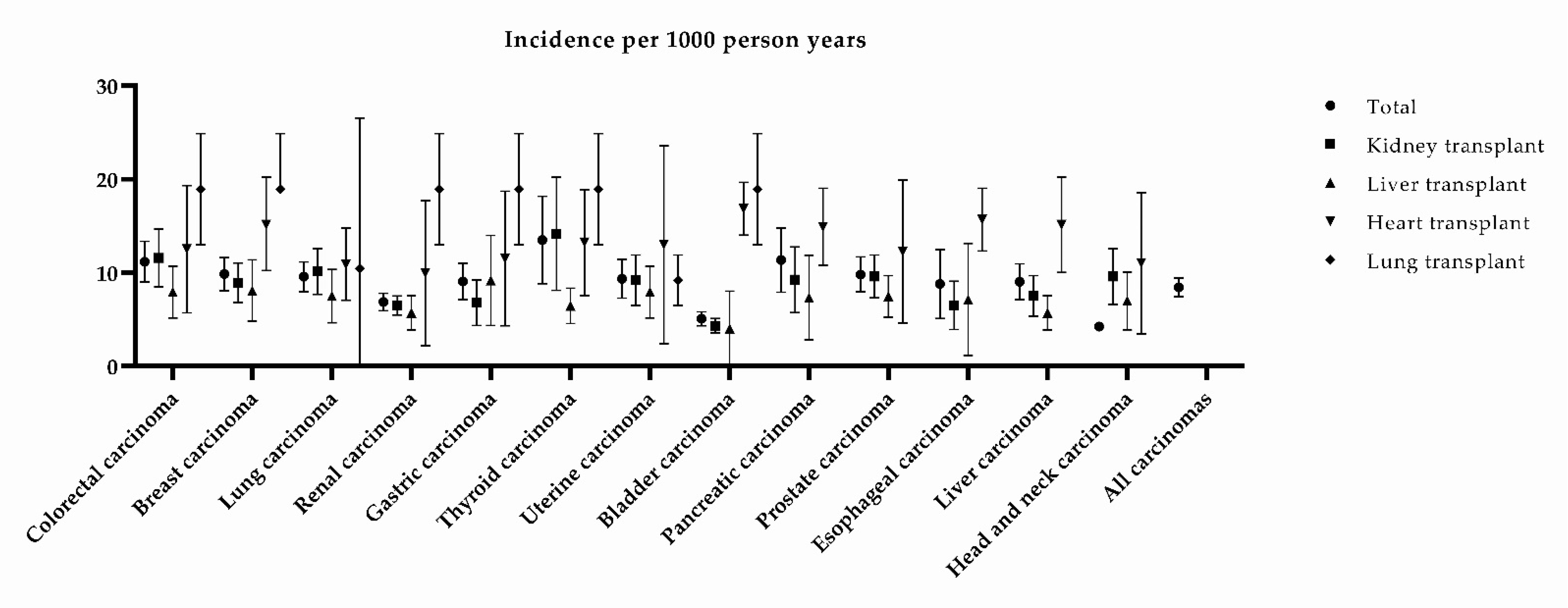
3.4. De Novo Carcinoma Occurrence
3.5. CsA Versus TAC, AZA, MMF, and SIR
3.6. AZA Versus TAC and MMF
3.7. MMF Versus TAC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Wiseman, A.C. Immunosuppressive Medications. Clin. J. Am. Soc. Nephrol. 2016, 11, 332–343. [Google Scholar] [CrossRef]
- Noble, S.; Markham, A. Cyclosporin. A review of the pharmacokinetic properties, clinical efficacy and tolerability of a microemulsion-based formulation (Neoral). Drugs 1995, 50, 924–941. [Google Scholar] [CrossRef] [PubMed]
- Placebo-controlled study of mycophenolate mofetil combined with cyclosporin and corticosteroids for prevention of acute rejection. European Mycophenolate Mofetil Cooperative Study Group. Lancet 1995, 345, 1321–1325. [CrossRef]
- Keown, P.; Landsberg, D.; Hardie, I.; Rigby, R.; Isoniemi, H.; Häyry, P.; Morris, P. A blinded, randomized clinical trial of mycophenolate mofetil for the prevention of acute rejection in cadaveric renal transplantation. The Tricontinental Mycophenolate Mofetil Renal Transplantation Study Group. Transplantation 1996, 61, 1029–1037. [Google Scholar]
- Mycophenolate mofetil for the prevention of acute rejection of primary cadaveric kidney transplants: Status of the MYC 1866 study at 1 year. The U.S. Mycophenolate Mofetil Study Group. Transplant. Proc. 1997, 29, 348–349. [CrossRef]
- Wagner, M.; Earley, A.K.; Webster, A.C.; Schmid, C.H.; Balk, E.M.; Uhlig, K. Mycophenolic acid versus azathioprine as primary immunosuppression for kidney transplant recipients. Cochrane Database Syst. Rev. 2015, Cd007746. [Google Scholar] [CrossRef] [PubMed]
- Chiu, B.; Sergi, C. Malignancy after Heart Transplantation: A Systematic Review of the Incidence and Risk Factors Compared with Other Solid Organ Transplants. J. Clin. Exp. Cardiol. 2013, S9, 5. [Google Scholar] [CrossRef]
- Liu, Z.N.; Wang, W.T.; Yan, L.N. De Novo Malignancies After Liver Transplantation With 14 Cases at a Single Center. Transplant. Proc. 2015, 47, 2483–2487. [Google Scholar] [CrossRef]
- Herrero, J.I. De novo malignancies following liver transplantation: Impact and recommendations. Liver Transplant. 2009, 15 (Suppl. S2), S90–S94. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 2 March 2021).
- Review Manager (RevMan) [Computer Program]. Version 5.3; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014.
- Ferlay, J.; Ervik, M.; Lam, F.; Colombet, M.; Mery, L.; Piñeros, M.; Znaor, A.; Soerjomataram, I.; Bray, F. Global Cancer Observatory: Cancer Today; International Agency for Research on Cancer: Lyon, France, 2020; Available online: https://gco.iarc.fr/today/home (accessed on 2 March 2021).
- Freedman, N.D.; Silverman, D.T.; Hollenbeck, A.R.; Schatzkin, A.; Abnet, C.C. Association between smoking and risk of bladder cancer among men and women. JAMA 2011, 306, 737–745. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Yuan, J.M.; Wang, R.; Gao, Y.T.; Yu, M.C. Alcohol, tobacco, and diet in relation to esophageal cancer: The Shanghai Cohort Study. Nutr. Cancer 2008, 60, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Botha, P.; Peaston, R.; White, K.; Forty, J.; Dark, J.H.; Parry, G. Smoking after cardiac transplantation. Am. J. Transplant. 2008, 8, 866–871. [Google Scholar] [CrossRef] [PubMed]
- Tjon, A.S.; Sint Nicolaas, J.; Kwekkeboom, J.; De Man, R.A.; Kazemier, G.; Tilanus, H.W.; Hansen, B.E.; Van der Laan, L.J.; Tha-In, T.; Metselaar, H.J. Increased incidence of early de novo cancer in liver graft recipients treated with cyclosporine: An association with C2 monitoring and recipient age. Liver Transplant. 2010, 16, 837–846. [Google Scholar] [CrossRef]
- Campistol, J.M.; Eris, J.; Oberbauer, R.; Friend, P.; Hutchison, B.; Morales, J.M.; Claesson, K.; Stallone, G.; Russ, G.; Rostaing, L.; et al. Sirolimus therapy after early cyclosporine withdrawal reduces the risk for cancer in adult renal transplantation. J. Am. Soc. Nephrol. 2006, 17, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.U.; Kim, L.K.; Choi, J.M. Revisiting the Concept of Targeting NFAT to Control T Cell Immunity and Autoimmune Diseases. Front. Immunol. 2018, 9, 2747. [Google Scholar] [CrossRef]
- Jiang, T.; Zhou, C.; Ren, S. Role of IL-2 in cancer immunotherapy. Oncoimmunology 2016, 5, e1163462. [Google Scholar] [CrossRef] [PubMed]
- Morteau, O.; Blundell, S.; Chakera, A.; Bennett, S.; Christou, C.M.; Mason, P.D.; Cornall, R.J.; O’Callaghan, C.A. Renal transplant immunosuppression impairs natural killer cell function in vitro and in vivo. PLoS ONE 2010, 5, e13294. [Google Scholar] [CrossRef] [PubMed]
- Sauma, D.; Fierro, A.; Mora, J.R.; Lennon-Duménil, A.M.; Bono, M.R.; Rosemblatt, M.; Morales, J. Cyclosporine preconditions dendritic cells during differentiation and reduces IL-2 and IL-12 production following activation: A potential tolerogenic effect. Transplant. Proc. 2003, 35, 2515–2517. [Google Scholar] [CrossRef] [PubMed]
- Tiefenthaler, M.; Hofer, S.; Ebner, S.; Ivarsson, L.; Neyer, S.; Herold, M.; Mayer, G.; Fritsch, P.; Heufler, C. In vitro treatment of dendritic cells with tacrolimus: Impaired T-cell activation and IP-10 expression. Nephrol. Dial. Transplant. 2004, 19, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Ren, Y.; Yang, Y.; Yang, J.; Xie, R.; Fan, H. Tolerogenic dendritic cells modified by tacrolimus suppress CD4(+) T-cell proliferation and inhibit collagen-induced arthritis in mice. Int. Immunopharmacol. 2014, 21, 247–254. [Google Scholar] [CrossRef]
- Weischer, M.; Rocken, M.; Berneburg, M. Calcineurin inhibitors and rapamycin: Cancer protection or promotion? Exp. Dermatol. 2007, 16, 385–393. [Google Scholar] [CrossRef]
- Durnian, J.M.; Stewart, R.M.; Tatham, R.; Batterbury, M.; Kaye, S.B. Cyclosporin-A associated malignancy. Clin. Ophthalmol. 2007, 1, 421–430. [Google Scholar] [PubMed]
- Andre, N.; Roquelaure, B.; Conrath, J. Molecular effects of cyclosporine and oncogenesis: A new model. Med. Hypotheses 2004, 63, 647–652. [Google Scholar] [CrossRef] [PubMed]
- Euvrard, S.; Ulrich, C.; Lefrancois, N. Immunosuppressants and skin cancer in transplant patients: Focus on rapamycin. Dermatol. Surg. 2004, 30, 628–633. [Google Scholar] [CrossRef] [PubMed]
- Jakowlew, S.B. Transforming growth factor-beta in cancer and metastasis. Cancer Metastasis Rev. 2006, 25, 435–457. [Google Scholar] [CrossRef] [PubMed]
- Zhou, A.Y.; Ryeom, S. Cyclosporin A promotes tumor angiogenesis in a calcineurin-independent manner by increasing mitochondrial reactive oxygen species. Mol. Cancer Res. 2014, 12, 1663–1676. [Google Scholar] [CrossRef] [PubMed]
- Denko, N.C. Hypoxia, HIF1 and glucose metabolism in the solid tumour. Nat. Rev. Cancer 2008, 8, 705–713. [Google Scholar] [CrossRef]
- Bieber, C.P.; Reitz, B.A.; Jamieson, S.W.; Oyer, P.E.; Stinson, E.B. Malignant lymphoma in cyclosporin A treated allograft recipients. Lancet 1980, 1, 43. [Google Scholar] [CrossRef]
- Cattaneo, D.; Gotti, E.; Perico, N.; Bertolini, G.; Kainer, G.; Remuzzi, G. Cyclosporine formulation and Kaposi’s sarcoma after renal transplantation. Transplantation 2005, 80, 743–748. [Google Scholar] [CrossRef] [PubMed]
- Rigotti, P.; Cadrobbi, R.; Baldan, N.; Sarzo, G.; Parise, P.; Furian, L.; Marchini, F.; Ancona, E. Mycophenolate mofetil (MMF) versus azathioprine (AZA) in pancreas transplantation: A single-center experience. Clin. Nephrol. 2000, 53, S52–S54. [Google Scholar]
- Ransom, J.T. Mechanism of action of mycophenolate mofetil. Ther. Drug Monit. 1995, 17, 681–684. [Google Scholar] [CrossRef]
- Van Scoik, K.G.; Johnson, C.A.; Porter, W.R. The pharmacology and metabolism of the thiopurine drugs 6-mercaptopurine and azathioprine. Drug Metab. Rev. 1985, 16, 157–174. [Google Scholar] [CrossRef]
- Van Os, E.C.; Zins, B.J.; Sandborn, W.J.; Mays, D.C.; Tremaine, W.J.; Mahoney, D.W.; Zinsmeister, A.R.; Lipsky, J.J. Azathioprine pharmacokinetics after intravenous, oral, delayed release oral and rectal foam administration. Gut 1996, 39, 63–68. [Google Scholar] [CrossRef]
- Jung, E.J.; Hur, M.; Kim, Y.L.; Lee, G.H.; Kim, J.; Kim, I.; Lee, M.; Han, H.K.; Kim, M.S.; Hwang, S.; et al. Oral administration of 1,4-aryl-2-mercaptoimidazole inhibits T-cell proliferation and reduces clinical severity in the murine experimental autoimmune encephalomyelitis model. J. Pharmacol. Exp. Ther. 2009, 331, 1005–1013. [Google Scholar] [CrossRef] [PubMed]
- Maltzman, J.S.; Koretzky, G.A. Azathioprine: Old drug, new actions. J. Clin. Invest. 2003, 111, 1122–1124. [Google Scholar] [CrossRef] [PubMed]
- Marinković, G.; Hamers, A.A.; De Vries, C.J.; De Waard, V. 6-Mercaptopurine reduces macrophage activation and gut epithelium proliferation through inhibition of GTPase Rac1. Inflamm. Bowel Dis. 2014, 20, 1487–1495. [Google Scholar] [CrossRef] [PubMed]
- Tiede, I.; Fritz, G.; Strand, S.; Poppe, D.; Dvorsky, R.; Strand, D.; Lehr, H.A.; Wirtz, S.; Becker, C.; Atreya, R.; et al. CD28-dependent Rac1 activation is the molecular target of azathioprine in primary human CD4+ T lymphocytes. J. Clin. Invest. 2003, 111, 1133–1145. [Google Scholar] [CrossRef] [PubMed]
- Marinković, G.; Kroon, J.; Hoogenboezem, M.; Hoeben, K.A.; Ruiter, M.S.; Kurakula, K.; Otermin Rubio, I.; Vos, M.; De Vries, C.J.M.; Van Buul, J.D.; et al. Inhibition of GTPase Rac1 in Endothelium by 6-Mercaptopurine Results in Immunosuppression in Nonimmune Cells: New Target for an Old Drug. J. Immunol. 2014, 192, 4370–4378. [Google Scholar] [CrossRef] [PubMed]
- Hessels, A.C.; Rutgers, A.; Sanders, J.S.F.; Stegeman, C.A. Thiopurine methyltransferase genotype and activity cannot predict outcomes of azathioprine maintenance therapy for antineutrophil cytoplasmic antibody associated vasculitis: A retrospective cohort study. PLoS ONE 2018, 13, e0195524. [Google Scholar] [CrossRef] [PubMed]
- Kahan, B.D. Sirolimus: A comprehensive review. Expert Opin. Pharmacother. 2001, 2, 1903–1917. [Google Scholar] [CrossRef] [PubMed]
- Hua, H.; Kong, Q.; Zhang, H.; Wang, J.; Luo, T.; Jiang, Y. Targeting mTOR for cancer therapy. J. Hematol. Oncol. 2019, 12, 71. [Google Scholar] [CrossRef] [PubMed]
- Hill, P.; Cross, N.B.; Barnett, A.N.R.; Palmer, S.C.; Webster, A.C. Polyclonal and monoclonal antibodies for induction therapy in kidney transplant recipients. Cochrane Database Syst. Rev. 2017, 1, CD004759. [Google Scholar] [CrossRef] [PubMed]
- Chapman, T.M.; Keating, G.M. Basiliximab: A review of its use as induction therapy in renal transplantation. Drugs 2003, 63, 2803–2835. [Google Scholar] [CrossRef]
- Meier-Kriesche, H.U.; Chu, A.H.; David, K.M.; Chi-Burris, K.; Steffen, B.J. Switching immunosuppression medications after renal transplantation--a common practice. Nephrol. Dial. Transplant. 2006, 21, 2256–2262. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Saraiya, M.; Unger, E.R.; Thompson, T.D.; Lynch, C.F.; Hernandez, B.Y.; Lyu, C.W.; Steinau, M.; Watson, M.; Wilkinson, E.J.; Hopenhayn, C.; et al. US assessment of HPV types in cancers: Implications for current and 9-valent HPV vaccines. J. Natl. Cancer Inst. 2015, 107, djv086. [Google Scholar] [CrossRef] [PubMed]
- Grulich, A.E.; Van Leeuwen, M.T.; Falster, M.O.; Vajdic, C.M. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef]
- Calne, R.Y.; White, D.J.; Thiru, S.; Evans, D.B.; McMaster, P.; Dunn, D.C.; Craddock, G.N.; Pentlow, B.D.; Rolles, K. Cyclosporin A in patients receiving renal allografts from cadaver donors. Lancet 1978, 2, 1323–1327. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Class of Inhibitor | Main Mechanism of Action | Immunosuppressive Drug |
|---|---|---|
| Calcineurin inhibitor | Inhibition of T cell proliferation | Cyclosporine A Tacrolimus |
| Antimetabolites | Inhibition DNA synthesis | Azathioprine Mofetil mycophenolate |
| mTOR inhibitors | Inhibition of mTOR kinase, involved in metabolism, growth, and proliferation | Sirolimus Everolimus |
| Variables | Transplant Recipients |
|---|---|
| Total solid organ transplant recipients, n | 237,540 |
| Kidney transplant | 207,304 |
| Liver transplant | 21,404 |
| Heart transplant | 5865 |
| Lung transplant | 2235 |
| Other transplant | 732 |
| Follow-up (in months), mean | 84.8 |
| Patients with PTC | |
| Sex (M/F), n | 1782/698 |
| Time until diagnosis (in months), mean | 66.8 (73/82) |
| Age at diagnosis, mean | 52.3 (42/82) |
| Living/cadaveric donor, n | 545/1642 (28/82) |
| Smokers, n | 250 |
| Induction therapy, n | 172 |
| Baseline immunosuppressive therapy, n | |
| AZA | 723 |
| MMF | 741 |
| CsA | 1055 |
| TAC | 627 |
| SIR | 201 |
| EVER | 6 |
| Combined triple therapies, n | |
| CsA + AZA + steroids | 296 |
| CsA + MMF + steroids | 90 |
| TAC + AZA + steroids | 10 |
| TAC + MMF + steroids | 203 |
| CsA + SIR + steroids | 90 |
| Survival | |
| 1-year (%) | 81.3 (12/82) |
| 3-year (%) | 75.5 (6/82) |
| 5-year (%) | 62.4 (16/82) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwart, E.S.; Yüksel, E.; Pannekoek, A.; de Vries, R.; Mebius, R.E.; Kazemier, G. De Novo Carcinoma after Solid Organ Transplantation to Give Insight into Carcinogenesis in General—A Systematic Review and Meta-Analysis. Cancers 2021, 13, 1122. https://doi.org/10.3390/cancers13051122
Zwart ES, Yüksel E, Pannekoek A, de Vries R, Mebius RE, Kazemier G. De Novo Carcinoma after Solid Organ Transplantation to Give Insight into Carcinogenesis in General—A Systematic Review and Meta-Analysis. Cancers. 2021; 13(5):1122. https://doi.org/10.3390/cancers13051122
Chicago/Turabian StyleZwart, Eline S., Esen Yüksel, Anne Pannekoek, Ralph de Vries, Reina E. Mebius, and Geert Kazemier. 2021. "De Novo Carcinoma after Solid Organ Transplantation to Give Insight into Carcinogenesis in General—A Systematic Review and Meta-Analysis" Cancers 13, no. 5: 1122. https://doi.org/10.3390/cancers13051122
APA StyleZwart, E. S., Yüksel, E., Pannekoek, A., de Vries, R., Mebius, R. E., & Kazemier, G. (2021). De Novo Carcinoma after Solid Organ Transplantation to Give Insight into Carcinogenesis in General—A Systematic Review and Meta-Analysis. Cancers, 13(5), 1122. https://doi.org/10.3390/cancers13051122