
Health-Related Quality of Life and Return to Work after Surgery for Spinal Meningioma: A Population-Based Cohort Study


 and
and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Samples
2.1.1. Spinal Meningioma Sample
2.1.2. General Population Sample
2.2. Measures
2.2.1. EQ-5D-3L
2.2.2. Study-Specific Questionnaire
2.2.3. Variables Retrieved from Electronic Medical Records
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
3.1. Characteristics of Samples
3.2. HRQoL in the Spinal Meningioma Sample
3.3. Comparison of HRQoL between Spinal Meningioma Sample and General Population Sample
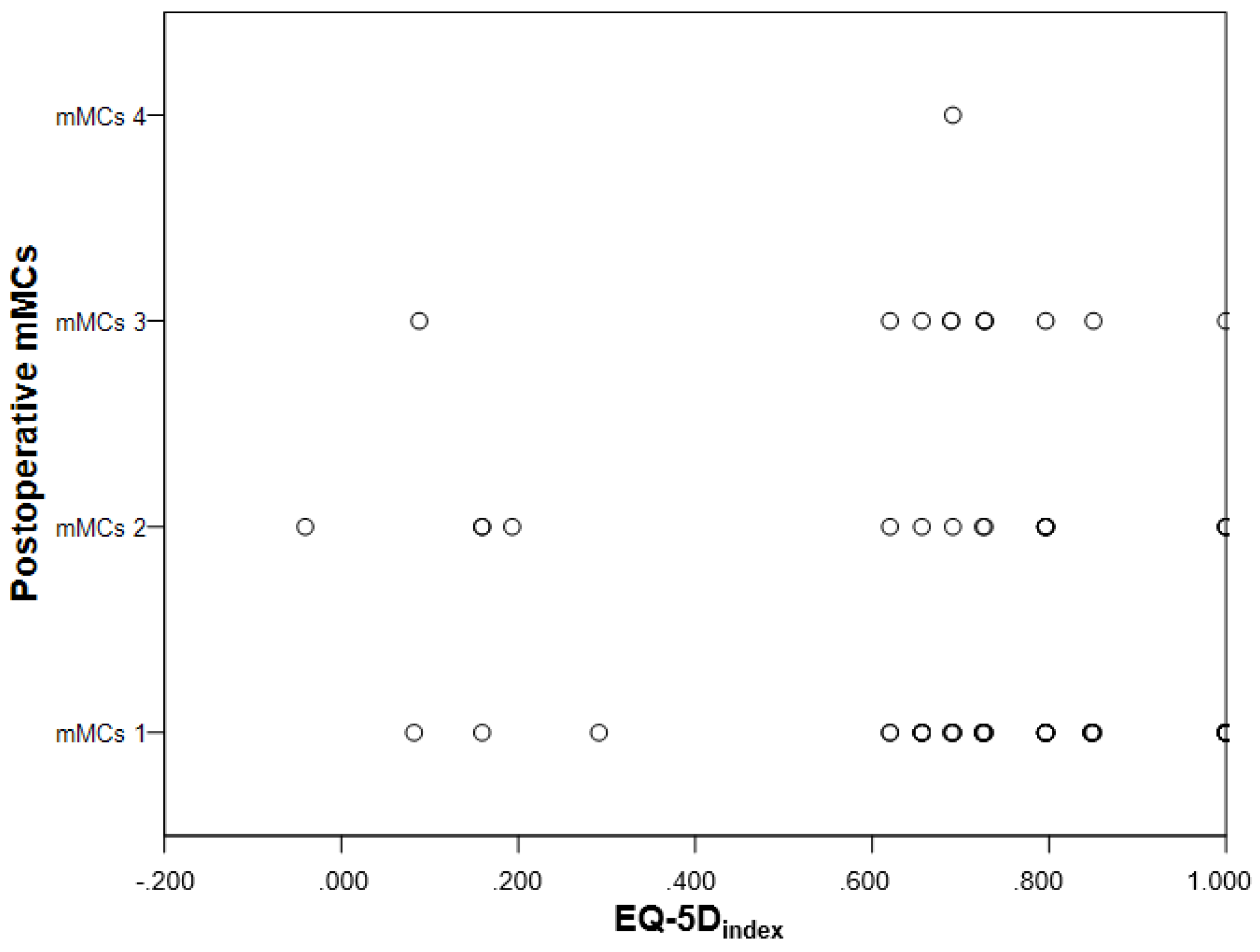
3.4. Comparison of HRQoL between Participants Differing in mMCs Grade
3.5. Employment Status and Return to Work after Spinal Meningioma Surgery
3.6. Comorbidity
3.7. Medication
3.8. Remaining Symptoms and Patient Reported Outcome
4. Discussion
Methodological Considerations, Strengths, and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ASA | American Society of Anesthesiologists |
| HRQoL | Health-Related Quality of Life |
| LSS | lumbar spinal stenosis |
| mMCs | modified McCormick scale |
| MRI | magnetic resonance imaging |
| OR | odds ratio |
| WHO | World Health Organization |
References
- Karimi, M.; Brazier, J. Health, Health-Related Quality of Life, and Quality of Life: What Is the Difference? PharmacoEconomics 2016, 34, 645–649. [Google Scholar] [CrossRef]
- Arwert, H.J.; Schults, M.; Meesters, J.J.L.; Wolterbeek, R.; Boiten, J.; Vliet Vlieland, T. Return to Work 2–5 Years After Stroke: A Cross Sectional Study in a Hospital-Based Population. J. Occup. Rehabil. 2016, 27, 239–246. [Google Scholar] [CrossRef]
- Corrigan, J.; Bogner, J.; Mysiw, W.; Clinchot, D.; Fugate, L. Life Satisfaction after Traumatic Brain Injury. J. Head Trauma Rehabil. 2001, 16, 543–555. [Google Scholar] [CrossRef] [PubMed]
- Fride, Y.; Adamit, T.; Maeir, A.; Assayag, E.; Bornstein, N.M.; Korczyn, A.D.; Katz, N. What Are the Correlates of Cognition and Participation to Return to Work after First Ever Mild Stroke? Top. Stroke Rehabil. 2015, 22, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Passier, P.; Visser-Meily, J.; Rinkel, G.; Lindeman, E.; Post, M. Life Satisfaction and Return to Work after Aneurysmal Subarachnoid Hemorrhage. J. Stroke Cerebrovasc. Dis. 2011, 20, 324–329. [Google Scholar] [CrossRef]
- Vestling, M.; Tufvesson, B.; Iwarsson, S. Indicators for Return to Work after Stroke and the Importance of Work for Subjective Well-Being and Life Satisfaction. J. Rehabil. Med. 2003, 35, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Matérne, M.; Lundqvist, L.; Strandberg, T. Opportunities and Barriers for Successful Return to Work after Acquired Brain Injury: A Patient Perspective. Work 2017, 56, 125–134. [Google Scholar] [CrossRef]
- Burström, K.; Johannesson, M.; Rehnberg, C. Deteriorating Health Status in Stockholm 1998–2002: Results from Repeated Population Surveys Using the EQ-5D. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2007, 16, 1547–1553. [Google Scholar] [CrossRef]
- Burström, K.; Johannesson, M.; Diderichsen, F. Swedish Population Health-Related Quality of Life Results Using the EQ-5D. Qual. Life Res. Int. J. Qual. Life Asp. Treat. Care Rehabil. 2001, 10, 621–635. [Google Scholar] [CrossRef]
- Kshettry, V.R.; Hsieh, J.K.; Ostrom, Q.T.; Kruchko, C.; Benzel, E.C.; Barnholtz-Sloan, J.S. Descriptive Epidemiology of Spinal Meningiomas in the United States. Spine 2015, 40, E886–E889. [Google Scholar] [CrossRef]
- Solero, C.; Fornari, M.; Giombini, S.; Lasio, G.; Oliveri, G.; Cimino, C.; Pluchino, F. Spinal Meningiomas: Review of 174 Operated Cases. Neurosurgery 1989, 25, 153–160. [Google Scholar] [CrossRef]
- Pettersson-Segerlind, J.; Fletcher-Sandersjöö, A.; Tatter, C.; Burström, G.; Persson, O.; Förander, P.; Mathiesen, T.; Bartek, J., Jr.; Edström, E.; Elmi-Terander, A. Long-Term Follow-Up and Predictors of Functional Outcome after Surgery for Spinal Meningiomas: A Population-Based Cohort Study. Cancers 2021, 13, 3244. [Google Scholar] [CrossRef]
- Abdulaziz, M.; Mallory, G.W.; Bydon, M.; De la Garza Ramos, R.; Ellis, J.A.; Laack, N.N.; Marsh, W.R.; Krauss, W.E.; Jallo, G.; Gokaslan, Z.L.; et al. Outcomes Following Myxopapillary Ependymoma Resection: The Importance of Capsule Integrity. Neurosurg. Focus 2015, 39, E8. [Google Scholar] [CrossRef] [PubMed]
- Jamilson Araújo Pereira, B.; Nogueira de Almeida, A.; Silva Paiva, W.; Henrique Pires de Aguiar, P.; Jacobsen Teixeira, M.; Kazue Nagahashi Marie, S. Neuro-Oncological Features of Spinal Meningiomas: Systematic Review. Neurochirurgie 2020, 66, 41–44. [Google Scholar] [CrossRef] [PubMed]
- Krauss, W.E.; Yolcu, Y.U.; Alvi, M.A.; Moinuddin, F.M.; Goyal, A.; Clarke, M.J.; Marsh, W.R.; Bydon, M. Clinical Characteristics and Management Differences for Grade II and III Spinal Meningiomas. J. Neuro-Oncol. 2021, 153, 313–320. [Google Scholar] [CrossRef]
- Voldřich, R.; Netuka, D.; Beneš, V. Spinal Meningiomas: Is Simpson Grade II Resection Radical Enough? Acta Neurochir. 2020, 162, 1401–1408. [Google Scholar] [CrossRef] [PubMed]
- Newman, W.; Berry-Candelario, J.; Villavieja, J.; Reiner, A.; Bilsky, M.; Laufer, I.; Barzilai, O. Improvement in Quality of Life Following Surgical Resection of Benign Intradural Extramedullary Tumors: A Prospective Evaluation of Patient-Reported Outcomes. Neurosurgery 2021, 88, 989–995. [Google Scholar] [CrossRef] [PubMed]
- Viereck, M.; Ghobrial, G.; Beygi, S.; Harrop, J. Improved Patient Quality of Life Following Intradural Extramedullary Spinal Tumor Resection. Journal of neurosurgery. Spine 2016, 25, 640–645. [Google Scholar] [CrossRef]
- Nassiri, F.; Price, B.; Shehab, A.; Au, K.; Cusimano, M.; Jenkinson, M.; Jungk, C.; Mansouri, A.; Santarius, T.; Suppiah, S.; et al. Life after Surgical Resection of a Meningioma: A Prospective Cross-Sectional Study Evaluating Health-Related Quality of Life. Neuro-Oncology 2019, 21, I32–I43. [Google Scholar] [CrossRef]
- Benz, L.; Wrensch, M.; Schildkraut, J.; Bondy, M.; Warren, J.; Wiemels, J.; Claus, E. Quality of Life after Surgery for Intracranial Meningioma. Cancer 2018, 124, 161–166. [Google Scholar] [CrossRef]
- Van Alkemade, H.; de Leau, M.; Dieleman, E.; Kardaun, J.; van Os, R.; Vandertop, P.; vam Furth, W.; Stalpers, L. Impaired Survival and Long-Term Neurological Problems in Benign Meningioma. Neuro-Oncology 2012, 14, 658–666. [Google Scholar] [CrossRef]
- Najafabadi, A.H.Z.; Peeters, M.C.M.; Dirven, L.; Lobatto, D.J.; Groen, J.L.; Broekman, M.L.D.; Peerdeman, S.M.; Peul, W.C.; Taphoorn, M.J.B.; van Furth, W.R. Impaired Health-Related Quality of Life in Meningioma Patients-a Systematic Review. Neuro-Oncology 2017, 19, 897–907. [Google Scholar] [CrossRef]
- Van der Vossen, S.; Schepers, V.; Berkelbach van der Sprenkel, J.; Visser-Meily, J.; Post, M. Cognitive and Emotional Problems in Patients after Cerebral Meningioma Surgery. J. Rehabil. Med. 2014, 46, 430–437. [Google Scholar] [CrossRef]
- Gupta, R.; Kumar, R. Benign Brain Tumours and Psychiatric Morbidity: A 5-Years Retrospective Data Analysis. Aust. N. Z. J. Psychiatry 2004, 38, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Bommakanti, K.; Gaddamanugu, P.; Alladi, S.; Purohit, A.; Chadalawadi, S.; Mekala, S.; Somayajula, S. Pre-Operative and Post-Operative Psychiatric Manifestations in Patients with Supratentorial Meningiomas. Clin. Neurol. Neurosurg. 2016, 147, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Schepers, V.; van der Vossen, S.; Berkelbach van der Sprenkel, J.; Visser-Meily, J.; Post, M. Participation Restrictions in Patients after Surgery for Cerebral Meningioma. J. Rehabil. Med. 2018, 50, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Sumkovski, R.; Micunovic, M.; Kocevski, I.; Ilievski, B.; Petrov, I. Surgical Treatment of Meningiomas—Outcome Associated With Type of Resection, Recurrence, Karnofsky Performance Score, Mitotic Count. Open Access Maced. J. Med Sci. 2019, 7, 56. [Google Scholar] [CrossRef]
- Krupp, W.; Klein, C.; Koschny, R.; Holland, H.; Seifert, V.; Meixensberger, J. Assessment of Neuropsychological Parameters and Quality of Life to Evaluate Outcome in Patients with Surgically Treated Supratentorial Meningiomas. Neurosurgery 2009, 64, 40–47. [Google Scholar] [CrossRef]
- Pettersson-Segerlind, J.; Orrego, A.; Lönn, S.; Mathiesen, T. Long-Term 25-Year Follow-up of Surgically Treated Parasagittal Meningiomas. World Neurosurg. 2011, 76, 564–571. [Google Scholar] [CrossRef]
- Mathiesen, T.; Lindquist, C.; Kihlström, L.; Karlsson, B. Recurrence of Cranial Base Meningiomas. Neurosurgery 1996, 39, 2–9. [Google Scholar] [CrossRef]
- Jääskeläinen, J. Seemingly Complete Removal of Histologically Benign Intracranial Meningioma: Late Recurrence Rate and Factors Predicting Recurrence in 657 Patients. A Multivariate Analysis. Surg. Neurol. 1986, 26, 461–469. [Google Scholar] [CrossRef]
- Sankila, R.; Kallio, M.; Jääskeläinen, J.; Hakulinen, T. Long-Term Survival of 1986 Patients with Intracranial Meningioma Diagnosed from 1953 to 1984 in Finland. Comparison of the Observed and Expected Survival Rates in a Population-Based Series. Cancer 1992, 70, 1568–1576. [Google Scholar] [CrossRef]
- Kalasauskas, D.; Keric, N.; Abu Ajaj, S.; von Cube, L.; Ringel, F.; Renovanz, M. Psychological Burden in Meningioma Patients under a Wait-and-Watch Strategy and after Complete Resection Is High-Results of a Prospective Single Center Study. Cancers 2020, 12, 3503. [Google Scholar] [CrossRef]
- Kalasauskas, D.; Keric, N.; Ajaj, S.A.; von Cube, L.; Ringel, F.; Renovanz, M. Distress and Quality of Life Do Not Change over Time in Patients with Operated and Conservatively Managed Intracranial Meningioma. Acta Neurochir. 2021, 163, 3417–3424. [Google Scholar] [CrossRef]
- Thurin, E.; Corell, A.; Gulati, S.; Smits, A.; Henriksson, R.; Bartek, J.; Salvesen, Ø.; Jakola, A. Return to Work Following Meningioma Surgery: A Swedish Nationwide Registry-Based Matched Cohort Study. Neuro-Oncol. Pract. 2020, 7, 320–328. [Google Scholar] [CrossRef]
- Battié, M.; Jones, C.; Schopflocher, D.; HuCC, R. Health-Related Quality of Life and Comorbidities Associated with Lumbar Spinal Stenosis. Spine J. Off. J. N. Am. Spine Soc. 2012, 12, 189–195. [Google Scholar] [CrossRef]
- Kobayashi, Y.; Ogura, Y.; Kitagawa, T.; Yonezawa, Y.; Takahashi, Y.; Yasuda, A.; Shinozaki, Y.; Ogawa, J. Gender Differences in Pre- and Postoperative Health-Related Quality of Life Measures in Patients Who Have Had Decompression Surgery for Lumbar Spinal Stenosis. Asian Spine J. 2019, 14, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, G.; Kurd, M.; Vaccaro, A. Lumbar Spinal Stenosis: How Is It Classified? J. Am. Acad. Orthop. Surg. 2016, 24, 843–852. [Google Scholar] [CrossRef] [PubMed]
- Weinsteinm, J.; Tosteson, T.; Lurie, J.; Tosteson, A.; Blood, E.; Hanscom, B.; Herkowitz, H.; Cammisa, F.; Albert, T.; Boden, S.; et al. Surgical versus Nonsurgical Therapy for Lumbar Spinal Stenosis. N. Engl. J. Med. 2008, 358, 794–810. [Google Scholar] [CrossRef]
- Oertel, M.F.; Ryang, Y.M.; Korinth, M.C.; Gilsbach, J.M.; Rohde, V. Long-Term Results of Microsurgical Treatment of Lumbar Spinal Stenosis by Unilateral Laminotomy for Bilateral Decompression. Neurosurgery 2006, 59, 1264–1269. [Google Scholar] [CrossRef] [PubMed]
- Truszczyńska, A.; Rąpała, K.; Truszczyński, O.; Tarnowski, A.; Łukawski, S. Return to Work after Spinal Stenosis Surgery and the Patient’s Quality of Life. Int. J. Occup. Med. Environ. Health 2013, 26, 394–400. [Google Scholar] [CrossRef] [PubMed]
- Rabin, R.; de Charro, F. EQ-5D: A Measure of Health Status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- Dolan, P.; Gudex, C.; Kind, P.; Williams, A. The Time Trade-off Method: Results from a General Population Study. Health Econ. 1996, 5, 141–154. [Google Scholar] [CrossRef]
- Dolan, P. Modeling Valuations for EuroQol Health States. Med. Care 1997, 35, 1095–1108. [Google Scholar] [CrossRef] [PubMed]
- McCormick, P.C.; Post, K.D.; Stein, B.M. Intradural Extramedullary Tumors in Adults. Neurosurg. Clin. N. Am. 1990, 1, 591–608. [Google Scholar] [CrossRef]
- Herno, A.; Airaksinen, O.; Saari, T.; Svomalainen, O. Pre- and Postoperative Factors Associated with Return to Work Following Surgery for Lumbar Spinal Stenosis. Am. J. Ind. Med. 1996, 30, 473–478. [Google Scholar] [CrossRef]
- Wagner, A.; Shiban, Y.; Lange, N.; Joerger, A.-K.; Hoffmann, U.; Meyer, B.; Shiban, E. The Relevant Psychological Burden of Having a Benign Brain Tumor: A Prospective Study of Patients Undergoing Surgical Treatment of Cranial Meningiomas. J. Neurosurg. 2019, 131, 1840–1847. [Google Scholar] [CrossRef]
- Wenström, I.; Eriksson, L.; Ebbeskog, B. Living in a Paradox--Women’s Experiences of Body and Life-World after Meningioma Surgery. J. Adv. Nurs. 2011, 68, 559–568. [Google Scholar] [CrossRef]
- Frati, A.; Pesce, A.; Toccaceli, G.; Fraschetti, F.; Caruso, R.; Raco, A. Spinal Meningiomas Prognostic Evaluation Score (SPES): Predicting the Neurological Outcomes in Spinal Meningioma Surgery. Neurosurg. Rev. 2018, 42, 115–125. [Google Scholar] [CrossRef]
- Takeuchi, A.; Miyamoto, K.; Hosoe, H.; Shimizu, K. Thoracic Paraplegia Due to Missed Thoracic Compressive Lesions after Lumbar Spinal Decompression Surgery. Report of Three Cases. J. Neurosurg. 2004, 100, 71–74. [Google Scholar] [CrossRef] [PubMed]
- Knafo, S.; Lonjon, G.; Vassal, M.; Bouyer, B.; Lonjon, N. Spinal Cord Compression Due to Undiagnosed Thoracic Meningioma Following Lumbar Surgery in an Elderly Patient: A Case Report. Orthop. Traumatol. Surg. Res. 2013, 99, 983–986. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ko, S.B.; Lee, S.W.; Shim, J.H. Paraplegia Due to Missed Thoracic Meningioma after Laminotomy for Lumbar Spinal Stenosis: Report of Two Cases. Asian Spine J. 2011, 5, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Tatter, C.; Fletcher-Sandersjöö, A.; Persson, O.; Burström, G.; Grane, P.; Edström, E.; Elmi-Terander, A. Incidence and Predictors of Kyphotic Deformity Following Resection of Cervical Intradural Tumors in Adults: A Population-Based Cohort Study. Acta Neurochir. 2020, 162, 2905–2913. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Value (n = 84) |
|---|---|
| Male sex | 12 (14.3%) |
| Age (years) at follow-up (range) | 70.6 ± 10.6 (42–92) |
| Arthritis | 44 (52.4%) |
| Time (years) from surgery to follow-up (range) | 8.7 ± 3.7 (3.1–15.7) |
| Tumor location * | |
| Cervical | 29 (34.5%) |
| Thoracic | 55 (65.5%) |
| Charlson Comorbidity Index | |
| 0 | 25 (29.8%) |
| 1 | 24 (28.6%) |
| 2 | 20 (23.8%) |
| 3 | 8 (9.5%) |
| 4 | 5 (6.0%) |
| 5 | 1 (1.2%) |
| Missing data | 1 (1.2%) |
| Laminectomy range (levels) | |
| 1 | 3 (3.6%) |
| 2 | 40 (47.6%) |
| 3 | 31 (36.9%) |
| 4 | 8 (9.5%) |
| 5 | 1 (1.2%) |
| 6 | 1 (1.2%) |
| Modified McCormick scale before surgery | |
| mMCs 1, neurologically intact | 22 (26.2%) |
| mMCs 2, mild motor or sensory deficits, functional independence | 37 (44.0%) |
| mMCs 3, moderate deficits, limited function, independent | 22 (26.2%) |
| mMCs 4, severe deficits, limited function, dependent | 3 (3.6%) |
| mMCs 5, paraplegia or quadriplegia | 0 (0.0%) |
| Modified McCormick scale after surgery | |
| mMCs 1, neurologically intact | 53 (63.1%) |
| mMCs 2, mild motor or sensory deficits, functional independence | 19 (22.6%) |
| mMCs 3, moderate deficits, limited function, independent | 11 (13.1%) |
| mMCs 4, severe deficits, limited function, dependent | 1 (1.2%) |
| mMCs 5, paraplegia or quadriplegia | 0 (0.0%) |
| Remaining symptoms after surgery | |
| Sensory symptoms upper extremities | 22 (26.2%) |
| Sensory symptoms lower extremities | 24 (28.6%) |
| Motor symptoms upper extremities | 29 (34.5%) |
| Motor symptoms lower extremities | 38 (45.2%) |
| Balance problems | 47 (56.0%) |
| Incontinence | 23 (27.4%) |
| Total | Men | Women | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| EQ-5D Dimensions | Spinal Meningioma n = 84 | General Population n = 252 | p1,2 | Spinal Meningioma n = 12 | General Population n = 36 | p1,2 | Spinal Meningioma n = 72 | General Population n = 216 | p1,2 | ||||||
| % | n | % | n | % | n | % | n | % | n | % | n | ||||
| Mobility | 0.221 | 0.414 | 0.108 | ||||||||||||
| No problems | 63.3 | 54 | 71.4 | 180 | 91.7 | 11 | 75.0 | 27 | 59.7 | 43 | 70.8 | 153 | |||
| Moderate problems | 35.7 | 30 | 28.2 | 71 | 8.3 | 1 | 25.0 | 9 | 40.3 | 29 | 28.7 | 61 | |||
| Severe problems | 0.0 | 0 | 0.4 | 1 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 0.5 | 1 | |||
| Self-care | 0.198 | ns | 0.196 | ||||||||||||
| No problems | 98.8 | 83 | 95.2 | 240 | 100.0 | 12 | 100.0 | 36 | 98.6 | 71 | 94.4 | 204 | |||
| Moderate problems | 1.2 | 1 | 3.6 | 9 | 0.0 | 0 | 0.0 | 0 | 1.4 | 1 | 4.2 | 9 | |||
| Severe problems | 0.0 | 0 | 1.2 | 3 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 1.4 | 3 | |||
| Usual activities | 0.878 | 1.000 | 1.000 | ||||||||||||
| No problems | 79.8 | 67 | 78.6 | 198 | 91.7 | 11 | 88.9 | 32 | 77.8 | 56 | 76.9 | 166 | |||
| Moderate problems | 20.2 | 17 | 17.5 | 44 | 8.3 | 1 | 11.1 | 4 | 22.2 | 16 | 18.5 | 40 | |||
| Severe problems | 0.0 | 0 | 4.0 | 10 | 0.0 | 0 | 0.0 | 0 | 0.0 | 0 | 4.6 | 10 | |||
| Pain/discomfort | 0.896 | 0.341 | 0.886 | ||||||||||||
| No problems | 36.9 | 31 | 36.1 | 91 | 58.3 | 7 | 41.7 | 15 | 33.3 | 24 | 35.2 | 76 | |||
| Moderate problems | 56.0 | 47 | 56.3 | 142 | 41.7 | 5 | 52.8 | 19 | 58.3 | 42 | 56.9 | 123 | |||
| Severe problems | 7.1 | 6 | 7.5 | 19 | 0.0 | 0 | 5.6 | 2 | 8.3 | 6 | 7.9 | 17 | |||
| Anxiety/depression | 0.589 | 1.000 | 0.571 | ||||||||||||
| No problems | 65.5 | 55 | 69.0 | 174 | 83.3 | 10 | 86.1 | 31 | 62.5 | 45 | 66.2 | 143 | |||
| Moderate problems | 31.0 | 26 | 29.8 | 75 | 8.3 | 1 | 13.9 | 5 | 34.7 | 25 | 32.4 | 70 | |||
| Severe problems | 3.6 | 3 | 1.2 | 3 | 8.3 | 1 | 0.0 | 0 | 2.8 | 2 | 1.4 | 3 | |||
| EQ-5Dindex mean (±SD) | 0.76 (±0.24) | 0.75 (±0.25) | 0.928 | 0.86 (±0.22) | 0.82 (±0.21) | 0.598 | 0.74 (±0.24) | 0.74 (±0.26) | 0.932 | ||||||
| EQVAS mean (±SD) | 74.0 (±17.9) | 71.7 (±21.7) | 0.392 | 78.7 (±15.4) | 78.2 (±17.4) | 0.934 | 73.1 (±18.3) 3 | 70.6 (±22.1) | 0.390 | ||||||
| EQ-5D Dimensions | mMCs 1–2 n = 72 | mMCs 3–5 n = 12 | p1 | ||
|---|---|---|---|---|---|
| % | n | % | n | ||
| Mobility | 0.023 | ||||
| No problems | 69.4 | 50 | 33.3 | 4 | |
| Moderate problems | 30.6 | 22 | 66.7 | 8 | |
| Severe problems | 0.0 | 0 | 0.0 | 0 | |
| Self-care | 1.000 | ||||
| No problems | 98.6 | 71 | 100.0 | 12 | |
| Moderate problems | 1.4 | 1 | 0.0 | 0 | |
| Severe problems | 0.0 | 0 | 0.0 | 0 | |
| Usual activities | 0.060 | ||||
| No problems | 83.3 | 60 | 58.3 | 7 | |
| Moderate problems | 16.7 | 12 | 41.7 | 5 | |
| Severe problems | 0.0 | 0 | 0.0 | 0 | |
| Pain/discomfort | 0.196 | ||||
| No problems | 40.3 | 29 | 16.7 | 2 | |
| Moderate problems | 52.8 | 38 | 75.0 | 9 | |
| Severe problems | 6.9 | 5 | 8.3 | 1 | |
| Anxiety/depression | 0.744 | ||||
| No problems | 66.7 | 48 | 58.3 | 7 | |
| Moderate problems | 29.2 | 21 | 41.7 | 5 | |
| Severe problems | 4.2 | 3 | 0.0 | 0 | |
| EQ-5Dindex mean (±SD) | 0.77 (±0.25) | 0.69 (±0.21) | 0.293 | ||
| EQVAS mean (±SD) | 74.0 (±18.1) 2 | 73.4 (±17.3) 3 | 0.908 | ||
| Employment Status and Timing for Return to Work | n (%) |
|---|---|
| Employment status before surgery, n = 84 | |
| Full time | 35 (41.7%) |
| Part time work | 6 (7.1%) |
| Full time sick leave | 3 (3.6%) |
| Sickness pension | 6 (7.1%) |
| Old-age pension | 34 (40.5%) |
| Employment status after surgery, n = 84 | |
| Full time | 35 (41.7%) |
| Part time work | 6 (7.1%) |
| Full time sick leave | 1 (1.2%) |
| Sickness pension | 3 (3.6%) |
| Old-age pension | 39 (46.4%) |
| Timing for return to work, n = 41 | |
| Return to full time work | |
| Within <3 months | 20 (48.9%) |
| From 3 to <6 months | 11 (26.8%) |
| From 6 to <12 months | 4 (9.6%) |
| ≥12 months | 0 (0.0%) |
| Return to part time work | |
| Within <3 months | 2 (4.9%) |
| From 3 to <6 months | 2 (4.9%) |
| From 6 to <12 months | 1 (2.4%) |
| ≥12 months | 1 (2.4%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pettersson-Segerlind, J.; von Vogelsang, A.-C.; Fletcher-Sandersjöö, A.; Tatter, C.; Mathiesen, T.; Edström, E.; Elmi-Terander, A. Health-Related Quality of Life and Return to Work after Surgery for Spinal Meningioma: A Population-Based Cohort Study. Cancers 2021, 13, 6371. https://doi.org/10.3390/cancers13246371
Pettersson-Segerlind J, von Vogelsang A-C, Fletcher-Sandersjöö A, Tatter C, Mathiesen T, Edström E, Elmi-Terander A. Health-Related Quality of Life and Return to Work after Surgery for Spinal Meningioma: A Population-Based Cohort Study. Cancers. 2021; 13(24):6371. https://doi.org/10.3390/cancers13246371
Chicago/Turabian StylePettersson-Segerlind, Jenny, Ann-Christin von Vogelsang, Alexander Fletcher-Sandersjöö, Charles Tatter, Tiit Mathiesen, Erik Edström, and Adrian Elmi-Terander. 2021. "Health-Related Quality of Life and Return to Work after Surgery for Spinal Meningioma: A Population-Based Cohort Study" Cancers 13, no. 24: 6371. https://doi.org/10.3390/cancers13246371
APA StylePettersson-Segerlind, J., von Vogelsang, A.-C., Fletcher-Sandersjöö, A., Tatter, C., Mathiesen, T., Edström, E., & Elmi-Terander, A. (2021). Health-Related Quality of Life and Return to Work after Surgery for Spinal Meningioma: A Population-Based Cohort Study. Cancers, 13(24), 6371. https://doi.org/10.3390/cancers13246371