
Survival in Advanced-Stage Epithelial Ovarian Cancer Patients with Cardiophrenic Lymphadenopathy Who Underwent Cytoreductive Surgery: A Systematic Review and Meta-Analysis

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Material and Methods
2.1. Data Sources and Searches
2.2. Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Data Synthesis and Analysis
3. Results
3.1. General Characteristic
3.2. Intervention
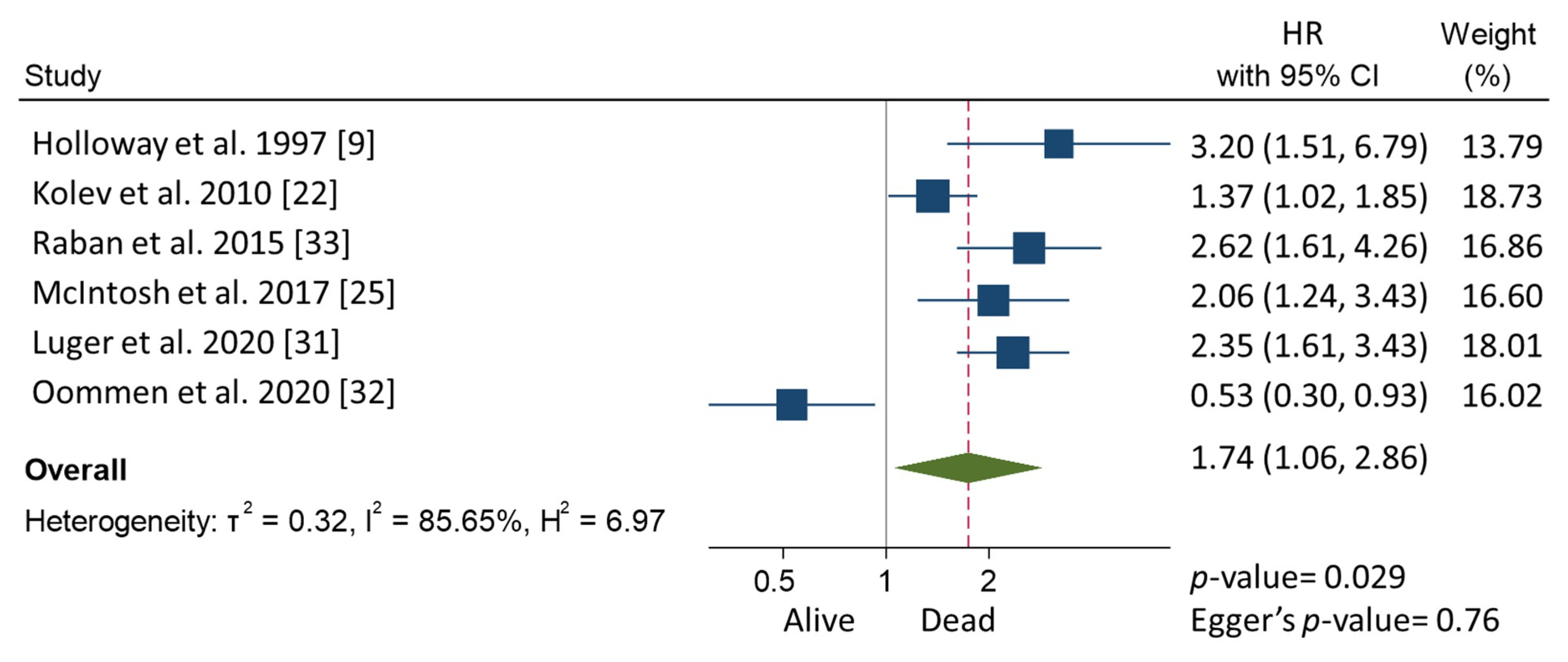
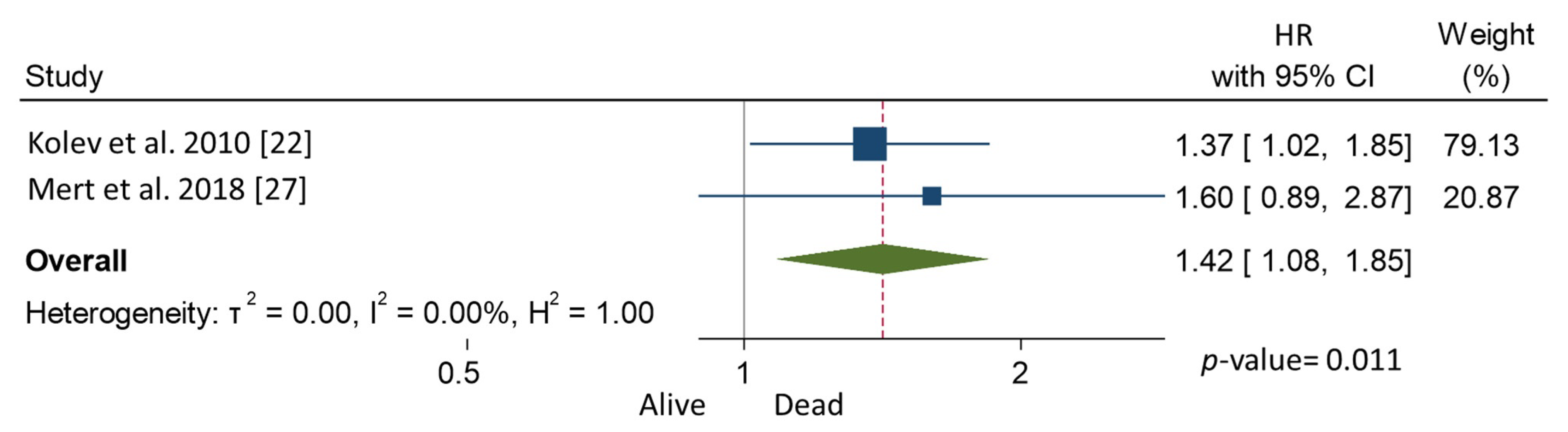
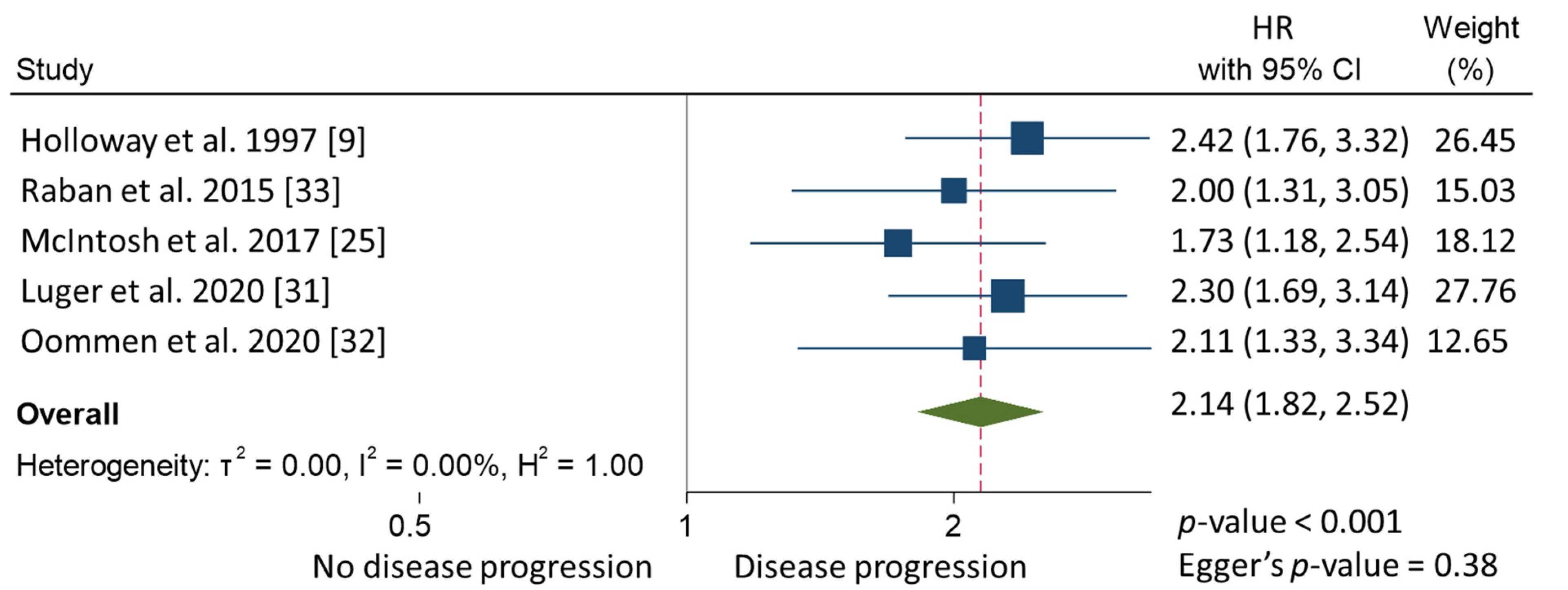
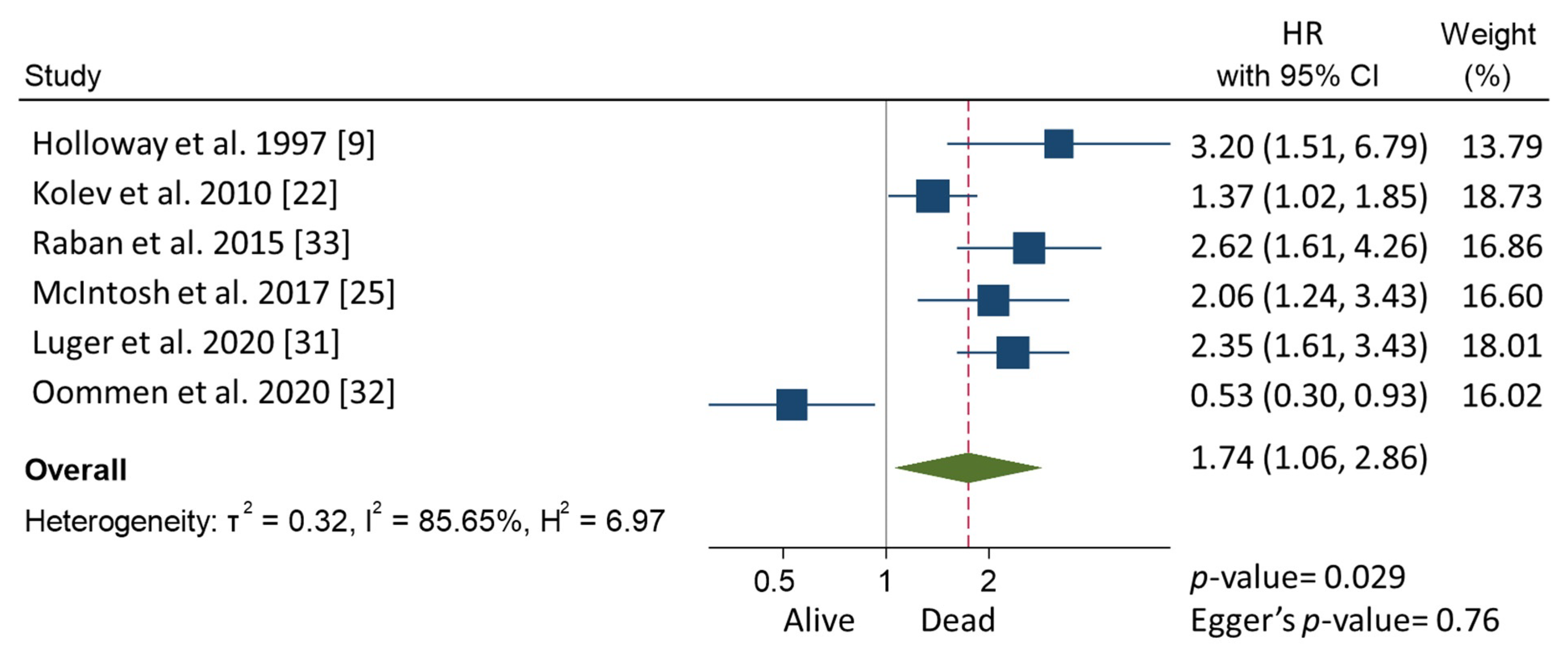
3.3. Meta-Analysis
4. Discussion
Strength and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ASA | American Society of Anesthesiologists |
| AEOC | Advanced-stage epithelial ovarian cancer |
| CPLN | Cardiophrenic lymph nodes |
| CT | Computed tomography scan |
| EOC | Epithelial ovarian cancer |
| ESGO | European Society of Gynecological Oncology |
| ESUR | European Society of Urogenital Radiology |
| FIGO | International Federation of Gynecology and Obstetrics |
| IDS | Interval debulking surgery |
| NACT | Neoadjuvant chemotherapy |
| MRI | Magnetic resonance imaging scan |
| OS | Overall survival |
| PFS | Progression-free survival |
| VATS | Video-assisted thoracic surgery |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Steinberga, I.; Jansson, K.; Sorbe, B. Quality Indicators and Survival Outcome in Stage IIIB-IVB Epithelial Ovarian Cancer Treated at a Single Institution. In Vivo 2019, 33, 1521–1530. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar]
- Bristow, R.E.; Tomacruz, R.S.; Armstrong, D.K.; Trimble, E.L.; Montz, F.J. Survival effect of maximal cytoreductive surgery for ad-vanced ovarian carcinoma during the platinum era: A meta-analysis. J. Clin. Oncol. 2002, 20, 1248–1259. [Google Scholar] [CrossRef] [PubMed]
- Chang, S.-J.; Hodeib, M.; Chang, J.; Bristow, R.E. Survival impact of complete cytoreduction to no gross residual disease for advanced-stage ovarian cancer: A meta-analysis. Gynecol. Oncol. 2013, 130, 493–498. [Google Scholar] [CrossRef]
- Colombo, P.-E.; Mourregot, A.; Fabbro, M.; Gutowski, M.; Saint-Aubert, B.; Quenet, F.; Gourgou, S.; Rouanet, P. Aggressive surgical strategies in advanced ovarian cancer: A monocentric study of 203 stage IIIC and IV patients. Eur. J. Surg. Oncol. 2009, 35, 135–143. [Google Scholar] [CrossRef]
- Berek, J.S.; Kehoe, S.T.; Kumar, L.; Friedlander, M. Cancer of the ovary, fallopian tube, and peritoneum. Int. J. Gynecol. Obstet. 2018, 143, 59–78. [Google Scholar] [CrossRef]
- Harter, P.; Sehouli, J.; Lorusso, D.; Reuss, A.; Vergote, I.; Marth, C.; Kim, J.-W.; Raspagliesi, F.; Lampe, B.; Aletti, G.; et al. A Randomized Trial of Lymphadenectomy in Patients with Advanced Ovarian Neoplasms. N. Engl. J. Med. 2019, 380, 822–832. [Google Scholar] [CrossRef]
- Holloway, B.; Gore, M.; A’Hern, R.; Parsons, C. The significance of paracardiac lymph node enlargement in ovarian cancer. Clin. Radiol. 1997, 52, 692–697. [Google Scholar] [CrossRef]
- Forstner, R.; Sala, E.; Kinkel, K.; Spencer, J.A. ESUR guidelines: Ovarian cancer staging and follow-up. Eur. Radiol. 2010, 20, 2773–2780. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.; Costa, R.L.R.; Di Paula, R.; Anton, C.; Calheiros, Y.; Sartorelli, V.; Kanashiro, Y.M.; De Lima, J.A.; Yamada, A.; Pinto, G.L.D.S.; et al. Cardiophrenic lymph node resection in cytoreduction for primary advanced or recurrent epithelial ovarian carcinoma: A cohort study. Int. J. Gynecol. Cancer 2019, 29, 188–194. [Google Scholar] [CrossRef]
- LaFargue, C.J.; Bristow, R.E. Transdiaphragmatic cardiophrenic lymph node resection for Stage IV ovarian cancer. Gynecol. Oncol. 2015, 138, 762–763. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; PRISMA-S Group; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B. PRISMA-S: An extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B.; et al. Meta-analysis of Observational Studies in Epidemiology. A Proposal for Reporting. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Harzing, A.W. Publish or Perish. 2007. Available online: https://harzing.com/resources/publish-or-perish (accessed on 1 June 2021).
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef] [Green Version]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Simes, R.J. Confronting publication bias: A cohort design for meta-analysis. Stat. Med. 1987, 6, 11–29. [Google Scholar] [CrossRef] [PubMed]
- Tierney, J.F.; Stewart, L.A.; Ghersi, D.; Burdett, S.; Sydes, M.R. Practical methods for incorporating summary time-to-event data into meta-analysis. Trials 2007, 8, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kolev, V.; Mironov, S.; Mironov, O.; Ishill, N.; Moskowitz, C.S.; Gardner, G.J.; Levine, D.A.; Hricak, H.; Barakat, R.R.; Chi, D.S. Prognostic Significance of Supradiaphragmatic Lymphadenopathy Identified on Preoperative Computed Tomography Scan in Patients Undergoing Primary Cytoreduction for Advanced Epithelial Ovarian Cancer. Int. J. Gynecol. Cancer 2010, 20, 979–984. [Google Scholar] [CrossRef]
- Kim, T.-H.; Lim, M.C.; Kim, S.I.; Seo, S.-S.; Kim, S.H.; Park, S.-Y. Preoperative Prediction of Cardiophrenic Lymph Node Metastasis in Advanced Ovarian Cancer Using Computed Tomography. Ann. Surg. Oncol. 2015, 23, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Cowan, R.A.; Tseng, J.; Murthy, V.; Srivastava, R.; Roche, K.C.L.; Zivanovic, O.; Gardner, G.J.; Chi, D.S.; Park, B.J.; Sonoda, Y. Feasibility, safety and clinical outcomes of cardiophrenic lymph node resection in advanced ovarian cancer. Gynecol. Oncol. 2017, 147, 262–266. [Google Scholar] [CrossRef]
- McIntosh, L.J.; O’Neill, A.C.; Bhanusupriya, S.; Matalon, S.A.; Abbeele, A.D.V.D.; Ramaiya, N.H.; Shinagare, A.B. Prognostic significance of supradiaphragmatic lymph nodes at initial presentation in patients with stage III high-grade serous ovarian cancer. Abdom. Radiol. 2017, 64, 9–2520. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.O.; Lee, J.Y.; Kim, H.J.; Nam, E.J.; Kim, S.; Kim, S.W. Prognostic Significance of Supradiaphragmatic Lymph Node Metastasis Detected by 18F-FDG PET/CT in Advanced Epithelial Ovarian Cancer; Springer: Berlin/Heidelberg, Germany, 2018. [Google Scholar]
- Mert, I.; Kumar, A.; Sheedy, S.P.; Weaver, A.L.; McGree, M.E.; Kim, B.; Cliby, W.A. Clinical significance of enlarged cardiophrenic lymph nodes in advanced ovarian cancer: Implications for survival. Gynecol. Oncol. 2018, 148, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Salehi, S.; Mohammar, R.; Suzuki, C.; Joneborg, U.; Hjerpe, E.; Torbrand, C.; Falconer, H. Cardiophrenic lymph node resection in advanced ovarian cancer: Surgical outcomes, pre- and postoperative imaging. Acta Oncol. 2018, 57, 820–824. [Google Scholar] [CrossRef] [Green Version]
- Prader, S.; Vollmar, N.; du Bois, A.; Heitz, F.; Schneider, S.; Ataseven, B.; Bommert, M.; Waltering, K.-U.; Heikaus, S.; Koch, J.A.; et al. Pattern and impact of metastatic cardiophrenic lymph nodes in advanced epithelial ovarian cancer. Gynecol. Oncol. 2019, 152, 76–81. [Google Scholar] [CrossRef]
- Komatsu, H.; Iida, Y.; Osaku, D.; Shimogai, R.; Chikumi, J.; Sato, S.; Oishi, T.; Harada, T. Effects of pretreatment radiological and pathological lymph node statuses on prognosis in patients with ovarian cancer who underwent interval debulking surgery with lymphadenectomy following neoadjuvant chemotherapy. J. Obstet. Gynaecol. Res. 2021, 47, 152–158. [Google Scholar] [CrossRef]
- Luger, A.K.; Steinkohl, F.; Aigner, F.; Jaschke, W.; Marth, C.; Zeimet, A.G.; Reimer, D. Enlarged cardiophrenic lymph nodes predict disease involvement of the upper abdomen and the outcome of primary surgical debulking in advanced ovarian cancer. Acta Obstet. Gynecol. Scand. 2020, 99, 1092–1099. [Google Scholar] [CrossRef] [Green Version]
- Oommen, I.; Chandramohan, A.; Raji, P.S.; Thomas, A.; Joel, A.; Ram, T.S.; Peedicayil, A. Clinical significance of CT detected enlarged cardiophrenic nodes in ovarian cancer patients. Abdom. Radiol. 2021, 46, 331–340. [Google Scholar] [CrossRef] [PubMed]
- Raban, O.; Peled, Y.; Krissi, H.; Goldberg, N.; Aviram, A.; Sabah, G.; Levavi, H.; Eitan, R. The significance of paracardiac lymph-node enlargement in patients with newly diagnosed stage IIIC ovarian cancer. Gynecol. Oncol. 2015, 138, 259–262. [Google Scholar] [CrossRef]
- Nuruzzaman, H.S.M.; Tan, G.H.C.; Nadarajah, R.; Teo, M. Relevance of enlarged cardiophrenic lymph nodes in determining prognosis of patients with advanced ovarian cancer. BMJ Case Rep. 2018, 2018. [Google Scholar] [CrossRef]
- Pinelli, C.; Morotti, M.; Casarin, J.; Tozzi, R.; Alazzam, M.; Mavroeidis, V.K.; Majd, H.S. The Feasibility of Cardiophrenic Lymphnode Assessment and Removal in Patients Requiring Diaphragmatic Resection during Interval Debulking Surgery for Ovarian Cancer. J. Investig. Surg. 2021, 34, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Ataseven, B.; Chiva, L.M.; Harter, P.; Gonzalez-Martin, A.; du Bois, A. FIGO stage IV epithelial ovarian, fallopian tube and peritoneal cancer revisited. Gynecol. Oncol. 2016, 142, 597–607. [Google Scholar] [CrossRef] [PubMed]
- Ataseven, B.; Grimm, C.; Harter, P.; Heitz, F.; Traut, A.; Prader, S.; du Bois, A. Prognostic impact of debulking surgery and residual tumor in patients with epithelial ovarian cancer FIGO stage IV. Gynecol. Oncol. 2016, 140, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Delga, B.; Classe, J.-M.; Houvenaeghel, G.; Blache, G.; Sabiani, L.; El Hajj, H.; Andrieux, N.; Lambaudie, E. 30 Years of Experience in the Management of Stage III and IV Epithelial Ovarian Cancer: Impact of Surgical Strategies on Survival. Cancers 2020, 12, 768. [Google Scholar] [CrossRef] [Green Version]
- Dabi, Y.; Huchon, C.; Ouldamer, L.; Bendifallah, S.; Collinet, P.; Bricou, A.; Daraï, E.; Ballester, M.; Lavoue, V.; Haddad, B.; et al. Patients with stage IV epithelial ovarian cancer: Understanding the determinants of survival. J. Transl. Med. 2020, 18, 134. [Google Scholar] [CrossRef] [Green Version]
- Farmakis, S.; Vejdani, K.; Muzaffar, R.; Parkar, N.; Osman, M.M. Detection of Metastatic Disease in Cardiophrenic Lymph Nodes: FDG PET/CT versus Contrast-Enhanced CT and Implications for Staging and Treatment of Disease. Front. Oncol. 2013, 3, 260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, H.J.; Lim, M.C.; Song, Y.J.; Jung, Y.-S.; Kim, S.H.; Yoo, C.W.; Park, S.-Y. Transabdominal cardiophrenic lymph node dissection (CPLND) via incised diaphragm replace conventional video-assisted thoracic surgery for cytoreductive surgery in advanced ovarian cancer. Gynecol. Oncol. 2013, 129, 341–345. [Google Scholar] [CrossRef] [PubMed]
- Diaz, J.; Park, B.; Stine, J.; Flores, R.; Sonoda, Y.; Abu-Rustum, N.; Barakat, R.; Chi, D. The feasibility of mediastinal lymphadenectomy in the management of advanced and recurrent ovarian carcinoma. Gynecol. Oncol. 2011, 120, S80. [Google Scholar] [CrossRef]
- LaFargue, C.; Sawyer, B.; Bristow, R. Short-term morbidity in transdiaphragmatic cardiophrenic lymph node resection for advanced stage gynecologic cancer. Gynecol. Oncol. Rep. 2016, 17, 33–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| Variable | CPLN Adenopathy | Number of Studies Total Study n = 15 | Available Data of Patients n = 727 | No-CPLN Adenopathy | Number of Studies Total Study = 9 | Available Data of Patients n = 981 |
|---|---|---|---|---|---|---|
| General | ||||||
| Mean age, years ± SD | 59.17 ± 11.87 | 10 | 350 | 60 ± 12.64 | 6 | 678 |
| Mean CA125, U/dL ± SD | 1166.36 ± 1259.22 | 8 | 278 | 1140.86 ± 1423.16 | 4 | 190 |
| Anesthesiologists’ score ≥ 3 | 49 (43.36) | 4 | 113 | 166 (43.57) | 2 | 381 |
| FIGO Stage IV * (other than CPLN) | 145 (73.23) | 6 | 198 | 164 (23.26) | 7 | 705 |
| High grade serous carcinoma | 364 (85.85) | 8 | 424 | 657 (81.92) | 7 | 802 |
| Complete abdominal cytoreduction | 248 (59.05) | 7 | 420 | 421 (59.21) | 5 | 711 |
| Optimal abdominal cytoreduction | 169 (50.30) | 7 | 336 | 275 (39.85) | 6 | 690 |
| High surgical complexity ** | 92 (85.98) | 4 | 107 | 250 (65.62) | 7 | 381 |
| Perioperative complication ≥ Clavien-Dindo grade IIIa | 36 (26.08) | 6 | 138 | 86 (22.57) | 2 | 381 |
| Metastatic disease | ||||||
| Ascites | 441 (92.45) | 8 | 477 | 284 (80.45) | 4 | 353 |
| Pleural metastases | 40 (27.97) | 3 | 143 | 21 (11.73) | 2 | 179 |
| Pleural effusion | 104 (25.81) | 5 | 403 | 50 (19.76) | 2 | 253 |
| Upper abdominal metastases | 250 (65.27) | 4 | 383 | 82 (26.28) | 3 | 312 |
| Pelvic adenopathy | 67 (19.14) | 5 | 350 | 36 (12.24) | 3 | 294 |
| Abdominal adenopathy | 106 (27.04) | 6 | 392 | 46 (14.74) | 3 | 312 |
| Carcinomatosis peritonii | 315 (73.94) | 6 | 426 | 179 (60.88) | 3 | 294 |
| Other extra abdominal metastases | 46 (13.06) | 4 | 352 | 20 (11.17) | 2 | 179 |
| Survival outcome | ||||||
| Median OS, months (95%CI) | 42.7 (10.8–74.6) | 6 | 188 | 47.3 (23.2–71.3) | 4 | 258 |
| Median PFS, months (95%CI) | 14.6 (4.9–24.4) | 8 | 327 | 27.8 (3.2–52.4) | 7 | 549 |
| Variable | Value | Number of Studies Total = 9 | Number of Patients Total = 2.09 |
|---|---|---|---|
| General | |||
| Mean size of CPLN *, mm ± SD | 9.16 ± 3.75 | 9 | 471 |
| Location *, total 152 | |||
| Right | 73 (48.03) | 4 | 152 |
| Left | 21 (13.82) | ||
| Bilateral | 20 (13.16) | ||
| Midline | 22 (14.47) | ||
| Missing | 16 (10.53) | ||
| Surgical techniques, total = 100 | |||
| Video-assisted thoracic surgery | 6 (6) | 5 | 100 |
| Transdiaphragmatic approach | 90 (90) | ||
| Substernal approach | 4 (4) | ||
| Pathologic CPLN node | 160 (82.47) | 7 | 194 |
| Perioperative complication ≥ Clavien-Dindo grade IIIa | 30 (30.30) | 4 | 99 |
| Survival outcome | |||
| Median OS, months (95%CI) | 54.7 (15.2–94.3) | 3 | 93 |
| Median PFS, months (95%CI) | 17.7 (7.9–27.4) | 4 | 145 |
| Variables | Number of Studies | Number of Patients | Odds Ratio with 95% CI | p-Value | I2 Index % | Q-Test p-Value = 0.567 | Egger’s Test p-Value |
|---|---|---|---|---|---|---|---|
| Metastatic disease | |||||||
| Ascites | 4 | 735 | 3.30 (1.90–5.72) | <0.01 | 0 | 0.771 | 0.709 |
| Pleuaral metastases | 2 | 313 | 2.58 (1.37–4.82) | 0.003 | 0 | 0.441 | – |
| Pleural effusion | 2 | 562 | 1.78 (1.17–2.69) | 0.007 | 0 | 0.642 | – |
| Upper abdominal metastases | 3 | 663 | 4.38 (0.36–54.01) | 0.249 | 97 | <0.001 | 0.612 |
| Pelvic adenopathy | 3 | 634 | 1.73 (0.82–3.64) | 0.145 | 59 | 0.089 | 0.320 |
| Abdomimal adenopathy | 3 | 663 | 2.30 (1.53–3.46) | <0.001 | 0 | 0.916 | 0.683 |
| Carcinomatosis peritonii | 3 | 634 | 2.02 (0.38–10.66) | 0.406 | 90 | <0.001 | 0.480 |
| Extra abdominal metastases | 2 | 313 | 3.27 (1.61–6.67) | 0.001 | 0 | 0.975 | – |
| Surgical outcome | |||||||
| Completely abdominally cytoreduction | 4 | 961 | 0.69 (0.17–2.82) | 0.604 | 92 | <0.001 | 0.085 |
| Optimally adbominallly cytoreduction | 5 | 924 | 1.32 (0.55–3.20) | 0.532 | 80 | <0.001 | 0.451 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kengsakul, M.; Nieuwenhuyzen-de Boer, G.M.; Bijleveld, A.H.J.; Udomkarnjananun, S.; Kerr, S.J.; Niehot, C.D.; van Beekhuizen, H.J. Survival in Advanced-Stage Epithelial Ovarian Cancer Patients with Cardiophrenic Lymphadenopathy Who Underwent Cytoreductive Surgery: A Systematic Review and Meta-Analysis. Cancers 2021, 13, 5017. https://doi.org/10.3390/cancers13195017
Kengsakul M, Nieuwenhuyzen-de Boer GM, Bijleveld AHJ, Udomkarnjananun S, Kerr SJ, Niehot CD, van Beekhuizen HJ. Survival in Advanced-Stage Epithelial Ovarian Cancer Patients with Cardiophrenic Lymphadenopathy Who Underwent Cytoreductive Surgery: A Systematic Review and Meta-Analysis. Cancers. 2021; 13(19):5017. https://doi.org/10.3390/cancers13195017
Chicago/Turabian StyleKengsakul, Malika, Gatske M. Nieuwenhuyzen-de Boer, Anna H. J. Bijleveld, Suwasin Udomkarnjananun, Stephen J. Kerr, Christa D. Niehot, and Heleen J. van Beekhuizen. 2021. "Survival in Advanced-Stage Epithelial Ovarian Cancer Patients with Cardiophrenic Lymphadenopathy Who Underwent Cytoreductive Surgery: A Systematic Review and Meta-Analysis" Cancers 13, no. 19: 5017. https://doi.org/10.3390/cancers13195017
APA StyleKengsakul, M., Nieuwenhuyzen-de Boer, G. M., Bijleveld, A. H. J., Udomkarnjananun, S., Kerr, S. J., Niehot, C. D., & van Beekhuizen, H. J. (2021). Survival in Advanced-Stage Epithelial Ovarian Cancer Patients with Cardiophrenic Lymphadenopathy Who Underwent Cytoreductive Surgery: A Systematic Review and Meta-Analysis. Cancers, 13(19), 5017. https://doi.org/10.3390/cancers13195017