
Development and Validation of a Novel Serum Prognostic Marker for Patients with Metastatic Colorectal Cancer on Regorafenib Treatment

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients, Data Process and Treatment
2.2. Response Evaluation and Endpoints
2.3. Cancer-Inflammation Prognostic Index (CIPI)
2.4. Statistics
3. Results
3.1. Patient Characteristics
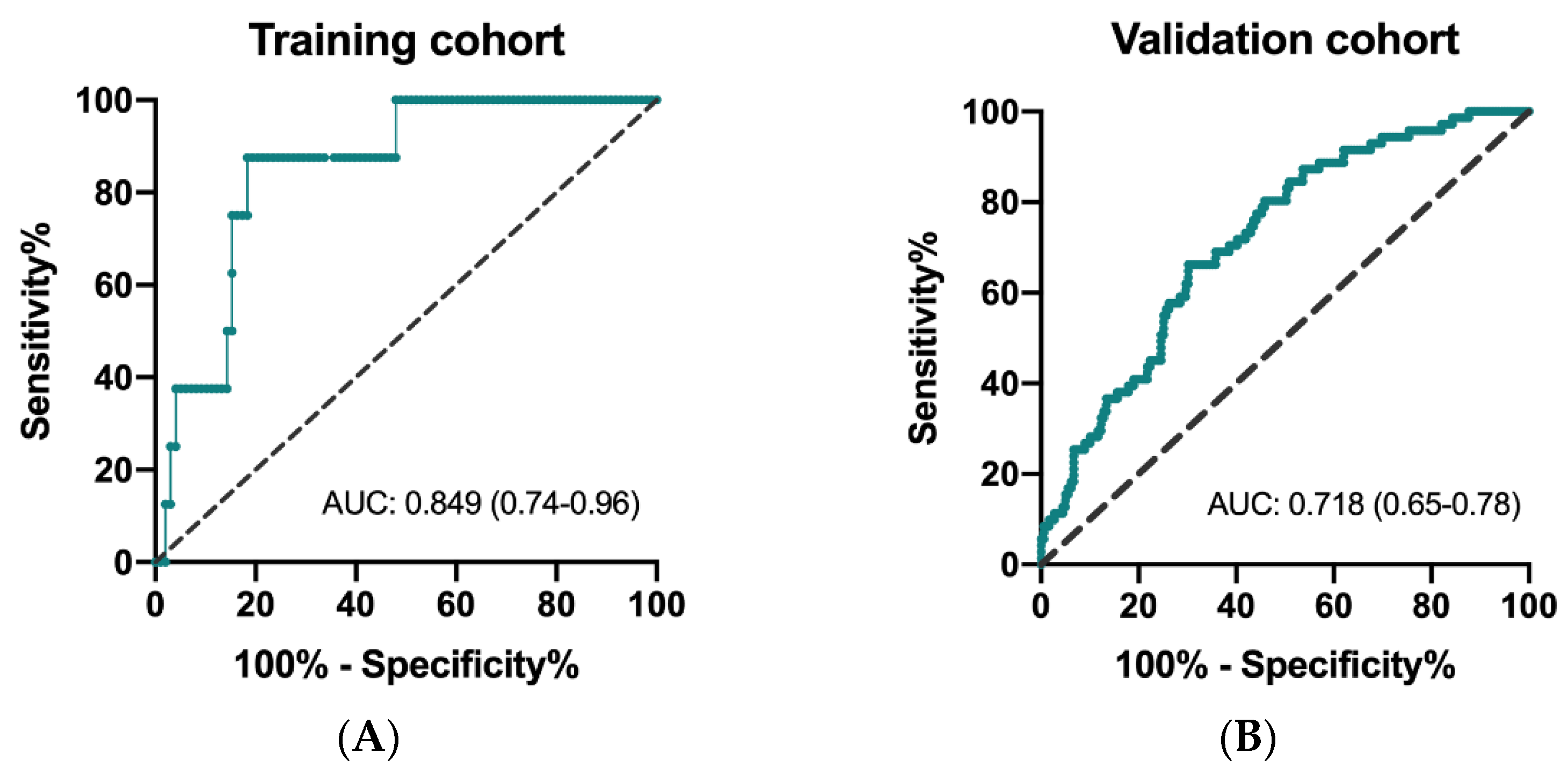
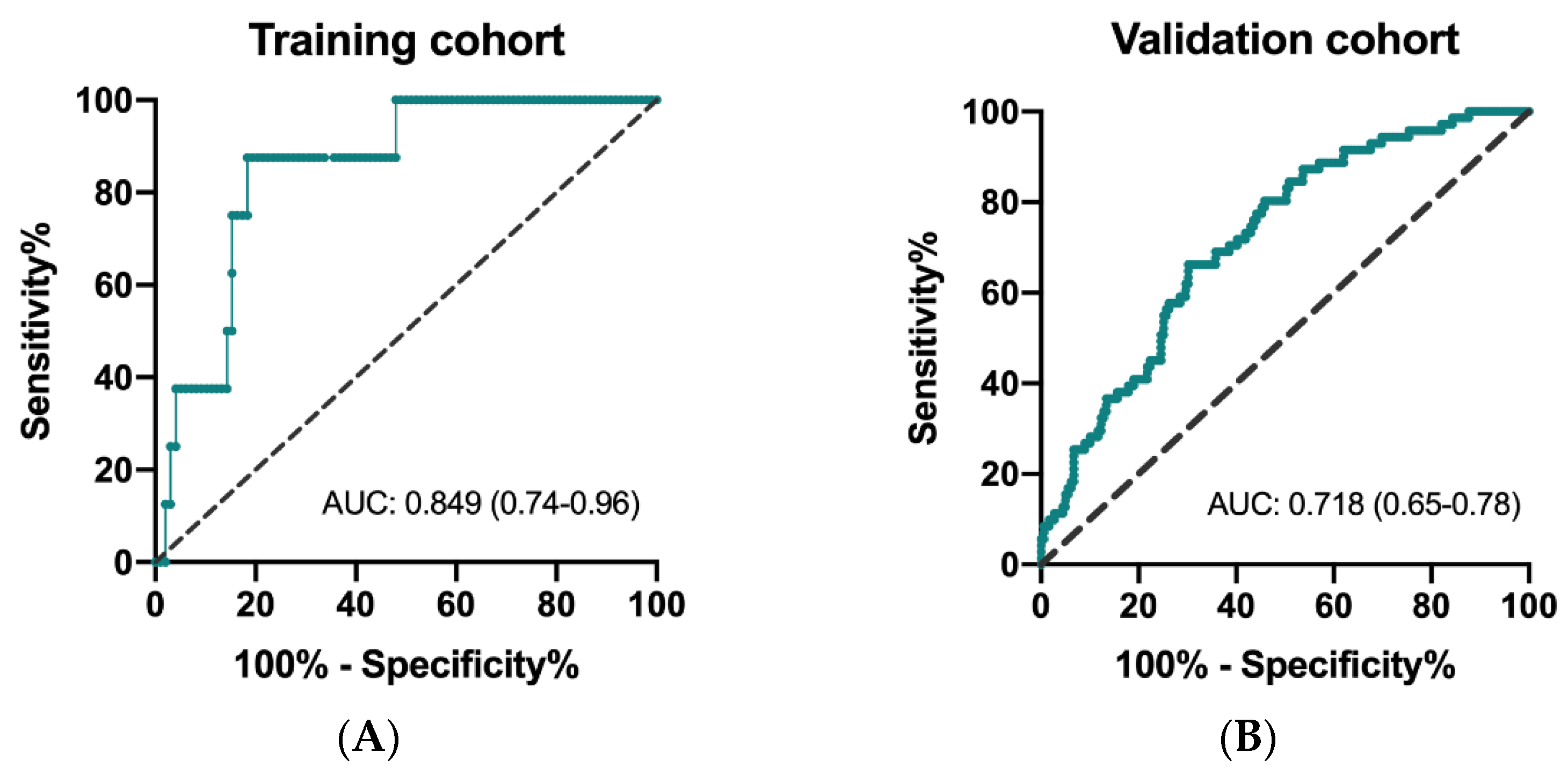
3.2. Determine the Cutoff Level of CIPI
3.3. Univariate and Multivariate Analysis of OS and PFS in the Training Cohort
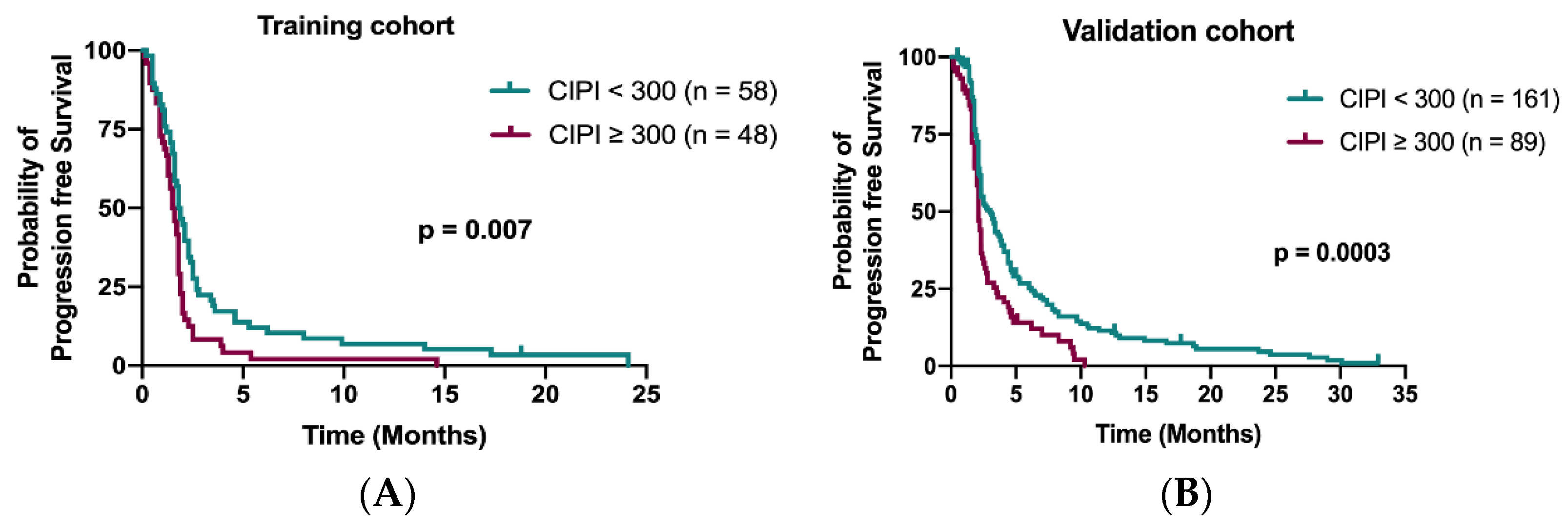
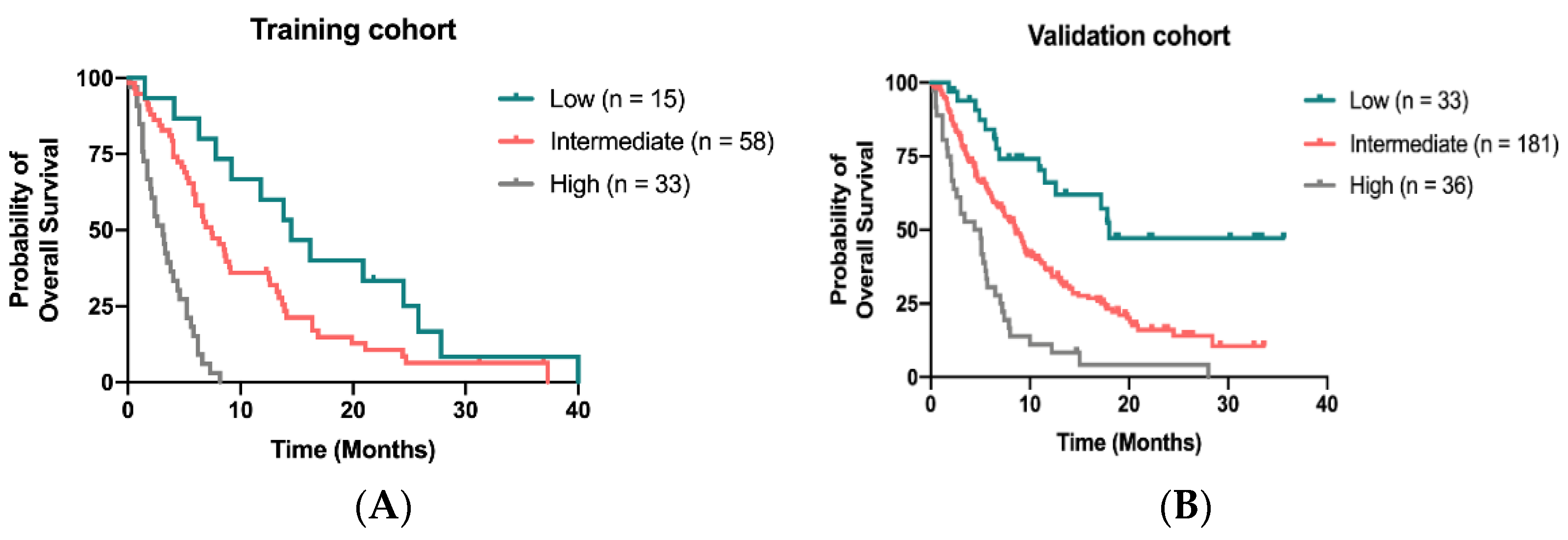
3.4. Build Up and Validation of the Prognostic Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef]
- Bray, F.; Me, J.F.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kopetz, S.; Chang, G.J.; Overman, M.J.; Eng, C.; Sargent, D.; Larson, D.W.; Grothey, A.; Vauthey, J.-N.; Nagorney, D.M.; McWilliams, R.R. Improved survival in metastatic colorectal cancer is associated with adoption of hepatic resection and improved chemotherapy. J. Clin. Oncol. 2009, 27, 3677–3683. [Google Scholar] [CrossRef] [PubMed]
- Meulenbeld, H.J.; van Steenbergen, L.N.; Janssen-Heijnen, M.L.G.; Lemmens, V.E.P.P.; Creemers, G.J. Significant improvement in survival of patients presenting with metastatic colon cancer in the south of The Netherlands from 1990 to 2004. Ann. Oncol. 2008, 19, 1600–1604. [Google Scholar] [CrossRef]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lupi, C.; Sensi, E.; Lonardi, S.; Mezi, S.; Tomasello, G.; Ronzoni, M.; Zaniboni, A.; et al. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: Updated overall survival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015, 16, 1306–1315. [Google Scholar] [CrossRef]
- Bridgewater, J.A.; Pugh, S.A.; Maishman, T.; Eminton, Z.; Mellor, J.; Whitehead, A.; Stanton, L.; Radford, M.; Corkhill, A.; Griffiths, G.O.; et al. Systemic chemotherapy with or without cetuximab in patients with resectable colorectal liver metastasis (New EPOC): Long-term results of a multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 398–411. [Google Scholar] [CrossRef]
- De Falco, V.; Napolitano, S.; Roselló, S.; Huerta, M.; Cervantes, A.; Ciardiello, F.; Troiani, T. How we treat metastatic colorectal cancer. ESMO Open 2020, 4, e000813. [Google Scholar] [CrossRef]
- Grothey, A.; Van Cutsem, E.; Sobrero, A.; Siena, S.; Falcone, A.; Ychou, M.; Humblet, Y.; Bouché, O.; Mineur, L.; Barone, C.; et al. Regorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): An international, multicentre, randomised, placebo-controlled, phase 3 trial. Lancet 2013, 381, 303–312. [Google Scholar] [CrossRef]
- Li, J.; Qin, S.; Xu, R.; Yau, T.C.C.; Ma, B.; Pan, H.; Xu, J.; Bai, Y.; Chi, Y.; Wang, L.; et al. Regorafenib plus best supportive care versus placebo plus best supportive care in Asian patients with previously treated metastatic colorectal cancer (CONCUR): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2015, 16, 619–629. [Google Scholar] [CrossRef]
- Mayer, R.J.; Van Cutsem, E.; Falcone, A.; Yoshino, T.; Garcia-Carbonero, R.; Mizunuma, N.; Yamazaki, K.; Shimada, Y.; Tabernero, J.; Komatsu, Y.; et al. Randomized trial of TAS-102 for refractory metastatic colorectal cancer. N. Engl. J. Med. 2015, 372, 1909–1919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilhelm, S.M.; Dumas, J.; Adnane, L.; Lynch, M.; Carter, C.A.; Schütz, G.; Thierauch, K.-H.; Zopf, D. Regorafenib (BAY 73-4506): A new oral multikinase inhibitor of angiogenic, stromal and oncogenic receptor tyrosine kinases with potent preclinical antitumor activity. Int. J. Cancer 2010, 129, 245–255. [Google Scholar] [CrossRef] [PubMed]
- Ducreux, M.; Petersen, L.N.; Öhler, L.; Bergamo, F.; Metges, J.-P.; de Groot, J.W.; Wang, J.-Y.; Paredes, B.G.; Dochy, E.; Fiala-Buskies, S.; et al. Safety and effectiveness of regorafenib in patients with metastatic colorectal cancer in routine clinical practice in the prospective, observational CORRELATE study. Eur. J. Cancer 2019, 123, 146–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, K.-H.; Yang, T.-S.; Hsu, T.-C.; Chen, W.T.-L.; Chen, H.-H.; Teng, H.-W.; Lin, B.-W.; Kuan, F.-C.; Chiang, F.-F.; Duann, C.-W.; et al. Real-world evidence of the safety and effectiveness of regorafenib in Taiwanese patients with metastatic colorectal cancer: CORRELATE Taiwan. J. Formos. Med Assoc. 2021. [Google Scholar] [CrossRef] [PubMed]
- Novakova-Jiresova, A.; Kopeckova, K.; Boublikova, L.; Chloupkova, R.; Melichar, B.; Petruzelka, L.; Finek, J.; Fiala, O.; Grell, P.; Batko, S.; et al. Regorafenib for metastatic colorectal cancer: An analysis of a registry-based cohort of 555 patients. Cancer Manag. Res. 2020, 12, 5365–5372. [Google Scholar] [CrossRef]
- Del Prete, M.; Giampieri, R.; Loupakis, F.; Prochilo, T.; Salvatore, L.; Faloppi, L.; Bianconi, M.; Bittoni, A.; Aprile, G.; Zaniboni, A.; et al. Prognostic clinical factors in pretreated colorectal cancer patients receiving regorafenib: Implications for clinical management. Oncotarget 2015, 6, 33982–33992. [Google Scholar] [CrossRef] [Green Version]
- Hsu, H.-C.; Huang, K.-C.; Chen, W.-S.; Jiang, J.-K.; Yang, S.-H.; Wang, H.-S.; Chang, S.-C.; Lan, Y.-T.; Lin, C.-C.; Lin, H.-H.; et al. Preference criteria for regorafenib in treating refractory metastatic colorectal cancer are the small tumor burden, slow growth and poor/scanty spread. Sci. Rep. 2021, 11, 1–13. [Google Scholar] [CrossRef]
- Camp, R.L.; Dolled-Filhart, M.; Rimm, D.L. X-Tile: A new bio-informatics tool for biomarker assessment and outcome-based cut-point optimization. Clin. Cancer Res. 2004, 10, 7252–7259. [Google Scholar] [CrossRef] [Green Version]
- Van Cutsem, E.; Cervantes, A.; Nordlinger, B.; Arnold, D.; Group, E.G.W. Metastatic colorectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2014, 25, iii1–iii9. [Google Scholar] [CrossRef]
- Yoshino, T.; Arnold, D.; Taniguchi, H.; Pentheroudakis, G.; Yamazaki, K.; Xu, R.-H.; Kim, T.; Ismail, F.; Tan, I.; Yeh, K.-H.; et al. Pan-Asian adapted ESMO consensus guidelines for the management of patients with metastatic colorectal cancer: A JSMO–ESMO initiative endorsed by CSCO, KACO, MOS, SSO and TOS. Ann. Oncol. 2018, 29, 44–70. [Google Scholar] [CrossRef]
- Bhatti, I.; Patel, M.; Dennison, A.R.; Thomas, M.W.; Garcea, G. Utility of postoperative CEA for surveillance of recurrence after resection of primary colorectal cancer. Int. J. Surg. 2015, 16, 123–128. [Google Scholar] [CrossRef]
- Tabernero, J.; Lenz, H.-J.; Siena, S.; Sobrero, A.; Falcone, A.; Ychou, M.; Humblet, Y.; Bouché, O.; Mineur, L.; Barone, C.; et al. Analysis of circulating DNA and protein biomarkers to predict the clinical activity of regorafenib and assess prognosis in patients with metastatic colo-rectal cancer: A retrospective, exploratory analysis of the CORRECT trial. Lancet Oncol. 2015, 16, 937–948. [Google Scholar] [CrossRef]
- Teufel, M.; Kalmus, J.; Rutstein, M.D.; Koechert, K.; Seidel, H.; Reischl, J.; Skubala, A.; Vonk, R.; Wilhelm, S.; Kobina, S.; et al. Analysis of plasma protein biomarkers from the phase 3 CONCUR study of regorafenib in Asian patients with metastatic colorectal cancer (mCRC). J. Clin. Oncol. 2016, 34, 672. [Google Scholar] [CrossRef]
- Dixon, M.R.; Haukoos, J.S.; Udani, S.M.; Naghi, J.J.; Arnell, T.D.; Kumar, R.R.; Stamos, M.J. Carcinoembryonic antigen and albumin predict survival in patients with advanced colon and rectal cancer. Arch. Surg. 2003, 138, 962. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moretto, R.; Rossini, D.; Conca, V.; Lonardi, S.; Rasola, C.; Antoniotti, C.; Santini, D.; Marmorino, F.; Tomasello, G.; Borelli, B.; et al. CEA increase as a marker of disease progression after first-line induction therapy in metastatic colorectal cancer patients. A pooled analysis of TRIBE and TRIBE2 studies. Br. J. Cancer 2021, 1–7. [Google Scholar] [CrossRef]
- Yoshino, T.; Obermannová, R.; Bodoky, G.; Garcia-Carbonero, R.; Ciuleanu, T.; Portnoy, D.C.; Kim, T.W.; Hsu, Y.; Ferry, D.; Nasroulah, F.; et al. Baseline carcinoembryonic antigen as a predictive factor of ramucirumab efficacy in RAISE, a second-line metastatic colorectal carcinoma phase III trial. Eur. J. Cancer 2017, 78, 61–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bramswig, K.H.; Pöttler, M.; Unseld, M.; Wrba, F.; Uhrin, P.; Zimmermann, W.; Zielinski, C.C.; Prager, M.G. Soluble carcinoembryonic antigen activates endothelial cells and tumor angiogenesis. Cancer Res. 2013, 73, 6584–6596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prager, G.W.; Braemswig, K.H.; Martel, A.; Unseld, M.; Heinze, G.; Brodowicz, T.; Scheithauer, W.; Kornek, G.; Zielinski, C.C. Baseline carcinoembryonic antigen (CEA) serum levels predict bevacizumab-based treatment response in metastatic colorectal cancer. Cancer Sci. 2014, 105, 996–1001. [Google Scholar] [CrossRef]
- Adenis, A.; De La Fouchardiere, C.; Paule, B.; Burtin, P.; Tougeron, D.; Wallet, J.; Dourthe, L.-M.; Etienne, P.-L.; Mineur, L.; Clisant, S.; et al. Survival, safety, and prognostic factors for outcome with Regorafenib in patients with metastatic colorectal cancer refractory to standard therapies: Results from a multicenter study (REBECCA) nested within a compassionate use program. BMC Cancer 2016, 16, 412. [Google Scholar] [CrossRef] [Green Version]
- Greten, F.R.; Grivennikov, S.I. Inflammation and cancer: Triggers, mechanisms, and consequences. Immunity 2019, 51, 27–41. [Google Scholar] [CrossRef]
- Mizuno, R.; Kawada, K.; Itatani, Y.; Ogawa, R.; Kiyasu, Y.; Sakai, Y. The role of tumor-associated neutrophils in colorectal cancer. Int. J. Mol. Sci. 2019, 20, 529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galdiero, M.R.; Bianchi, P.; Grizzi, F.; Di Caro, G.; Basso, G.; Ponzetta, A.; Bonavita, E.; Barbagallo, M.; Tartari, S.; Polentarutti, N.; et al. Occurrence and significance of tumor-associated neutrophils in patients with colorectal cancer: Significance of tumor-associated neutrophils in colorectal cancer. Int. J. Cancer 2016, 139, 446–456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiffmann, L.M.; Fritsch, M.; Gebauer, F.; Günther, S.D.; Stair, N.R.; Seeger, J.M.; Thangarajah, F.; Dieplinger, G.; Bludau, M.; Alakus, H.; et al. Tumour-infiltrating neutrophils counteract anti-VEGF therapy in metastatic colorectal cancer. Br. J. Cancer 2019, 120, 69–78. [Google Scholar] [CrossRef] [Green Version]
- Khan, U.; Chowdhury, S.; Billah, M.; Islam, K.; Thorlacius, H.; Rahman, M. Neutrophil extracellular traps in colorectal cancer progression and metastasis. Int. J. Mol. Sci. 2021, 22, 7260. [Google Scholar] [CrossRef] [PubMed]
- Watt, D.G.; Martin, J.C.; Park, J.H.; Horgan, P.G.; McMillan, D.C. Neutrophil count is the most important prognostic component of the differential white cell count in patients undergoing elective surgery for colorectal cancer. Am. J. Surg. 2015, 210, 24–30. [Google Scholar] [CrossRef] [PubMed]
- Grothey, A.; Yoshino, T.; Bodoky, G.; Ciuleanu, T.E.; Garcia-Carbonero, R.; García-Alfonso, P.; Van Cutsem, E.; Muro, K.; Mytelka, D.S.; Li, L.; et al. Association of baseline absolute neutrophil counts and survival in patients with metastatic colorectal cancer treated with second-line antiangiogenic therapies: Exploratory analyses of the RAISE trial and validation in an electronic medical record data set. ESMO Open 2018, 3, e000347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feliciano, E.M.C.; Kroenke, C.H.; Meyerhardt, J.A.; Prado, C.M.; Bradshaw, P.T.; Kwan, M.L.; Xiao, J.; Alexeeff, S.; Corley, D.; Weltzien, E.; et al. Association of systemic inflammation and sarcopenia with survival in nonmetastatic colorectal cancer: Results from the C SCANS Study. JAMA Oncol. 2017, 3, e172319. [Google Scholar] [CrossRef]
- Jakubowska, K.; Koda, M.; Kisielewski, W.; Kańczuga-Koda, L.; Grudzińska, M.; Famulski, W. Pre- and postoperative neutrophil and lymphocyte count and neutrophil-to-lymphocyte ratio in patients with colorectal cancer. Mol. Clin. Oncol. 2020, 13, 561. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, S.; Sheth, R.A.; Niekamp, A.S.; Aloia, T.A.; Chun, Y.S.; Lee, J.E.; Vauthey, J.-N.; Conrad, C. Comprehensive complication index predicts cancer-specific survival after resection of colorectal metastases independent of RAS mutational status. Ann. Surg. 2017, 266, 1045–1054. [Google Scholar] [CrossRef]
- Pietrantonio, F.; Miceli, R.; Rimassa, L.; Lonardi, S.; Aprile, G.; Mennitto, A.; Marmorino, F.; Bozzarelli, S.; Antonuzzo, L.; Tamburini, E.; et al. Estimating 12-week death probability in patients with refractory metastatic colorectal cancer: The Colon Life nomogram. Ann. Oncol. 2016, 28, 555–561. [Google Scholar] [CrossRef]
- Bekaii-Saab, T.S.; Ou, F.-S.; Ahn, D.H.; Boland, P.M.; Ciombor, K.K.; Heying, E.N.; Dockter, T.J.; Jacobs, N.L.; Pasche, B.C.; Cleary, J.M.; et al. Regorafenib dose-optimisation in patients with refractory metastatic colorectal cancer (ReDOS): A randomised, multicentre, open-label, phase 2 study. Lancet Oncol. 2019, 20, 1070–1082. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All (n, %) | Training Cohort (n, %) | Validation Cohort (n, %) | p-Value |
|---|---|---|---|---|
| n | 356 | 106 | 250 | |
| Age (mean, SD), years | 60.38 ± 11.2 | 62.02 ± 10.3 | 59.69 ± 11.5 | |
| Median (range) | 61 (17–97) | 64 (39–83) | 60 (17–97) | |
| Sex | ||||
| Female | 146 (41.0) | 43 (40.6) | 103 (41.2) | 0.99 |
| Male | 210 (59.0) | 63 (59.4) | 147 (58.8) | |
| ECOG PS | ||||
| 0–1 | 332 (93.3) | 93 (87.7) | 239 (95.6) | 0.01 |
| ≥2 | 24 (6.7) | 13 (12.3) | 11 (4.4) | |
| Primary site | ||||
| Left | 266 (74.7) | 75 (70.8) | 191 (76.4) | 0.17 |
| Right | 83 (23.3) | 30 (28.3) | 53 (21.2) | |
| Multifocal | 7 (2.0) | 1 (0.9) | 6 (2.4) | |
| Primary tumor resection | ||||
| Yes | 299 (84.0) | 91 (85.8) | 208 (83.2) | 0.64 |
| No | 57 (16.0) | 15 (14.2) | 42 (16.8) | |
| RAS status | ||||
| Wild | 175 (49.2) | 47 (44.3) | 128 (51.2) | 0.2 |
| Mutant | 177 (49.7) | 59 (55.7) | 118 (47.2) | |
| NA | 4 (1.1) | 0 | 4 (1.6) | |
| MMR status | ||||
| Proficient MMR | 154 (43.3) | 55 (51.9) | 99 (39.6) | 0.09 |
| Deficient MMR | 6 (1.7) | 2 (1.9) | 4 (1.6) | |
| NA | 196 (55.1) | 49 (46.2) | 147 (58.8) | |
| Organ metastasis | ||||
| Liver | 196 (55.1) | 64 (60.4) | 132 (52.8) | 0.2 |
| Lung | 226 (63.5) | 70 (66.0) | 156 (62.4) | 0.55 |
| Bone | 34 (9.6) | 8 (7.5) | 26 (10.4) | 0.55 |
| Peritoneum | 64 (18.0) | 24 (22.6) | 40 (16.0) | 0.17 |
| Previous treatment | ||||
| Anti-VEGF | 340 (95.5) | 103 (97.2) | 237 (94.8) | 0.41 |
| Anti-EGFR | 168 (47.2) | 49 (46.2) | 119 (47.6) | 0.82 |
| Time to regorafenib (month) | ||||
| ≥24 | 180 (50.6) | 50 (47.2) | 130 (52.0) | 0.42 |
| <24 | 176 (49.4) | 56 (52.8) | 120 (48.0) | |
| NLR | ||||
| <4 | 241 (67.7) | 71 (67.0) | 170 (68.0) | 0.9 |
| ≥4 | 115 (32.3) | 35 (33.0) | 80 (32.0) | |
| Hemoglobin (g/dL) | ||||
| ≥10 | 278 (78.1) | 83 (78.3) | 195 (78.0) | 0.99 |
| <10 | 78 (21.9) | 23 (21.7) | 55 (22.0) | |
| Initial dose of Regorafenib | ||||
| mean ± SD | 133.8 ± 30.7 | 103.8 ± 23.3 | 146.6 ± 23.7 | <0.001 |
| 160 mg | 186 (52.2) | 5 (4.7) | 181 (72.4) | |
| 120 mg | 108 (30.3) | 53 (50.0) | 55 (22.0) | |
| 80 mg or less | 62 (17.5) | 48 (45.3) | 14 (5.6) | |
| CEA, median, (ng/mL) | 53.1 | 62 | 47.9 | 0.15 |
| CEA (ng/mL) | ||||
| <50 | 173 (48.6) | 46 (43.4) | 127 (50.8) | 0.21 |
| ≥50 | 183 (51.4) | 60 (56.6) | 123 (49.2) |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p | HR (95% CI) | p |
| Sex (male vs. female) | 0.92 (0.61–1.38) | 0.67 | ||
| Age, years (≥60 vs. <60) | 0.71 (0.47–1.09) | 0.11 | ||
| ECOG PS (≥2 vs. 0–1) | 2.42 (1.30–4.52) | 0.004 | 1.40 (0.69–2.87) | 0.36 |
| Primary site (right vs. left) | 1.02 (0.65–1.59) | 0.95 | ||
| Primary tumor resection (no vs. yes) | 2.45 (1.39–4.31) | 0.001 | 0.85 (0.42–1.71) | 0.65 |
| RAS status (MT vs. WT) | 1.19 (0.79–1.78) | 0.41 | ||
| Time to regorafenib, mo (<24 vs. ≥24) | 1.91 (1.27–2.89) | 0.002 | 2.27 (1.44–3.60) | <0.0001 |
| Liver metastasis (yes vs. no) | 2.02 (1.33–3.07) | 0.001 | 1.61 (1.00–2.64) | 0.05 |
| Lung metastasis (yes vs. no) | 0.93 (0.61–1.43) | 0.75 | ||
| Bone metastasis (yes vs. no) | 2.77 (1.32–5.81) | 0.005 | 1.66 (0.73–3.78) | 0.23 |
| Peritoneum metastasis (yes vs. no) | 1.87 (1.13–3.09) | 0.013 | 1.68 (0.96–2.93) | 0.07 |
| NLR (≥4 vs. <4) | 2.01 (1.30–3.10) | 0.001 | ||
| Hemoglobin, g/dL (<10 vs. ≥10) | 2.25 (1.37–3.69) | 0.001 | 1.42 (0.79–2.56) | 0.24 |
| CEA, ng/mL (≥50 vs. <50) | 1.93 (1.27–2.94) | 0.002 | ||
| Initial dose of regorafenib ¶ (low vs. high) | 1.75 (1.16–2.64) | 0.007 | 1.48 (0.94–2.33) | 0.09 |
| CIPI (≥300 vs. <300) | 2.78 (1.82–4.23) | <0.0001 | 2.14 (1.23–3.74) | 0.007 |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Variables | HR (95% CI) | p | HR (95% CI) | p |
| Sex (male vs. female) | 1.07 (0.61–1.38) | 0.73 | ||
| Age, y (≥60 vs. <60) | 0.72 (0.48–1.08) | 0.10 | ||
| ECOG PS (≥2 vs. 0–1) | 1.82 (1.01–3.29) | 0.04 | 1.14 (0.61–2.15) | 0.68 |
| Primary site (right vs. left) | 0.98 (0.64–1.52) | 0.94 | ||
| Primary tumor resection (no vs. yes) | 1.56 (0.90–2.72) | 0.11 | ||
| RAS status (MT vs. WT) | 1.12 (0.76–1.65) | 0.57 | ||
| Time to regorafenib, month (<24 vs. ≥24) | 1.74 (1.16–2.60) | 0.006 | 1.76 (1.15–2.68) | 0.009 |
| Liver metastasis (yes vs. no) | 1.66 (1.10–2.48) | 0.01 | 1.52 (0.94–2.45) | 0.09 |
| Lung metastasis (yes vs. no) | 0.75 (0.50–1.13) | 0.17 | ||
| Bone metastasis (yes vs. no) | 1.31 (0.63–2.70) | 0.47 | ||
| Peritoneum metastasis (yes vs. no) | 2.10 (1.31–3.37) | 0.001 | 2.18 (1.34–3.56) | 0.002 |
| NLR (≥4 vs. <4) | 1.65 (1.08–2.50) | 0.02 | ||
| Hemoglobin, g/dL (<10 vs. ≥10) | 1.68 (1.05–2.70) | 0.03 | 1.36 (0.83–2.23) | 0.23 |
| CEA, ng/mL (≥50 vs. <50) | 1.31 (0.88–1.94) | 0.17 | ||
| Dose of regorafenib ¶ (low vs. high) | 1.04 (0.70–1.54) | 0.84 | ||
| CIPI (≥300 vs. <300) | 1.69 (1.14–2.51) | 0.007 | 1.24 (1.77–1.98) | 0.38 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, Y.-L.; Tsai, K.-L.; Chiu, T.-J.; Lin, Y.-M.; Lee, K.-C.; Lu, C.-C.; Chen, H.-H.; Wu, C.-C.; Hsu, H.-C. Development and Validation of a Novel Serum Prognostic Marker for Patients with Metastatic Colorectal Cancer on Regorafenib Treatment. Cancers 2021, 13, 5080. https://doi.org/10.3390/cancers13205080
Su Y-L, Tsai K-L, Chiu T-J, Lin Y-M, Lee K-C, Lu C-C, Chen H-H, Wu C-C, Hsu H-C. Development and Validation of a Novel Serum Prognostic Marker for Patients with Metastatic Colorectal Cancer on Regorafenib Treatment. Cancers. 2021; 13(20):5080. https://doi.org/10.3390/cancers13205080
Chicago/Turabian StyleSu, Yu-Li, Kai-Lung Tsai, Tai-Jan Chiu, Yueh-Ming Lin, Ko-Chao Lee, Chien-Chang Lu, Hong-Hwa Chen, Chia-Che Wu, and Hung-Chih Hsu. 2021. "Development and Validation of a Novel Serum Prognostic Marker for Patients with Metastatic Colorectal Cancer on Regorafenib Treatment" Cancers 13, no. 20: 5080. https://doi.org/10.3390/cancers13205080
APA StyleSu, Y.-L., Tsai, K.-L., Chiu, T.-J., Lin, Y.-M., Lee, K.-C., Lu, C.-C., Chen, H.-H., Wu, C.-C., & Hsu, H.-C. (2021). Development and Validation of a Novel Serum Prognostic Marker for Patients with Metastatic Colorectal Cancer on Regorafenib Treatment. Cancers, 13(20), 5080. https://doi.org/10.3390/cancers13205080