
Prognostic Value of Routinely Measured Inflammatory Biomarkers in Older Cancer Patients: Pooled Analysis of Three Cohorts

 ,
,  , ,
, ,  , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
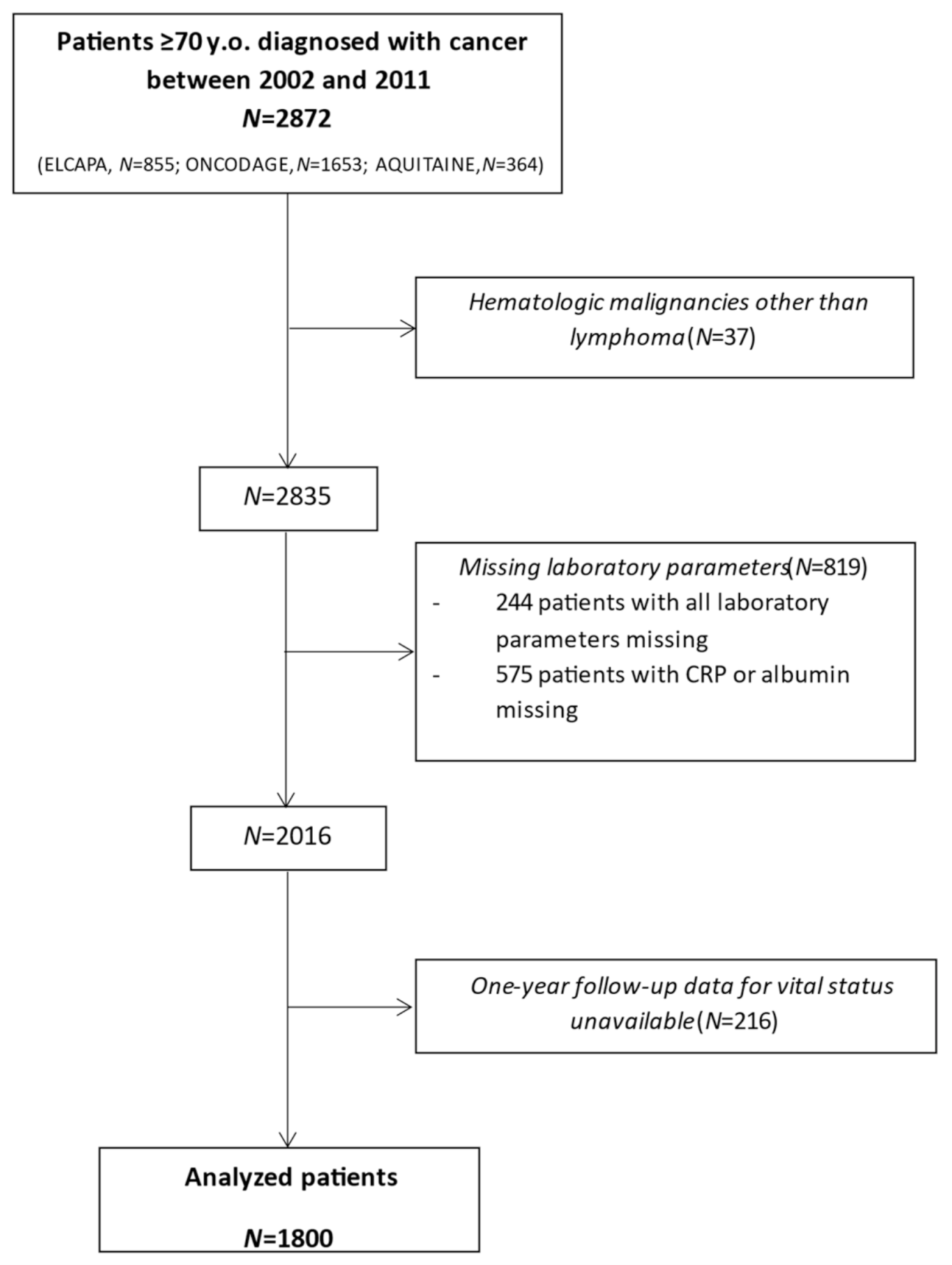
2.1. Study Design and Population
2.2. Ethical Considerations
2.3. Data Recorded
3. Endpoints
Statistical Analyses
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Amano, K.; Morita, T.; Tatara, R.; Katayama, H.; Uno, T.; Takagi, I. Association between early palliative care referrals, inpatient hospice utilization, and aggressiveness of care at the end of life. J. Palliat. Med. 2015, 18, 270–273. [Google Scholar] [CrossRef]
- Seaman, R.; Hohn, A.; Lindahl-Jacobsen, R.; Martikainen, P.; van Raalte, A.; Christensen, K. Rethinking morbidity compression. Eur. J. Epidemiol. 2020, 35, 381–388. [Google Scholar] [CrossRef]
- Canoui-Poitrine, F.; Lievre, A.; Dayde, F.; Lopez-Trabada-Ataz, D.; Baumgaertner, I.; Dubreuil, O.; Brunetti, F.; Coriat, R.; Maley, K.; Pernot, S.; et al. Inclusion of Older Patients with Cancer in Clinical Trials: The SAGE Prospective Multicenter Cohort Survey. Oncologist 2019, 24, e1351–e1359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenis, C.; Baitar, A.; Decoster, L.; De Greve, J.; Lobelle, J.P.; Flamaing, J.; Milisen, K.; Wildiers, H. The added value of geriatric screening and assessment for predicting overall survival in older patients with cancer. Cancer 2018, 124, 3753–3763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kenis, C.; Decoster, L.; Van Puyvelde, K.; De Greve, J.; Conings, G.; Milisen, K.; Flamaing, J.; Lobelle, J.P.; Wildiers, H. Performance of two geriatric screening tools in older patients with cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Tapia, C.; Paillaud, E.; Liuu, E.; Tournigand, C.; Ibrahim, R.; Fossey-Diaz, V.; Culine, S.; Canoui-Poitrine, F.; Audureau, E. Prognostic value of the G8 and modified-G8 screening tools for multidimensional health problems in older patients with cancer. Eur. J. Cancer 2017, 83, 211–219. [Google Scholar] [CrossRef]
- Min, L.; Yoon, W.; Mariano, J.; Wenger, N.S.; Elliott, M.N.; Kamberg, C.; Saliba, D. The vulnerable elders-13 survey predicts 5-year functional decline and mortality outcomes in older ambulatory care patients. J. Am. Geriatr. Soc. 2009, 57, 2070–2076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soubeyran, P.; Bellera, C.; Goyard, J.; Heitz, D.; Cure, H.; Rousselot, H.; Albrand, G.; Servent, V.; Jean, O.S.; van Praagh, I.; et al. Screening for vulnerability in older cancer patients: The ONCODAGE Prospective Multicenter Cohort Study. PLoS ONE 2014, 9, e115060. [Google Scholar] [CrossRef]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology consensus on geriatric assessment in older patients with cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef] [Green Version]
- Ferrat, E.; Paillaud, E.; Laurent, M.; Le Thuaut, A.; Caillet, P.; Tournigand, C.; Lagrange, J.L.; Canoui-Poitrine, F.; Bastuji-Garin, S.; Group, E.S. Predictors of 1-Year Mortality in a Prospective Cohort of Elderly Patients With Cancer. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2015, 70, 1148–1155. [Google Scholar] [CrossRef]
- Frasca, M.; Soubeyran, P.; Bellera, C.; Rainfray, M.; Leffondre, K.; Mathoulin-Pelissier, S. Alterations in comprehensive geriatric assessment decrease survival of elderly patients with cancer. Eur. J. Cancer 2018, 90, 10–18. [Google Scholar] [CrossRef]
- Hoppe, S.; Rainfray, M.; Fonck, M.; Hoppenreys, L.; Blanc, J.F.; Ceccaldi, J.; Mertens, C.; Blanc-Bisson, C.; Imbert, Y.; Cany, L.; et al. Functional decline in older patients with cancer receiving first-line chemotherapy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2013, 31, 3877–3882. [Google Scholar] [CrossRef] [PubMed]
- Boulahssass, R.; Gonfrier, S.; Ferrero, J.M.; Sanchez, M.; Mari, V.; Moranne, O.; Rambaud, C.; Auben, F.; Hannoun Levi, J.M.; Bereder, J.M.; et al. Predicting early death in older adults with cancer. Eur. J. Cancer 2018, 100, 65–74. [Google Scholar] [CrossRef] [PubMed]
- Brunello, A.; Fontana, A.; Zafferri, V.; Panza, F.; Fiduccia, P.; Basso, U.; Copetti, M.; Lonardi, S.; Roma, A.; Falci, C.; et al. Development of an oncological-multidimensional prognostic index (Onco-MPI) for mortality prediction in older cancer patients. J. Cancer Res. Clin. Oncol. 2016, 142, 1069–1077. [Google Scholar] [CrossRef] [Green Version]
- Kanesvaran, R.; Li, H.; Koo, K.N.; Poon, D. Analysis of prognostic factors of comprehensive geriatric assessment and development of a clinical scoring system in elderly Asian patients with cancer. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 3620–3627. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar] [CrossRef] [Green Version]
- Roxburgh, C.S.; McMillan, D.C. Role of systemic inflammatory response in predicting survival in patients with primary operable cancer. Future Oncol. 2010, 6, 149–163. [Google Scholar] [CrossRef]
- McMillan, D.C.; Watson, W.S.; O’Gorman, P.; Preston, T.; Scott, H.R.; McArdle, C.S. Albumin concentrations are primarily determined by the body cell mass and the systemic inflammatory response in cancer patients with weight loss. Nutr. Cancer 2001, 39, 210–213. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E.; Thomas, D.R.; Wilson, M.M. Cachexia: Pathophysiology and clinical relevance. Am. J. Clin. Nutr. 2006, 83, 735–743. [Google Scholar] [CrossRef] [Green Version]
- Colotta, F.; Allavena, P.; Sica, A.; Garlanda, C.; Mantovani, A. Cancer-related inflammation, the seventh hallmark of cancer: Links to genetic instability. Carcinogenesis 2009, 30, 1073–1081. [Google Scholar] [CrossRef] [Green Version]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Dunlop, D.J. Evaluation of cumulative prognostic scores based on the systemic inflammatory response in patients with inoperable non-small-cell lung cancer. Br. J. Cancer 2003, 89, 1028–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMillan, D.C.; Crozier, J.E.; Canna, K.; Angerson, W.J.; McArdle, C.S. Evaluation of an inflammation-based prognostic score (GPS) in patients undergoing resection for colon and rectal cancer. Int. J. Colorectal Dis. 2007, 22, 881–886. [Google Scholar] [CrossRef]
- Xu, H.J.; Ma, Y.; Deng, F.; Ju, W.B.; Sun, X.Y.; Wang, H. The prognostic value of C-reactive protein/albumin ratio in human malignancies: An updated meta-analysis. OncoTargets Ther. 2017, 10, 3059–3070. [Google Scholar] [CrossRef] [Green Version]
- Revythis, A.; Shah, S.; Kutka, M.; Moschetta, M.; Ozturk, M.A.; Pappas-Gogos, G.; Ioannidou, E.; Sheriff, M.; Rassy, E.; Boussios, S. Unraveling the Wide Spectrum of Melanoma Biomarkers. Diagnostics 2021, 11, 1341. [Google Scholar] [CrossRef] [PubMed]
- Caillet, P.; Canoui-Poitrine, F.; Vouriot, J.; Berle, M.; Reinald, N.; Krypciak, S.; Bastuji-Garin, S.; Culine, S.; Paillaud, E. Comprehensive geriatric assessment in the decision-making process in elderly patients with cancer: ELCAPA study. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2011, 29, 3636–3642. [Google Scholar] [CrossRef] [PubMed]
- Bellera, C.A.; Rainfray, M.; Mathoulin-Pelissier, S.; Mertens, C.; Delva, F.; Fonck, M.; Soubeyran, P.L. Screening older cancer patients: First evaluation of the G-8 geriatric screening tool. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2012, 23, 2166–2172. [Google Scholar] [CrossRef]
- Martinez-Tapia, C.; Canoui-Poitrine, F.; Bastuji-Garin, S.; Soubeyran, P.; Mathoulin-Pelissier, S.; Tournigand, C.; Paillaud, E.; Laurent, M.; Audureau, E. Optimizing the G8 Screening Tool for Older Patients With Cancer: Diagnostic Performance and Validation of a Six-Item Version. Oncologist 2016, 21, 188–195. [Google Scholar] [CrossRef] [Green Version]
- Hilden, J.; Glasziou, P. Regret graphs, diagnostic uncertainty and Youden’s Index. Stat. Med. 1996, 15, 969–986. [Google Scholar] [CrossRef]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Kerr, K.F.; Wang, Z.; Janes, H.; McClelland, R.L.; Psaty, B.M.; Pepe, M.S. Net reclassification indices for evaluating risk prediction instruments: A critical review. Epidemiology 2014, 25, 114–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pencina, M.J.; D’Agostino, R.B., Sr.; D’Agostino, R.B., Jr.; Vasan, R.S. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Stat. Med. 2008, 27, 157–172. [Google Scholar] [CrossRef]
- Pencina, M.J.; D’Agostino, R.B., Sr.; Steyerberg, E.W. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat. Med. 2011, 30, 11–21. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Guner, A.; Kim, S.Y.; Yu, J.E.; Min, I.K.; Roh, Y.H.; Roh, C.; Seo, W.J.; Cho, M.; Choi, S.; Choi, Y.Y.; et al. Parameters for Predicting Surgical Outcomes for Gastric Cancer Patients: Simple Is Better Than Complex. Ann. Surg. Oncol. 2018, 25, 3239–3247. [Google Scholar] [CrossRef]
- Dolan, R.D.; Lim, J.; McSorley, S.T.; Horgan, P.G.; McMillan, D.C. The role of the systemic inflammatory response in predicting outcomes in patients with operable cancer: Systematic review and meta-analysis. Sci. Rep. 2017, 7, 16717. [Google Scholar] [CrossRef]
- Dolan, R.D.; McSorley, S.T.; Horgan, P.G.; Laird, B.; McMillan, D.C. The role of the systemic inflammatory response in predicting outcomes in patients with advanced inoperable cancer: Systematic review and meta-analysis. Crit. Rev. Oncol. Hematol. 2017, 116, 134–146. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Ji, P.; Zhang, Z.; He, M. Predictive value of Glasgow prognostic score in patients with severe acute pancreatitis. Asian J. Surg. 2021, 44, 1427–1428. [Google Scholar] [CrossRef] [PubMed]
- Itagaki, T.; Motoki, H.; Otagiri, K.; Machida, K.; Takeuchi, T.; Kanai, M.; Kimura, K.; Higuchi, S.; Minamisawa, M.; Kitabayashi, H.; et al. Inflammation-based assessment for the risk stratification of mortality in patients with heart failure. Sci. Rep. 2021, 11, 14989. [Google Scholar] [CrossRef]
- Matsuo, H.; Yoshimura, Y.; Fujita, S.; Maeno, Y.; Tanaka, S. Role of systemic inflammation in functional recovery, dysphagia, and 1-y mortality in heart failure: A prospective cohort study. Nutrition 2021, 91–92, 111465. [Google Scholar] [CrossRef]
- Celik, A.I.; Bezgin, T.; Biteker, M. Predictive role of the modified Glasgow prognostic score for in-hospital mortality in stable acute pulmonary embolism. Med. Clínica 2021. [Google Scholar] [CrossRef] [PubMed]
- Kuluozturk, M.; Deveci, F. The Glasgow prognostic score can be a predictor of mortality in acute exacerbation of chronic obstructive pulmonary disease. Expert Rev. Respir. Med. 2020, 14, 521–525. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Tang, C.; Yu, J.; Ma, J.; Qiao, M.; Zhou, W.; Chen, Y.; Zhang, X. Combining C reactive protein and serum albumin to predict 90-day mortality in systemic lupus erythematosus with serious community-acquired infections. Lupus Sci. Med. 2021, 8, e000505. [Google Scholar] [CrossRef]
- Park, J.E.; Chung, K.S.; Song, J.H.; Kim, S.Y.; Kim, E.Y.; Jung, J.Y.; Kang, Y.A.; Park, M.S.; Kim, Y.S.; Chang, J.; et al. The C-Reactive Protein/Albumin Ratio as a Predictor of Mortality in Critically Ill Patients. J. Clin. Med. 2018, 7, 333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirashima, K.; Watanabe, M.; Shigaki, H.; Imamura, Y.; Ida, S.; Iwatsuki, M.; Ishimoto, T.; Iwagami, S.; Baba, Y.; Baba, H. Prognostic significance of the modified Glasgow prognostic score in elderly patients with gastric cancer. J. Gastroenterol. 2014, 49, 1040–1046. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, T.; Yamasaki, N.; Tsuchiya, T.; Matsumoto, K.; Kunizaki, M.; Taniguchi, D.; Nagayasu, T. Inflammation-based scoring is a useful prognostic predictor of pulmonary resection for elderly patients with clinical stage I non-small-cell lung cancer. Eur. J. Cardio-Thorac. Surg. Off. J. Eur. Assoc. Cardio-Thorac. Surg. 2015, 47, e140–e145. [Google Scholar] [CrossRef]
- Ohki, S.; Kase, K.; Chida, S.; Hayase, S.; Fujita, S.; Monma, T.; Takawa, M.; Kono, K.; Ohtake, T.; Takenoshita, S. Risk Evaluation and Prognostic Prediction of Colorectal Cancer in Elderly Patients Over 80 Years of Age. Gan Kagaku Ryoho. Cancer Chemother. 2016, 43, 1532–1534. [Google Scholar]
- Baitar, A.; Kenis, C.; Decoster, L.; De Greve, J.; Lobelle, J.P.; Flamaing, J.; Milisen, K.; Wildiers, H. The prognostic value of 3 commonly measured blood parameters and geriatric assessment to predict overall survival in addition to clinical information in older patients with cancer. Cancer 2018, 124, 3764–3775. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, T.; Yamasaki, N.; Tsuchiya, T.; Matsumoto, K.; Kunizaki, M.; Kamohara, R.; Hatachi, G.; Doi, R.; Obata, T.; Nagayasu, T. Ratio of C-reactive protein to albumin is a prognostic factor for operable non-small-cell lung cancer in elderly patients. Surg. Today 2017, 47, 836–843. [Google Scholar] [CrossRef]
- Canoui-Poitrine, F.; Zebachi, S.; Paillaud, E.; Chouaid, C.; Corre, R. Geriatric and oncological predictors of survival and chemotherapy toxicities in elderly patients with metastatic Non Small Cell Lung Cancer: An analysis of ESOGIA trial. In Proceedings of the 19th Conference of the International Society of Geriatric Oncology, Geneva, Switzerland, 14–16 November 2019. [Google Scholar]
- Audureau, E.; Soubeyran, P.-L.; Martinez-Tapia, C.; Bellera, C.A.; Bastuji-Garin, S.; Boudou-Rouquette, P.; Rainfray, M.; Chahwakilian, A.; Grellety, T.; Hanon, O.; et al. Using machine learning to predict mortality in older patients with cancer: Decision tree and random forest analyses from the ELCAPA and ONCODAGE prospective cohorts. J. Clin. Oncol. 2019, 37, 11516. [Google Scholar] [CrossRef]
- Retornaz, F.; Guillem, O.; Gholam, D.; Codoul, J.-F.; Brativesic, C.; Morvan, F.; Rinaldi, Y.; Barriere, N.; Nahon, S.; Butaud, C.; et al. Predicting chemotherapy toxicity and death in older adults with colon cancer: Results of MOST (Massilia Oncologic Senior Tests) study. J. Clin. Oncol. 2018, 36, 10041. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. (%) Total (n = 1800) | |
|---|---|
| Age, mean ± SD | 79 ± 6 |
| Female sex | 690 (38) |
| Tumor site | |
| Colon/rectum | 318 (18) |
| Pancreas | 52 (3) |
| Other digestive tract malignancies a | 74 (4) |
| Breast | 629 (35) |
| Prostate | 173 (10) |
| Other urinary tract malignancies b | 90 (5) |
| Lung and bronchial | 141 (8) |
| Head and neck | 62 (3) |
| Lymphoma | 205 (11) |
| Other cancers c | 56 (3) |
| Metastatic status (n = 1735) d | |
| M0 | 864 (50) |
| M1 | 502 (29) |
| Mx | 164 (9) |
| NA | 205 (12) |
| Social characteristics | |
| Living alone (n = 1793) | 719 (40) |
| Functional status | |
| ADL score ≤ 5 out of 6 (n = 1794) | 601 (34) |
| IADL score < 8 out of 8 (n = 1690) | 951 (56) |
| ECOG-PS ≥ 2 out of 4 (n = 1729) | 559 (32) |
| TGUG > 20 s (n = 1514) | 213 (14) |
| Malnutritione (n = 1774) | 1004 (57) |
| G8 score ≤ 14 (n = 1733) | 1225 (71) |
| Cognitive and emotional status | |
| MMSE < 24 out of 30 (n = 1687) | 371 (22) |
| GDS-15 ≥ 6 out of 15 or GDS4 ≥ 1 out of 4 (n = 1664) | 580 (35) |
| Comorbidity | |
| CIRS-G, median [IQR] (n = 1741) | 9 [6–13] |
| CIRS-G grade 3 or 4 (n = 1747) | 932 (53) |
| Renal insufficiency (Cockcroft-Gault, mL/min) (n = 1755) | |
| absent (clearance ≥ 60) | 831 (47) |
| moderate (30 ≤ clearance < 60) | 825 (47) |
| severe (clearance < 30) | 99 (6) |
| Inflammatory biomarkers | |
| CRP > 10 mg/L (n = 1800) | 716 (39.78) |
| CRP, median [IQR] (n = 1800) | 6 [2.70–27.25] |
| Albumin < 35 g/L (n = 1800) | 586 (33) |
| Albumin, median [IQR] (n = 1800) | 38.0 [33.00–42.00] |
| Prealbumin < 140 mg/L, (n = 1497) | 262 (18) |
| GPS (n = 1800) | |
| GPS = 0 | 921 (51) |
| GPS = 1 | 456 (25) |
| GPS = 2 | 423 (24) |
| mGPS (n = 1800) | |
| mGPS = 0 | 1084 (60) |
| mGPS = 1 | 293 (16) |
| mGPS = 2 | 423 (24) |
| CRP/albumin ratio > 0.215 (n = 1800) | 816 (45) |
| CRP/albumin ratio, median [IQR] (n = 1800) | 0.17 [0.07–0.80] |
| One-Year Survivors (n, %) n = 1294 | Deceased at One Year (n, %) n = 506 | Unadjusted Hazard Ratio [95% CI] | p | |
|---|---|---|---|---|
| Age, mean ± SD | 78 ± 5 | 80 ± 6 | 1.05 [1.04–1.07] | <0.001 |
| Female sex | 465 (36) | 225 (44) | 1.36 [1.14–1.62] | 0.001 |
| Tumor site | ||||
| Colorectal | 222 (17) | 96 (19) | 1.00 (ref) | <0.001 |
| Pancreas | 11 (1) | 41 (8) | 4.73 [3.28–6.83] | |
| Other digestive tract malignancies a | 35 (3) | 39 (8) | 2.03 [1.40–2.95] | |
| Breast | 572 (44) | 57 (11) | 0.26 [0.19–0.37] | |
| Prostate | 136 (11) | 37 (7) | 0.67 [0.46–0.99] | |
| Other urinary tract malignancies b | 44 (3) | 46 (9) | 1.99 [1.40–2.82] | |
| Lung and bronchial | 64 (5) | 77 (15) | 2.23 [1.65–3.01] | |
| Head and neck | 34 (3) | 28 (6) | 1.62 [1.06–2.46] | |
| Hematologic | 160 (12) | 45 (9) | 0.69 [0.48–0.98] | |
| Other cancers c | 16 (1) | 40 (8) | 3.41 [2.35–4.93] | |
| Metastatic status (n = 1735) | ||||
| M0 | 714 (57) | 150 (31) | 1.00 (ref) | <0.001 |
| M1 | 234 (19) | 268 (55) | 4.12 [3.37–5.04] | |
| Mx | 142 (11) | 22 (5) | 0.76 [0.49–1.20] | |
| NA | 160 (13) | 45 (9) | 1.31 [0.94–1.83] | |
| ECOG-PS ≥ 2 out of 4 | 258 (21) | 301 (62) | 4.84 [4.03–5.82] | <0.001 |
| G8 score ≤ 14 | 797 (63) | 428 (92) | 5.62 [4.03–7.84] | <0.001 |
| Biomarkers | ||||
| CRP > 10 mg/L | 354 (27) | 362 (72) | 5.14 [4.24–6.24] | <0.001 |
| Albumin < 35 g/L | 268 (21) | 318 (63) | 4.92 [4.11–5.90] | <0.001 |
| GPS | ||||
| GPS = 0 | 837 (65) | 84 (17) | 1.00 (ref) | <0.001 |
| GPS = 1 | 292 (22) | 164 (32) | 4.54 [3.49–5.91] | |
| GPS = 2 | 165 (13) | 258 (51) | 10.82 [8.45–13.85] | |
| mGPS | ||||
| mGPS = 0 | 940 (73) | 144 (28) | 1.00 (ref) | <0.001 |
| mGPS = 1 | 189 (14) | 104 (21) | 3.00 [2.33–3.86] | |
| mGPS = 2 | 165 (13) | 258 (51) | 7.26 [5.92–8.92] | |
| CRP/albumin ratio > 0.215 | 414 (32) | 402 (79) | 6.29 [5.06–7.80] | <0.001 |
| Model | Harrell’s C [95% CI] | NRI+ [95% CI] | NRI− [95% CI] |
|---|---|---|---|
| Baseline model: age, sex, tumor site, metastatic status, ECOG-PS, G8 | 0.82 [0.80; 0.83] | - | - |
| Baseline model + GPS | 0.84 [0.82; 0.85] | 0.10 [0.02; 0.16] | 0.01 [−0.02; 0.09] |
| Baseline model + mGPS | 0.83 [0.82; 0.85] | 0.08 [−0.03; 0.14] | 0.01 [−0.03; 0.09] |
| Baseline model + CRP | 0.83 [0.82; 0.85] | 0.11 [−0.01; 0.15] | −0.01 [−0.05; 0.09] |
| Baseline model + albumin | 0.83 [0.81; 0.85] | 0.07 [−0.04; 0.13] | 0.00 [−0.04; 0.09] |
| Baseline model + CRP/albumin ratio | 0.83 [0.82; 0.85] | 0.14 [0.02; 0.17] | −0.01 [−0.05; 0.08] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oubaya, N.; Soubeyran, P.; Reinald, N.; Fonck, M.; Allain, M.; Zebachi, S.; Heitz, D.; Laurent, M.; Delattre, C.; Caillet, P.; et al. Prognostic Value of Routinely Measured Inflammatory Biomarkers in Older Cancer Patients: Pooled Analysis of Three Cohorts. Cancers 2021, 13, 6154. https://doi.org/10.3390/cancers13246154
Oubaya N, Soubeyran P, Reinald N, Fonck M, Allain M, Zebachi S, Heitz D, Laurent M, Delattre C, Caillet P, et al. Prognostic Value of Routinely Measured Inflammatory Biomarkers in Older Cancer Patients: Pooled Analysis of Three Cohorts. Cancers. 2021; 13(24):6154. https://doi.org/10.3390/cancers13246154
Chicago/Turabian StyleOubaya, Nadia, Pierre Soubeyran, Nicoleta Reinald, Marianne Fonck, Mylène Allain, Sonia Zebachi, Damien Heitz, Marie Laurent, Cécile Delattre, Philippe Caillet, and et al. 2021. "Prognostic Value of Routinely Measured Inflammatory Biomarkers in Older Cancer Patients: Pooled Analysis of Three Cohorts" Cancers 13, no. 24: 6154. https://doi.org/10.3390/cancers13246154
APA StyleOubaya, N., Soubeyran, P., Reinald, N., Fonck, M., Allain, M., Zebachi, S., Heitz, D., Laurent, M., Delattre, C., Caillet, P., Dauba, J., Bastuji-Garin, S., Albrand, G., Bringuier, M., Rainfray, M., Brain, E., Grellety, T., Paillaud, E., Mathoulin-Pélissier, S., ... Canouï-Poitrine, F. (2021). Prognostic Value of Routinely Measured Inflammatory Biomarkers in Older Cancer Patients: Pooled Analysis of Three Cohorts. Cancers, 13(24), 6154. https://doi.org/10.3390/cancers13246154