The Impact of Multidisciplinary Team Meetings on Patient Management in Oncologic Thoracic Surgery: A Single-Center Experience

 ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Specchia, M.L.; Frisicale, E.M.; Carini, E. The impact of tumor board on cancer care: Evidence from an umbrella review. BMC Health Serv. Res. 2020, 20, 73. [Google Scholar] [CrossRef] [PubMed]
- Lesslie, M.; Parikh, J.R. Implementing a Multidisciplinary Tumor Board in the Community Practice Setting. Diagnostic 2017, 7, 55. [Google Scholar] [CrossRef] [PubMed]
- Stone, E.; Rankin, N.; Kerr, S.; Fong, K.; Currow, D.C.; Phillips, J.; Connon, T.; Zhang, L.; Shaw, T. Does presentation at multidisciplinary team meetings improve lung cancer survival? Findings from a consecutive cohort study. Lung Cancer 2018, 124, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Bilfinger, T.V.; Albano, D.; Perwaiz, M.; Keresztes, R.; Nemesure, B. Survival outcomes among lung cancer patients treated using a multidisciplinary team approach. Clin. Lung Cancer 2018, 19, 346–351. [Google Scholar] [CrossRef]
- Boxer, M.M.; Vinod, S.K.; Shafiq, J.; Duggan, K.J. Do multidisciplinary team meetings make a difference in the management of lung cancer? Cancer 2011, 117, 5112–5120. [Google Scholar] [CrossRef]
- Pillay, B.; Wootten, A.C.; Crowe, H.; Corcoran, N.; Tran, B.; Bowden, P.; Crowe, J.; Costello, A.J. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat. Rev. 2016, 42, 56–72. [Google Scholar] [CrossRef]
- Ung, K.A.; Campbell, B.A.; Duplan, D.; Ball, D.; David, S. Impact of the lung oncology multidisciplinary team meetings on the management of patients with cancer. Asia Pac. J. Clin. Oncol. 2016, 12, e298–e304. [Google Scholar] [CrossRef]
- Conron, M.; Phuah, S.; Steinfort, D.; Dabscheck, E.; Wright, G.; Hart, D. Analysis of multidisciplinary lung cancer practice. Intern. Med. J. 2007, 37, 18–25. [Google Scholar] [CrossRef]
- Smeltzer, M.P.; Rugless, F.E.; Jackson, B.M.; Berryman, C.L.; Faris, N.R.; Ray, M.A.; Meadows, M.; Patel, A.A.; Roark, K.S.; Kedia, S.K.; et al. Pragmatic trial of a multidisciplinary lung cancer care model in a community healthcare setting: Study design, implementation evaluation, and baseline clinical results. Transl. Lung Cancer Res. 2018, 7, 88–102. [Google Scholar] [CrossRef]
- Lamprell, K.; Arnolda, G.; Delaney, G.P.; Liauw, W.; Braithwaite, J. The challenge of putting principles into practice: Resource tensions and real-world constraints in multidisciplinary oncology team meetings. Asia Pac. J. Clin. Oncol. 2019, 15, 199–207. [Google Scholar] [CrossRef]
- Campbell, B.A.; Ball, D.; Mornex, F. Multidisciplinary lung cancer meetings: Improving the practice of radiation oncology and facing future challenges. Respirology 2015, 20, 192–198. [Google Scholar] [CrossRef] [PubMed]
- Stone, E.; Rankin, N.; Phillips, J.; Fong, K.; Currow, D.C.; Miller, A.; Largey, G.; Zielinski, R.; Flynn, P.; Shaw, T.; et al. Consensus minimum data set for lung cancer multidisciplinary teams: Results of a Delphi process. Respirology 2018, 23, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Fennell, M.L.; Das, I.P.; Clauser, S.; Petrelli, N.; Salner, A. The Organization of Multidisciplinary Care Teams: Modeling internal and external influences on Cancer care quality. J. Natl. Cancer Inst. Monogr. 2010, 40, 72–80. [Google Scholar] [CrossRef] [PubMed]
- Kurpad, R.; Kim, W.; Rathmell, W.K.; Godley, P.; Whang, Y.; Fielding, J.; Smith, L.; Pettiford, A.; Schultz, H.; Nielsen, M.; et al. A multidisciplinary approach to the management of urologic malignancies: Does it influence diagnostic and treatment decisions? Urol. Oncol. Semin. Orig. Investig. 2011, 29, 378–382. [Google Scholar] [CrossRef] [PubMed]
- American College of Chest Physicians; Health and Science Policy Committee. Diagnosis and management of lung cancer: ACCP evidence-based guidelines. Chest 2003, 123 (Suppl. 1), 1S–19S. [Google Scholar] [CrossRef]
- Cancer Council Australia. Clinical Practice Guidelines for the Prevention, Diagnosis and Management of Lung Cancer. Cancer Council Australia. 2004. Available online: http://www.nhmrc.gov.au/publications/subjects/cancer.htm (accessed on 8 October 2020).
- The Lung Cancer Working Party of the British Thoracic Society Standards of Care Committee. BTS recommendations to respiratory physicians for organising the care of patients with lung cancer. The Lung Cancer Working Party of the British Thoracic Society Standards of Care Committee. Thorax 1998, 53 (Suppl. 1), S1–S8. [Google Scholar] [CrossRef] [PubMed]
- Coory, M.; Gkolia, P.; Yang, I.A. Systematic review of multidisciplinary teams in the management of lung cancer. Lung Cancer 2008, 60, 4–21. [Google Scholar] [CrossRef]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Dunlop, D.J. An evaluation of the impact of a multidisciplinary team, in a single centre, on treatment and survival in patients with inoperable non-smallcell lung cancer. Br. J. Cancer 2005, 93, 977–978. [Google Scholar] [CrossRef]
- Price, A.; Kerr, G.; Gregor, A.; Ironside, J.; Little, F. The impact of multidisciplinary teams and site specialisation on the use of radiotherapy in elderly people with non-small cell lung cancer (NSCLC). Radiother. Oncol. 2002, 64 (Suppl. 1). [Google Scholar]
- Murray, P.V.; O’Brien, M.E.R.; Sayer, R.; Cooke, N.; Knowles, A.C.; Miller, A.C.; Varney, V.; Rowell, N.P.; Padhani, A.R.; MacVicar, D.; et al. The pathway study: Results of a pilot feasibility study in patients suspected of having lung carcinoma investigated in a conventional chest clinic setting compared to a centralised two-stop pathway. Lung Cancer 2003, 42, 283–290. [Google Scholar] [CrossRef]
- Martin-Ucar, A.E.; Waller, D.A.; Atkins, J.L.; Swinson, D.; O’Byrne, K.J.; Peake, M.D. The beneficial effects of specialist thoracic surgery on the resection rate for non-small-cell lung cancer. Lung Cancer 2004, 46, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Dillman, R.O.; Chico, S.D. Cancer patient survival improvement is correlated with the opening of a community cancer centre: Comparisons with intramural and extramural benchmarks. J. Oncol. Pract. 2005, 1, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Wheless, S.A.; McKinney, K.A.; Zanation, A.M. A prospective study of the clinical impact of a multidisciplinary head and neck tumor board. Otolaryngol. Head Neck 2010, 143, 650–654. [Google Scholar] [CrossRef] [PubMed]
- Gatcliffe, T.A.; Coleman, R.L. Tumor board: More than treatment planning: A 1-year prospective survey. J. Cancer Educ. 2008, 23, 235–237. [Google Scholar] [CrossRef] [PubMed]
- Acher, P.L.; Young, A.J.; Etherington-Foy, R.; McCahy, P.J.; Deane, A.M. Improving outcomes in urological cancers: The impact of “multidisciplinary team meetings”. Int. J. Surg. 2005, 3, 121–123. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Greer, H.O.; Frederick, P.J.; Falls, N.M.; Tapley, E.B.; Samples, K.L.; Kimball, K.J.; Kendrick, J.E.; Conner, M.G.; Novak, L.; Michael, J.; et al. Impact of a weekly multidisciplinary tumor board conference on the management of women with gynecologic malignancies. Int. J. Gynecol. Cancer 2010, 20, 1321–1325. [Google Scholar]
- Newman, E.A.; Guest, A.B.; Helvie, M.A.; Roubidoux, M.A.; Chang, A.E.; Kleer, C.G.; Diehl, K.M.; Cimmino, V.M.; Pierce, L.; Hayes, D.; et al. Changes in surgical management resulting from case review at a breast cancer multidisciplinary tumor board. Cancer 2006, 107, 2346–2351. [Google Scholar] [CrossRef]
- Casiraghi, M.; Bertolaccini, L.; Sedda, G.; Petrella, F.; Galetta, D.; Guarize, J.; Maisonneuve, P.; De Marinis, F.; Spaggiari, L. Lung cancer surgery in oligometastatic patients: Outcome and survival. Eur. J. Cardiothorac. Surg. 2020, 57, 1173–1180. [Google Scholar] [CrossRef]
- Bini, A.; Grazia, M.; Petrella, F.; Chittolini, M. Multiple chondromatous hamartomas of the lung. Interact. Cardiovasc. Thorac. Surg. 2002, 1, 78–80. [Google Scholar] [CrossRef]
- Petrella, F.; Rizzo, S.; Radice, D.; Borri, A.; Galetta, D.; Gasparri, R.; Solli, P.; Veronesi, G.; Bellomi, M.; Spaggiari, L. Predicting prolonged air leak after standard pulmonary lobectomy: Computed tomography assessment and risk factors stratification. Surgeon 2011, 9, 72–77. [Google Scholar] [CrossRef]
- Petrella, F.; Chieco, P.; Solli, P.; Veronesi, G.; Borri, A.; Galetta, D.; Gasparri, R.; Spaggiari, L. Which factors affect pulmonary function after lung metastasectomy? Eur. J. Cardiothorac. Surg. 2009, 35, 792–796. [Google Scholar] [CrossRef] [PubMed]
- Casiraghi, M.; Maisonneuve, P.; Piperno, G. Salvage Surgery after Definitive Chemoradiotherapy for Non–small Cell Lung Cancer. Semin. Thorac. Cardiovasc. Surg. 2017, 29, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Fanti, S.; Farsad, M.; Battista, G. Somatostatin Receptor Scintigraphy for Bronchial Carcinoid Follow-Up. Clin. Nucl. Med. 2003, 28, 548–552. [Google Scholar] [CrossRef] [PubMed]
- Pelosi, G.; Petrella, F.; Sandri, M.T.; Spaggiari, L.; Galetta, D.; Viale, G. A primary pure yolk sac tumor of the lung exhibiting CDX-2 immunoreactivity and increased serum levels of alkaline phosphatase intestinal isoenzyme. Int. J. Surg. Pathol. 2006, 14, 247–251. [Google Scholar] [CrossRef] [PubMed]
- Klarenbeek, S.E.; Schuurbiers-Siebers, O.C.J.; van den Heuvel, M.M.; Prokop, M.; Tummers, M. Barriers and Facilitators for Implementation of a Computerized Clinical Decision Support System in Lung Cancer Multidisciplinary Team Meetings—A Qualitative Assessment. Biology 2020, 10, 9. [Google Scholar] [CrossRef]
- Shashi, K.K.; Madan, R.; Hammer, M.M.; van Hedent, S.; Byrne, S.C.; Schmidlin, E.J.; Mamon, H.; Hatabu, H.; Enzinger, P.C.; Gerbaudo, V.H. Contribution of FDG-PET/CT to the management of esophageal cancer patients at multidisciplinary tumor board conferences. Eur. J. Radiol. Open 2020, 7, 100291. [Google Scholar] [CrossRef]
- Crichi, B.; Sebuhyan, M.; Abdallah, N.A.; Montlahuc, C.; Bonnet, C.; Villiers, S.; Maignan, C.L.; Yannoutsos, A.; Farge, D. How to treat venous thromboembolism (TVE) in cancer patients: Ten years of multidisciplinary team meetings (MDTM) at Saint-Louis Hospital. J. Med. Vasc. 2020, 45, S24–S26. [Google Scholar]
- Graetz, D.E.; Chen, Y.; Devidas, M.; Antillon-Klussmann, F.; Fu, L.; Quintero, K.; Fuentes-Alabi, S.L.; Gassant, P.Y.; Kaye, E.C.; Baker, J.N. Interdisciplinary care of pediatric oncology patients in Central America and the Caribbean. Cancer 2020. [Google Scholar] [CrossRef]
- Karas, P.L.; Rankin, N.M.; Stone, E. Medicolegal Considerations in Multidisciplinary Cancer Care. JTO Clin. Res. Rep. 2020, 1, 100073. [Google Scholar] [CrossRef]
- Zhao, S.; Qi, W.; Chen, J. Role of a multidisciplinary team in administering radiotherapy for esophageal cancer. BMC Cancer 2020, 20, 974. [Google Scholar] [CrossRef]
- Dijkstra, S.; Kraal, K.C.J.M.; Ruijters, V.J.; Kremer, L.C.M.; Hoogerbrugge, P.M. Examining the Potential Relationship between Multidisciplinary Team Meetings and Patient Survival in Pediatric Oncology Settings: A Systematic Review. J. Pediatr. Hematol. Oncol. 2020, 102, 125–134. [Google Scholar] [CrossRef] [PubMed]
- Warner, R.; Hoinville, L.; Pottle, E.; Taylor, C.; Green, J. Refocusing cancer multidisciplinary team meetings in the United Kingdom: Comparing urology with other specialties. Ann. R. Coll. Surg. Engl. 2021, 103, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Liam, C.K.; Liam, Y.S.; Poh, M.E.; Wong, C.K. Accuracy of lung cancer staging in the multidisciplinary team setting. Transl. Lung Cancer Res. 2020, 9, 1654–1666. [Google Scholar] [CrossRef] [PubMed]
- Pluyter, J.R.; Jacobs, I.; Langereis, S.; Cobben, D.; Williams, S.; Curfs, J.; van den Borne, B. Looking through the eyes of the multidisciplinary team: The design and clinical evaluation of a decision support system for lung cancer care. Transl. Lung Cancer Res. 2020, 9, 1422–1432. [Google Scholar] [CrossRef]
- Petrella, F.; Toffalorio, F.; Brizzola, S.; De Pas, T.M.; Rizzo, S.; Barberis, M.; Pelicci, P.; Spaggiari, L.; Acocella, F. Stem cell transplantation effectively occludes bronchopleural fistula in an animal model. Ann. Thorac. Surg. 2014, 97, 480–483. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Characteristic | Statistics a | ||
|---|---|---|---|
| Age, years | 65.2 (11.1) | ||
| Out-patient time/MDT (days) | 33.0 (27.0–43.5) | ||
| Gender | Male | 590 (59.0) | |
| Female | 410 (41.0) | ||
| Histology | Available | not available | 776 (77.6) |
| Lung adenocarcinoma | 128 (57.1) | ||
| Squamous cell | 40 (17.9) | ||
| Pulmonary carcinoid | 12 (5.4) | ||
| Small cell lung cancer | 6 (2.7) | ||
| Other histology | 38 (17.0) | ||
| Overall available | 224 (22.4) | ||
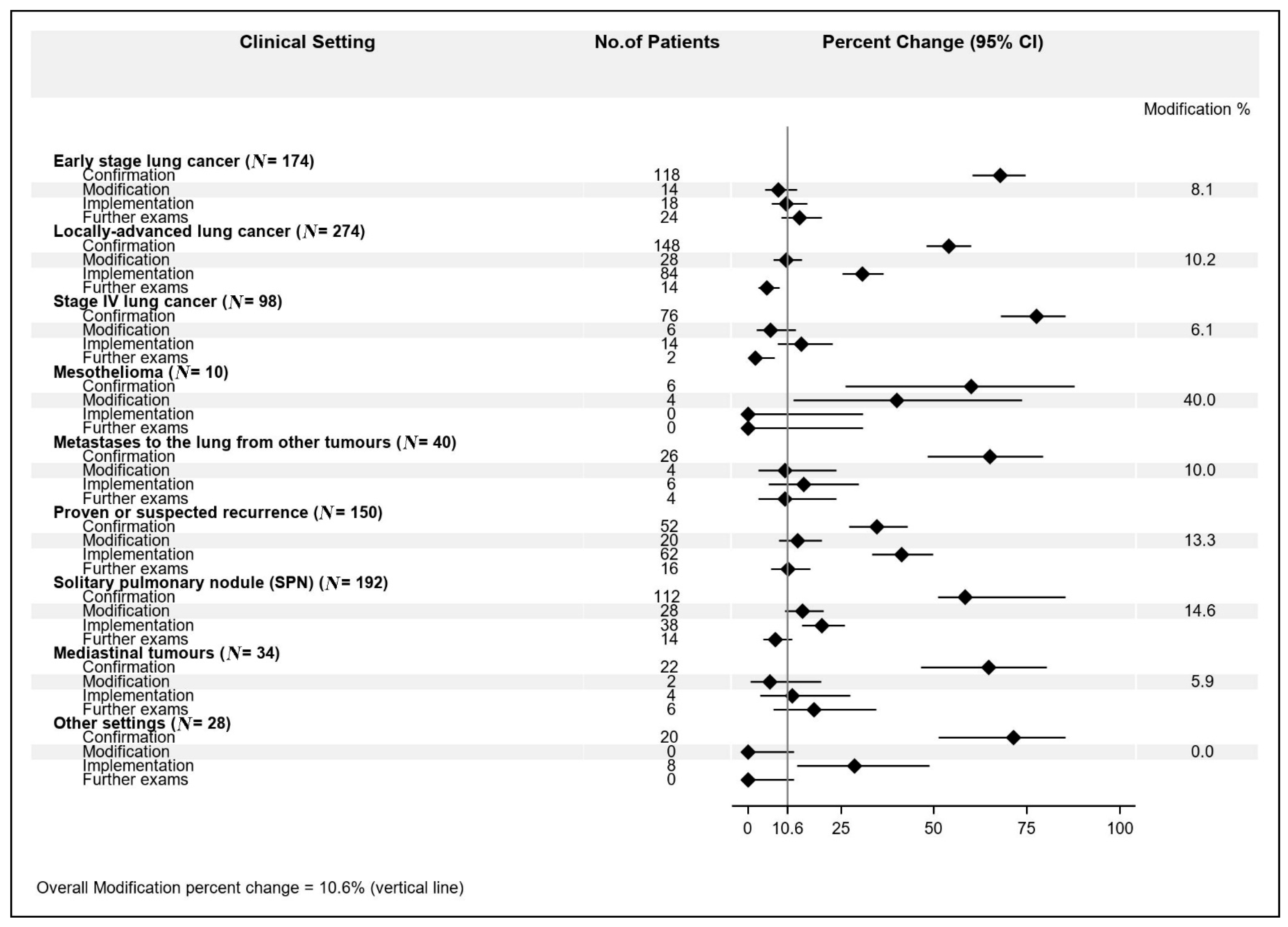
| Clinical settings | Locally advanced lung cancer | 274 (27.4) | |
| Solitary pulmonary nodule | 192 (19.2) | ||
| Early stage lung cancer | 174 (17.4) | ||
| Proven or suspected recurrence | 150 (15.0) | ||
| Stage IV lung cancer | 98 (9.8) | ||
| Metastases to the lung from other tumors | 40 (4.0) | ||
| Mediastinal tumors | 34(3.4) | ||
| Mesothelioma | 10 (1.0) | ||
| Other | 28 (2.8) | ||
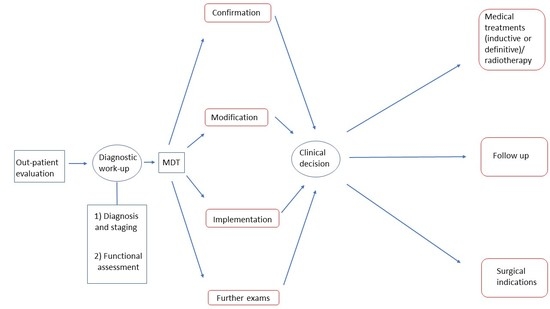
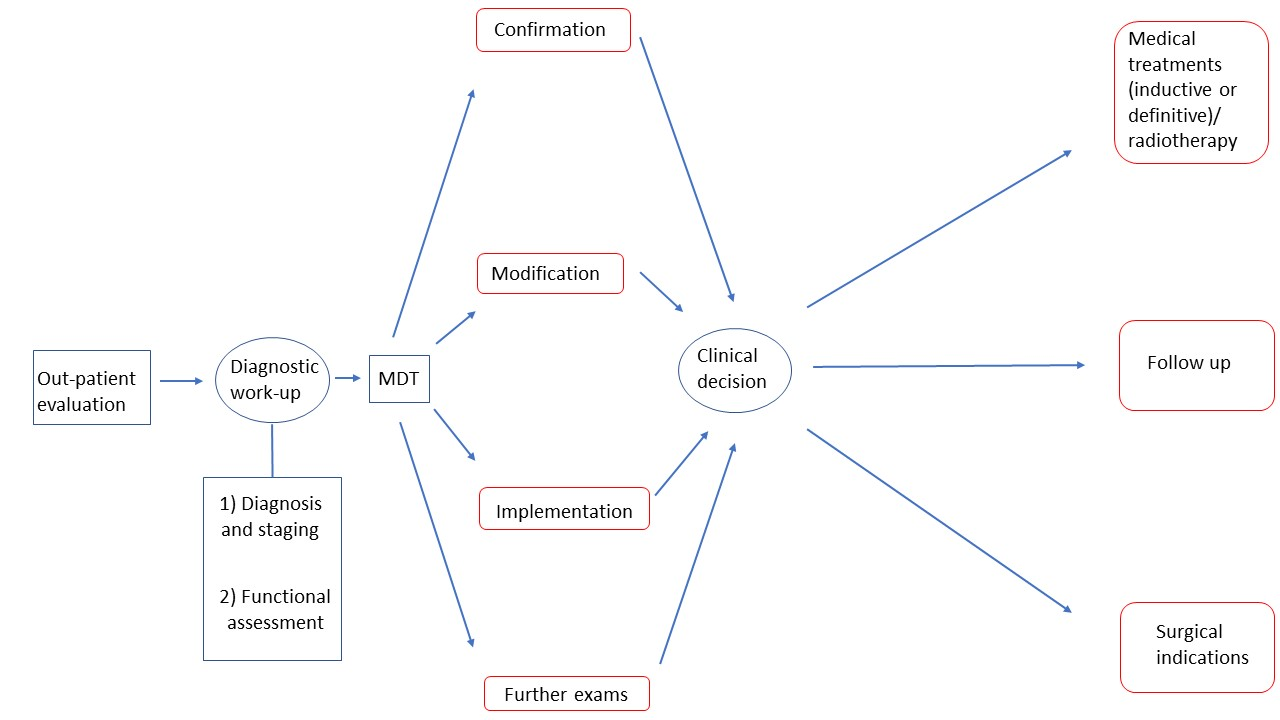
| Impact of MDT discussion | Confirmation | 580 (58.0) | |
| Modification | 106 (10.6) | ||
| Implementation | 234 (23.4) | ||
| Further exams | 80 (8.0) | ||
| Specific Examination | Biopsy | 18 (22.5) | |
| Biopsy + further imaging exams | 26 (32.5) | ||
| Colonoscopy/esophago-gastroscopy | 10 (12.5) | ||
| Further imaging exams | 18 (22.5) | ||
| Specialist consultation b | 8 (10.0) |
| Histology | Overall N (%) | Confirmation N = 156 | MDT Impact Level, N (Row %) | Further Exams N = 18 | p-Value | |
|---|---|---|---|---|---|---|
| Modification N = 26 | Implementation N = 24 | |||||
| Lung adenocarcinoma | 128 (57.1) | 88 (68.8) | 16 (12.5) | 12 (9.4) | 12 (9.4) | |
| Squamous cell | 40 (18.0) | 20 (50.0) | 6 (15.0) | 8 (20.0) | 6 (15.0) | |
| Pulmonary carcinoid | 12 (5.4) | 12 (100) | 0 | 0 | 0 | 0.03 |
| Small cell lung cancer | 6 (2.7) | 4 (66.7) | 2 (33.3) | 0 | 0 | |
| Other | 38 (16.7) | 32 (84.2) | 2 (5.3) | 4 (10.5) | 0 | |
| Clinical Setting | Histology | MDT Impact, N (col %) | p-Value | |
|---|---|---|---|---|
| Modification | Other | |||
| Early Stage Lung Cancer | Not yet available | 14 (100) | 98 (61.3) | |
| Available | 0 | 62 (38.8) | 0.002 | |
| Locally Advanced Lung Cancer | Not yet available | 8 (28.6) | 152 (61.8) | |
| Available | 20 (71.4) | 94 (38.2) | 0.001 | |
| Stage IV Lung Cancer | Not yet available | 4 (66.7) | 66 (71.7) | |
| Available | 2 (33.3) | 26 (28.3) | 1.00 | |
| Mesothelioma | Not yet available | 2 (50.0) | 4 (66.7) | |
| Available | 2 (50.0) | 2 (33.3) | 1.00 | |
| Metastases to the lung from other tumors | Not yet available | 4 (100) | 34 (94.4) | |
| Available | 0 | 2 (5.6) | 1.00 | |
| Proven or suspected recurrence | Not yet available | 20 (100) | 120 (92.3) | |
| Available | 0 | 10 (7.7) | 0.36 | |
| Solitary pulmonary nodule | Not yet available | 28 (100) | 164 (100) | |
| Available | 0 | 0 | - | |
| Mediastinal tumor | Not yet available | 2 (100) | 30 (93.8) | |
| Available | 0 | 2 (6.3) | 1.00 | |
| Other | Not yet available | 0 | 28 (100) | |
| Available | 0 | 0 | - | |
| Clinical Setting | Factor | Level | OR (95% CI) | p-Value |
|---|---|---|---|---|
| Early Stage Lung Cancera | Sex | Female | 1 | |
| Male | 1.21 (0.35–4.16) | 0.76 | ||
| Age | 0.95 (0.72–1.25) | 0.71 | ||
| Out-patient time/MDT days | 1.57 (1.00–2.47) | 0.05 | ||
| Locally Advanced Lung Cancer | Sex | Female | 1 | |
| Male | 1.08 (0.48–2.43) | 0.76 | ||
| Histology | Not yet available | 1 | ||
| Available | 4.04 (1.71–0.45) | 0.001 | ||
| Age | 1.21 (0.97–1.52) | 0.10 | ||
| Out-patient time/MDT days | 1.66 (1.15–2.41) | 0.007 | ||
| Stage IV Lung Cancer | Sex | Female | 1 | |
| Male | 1.17 (0.20–6.72) | 0.86 | ||
| Histology | Not Available | 1 | ||
| Available | 4.57 (0.79–26.4) | 0.09 | ||
| Age | 0.91 (0.61–1.36) | 0.64 | ||
| Out-patient time/MDT days | 0.50 (0.17–1.46) | 0.20 | ||
| Mesotheliomab | Histology | Not Available | 1 | |
| Available | 2.00 (0.15–26.7) | 0.60 | ||
| Age | Not estimable | - | ||
| Out-patient time/MDT days | 2.56 (0.64–10.3) | 0.18 | ||
| Metastases to the lung from other tumors c | Sex | Female | 1 | |
| Male | Not estimabled | 0.76 | ||
| Age | 0.59§ (0.23–1.51) | 0.27 | ||
| Out-patient time/MDT days | 0.96 (0.32–2.86) | 0.94 | ||
| Proven or suspected recurrencee | Sex | Female | 1 | |
| Male | 1.77 (0.68–4.63) | 0.25 | ||
| Age | 1.05 (0.84–1.32) | 0.67 | ||
| Out-patient time/MDT days | 0.66 (0.38–1.15) | 0.94 | ||
| Solitary pulmonary nodulef | Sex | Female | 1 | |
| Male | 0.99 (0.44–2.23) | 0.99 | ||
| Age | 1.31 (1.03–1.68) | 0.03 | ||
| Out-patient time/MDT days | 1.11 (0.74–1.66) | 0.61 | ||
| Mediastinal tumorg | Sex | Female | 1 | |
| Male | Not estimable d | - | ||
| Age | 0.77 (0.42–1.42) | 0.41 | ||
| Out-patient time/MDT days | 0.99 (0.17–5.71) | 0.99 |
| Factor | Level | OR (95% CI) | p-Value |
|---|---|---|---|
| Histology | Not yet available | 1 | |
| Available | 5.55 (2.23–13.7) | < 0.001 | |
| Out-patient time/MDT days a | 1.04 (1.02–1.07) | < 0.001 |
| Author (ref n.) | Year | Clinical Setting |
|---|---|---|
| Klarenbeek SE (36) | 2020 | Lung cancer |
| Shashi KK (37) | 2020 | Esophageal cancer |
| Crichi B (38) | 2020 | Venous thromboembolism in cancer patient |
| Graetz DE (39) | 2020 | Pediatric oncology |
| Karas PL (40) | 2020 | Medicolegal aspects in cancer care |
| Zhao S (41) | 2020 | Esophageal cancer |
| Dijkstra S (42) | 2020 | Pediatric oncology |
| Warner R (43) | 2021 | Urologic cancer |
| Liam CK (44) | 2020 | Lung cancer |
| Pluyter JR (45) | 2020 | Lung cancer |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrella, F.; Radice, D.; Guarize, J.; Piperno, G.; Rampinelli, C.; de Marinis, F.; Spaggiari, L. The Impact of Multidisciplinary Team Meetings on Patient Management in Oncologic Thoracic Surgery: A Single-Center Experience. Cancers 2021, 13, 228. https://doi.org/10.3390/cancers13020228
Petrella F, Radice D, Guarize J, Piperno G, Rampinelli C, de Marinis F, Spaggiari L. The Impact of Multidisciplinary Team Meetings on Patient Management in Oncologic Thoracic Surgery: A Single-Center Experience. Cancers. 2021; 13(2):228. https://doi.org/10.3390/cancers13020228
Chicago/Turabian StylePetrella, Francesco, Davide Radice, Juliana Guarize, Gaia Piperno, Cristiano Rampinelli, Filippo de Marinis, and Lorenzo Spaggiari. 2021. "The Impact of Multidisciplinary Team Meetings on Patient Management in Oncologic Thoracic Surgery: A Single-Center Experience" Cancers 13, no. 2: 228. https://doi.org/10.3390/cancers13020228
APA StylePetrella, F., Radice, D., Guarize, J., Piperno, G., Rampinelli, C., de Marinis, F., & Spaggiari, L. (2021). The Impact of Multidisciplinary Team Meetings on Patient Management in Oncologic Thoracic Surgery: A Single-Center Experience. Cancers, 13(2), 228. https://doi.org/10.3390/cancers13020228