1. Introduction
The standard treatment for locally advanced non-small cell lung cancer (LA-NSCLC) is concurrent chemoradiotherapy [
1]. Intensity-modulated radiotherapy (IMRT) is the state-of-the-art radiation technique, allowing optimal shaping of the delivered dose to the target. IMRT has improved outcomes compared to conformal radiotherapy, but side effects are still common and potentially severe [
2]. Decreasing the radiation dose to organs at risk (OARs) is desirable both for toxicity reduction and the potential for dose escalation [
1,
3].
The aim of radiotherapy treatment planning is to establish treatment unit settings for each patient that will result in a high-quality dose distribution, i.e., a high dose inside the target volume and limited dose outside, especially in the OARs. IMRT treatment plans are generated using a cost function that defines the planning objectives for the target, OARs and other tissues, and their relative weights. A mathematical optimizer derives patient-specific beam intensity profiles that minimize the cost function value. In manual IMRT treatment planning, the general approach is to begin the plan generation for a new patient using a tumor-site-specific template for the cost function. In an iterative trial-and-error process, the objectives and weights are then adapted by the manual planner to account for the patient’s anatomy. For fixed-beam IMRT treatment in the thorax, the beam angles should also be individually tuned, as IMRT with carefully selected beam angles can reduce OAR doses compared to volumetric modulated arc therapy (VMAT) or IMRT with non-optimized beam angles [
4]. In clinical routine, time pressure limits the possibility to test many different objective and beam angle settings, and the planner’s experience or skills may affect the quality of the plans. A number of studies have demonstrated that manually created plans may be suboptimal [
5,
6,
7,
8,
9].
In recent years, several systems for automated treatment planning have been presented. Compared to manual planning, automated planning can considerably increase the plan quality while dramatically reducing the planning workload [
7].
Erasmus-iCycle, developed at the Erasmus University Medical Center (Erasmus MC, Rotterdam, The Netherlands), is a system for automated multi-criterial treatment planning that can generate beam profiles for pre-selected beam directions, but it also features integrated beam profile and beam angle optimization (BAO) [
10,
11,
12,
13,
14,
15,
16]. With appropriate treatment-site-specific configuration (creation of a “wish-list”), the generated Pareto-optimal plans are also clinically favorable. Erasmus-iCycle generates plans using fluence map optimization (FMO), but there is no consecutive segmentation, and therefore the plans are not directly deliverable. For the generation of clinically deliverable plans at Erasmus MC, Erasmus-iCycle is used as a pre-optimizer, with consecutive automatic reconstruction of FMO plans into segmented plans in the Monaco treatment planning system (TPS) (Elekta AB, Stockholm, Sweden). For this purpose, patient-specific Monaco optimization templates are created based on the achieved constraint and objective values in the Erasmus-iCycle FMO plan. Several publications have demonstrated the effectiveness of this approach in reducing OAR doses and planning time for different treatment sites [
17,
18,
19,
20,
21], including VMAT of LA-NSCLC [
8]. The Erasmus-iCycle wish-list-based lexicographic optimization approach for automated multi-criterial treatment planning has recently been adopted by a commercial party [
22].
The Eclipse TPS (Varian Medical Systems, Inc., Palo Alto, CA, USA) features the RapidPlan system for automated knowledge-based treatment planning, whereby a library of previous treatment plans is used to predict feasible patient-specific OAR dose-volume histograms (DVHs) for new patients [
23]. The predicted DVHs are converted into optimization parameters for automatic generation of deliverable treatment plans. A limitation of RapidPlan for automated IMRT planning for LA-NSCLC is that it does not feature patient-specific BAO. Therefore, the beam configuration must be determined manually by trial-and-error.
While treatment planning systems featuring advanced BAO are not commercially available, BAO methods have been investigated for their use in radiotherapy of lung cancer. Yuan et al. used a wide range of lung tumors to tune a BAO system for coplanar configurations, and applied it for more complex, non-coplanar plans [
24]. Amit et al. presented a learning-based method which was applied for various thoracic indications [
25]. In both studies, beam angle and beam profile optimization were not integrated; first, patient-specific beam angles were established, followed by IMRT optimization for the selected (fixed) angles. The results showed that plans with optimized beam angles had similar quality to clinical plans with manually selected beam angles.
The aim in this study was to automatically create IMRT plans with integrated optimization of beam angles for a prospective database of LA-NSCLC patients, in order to improve plan quality compared to manually created plans and to investigate the impact of beam angles on plan quality. For this purpose, Erasmus-iCycle was coupled with Eclipse to establish the novel “iCE” system. In iCE, Erasmus-iCycle is used as a pre-optimizer to automatically generate an initial Pareto-optimal FMO treatment plan with optimized beam angles for each patient. The OAR DVHs of this plan are converted into patient-specific optimization parameters for automated generation of the final deliverable plan in Eclipse. Both iCE plans and autoplans using the manually selected beam angles were compared to the manually generated, clinically delivered plans. Finally, iCE was used to investigate the effect of changing the number of IMRT beams.
2. Materials and Methods
2.1. Patients and Clinical Treatment Planning
Twenty-five consecutive patients with stage IIB-IIIC non-small cell lung cancer were prospectively included in this study. One patient with stage IVA, who had a single brain metastasis surgically removed prior to radiotherapy, received radiotherapy according to the protocol for LA-NSCLC and was also included. All patients received IMRT and concurrent or sequential chemotherapy at Haukeland University Hospital (HUH) between October 2019 and August 2021. The study was approved by the regional committee for medical and health research ethics (protocol code 2019/749) and all participants provided their informed consent.
All patients had both a 10-phase 4DCT and a deep inspiration breath-hold (DIBH) CT at planning. Treatment plans were created on the average intensity projection (AIP) of the 4DCT and treatment was given in free breathing (FB) conditions as a standard. However, for patients with very large breathing motion or where lung dose constraints could not be met with the AIP, the treatment plans were created on the DIBH CT instead (four patients).
The responsible oncologist delineated the gross tumor volumes (GTVs) for the primary tumor and lymph nodes according to ESTRO guidelines [
26]. For FB treatment, the internal GTVs (IGTVs) included the GTV positions on all 4DCT phases. For DIBH treatment, three repeated DIBH scans were taken at planning and the IGTVs encompassed the GTV positions on all three scans. The clinical target volume (CTV) was defined by expanding the IGTV by 5 mm without extending into uninvolved organs such as bone, heart, esophagus and major vessels. A 5 mm isotropic margin from the CTV was used to define the planning target volume (PTV). As OARs, the lungs, heart, esophagus, spinal canal and brachial plexus (if relevant) were delineated according to RTOG guidelines [
27].
The clinical plans (CLIN) were manually created by expert planners in Eclipse v. 15.6 or 16.1 using the Photon Optimizer algorithm for optimization and the Acuros External Beam algorithm for dose calculation. All plans included 6 coplanar IMRT beams with beam angles based on a template that was individually adapted. In accordance with national guidelines, the prescribed dose was 60 or 66 Gy for concomitant treatment (depending on lung function, lung dose and proximity of the brachial plexus to the PTV) and 70 Gy for sequential treatment, all administered in 2 Gy fractions. The plans were normalized to the median dose in the PTV. The dose constraints applied for planning are provided in
Table 1.
2.2. iCE Treatment Planning
2.2.1. Erasmus-iCycle Wish-List Creation and FMO Plan Generation
A detailed description of Erasmus-iCycle functionality and wish-list creation can be found elsewhere [
10,
28]. In this study, an Erasmus-iCycle wish-list for LA-NSCLC was established and tuned according to clinical priorities at HUH. An oncologist (IMS) and an expert planner (THS) were involved in the evaluation of treatment plans during this process. In the first phase of tuning, five of the patients treated in FB with 66 Gy were used. The PTV coverage and high dose conformity were kept similar to the clinical plans, while the dose to the OARs and undefined normal tissue was minimized. The wish-list was then applied for an additional four patients with a 60 Gy prescription and/or DIBH CT, and some final adjustments were made.
In the final wish-list, hard constraints were used for the maximum dose to the spinal canal, brachial plexus and PTV, and for an external ring to prevent high entrance doses. Target and OAR objectives were added with the following order of priority (in line with clinical priorities): PTV coverage, lung D
mean, heart D
mean and esophagus D
mean. In addition, constraints and objectives were applied for normal tissue at specified distances from the PTV to steer conformity. The full wish-list is provided in
Table 2.
In the multi-criterial plan generation, the objective functions are consecutively minimized following the allotted priorities. After the minimization of an objective function, a constraint is added to the problem to avoid quality loss for this objective when minimizing the following lower priority objectives. Two rounds of consecutive minimizations of objective functions are applied. In the first round, the constraint that is added after an objective minimization is the Goal value (second to last column in
Table 2), if it could be obtained, regardless of the possibility for further improvement. If the Goal value is not achieved, the obtained objective value, with some relaxation, is added as a constraint. In the second round, all objectives without a Sufficient value (last column in
Table 2) are minimized to the fullest extent, following the order of priority. In this way, the Goal and Sufficient values make sure undesired and unnecessary greediness in minimizing objectives is avoided, leaving room for minimizing lower priority objectives [
10].
The candidate beam angles for BAO were in the range of 140–40° for right-sided tumors and 320–220° for left-sided tumors with 5° spacing.
2.2.2. Generation of the Final iCE Plan Based on an Initial Erasmus-iCycle FMO Plan
The Erasmus-iCycle FMO plan was used to create a patient-specific objective template for automated generation of the final deliverable plan in Eclipse. This was performed automatically by a script that moved information from the OAR DVHs in .csv format into an objective template in .xml format (see
Supplementary Materials). For each OAR involved, a line objective was created. Line objectives are defined by a collection of dose-volume pairs and limit the dose for all volume levels [
29]. The distance between dose-volume points defining the line was set to 0.7 Gy. For the PTV objectives, the same fixed settings as in the clinical plans were used. Priorities and normal tissue objective settings were kept constant after tuning based on the first five patients.
Table 3 shows the final template that was used for all of the patients.
The generated objective templates as well as the optimized beam angles from Erasmus-iCycle were used for automated IMRT plan optimization in Eclipse, with no manual fine-tuning. The applied Eclipse version was the same as the version used for clinical planning. The final iCE plans were visually inspected to ensure that the high-dose conformity and the dose to undefined normal tissue was acceptable and comparable to the CLIN plans.
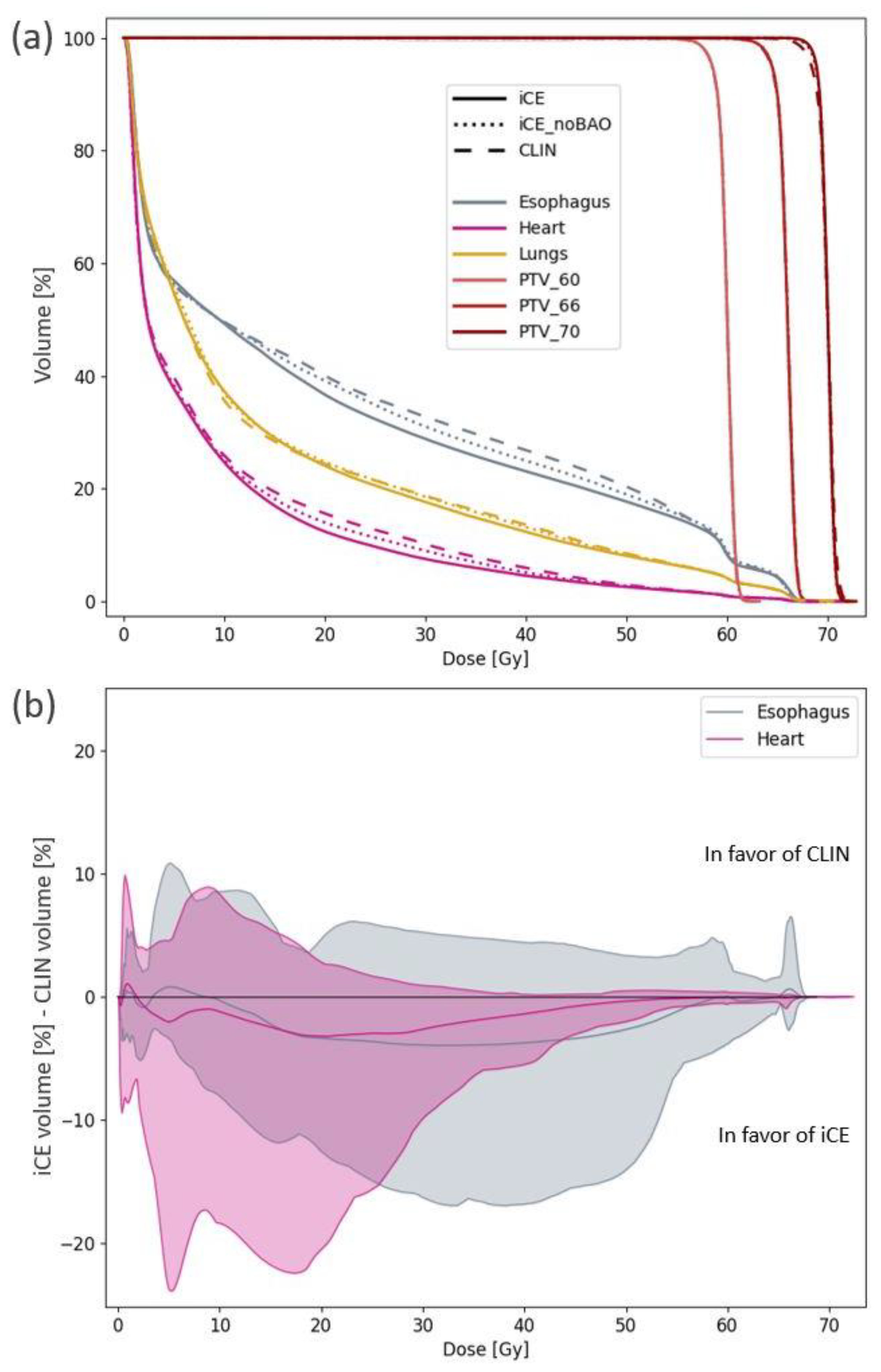
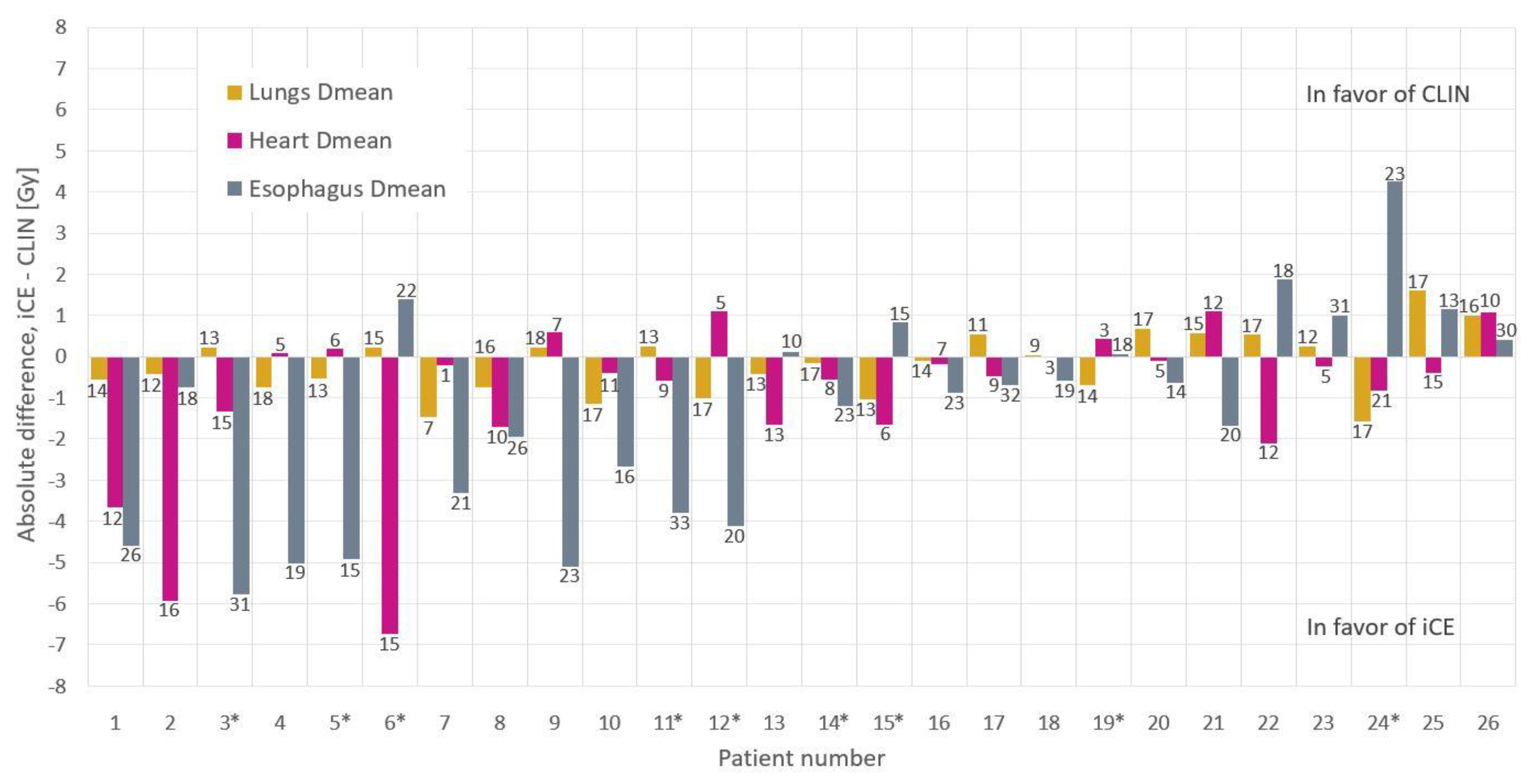
2.3. Comparison of iCE and CLIN Plans
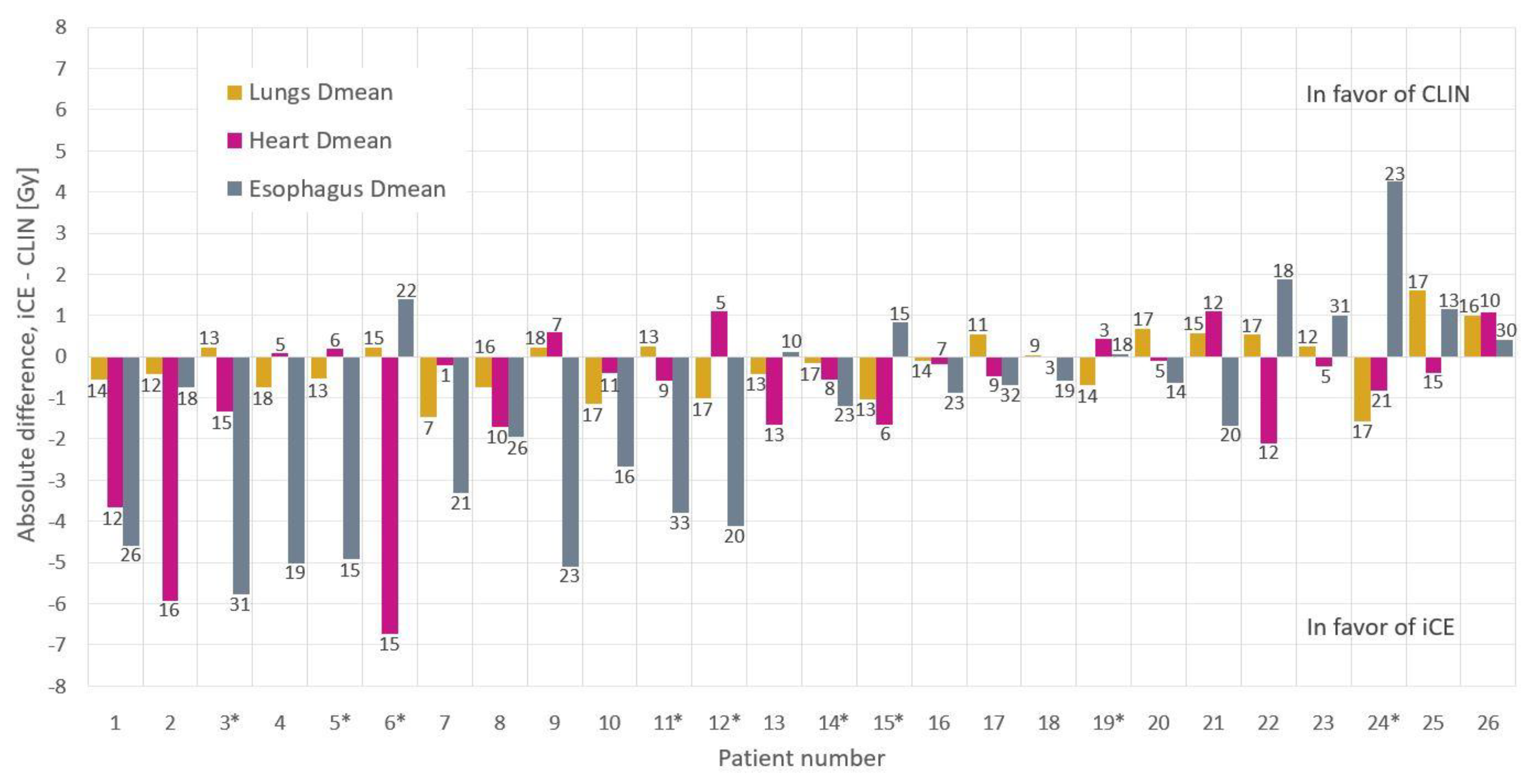
For each patient, a 6-beam iCE plan (same beam number as clinically used) was generated, and compared to the corresponding CLIN plan using relevant dose-volume metrics for the target and OARs. The mean dose to the lungs, heart and esophagus are commonly reported parameters related to toxicity, and were therefore used for evaluation of per-patient differences. To separately assess the benefit of BAO in iCE, a second iCE plan (iCE_noBAO) was generated for each patient, using the same beam angles as the CLIN plan, i.e., BAO in iCE was switched off.
2.4. Planning Times
The manual planning time was estimated from discussions with three treatment planners involved in clinical LA-NSCLC planning. The hands-on time in iCE planning, related to starting autoplanning and transfer of data between systems, was recorded.
2.5. Dosimetric QA of Plan Deliverability
For 10 randomly selected patients, the deliverability of the iCE plans was evaluated following the current clinical quality assurance (QA) procedure for this diagnosis at HUH. Electronic Portal Imaging Device measurements were performed, followed by analysis in the Portal Dosimetry system in Eclipse. A gamma passing rate of 95%, with a global criterion of 3%/3 mm, was required. In addition, the number of monitor units (MUs) in CLIN and iCE plans were compared.
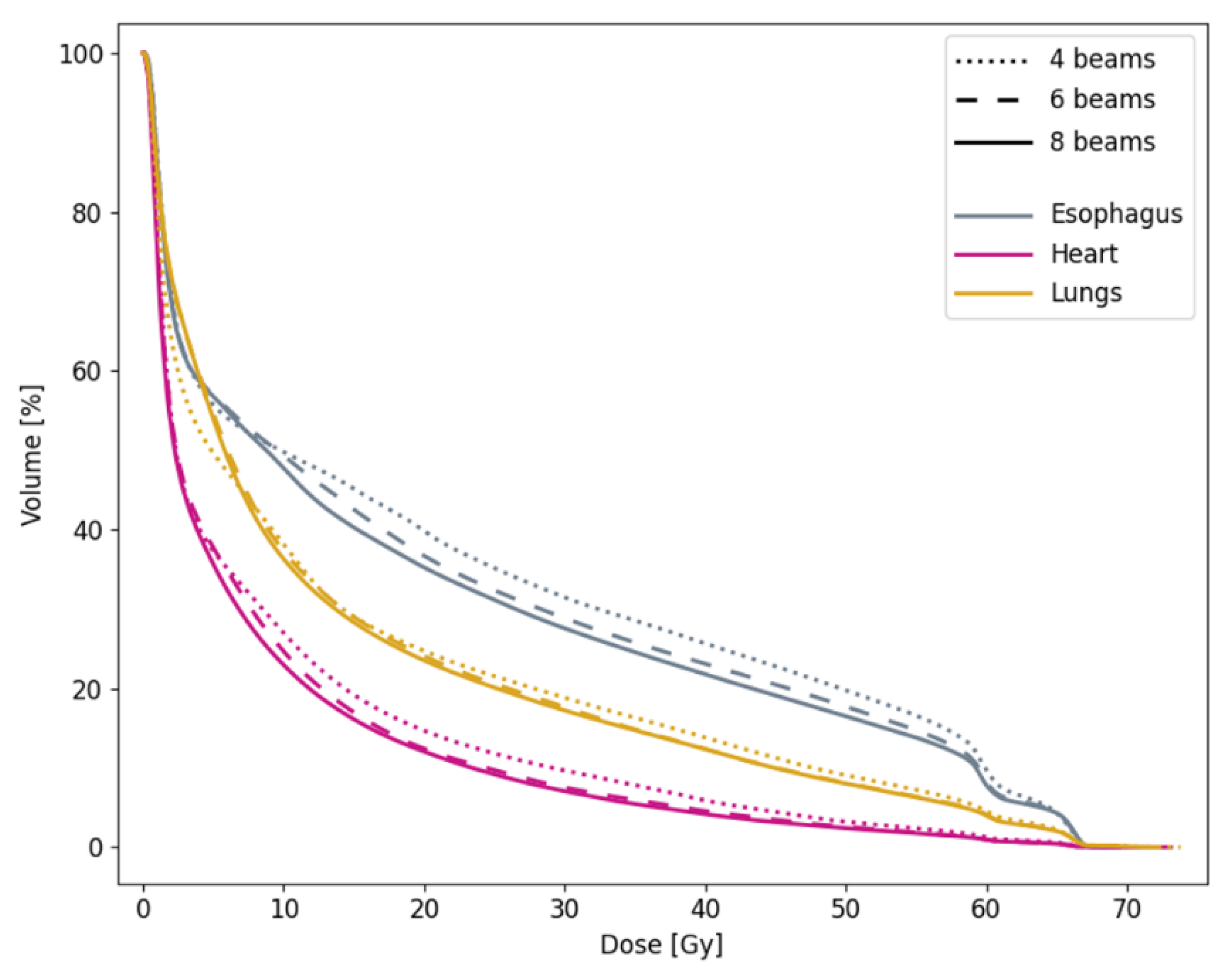
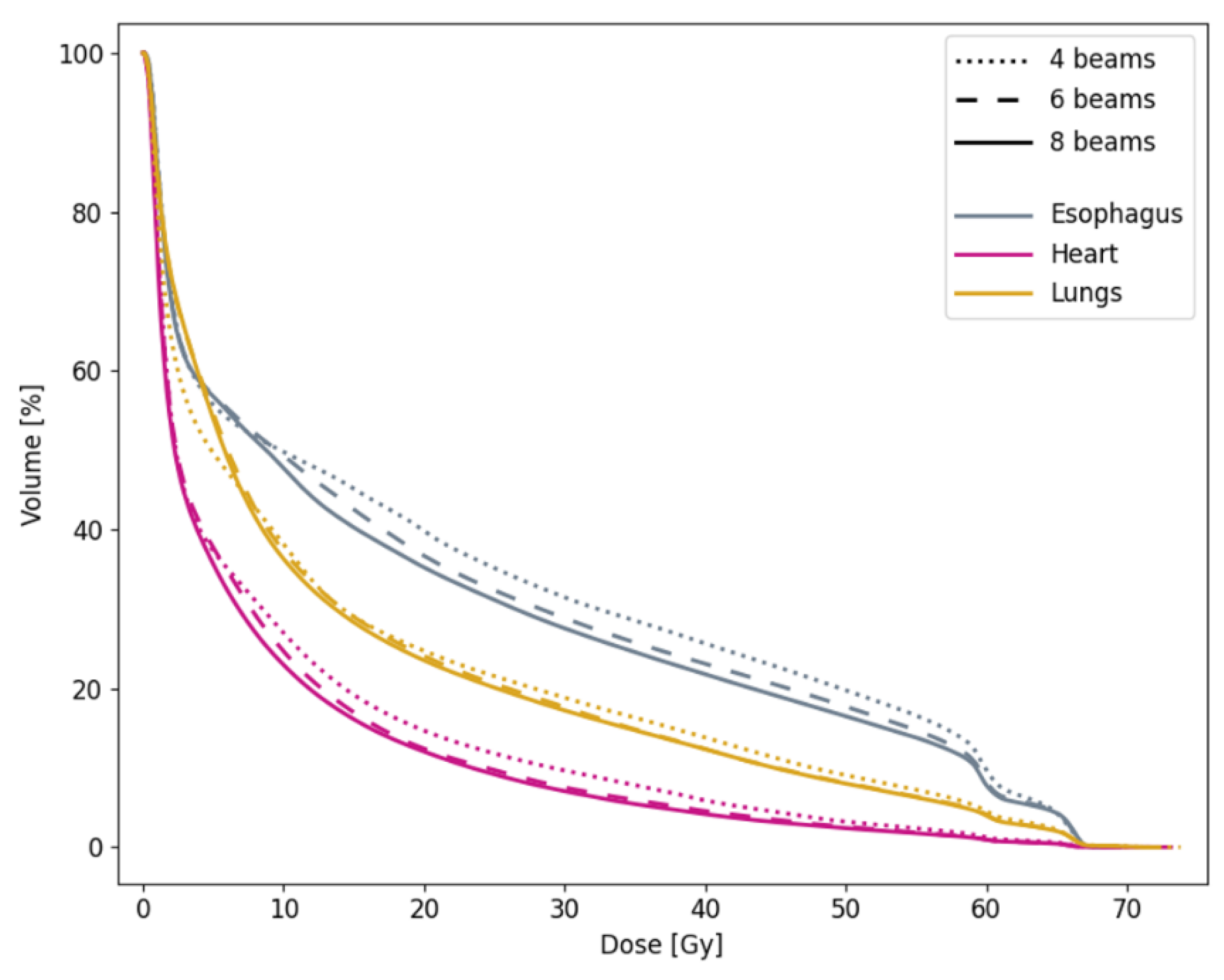
2.6. 6-Beam vs. 4- and 8-Beam iCE
In addition to the 6-beam plans, iCE was also used to generate plans with 4 and 8 beams, to validate the clinical use of 6 beams for all patients. Relevant target and OAR dose-volume metrics were compared for the different numbers of beams.
2.7. Statistical Analysis
The two-tailed Wilcoxon signed-rank test was used for the statistical testing of dose-volume parameters for CLIN vs. iCE and iCE_noBAO plans, and 6-beam vs. 4- and 8-beam plans. p-values ≤ 0.05 were considered as statistically significant.
4. Discussion
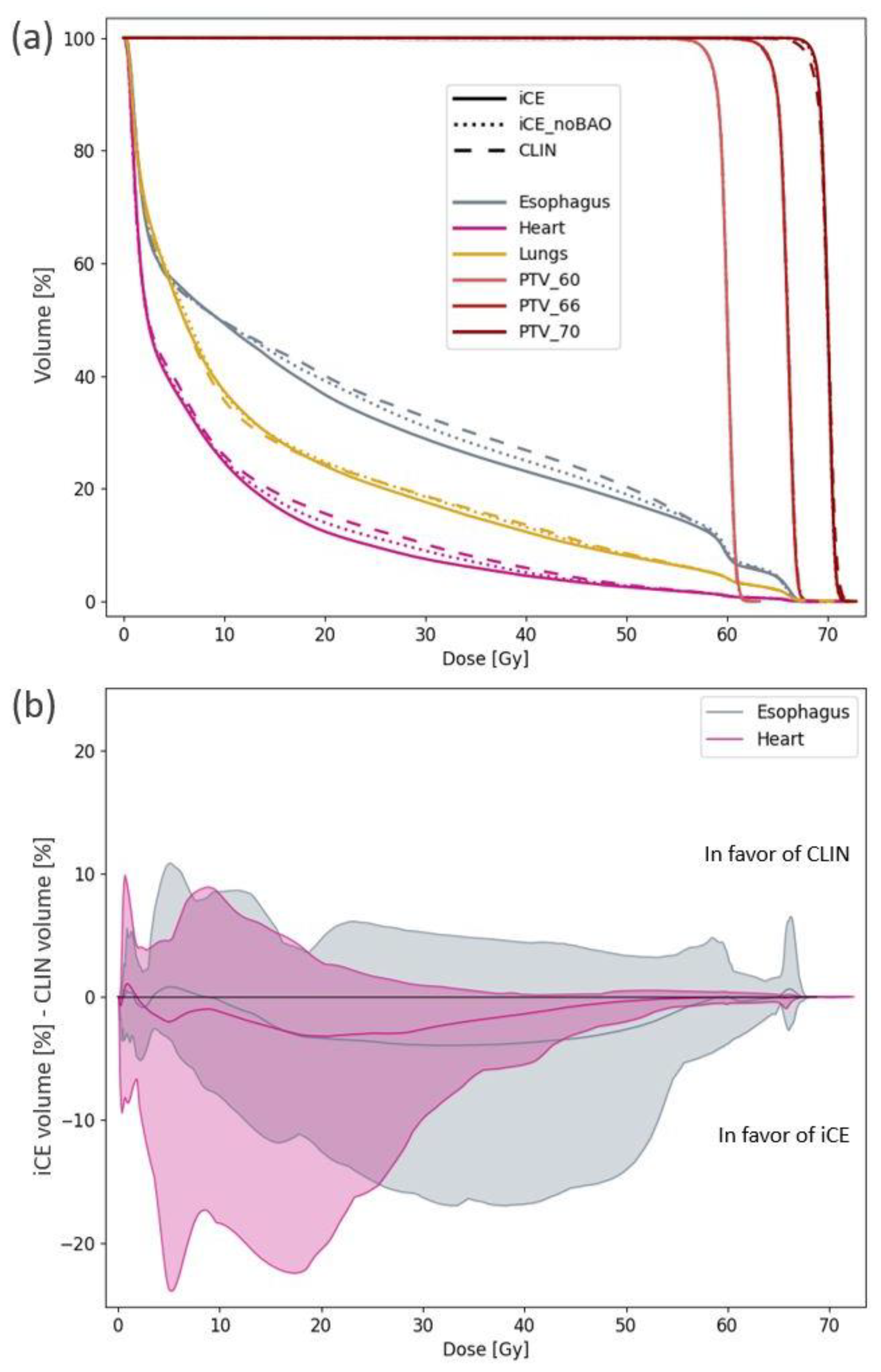
The novel iCE system for automated multi-criterial treatment planning with integrated BAO was developed, and used to investigate opportunities for OAR sparing in LA-NSCLC patients, and to systematically investigate the impact of beam angles on the radiotherapy dose. Compared to clinical plans, significant reductions in heart Dmean and V30Gy and esophagus Dmean and V20Gy were achieved with iCE. When using iCE with integrated patient-specific BAO, OAR sparing was found to be superior compared to using iCE for clinically applied beam angles. Increasing the number of optimized beams can improve OAR sparing. On average, differences in OAR sparing were found to be larger between 4 and 6 beams than between 6 and 8. The impact of the beam number varied largely between patients, and for some patients, changing the number of beams did not have a clinically relevant impact on the dose to any OAR.
While the reductions with iCE compared to CLIN in median D
mean for OARs were 0.5–1.8 Gy, a substantial sparing of >5 Gy was seen for the heart and esophagus for individual patients. This confirms one of the main strengths of automated planning; the ability to achieve a more homogeneous plan quality by avoiding occasional highly suboptimal plans. Bradley et al. reported an association between increased heart V
30Gy and increased risk of death, and Dess et al. found that mean heart dose, V
5Gy and V
30Gy were associated with grade ≥3 cardiac events [
31,
32]. Wijsman et al. reported on a correlation between mean esophagus dose and grade ≥2 acute esophageal toxicity [
33]. These correlations suggest that the observed reductions in heart D
mean and V
30Gy and esophagus D
mean with iCE compared to CLIN are of clinical importance. Only minor differences were observed for lung dose, possibly because the lungs received the most attention in clinical planning. The dose to the spinal canal and brachial plexus were not studied in detail, as reductions below the maximum dose constraints are not considered a priority. An additional advantage of iCE compared to manual planning is the dramatic decrease in hands-on planning time, as the trial-and-error process of finding objectives and beam angles manually is avoided.
A previous study using Erasmus-iCycle for LA-NSCLC found reductions in the average D
mean of the lungs, heart and esophagus of 0.9, 1.5 and 3.6 Gy for automatically generated VMAT plans compared to manually created IMRT plans [
8]. Although not directly comparable to our results, as the dose prescription, clinical priorities, delivery technique and TPS differed, the potential for reducing OAR doses for most patients with automated planning was found in both studies. The same has been found for other autoplanning strategies, including knowledge-based planning in Eclipse and multi-criteria optimization in RayStation (RaySearch Laboratories, Stockholm, Sweden) [
9,
23]. These findings highlight the potential of improving the plan quality in LA-NSCLC by increasing the availability, integration and utilization of autoplanning systems.
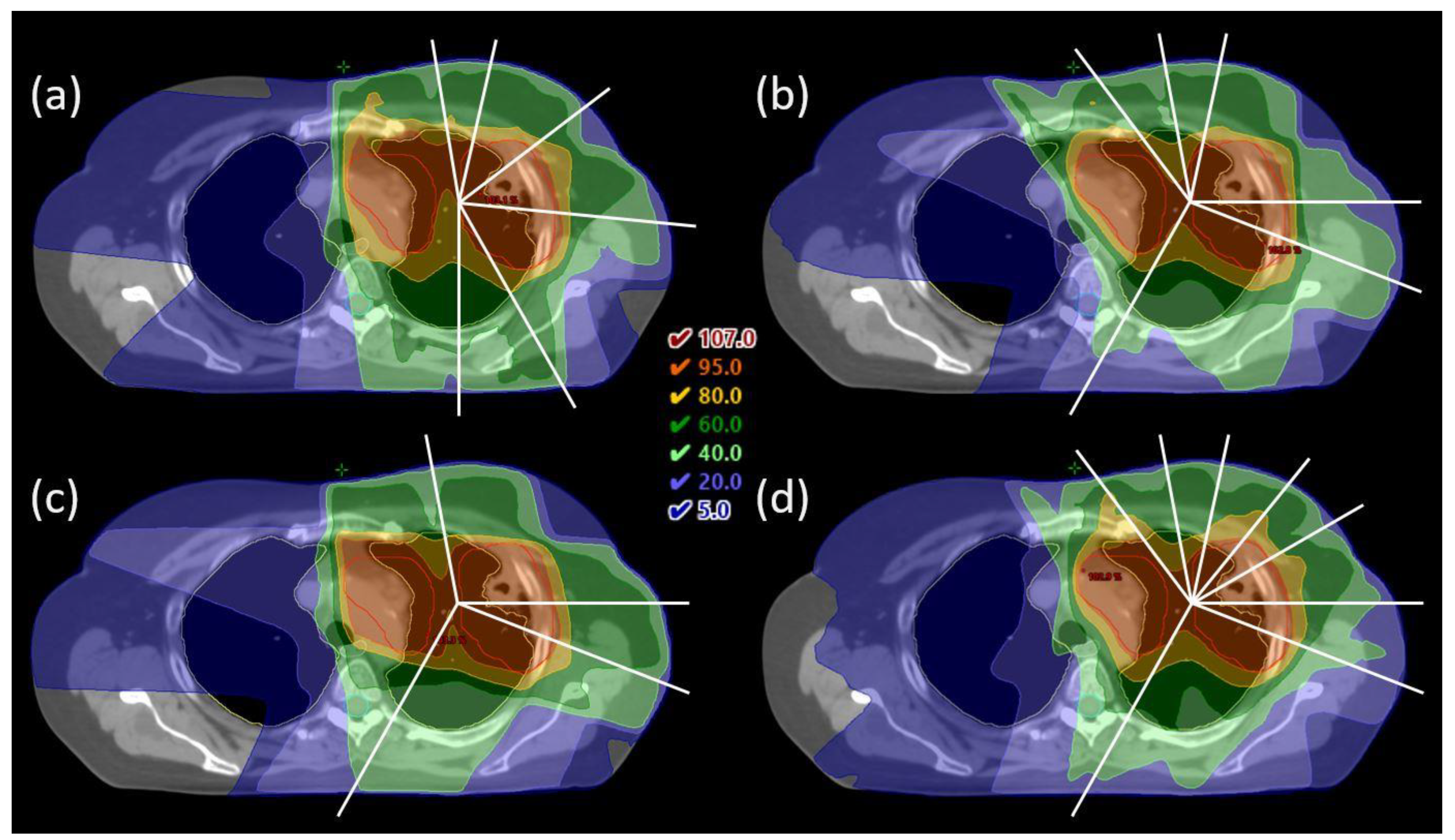
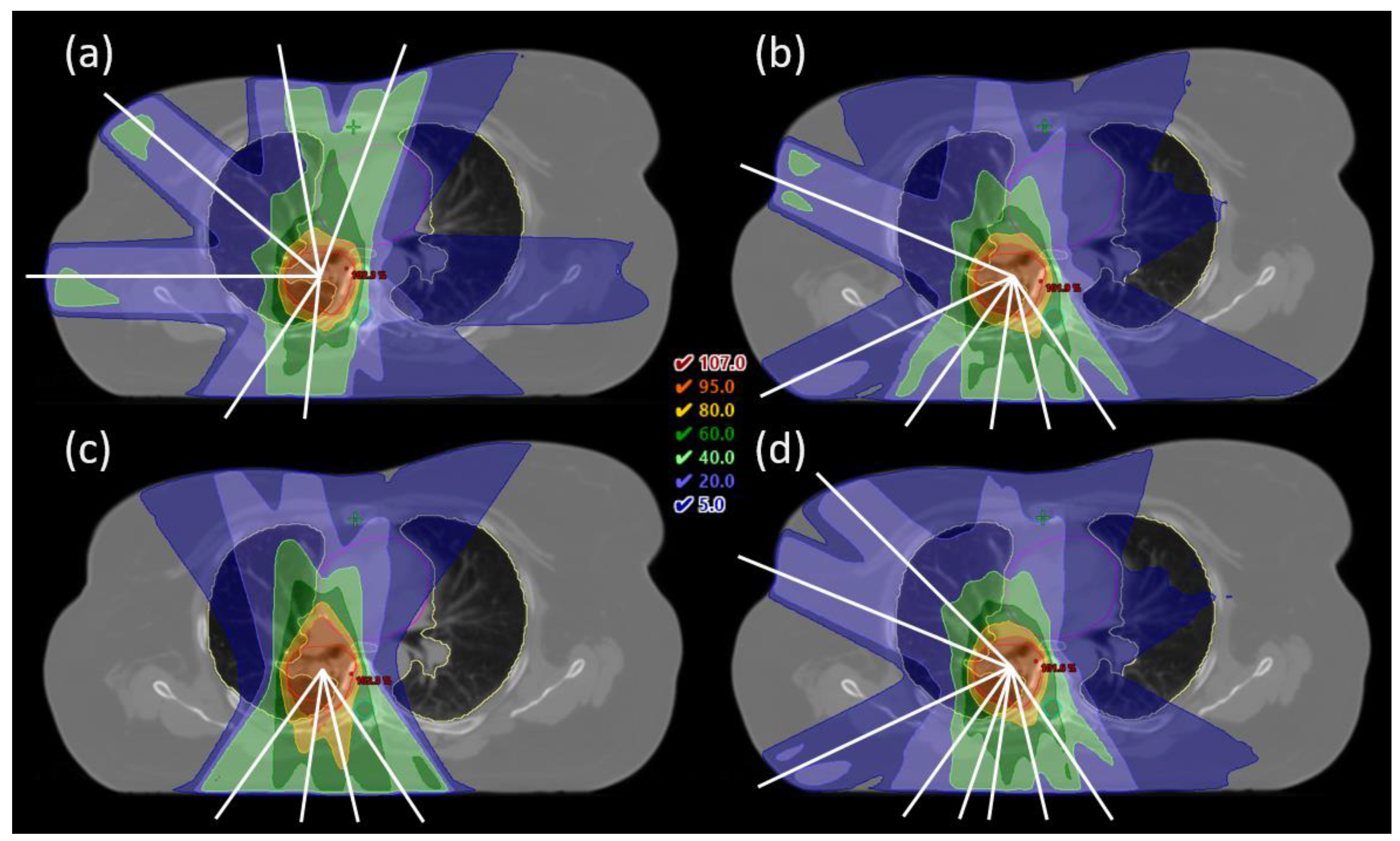
None of the published studies on automated planning for LA-NSCLC included integrated BAO to systematically investigate the impact of beam angles on plan quality, as has been performed in this study. Fixed-beam IMRT has the potential to reduce low dose to the lungs compared to VMAT, but exploiting this requires individual selection of appropriate beam angles [
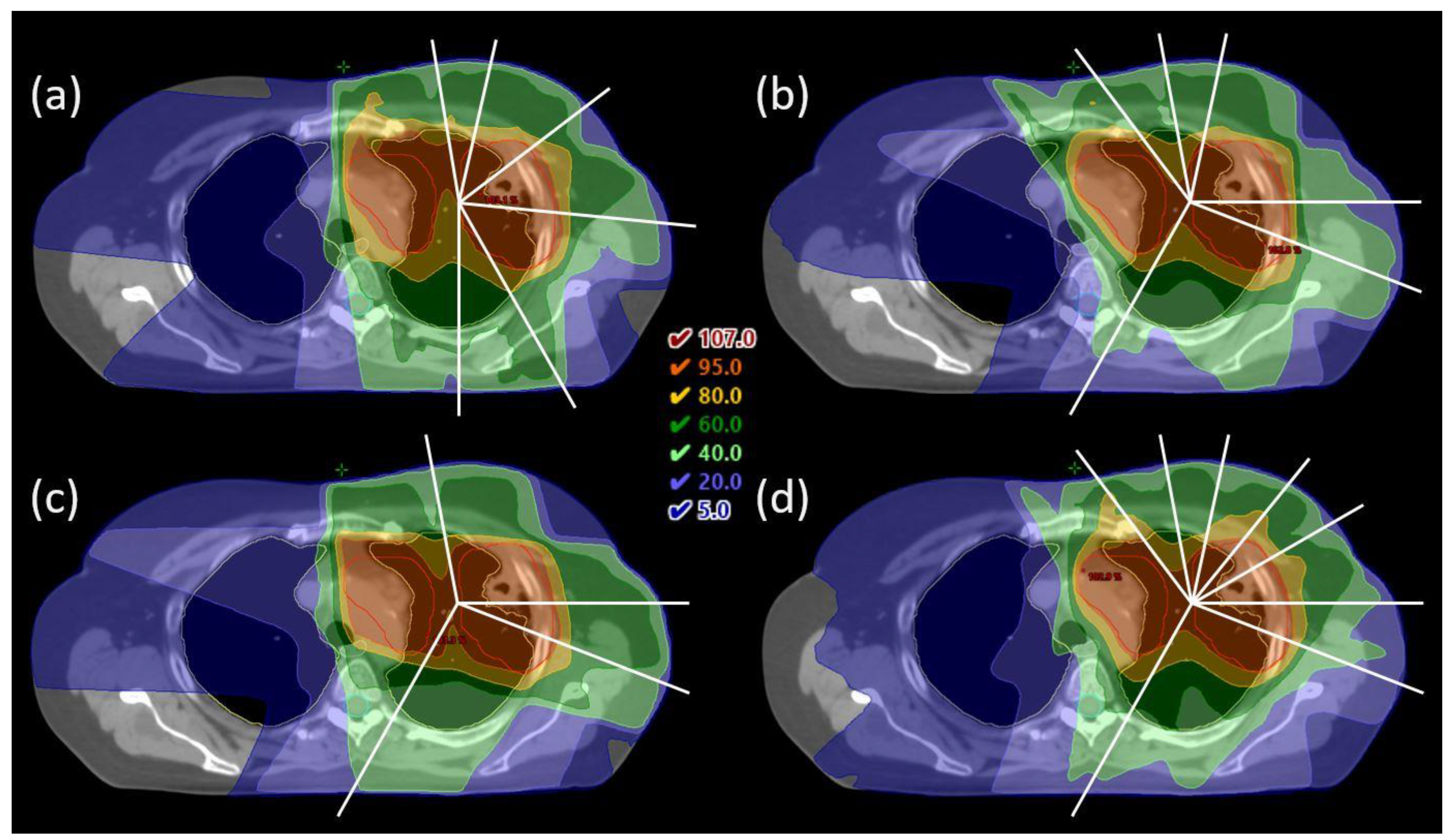
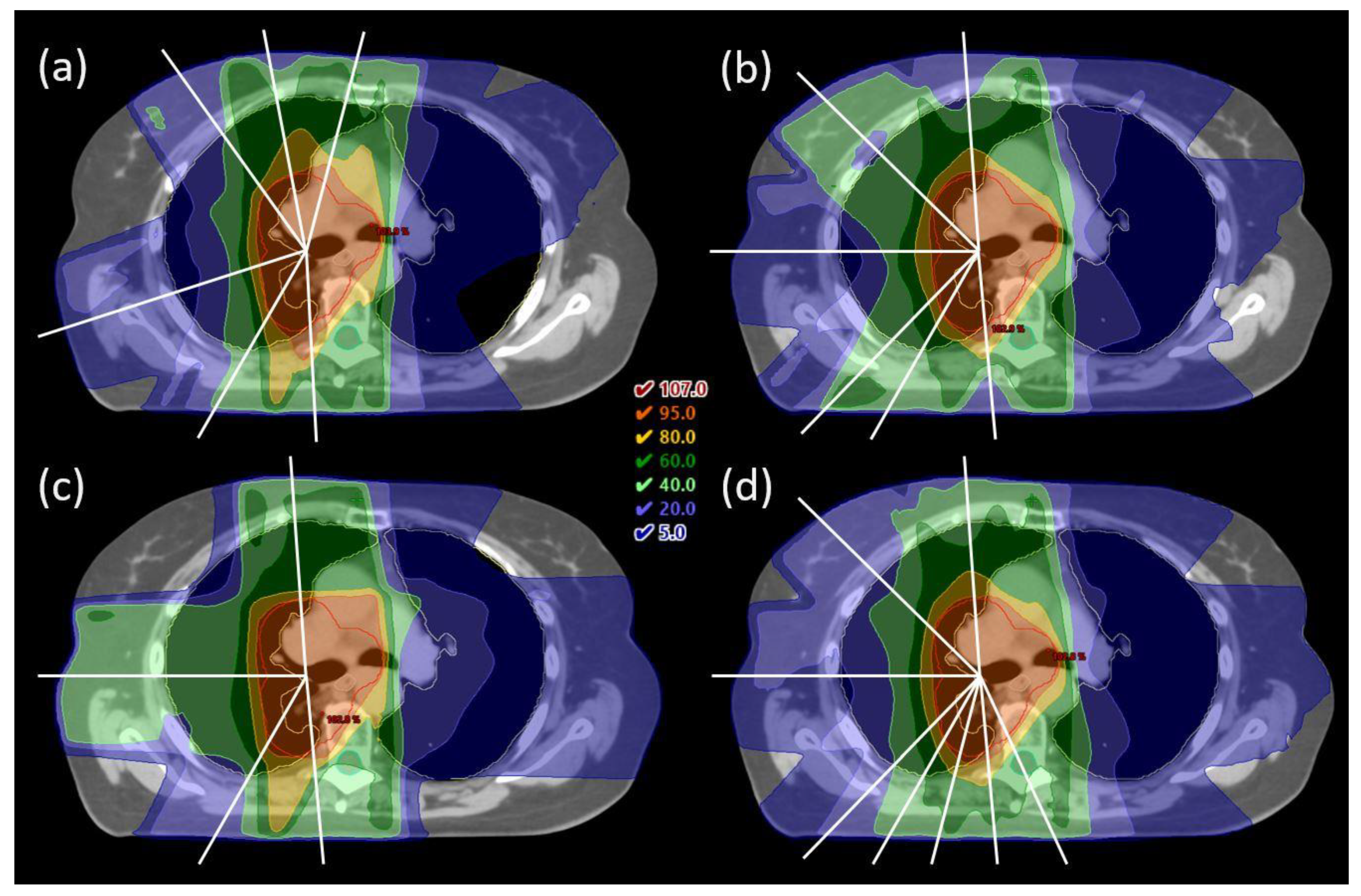
4]. LA-NSCLC is a heterogeneous patient group, and the position of the tumor in relation to OARs strongly affects which beam angles are most beneficial. The beam configurations in the CLIN plans, based on a template with emphasis on the anterior-posterior direction and a couple of additional lateral fields, were well suited for central tumors. For frontal and dorsal tumors, more oblique configurations, sometimes with opposing fields to cover nodal volumes, were selected by iCE and could spare dose to the heart, esophagus and/or contralateral lung for specific patients. Clearly, beam angles should be optimized individually in IMRT for LA-NSCLC.
In general, 6-beam plans appear to be a reasonable choice for this patient group. In some situations, reducing the number of beams in a treatment plan might be desirable, e.g., when the treatment time is of particular concern due to large target volume, split fields, DIBH treatment or poor condition of the patient. Similarly, increasing the number of beams might be appropriate in some situations, e.g., if OAR doses are above constraints. With the iCE method, creating several treatment plans with different numbers of optimized beams can be performed automatically, allowing for individual assessment of alternative plans. Plans with different numbers of beams can be created in a single round of optimization in Erasmus-iCycle, only the reconstruction in Eclipse must be done separately. Note that not all of the 4-beam iCE plans would be clinically acceptable. The wish-list constraints for the Dmax in the spinal canal and patient body as well as the high dose conformity were always achieved by default in Erasmus-iCycle. However, Eclipse struggled to reproduce the 4-beam dose distribution for some patients, and as hard constraints are not applied in Eclipse optimization, unacceptable plans could occur.
Increasing the number of beams on average improved OAR sparing, but the effect varied between patients. This is not surprising given the large heterogeneity in the anatomy of the LA-NSCLC patients. While the reasons behind the patient-specific differences were not investigated in detail, they appeared to be related to the OAR doses. Patients with high OAR doses had a greater benefit of increasing the number of beams than patients with low OAR doses. No impact of the size or location of the tumor was observed.
The average number of MUs was higher in the iCE plans than the CLIN plans (778 vs. 687). This could possibly be related to choices in the collimator angles, which were fixed at 2° in iCE plans, while in the CLIN plans, the collimator angle for each field was tuned to narrow the field size in the X direction, leading to larger field openings and fewer MUs. In our clinic, the enhanced MUs with iCE were not a concern, given the excellent deliverability of the plans. No restriction on the number of MUs was applied in the optimization of CLIN or iCE plans. Nonetheless, if desired, adjusting the collimator with regard to the optimized beam angles is a simple operation.
Different systems for automated treatment planning have different characteristics, advantages and limitations [
7]. Advantages of Erasmus-iCycle are that configuration with a high-quality wish-list will result in optimal dose distributions according to the clinic’s priorities, and that few (or even zero) example plans are needed for the wish-list configuration. In many studies, Erasmus-iCycle plans proved superior to the example plans used for configuration [
13,
17,
19,
34,
35]. A limitation is that the generated dose distributions are not directly deliverable. Therefore, translations into segmented treatment plans must be performed. In this study, the translations were performed by the Eclipse TPS, with use of line objectives that offer a simple way of controlling the entire dose-volume range simultaneously. It also makes the configuration for new treatment sites simple, as the only tuning required for plan recreation in Eclipse is of the priorities and normal tissue objective.
RapidPlan is a tool for automated planning already integrated in Eclipse, using so-called knowledge-based planning. Comparing the quality of iCE and RapidPlan plans was not within the scope of this study, in part because RapidPlan does not feature BAO. Studies have shown the dependence of the output plan quality on the quality of plans in the RapidPlan library [
36,
37]. In future work, we plan to explore the possibility of building a RapidPlan library containing iCE plans.
A limitation of the current study is the total number of investigated patients. However, all patients had LA-NSCLC and they were prospectively included. Moreover, there was a large variation in the tumor location and OAR dose-volume parameters among these LA-NSCLC patients. In order to strengthen the statistics, some patients were used for both Erasmus-iCycle wish-list tuning and for comparisons between CLIN and iCE. This is not a concern in the same way as for library-based methods, as the wish-list is based on the clinical protocol and priorities and not directly on the test patients used for guiding the wish-list creation.
Furthermore, some information from the clinical planning (choice of FB vs. DIBH technique and 60 Gy vs. 66 Gy prescription) was transferred to the automated planning, as required for fair comparison. These properties are sometimes changed during the planning process in response to the obtained OAR doses. With automated planning, several plans can be created with little additional work to find the most suitable option for each individual patient.
This study has been evaluated using the RATING criteria for treatment planning studies and a score of 96% was achieved [
38].


 ,
, 



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}