
The Effect of Intraocular Pressure-Lowering Medication on Metastatic Uveal Melanomas

 ,
,  , ,
, ,
Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Study Population
2.2. Assessment of Exposure
2.3. Assessment of Main Outcomes
2.4. Statistical Analyses
3. Results
3.1. Choroidal Melanoma
3.1.1. PP-Users
3.1.2. Alpha2-agonists
3.1.3. Beta-Blockers, CAI, and Oral IOP-Lowering Medication
3.2. Ciliary Body Melanoma
3.3. Uveal Melanoma (CM and CBM Pooled)
3.3.1. PP-Users
3.3.2. Alpha2-agonists
3.3.3. Beta-Blockers, CAI, and Oral IOP-Lowering Medication
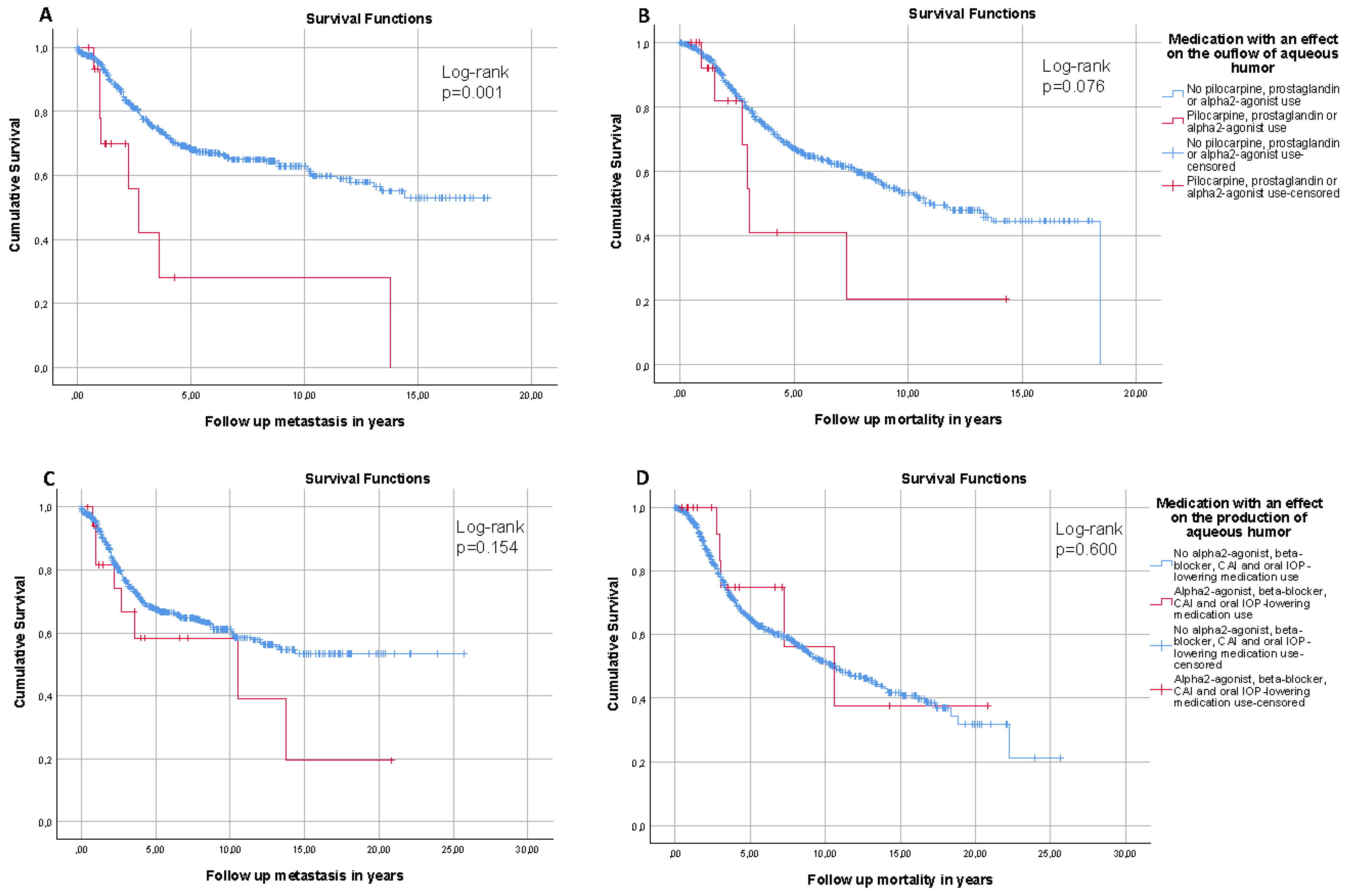
3.4. IOP-Lowering Medications That Increase Aqueous Humor Outflow and IOP-Lowering Medications That Reduce the Production of Aqueous Humor
3.5. IOP and Risk of Metastasis and Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Shields, C.L.; Furuta, M.; Thangappan, A.; Nagori, S.; Mashayekhi, A.; Lally, D.R.; Kelly, C.C.; Rudich, D.S.; Nagori, A.V.; Wakade, O.A.; et al. Metastasis of uveal melanoma millimeter-by-millimeter in 8033 consecutive eyes. Arch. Ophthalmol. 2009, 127, 989–998. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.D.; Turell, M.E.; Topham, A.K. Uveal melanoma: Trends in incidence, treatment, and survival. Ophthalmology 2011, 118, 1881–1885. [Google Scholar] [CrossRef] [PubMed]
- Rietschel, P.; Panageas, K.S.; Hanlon, C.; Patel, A.; Abramson, D.H.; Chapman, P.B. Variates of survival in metastatic uveal melanoma. J. Clin. Oncol. 2005, 23, 8076–8080. [Google Scholar] [CrossRef]
- Kujala, E.; Makitie, T.; Kivela, T. Very long-term prognosis of patients with malignant uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4651–4659. [Google Scholar] [CrossRef]
- McLean, I.W. The biology of haematogenous metastasis in human uveal malignant melanoma. Virchows. Arch. A Pathol. Anat. Histopathol. 1993, 422, 433–437. [Google Scholar] [CrossRef]
- Van Beek, J.G.M.; Van den Bosch, Q.C.C.; Naus, N.; Paridaens, D.; de Klein, A.; Kilic, E.; Verdijk, R.M. Absence of intraocular lymphatic vessels in uveal melanomas with extrascleral growth. Cancers 2019, 11, 228. [Google Scholar] [CrossRef]
- Bakalian, S.; Marshall, J.C.; Logan, P.; Faingold, D.; Maloney, S.; Di Cesare, S.; Martins, C.; Fernandes, B.F.; Burnier, M.N., Jr. Molecular pathways mediating liver metastasis in patients with uveal melanoma. Clin. Cancer Res. 2008, 14, 951–956. [Google Scholar] [CrossRef]
- Jochems, A.; Van der Kooij, M.K.; Fiocco, M.; Schouwenburg, M.G.; Aarts, M.J.; van Akkooi, A.C.; Van den Berkmortel, F.; Blank, C.U.; van den Eertwegh, A.J.M.; Franken, M.G.; et al. Metastatic uveal melanoma: Treatment strategies and survival-results from the dutch melanoma treatment registry. Cancers 2019, 11, 1007. [Google Scholar] [CrossRef]
- Souto, E.B.; Zielinska, A.; Luis, M.; Carbone, C.; Martins-Gomes, C.; Souto, S.B.; Silva, A.M. Uveal melanoma: Physiopathology and new in situ-specific therapies. Cancer Chemother. Pharmacol. 2019, 84, 15–32. [Google Scholar] [CrossRef]
- Yavuzyigitoglu, S.; Koopmans, A.E.; Verdijk, R.M.; Vaarwater, J.; Eussen, B.; van Bodegom, A.; Paridaens, D.; Kilic, E.; de Klein, A.; Rotterdam Ocular Melanoma Study, G. Uveal melanomas with sf3b1 mutations: A distinct subclass associated with late-onset metastases. Ophthalmology 2016, 123, 1118–1128. [Google Scholar] [CrossRef] [PubMed]
- Camp, D.A.; Yadav, P.; Dalvin, L.A.; Shields, C.L. Glaucoma secondary to intraocular tumors: Mechanisms and management. Curr. Opin. Ophthalmol. 2019, 30, 71–81. [Google Scholar] [CrossRef]
- Shields, C.L.; Shields, J.A.; Shields, M.B.; Augsburger, J.J. Prevalence and mechanisms of secondary intraocular pressure elevation in eyes with intraocular tumors. Ophthalmology 1987, 94, 839–846. [Google Scholar] [CrossRef]
- van der Valk, R.; Webers, C.A.; Schouten, J.S.; Zeegers, M.P.; Hendrikse, F.; Prins, M.H. Intraocular pressure-lowering effects of all commonly used glaucoma drugs: A meta-analysis of randomized clinical trials. Ophthalmology 2005, 112, 1177–1185. [Google Scholar] [CrossRef]
- Toris, C.B.; Gabelt, B.T.; Kaufman, P.L. Update on the mechanism of action of topical prostaglandins for intraocular pressure reduction. Surv. Ophthalmol. 2008, 53 (Suppl. 1), S107–S120. [Google Scholar] [CrossRef] [PubMed]
- Flocks, M.; Zweng, H.C. Studies on the mode of action of pilocarpine on aqueous outflow. Am. J. Ophthalmol. 1957, 44, 380–386, discussion 387–388. [Google Scholar] [CrossRef]
- Skaat, A.; Rosman, M.S.; Chien, J.L.; Mogil, R.S.; Ren, R.; Liebmann, J.M.; Ritch, R.; Park, S.C. Effect of pilocarpine hydrochloride on the schlemm canal in healthy eyes and eyes with open-angle glaucoma. JAMA Ophthalmol. 2016, 134, 976–981. [Google Scholar] [CrossRef] [PubMed]
- Toris, C.B.; Gleason, M.L.; Camras, C.B.; Yablonski, M.E. Effects of brimonidine on aqueous humor dynamics in human eyes. Arch. Ophthalmol. 1995, 113, 1514–1517. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.L.; Galin, M.A.; Obstbaum, S.A.; Katz, I. Longterm timolol therapy. Surv. Ophthalmol. 1979, 23, 377–380. [Google Scholar] [CrossRef]
- Sugrue, M.F. Pharmacological and ocular hypotensive properties of topical carbonic anhydrase inhibitors. Prog. Retin. Eye Res. 2000, 19, 87–112. [Google Scholar] [CrossRef]
- Girkin, C.A.; Goldberg, I.; Mansberger, S.L.; Shields, J.A.; Shields, C.L. Management of iris melanoma with secondary glaucoma. J. Glaucoma 2002, 11, 71–74. [Google Scholar] [CrossRef]
- Shields, C.L.; Shields, J.A.; Materin, M.; Gershenbaum, E.; Singh, A.D.; Smith, A. Iris melanoma: Risk factors for metastasis in 169 consecutive patients. Ophthalmology 2001, 108, 172–178. [Google Scholar] [CrossRef]
- Koopmans, A.E.; Verdijk, R.M.; Brouwer, R.W.; van den Bosch, T.P.; van den Berg, M.M.; Vaarwater, J.; Kockx, C.E.; Paridaens, D.; Naus, N.C.; Nellist, M.; et al. Clinical significance of immunohistochemistry for detection of bap1 mutations in uveal melanoma. Mod. Pathol. 2014, 27, 1321–1330. [Google Scholar] [CrossRef] [PubMed]
- Smit, K.N.; van Poppelen, N.M.; Vaarwater, J.; Verdijk, R.; van Marion, R.; Kalirai, H.; Coupland, S.E.; Thornton, S.; Farquhar, N.; Dubbink, H.J.; et al. Combined mutation and copy-number variation detection by targeted next-generation sequencing in uveal melanoma. Mod. Pathol. 2018, 31, 763–771. [Google Scholar] [CrossRef]
- European glaucoma society terminology and guidelines for glaucoma, 4th edition—Chapter 3: Treatment principles and options supported by the egs foundation: Part 1: Foreword; introduction; glossary; chapter 3 treatment principles and options. Br. J. Ophthalmol. 2017, 101, 130–195. [CrossRef]
- Doucette, L.P.; Walter, M.A. Prostaglandins in the eye: Function, expression, and roles in glaucoma. Ophthalmic. Genet. 2017, 38, 108–116. [Google Scholar] [CrossRef]
- Matsuo, T.; Cynader, M.S. Localisation of prostaglandin f2 alpha and e2 binding sites in the human eye. Br. J. Ophthalmol. 1992, 76, 210–213. [Google Scholar] [CrossRef]
- Bamba, H.; Ota, S.; Kato, A.; Kawamoto, C.; Fujiwara, K. Prostaglandins up-regulate vascular endothelial growth factor production through distinct pathways in differentiated u937 cells. Biochem. Biophys. Res. Commun. 2000, 273, 485–491. [Google Scholar] [CrossRef]
- Sabaner, M.C.; Duman, R.; Vurmaz, A.; Ertekin, T. Effects of topical prostaglandin drops on angiogenesis in an in ovo chick chorioallantoic membrane model. Cutan. Ocul. Toxicol. 2021, 40, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Sales, K.J.; List, T.; Boddy, S.C.; Williams, A.R.; Anderson, R.A.; Naor, Z.; Jabbour, H.N. A novel angiogenic role for prostaglandin f2alpha-fp receptor interaction in human endometrial adenocarcinomas. Cancer Res. 2005, 65, 7707–7716. [Google Scholar] [CrossRef] [PubMed]
- Tamura, K.; Sakurai, T.; Kogo, H. Relationship between prostaglandin e2 and vascular endothelial growth factor (vegf) in angiogenesis in human vascular endothelial cells. Vascul. Pharmacol. 2006, 44, 411–416. [Google Scholar] [CrossRef]
- Omori, K.; Kida, T.; Hori, M.; Ozaki, H.; Murata, T. Multiple roles of the pge2 -ep receptor signal in vascular permeability. Br. J. Pharmacol. 2014, 171, 4879–4889. [Google Scholar] [CrossRef]
- Kim, J.W.; Lindsey, J.D.; Wang, N.; Weinreb, R.N. Increased human scleral permeability with prostaglandin exposure. Investig. Ophthalmol. Vis. Sci. 2001, 42, 1514–1521. [Google Scholar]
- Mori, A.; Saito, M.; Sakamoto, K.; Nakahara, T.; Ishii, K. Intravenously administered vasodilatory prostaglandins increase retinal and choroidal blood flow in rats. J. Pharmacol. Sci. 2007, 103, 103–112. [Google Scholar] [CrossRef]
- Amano, H.; Hayashi, I.; Endo, H.; Kitasato, H.; Yamashina, S.; Maruyama, T.; Kobayashi, M.; Satoh, K.; Narita, M.; Sugimoto, Y.; et al. Host prostaglandin e(2)-ep3 signaling regulates tumor-associated angiogenesis and tumor growth. J. Exp. Med. 2003, 197, 221–232. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Hashimoto, Y.; Cho, S.N.; Roszik, J.; Milton, D.R.; Dal, F.; Kim, S.F.; Menter, D.G.; Yang, P.; Ekmekcioglu, S.; et al. Microsomal pge2 synthase-1 regulates melanoma cell survival and associates with melanoma disease progression. Pigment Cell Melanoma Res. 2016, 29, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Bustamante, P.; Miyamoto, D.; Goyeneche, A.; de Alba Graue, P.G.; Jin, E.; Tsering, T.; Dias, A.B.; Burnier, M.N.; Burnier, J.V. Beta-blockers exert potent anti-tumor effects in cutaneous and uveal melanoma. Cancer Med. 2019, 8, 7265–7277. [Google Scholar] [CrossRef]
- Haapasalo, J.; Nordfors, K.; Jarvela, S.; Bragge, H.; Rantala, I.; Parkkila, A.K.; Haapasalo, H.; Parkkila, S. Carbonic anhydrase ii in the endothelium of glial tumors: A potential target for therapy. Neuro. Oncol. 2007, 9, 308–313. [Google Scholar] [CrossRef]
- Yoshiura, K.; Nakaoka, T.; Nishishita, T.; Sato, K.; Yamamoto, A.; Shimada, S.; Saida, T.; Kawakami, Y.; Takahashi, T.A.; Fukuda, H.; et al. Carbonic anhydrase ii is a tumor vessel endothelium-associated antigen targeted by dendritic cell therapy. Clin. Cancer Res. 2005, 11, 8201–8207. [Google Scholar] [CrossRef]
- Linden, C.; Alm, A. Prostaglandin analogues in the treatment of glaucoma. Drugs Aging 1999, 14, 387–398. [Google Scholar] [CrossRef]
- Sun, L.L.; Welch, R.T.; Vu, P. Lower eyelid melanoma during bimatoprost (lumigan) therapy. Clin. Exp. Ophthalmol. 2012, 40, 213–214. [Google Scholar] [CrossRef]
- Esteve, E.; Beau-Salinas, F.; Esteve, L.; Lemacon, J.M.; Autret-Leca, E.; Le Louet, H.; Hocine, R.; Wolkenstein, P.; Plaquet, J.L. [melanoma during latanoprost therapy: Three cases] melanomes associes au latanoprost: Trois cas. Ann. Dermatol. Venereol. 2009, 136, 60–61. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| CM | CBM | CM (Total) | CBM (Total) | p-Value | |
|---|---|---|---|---|---|
| PP | 5 Prostaglandin 1 Pilocarpine | 3 Prostaglandin 1 Prostaglandin/beta-blocker | 6 (1.1) | 4 (5.6) | 0.018 * |
| Alpha2-agonist | 3 Alpha2-agonist | 1 Alpha2-agonist | 3 (0.5) | 1 (1.4) | 0.379 |
| Beta-blocker | 3 Beta-blocker 7 Beta-blocker/CAI | 1 Beta-blocker 1 Beta-blocker/prostaglandin 1 Beta-blocker/CAI | 10 (1.8) | 3 (4.2) | 0.170 |
| CAI | 2 CAI 7 CAI/beta-blocker | 1 CAI/beta-blocker | 9 (1.6) | 1 (1.4) | 1.000 |
| Oral | NA | NA | 7 (1.2) | 4 (5.6) | 0.026 * |
| Risk of Metastasis | Risk of Mortality | |||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| A. CM α | ||||||
| -PP | 11.413 | 2.773–46.968 | 0.001 * | 10.367 | 2.424–44.342 | 0.002 * |
| -Beta-blocker | 37.725 | 2.353–604.867 | 0.010 * | 12.834 | 0.028–5891.620 | 0.414 |
| -CAI | 0.085 | 0.003–2.060 | 0.130 | 0.000 | 0.000–3.218 × 10−44 | 0.870 |
| -Oral | 0.045 | 0.001–1.477 | 0.082 | 0.057 | 0.000–26.693 | 0.361 |
| B. UM (CM+CBM) β | ||||||
| -PP | 4.840 | 1.452–16.133 | 0.010 * | 7.528 | 1.836–30.867 | 0.005 * |
| -Beta-blocker | 6.024 | 0.701–51.786 | 0.102 | 1.039 | 0.094–11.546 | 0.975 |
| -CAI | 0.575 | 0.064–5.150 | 0.621 | 0.000 | 0.000–7.741 × 10−100 | 0.933 |
| -Oral | 0.112 | 0.010–1.204 | 0.071 | 0.234 | 0.025–2.201 | 0.204 |
| Risk of Metastasis | Risk of Mortality | |||||
|---|---|---|---|---|---|---|
| HR | 95%CI | p-Value | HR | 95%CI | p-Value | |
| Outflow β | 6.344 | 1.615–24.918 | 0.008 * | 9.743 | 2.475–38.353 | 0.001 * |
| Production β | 0.481 | 0.127–1.814 | 0.280 | 0.143 | 0.030–0.686 | 0.015 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pals, J.; Mensink, H.W.; Brosens, E.; Verdijk, R.M.; Naus, N.C.; Paridaens, D.A.; Kilic, E.; Ramdas, W.D. The Effect of Intraocular Pressure-Lowering Medication on Metastatic Uveal Melanomas. Cancers 2021, 13, 5657. https://doi.org/10.3390/cancers13225657
Pals J, Mensink HW, Brosens E, Verdijk RM, Naus NC, Paridaens DA, Kilic E, Ramdas WD. The Effect of Intraocular Pressure-Lowering Medication on Metastatic Uveal Melanomas. Cancers. 2021; 13(22):5657. https://doi.org/10.3390/cancers13225657
Chicago/Turabian StylePals, Jan, Hanneke W. Mensink, Erwin Brosens, Robert M. Verdijk, Nicole C. Naus, Dion A. Paridaens, Emine Kilic, and Wishal D. Ramdas. 2021. "The Effect of Intraocular Pressure-Lowering Medication on Metastatic Uveal Melanomas" Cancers 13, no. 22: 5657. https://doi.org/10.3390/cancers13225657
APA StylePals, J., Mensink, H. W., Brosens, E., Verdijk, R. M., Naus, N. C., Paridaens, D. A., Kilic, E., & Ramdas, W. D. (2021). The Effect of Intraocular Pressure-Lowering Medication on Metastatic Uveal Melanomas. Cancers, 13(22), 5657. https://doi.org/10.3390/cancers13225657