Aromatase and CDK4/6 Inhibitor-Induced Musculoskeletal Symptoms: A Systematic Review
by
 , , and
, , and
Angeliki Andrikopoulou
1,2, 
Oraianthi Fiste
1,2,
Michalis Liontos
1,2,
Meletios-Athanasios Dimopoulos
1,2 and
and
Flora Zagouri
1,2,* 1
Department of Clinical Therapeutics, Alexandra Hospital, Medical School, 11528 Athens, Greece
2
Medical School, National and Kapodistrian University of Athens, 80 Vasilissis Sofias Avenue, 11528 Athens, Greece
*
Author to whom correspondence should be addressed.
Cancers 2021, 13(3), 465; https://doi.org/10.3390/cancers13030465
Submission received: 14 November 2020
/
Revised: 19 January 2021
/
Accepted: 21 January 2021
/
Published: 26 January 2021
(This article belongs to the Section Systematic Review or Meta-Analysis in Cancer Research)
{kind=link}
Simple Summary
Aromatase inhibitor-induced musculoskeletal symptoms (AIMSS) occurs in up 50% of postmenopausal patients and is the reason for treatment discontinuation in 25% of patients with breast cancer. CDK4/6 inhibitors have been established in the treatment of hormone receptor-positive (HR) breast cancer. We aimed to assess the effect of treatment with CDK4/6 inhibitors on AIMSS. Arthralgia rate was lower in patients receiving aromatase inhibitors (AIs) in combination with CDK4/6 inhibitors (5.8–33.3%) compared with monotherapy with AIs (1–47%). Myalgias, back pain and bone pain also tended to be reduced in patients treated with CDK4/6 inhibitors. CDK4/6 inhibitors may alleviate musculoskeletal pain caused by AIs, although further studies are warranted.
Abstract
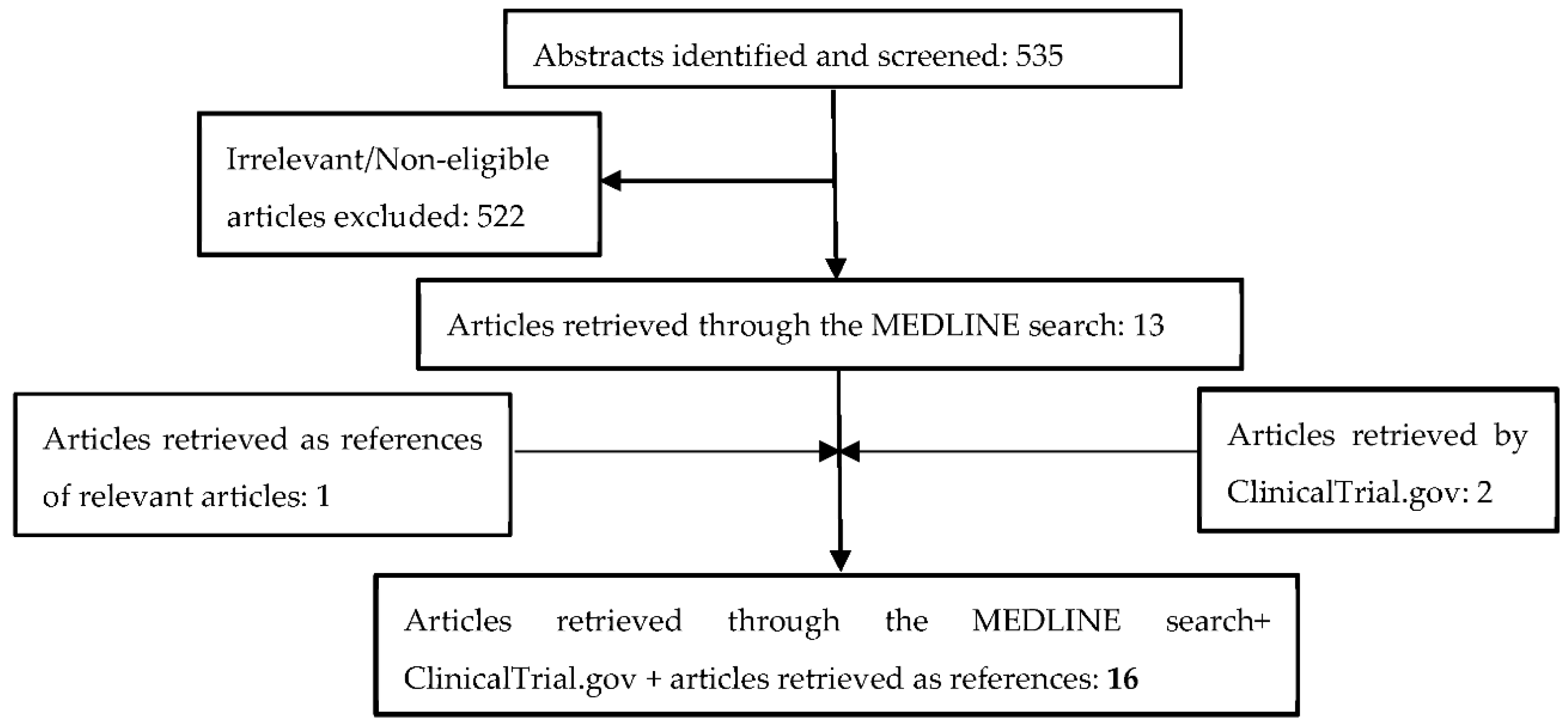
Background: Treatment with aromatase inhibitors (AIs) is fundamental in women with hormone receptor-positive breast cancer in the adjuvant as well as the metastatic setting. Even though it is considered to be a well-tolerated therapy, aromatase inhibitor-associated musculoskeletal syndrome (AIMSS) is the most common adverse event encountered by breast cancer patients. CDK4/6 inhibitors have emerged as a new treatment strategy in metastatic hormone receptor-positive breast cancer. However, the impact of CDK4/6 inhibitors on musculoskeletal symptoms caused by AIs is not well-defined. Objectives: This systematic review aims to identify the frequency of joint symptoms induced by treatment with AIs and CDK4/6 inhibitors in the metastatic setting. Search strategy: Eligible articles were identified by a search of existing literature for the period 2005/01/01–2021/01/01; The algorithm consisted of a predefined combination of the following keywords “breast”, “cancer”, “aromatase inhibitors”, “CDK4/6”, “phase III”. Selection criteria: This study was performed in accordance with PRISMA guidelines. All randomized controlled Phase III trials (RCTs) evaluating the administration of third-generation aromatase inhibitors (AIs) and CDK4/6 inhibitors in postmenopausal women in the metastatic setting were considered eligible for this review. Data collection: Overall, 16 randomized control trials (RCTs) were retrieved, of which nine studies explored the administration of AIs in the metastatic setting and seven studies investigated the combination of CDK4/6 inhibitors and AIs. Arthralgia was reported in 1–47% of patients treated with AIs and 5.8–33.3% of patients treated with CDK4/6 inhibitors. Myalgias occurred in 2–23.7% of patients receiving AIs compared with 4.8–11.9% of patients treated with CDK4/6 inhibitors. The incidence of back pain was 7–32.9% vs. 2.9–8.5% in postmenopausal women with metastatic disease treated with AIs and CDK4/6 inhibitors, respectively. Bone pain was reported in 7–32.9% of postmenopausal women treated with AIs and 2.9–8.5% of women treated with CDK4/6 inhibitors. Conclusions: AI treatment-induced musculoskeletal syndrome is an adverse event affecting over one-third (20–47%) of postmenopausal patients treated with AIs that often leads to treatment discontinuation. Data from RCTs provide evidence that the incidence of musculoskeletal symptoms is relatively decreased upon CDK4/6 inhibitor administration. CDK4/6 inhibitors may provide a protective role against AIMSS development.
Keywords:
breast; cancer; aromatase; CDK4/6 inhibitors; arthralgia; musculoskeletal