
High Grade of Amplification of Six Regions on Chromosome 2p in a Neuroblastoma Patient with Very Poor Outcome: The Putative New Oncogene TSSC1

 , , , , and
, , , , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Case Description
2.2. Genomic Profile Analysis
2.3. Data Source
2.4. Immunofluorescence Detection
2.5. Statistical Analysis
3. Results
3.1. Genomic Profile Analysis
3.2. Association between Patient Survival and Expression of RNF144A
3.3. Association between Patient Survival and Expression of MYT1L
3.4. Association between Patient Survival and Expression of TSSC1
3.5. Association between Patient Survival and Expression of LOC730811
3.6. Association between Patient Survival and Expression of CMPK2
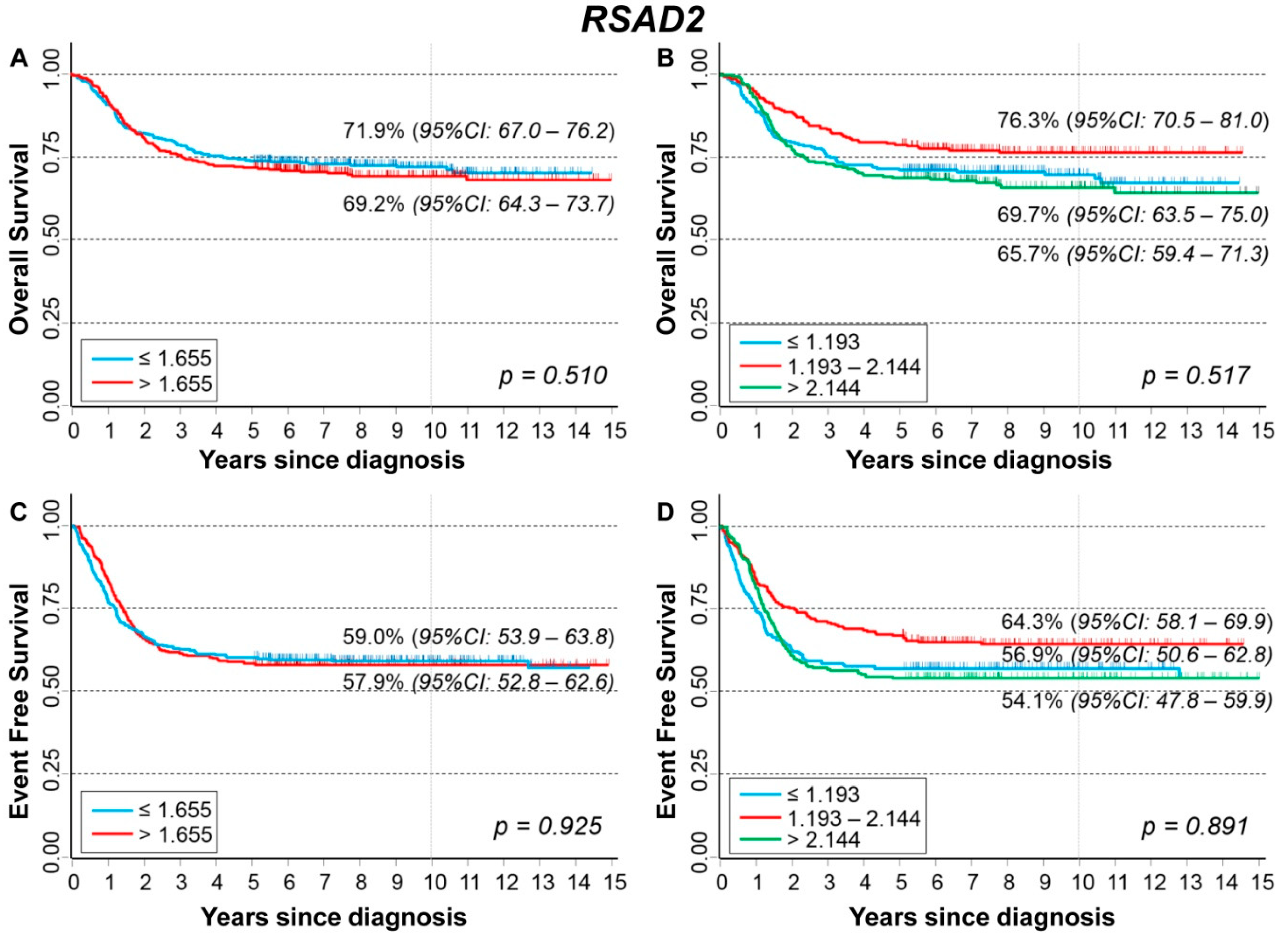
3.7. Association between Patient Survival and Expression of RSAD2
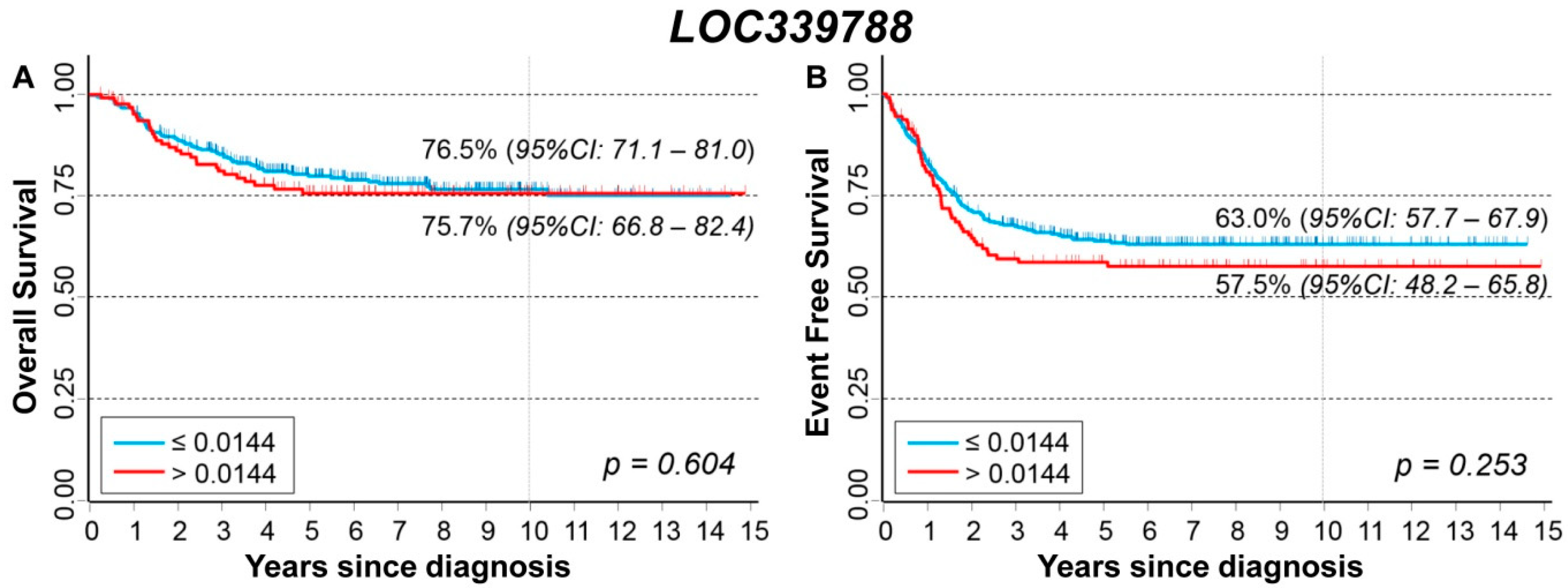
3.8. Association between Patient Survival and Expression of LOC339788
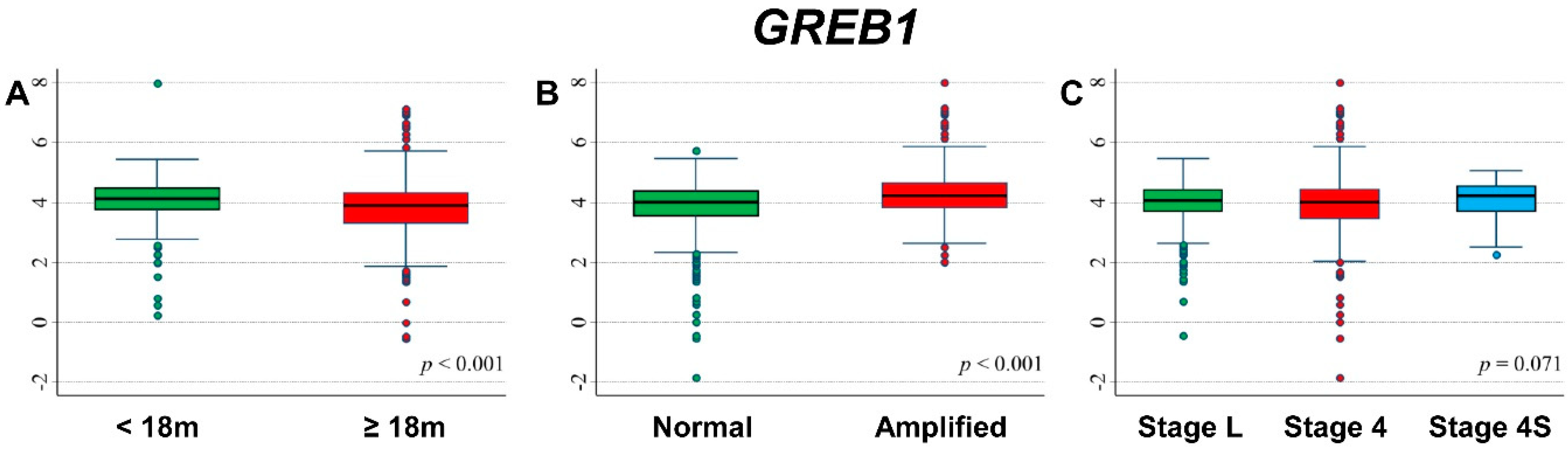
3.9. Association between Patient Survival and Expression of GREB1
3.10. Association between Patient Survival and Expression of NTSR2
3.11. Association between Patient Survival and Expression of LPIN1
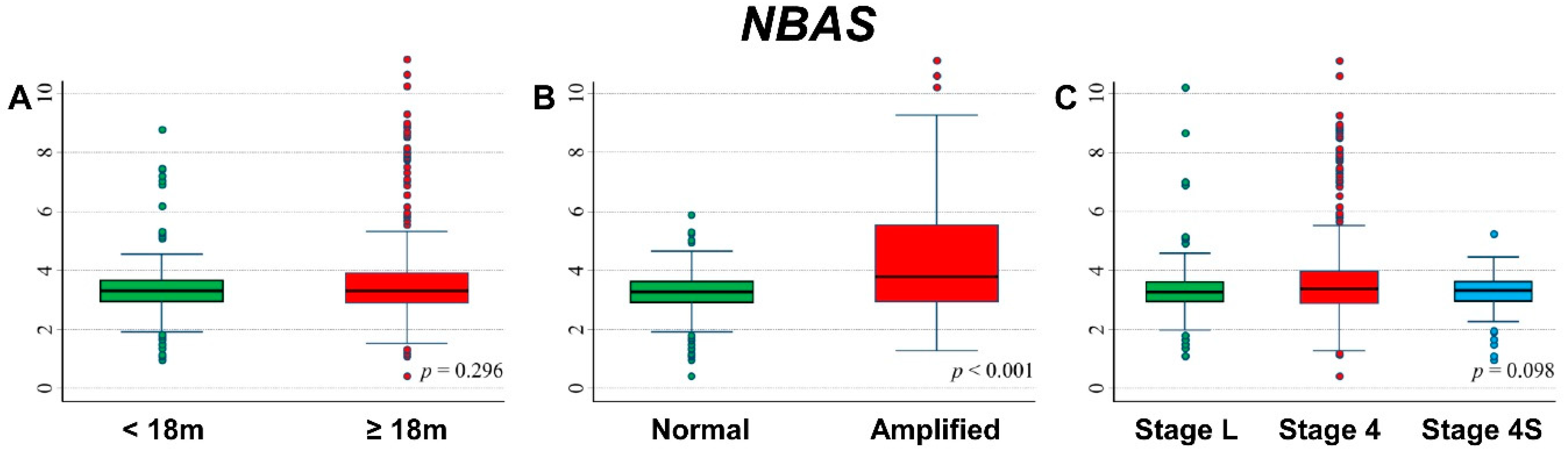
3.12. Association between Patient Survival and Expression of NBAS
3.13. TSSC1 Protein Expression in Stage 4 NB
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cheung, N.K.; Dyer, M.A. Neuroblastoma: Developmental biology, cancer genomics and immunotherapy. Nat. Rev. Cancer 2013, 13, 397–411. [Google Scholar] [CrossRef] [Green Version]
- Louis, C.U.; Shohet, J.M. Neuroblastoma: Molecular pathogenesis and therapy. Annu. Rev. Med. 2015, 66, 49–63. [Google Scholar] [CrossRef] [Green Version]
- Cheung, N.K.; Zhang, J.; Lu, C.; Parker, M.; Bahrami, A.; Tickoo, S.K.; Heguy, A.; Pappo, A.S.; Federico, S.; Dalton, J.; et al. Association of age at diagnosis and genetic mutations in patients with neuroblastoma. J. Am. Med. Assoc. 2012, 307, 1062–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janoueix-Lerosey, I.; Schleiermacher, G.; Michels, E.; Mosseri, V.; Ribeiro, A.; Lequin, D.; Vermeulen, J.; Couturier, J.; Peuchmaur, M.; Valent, A.; et al. Overall genomic pattern is a predictor of outcome in neuroblastoma. J. Clin. Oncol. 2009, 27, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Matthay, K.K.; Maris, J.M.; Schleiermacher, G.; Nakagawara, A.; Mackall, C.L.; Diller, L.; Weiss, W.A. Neuroblastoma. Nat. Rev. Dis. Primers 2016, 2, 16078. [Google Scholar] [CrossRef] [PubMed]
- Schleiermacher, G.; Janoueix-Lerosey, I.; Ribeiro, A.; Klijanienko, J.; Couturier, J.; Pierron, G.; Mosseri, V.; Valent, A.; Auger, N.; Plantaz, D.; et al. Accumulation of segmental alterations determines progression in neuroblastoma. J. Clin. Oncol. 2010, 28, 3122–3130. [Google Scholar] [CrossRef]
- Carr, J.; Bown, N.P.; Case, M.C.; Hall, A.G.; Lunec, J.; Tweddle, D.A. High-resolution analysis of allelic imbalance in neuroblastoma cell lines by single nucleotide polymorphism arrays. Cancer Genet. Cytogenet. 2007, 172, 127–138. [Google Scholar] [CrossRef]
- Peifer, M.; Hertwig, F.; Roels, F.; Dreidax, D.; Gartlgruber, M.; Menon, R.; Krämer, A.; Roncaioli, J.L.; Sand, F.; Heuckmann, J.M.; et al. Telomerase activation by genomic rearrangements in high-risk neuroblastoma. Nature 2015, 526, 700–704. [Google Scholar] [CrossRef]
- Westermann, F.; Muth, D.; Benner, A.; Bauer, T.; Henrich, K.O.; Oberthuer, A.; Brors, B.; Beissbarth, T.; Vandesompele, J.; Pattyn, F.; et al. Distinct transcriptional MYCN/c-MYC activities are associated with spontaneous regression or malignant progression in neuroblastomas. Genome Biol. 2008, 9, R150. [Google Scholar] [CrossRef] [Green Version]
- Zeineldin, M.; Federico, S.; Chen, X.; Fan, Y.; Xu, B.; Stewart, E.; Zhou, X.; Jeon, J.; Griffiths, L.; Nguyen, R.; et al. MYCN amplification and ATRX mutations are incompatible in neuroblastoma. Nat. Commun. 2020, 11, 913. [Google Scholar] [CrossRef] [Green Version]
- Corvi, R.; Savelyeva, L.; Breit, S.; Wenzel, A.; Handgretinger, R.; Barak, J.; Oren, M.; Amler, L.; Schwab, M. Non syntenic amplification of MDM2 and MYCN in human neuroblastoma. Oncogene 1995, 10, 1081–1086. [Google Scholar]
- Fix, A.; Lucchesi, C.; Ribeiro, A.; Lequin, D.; Pierron, G.; Schleiermacher, G.; Delattre, O.; Janoueix-Lerosey, I. Characterization of amplicons in neuroblastoma: High-resolution mapping using DNA microarrays, relationship with outcome, and identification of overexpressed genes. Genes Chromosomes Cancer 2008, 47, 819–834. [Google Scholar] [CrossRef] [PubMed]
- Fix, A.; Peter, M.; Pierron, G.; Aurias, A.; Delattre, O.; Janoueix-Lerosey, I. High-resolution mapping of amplicons of the short arm of chromosome 1 in two neuroblastoma tumors by microarray-based comparative genomic hybridization. Genes Chromosomes Cancer 2004, 40, 266–270. [Google Scholar] [CrossRef]
- Molenaar, J.J.; Van Sluis, P.; Boon, K.; Versteeg, R.; Caron, H.N. Rearrangements and increased expression of cyclin D1 (CCND1) in neuroblastoma. Genes Chromosomes Cancer 2003, 36, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Su, W.T.; Alaminos, M.; Mora, J.; Cheung, N.K.; La Quaglia, M.P.; Gerald, W.L. Positional gene expression analysis identifies 12q overexpression and amplification in a subset of neuroblastomas. Cancer Genet. Cytogenet. 2004, 154, 131–137. [Google Scholar] [CrossRef]
- Guimier, A.; Ferrand, S.; Pierron, G.; Couturier, J.; Janoueix-Lerosey, I.; Combaret, V.; Mosseri, V.; Thebaud, E.; Gambart, M.; Plantaz, D.; et al. Clinical characteristics and outcome of patients with neuroblastoma presenting genomic amplification of loci other than MYCN. PLoS ONE 2014, 9, e101990. [Google Scholar] [CrossRef] [PubMed]
- Depuydt, P.; Boeva, V.; Hocking, T.D.; Cannoodt, R.; Ambros, I.M.; Ambros, P.F.; Asgharzadeh, S.; Attiyeh, E.F.; Combaret, V.; Defferrari, R.; et al. Genomic Amplifications and Distal 6q Loss: Novel Markers for Poor Survival in High-risk Neuroblastoma Patients. J. Natl. Cancer Inst. 2018, 110, 1084–1093. [Google Scholar] [CrossRef]
- Amoroso, L.; Ognibene, M.; Morini, M.; Conte, M.; Di Cataldo, A.; Tondo, A.; D’Angelo, P.; Castellano, A.; Garaventa, A.; Lasorsa, V.A.; et al. Genomic co-amplification of CDK4/MDM2/FRS2 is associated with very poor prognosis and atypical clinical features in neuroblastoma patients. Genes Chromosomes Cancer 2020, 59, 277–285. [Google Scholar] [CrossRef]
- Wagner, A.H.; Coffman, A.C.; Ainscough, B.J.; Spies, N.C.; Skidmore, Z.L.; Campbell, K.M.; Krysiak, K.; Pan, D.; McMichael, J.F.; Eldred, J.M.; et al. DGIdb 2.0: Mining clinically relevant drug-gene interactions. Nucleic Acids Res. 2016, 44, 1036–1044. [Google Scholar] [CrossRef] [Green Version]
- Sholler, G.L.; Gerner, E.W.; Bergendahl, G.; MacArthur, R.B.; VanderWerff, A.; Ashikaga, T.; Bond, J.P.; Ferguson, W.; Roberts, W.; Wada, R.K.; et al. A phase I trial of DFMO targeting polyamine addiction in patients with relapsed/refractory neuroblastoma. PLoS ONE 2015, 10, e0127246. [Google Scholar] [CrossRef]
- Burgess, A.; Chia, K.M.; Haupt, S.; Thomas, D.; Haupt, Y.; Lim, E. Clinical overview of MDM2/X-targeted therapies. Front. Oncol. 2016, 6, 7. [Google Scholar] [CrossRef]
- Sato, T.M.; Gotoh, N. The FRS2 family of docking/scaffolding adaptor proteins as therapeutic targets of cancer treatment. Expert Opin. Ther. Targets 2009, 13, 689–700. [Google Scholar] [CrossRef]
- Scott, D.; Elsden, J.; Pearson, A.; Lunec, J. Genes co-amplified with MYCN in neuroblastoma: Silent passengers or co-determinants of phenotype? Cancer Lett. 2003, 197, 81–86. [Google Scholar] [CrossRef]
- Carr-Wilkinson, J.; Griffiths, R.; Elston, R.; Gamble, L.D.; Goranov, B.; Redfern, C.P.F.; Lunec, J.; Tweddle, D.A. Outcome of the p53-mediated DNA damage response in neuroblastoma is determined by morphological subtype and MYCN expression. Cell Cycle 2011, 10, 3778–3787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Preter, K.; Speleman, F.; Combaret, V.; Lunec, J.; Board, J.; Pearson, A.; De Paepe, A.; Van Roy, N.; Laureys, G.; Vandesompele, J. No Evidence for Correlation of DDX1 Gene Amplification with Improved Survival Probability in Patients with MYCN-Amplified Neuroblastomas. J. Clin. Oncol. 2005, 23, 3167–3168. [Google Scholar] [CrossRef]
- Cetinkaya, C.; Martinsson, T.; Sandgren, J.; Träger, C.; Kogner, P.; Dumanski, J.; Díaz De Ståhl, T.; Hedborg, F. Age dependence of tumor genetics in unfavorable neuroblastoma: Array-CGH profiles of 34 consecutive cases, using a Swedish 25-year neuroblastoma cohort for validation. BMC Cancer 2013, 13, 231–245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.G.; Armstrong, R.C.; Agoston, D.; Robinsky, A.; Wiese, C.; Nagle, J.; Hudson, L.D. Myelin transcription factor 1 (Myt1) of the oligodendrocyte lineage, along with a closely related CCHC zinc finger, is expressed in developing neurons in the mammalian central nervous system. J. Neurosci. Res. 1997, 50, 272–290. [Google Scholar] [CrossRef] [Green Version]
- Chang, X.; Bakay, M.; Liu, Y.; Glessner, J.; Rathi, K.S.; Hou, C.; Qu, H.; Vaksman, Z.; Nguyen, K.; Sleiman, P.M.A.; et al. Mitochondrial DNA haplogroups and susceptibility to neuroblastoma. J. Natl. Cancer Inst. 2020, 112, 1259–1266. [Google Scholar] [CrossRef]
- Park, J.R.; Bagatell, R.; Cohn, S.L.; Pearson, A.D.; Villablanca, G.J.; Berthold, F.; Burchill, S.; Boubaker, A.; McHugh, K.; Nuchtern, J.G.; et al. Revisions to the International neuroblastoma response criteria: A consensus statement from the National Cancer Institute clinical trials planning meeting. J. Clin. Oncol. 2017, 35, 2580–2587. [Google Scholar] [CrossRef]
- Ladenstein, R.; Valteau-Couanet, D.; Brock, P.; Yaniv, I.; Castel, V.; Laureys, G.; Malis, J.; Papadakis, V.; Lacerda, A.; Ruud, E.; et al. Randomized Trial of prophylactic granulocyte colony-stimulating factor during rapid COJEC induction in pediatric patients with high-risk neuroblastoma: The European HR-NBL1/SIOPEN study. J. Clin. Oncol. 2010, 28, 3516–3524. [Google Scholar] [CrossRef] [PubMed]
- Ognibene, M.; Morini, M.; Garaventa, A.; Podestà, M.; Pezzolo, A. Identification of a minimal region of loss on chromosome 6q27 associated with poor survival of high-risk neuroblastoma patients. Cancer Biol. Ther. 2020, 21, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Pezzolo, A.; Sementa, A.R.; Lerone, M.; Morini, M.; Ognibene, M.; Defferrari, R.; Mazzocco, K.; Conte, M.; Gigliotti, A.R.; Garaventa, A.; et al. Constitutional 3p26.3 terminal microdeletion in an adolescent with neuroblastoma. Cancer Biol. Ther. 2017, 18, 285–289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cangelosi, D.; Morini, M.; Zanardi, N.; Sementa, A.R.; Muselli, M.; Conte, M.; Garaventa, A.; Pfeffer, U.; Bosco, M.C.; Varesio, L.; et al. Hypoxia Predicts Poor Prognosis in Neuroblastoma Patients and Associates with Biological Mechanisms Involved in Telomerase Activation and Tumor Microenvironment Reprogramming. Cancers 2020, 12, 2343. [Google Scholar] [CrossRef]
- Zhang, W.; Yu, Y.; Hertwig, F.; Thierry-Mieg, J.; Zhang, W.; Thierry-Mieg, D.; Wang, J.; Furlanello, C.; Devanarayan, V.; Cheng, J.; et al. Comparison of RNA-seq and microarray-based models for clinical endpoint prediction. Genome Biol. 2015, 16, 133. [Google Scholar] [CrossRef] [Green Version]
- Oberthuer, A.; Juraeva, D.; Hero, B.; Volland, R.; Sterz, C.; Schmidt, R.; Faldum, A.; Kahlert, Y.; Engesser, A.; Asgharzadeh, S.; et al. Revised risk estimation and treatment stratification of low- and intermediate-risk neuroblastoma patients by integrating clinical and molecular prognostic markers. Clin. Cancer Res. 2015, 21, 1904–1915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GTEx Consortium. The Genotype-Tissue Expression (GTEx) project. Nat. Genet. 2013, 45, 580–585. [Google Scholar] [CrossRef]
- Ognibene, M.; Podestà, M.; Garaventa, A.; Pezzolo, A. Role of GOLPH3 and TPX2 in Neuroblastoma DNA Damage Response and Cell Resistance to Chemotherapy. Int. J. Mol. Sci. 2019, 20, 4764. [Google Scholar] [CrossRef] [Green Version]
- Hosmer, D.W.; Lemeshow, S.; May, S. Applied Survival Analysis—Regression Modelling of Time to Event Data, 2nd ed.; John Wiley & Sons, Inc.: New York, NY, USA, 2008; pp. 1–416. [Google Scholar]
- Turner, K.M.; Deshpande, V.; Beyter, D.; Koga, T.; Rusert, J.; Lee, C.; Li, B.; Arden, K.; Ren, B.; Nathanson, D.A.; et al. Extrachromosomal oncogene amplification drives tumour evolution and genetic heterogeneity. Nature 2017, 543, 122–125. [Google Scholar] [CrossRef]
- Schwab, M.; Alitalo, K.; Klempnauer, K.H.; Varmus, H.E.; Bishop, J.M.; Gilbert, F.; Brodeur, G.; Goldstein, M.; Trent, J. Amplified DNA with limited homology to myc cellular oncogene is shared by human neuroblastoma cell lines and a neuroblastoma tumour. Nature 1983, 305, 245–248. [Google Scholar] [CrossRef]
- Koche, R.P.; Rodriguez-Fos, E.; Helmsauer, K.; Burkert, M.; MacArthur, I.C.; Maag, J.; Chamorro, R.; Munoz-Perez, N.; Puiggròs, M.; Dorado Garcia, H.; et al. Extrachromosomal circular DNA drives oncogenic genome remodeling in neuroblastoma. Nat. Genet. 2020, 52, 29–34. [Google Scholar] [CrossRef]
- Cobrinik, D.; Ostrovnaya, I.; Hassimi, M.; Tickoo, S.K.; Cheung, I.Y.; Cheung, N.K. Recurrent pre-existing and acquired DNA copy number alterations, including focal TERT gains, in neuroblastoma central nervous system metastases. Genes Chromosomes Cancer 2013, 52, 1150–1166. [Google Scholar] [CrossRef]
- Mall, M.; Kareta, M.S.; Chanda, S.; Ahlenius, H.; Perotti, N.; Zhou, B.; Grieder, S.D.; Ge, X.; Drake, S.; Ang, C.E.; et al. Myt1l safeguards neuronal identity by actively repressing many non-neuronal fates. Nature 2017, 544, 245–249. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.C.; Wang, H.F.; Yuan, Z.N. Runx2 induces bone osteolysis by transcriptional suppression of TSSC1. Biochem. Biophys. Res. Commun. 2013, 438, 635–639. [Google Scholar] [CrossRef] [PubMed]
- Gershlick, D.C.; Schindler, C.; Chen, Y.; Bonifacino, J.S. TSSC1 is novel component of the endosomal retrieval machinery. Mol. Biol. Cell. 2016, 27, 2867–2878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Che, Y.; Siprashvili, Z.; Kovalski, J.R.; Jiang, T.; Wozniak, G.; Elcavage, L.; Khavari, P.A. KRAS regulation by small non-coding RNAs and SNARE proteins. Nat. Commun. 2019, 10, 5118. [Google Scholar] [CrossRef] [PubMed]
- Brady, S.W.; Liu, Y.; Ma, X.; Gout, A.M.; Hagiwara, K.; Zhou, X.; Wang, J.; Macias, M.; Chen, X.; Easton, J.; et al. Pan-neuroblastoma analysis reveals age- and signature-associated driver alterations. Nat. Commun. 2020, 11, 5183. [Google Scholar] [CrossRef]
- Durbin, A.D.; Zimmerman, M.W.; Dharia, N.V.; Abraham, B.J.; Iniguez, A.B.; Weichert-Leahey, N.; He, S.; Krill-Burger, J.M.; Root, D.E.; Vazquez, F.; et al. Selective gene dependencies in MYCN-amplified neuroblastoma include the core transcriptional regulatory circuitry. Nat. Genet. 2018, 50, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
























{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cangelosi et al. [33] | E-MTAB-1781 | SEQC-498 | ||||
|---|---|---|---|---|---|---|
| Patient Characteristics | N | % | N | % | N | % |
| Age at diagnosis | ||||||
| <18 months | 449 | 57.1 | 431 | 60.8 | 305 | 61.2 |
| ≥18 months | 337 | 42.9 | 278 | 39.2 | 198 | 38.8 |
| MYCN status | ||||||
| Not amplified | 629 | 80.0 | 581 | 82.0 | 401 | 80.5 |
| Amplified | 153 | 19.5 | 122 | 17.2 | 92 | 18.5 |
| Missing | 4 | 0.5 | 6 | 0.8 | 5 | 1.0 |
| INSS Stage | ||||||
| 1 | 143 | 18.2 | 159 | 22.4 | 121 | 24.3 |
| 2 | 125 | 15.9 | 118 | 16.6 | 78 | 15.7 |
| 3 | 105 | 13.4 | 93 | 13.1 | 63 | 12.7 |
| 4 | 320 | 40.7 | 259 | 36.5 | 183 | 36.8 |
| 4s | 92 | 11.7 | 80 | 11.3 | 53 | 10.6 |
| Missing | 1 | 0.1 | 0 | 0.0 | 0 | 0.0 |
| Events | 320 | 40.7 1 | 256 2 | 36.1 | 183 | 36.9 |
| Deaths | 229 | 29.1 | 161 | 22.7 | 105 | 21.1 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Median | <0.001 | 0.022 | |||||
| ≤4.544 | 393/151 | 1 | ref | 1 | Ref | ||
| >4.544 | 393/78 | 0.46 | 0.35–0.60 | 0.72 | 0.54–0.96 | ||
| Tertiles | <0.001 | 0.010 | |||||
| ≤4.299 | 262/105 | 1 | ref | 1 | ref | ||
| 4.299–4.759 | 262/81 | 0.73 | 0.55–0.98 | 1.0 | 0.75–1.4 | ||
| >4.759 | 262/43 | 0.36 | 0.25–0.51 | 0.61 | 0.42–0.88 | ||
| Continuous variable | 786/229 | 0.55 | 0.45–0.66 | <0.001 | 0.73 | 0.59–0.90 | 0.004 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Median | <0.001 | 0.129 | |||||
| ≤4.544 | 378/189 | 1 | ref | 1 | ref | ||
| >4.544 | 391/131 | 0.61 | 0.49–0.76 | 0.83 | 0.66–1.1 | ||
| Tertiles | <0.001 | 0.115 | |||||
| ≤4.299 | 247/127 | 1 | ref | 1 | ref | ||
| 4.299–4.759 | 260/112 | 0.83 | 0.64–1.1 | 1.1 | 0.82–1.4 | ||
| >4.759 | 262/81 | 0.54 | 0.41–0.71 | 0.79 | 0.59–1.1 | ||
| Continuous variable | 769/320 | 0.62 | 0.52–0.75 | <0.001 | 0.81 | 0.67–0.98 | 0.029 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Median | <0.001 | 0.004 | |||||
| ≤4.316 | 393/171 | 1 | ref | 1 | ref | ||
| >4.316 | 393/58 | 0.28 | 0.21–0.38 | 0.64 | 0.46–0.87 | ||
| Tertiles | <0.001 | 0.006 | |||||
| ≤3.991 | 262/128 | 1 | ref | 1 | ref | ||
| 3.991–4.589 | 262/69 | 0.47 | 0.35–0.63 | 0.80 | 0.59–1.1 | ||
| >4.589 | 262/32 | 0.20 | 0.13–0.29 | 0.53 | 0.35–0.80 | ||
| Continuous variable | 786/229 | 0.53 | 0.47–0.60 | <0.001 | 0.73 | 0.62–0.86 | <0.001 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Median | <0.001 | 0.003 | |||||
| ≤4.316 | 383/212 | 1 | ref | 1 | ref | ||
| >4.316 | 386/108 | 0.41 | 0.33–0.52 | 0.68 | 0.53–0.88 | ||
| Tertiles | <0.001 | 0.002 | |||||
| ≤3.991 | 253/151 | 1 | ref | 1 | ref | ||
| 3.991–4.589 | 257/107 | 0.64 | 0.50–0.82 | 0.90 | 0.70–1.2 | ||
| >4.589 | 259/62 | 0.31 | 0.23–0.42 | 0.57 | 0.41–0.79 | ||
| Continuous variable | 769/320 | 0.59 | 0.52–0.66 | <0.001 | 0.75 | 0.65–0.86 | <0.001 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Median | <0.001 | <0.001 | |||||
| ≤3.346 | 393/75 | 1 | ref | 1 | ref | ||
| >3.346 | 393/154 | 2.4 | 1.8–3.1 | 1.7 | 1.3–2.2 | ||
| Tertiles | <0.001 | 0.002 | |||||
| ≤3.162 | 262/43 | 1 | ref | 1 | ref | ||
| 3.162–3.520 | 262/66 | 1.7 | 1.1–2.5 | 1.5 | 1.0–2.2 | ||
| >3.520 | 262/120 | 3.5 | 2.5–5.0 | 1.9 | 1.3–2.7 | ||
| Continuous variable | 786/229 | 2.93 | 2.27–3.79 | <0.001 | 1.48 | 1.16–1.90 | 0.002 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Median | <0.001 | 0.178 | |||||
| ≤1.877 | 383/138 | 1 | ref | 1 | ref | ||
| >1.877 | 386/182 | 1.5 | 1.2–1.8 | 1.2 | 0.93–1.5 | ||
| Tertiles | <0.001 | 0.376 | |||||
| ≤3.162 | 256/89 | 1 | ref | 1 | ref | ||
| 3.162–3.520 | 257/97 | 1.2 | 0.87–1.5 | 1.1 | 0.82–1.5 | ||
| >3.520 | 256/134 | 1.8 | 1.4–2.3 | 1.2 | 0.92–1.6 | ||
| Continuous variable | 769/320 | 1.83 | 1.45–2.33 | <0.001 | 1.2 | 0.96–1.5 | 0.103 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.005 | 0.820 | |||||
| ≤0.535 | 248/40 | 1 | ref | 1 | ref | ||
| >0.535 | 250/65 | 1.7 | 1.2–2.6 | 1.0 | 0.69–1.6 | ||
| Tertiles | 0.191 | 0.451 | |||||
| ≤0.438 | 166/31 | 1 | ref | 1 | ref | ||
| 0.438–0.638 | 166/32 | 1.0 | 0.63–1.7 | 0.74 | 0.44–1.2 | ||
| >0.638 | 166/42 | 1.5 | 0.92–2.3 | 0.93 | 0.57–1.5 | ||
| Continuous variable | 498/105 | 3.07 | 1.67–5.7 | <0.001 | 1.26 | 0.68–2.34 | 0.460 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.073 | 0.977 | |||||
| ≤0.535 | 248/82 | 1 | ref | 1 | ref | ||
| >0.535 | 250/101 | 1.3 | 0.97–1.7 | 1.0 | 0.73–1.4 | ||
| Tertiles | 0.883 | 0.358 | |||||
| ≤0.438 | 166/63 | 1 | ref | 1 | ref | ||
| 0.438–0.638 | 166/60 | 0.92 | 0.64–1.3 | 0.79 | 0.55–1.1 | ||
| >0.638 | 166/60 | 0.97 | 0.68–1.4 | 0.79 | 0.54–1.1 | ||
| Continuous variable | 498/183 | 1.44 | 0.86–2.40 | 0.173 | 0.91 | 0.54–1.52 | 0.723 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.020 | 0.498 | |||||
| ≤1.877 | 393/99 | 1 | ref | 1 | ref | ||
| >1.877 | 393/130 | 1.4 | 1.0–1.8 | 0.91 | 0.70–1.2 | ||
| Tertiles | 0.132 | 0.612 | |||||
| ≤1.541 | 262/66 | 1 | ref | 1 | ref | ||
| 1.541–2.250 | 262/74 | 1.1 | 0.81–1.56 | 1.0 | 0.73–1.4 | ||
| >2.250 | 262/89 | 1.4 | 1.0–1.9 | 0.88 | 0.64–1.2 | ||
| Continuous variable | 786/229 | 1.08 | 0.96–1.23 | 0.194 | 0.99 | 0.86–1.12 | 0.827 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.015 | 0.910 | |||||
| ≤1.877 | 387/141 | 1 | ref | 1 | Ref | ||
| >1.877 | 382/179 | 1.3 | 1.1–1.6 | 0.99 | 0.79–1.2 | ||
| Tertiles | 0.125 | 0.759 | |||||
| ≤1.541 | 258/94 | 1 | ref | 1 | ref | ||
| 1.541–2.250 | 258/105 | 1.1 | 0.85–1.5 | 1.1 | 0.80–1.4 | ||
| >2.250 | 253/121 | 1.3 | 1.0–1.7 | 0.96 | 0.73–1.3 | ||
| Continuous variable | 769/320 | 1.09 | 0.98–1.21 | 0.120 | 1.01 | 0.91–1.12 | 0.840 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.510 | 0.517 | |||||
| ≤1.655 | 393/110 | 1 | ref | 1 | ref | ||
| >1.655 | 393/119 | 1.1 | 0.84–1.4 | 0.92 | 0.71–1.2 | ||
| Tertiles | 0.021 | 0.529 | |||||
| ≤1.193 | 262/80 | 1 | ref | 1 | ref | ||
| 1.193–2.144 | 262/61 | 0.71 | 0.51–0.99 | 0.82 | 0.59–1.2 | ||
| >2.144 | 262/88 | 1.1 | 0.81–1.5 | 0.90 | 0.66–1.2 | ||
| Continuous variable | 786/229 | 0.95 | 0.86–1.0 | 0.266 | 0.94 | 0.85–1.03 | 0.176 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.925 | 0.194 | |||||
| ≤1.655 | 382/157 | 1 | ref | 1 | ref | ||
| >1.655 | 387/163 | 0.99 | 0.79–1.2 | 0.86 | 0.69–1.1 | ||
| Tertiles | 0.024 | 0.188 | |||||
| ≤1.193 | 253/110 | 1 | ref | 1 | ref | ||
| 1.193–2.144 | 257/91 | 0.72 | 0.55–0.95 | 0.77 | 0.58–1.0 | ||
| >2.144 | 259/119 | 1.0 | 0.78–1.3 | 0.84 | 0.65–1.1 | ||
| Continuous variable | 769/320 | 0.94 | 0.86–1.03 | 0.223 | 0.93 | 0.85–1.02 | 0.123 |
| LOC339788 Expression Levels | |||||
|---|---|---|---|---|---|
| ≤0.01436 | >0.01436 | ||||
| Patient Characteristics | N | % | N | % | p |
| Age | 0.898 | ||||
| <18 months | 226 | 61.1 | 79 | 61.7 | |
| ≥18 months | 144 | 38.9 | 49 | 38.3 | |
| MYCN status | 0.024 | ||||
| Not amplified | 307 | 83.7 | 94 | 74.6 | |
| Amplified | 60 | 16.4 | 32 | 25.4 | |
| Stage | 0.498 | ||||
| Localized | 195 | 52.7 | 67 | 52.3 | |
| Stage 4 | 139 | 37.6 | 44 | 34.4 | |
| Stage 4S | 36 | 9.7 | 17 | 13.3 | |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Cut-off | 0.607 | 0.921 | |||||
| ≤0.01436 | 370/76 | 1 | ref | 1 | ref | ||
| >0.01436 | 128/29 | 1.1 | 0.73–1.7 | 0.98 | 0.63–1.5 | ||
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Cut-off | 0.261 | 0.471 | |||||
| ≤0.01436 | 370/131 | 1 | ref | 1 | ref | ||
| >0.01436 | 128/52 | 1.2 | 0.87–1.7 | 1.1 | 0.81–1.6 | ||
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.811 | 0.738 | |||||
| ≤4.029 | 393/114 | 1 | ref | 1 | ref | ||
| >4.029 | 393/115 | 1.0 | 0.80–1.3 | 0.95 | 0.73–1.3 | ||
| Tertiles | 0.058 | 0.367 | |||||
| ≤3.791 | 262/89 | 1 | ref | 1 | ref | ||
| 3.791–4.311 | 262/62 | 0.68 | 0.49–0.94 | 0.80 | 0.58–1.1 | ||
| >4.311 | 262/78 | 0.88 | 0.65–1.2 | 0.84 | 0.61–1.2 | ||
| Continuous variable | 786/229 | 0.97 | 0.83–1.1 | 0.672 | 0.89 | 0.78–1.0 | 0.118 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.398 | 0.265 | |||||
| ≤4.029 | 384/167 | 1 | ref | 1 | ref | ||
| >4.029 | 385/153 | 0.91 | 0.73–1.1 | 0.88 | 0.70–1.1 | ||
| Tertiles | 0.007 | 0.113 | |||||
| ≤3.791 | 253/127 | 1 | ref | 1 | ref | ||
| 3.791–4.311 | 260/91 | 0.65 | 0.50–0.86 | 0.77 | 0.58–1.0 | ||
| >4.311 | 256/102 | 0.78 | 0.60–1.0 | 0.79 | 0.60–1.0 | ||
| Continuous variable | 769/320 | 0.87 | 0.77–0.99 | 0.039 | 0.86 | 0.76–0.97 | 0.014 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.033 | 0.192 | |||||
| ≤−0.944 | 354/90 | 1 | ref | 1 | ref | ||
| >−0.944 | 355/71 | 0.71 | 0.52–0.97 | 0.81 | 0.59–1.1 | ||
| Tertiles | 0.066 | 0.578 | |||||
| ≤−1.303 | 236/62 | 1 | ref | 1 | ref | ||
| −1.303–−0.594 | 236/44 | 0.63 | 0.43–0.93 | 0.86 | 0.58–1.3 | ||
| >−0.594 | 237/55 | 0.79 | 0.55–1.1 | 0.83 | 0.57–1.2 | ||
| Continuous variable | 709/161 | 0.92 | 0.85–0.99 | 0.036 | 0.96 | 0.90–1.0 | 0.199 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.066 | 0.131 | |||||
| ≤−0.944 | 349/138 | 1 | ref | 1 | ref | ||
| >−0.944 | 346/118 | 0.79 | 0.62–1.0 | 0.82 | 0.64–1.1 | ||
| Tertiles | 0.088 | 0.166 | |||||
| ≤−1.303 | 231/96 | 1 | ref | 1 | ref | ||
| −1.303–−0.594 | 235/79 | 0.75 | 0.55–1.0 | 0.90 | 0.66–1.2 | ||
| >−0.594 | 229/81 | 0.75 | 0.56–1.0 | 0.75 | 0.55–1.0 | ||
| Continuous variable | 695/256 | 0.95 | 0.89–1.0 | 0.105 | 0.97 | 0.91–1.0 | 0.244 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Median | <0.001 | 0.075 | |||||
| ≤4.313 | 393/149 | 1 | ref | 1 | ref | ||
| >4.313 | 393/80 | 0.49 | 0.37–0.64 | 0.78 | 0.59–1.0 | ||
| Tertiles | <0.001 | 0.004 | |||||
| ≤4.102 | 262/113 | 1 | ref | 1 | ref | ||
| 4.102–4.512 | 262/67 | 0.55 | 0.40–0.74 | 1.0 | 0.75–1.4 | ||
| >4.512 | 262/49 | 0.38 | 0.27–0.53 | 0.60 | 0.42–0.84 | ||
| Continuous variable | 786/229 | 0.59 | 0.48–0.73 | <0.001 | 0.75 | 0.61–0.91 | 0.003 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Median | <0.001 | 0.064 | |||||
| ≤4.313 | 376/189 | 1 | ref | 1 | ref | ||
| >4.313 | 393/131 | 0.60 | 0.48–0.75 | 0.81 | 0.64–1.0 | ||
| Tertiles | <0.001 | 0.060 | |||||
| ≤4.102 | 245/135 | 1 | ref | 1 | ref | ||
| 4.102–4.512 | 262/98 | 0.62 | 0.48–0.81 | 0.94 | 0.72–1.2 | ||
| >4.512 | 262/87 | 0.53 | 0.40–0.69 | 0.73 | 0.55–0.96 | ||
| Continuous variable | 769/320 | 0.62 | 0.50–0.76 | <0.001 | 0.77 | 0.64–0.92 | 0.004 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/D | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.010 | 0.153 | |||||
| ≤3.311 | 393/99 | 1 | ref | 1 | ref | ||
| >3.311 | 393/130 | 1.4 | 1.1–1.8 | 1.2 | 0.93–1.6 | ||
| Tertiles | <0.001 | 0.301 | |||||
| ≤3.074 | 261/71 | 1 | ref | 1 | ref | ||
| 3.074–3.585 | 263/62 | 0.83 | 0.59–1.2 | 1.3 | 0.90–1.8 | ||
| >3.585 | 262/96 | 1.5 | 1.1–2.0 | 1.2 | 0.90–1.7 | ||
| Continuous variable | 786/229 | 1.26 | 1.16–1.37 | <0.001 | 0.96 | 0.89–1.03 | 0.231 |
| Univariable Analysis | Multivariable Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Gene Expression | N/E | HR | 95% CI | p | HR | 95% CI | p |
| Median | 0.063 | 0.340 | |||||
| ≤3.311 | 376/146 | 1 | ref | 1 | ref | ||
| >3.311 | 393/174 | 1.2 | 0.99–1.5 | 1.1 | 0.89–1.4 | ||
| Tertiles | 0.008 | 0.183 | |||||
| ≤3.074 | 244/95 | 1 | ref | 1 | ref | ||
| 3.074–3.585 | 263/99 | 0.99 | 0.74–1.3 | 1.3 | 0.95–1.7 | ||
| >3.585 | 262/126 | 1.4 | 1.1–1.9 | 1.2 | 0.95–1.6 | ||
| Continuous variable | 769/320 | 1.17 | 1.09–1.26 | <0.001 | 0.98 | 0.91–1.05 | 0.574 |
| Case N° | Age at Onset (Months) | INSS Stage | INRG Stage | Subtype | MYCN Status | Percentage of TSSC1 Positive Cells | Relapse | Follow-Up | Disease State |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 35 | 4 | M | NB/GNBL | gain | 85 | yes | dead | |
| 2 | 15 | 4 | M | NB/GNBL | amp | 70 | yes | dead | |
| 3 | 49 | 4 | M | NB/GNBL | amp | 73 | yes | dead | |
| 4 | 36 | 4 | M | NB/GNBL | sc | 20 | no | alive | CR |
| 5 | 12 | 4 | M | NB/GNBL | sc | 15 | no | alive | CR |
| 6 | 11 | 4 | M | NB/GNBL | amp | 67 | yes | dead | |
| 7 | 18 | 4 | M | NB/GNBL | amp | 75 | yes | dead | |
| 8 | 22 | 4 | M | NB/GNBL | amp | 68 | yes | dead | |
| 9 | 7 | 4 | M | NB/GNBL | amp | 78 | no | dead | |
| 10 | 3 | 4 | M | NB/GNBL | sc | 12 | no | alive | CR |
| 11 | 47 | 4 | M | NB/GNBL | gain | 54 | yes | dead | |
| 12 | 9 | 4 | M | NB/GNBL | amp | 9 | no | alive | CR |
| 13 | 26 | 4 | M | NB/GNBL | amp | 62 | yes | dead | |
| 14 | 63 | 4 | M | NB NAS | amp | 78 | yes | dead | |
| 15 | 46 | 4 | M | NB/GNBL | amp | 64 | yes | dead | |
| 16 | 165 | 4 | M | NB/GNBL | sc | 11 | no | alive | CR |
| 17 | 114 | 4 | M | NB/GNBL | amp | 72 | yes | dead | |
| 18 | 23 | 4 | M | NB/GNBL | sc | 7 | no | alive | CR |
| 19 | 33 | 4 | M | NB/GNBL | sc | 13 | no | alive | CR |
| 20 | 32 | 4 | M | NB/GNBL | gain | 45 | yes | dead | |
| 21 | 45 | 4 | M | NB/GNBL | gain | 59 | yes | dead | |
| 22 | 28 | 4 | M | NB/GNBL | gain | 63 | yes | dead | |
| 23 | 57 | 4 | M | NB/GNBL | amp | 54 | no | alive | AD |
| 24 | 7 | 4 | M | NB/GNBL | sc | 6 | no | alive | CR |
| 25 | 28 | 4 | M | NB/GNBL | gain | 77 | yes | dead | |
| 26 | 54 | 4 | M | NB/GNBL | amp | 55 | yes | dead | |
| 27 | 55 | 4 | M | NB/GNBL | amp | 59 | no | dead | |
| 28 | 52 | 4 | M | NB/GNBL | gain | 62 | yes | dead | |
| 29 | 5 | 4 | M | NB/GNBL | amp | 4 | no | alive | CR |
| 30 | 15 | 4 | M | NB/GNBL | amp | 81 | yes | dead |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ognibene, M.; Amoroso, L.; Melchionda, F.; Cangelosi, D.; Zara, F.; Parodi, S.; Pezzolo, A. High Grade of Amplification of Six Regions on Chromosome 2p in a Neuroblastoma Patient with Very Poor Outcome: The Putative New Oncogene TSSC1. Cancers 2021, 13, 5792. https://doi.org/10.3390/cancers13225792
Ognibene M, Amoroso L, Melchionda F, Cangelosi D, Zara F, Parodi S, Pezzolo A. High Grade of Amplification of Six Regions on Chromosome 2p in a Neuroblastoma Patient with Very Poor Outcome: The Putative New Oncogene TSSC1. Cancers. 2021; 13(22):5792. https://doi.org/10.3390/cancers13225792
Chicago/Turabian StyleOgnibene, Marzia, Loredana Amoroso, Fraia Melchionda, Davide Cangelosi, Federico Zara, Stefano Parodi, and Annalisa Pezzolo. 2021. "High Grade of Amplification of Six Regions on Chromosome 2p in a Neuroblastoma Patient with Very Poor Outcome: The Putative New Oncogene TSSC1" Cancers 13, no. 22: 5792. https://doi.org/10.3390/cancers13225792
APA StyleOgnibene, M., Amoroso, L., Melchionda, F., Cangelosi, D., Zara, F., Parodi, S., & Pezzolo, A. (2021). High Grade of Amplification of Six Regions on Chromosome 2p in a Neuroblastoma Patient with Very Poor Outcome: The Putative New Oncogene TSSC1. Cancers, 13(22), 5792. https://doi.org/10.3390/cancers13225792