
Her2 Expression in Circulating Tumor Cells Is Associated with Poor Outcomes in Patients with Metastatic Castration-Resistant Prostate Cancer

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Design
2.3. CTC Isolation and Detection
2.4. CTC-Based HER2 and AR-V7 Detection
2.5. Statistical Analyses
3. Results
3.1. Patients Characteristics According to HER2 Status
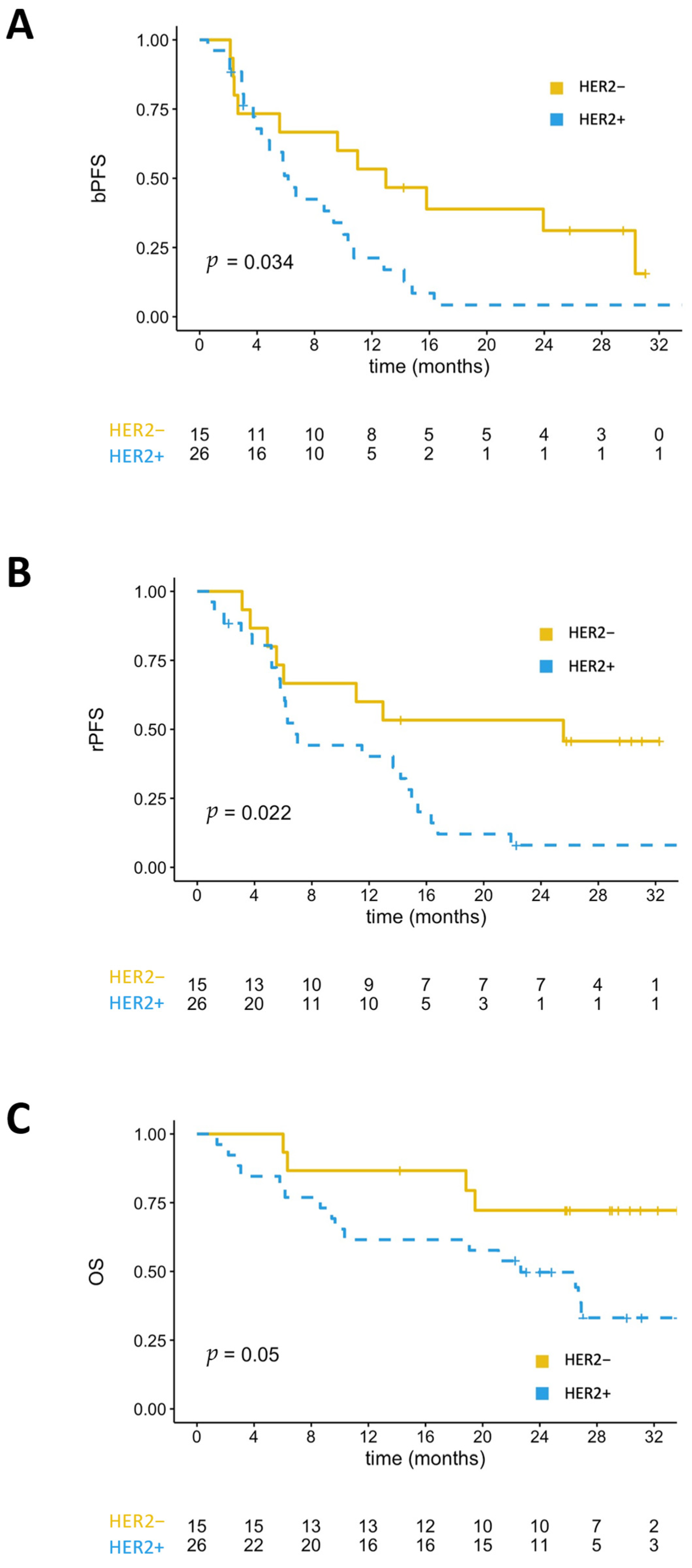
3.2. Clinical Outcomes According to HER2 Status
3.3. Survival Outcomes According to the Detection of CTCs
3.4. Adjusted Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parker, C.; Castro, E.; Fizazi, K.; Heidenreich, A.; Ost, P.; Procopio, G. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1119–1134. [Google Scholar] [CrossRef] [PubMed]
- Buttigliero, C.; Tucci, M.; Bertaglia, V.; Vignani, F.; Bironzo, P.; Di Maio, M.; Scagliotti, G.V. Understanding and overcoming the mechanisms of primary and acquired resistance to abiraterone and enzalutamide in castration resistant prostate cancer. Cancer Treat. Rev. 2015, 41, 884–892. [Google Scholar] [CrossRef]
- Edwards, J.; Traynor, P.; Munro, A.F.; Pirret, C.F.; Dunne, B.; Bartlett, J.M.S. The role of HER1-HER4 and EGFRvIII in hormone-refractory prostate cancer. Clin. Cancer Res. 2006, 12, 123–130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, Y.; Hu, M.C.T.; Makino, K.; Spohn, B.; Bartholomeusz, G.; Yan, D.H.; Hung, M.C. HER-2/neu promotes androgen-independent survival and growth of prostate cancer cells through the Akt pathway. Cancer Res. 2000, 60, 6841–6845. [Google Scholar] [PubMed]
- Li, T.-G.J.; Ghazaryan, D.; Shu, S.; Wu, L. ERBB2 Increases Metastatic Potentials Specifically in Androgen-Insensitive Prostate Cancer Cells. PLoS ONE 2014, 9, e99525. [Google Scholar] [CrossRef] [Green Version]
- Carles, J.; Lloreta, J.; Salido, M.; Font, A.; Suarez, M.; Baena, V.; Nogue, M.; Domenech, M.; Fabregat, X. Her-2/neu expression in prostate cancer: A dynamic process? Clin. Cancer Res. 2004, 10, 4742–4745. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gregory, C.W.; Whang, Y.E.; McCall, W.; Fei, X.; Liu, Y.; Ponguta, L.A.; French, F.S.; Wilson, E.M.; Earp, H.S. Heregulin-induced activation of HER2 and HER3 increases androgen receptor transactivation and CWR-R1 human recurrent prostate cancer cell growth. Clin. Cancer Res. 2005, 11, 1704–1712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minner, S.; Jessen, B.; Stiedenroth, L.; Burandt, E.; Köllermann, J.; Mirlacher, M.; Erbersdobler, A.; Eichelberg, C.; Fisch, M.; Brümmendorf, T.H.; et al. Low level Her2 overexpression is associated with rapid tumor cell proliferation and poor prognosis in prostate cancer. Clin. Cancer Res. 2010, 16, 1553–1560. [Google Scholar] [CrossRef] [Green Version]
- Montironi, R.; Mazzucchelli, R.; Barbisan, F.; Stramazzotti, D.; Santinelli, A.; Scarpelli, M.; Lòpez Beltran, A. HER2 expression and gene amplification in pT2a Gleason score 6 prostate cancer incidentally detected in cystoprostatectomies: Comparison with clinically detected androgen-dependent and androgen-independent cancer. Hum. Pathol. 2006, 37, 1137–1144. [Google Scholar] [CrossRef]
- Day, K.C.; Hiles, G.L.; Kozminsky, M.; Dawsey, S.J.; Paul, A.; Broses, L.J.; Shah, R.; Kunja, L.P.; Hall, C.; Palanisamy, N.; et al. HER2 and EGFR overexpression support metastatic progression of prostate cancer to bone. Cancer Res. 2017, 77, 74–85. [Google Scholar] [CrossRef] [Green Version]
- Scher, H.I.; Morris, M.J.; Stadler, W.M.; Higano, C.; Basch, E.; Fizazi, K.; Antonarakis, E.S.; Beer, T.M.; Carducci, M.A.; Chi, K.N.; et al. Trial Design and Objectives for Castration-Resistant Prostate Cancer: Updated Recommendations from the Prostate Cancer Clinical Trials Working Group 3. J. Clin. Oncol. 2016, 34, 1402–1418. [Google Scholar] [CrossRef] [Green Version]
- Maillet, D.; Allioli, N.; Peron, J.; Plesa, A.; Decaussin-Petrucci, M.; Tartas, S.; Ruffion, A.; Crouzet, S.; Rimokh, R.; Gillet, P.-G.; et al. Improved Androgen Receptor Splice Variant 7 Detection Using a Highly Sensitive Assay to Predict Resistance to Abiraterone or Enzalutamide in Metastatic Prostate Cancer Patients. Eur. Urol. Oncol. 2019. [Google Scholar] [CrossRef] [Green Version]
- Antonarakis, E.S.; Lu, C.; Wang, H.; Luber, B.; Nakazawa, M.; Roeser, J.C.; Chen, Y.; Mohammad, T.A.; Chen, Y.; Fedor, H.L.; et al. AR-V7 and resistance to enzalutamide and abiraterone in prostate cancer. N. Engl. J. Med. 2014, 371, 1028–1038. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, N.P.; Reyes, E.; Fuentealba, C.; Jacob, O.; Orellana, N. Possible role of HER-2 in the progression of prostate cancer from primary tumor to androgen independence. Asian Pacific J. Cancer Prev. 2015, 16, 6615–6619. [Google Scholar] [CrossRef] [Green Version]
- O’Hara, S.M.; Moreno, J.G.; Zweitzig, D.R.; Gross, S.; Gomella, L.G.; Terstappen, L.W.M.M. Multigene reverse transcription-PCR profiling of circulating tumor cells in hormone-refractory prostate cancer. Clin. Chem. 2004, 50, 826–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ady, N.; Morat, L.; Fizazi, K.; Soria, J.C.; Mathieu, M.C.; Prapotnich, D.; Sabatier, L.; Chauveinc, L. Detection of HER-2/neu-positive circulating epithelial cells in prostate cancer patients. Br. J. Cancer 2004, 90, 443–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Josefsson, A.; Larsson, K.; Månsson, M.; Björkman, J.; Rohlova, E.; Åhs, D.; Brisby, H.; Damber, J.E.; Welén, K. Circulating tumor cells mirror bone metastatic phenotype in prostate cancer. Oncotarget 2018, 9, 29403–29413. [Google Scholar] [CrossRef] [PubMed]
- Fantinato, A.P.; Tobias-Machado, M.; Fonseca, F.; Pinto, J.L.F.; Wroclawski, M.L.; Wroclawski, E.; Verotti, M.; Del Giglio, A. Her2/neu expression by reverse transcriptase-polymerase chain reaction in the peripheral blood of prostate cancer patients. Tumori 2007, 93, 467–472. [Google Scholar] [CrossRef] [PubMed]
- Domingo-Domenech, J.; Fernandez, P.L.; Filella, X.; Martinez-Fernandez, A.; Molina, R.; Fernandez, E.; Alcaraz, A.; Codony, J.; Gascon, P.; Mellado, B. Serum HER2 extracellular domain predicts an aggressive clinical outcome and biological PSA response in hormone-independent prostate cancer patients treated with docetaxel. Ann. Oncol. 2008, 19, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Tambo, M.; Higashihara, E.; Terado, Y.; Nutahara, K.; Okegawa, T. Comparison of serum HER2/neu with immunohistochemical HER2/neu expression for the prediction of biochemical progression in metastatic prostate cancer. Int. J. Urol. 2009, 16, 369–374. [Google Scholar] [CrossRef] [PubMed]
- Okegawa, T.; Kinjo, M.; Nutahara, K.; Higashihara, E. Pretreatment serum level of HER2/nue as a prognostic factor in metastatic prostate cancer patients about to undergo endocrine therapy. Int. J. Urol. 2006, 13, 1197–1201. [Google Scholar] [CrossRef]
- Yeo, S.K.; Wen, J.; Chen, S.; Guan, J.L. Autophagy differentially regulates distinct breast cancer stem-like cells in murine models via EGFR/Stat3 and Tgfβ/Smad signaling. Cancer Res. 2016, 76, 3397–3410. [Google Scholar] [CrossRef] [Green Version]
- Le Page, C.; Koumakpayi, I.H.; Péant, B.; Delvoye, N.; Saad, F.; Mes-Masson, A.M. ErbB2/Her-2 regulates the expression of Akt2 in prostate cancer cells. Prostate 2012, 72, 777–788. [Google Scholar] [CrossRef]
- Festuccia, C.; Gravina, G.L.; Muzi, P.; Pomante, R.; Ventura, L.; Vessella, R.L.; Vicentini, C.; Bologna, M. Bicalutamide increases phospho-Akt levels through Her2 in patients with prostate cancer. Endocr. Relat. Cancer 2007, 14, 601–611. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.; Ye, H.; Gerrin, S.; Wang, H.; Sharma, A.; Chen, S.; Patnaik, A.; Sowalsky, A.G.; Voznesensky, O.; Han, W.; et al. ErbB2 Signaling Increases Androgen Receptor Expression in Abiraterone-Resistant Prostate Cancer Analysis and interpretation of data: HHS Public Access. Clin. Cancer Res. 2016, 22, 3672–3682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, H.K.; Hu, Y.C.; Yang, L.; Altuwaijri, S.; Chen, Y.T.; Kang, H.Y.; Chang, C. Suppression Versus Induction of Androgen Receptor Functions by the Phosphatidylinositol 3-Kinase/Akt Pathway in Prostate Cancer LNCaP Cells with Different Passage Numbers. J. Biol. Chem. 2003, 278, 50902–50907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varisli, L.; Gonen-Korkmaz, C.; Syed, H.M.; Bogurcu, N.; Debelec-Butuner, B.; Erbaykent-Tepedelen, B.; Korkmaz, K.S. Androgen regulated HN1 leads proteosomal degradation of androgen receptor (AR) and negatively influences AR mediated transactivation in prostate cells. Mol. Cell. Endocrinol. 2012, 350, 107–117. [Google Scholar] [CrossRef] [PubMed]
- Muniyan, S.; Chen, S.J.; Lin, F.F.; Wang, Z.; Mehta, P.P.; Batra, S.K.; Lin, M.F. ErbB-2 signaling plays a critical role in regulating androgen-sensitive and castration-resistant androgen receptor-positive prostate cancer cells. Cell. Signal. 2015, 27, 2261–2271. [Google Scholar] [CrossRef] [Green Version]
- Der Chuang, T.; Chen, S.J.; Lin, F.F.; Veeramani, S.; Kumar, S.; Batra, S.K.; Tu, Y.; Lin, M.F. Human prostatic acid phosphatase, an authentic tyrosine phosphatase, dephosphorylates ErbB-2 and regulates prostate cancer cell growth. J. Biol. Chem. 2010, 285, 23598–23606. [Google Scholar] [CrossRef] [Green Version]
- Recchia, A.G.; Musti, A.M.; Lanzino, M.; Panno, M.L.; Turano, E.; Zumpano, R.; Belfiore, A.; Andò, S.; Maggiolini, M. A cross-talk between the androgen receptor and the epidermal growth factor receptor leads to p38MAPK-dependent activation of mTOR and cyclinD1 expression in prostate and lung cancer cells. Int. J. Biochem. Cell Biol. 2009, 41, 603–614. [Google Scholar] [CrossRef] [PubMed]
- Whang, Y.E.; Armstrong, A.J.; Rathmell, W.K.; Godley, P.A.; Kim, W.Y.; Pruthi, R.S.; Wallen, E.M.; Crane, J.M.; Moore, D.T.; Grigson, G.; et al. A phase II study of lapatinib, a dual EGFR and HER-2 tyrosine kinase inhibitor, in patients with castration-resistant prostate cancer. Urol. Oncol. Semin. Orig. Investig. 2013, 31, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Jathal, M.K.; Steele, T.M.; Siddiqui, S.; Mooso, B.A.; D’abronzo, L.S.; Drake, C.M.; Whang, Y.E.; Ghosh, P.M. Dacomitinib, but not lapatinib, suppressed progression in castration-resistant prostate cancer models by preventing HER2 increase. Br. J. Cancer 2019, 121, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Shiota, M.; Bishop, J.L.; Takeuchi, A.; Nip, K.M.; Cordonnier, T.; Beraldi, E.; Kuruma, H.; Gleave, M.E.; Zoubeidi, A. Inhibition of the HER2−YB1-AR axis with lapatinib synergistically enhances enzalutamide anti-tumor efficacy in castration resistant prostate cancer. Oncotarget 2015, 6, 9086–9098. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Characteristic | CTC HER2+ (n = 26) | CTC HER2− (n = 15) | p-Value | Total (n = 41) |
|---|---|---|---|---|
| Median age (years) | 76 | 74.7 | 0.27 | 73 |
| Gleason sum ≥ 8 at diagnosis (%) | 14 (54%) | 9 (60%) | 0.75 | 23 (56%) |
| M1 disease at PCa diagnosis (%) | 9 (35%) | 3 (20%) | 0.45 | 12 (29%) |
| Previous local treatment (%) - Radical prostatectomy alone or with salvage or adjuvant radiotherapy - Radiotherapy alone - Other | 17 (65%) 9 (35%) 7 (27%) 1 (4%) | 11 (73%) 6 (40%) 5 (33%) 0 (0%) | 0.73 - - - | 28 (68%) 15 (37%) 12(29%) 1 (2%) |
| Time to castration resistance <1 year (%) | 14 (54%) | 1 (7%) | 0.003 | 15 (37%) |
| Presence of pain (%) | 11 (42%) | 5 (33%) | 1.0 | 16 (39%) |
| Prior treatment before subsequent treatment initiation (%) - 1 line - ≥2 lines | 11 (42%) 4 (15%) 7 (27%) | 5 (33%) 1 (7%) 4 (27%) | 0.76 | 16 (39%) 5 (12%) 11 (27%) |
| Prior treatment with ARSI (%) | 5 (19%) | 5 (33%) | 0.45 | 10 (24%) |
| Prior treatment with chemotherapy (%) | 9 (35%) | 4 (27%) | 0.72 | 13 (32%) |
| Presence of visceral metastases (%) | 5 (19%) | 4 (27%) | 0.70 | 9 (22%) |
| Presence of lymph node metastases (%) | 11 (42%) | 7 (47%) | 1.0 | 18 (44%) |
| Presence of bone metastases (%) | 24 (92%) | 12 (80%) | 0.34 | 36 (88%) |
| Median baseline PSA (ng/mL) | 69.9 | 28.3 | 0.27 | 35 |
| Median baseline CTC count on CellSearch (per 7.5 mL of blood) | 10 | 8 | 0.82 | 9 |
| Detection of CTCs (AdnaTest) | 23 (88%) | 9 (60%) | 0.052 | 32 (78%) |
| Detection of AR-V7 (AdnaPanel) | 16 (61%) | 7 (47%) | 0.51 | 23 (56%) |
| Type of subsequent therapy (%) - ARSI - Chemotherapy - None | 19 (73%) 6 (23%) 1 (4%) | 12 (80%) 3 (20%) 0 (0%) | - | 31 (75%) 9 (22%) 1 (2%) |
| Clinical Outcome | CTC HER2+ (n = 26) | CTC HER2− (n = 15) | p-Value |
|---|---|---|---|
| PSA response | 73% | 73% | - |
| Median PSA-PFS (months) | 6.2 | 13.0 | 0.034 * HR = 2.20 (95% CI, 1.0–4.6) |
| Median radiological-PFS (months) | 6.8 | 25.6 | 0.022 * HR = 2.55 (95% CI, 1.1–5.9) |
| Median overall-survival (months) | 22.7 | NR | 0.05 * HR = 2.85 (95% CI, 0.95–8.5) |
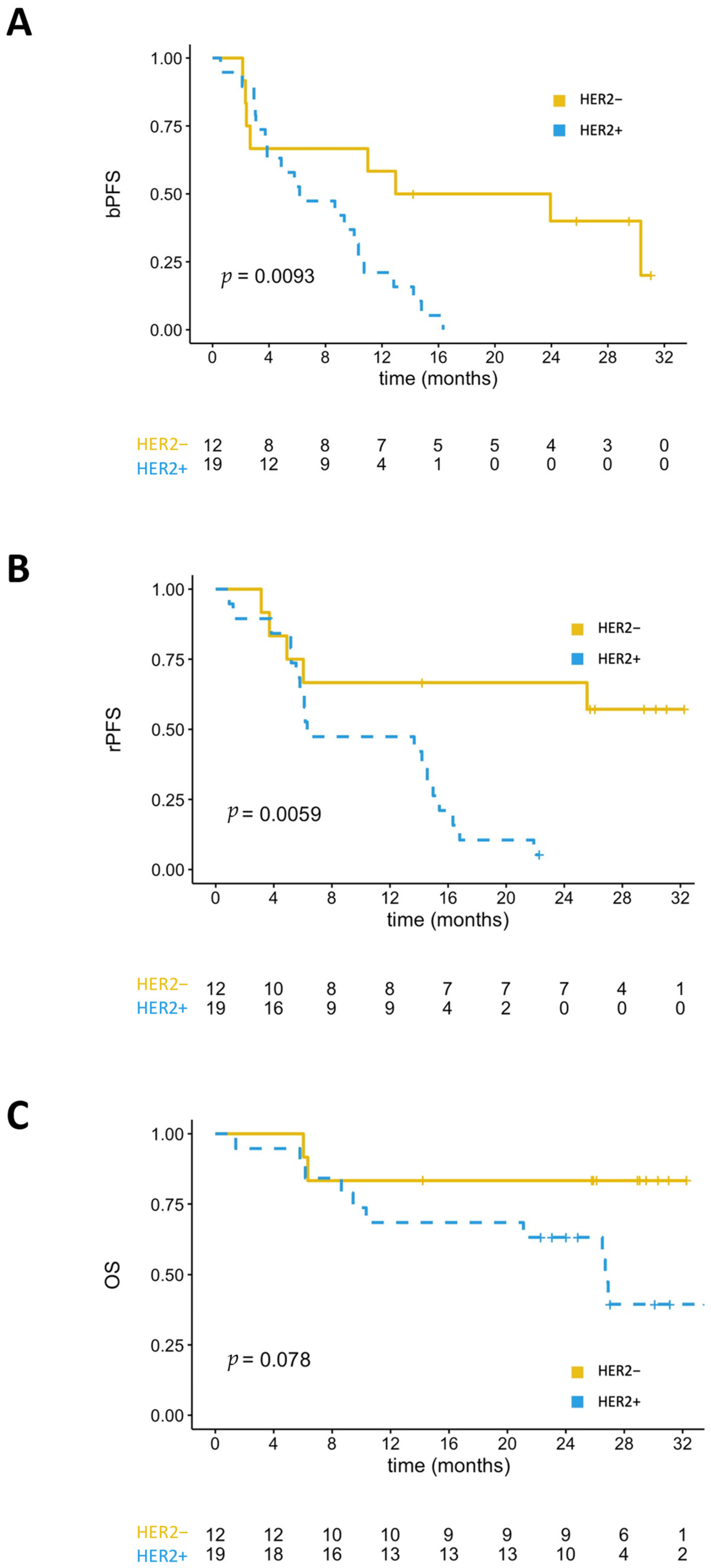
| Clinical Outcome | HER2+ (n = 19) | HER2− (n = 12) | p-Value |
|---|---|---|---|
| PSA response | 74% | 92% | - |
| Median PSA-PFS (months) | 6.2 | 18.5 | 0.009 * HR = 3.35 (95% CI, 1.3–8.7) |
| Median radiological-PFS months) | 6.3 | NR | 0.006 * HR = 4.26 (95% CI, 1.4–12.9) |
| Median overall-survival (months) | 22.7 | NR | 0.078 * HR = 3.59 (95% CI, 0.8–16.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maillet, D.; Allioli, N.; Péron, J.; Plesa, A.; Decaussin-Petrucci, M.; Tartas, S.; Sajous, C.; Ruffion, A.; Crouzet, S.; Freyer, G.; et al. Her2 Expression in Circulating Tumor Cells Is Associated with Poor Outcomes in Patients with Metastatic Castration-Resistant Prostate Cancer. Cancers 2021, 13, 6014. https://doi.org/10.3390/cancers13236014
Maillet D, Allioli N, Péron J, Plesa A, Decaussin-Petrucci M, Tartas S, Sajous C, Ruffion A, Crouzet S, Freyer G, et al. Her2 Expression in Circulating Tumor Cells Is Associated with Poor Outcomes in Patients with Metastatic Castration-Resistant Prostate Cancer. Cancers. 2021; 13(23):6014. https://doi.org/10.3390/cancers13236014
Chicago/Turabian StyleMaillet, Denis, Nathalie Allioli, Julien Péron, Adriana Plesa, Myriam Decaussin-Petrucci, Sophie Tartas, Christophe Sajous, Alain Ruffion, Sébastien Crouzet, Gilles Freyer, and et al. 2021. "Her2 Expression in Circulating Tumor Cells Is Associated with Poor Outcomes in Patients with Metastatic Castration-Resistant Prostate Cancer" Cancers 13, no. 23: 6014. https://doi.org/10.3390/cancers13236014