
Epidemiology of Kaposi’s Sarcoma

{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. History of KS: A Disease Understood Step by Step
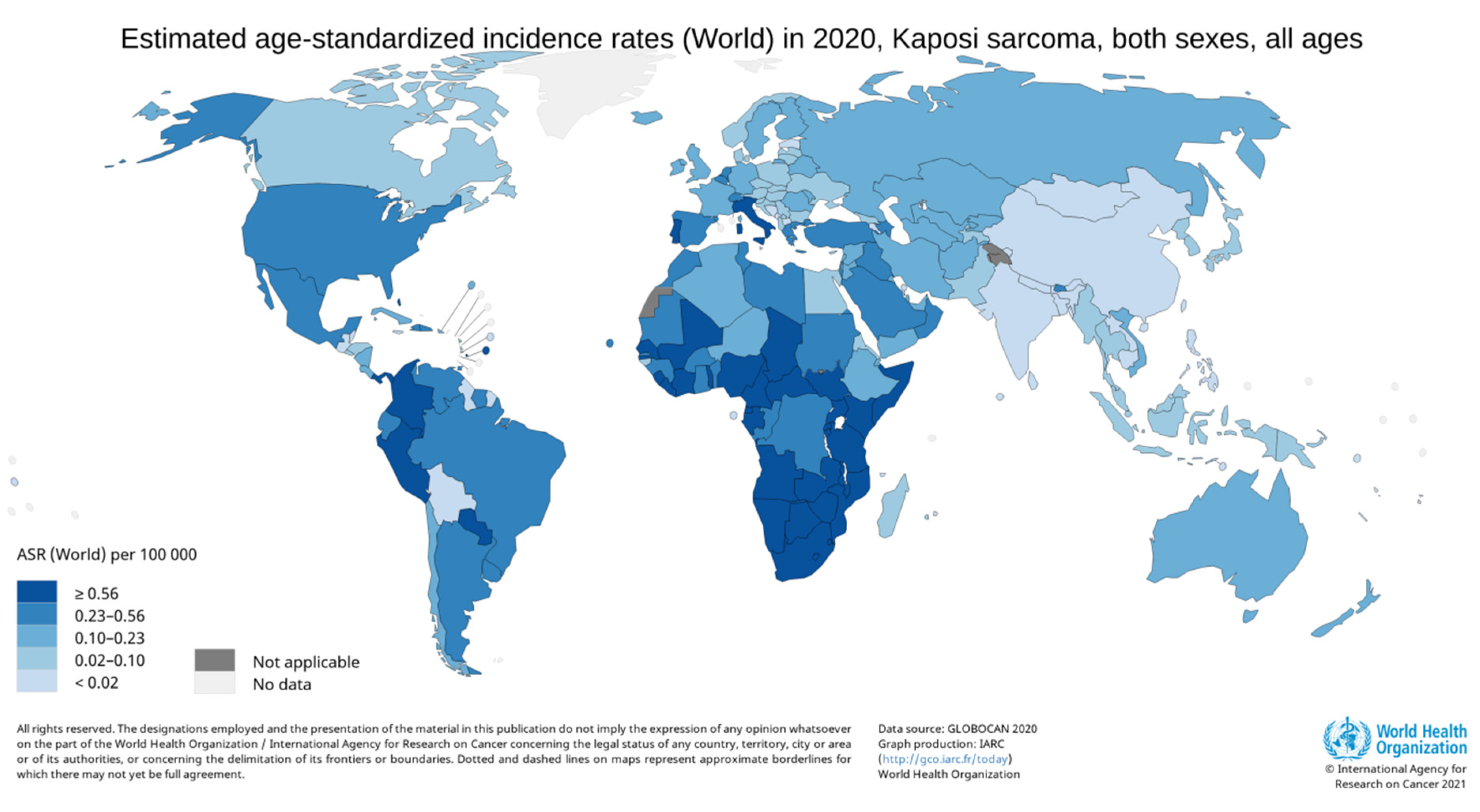
2. Geographical and Population Disparities
3. KS in PLHIV
3.1. Incidence and Risk vs. That in the General Population
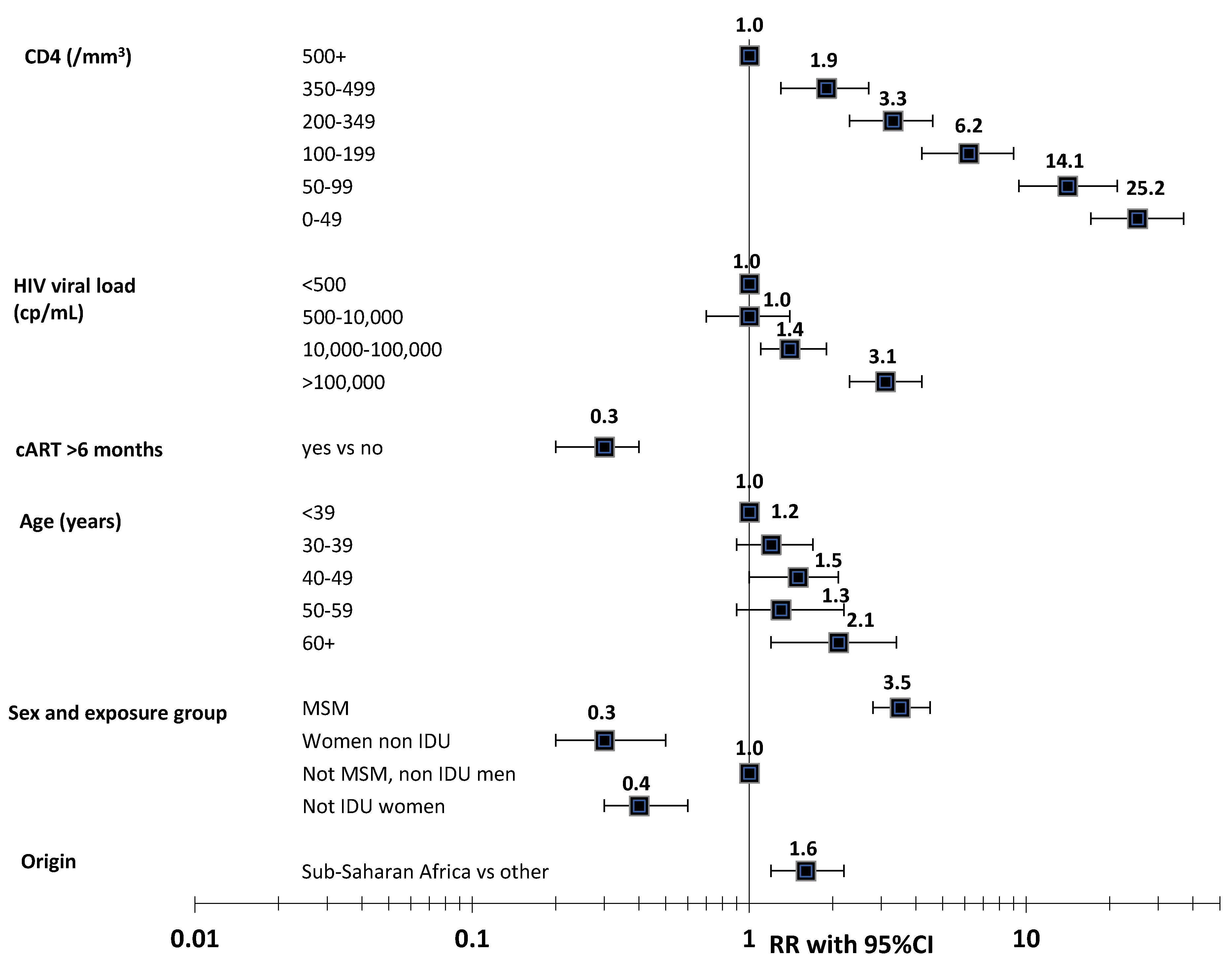
3.2. Immuno-Deficiency, HIV Viral Load, and CD4/CD8 Ratio
3.3. Immune Reconstitution Inflammatory Syndrome (IRIS)
3.4. Impact of Early cART Initiation on the Risk of KS
3.5. Age and KS: Little Evidence for Premature Aging in PLHIV
3.6. Treatment of KS in PLHIV
4. KS in Immune-Suppressed Transplanted Patients
5. The Other Forms of KS: The Classic KS and Endemic KS
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Friedman-Kien, A.E.; Saltzman, B.R. Clinical manifestations of classical, endemic African, and epidemic AIDS-associated Kaposi’s sarcoma. J. Am. Acad. Dermatol. 1990, 22 Pt 2, 1237–1250. [Google Scholar] [CrossRef]
- Penn, I. Kaposi’s Sarcoma in Transplant Recipients. Transplantation 1997, 64, 669–673. [Google Scholar] [CrossRef]
- Centers for Disease Control (CDC). Kaposi’s sarcoma and Pneumocystis pneumonia among homosexual men—New York City and California. Morb. Mortal Wkly. Rep. 1981, 30, 305–308. [Google Scholar]
- Hymes, K.; Cheung, T.; Greene, J.; Prose, N.; Marcus, A.; Ballard, H.; William, D.; Laubenstein, L. Kaposi’s Sarcoma in Homosexual Men—A Report of Eight Cases. Lancet 1981, 318, 598–600. [Google Scholar] [CrossRef]
- Chang, Y.; Cesarman, E.; Pessin, M.S.; Lee, F.; Culpepper, J.; Knowles, D.M.; Moore, P.S. Identification of herpesvirus-like DNA sequences in AIDS-associated Kaposi’s sarcoma. Science 1994, 266, 1865–1869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beral, V. Epidemiology of Kaposi’s sarcoma. Cancer Surv. 1991, 10, 5–22. [Google Scholar]
- Beral, V.; Peterman, T.A.; Berkelman, R.L.; Jaffe, H.W. Kaposi’s sarcoma among persons with AIDS: A sexually transmitted infection? Lancet 1990, 335, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Gao, S.J.; Kingsley, L.; Li, M.; Zheng, W.; Parravicini, C.; Ziegler, J.; Newton, R.; Rinaldo, C.R.; Saah, A.; Phair, J.; et al. KSHV antibodies among Americans, Italians and Ugandans with and without Kaposi’s sarcoma. Nat. Med. 1996, 2, 925–928. [Google Scholar] [CrossRef]
- Pauk, J.; Huang, M.-L.; Brodie, S.J.; Wald, A.; Koelle, D.; Schacker, T.; Celum, C.; Selke, S.; Corey, L. Mucosal Shedding of Human Herpesvirus 8 in Men. N. Engl. J. Med. 2000, 343, 1369–1377. [Google Scholar] [CrossRef]
- Martin, J.N.; Ganem, D.E.; Osmond, D.H.; Page, K.; Macrae, D.; Kedes, D.H. Sexual Transmission and the Natural History of Human Herpesvirus 8 Infection. N. Engl. J. Med. 1998, 338, 948–954. [Google Scholar] [CrossRef]
- Butler, L.M.; Were, W.A.; Balinandi, S.; Downing, R.; Dollard, S.C.; Neilands, T.B.; Gupta, S.; Rutherford, G.W.; Mermin, J. Human Herpesvirus 8 Infection in Children and Adults in a Population-based Study in Rural Uganda. J. Infect. Dis. 2011, 203, 625–634. [Google Scholar] [CrossRef] [Green Version]
- Dollard, S.C.; Butler, L.M.; Jones, A.M.G.; Mermin, J.H.; Chidzonga, M.; Chipato, T.; Shiboski, C.H.; Brander, C.; Mosam, A.; Kiepiela, P.; et al. Substantial regional differences in human herpesvirus 8 seroprevalence in sub-Saharan Africa: Insights on the origin of the “Kaposi’s sarcoma belt”. Int. J. Cancer 2010, 127, 2395–2401. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, M.J.; Schutz, C.; Barr, D.; Locketz, M.; Marshall, V.; Whitby, D.; A Katz, A.; Uldrick, T.; Meintjes, G.; Schäfer, G. The Contribution of Kaposi’s Sarcoma–Associated Herpesvirus to Mortality in Hospitalized Human Immunodeficiency Virus–Infected Patients Being Investigated for Tuberculosis in South Africa. J. Infect. Dis. 2019, 220, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Fang, Q.; Zuo, J.; Chen, Y.; Minhas, V.; Wood, C.; Zhang, T. Global epidemiology of human herpesvirus 8 in men who have sex with men: A systematic review and meta-analysis. J. Med. Virol. 2017, 90, 582–591. [Google Scholar] [CrossRef]
- Rohner, E.; Wyss, N.; Heg, Z.; Faralli, Z.; Mbulaiteye, S.M.; Novak, U.; Zwahlen, M.; Egger, M.; Bohlius, J. HIV and human herpesvirus 8 co-infection across the globe: Systematic review and meta-analysis. Int. J. Cancer 2015, 138, 45–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mercader, M.; Taddeo, B.; Panella, J.R.; Chandran, B.; Nickoloff, B.J.; Foreman, K.E. Induction of HHV-8 Lytic Cycle Replication by Inflammatory Cytokines Produced by HIV-1-Infected T Cells. Am. J. Pathol. 2000, 156, 1961–1971. [Google Scholar] [CrossRef] [Green Version]
- Caselli, E.; Galvan, M.; Santoni, F.; Rotola, A.; Caruso, A.; Cassai, E.; Di Luca, D. Human herpesvirus-8 (Kaposi’s sarcoma-associated virus) ORF50 increases in vitro cell susceptibility to human immunodeficiency virus type 1 infection. J. Gen. Virol. 2003, 84, 1123–1131. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- AIDS-Defining Cancer Project Working Group for IeDEA, Cohere in EuroCoord. Comparison of Kaposi Sarcoma Risk in Human Immunodeficiency Virus-Positive Adults Across 5 Continents: A Multiregional Multicohort Study. Clin. Infect. Dis. 2017, 65, 1316–1326. [Google Scholar] [CrossRef] [Green Version]
- Guiguet, M.; Boué, F.; Cadranel, J.; Lang, J.-M.; Rosenthal, E.; Costagliola, D. Effect of immunodeficiency, HIV viral load, and antiretroviral therapy on the risk of individual malignancies (FHDH-ANRS CO4): A prospective cohort study. Lancet Oncol. 2009, 10, 1152–1159. [Google Scholar] [CrossRef]
- Hleyhel, M.; Belot, A.; Bouvier, A.M.; Tattevin, P.; Pacanowski, J.; Genet, P.; De Castro, N.; Berger, J.-L.; Dupont, C.; Lavolé, A.; et al. Risk of AIDS-Defining Cancers Among HIV-1–Infected Patients in France Between 1992 and 2009: Results From the FHDH-ANRS CO4 Cohort. Clin. Infect. Dis. 2013, 57, 1638–1647. [Google Scholar] [CrossRef] [Green Version]
- Mocroft, A.; Kirk, O.; Clumeck, N.; Gargalianos-Kakolyris, P.; Trocha, H.; Chentsova, N.; Antunes, F.; Phillips, A.N.; Lundgren, J. The changing pattern of Kaposi sarcoma in patients with HIV, 1994-2003. Cancer 2004, 100, 2644–2654. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Chingonzoh, T.; Vuma, S.; Liu, B.; Chokunonga, E.; Ndlovu, N.; Borok, M. Changes in the Incidence of Cancer in Bulawayo, Zimbabwe over a 50-Year Period. Cancer Epidemiol. Biomarkers Prev. 2021, 30, 867–873. [Google Scholar] [CrossRef] [PubMed]
- Wabinga, H.R.; Nambooze, S.; Amulen, P.M.; Okello, C.; Mbus, L.; Parkin, D.M. Trends in the incidence of cancer in Kampala, Uganda 1991–2010. Int. J. Cancer 2013, 135, 432–439. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Revision of the CDC surveillance case definition for acquired immunodeficiency syndrome. Council of State and Territorial Epidemiologists; AIDS Program, Center for Infectious Diseases. MMWR Suppl. 1987, 36, 1S–15S. [Google Scholar]
- Centers for Disease Control and Prevention. Impact of the expanded AIDS surveillance case definition on AIDS case reporting-United States, first quarter, 1993. MMWR Morb. Mortal Wkly. Rep. 1993, 42, 308–310. [Google Scholar]
- Grabar, S.; Lanoy, E.; Allavena, C.; Mary-Krause, M.; Bentata, M.; Fischer, P.; Mahamat, A.; Rabaud, C.; Costagliola, D.; on behalf of the Clinical Epidemiology Group of the French Hospital Database on HIV. Causes of the first AIDS-defining illness and subsequent survival before and after the advent of combined antiretroviral therapy. HIV Med. 2008, 9, 246–256. [Google Scholar] [CrossRef]
- Elford, J.; McDonald, A.; Kaldor, J. Kaposi’s sarcoma as a sexually transmissible infection: An analysis of Australian AIDS surveillance data. The National HIV Surveillance Committee. AIDS 1993, 7, 1667–1671. [Google Scholar] [CrossRef]
- Grabar, S.; Abraham, B.; Mahamat, A.; Del Giudice, P.; Rosenthal, E.; Costagliola, D. Differential Impact of Combination Antiretroviral Therapy in Preventing Kaposi’s Sarcoma with and without Visceral Involvement. J. Clin. Oncol. 2006, 24, 3408–3414. [Google Scholar] [CrossRef]
- Grulich, A.E.; Li, Y.; McDonald, A.M.; Correll, P.K.; Law, M.G.; Kaldor, J.M. Decreasing rates of Kaposi’s sarcoma and non-Hodgkin’s lymphoma in the era of potent combination anti-retroviral therapy. AIDS 2001, 15, 629–633. [Google Scholar] [CrossRef]
- Hernández-Ramírez, R.U.; Shiels, M.S.; Dubrow, R.; Engels, E.A. Cancer risk in HIV-infected people in the USA from 1996 to 2012: A population-based, registry-linkage study. Lancet HIV 2017, 4, e495–e504. [Google Scholar] [CrossRef]
- Jacobson, L.P.; Yamashita, T.E.; Detels, R.; Margolick, J.B.; Chmiel, J.S.; Kingsley, L.A.; Melnick, S.; Muñoz, A. Impact of potent antiretroviral therapy on the incidence of Kaposi’s sarcoma and non-Hodgkin’s lymphomas among HIV-1-infected individuals. Multicenter AIDS Cohort Study. JAIDS 1999, 21 (Suppl. 1), S34–S41. [Google Scholar]
- Peprah, S.; Engels, E.A.; Horner, M.-J.; Monterosso, A.; Hall, H.I.; Johnson, A.S.; Pfeiffer, R.M.; Shiels, M.S. Kaposi Sarcoma Incidence, Burden, and Prevalence in United States People with HIV, 2000–2015. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1627–1633. [Google Scholar] [CrossRef] [PubMed]
- Patel, P.; Hanson, D.L.; Sullivan, P.S.; Novak, R.M.; Moorman, A.C.; Tong, T.C.; Holmberg, S.D.; Brooks, J.T. Incidence of types of cancer among HIV-infected persons compared with the general population in the United States, 1992–2003. Ann. Intern. Med. 2008, 148, 728–736. [Google Scholar] [CrossRef] [PubMed]
- Robbins, H.A.; Shiels, M.S.; Pfeiffer, R.M.; Engels, E.A. Epidemiologic contributions to recent cancer trends among HIV-infected people in the United States. AIDS 2014, 28, 881–890. [Google Scholar] [CrossRef] [Green Version]
- Luo, Q.; Johnson, A.S.; Hall, H.I.; Cahoon, E.K.; Shiels, M. Kaposi Sarcoma Rates Among Persons Living With Human Immunodeficiency Virus in the United States: 2008—2016. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Poizot-Martin, I.; Lions, C.; Cheret, A.; Rey, D.; Duvivier, C.; Jacomet, C.; Allavena, C.; Huleux, T.; Bani-Sadr, F.; Obry-Roguet, V.; et al. Kaposi sarcoma in people living with HIV: Incidence and associated factors in a French cohort between 2010 and 2015. AIDS 2020, 34, 569–577. [Google Scholar] [CrossRef]
- Mocroft, A.; Furrer, H.J.; Miro, J.M.; Reiss, P.; Mussini, C.; Kirk, O.; Abgrall, S.; Ayayi, S.; Bartmeyer, B.; Braun, D.; et al. The incidence of AIDS-defining illnesses at a current CD4 count >/= 200 cells/muL in the post-combination antiretroviral therapy era. Clin. Infect. Dis. 2013, 57, 1038–1047. [Google Scholar] [CrossRef] [Green Version]
- Silverberg, M.J.; Chao, C.; Leyden, W.A.; Xu, L.; Horberg, M.A.; Klein, D.; Towner, W.J.; Dubrow, R.; Quesenberry, C.P., Jr.; Neugebauer, R.S.; et al. HIV infection, immunodeficiency, viral replication, and the risk of cancer. Cancer Epidemiol. Biomark. Prev. 2011, 20, 2551–2559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubrow, R.; Qin, L.; Lin, H.; Hernández-Ramírez, R.U.; Neugebauer, R.S.; Leyden, W.; Althoff, K.N.; Achenbach, C.J.; Hessol, N.A.; Modur, S.P.; et al. Association of CD4+ T-cell Count, HIV-1 RNA Viral Load, and Antiretroviral Therapy With Kaposi Sarcoma Risk Among HIV-infected Persons in the United States and Canada. JAIDS J. Acquir. Immune Defic. Syndr. 2017, 75, 382–390. [Google Scholar] [CrossRef]
- Silverberg, M.J.; Lau, B.; Achenbach, C.J.; Jing, Y.; Althoff, K.N.; D’Souza, G.; Engels, E.A.; Hessol, N.A.; Brooks, J.T.; Burchell, A.N.; et al. Cumulative Incidence of Cancer Among Persons With HIV in North America: A Cohort Study. Ann. Intern. Med. 2015, 163, 507–518. [Google Scholar] [CrossRef] [Green Version]
- Park, L.S.; Tate, J.P.; Sigel, K.; Brown, S.T.; Crothers, K.; Gibert, C.; Goetz, M.B.; Rimland, D.; Rodriguez-Barradas, M.C.; Bedimo, R.J.; et al. Association of Viral Suppression With Lower AIDS-Defining and Non-AIDS-Defining Cancer Incidence in HIV-Infected Veterans: A Prospective Cohort Study. Ann. Intern. Med. 2018, 169, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Mani, D.; Neil, N.; Israel, R.; Aboulafia, D.M. A Retrospective Analysis of AIDS-Associated Kaposi’s Sarcoma in Patients With Undetectable HIV Viral Loads and CD4 Counts Greater Than 300 cells/mm3. J. Int. Assoc. Physicians AIDS Care 2009, 8, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Palich, R.; Veyri, M.; Valantin, M.A.; Marcelin, A.G.; Guihot, A.; Pourcher, V.; Jary, A.; Solas, C.; Makinson, A.; Poizot-Martin, I.; et al. Recurrence and Occurrence of Kaposi’s Sarcoma in Patients Living with Human Immunodeficiency Virus (HIV) and on Antiretroviral Therapy, Despite Suppressed HIV Viremia. Clin. Infect. Dis. 2020, 70, 2435–2438. [Google Scholar] [CrossRef]
- Séverin, D.; Bessaoud, F.; Meftah, N.; Du Thanh, A.; Tretarre, B.; Guillot, B.; Makinson, A. A comparative study of classic and HIV-viremic and aviremic AIDS Kaposi sarcoma. AIDS 2020, 35, 399–405. [Google Scholar] [CrossRef]
- Caby, F.; Guiguet, M.; Weiss, L.; Winston, A.; Miro, J.M.; Konopnicki, D.; Le Moing, V.; Bonnet, F.; Reiss, P.; Mussini, C.; et al. CD4/CD8 Ratio and the Risk of Kaposi Sarcoma or Non-Hodgkin Lymphoma in the Context of Efficiently Treated Human Immunodeficiency Virus (HIV) Infection: A Collaborative Analysis of 20 European Cohort Studies. Clin. Infect. Dis. 2020, 73, 50–59. [Google Scholar] [CrossRef]
- A French, M.; Price, P.; Stone, S.F. Immune restoration disease after antiretroviral therapy. AIDS 2004, 18, 1615–1627. [Google Scholar] [CrossRef]
- Cancer Project Working Group for the Collaboration of Observational HIV Epidemiological Research Europe Study in EuroCoord. Changing Incidence and Risk Factors for Kaposi Sarcoma by Time Since Starting Antiretroviral Therapy: Collaborative Analysis of 21 European Cohort Studies. Clin. Infect. Dis. 2016, 63, 1373–1379. [Google Scholar] [CrossRef] [Green Version]
- Lacombe, J.-M.; Boue, F.; Grabar, S.; Viget, N.; Gazaignes, S.; Lascaux-Cametz, A.-S.; Pacanowski, J.; Partisani, M.; Launay, O.; Matheron, S.; et al. Risk of Kaposi sarcoma during the first months on combination antiretroviral therapy. AIDS 2013, 27, 635–643. [Google Scholar] [CrossRef] [Green Version]
- Lodi, S.; Guiguet, M.; Costagliola, D.; Fisher, M.; De Luca, A.; Porter, K. The CASCADE Collaboration Kaposi Sarcoma Incidence and Survival Among HIV-Infected Homosexual Men After HIV Seroconversion. J. Natl. Cancer Inst. 2010, 102, 784–792. [Google Scholar] [CrossRef] [Green Version]
- Group, I.S.S.; Lundgren, J.D.; Babiker, A.G.; Gordin, F.; Emery, S.; Grund, B.; Sharma, S.; Avihingsanon, A.; Cooper, D.A.; Fätkenheuer, G.; et al. Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. N. Engl. J. Med. 2015, 373, 795–807. [Google Scholar]
- Chammartin, F.; Lodi, S.; Logan, R.; Ryom, L.; Mocroft, A.; Kirk, O.; d’Arminio Monforte, A.; Reiss, P.; Phillips, A.; El-Sadr, W.; et al. Risk for Non-AIDS-Defining and AIDS-Defining Cancer of Early Versus Delayed Initiation of Antiretroviral Therapy: A Multinational Prospective Cohort Study. Ann. Intern. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, M.J.; Leyden, W.; Hernandez-Ramirez, R.U.; Qin, L.; Lin, H.; Justice, A.C.; Hessol, N.A.; Achenbach, C.J.; D’Souza, G.; Engels, E.A.; et al. Timing of Antiretroviral Therapy Initiation and Risk of Cancer among Persons Living with HIV. Clin. Infect. Dis. 2020, 11, 1900–1909. [Google Scholar]
- Rasmussen, L.D.; May, M.T.; Kronborg, G.; Larsen, C.S.; Pedersen, C.; Gerstoft, J.; Obel, N. Time trends for risk of severe age-related diseases in individuals with and without HIV infection in Denmark: A nationwide population-based cohort study. Lancet HIV 2015, 2, e288–e298. [Google Scholar] [CrossRef]
- Shiels, M.S.; Pfeiffer, R.M.; Engels, E.A. Age at Cancer Diagnosis Among Persons With AIDS in the United States. Ann. Intern. Med. 2010, 153, 452. [Google Scholar] [CrossRef]
- Dupin, N. Update on oncogenesis and therapy for Kaposi sarcoma. Curr. Opin. Oncol. 2020, 32, 122–128. [Google Scholar] [CrossRef]
- Lebbe, C.; Garbe, C.; Stratigos, A.J.; Harwood, C.; Peris, K.; del Marmol, V.; Malvehy, J.; Zalaudek, I.; Hoeller, C.; Dummer, R. Diagnosis and treatment of Kaposi’s sarcoma: European consensus-based interdisciplinary guideline (EDF/EADO/EORTC). Eur. J. Cancer 2019, 114, 117–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martellotta, F.; Berretta, M.; Vaccher, E.; Schioppa, O.; Zanet, E.; Tirelli, U. AIDS-Related Kaposis Sarcoma: State of the Art and Therapeutic Strategies. Curr. HIV Res. 2009, 7, 634–638. [Google Scholar] [CrossRef]
- Yarchoan, R.; Uldrick, T.S. HIV-Associated Cancers and Related Diseases. N. Engl. J. Med. 2018, 378, 1029–1041. [Google Scholar] [CrossRef]
- Au, E.; Wong, G.; Chapman, J.R. Cancer in kidney transplant recipients. Nat. Rev. Nephrol. 2018, 14, 508–520. [Google Scholar] [CrossRef] [PubMed]
- Engels, E.A.; Pfeiffer, R.M.; Fraumeni, J.F.; Kasiske, B.L.; Israni, A.K.; Snyder, J.J.; Wolfe, R.A.; Goodrich, N.P.; Bayakly, A.R.; Clarke, C.A.; et al. Spectrum of Cancer Risk Among US Solid Organ Transplant Recipients. JAMA 2011, 306, 1891–1901. [Google Scholar] [CrossRef]
- Grulich, A.E.; van Leeuwen, M.T.; Falster, M.O.; Vajdic, C.M. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef]
- Vajdic, C.M.; McDonald, S.P.; McCredie, M.R.E.; van Leeuwen, M.; Stewart, J.H.; Law, M.; Chapman, J.R.; Webster, A.; Kaldor, J.M.; Grulich, A.E. Cancer Incidence Before and After Kidney Transplantation. JAMA 2006, 296, 2823–2831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vajdic, C.M.; van Leeuwen, M.T. Cancer incidence and risk factors after solid organ transplantation. Int. J. Cancer 2009, 125, 1747–1754. [Google Scholar] [CrossRef] [PubMed]
- Taborelli, M.; Piselli, P.; Ettorre, G.M.; Lauro, A.; Galatioto, L.; Baccarani, U.; Rendina, M.; Shalaby, S.; Petrara, R.; Nudo, F.; et al. Risk of virus and non-virus related malignancies following immunosuppression in a cohort of liver transplant recipients. Italy, 1985–2014. Int. J. Cancer 2018, 143, 1588–1594. [Google Scholar] [CrossRef] [PubMed]
- Lebbe, C.; Legendre, C.; Frances, C. Kaposi sarcoma in transplantation. Transplant. Rev. 2008, 22, 252–261. [Google Scholar] [CrossRef]
- Cahoon, E.K.; Linet, M.S.; Clarke, C.A.; Pawlish, K.S.; Engels, E.A.; Pfeiffer, R.M. Risk of Kaposi sarcoma after solid organ transplantation in the United States. Int. J. Cancer 2018, 143, 2741–2748. [Google Scholar] [CrossRef] [Green Version]
- Piselli, P.; Taborelli, M.; Cimaglia, C.; Serraino, D.; Italian, T.; Cancer Cohort, S. Decreased incidence of Kaposi sarcoma after kidney transplant in Italy and role of mTOR-inhibitors: 1997–2016. Int. J. Cancer 2019, 145, 597–598. [Google Scholar] [CrossRef]
- Chiereghin, A.; Barozzi, P.; Petrisli, E.; Piccirilli, G.; Gabrielli, L.; Riva, G.; Potenza, L.; Cappelli, G.; De Ruvo, N.; Libri, I.; et al. Multicenter Prospective Study for Laboratory Diagnosis of HHV8 Infection in Solid Organ Donors and Transplant Recipients and Evaluation of the Clinical Impact After Transplantation. Transplantation 2017, 101, 1935–1944. [Google Scholar] [CrossRef] [PubMed]
- Lebbe, C.; Porcher, R.; Marcelin, A.-G.; Agbalika, F.; Dussaix, E.; Samuel, D.; Varnous, S.; Euvrard, S.; Bigorie, A.; Creusvaux, H.; et al. Human Herpesvirus 8 (HHV8) Transmission and Related Morbidity in Organ Recipients. Arab. Archaeol. Epigr. 2012, 13, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Cesarman, E.; Damania, B.; Krown, S.E.; Martin, J.; Bower, M.; Whitby, D. Kaposi sarcoma. Nat. Rev. Dis. Primers 2019, 5, 9. [Google Scholar] [CrossRef]
- Cottoni, F.; De Marco, R.; Montesu, M. Classical Kaposi’s sarcoma in north-east Sardinia: An overview from 1977 to 1991. Br. J. Cancer 1996, 73, 1132–1133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grulich, A.; Beral, V.; Swerdlow, A. Kaposi’s sarcoma in England and Wales before the AIDS epidemic. Br. J. Cancer 1992, 66, 1135–1137. [Google Scholar] [CrossRef] [Green Version]
- Denis, D.; Seta, V.; Regnier-Rosencher, E.; Kramkimel, N.; Chanal, J.; Avril, M.F.; Dupin, N. A fifth subtype of Kaposi’s sarcoma, classic Kaposi’s sarcoma in men who have sex with men: A cohort study in Paris. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1377–1384. [Google Scholar] [CrossRef]
- Pelser, C.; Dazzi, C.; Graubard, B.I.; Lauria, C.; Vitale, F.; Goedert, J.J. Risk of Classic Kaposi Sarcoma with Residential Exposure to Volcanic and Related Soils in Sicily. Ann. Epidemiol. 2009, 19, 597–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pelser, C.; Vitale, F.; Whitby, D.; Graubard, B.I.; Messina, A.; Gafà, L.; Brown, E.E.; Anderson, L.; Romano, N.; Lauria, C.; et al. Socio-economic and other correlates of Kaposi sarcoma-associated herpesvirus seroprevalence among older adults in Sicily. J. Med. Virol. 2009, 81, 1938–1944. [Google Scholar] [CrossRef] [Green Version]
- Ziegler, J.; Newton, R.; Bourboulia, D.; Casabonne, D.; Beral, V.; Mbidde, E.; Carpenter, L.; Reeves, G.; Parkin, D.M.; Wabinga, H.; et al. Risk factors for Kaposi’s sarcoma: A case-control study of HIV-seronegative people in Uganda. Int. J. Cancer 2002, 103, 233–240. [Google Scholar] [CrossRef]
- Masala, M.V.; Carcassi, C.; Cottoni, F.; Mulargia, M.; Contu, L.; Cerimele, D. Classic Kaposi’s sarcoma in Sardinia: HLA positive and negative associations. Int. J. Dermatol. 2005, 44, 743–745. [Google Scholar] [CrossRef]
- Blumenthal, M.J.; Castro, E.M.C.; Whitby, D.; Katz, A.A.; Schäfer, G. Evidence for altered host genetic factors in KSHV infection and KSHV -related disease development. Rev. Med. Virol. 2020, 31, e2160. [Google Scholar] [CrossRef] [PubMed]
- Benajiba, L.; Lambert, J.; La Selva, R.; Cochereau, D.; Baroudjian, B.; Roux, J.; Le Goff, J.; Pages, C.; Battistella, M.; Delyon, J.; et al. Systemic Treatment Initiation in Classical and Endemic Kaposi’s Sarcoma: Risk Factors and Global Multi-State Modelling in a Monocentric Cohort Study. Cancers 2021, 13, 2519. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grabar, S.; Costagliola, D. Epidemiology of Kaposi’s Sarcoma. Cancers 2021, 13, 5692. https://doi.org/10.3390/cancers13225692
Grabar S, Costagliola D. Epidemiology of Kaposi’s Sarcoma. Cancers. 2021; 13(22):5692. https://doi.org/10.3390/cancers13225692
Chicago/Turabian StyleGrabar, Sophie, and Dominique Costagliola. 2021. "Epidemiology of Kaposi’s Sarcoma" Cancers 13, no. 22: 5692. https://doi.org/10.3390/cancers13225692
APA StyleGrabar, S., & Costagliola, D. (2021). Epidemiology of Kaposi’s Sarcoma. Cancers, 13(22), 5692. https://doi.org/10.3390/cancers13225692