
Pre-Transplant Alpha-Fetoprotein > 25.5 and Its Dynamic on Waitlist Are Predictors of HCC Recurrence after Liver Transplantation for Patients Meeting Milan Criteria

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Data Collection
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patients Recipients
3.2. Donors
3.3. Histological Features of Explanted Livers
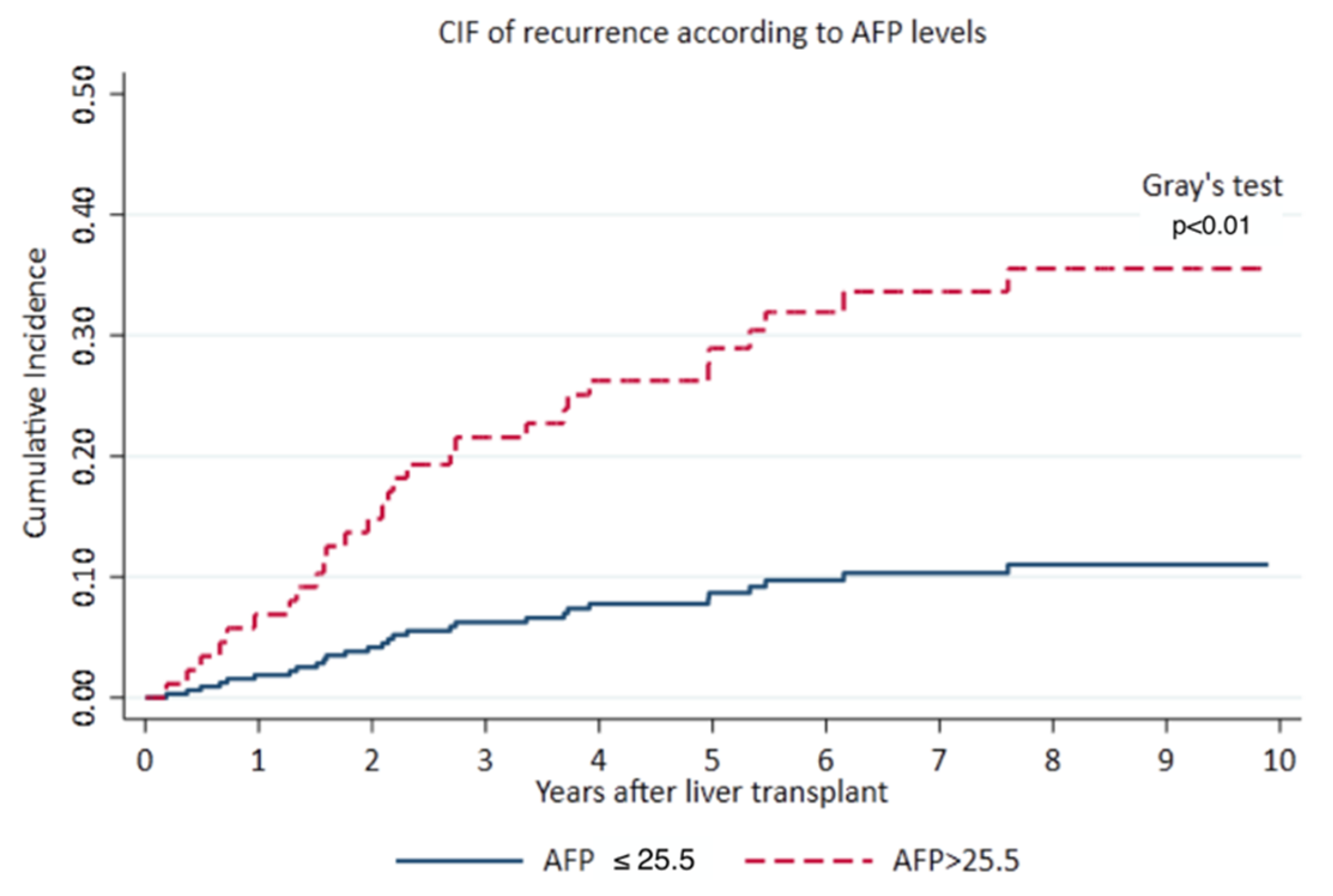
3.4. Primary Outcome
3.5. Patients with Increased AFP on Waitlist
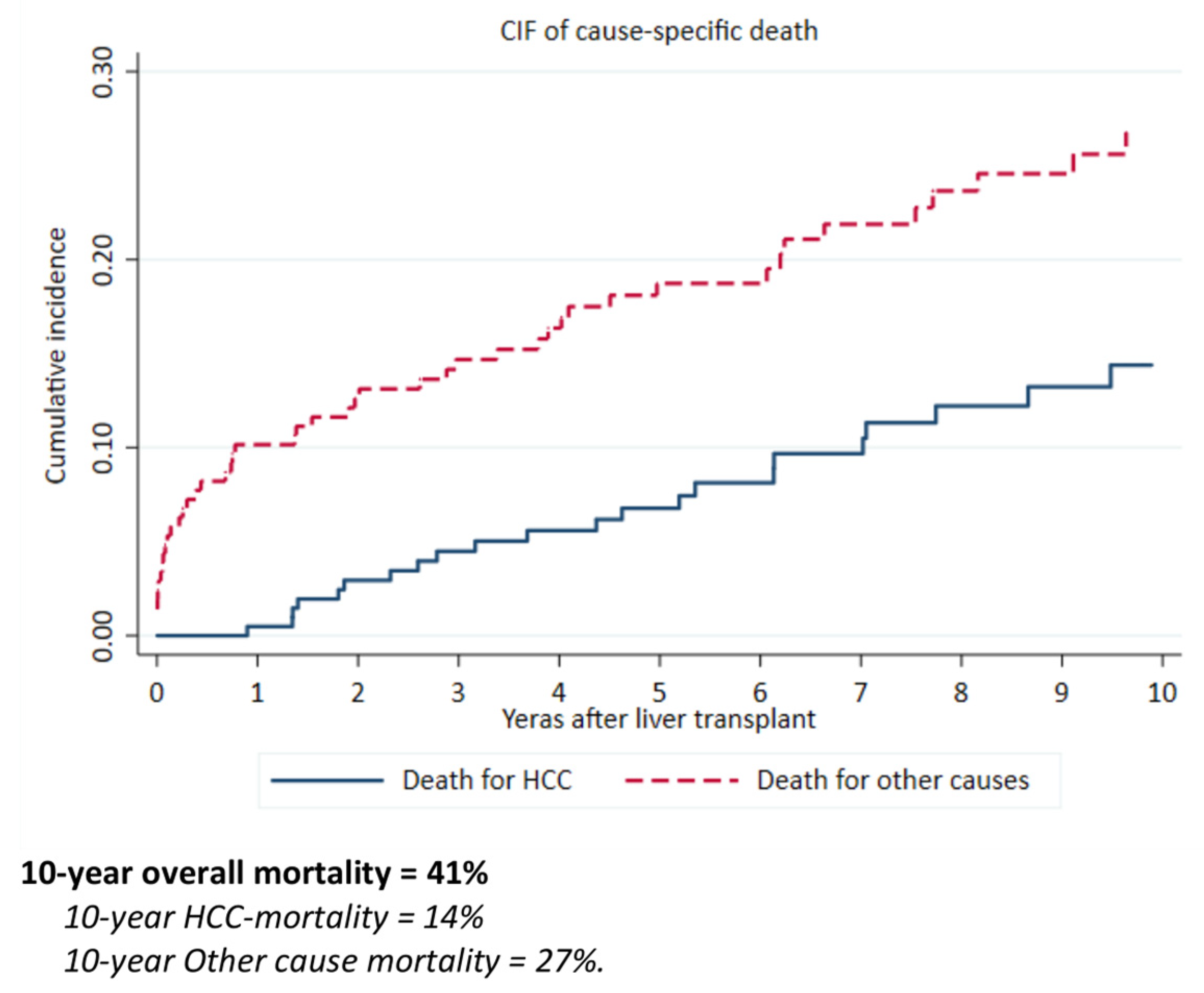
3.6. Secondary Outcomes
3.7. Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012: Globocan 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.J.; von Felden, J.; Garcia-Lezana, T.; Sarcognato, S.; Villanueva, A. Tumour evolution in hepatocellular carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 139–152. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver Transplantation for the Treatment of Small Hepatocellular Carcinomas in Patients with Cirrhosis. N. Engl. J. Med. 1996, 334, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Yao, F.Y.; Xiao, L.; Bass, N.M.; Kerlan, R.; Ascher, N.L.; Roberts, J.P. Liver Transplantation for Hepatocellular Carcinoma: Validation of the UCSF-Expanded Criteria Based on Preoperative Imaging. Am. J. Transplant. 2007, 7, 2587–2596. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.-Y. Up-to-seven criteria for hepatocellular carcinoma liver transplantation: A single center analysis. World J. Gastroenterol. 2013, 19, 6077. [Google Scholar] [CrossRef] [PubMed]
- Sapisochin, G.; Goldaracena, N.; Laurence, J.M.; Dib, M.; Barbas, A.; Ghanekar, A.; Cleary, S.P.; Lilly, L.; Cattral, M.S.; Marquez, M.; et al. The extended Toronto criteria for liver transplantation in patients with hepatocellular carcinoma: A prospective validation study. Hepatology 2016, 64, 2077–2088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takada, Y.; Uemoto, S. Liver transplantation for hepatocellular carcinoma: The Kyoto experience. J. Hepato-Biliary-Pancreat. Sci. 2010, 17, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Meguro, M.; Mizuguchi, T.; Nishidate, T.; Okita, K.; Ishii, M.; Ota, S.; Ueki, T.; Akizuki, E.; Hirata, K. Prognostic roles of preoperative α-fetoprotein and des-γ-carboxy prothrombin in hepatocellular carcinoma patients. World J. Gastroenterol. 2015, 21, 4933–4945. [Google Scholar] [CrossRef]
- Perricone, G.; Duvoux, C.; Berenguer, M.; Cortesi, P.A.; Vinaixa, C.; Facchetti, R.; Mazzarelli, C.; Rockenschaub, S.-R.; Martini, S.; Morelli, C.; et al. Delisting HCV-infected liver transplant candidates who improved after viral eradication: Outcome 2 years after delisting. Liver Int. 2018, 38, 2170–2177. [Google Scholar] [CrossRef] [PubMed]
- Au, K.P.; Chok, K.S.H. Multidisciplinary approach for post-liver transplant recurrence of hepatocellular carcinoma: A proposed management algorithm. World J. Gastroenterol. 2018, 24, 5081–5094. [Google Scholar] [CrossRef] [PubMed]
- Position Paper of the Italian Association for the Study of the Liver: The Multidisciplinary Clinical Approach to Hepatocellular Carcinoma-AISF-ASSOCIAZIONE ITALIANA STUDIO DEL FEGATO. Available online: https://www.webaisf.org/2013/03/11/position-paper-of-the-italian-association-for-the-study-of-the-liver-the-multidisciplinary-clinical-approach-to-hepatocellular-carcinoma/ (accessed on 9 October 2020).
- Verna, E.C.; Patel, Y.A.; Aggarwal, A.; Desai, A.P.; Frenette, C.; Pillai, A.A.; Salgia, R.; Seetharam, A.; Sharma, P.; Sherman, C.; et al. Liver transplantation for hepatocellular carcinoma: Management after the transplant. Am. J. Transplant. 2020, 20, 333–347. [Google Scholar] [CrossRef] [PubMed]
- Vagefi, P.A.; Dodge, J.L.; Yao, F.Y.; Roberts, J.P. Potential role of the donor in hepatocellular carcinoma recurrence after liver transplantation: DONOR FACTORS AND HCC RECURRENCE. Liver Transpl. 2015, 21, 187–194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, S.; Yoshida, A.; Facciuto, M.; Moonka, D.; Abouljoud, M.S.; Schwartz, M.E.; Florman, S.S. Ischemia time impacts recurrence of hepatocellular carcinoma after liver transplantation. Hepatology 2015, 61, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Orci, L.A.; Lacotte, S.; Oldani, G.; Slits, F.; De Vito, C.; Crowe, L.A.; Rubbia-Brandt, L.; Vallée, J.-P.; Morel, P.; Toso, C. Effect of ischaemic preconditioning on recurrence of hepatocellular carcinoma in an experimental model of liver steatosis. Br. J. Surg. 2016, 103, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Jonas, S. Vascular invasion and histopathologic grading determine outcome after liver transplantation for hepatocellular carcinoma in cirrhosis. Hepatology 2001, 33, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Perálvarez, M.; Tsochatzis, E.; Naveas, M.C.; Pieri, G.; García-Caparrós, C.; O’Beirne, J.; Poyato-González, A.; Ferrín-Sánchez, G.; Montero-Álvarez, J.L.; Patch, D.; et al. Reduced exposure to calcineurin inhibitors early after liver transplantation prevents recurrence of hepatocellular carcinoma. J. Hepatol. 2013, 59, 1193–1199. [Google Scholar] [CrossRef]
- Cucchetti, A.; Serenari, M.; Sposito, C.; Di Sandro, S.; Mosconi, C.; Vicentin, I.; Garanzini, E.; Mazzaferro, V.; De Carlis, L.; Golfieri, R.; et al. Including mRECIST in the Metroticket 2.0 criteria improves prediction of hepatocellular carcinoma-related death after liver transplant. J. Hepatol. 2020, 73, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Centonze, L.; Di Sandro, S.; Lauterio, A.; De Carlis, R.; Sgrazzutti, C.; Ciulli, C.; Vella, I.; Vicentin, I.; Incarbone, N.; Bagnardi, V.; et al. A retrospective single-centre analysis of the oncological impact of LI-RADS classification applied to Metroticket 2.0 calculator in liver transplantation: Every nodule matters. Transpl. Int. 2021, 34, 1712–1721. [Google Scholar] [CrossRef]
- Vivarelli, M.; Cucchetti, A.; Piscaglia, F.; La Barba, G.; Bolondi, L.; Cavallari, A.; Pinna, A.D. Analysis of risk factors for tumor recurrence after liver transplantation for hepatocellular carcinoma: Key role of immunosuppression. Liver Transpl. 2005, 11, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Guba, M.; von Breitenbuch, P.; Steinbauer, M.; Koehl, G.; Flegel, S.; Hornung, M.; Bruns, C.J.; Zuelke, C.; Farkas, S.; Anthuber, M.; et al. Rapamycin inhibits primary and metastatic tumor growth by antiangiogenesis: Involvement of vascular endothelial growth factor. Nat. Med. 2002, 8, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.X.; Abrams, T.A.; Miksad, R.; Blaszkowsky, L.S.; Meyerhardt, J.A.; Zheng, H.; Muzikansky, A.; Clark, J.W.; Kwak, E.L.; Schrag, D.; et al. Phase 1/2 study of everolimus in advanced hepatocellular carcinoma. Cancer 2011, 117, 5094–5102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma: Heimbach et al. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serum Alpha-Fetoprotein in the Early Stage of Human Hepatocellular Carcinoma-PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/6201411/ (accessed on 9 October 2020).
- Ryder, S.D. British Society of Gastroenterology Guidelines for the diagnosis and treatment of hepatocellular carcinoma (HCC) in adults. Gut 2003, 52 (Suppl. 3), iii1–iii8. [Google Scholar] [CrossRef] [Green Version]
- Llovet, J.M.; Brú, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Jha, R.C.; Mitchell, D.G.; Weinreb, J.C.; Santillan, C.S.; Yeh, B.M.; Francois, R.; Sirlin, C.B. LI-RADS categorization of benign and likely benign findings in patients at risk of hepatocellular carcinoma: A pictorial atlas. Am. J. Roentgenol. 2014, 203, W48–W69. [Google Scholar] [CrossRef] [Green Version]
- Zhou, L.; Rui, J.-A.; Ye, D.-X.; Wang, S.-B.; Chen, S.-G.; Qu, Q. Edmondson-Steiner grading increases the predictive efficiency of TNM staging for long-term survival of patients with hepatocellular carcinoma after curative resection. World J. Surg. 2008, 32, 1748–1756. [Google Scholar] [CrossRef] [PubMed]
- Vivarelli, M.; Cucchetti, A.; Barba, G.L.; Ravaioli, M.; Del Gaudio, M.; Lauro, A.; Grazi, G.L.; Pinna, A.D. Liver Transplantation for Hepatocellular Carcinoma Under Calcineurin Inhibitors: Reassessment of Risk Factors for Tumor Recurrence. Ann. Surg. 2008, 248, 857–862. [Google Scholar] [CrossRef] [PubMed]
- Duvoux, C.; Roudot–Thoraval, F.; Decaens, T.; Pessione, F.; Badran, H.; Piardi, T.; Francoz, C.; Compagnon, P.; Vanlemmens, C.; Dumortier, J.; et al. Liver Transplantation for Hepatocellular Carcinoma: A Model Including α-Fetoprotein Improves the Performance of Milan Criteria. Gastroenterology 2012, 143, 986–994.e3. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Heimbach, J.; Harnois, D.M.; Sapisochin, G.; Dodge, J.L.; Lee, D.; Burns, J.M.; Sanchez, W.; Greig, P.D.; Grant, D.R.; et al. Validation of a Risk Estimation of Tumor Recurrence After Transplant (RETREAT) Score for Hepatocellular Carcinoma Recurrence After Liver Transplant. JAMA Oncol. 2017, 3, 493. [Google Scholar] [CrossRef] [PubMed]
- De Giorgio, M.; Vezzoli, S.; Cohen, E.; Armellini, E.; Lucà, M.G.; Verga, G.; Pinelli, D.; Nani, R.; Valsecchi, M.G.; Antolini, L.; et al. Prediction of progression-free survival in patients presenting with hepatocellular carcinoma within the Milan criteria: Prediction of Progression-Free Survival. Liver Transpl. 2010, 16, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V. Squaring the circle of selection and allocation in liver transplantation for HCC: An adaptive approach. Hepatology 2016, 63, 1707–1717. [Google Scholar] [CrossRef] [Green Version]
- Di Sandro, S.; Bagnardi, V.; Cucchetti, A.; Lauterio, A.; De Carlis, R.; Benuzzi, L.; Danieli, M.; Botta, F.; Centonze, L.; Najjar, M.; et al. From a Philosophical Framework to a Valid Prognostic Staging System of the New “Comprehensive Assessment” for Transplantable Hepatocellular Carcinoma. Cancers 2019, 11, 741. [Google Scholar] [CrossRef] [Green Version]
- Geissler, E.K.; Schnitzbauer, A.A.; Zülke, C.; Lamby, P.E.; Proneth, A.; Duvoux, C.; Burra, P.; Jauch, K.-W.; Rentsch, M.; Ganten, T.M.; et al. Sirolimus Use in Liver Transplant Recipients With Hepatocellular Carcinoma: A Randomized, Multicenter, Open-Label Phase 3 Trial. Transplantation 2016, 100, 116–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahmud, N.; John, B.; Taddei, T.H.; Goldberg, D.S. Pre-transplant alpha-fetoprotein is associated with post-transplant hepatocellular carcinoma recurrence mortality. Clin. Transpl. 2019, 33. [Google Scholar] [CrossRef] [PubMed]
- Koch, C.; Bette, T.; Waidmann, O.; Filmann, N.; Schrecker, C.; Trojan, J.; Weiler, N.; Vermehren, J.; Schnitzbauer, A.A.; Bechstein, W.O.; et al. AFP ratio predicts HCC recurrence after liver transplantation. PLoS ONE 2020, 15, e0235576. [Google Scholar] [CrossRef]
- Hameed, B.; Mehta, N.; Sapisochin, G.; Roberts, J.P.; Yao, F.Y. Alpha-fetoprotein level > 1000 ng/mL as an exclusion criterion for liver transplantation in patients with hepatocellular carcinoma meeting the Milan criteria. Liver Transpl. 2014, 20, 945–951. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Dodge, J.L.; Grab, J.D.; Yao, F.Y. National Experience on Down-Staging of Hepatocellular Carcinoma Before Liver Transplant: Influence of Tumor Burden, Alpha-Fetoprotein, and Wait Time. Hepatology 2020, 71, 943–954. [Google Scholar] [CrossRef]
- Halazun, K.J.; Rosenblatt, R.E.; Mehta, N.; Lai, Q.; Hajifathalian, K.; Gorgen, A.; Brar, G.; Sasaki, K.; Doyle, M.B.M.; Tabrizian, P.; et al. Dynamic α-Fetoprotein Response and Outcomes After Liver Transplant for Hepatocellular Carcinoma. JAMA Surg. 2021, 156, 559. [Google Scholar] [CrossRef]
- Clavien, P.-A.; Lesurtel, M.; Bossuyt, P.M.M.; Gores, G.J.; Langer, B.; Perrier, A. OLT for HCC Consensus Group Recommendations for liver transplantation for hepatocellular carcinoma: An international consensus conference report. Lancet Oncol. 2012, 13, e11–e22. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Recurrence | p * | ||
|---|---|---|---|
| No (n = 173) | Yes (n = 34) | ||
| Donor’s characteristics | |||
| Age, media ± SD | 58.3 ± 17.8 | 60.7 ± 16.9 | 0.454 |
| Steatosis | |||
| >50 | 4 (2.3%) | 0 (0.0%) | 0.785 |
| 30–50 | 4 (2.3%) | 1 (2.9%) | |
| <30 | 152 (87.9%) | 28 (82.4%) | |
| NA | 13 | 5 | |
| Ischemia time, mean ± SD | 392.5 ± 110.9 | 406.7 ± 141.9 | 0.516 |
| Recipient’s characteristics | |||
| Age, mean ± SD | 56.9 ± 6.6 | 55.9 ± 7.9 | 0.431 |
| Gender | |||
| Male | 145 (83.8%) | 33 (97.1%) | 0.055 |
| Female | 28 (16.2%) | 1 (2.9%) | |
| BMI, median (Q1, Q3) NA | 25.4 (23.2, 27.4) 1 | 27.0 (23.3, 30.1) 0 | 0.115 |
| Child-Pugh class | |||
| A | 69 (39.9%) | 15 (44.1%) | 0.379 |
| B | 67 (38.7%) | 16 (47.1%) | |
| C | 32 (18.5%) | 3 (8.8%) | |
| NA | 5 | 0 | |
| Waitlist, months | |||
| ≤60 | 60 (34.7%) | 7 (20.6%) | 0.049 * |
| 61–120 | 48 (27.7%) | 6 (17.6%) | |
| 121–240 | 39 (22.5%) | 10 (29.4%) | |
| >241 | 26 (15.0%) | 11 (32.4%) | |
| Median time of waitlist (Q1, Q3) | 92.0 (41.0, 170.0) | 172.0 (70.0, 312.0) | 0.009 * |
| MELD score NA | 12.0 (9.0, 16.0) 9 | 12.0 (10.0, 14.0) 0 | 0.765 |
| Bilirubin NA | 1.5 (1.0, 2.8) 37 | 2.0 (1.3, 2.5) 4 | 0.672 |
| INR NA | 1.3 (1.2, 1.5) 20 | 1.3 (1.2, 1.6) 2 | 0.637 |
| Creatinine NA | 0.8 (0.7, 0.9) 23 | 0.8 (0.7, 0.9) 2 | 0.804 |
| AFP at transplant NA | 8.4 (3.8, 21.3) 15 | 27.5 (7.6, 87.2) 3 | 0.001 * |
| Cirrhosis etiology | |||
| HCV | 83 (48.0%) | 23 (67.6%) | 0.008 * |
| HBV | 60 (34.7%) | 3 (8.8%) | |
| HBV and HCV | 6 (3.5%) | 2 (5.9%) | |
| Others | 20 (11.6%) | 6 (17.6%) | |
| NA | 4 | 0 | |
| Pre-LT characteristics | |||
| Number of nodules | |||
| 1 | 111 (64.2%) | 24 (70.6%) | 0.709 |
| 2 | 43 (24.9%) | 8 (23.5%) | |
| 3 | 19 (11.0%) | 2 (5.9%) | |
| Largest tumour diameter(cm) | 2.4 (1.8, 3.0) | 2.5 (2.0, 3.0) | 0.364 |
| Sum of the diameters | 3.0 (2.0, 4.0) | 3.0 (2.0, 4.0) | 0.950 |
| TTV | 8.2 (4.2, 15.2) | 10.7 (4.2, 18.3) | 0.314 |
| Bridge therapies | 147 (85.0%) | 31 (91.2%) | 0.34 |
| Number, mean ± SD | 1.2 ± 0.8 | 1.4 ± 1.0 | 0.15 |
| Surgery | 8 (4.6%) | 1 (2.9%) | 0.66 |
| Alcoholization | 6 (3.5%) | 3 (8.8%) | 0.16 |
| RFA | 106 (61.3%) | 24 (70.6%) | 0.30 |
| TACE | 74 (42.8%) | 17 (50.0%) | 0.44 |
| Post LT characteristics | |||
| Number of nodules | |||
| 1–3 | 143 (82.7%) | 24 (70.6%) | 0.103 |
| >3 | 30 (17.3%) | 10 (29.4%) | |
| Largest tumour diameter (cm) NA | 2.5 (2.0, 3.5) 1 | 2.9 (2.0, 3.7) 0 | 0.237 |
| Microvascular invasion | |||
| No | 148 (85.5%) | 26 (76.5%) | 0.214 |
| Yes | 22 (12.7%) | 7 (20.6%) | |
| NA | 3 | 1 | |
| Necrosis | |||
| Total | 36 (20.8%) | 2 (5.9%) | 0.069 |
| Partial | 103 (59.5%) | 26 (76.5%) | |
| Absent | 17 (9.8%) | 2 (5.9%) | |
| NA | 17 | 4 | |
| Immunosuppression | |||
| CNI | 145 (83.8%) | 33 (97.1%) | 0.57 |
| NA | 20 | 0 | |
| mTOR | 25 (16.2%) | 11 (32.4%) | 0.031 * |
| NA | 19 | 0 | |
| MMF | 23 (14.9%) | 3 (8.8%) | 0.35 |
| NA | 19 | 0 | |
| Median time from transplant to latest therapy, (months) Q1–Q2 | 12.3 (6.8–22.0) | 10.8 (6.5–19.1) | 0.65 |
| Median time from latest therapy to last fup, (years) Q1–Q2 | 6.3 (4.2–9.8) | 6.4 (4.5–8.8) | 0.82 |
| sHR (95% CI) | p | |
|---|---|---|
| AFP at transplant | ||
| ≤25.5 | 1.00 (reference) | |
| >25.5 | 2.50 (1.20–5.21) | 0.014 |
| MVI | 2.13 (0.90–5.04) | 0.085 |
| Etiology HBV (vs. others) | 0.33 (0.10–1.13) | 0.077 |
| Waitlist | ||
| ≤6 months | 1.00 (reference) | |
| >6 months | 1.76 (0.85–3.64) | 0.127 |
| Total | No Recurrence | Recurrence | p-Value | |
|---|---|---|---|---|
| n = 75 | n = 62 | n = 13 | ||
| ∆AFP ≥ 20.8% | 43 (57.3%) | 32 (51.6%) | 11 (84.6%) | 0.034 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magro, B.; Pinelli, D.; De Giorgio, M.; Lucà, M.G.; Ghirardi, A.; Carrobio, A.; Baronio, G.; Del Prete, L.; Nounamo, F.; Gianatti, A.; et al. Pre-Transplant Alpha-Fetoprotein > 25.5 and Its Dynamic on Waitlist Are Predictors of HCC Recurrence after Liver Transplantation for Patients Meeting Milan Criteria. Cancers 2021, 13, 5976. https://doi.org/10.3390/cancers13235976
Magro B, Pinelli D, De Giorgio M, Lucà MG, Ghirardi A, Carrobio A, Baronio G, Del Prete L, Nounamo F, Gianatti A, et al. Pre-Transplant Alpha-Fetoprotein > 25.5 and Its Dynamic on Waitlist Are Predictors of HCC Recurrence after Liver Transplantation for Patients Meeting Milan Criteria. Cancers. 2021; 13(23):5976. https://doi.org/10.3390/cancers13235976
Chicago/Turabian StyleMagro, Bianca, Domenico Pinelli, Massimo De Giorgio, Maria Grazia Lucà, Arianna Ghirardi, Alessandra Carrobio, Giuseppe Baronio, Luca Del Prete, Franck Nounamo, Andrea Gianatti, and et al. 2021. "Pre-Transplant Alpha-Fetoprotein > 25.5 and Its Dynamic on Waitlist Are Predictors of HCC Recurrence after Liver Transplantation for Patients Meeting Milan Criteria" Cancers 13, no. 23: 5976. https://doi.org/10.3390/cancers13235976
APA StyleMagro, B., Pinelli, D., De Giorgio, M., Lucà, M. G., Ghirardi, A., Carrobio, A., Baronio, G., Del Prete, L., Nounamo, F., Gianatti, A., Colledan, M., & Fagiuoli, S. (2021). Pre-Transplant Alpha-Fetoprotein > 25.5 and Its Dynamic on Waitlist Are Predictors of HCC Recurrence after Liver Transplantation for Patients Meeting Milan Criteria. Cancers, 13(23), 5976. https://doi.org/10.3390/cancers13235976