
The Role of Trastuzumab in Patients with HER2 Positive Small (pT1mi/a) Breast Cancers, a Multicenter Retrospective Study

 , ,
, ,  ,
,  ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analyses
3. Results
3.1. Sample Description
3.2. Tumor Characteristics: pT1mi vs. pT1a
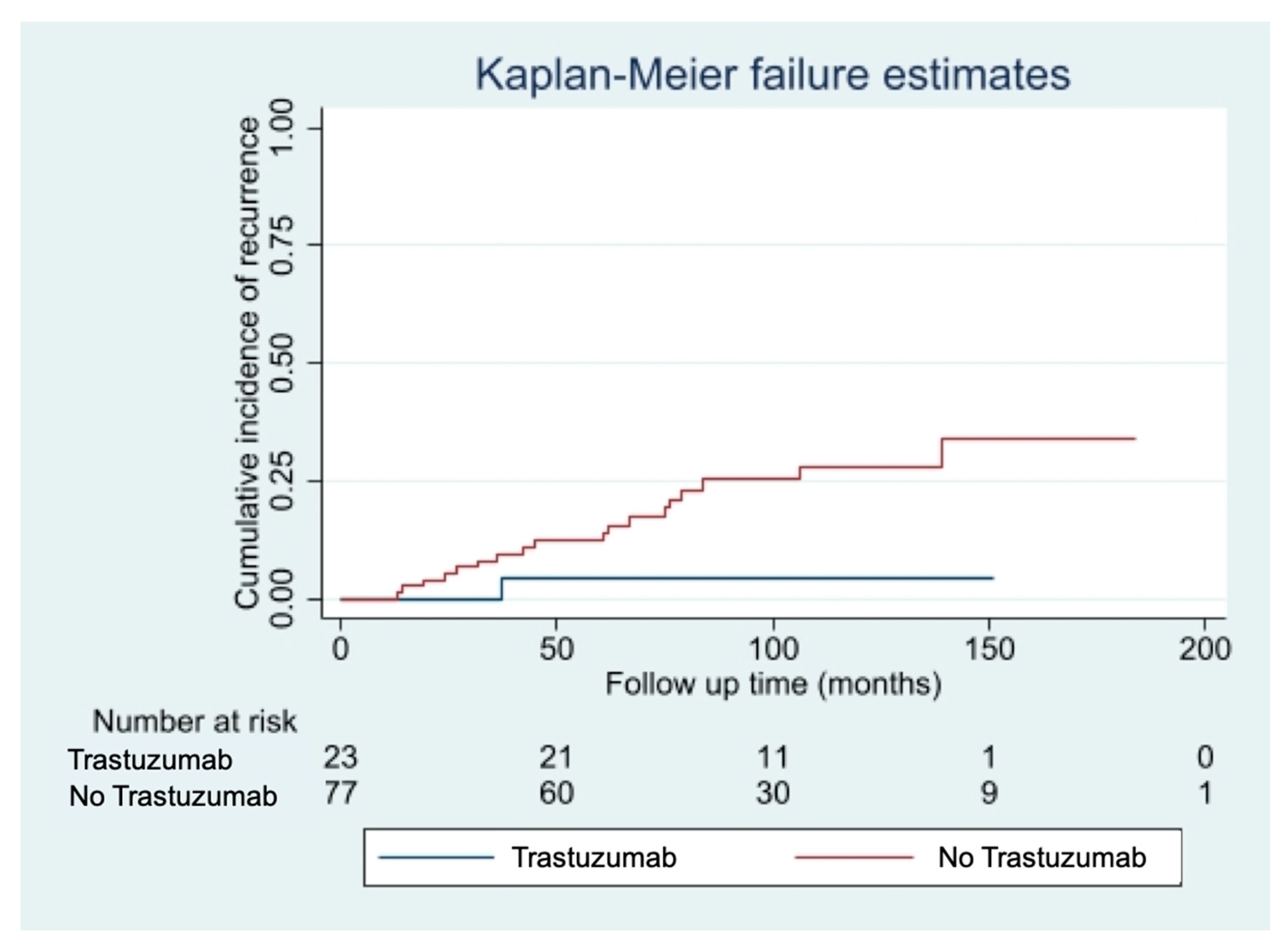
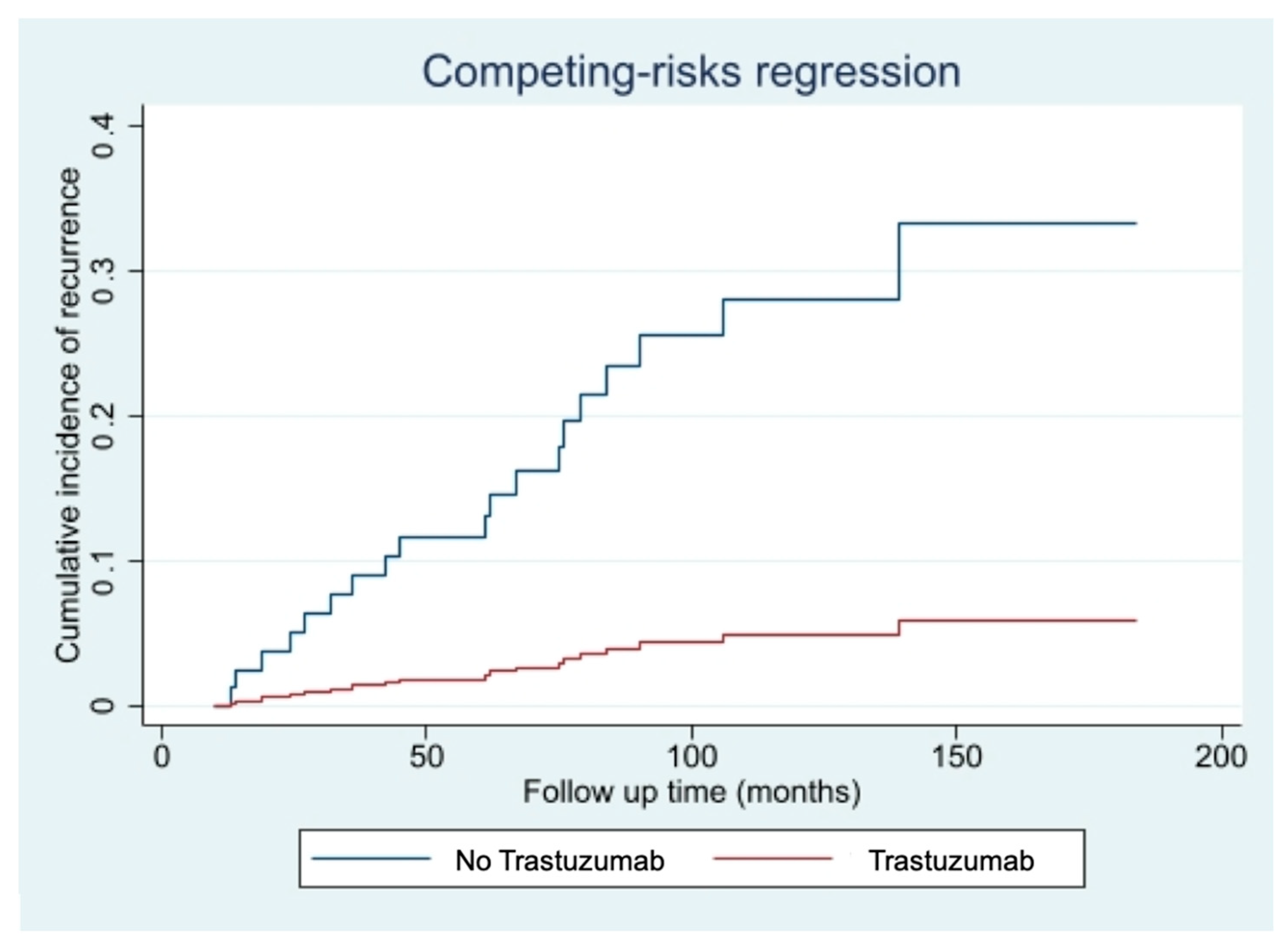
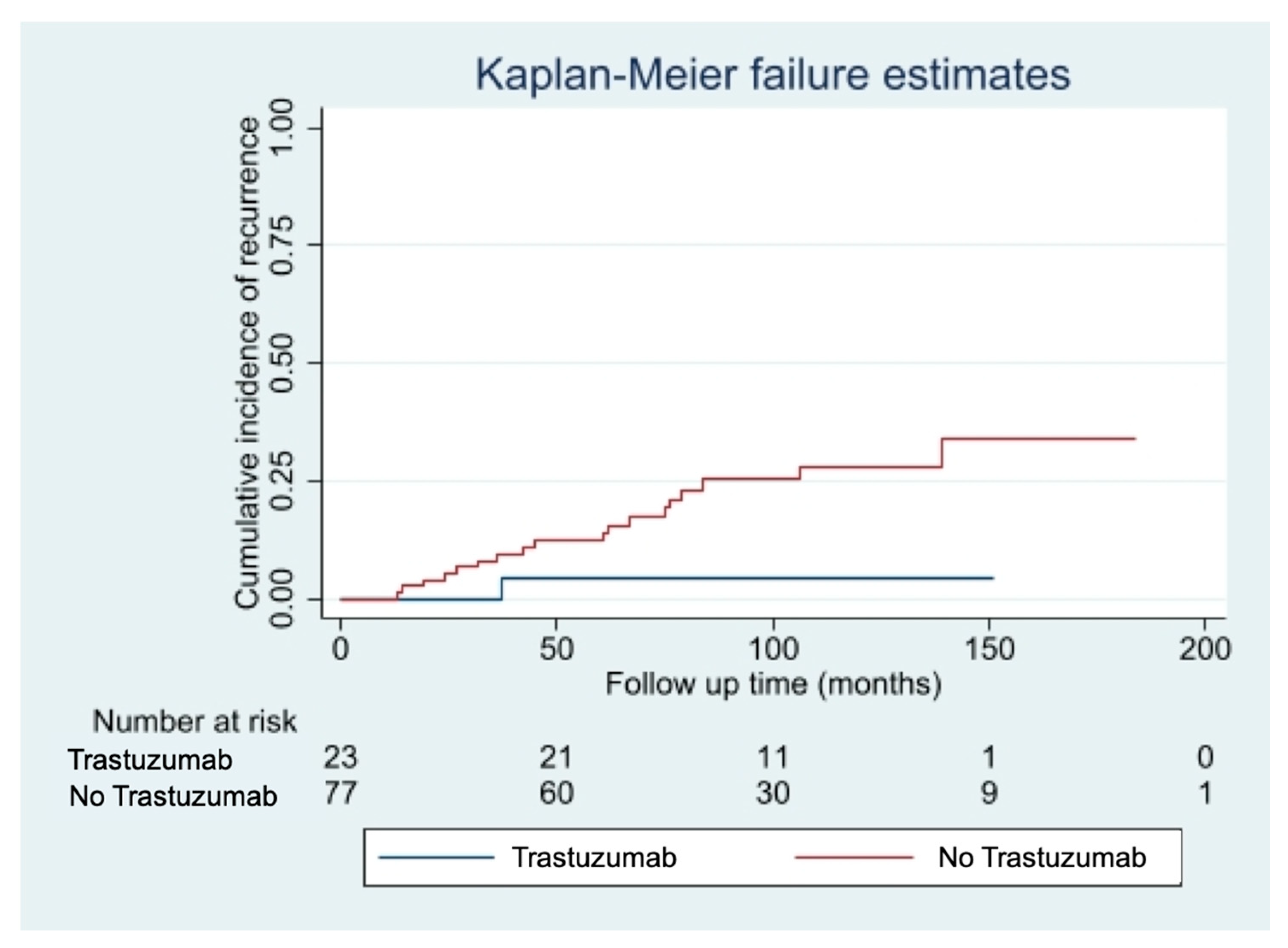
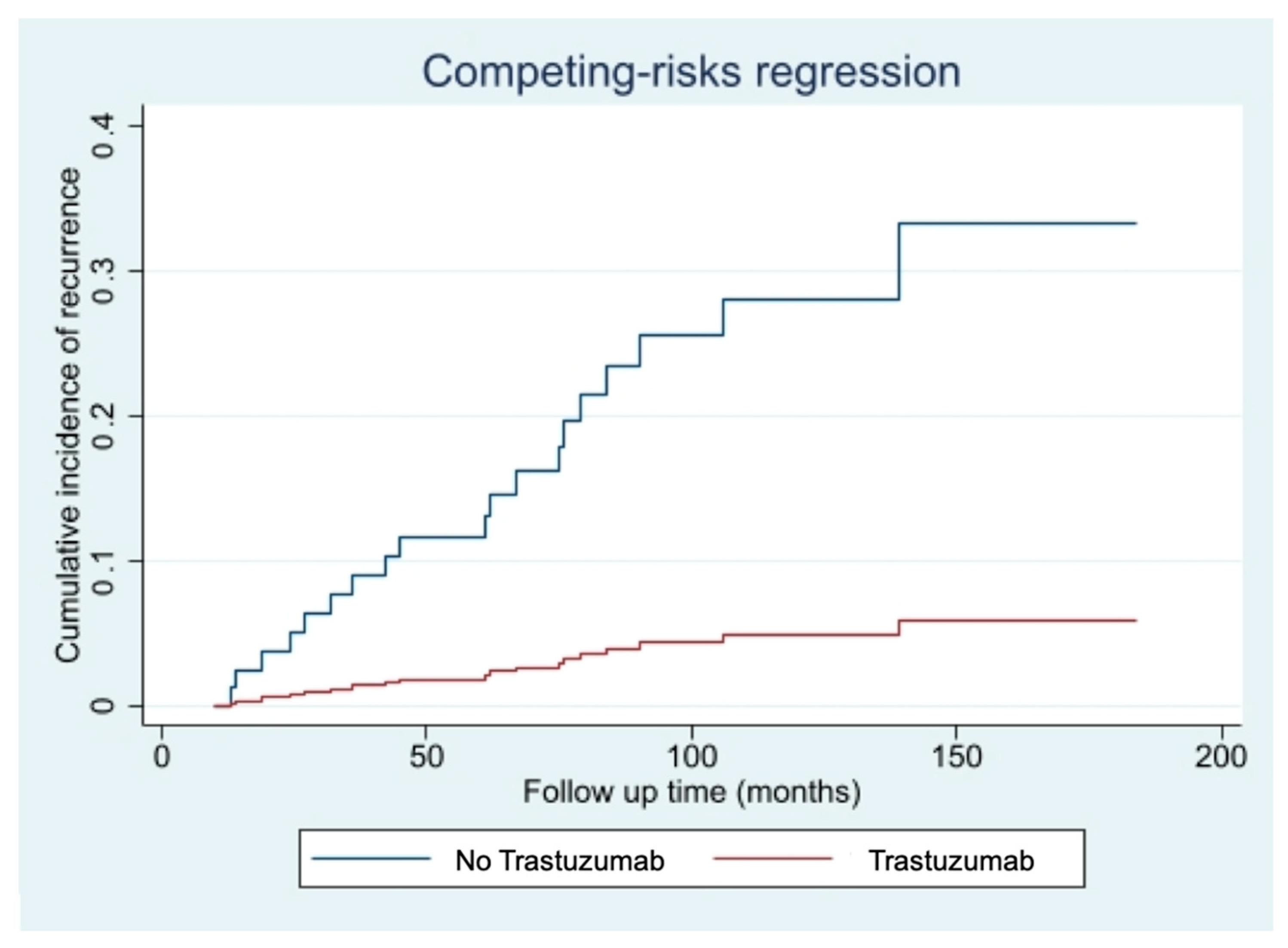
3.3. Trastuzumab Administration and Disease Recurrence Analysis
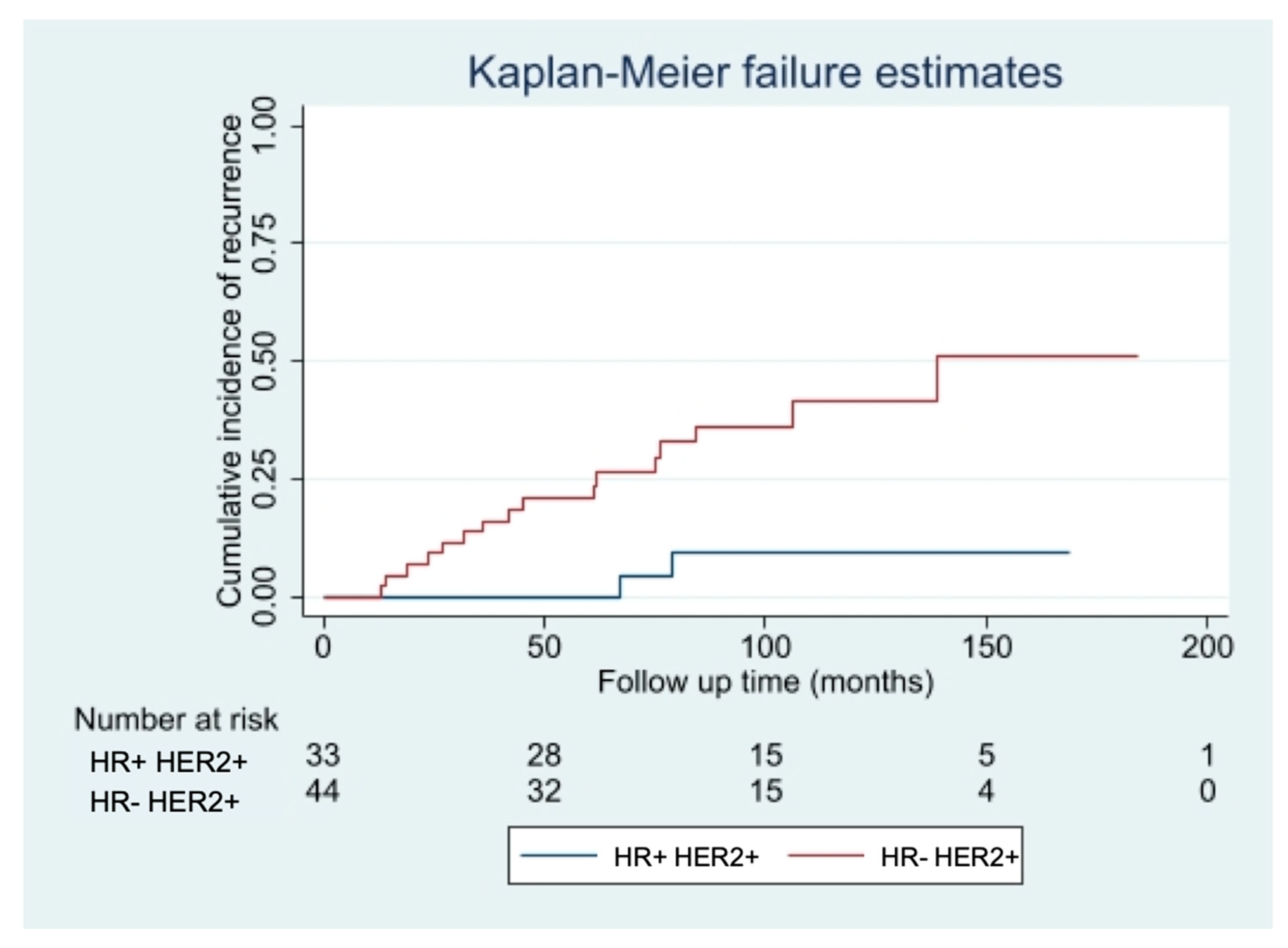
3.4. Disease Recurrence Risk Factors
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Welch, H.G.; Prorok, P.C.; O’Malley, A.J.; Kramer, B.S. Breast-Cancer Tumor Size, Overdiagnosis, and Mammography Screening Effectiveness. N. Engl. J. Med. 2016, 375, 1438–1447. [Google Scholar] [CrossRef] [PubMed]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. (Eds.) AJCC Cancer Staging Handbook: TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2017. [Google Scholar]
- De Mascarel, I.; MacGrogan, G.; Mathoulin-Pélissier, S.; Soubeyran, I.; Picot, V.; Coindre, J.M. Breast ductal carcinoma in situ with microinvasion: A definition supported by a long-term study of 1248 serially sectioned ductal carcinomas. Cancer 2002, 94, 2134–2142. [Google Scholar] [CrossRef]
- Hanrahan, E.O.; Valero, V.; Gonzalez-Angulo, A.M.; Hortobagyi, G.N. Prognosis and management of patients with node-negative invasive breast carcinoma that is 1 cm or smaller in size (stage 1; T1a,bN0M0): A review of the literature. J. Clin. Oncol. 2006, 24, 2113–2122. [Google Scholar] [CrossRef]
- Cancello, G.; Maisonneuve, P.; Rotmensz, N.; Viale, G.; Mastropasqua, M.G.; Pruneri, G.; Montagna, E.; Dellapasqua, S.; Iorfida, M.; Cardillo, A.; et al. Prognosis in women with small (T1mic,T1a,T1b) node-negative operable breast cancer by immunohistochemically selected subtypes. Breast Cancer Res. Treat. 2011, 127, 713–720. [Google Scholar] [CrossRef] [Green Version]
- Hanrahan, E.O.; Gonzalez-Angulo, A.M.; Giordano, S.H.; Rouzier, R.; Broglio, K.R.; Hortobagyi, G.N.; Valero, V. Overall survival and cause-specific mortality of patients with stage T1a,bN0M0 breast carcinoma. J. Clin. Oncol. 2007, 25, 4952–4960. [Google Scholar] [CrossRef] [Green Version]
- Slamon, D.J.; Clark, G.M.; Wong, S.G.; Levin, W.J.; Ullrich, A.; McGuire, W.L. Human breast cancer: Correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987, 235, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shak, S. Overview of the trastuzumab (Herceptin) anti-HER2 monoclonal antibody clinical program in HER2-overexpressing metastatic breast cancer. Herceptin Multinational Investigator Study Group. Semin. Oncol. 1999, 26, 71–77. [Google Scholar] [PubMed]
- Garattini, L.; van de Vooren, K.; Curto, A. Cost-effectiveness of trastuzumab in metastatic breast cancer: Mainly a matter of price in the EU? Health Policy 2015, 119, 212–216. [Google Scholar] [CrossRef]
- Viani, G.A.; Afonso, S.L.; Stefano, E.J.; De Fendi, L.I.; Soares, F.V. Adjuvant trastuzumab in the treatment of her-2-positive early breast cancer: A meta-analysis of published randomized trials. BMC Cancer 2007, 7, 153. [Google Scholar] [CrossRef] [Green Version]
- Templeton, A.; Ocaña, A.; Seruga, B.; Vera-Badillo, F.; Carlsson, L.; Bedard, P.; Amir, E. Management of small HER2 overexpressing tumours. Breast Cancer Res. Treat. 2012, 136, 289–293. [Google Scholar] [CrossRef]
- Joerger, M.; Thürlimann, B.; Huober, J. Small HER2-positive, node-negative breast cancer: Who should receive systemic adjuvant treatment? Ann. Oncol. 2011, 22, 17–23. [Google Scholar] [CrossRef]
- Petrelli, F.; Barni, S. Role of HER2-neu as a prognostic factor for survival and relapse in pT1a-bN0M0 breast cancer: A systematic review of the literature with a pooled-analysis. Med. Oncol. 2012, 29, 2586–2593. [Google Scholar] [CrossRef] [PubMed]
- Rouanet, P.; Roger, P.; Rousseau, E.; Thibault, S.; Romieu, G.; Mathieu, A.; Cretin, J.; Barneon, G.; Granier, M.; Maran-Gonzalez, A.; et al. HER2 overexpression a major risk factor for recurrence in pT1a-bN0M0 breast cancer: Results from a French regional cohort. Cancer Med. 2014, 3, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Horio, A.; Fujita, T.; Hayashi, H.; Hattori, M.; Kondou, N.; Yamada, M.; Adachi, E.; Ushio, A.; Gondou, N.; Sueta, A.; et al. High recurrence risk and use of adjuvant trastuzumab in patients with small, HER2-positive, node-negative breast cancers. Int. J. Clin. Oncol. 2012, 17, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative group (EBCTCG). Trastuzumab for early-stage, HER2-positive breast cancer: A meta-analysis of 13 864 women in seven randomised trials. Lancet Oncol. 2021, 22, 1139–1150. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Breast Cancer (Version 1). 2021. Available online: https://www.nccn.org/professionals/physician_gls/pdf/breast.pdf (accessed on 20 January 2021).
- Gori, S.; Turazza, M.; Modena, A.; Duranti, S.; Zamboni, G.; Alongi, F.; Carbognin, G.; Massocco, A.; Salgarello, M.; Inno, A. When and how to treat women with HER2-positive, small (pT1a-b), node-negative breast cancer? Crit. Rev. Oncol. Hematol. 2018, 128, 130–138. [Google Scholar] [CrossRef]
- Petrelli, F.; Barni, S. Should adjuvant trastuzumab be offered in very early-stage (pT1a/bN0M0) HER2-neu-positive breast cancer? A current debate. Med. Oncol. 2011, 28, 401–408. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.S.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef]
- Wolters, R.; Ebner, F.; Janni, W.; Novopashenny, I.; Wöckel, A.; Kreienberg, R.; Wischnewsky, M.; Schwentner, L. Brenda study group. Do T1a breast cancers profit from adjuvant systemic therapy? A multicenter retrospective cohort study of 325 T1a-patients. Arch. Gynecol. Obstet. 2016, 294, 377–384. [Google Scholar] [CrossRef]
- Vaz-Luis, I.; Ottesen, R.A.; Hughes, M.E.; Mamet, R.; Burstein, H.J.; Edge, S.B.; Gonzalez-Angulo, A.M.; Moy, B.; Rugo, H.S.; Theriault, R.L.; et al. Outcomes by tumor subtype and treatment pattern in women with small, node-negative breast cancer: A multi-in-stitutional study. J. Clin. Oncol. 2014, 32, 2142–2150. [Google Scholar] [CrossRef] [PubMed]
- Fehrenbacher, L.; Capra, A.M.; Quesenberry, C.P., Jr.; Fulton, R.; Shiraz, P.; Habel, L.A. Distant invasive breast cancer recurrence risk in human epidermal growth factor receptor 2-positive T1a and T1b node-negative localized breast cancer diagnosed from 2000 to 2006: A cohort from an integrated health care delivery system. J. Clin. Oncol. 2014, 32, 2151–2158. [Google Scholar] [CrossRef]
- Wang, W.; Zhu, W.; Du, F.; Luo, Y.; Xu, B. The Demographic Features, Clinicopathological Characteristics and Cancer-specific Outcomes for Patients with Microinvasive Breast Cancer: A SEER Database Analysis. Sci Rep. 2017, 7, 42045. [Google Scholar] [CrossRef] [Green Version]
- Kapoor, N.S.; Shamonki, J.; Sim, M.S.; Chung, C.T.; Giuliano, A.E. Impact of multifocality and lymph node metastasis on the prognosis and management of microinvasive breast cancer. Ann. Surg. Oncol. 2013, 20, 2576–2581. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Moisini, I.; Turner, B.M.; Wang, X.; Dhakal, A.; Yang, Q.; Kovar, S.; Schiffhauer, L.M.; Hicks, D.G. Significance of HER2 in Microinvasive Breast Carcinoma: A Single Academic Institution Experience. Am. J. Clin. Pathol. 2021, 156, 155–165. [Google Scholar] [CrossRef]
- Kim, M.; Kim, H.J.; Chung, Y.R.; Kang, E.; Kim, E.K.; Kim, S.H.; Kim, Y.J.; Kim, J.H.; Kim, I.A.; Park, S.Y. Microinvasive Carcinoma versus Ductal Carcinoma In Situ: A Comparison of Clinicopathological Features and Clinical Outcomes. J. Breast Cancer 2018, 21, 197–205. [Google Scholar] [CrossRef]
- Costarelli, L.; Cianchetti, E.; Corsi, F.; Friedman, D.; Ghilli, M.; Lacaria, M.; Menghini, L.; Murgo, R.; Ponti, A.; Rinaldi, S.; et al. Microinvasive breast carcinoma: An analysis from ten Senonetwork Italia breast centres. Eur. J. Surg. Oncol. 2019, 45, 147–152. [Google Scholar] [CrossRef]
- Lee, H.Y.; Shin, I.S.; Rim, C.H. Benefits of adjuvant treatment including trastuzumab in HER2-positive pT1a-bN0M0 breast cancer: A systematic review and meta-analysis. Ann. Transl. Med. 2020, 8, 187. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.; Zhou, T.; Li, F.; Shi, J.; Zhang, L. Clinic-Pathological Features of Breast Ductal Carcinoma in Situ with Micro-Invasion. Cancer Investig. 2020, 38, 113–121. [Google Scholar] [CrossRef]
- Yu, K.D.; Wu, L.M.; Liu, G.Y.; Wu, J.; Di, G.H.; Shen, Z.Z.; Shao, Z.M. Different distribution of breast cancer subtypes in breast ductal carcinoma in situ (DCIS), DCIS with microinvasion, and DCIS with invasion component. Ann. Surg. Oncol. 2011, 18, 1342–1348. [Google Scholar] [CrossRef] [PubMed]
- Slamon, D.; Eiermann, W.; Robert, N.; Pienkowski, T.; Martin, M.; Press, M.; Mackey, J.; Glaspy, J.; Chan, A.; Pawlicki, M.D.; et al. Adjuvant trastuzumab in HER2-positive breast cancer. N. Engl. J. Med. 2011, 365, 1273–1283. [Google Scholar] [CrossRef] [Green Version]
- Zhou, Q.; Yin, W.; Du, Y.; Lu, J. For or against adjuvant trastuzumab for pT1a-bN0M0 breast cancer patients with HER2-positive tumors: A meta-analysis of published literatures. PLoS ONE 2014, 9, e83646. [Google Scholar] [CrossRef] [PubMed]
- O’Sullivan, C.C.; Bradbury, I.; Campbell, C.; Spielmann, M.; Perez, E.A.; Joensuu, H.; Costantino, J.P.; Delaloge, S.; Rastogi, P.; Zardavas, D.; et al. Efficacy of adjuvant trastuzumab for patients with human epidermal growth factor receptor 2-positive early breast cancer and tumors ≤ 2 cm: A meta-analysis of the randomized trastuzumab trials. J. Clin. Oncol. 2015, 33, 2600–2608. [Google Scholar] [CrossRef] [PubMed]
- Tognela, A.; Beith, J.; Kiely, B.; Bastick, P.; Lynch, J.; Descallar, J.; Mok, K. Small HER2-positive breast cancer: Should size affect adjuvant treatment? Clin. Breast Cancer 2015, 15, 277–284. [Google Scholar] [CrossRef]
- Migdady, Y.; Sakr, B.J.; Sikow, W.M.; Olszewski, A.J. Adjuvant chemotherapy in T1a/ bN0 HER2-positive or triple-negative breast cancers: Application and outcomes. Breast 2013, 22, 793–798. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Median Age at Diagnosis (Years) | 57 | SD 13 |
|---|---|---|
| n = 100 | % | |
| Menopausal status at diagnosis | ||
| Pre-menopausal | 34 | 34 |
| Post-menopausal | 66 | 66 |
| pT status | ||
| pT1mic | 58 | 58 |
| pT1a | 42 | 42 |
| Nodal status | ||
| pN0 | 92 | 92 |
| pN1mi | 8 | 8 |
| Grading | ||
| G1 | 0 | 0 |
| G2 | 24 | 24 |
| G3 | 72 | 72 |
| Unknown | 4 | 4 |
| Ki-67 | ||
| Low < 20% | 20 | 20 |
| High > 20% | 35 | 35 |
| Unknown | 45 | 45 |
| IHC subtype | ||
| HR+ HER2+ | 45 | 45 |
| HR− HER2+ | 55 | 55 |
| Type of surgery | ||
| Conservative surgery | 51 | 51 |
| Mastectomy | 49 | 49 |
| Radiation Therapy | ||
| Yes | 46 | 46 |
| No | 54 | 54 |
| Hormone therapy | ||
| None | 65 | 65 |
| Aromatase Inhibitors | 16 | 16 |
| Tamoxifen | 19 | 19 |
| Chemotherapy | ||
| Yes | 27 | 27 |
| No | 73 | 73 |
| Trastuzumab therapy | ||
| Yes | 23 | 23 |
| No | 77 | 77 |
| Relapse | ||
| Local recurrence | 16 | 16 |
| Distant metastases | 4 | 4 |
| No | 80 | 80 |
| Categories | pT1mic | pT1a | |||
|---|---|---|---|---|---|
| n = 58 | % | n = 42 | % | p-Value | |
| Menopausal status | 0.508 | ||||
| Pre-menopausal Post-menopausal | 16 41 | 28 71 | 16 25 | 38 60 | |
| Grade | 0.003 | ||||
| 1 | 0 | 0 | 0 | 0 | |
| 2 | 8 | 14 | 16 | 38 | |
| 3 | 49 | 84 | 23 | 55 | |
| Ki67 | 0.007 | ||||
| Low < 20% | 5 | 9 | 15 | 54 | |
| High > 20% | 22 | 81 | 13 | 46 | |
| IHC- subtype | 0.001 | ||||
| HR− HER2+ | 40 | 69 | 15 | 36 | |
| HR+ HER2+ | 18 | 31 | 27 | 64 | |
| Trastuzumab therapy Yes No | 10 48 | 17 83 | 13 29 | 31 69 | 0.149 |
| Categories | pT1mic | pT1a | |||
|---|---|---|---|---|---|
| n = 10 | % | n = 13 | % | p-Value | |
| Chemotherapy schemes | 0.85 | ||||
| 4 cycles of Docetaxel 75 mg/m2 + Cyclophosphamide 600 mg/m2 and Trastuzumab for 1 year | 9 | 90 | 12 | 92 | |
| Paclitaxel 80 mg/m2 weekly for 12 weeks and Trastuzumab for 1 year | 1 | 10 | 1 | 8 | |
| Categories | Trastuzumab Group | Non-Trastuzumab Group | |||
|---|---|---|---|---|---|
| n = 23 | % | n = 77 | % | p-Value | |
| Menopausal status at diagnosis | 0.71 | ||||
| Pre-menopausal | 7 | 30 | 25 | 32 | |
| Post-menopausal | 16 | 70 | 50 | 65 | |
| Unknown | 0 | 0 | 2 | 3 | |
| Size | 0.11 | ||||
| pT1mic | 10 | 43 | 48 | 62 | |
| pT1a | 13 | 57 | 29 | 38 | |
| Lymph node status | 0.38 | ||||
| pN0 | 20 | 87 | 72 | 94 | |
| pN1mi | 3 | 13 | 5 | 6 | |
| Grade | 0.07 | ||||
| G1 | 0 | 0 | 0 | 0 | |
| G2 | 9 | 39 | 15 | 20 | |
| G3 | 14 | 61 | 58 | 75 | |
| Unknown | 0 | 0 | 4 | 5 | |
| Ki 67 | 0.25 | ||||
| Low < 20% | 3 | 14 | 17 | 22 | |
| High > 20% | 10 | 43 | 25 | 32 | |
| Unknown | 10 | 43 | 35 | 46 | |
| IHC- subtype | 0.43 | ||||
| HR+ HER2+ | 12 | 52,2 | 33 | 43 | |
| HR− HER2+ | 11 | 47,8 | 44 | 57 | |
| Type of surgery | 0.73 | ||||
| Conservative surgery | 11 | 48 | 40 | 52 | |
| Mastectomy | 12 | 52 | 37 | 48 | |
| Radiation Therapy | 0.78 | ||||
| Yes | 10 | 43 | 36 | 47 | |
| No | 13 | 57 | 41 | 53 | |
| Hormone therapy | 0.19 | ||||
| Yes | 11 | 48 | 25 | 32 | |
| No | 12 | 52 | 52 | 68 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villasco, A.; Actis, S.; Bounous, V.E.; Borella, F.; D’Alonzo, M.; Ponzone, R.; De Sanctis, C.; Benedetto, C.; Biglia, N. The Role of Trastuzumab in Patients with HER2 Positive Small (pT1mi/a) Breast Cancers, a Multicenter Retrospective Study. Cancers 2021, 13, 5836. https://doi.org/10.3390/cancers13225836
Villasco A, Actis S, Bounous VE, Borella F, D’Alonzo M, Ponzone R, De Sanctis C, Benedetto C, Biglia N. The Role of Trastuzumab in Patients with HER2 Positive Small (pT1mi/a) Breast Cancers, a Multicenter Retrospective Study. Cancers. 2021; 13(22):5836. https://doi.org/10.3390/cancers13225836
Chicago/Turabian StyleVillasco, Andrea, Silvia Actis, Valentina Elisabetta Bounous, Fulvio Borella, Marta D’Alonzo, Riccardo Ponzone, Corrado De Sanctis, Chiara Benedetto, and Nicoletta Biglia. 2021. "The Role of Trastuzumab in Patients with HER2 Positive Small (pT1mi/a) Breast Cancers, a Multicenter Retrospective Study" Cancers 13, no. 22: 5836. https://doi.org/10.3390/cancers13225836
APA StyleVillasco, A., Actis, S., Bounous, V. E., Borella, F., D’Alonzo, M., Ponzone, R., De Sanctis, C., Benedetto, C., & Biglia, N. (2021). The Role of Trastuzumab in Patients with HER2 Positive Small (pT1mi/a) Breast Cancers, a Multicenter Retrospective Study. Cancers, 13(22), 5836. https://doi.org/10.3390/cancers13225836