
Role of Resin Microsphere Y90 Dosimetry in Predicting Objective Tumor Response, Survival and Treatment Related Toxicity in Surgically Unresectable Colorectal Liver Metastasis: A Retrospective Single Institution Study

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Baseline Demographic Characteristics
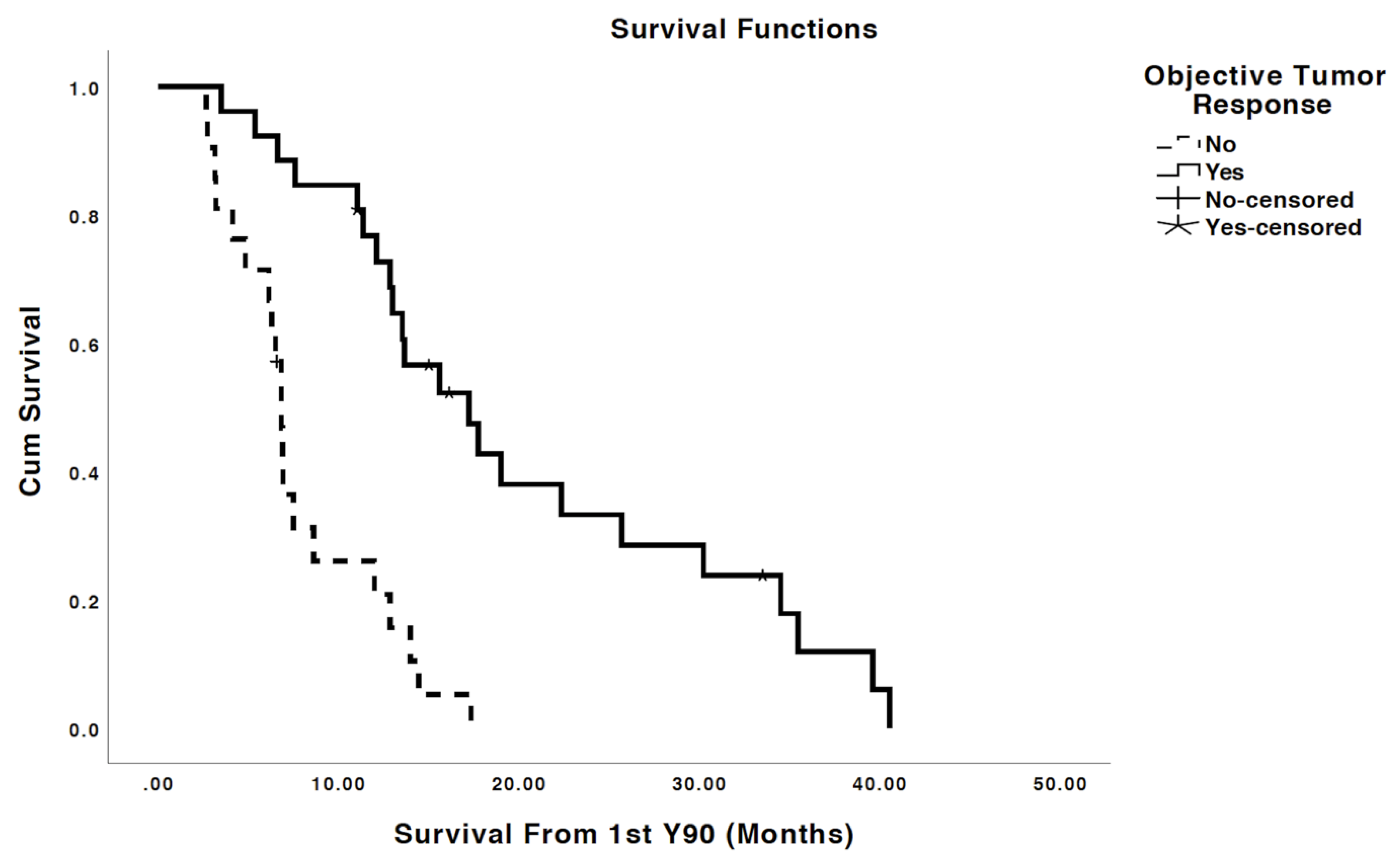
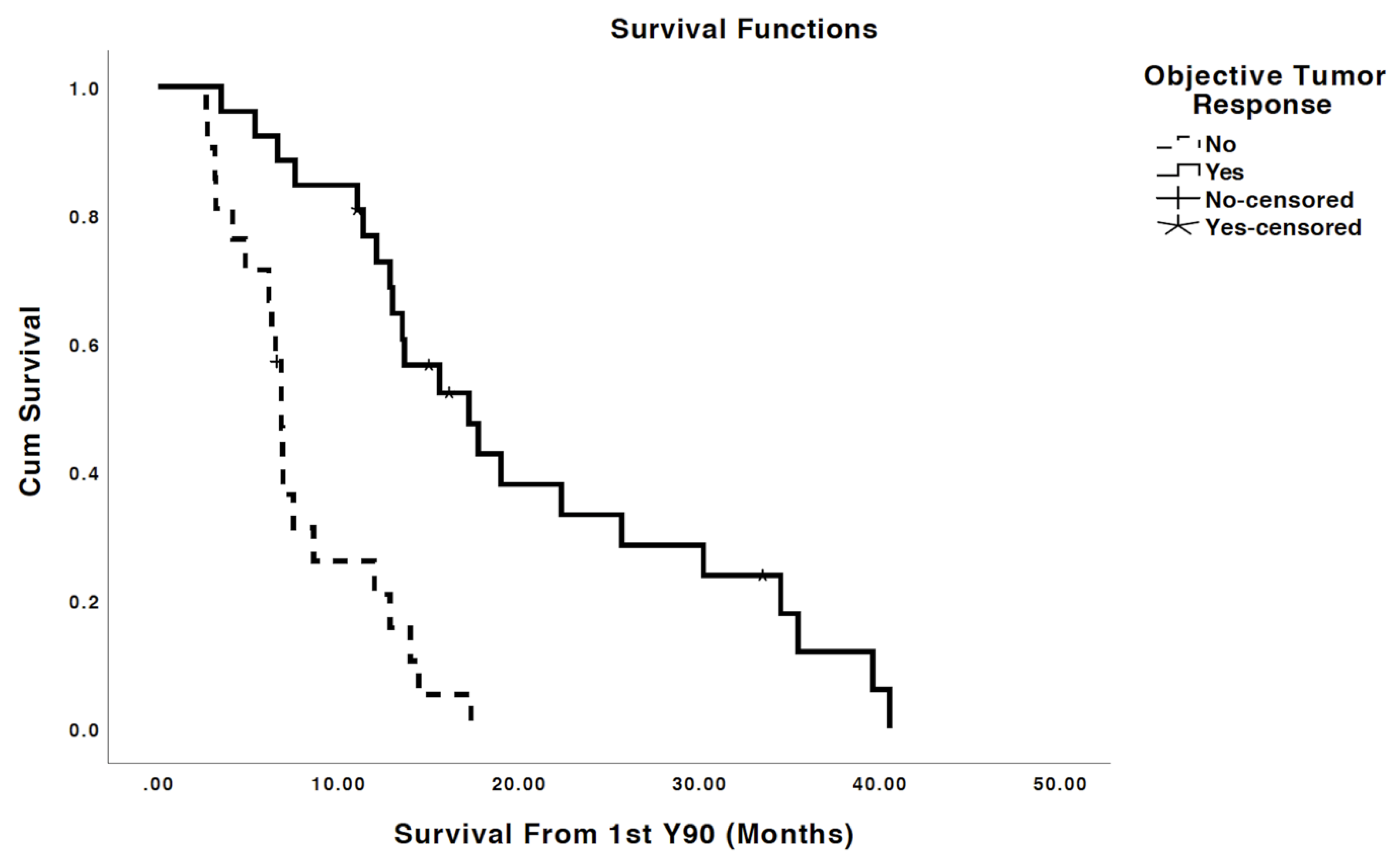
2.2. Tumor Response and Overall Survival
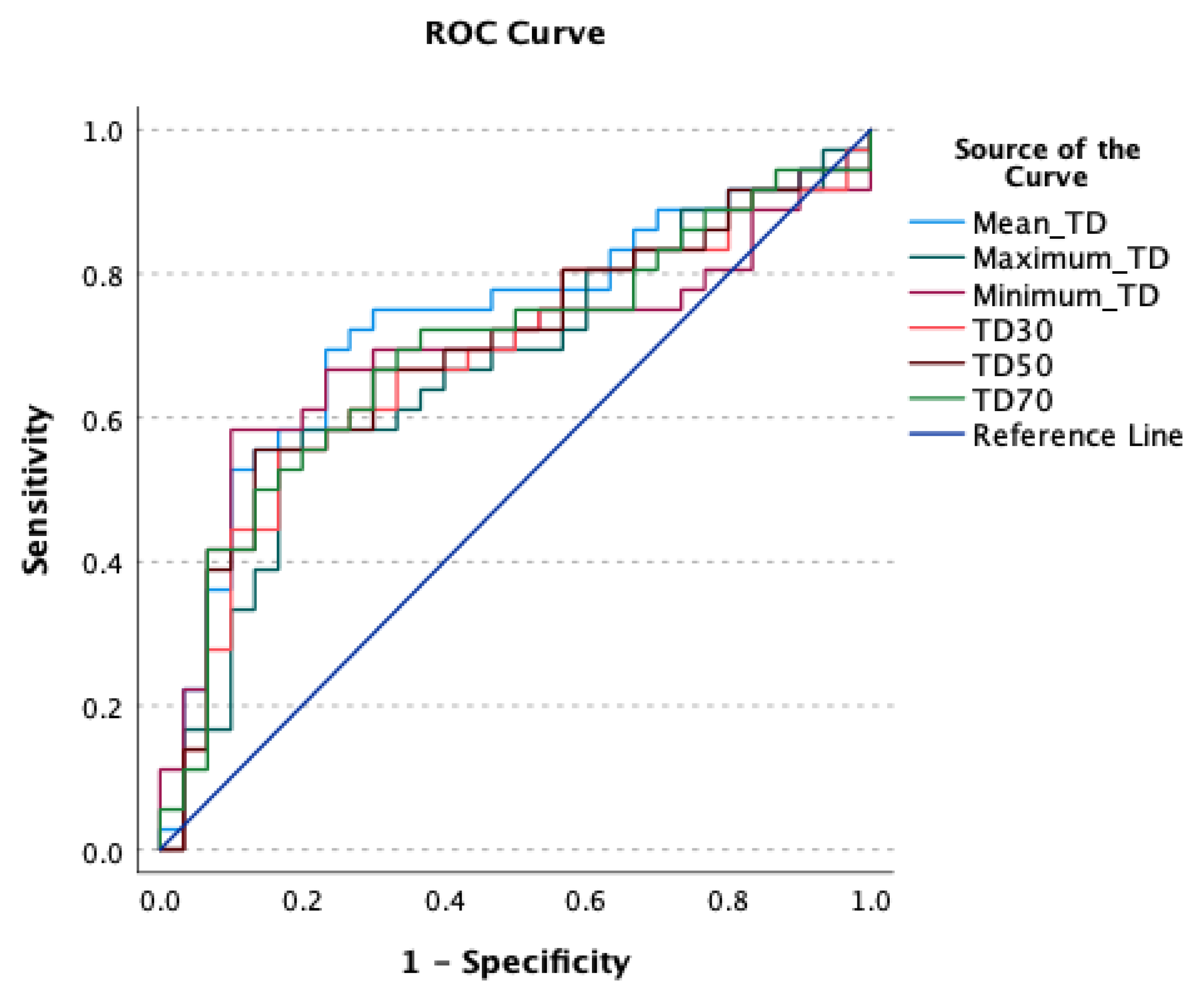
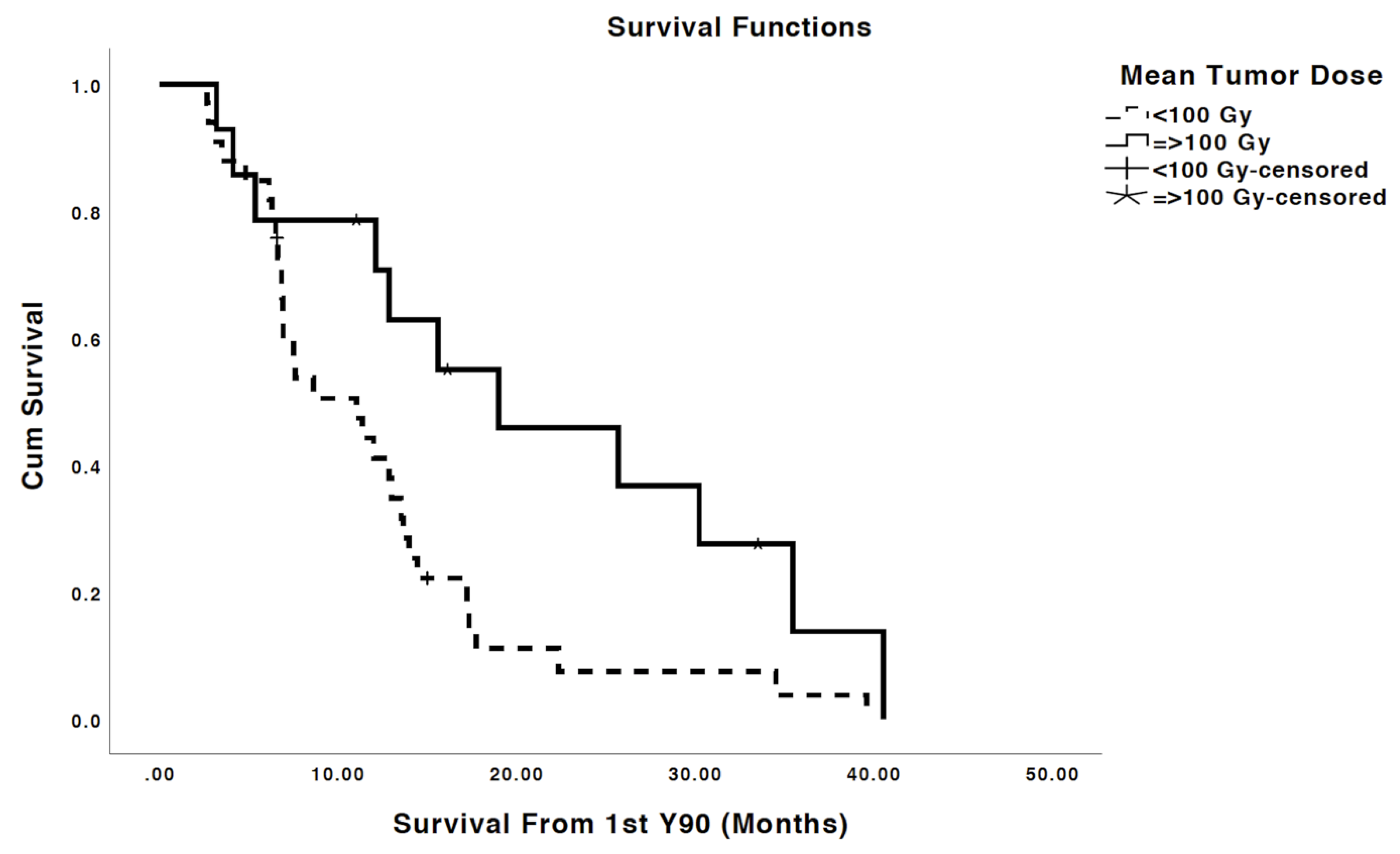
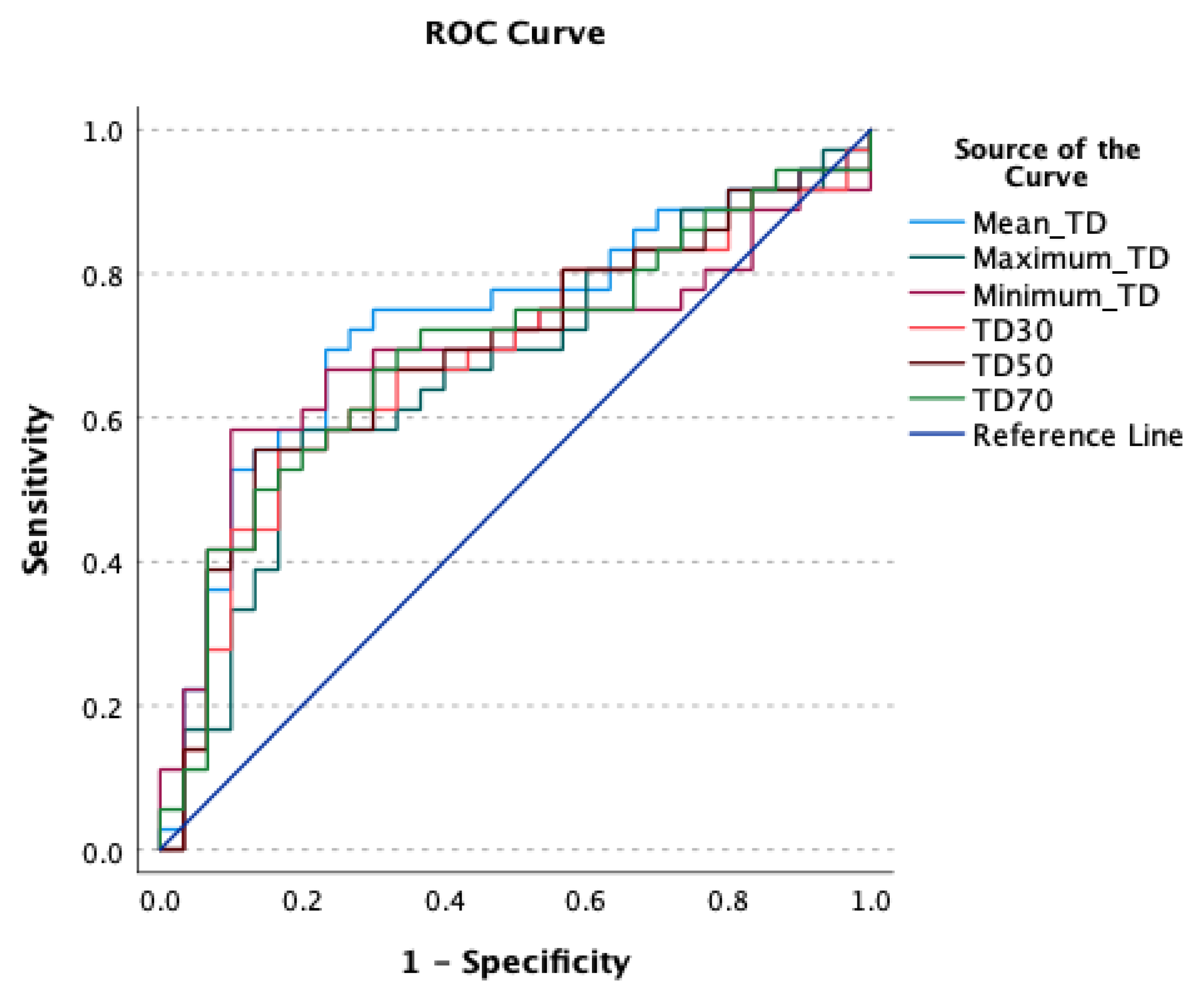
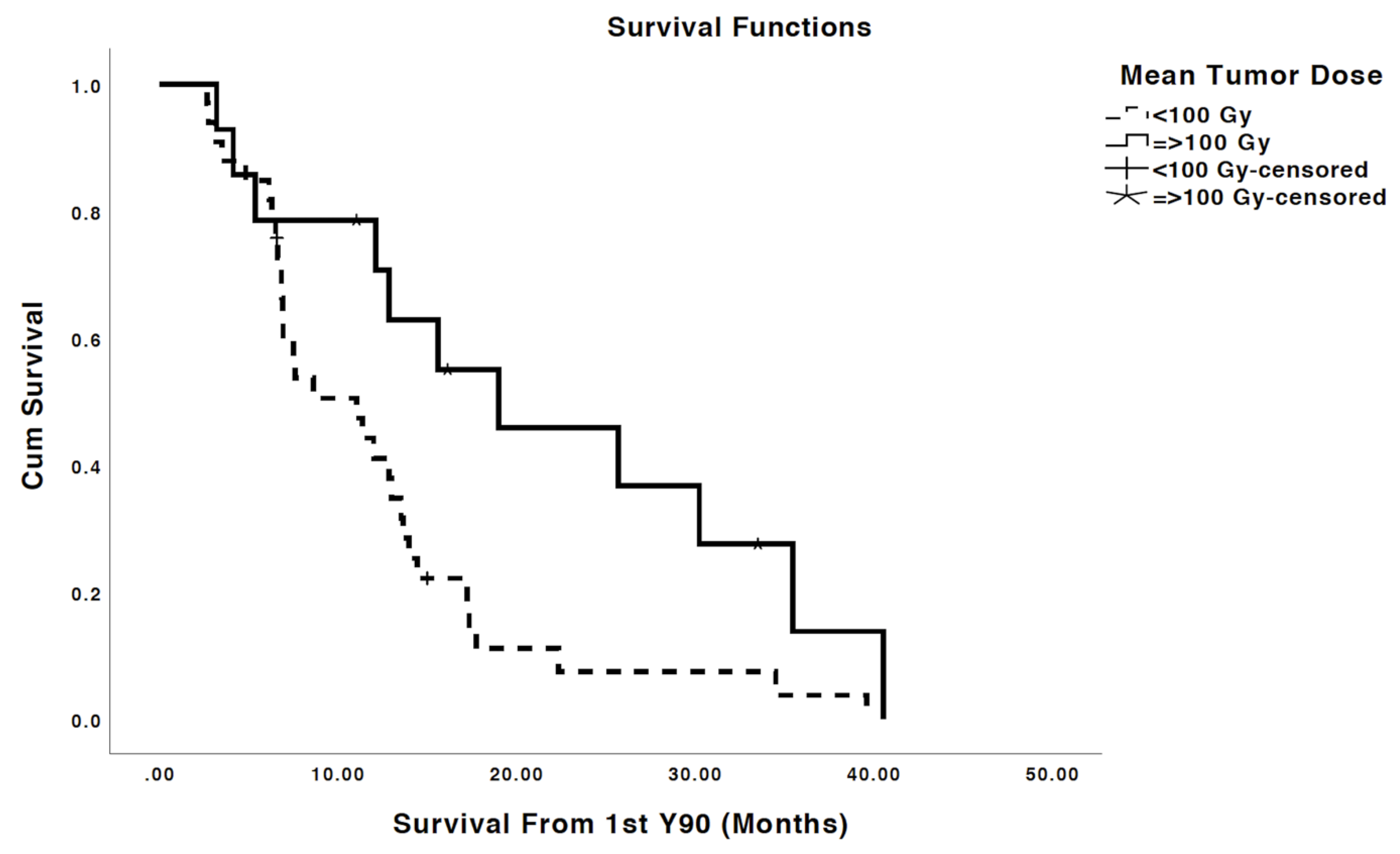
2.3. Tumor Dosimetry, Dose Response Thresholds, Implication on Survival
2.4. Other Predictors of Survival
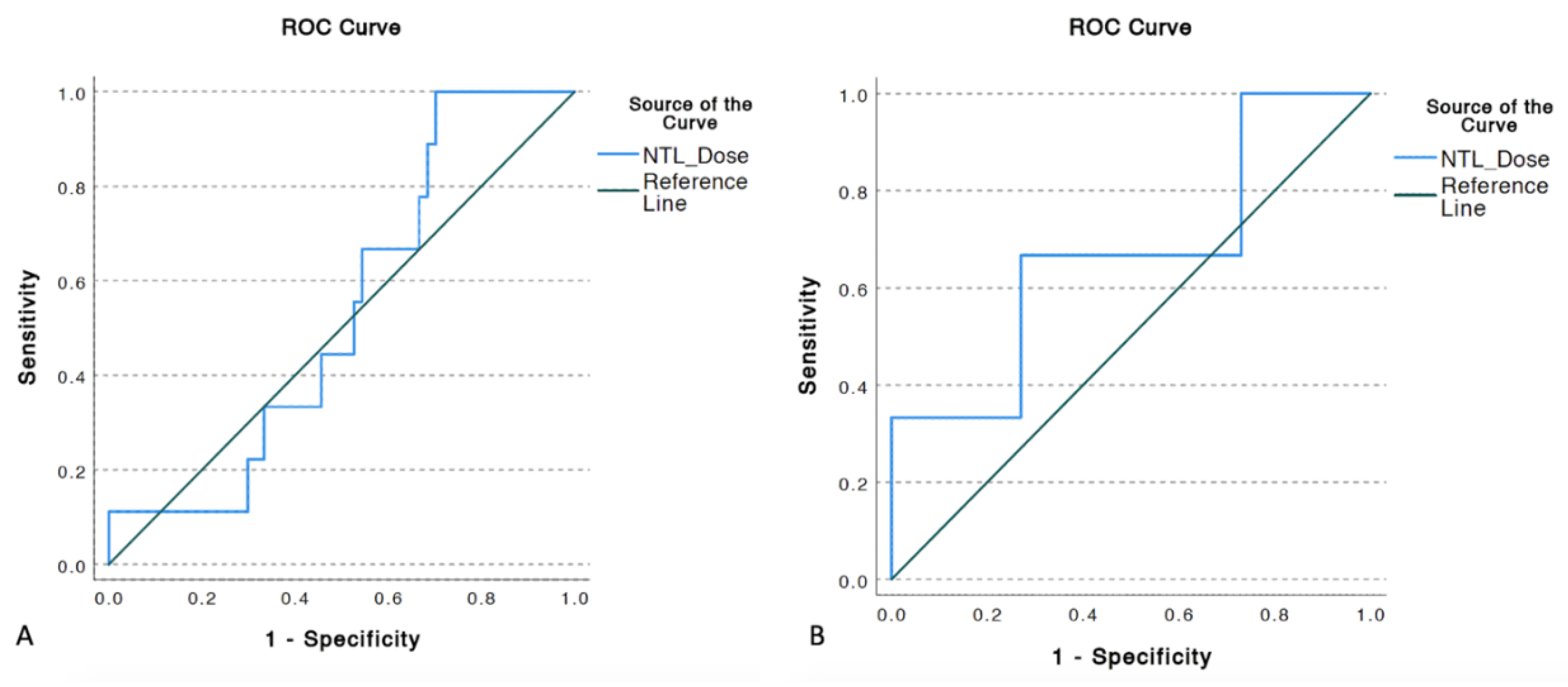
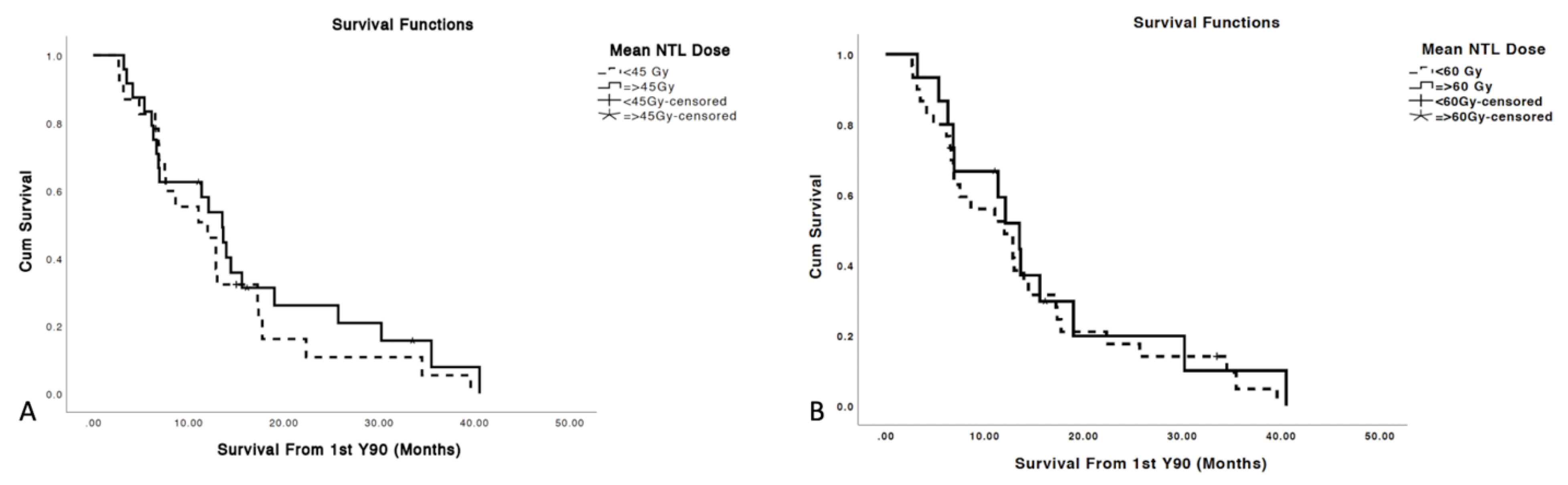
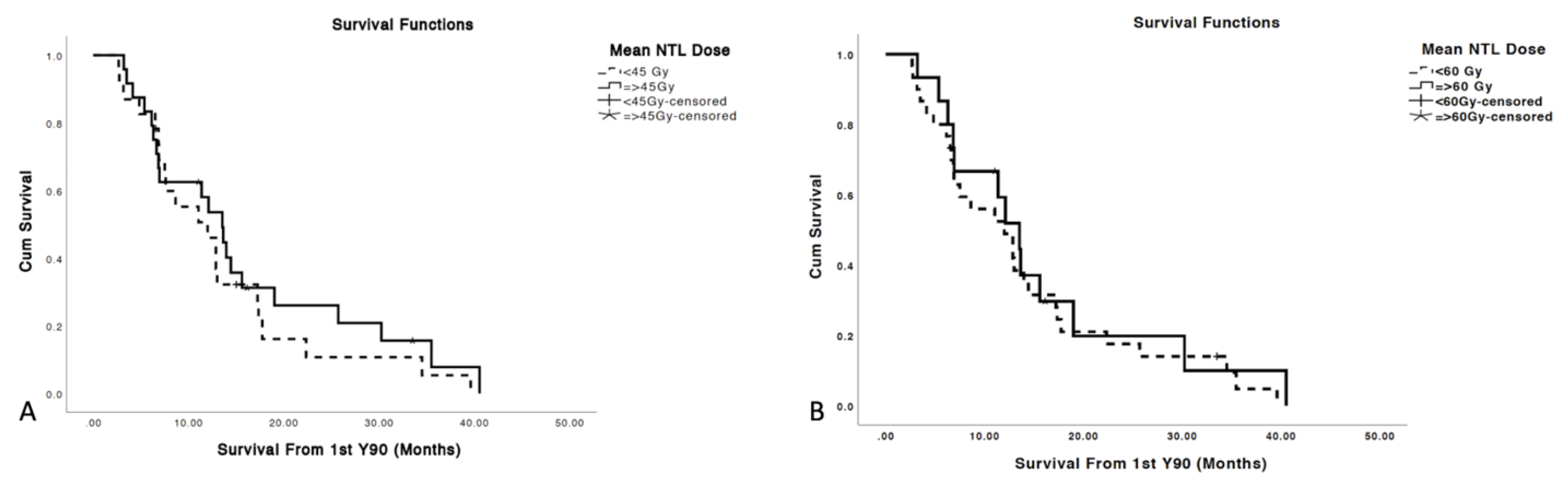
2.5. NTL Dose Implication on Toxicity and Survival
3. Discussion
4. Materials and Methods
4.1. Study Design and Population
4.2. Ytrrium-90 Selective Internal Radiation Therapy (Y90 SIRT) Technique
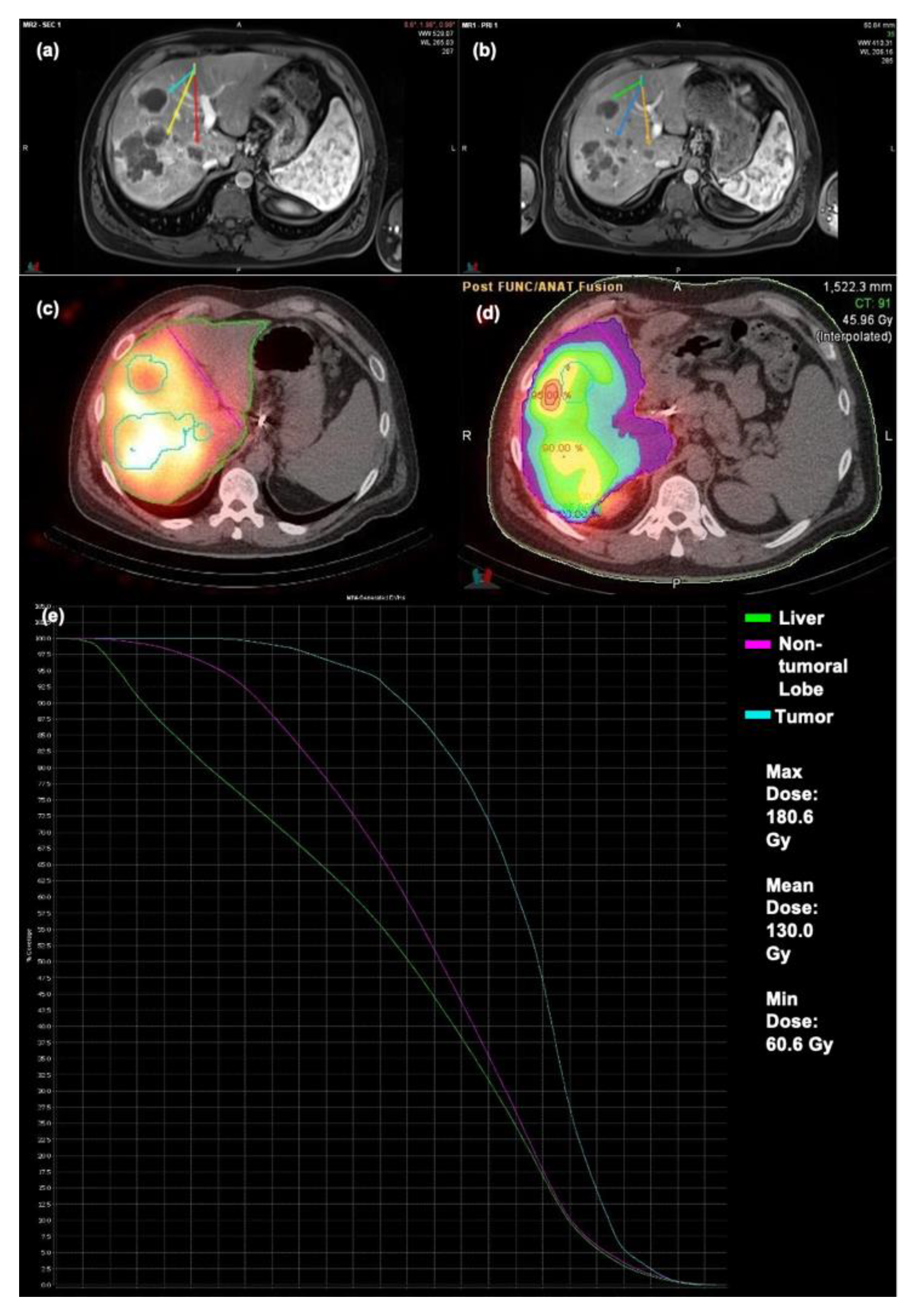
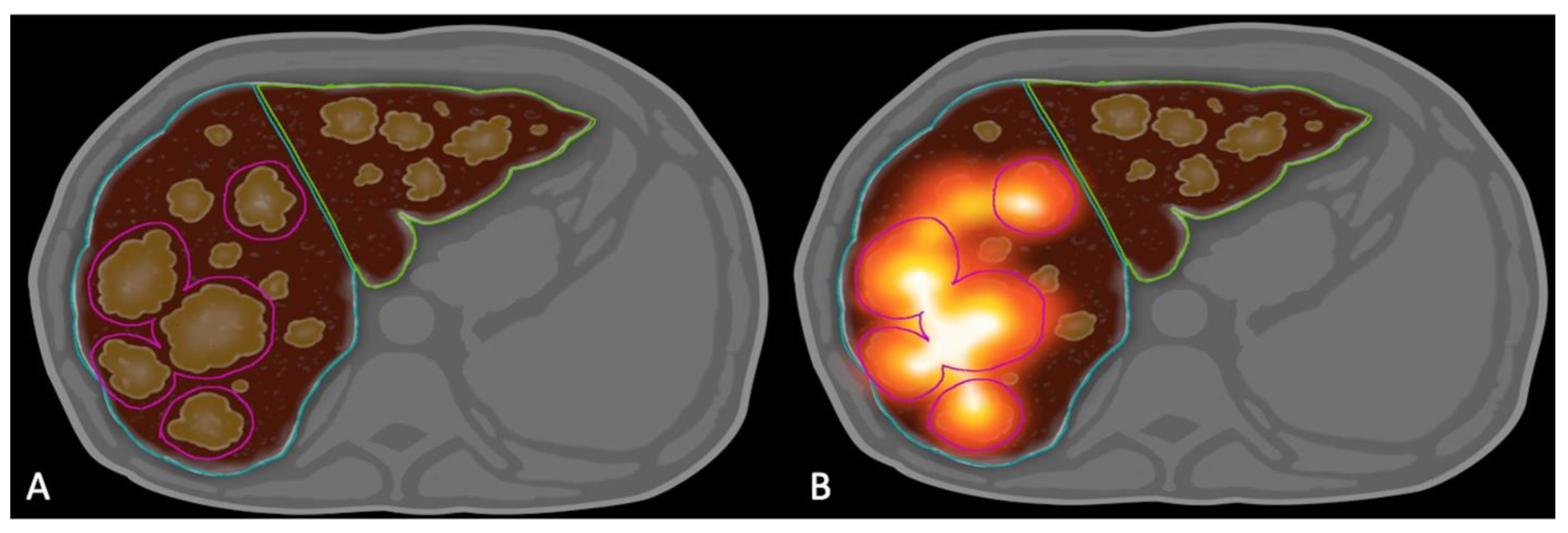
4.3. Dosimetry Analysis
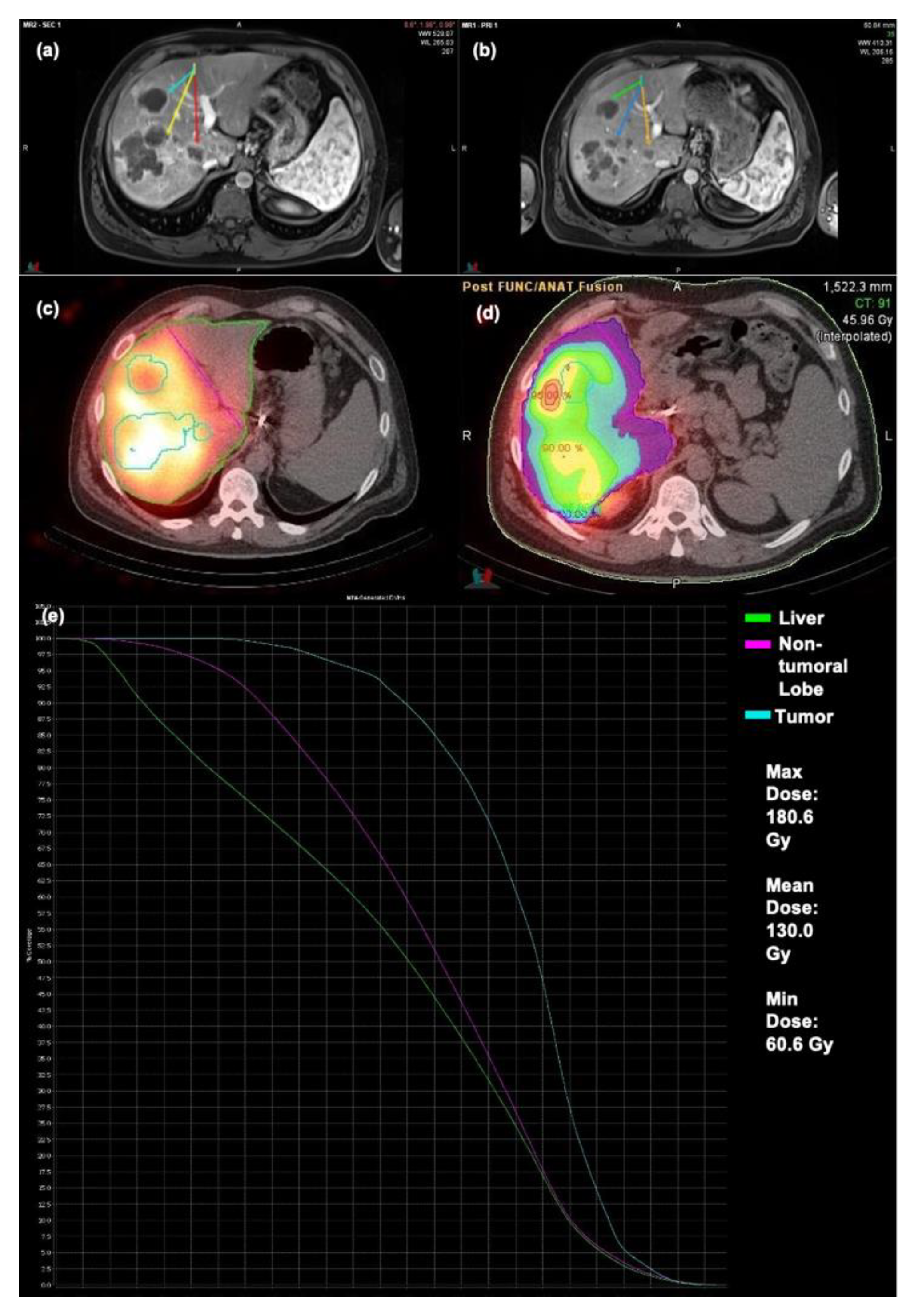
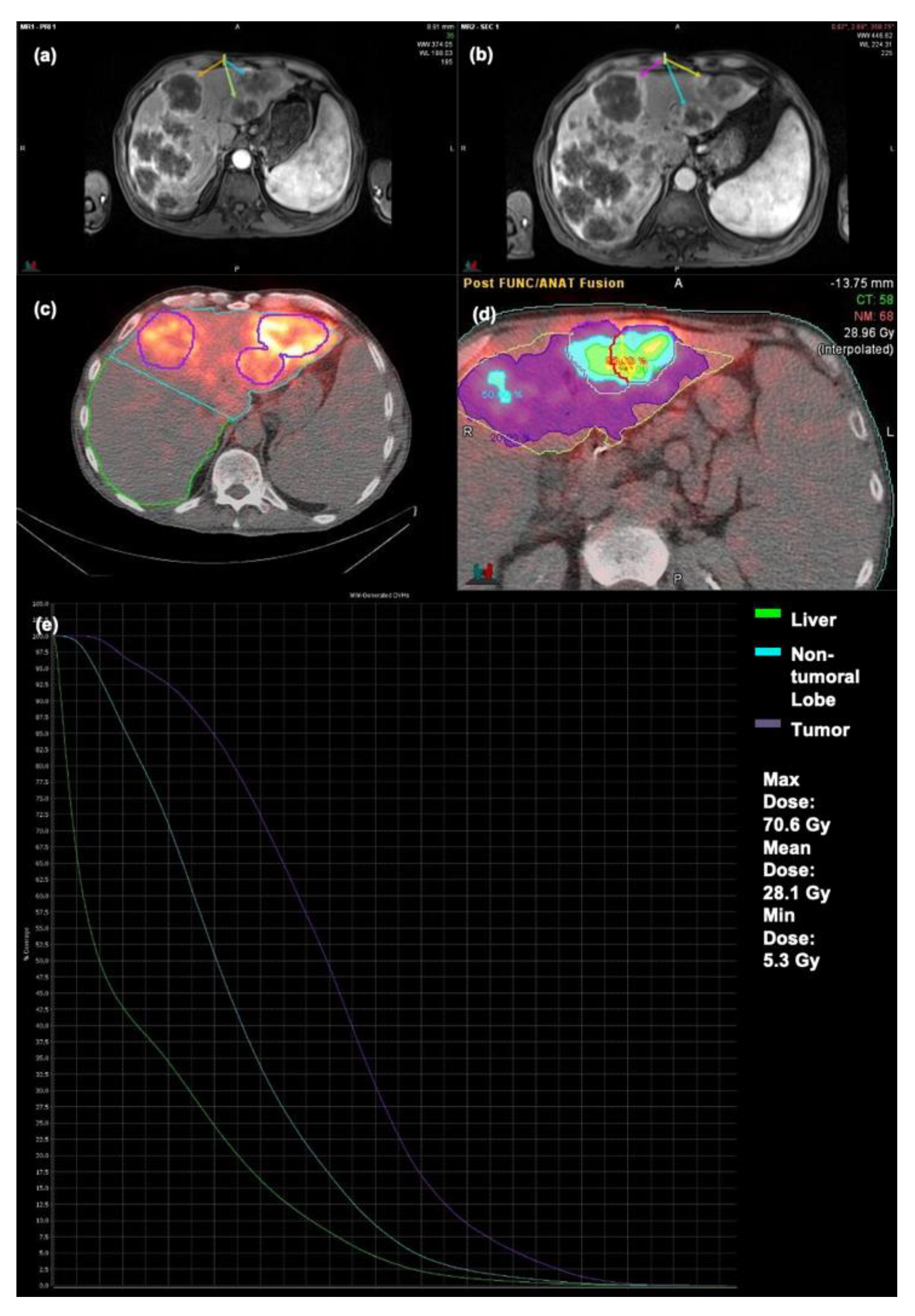
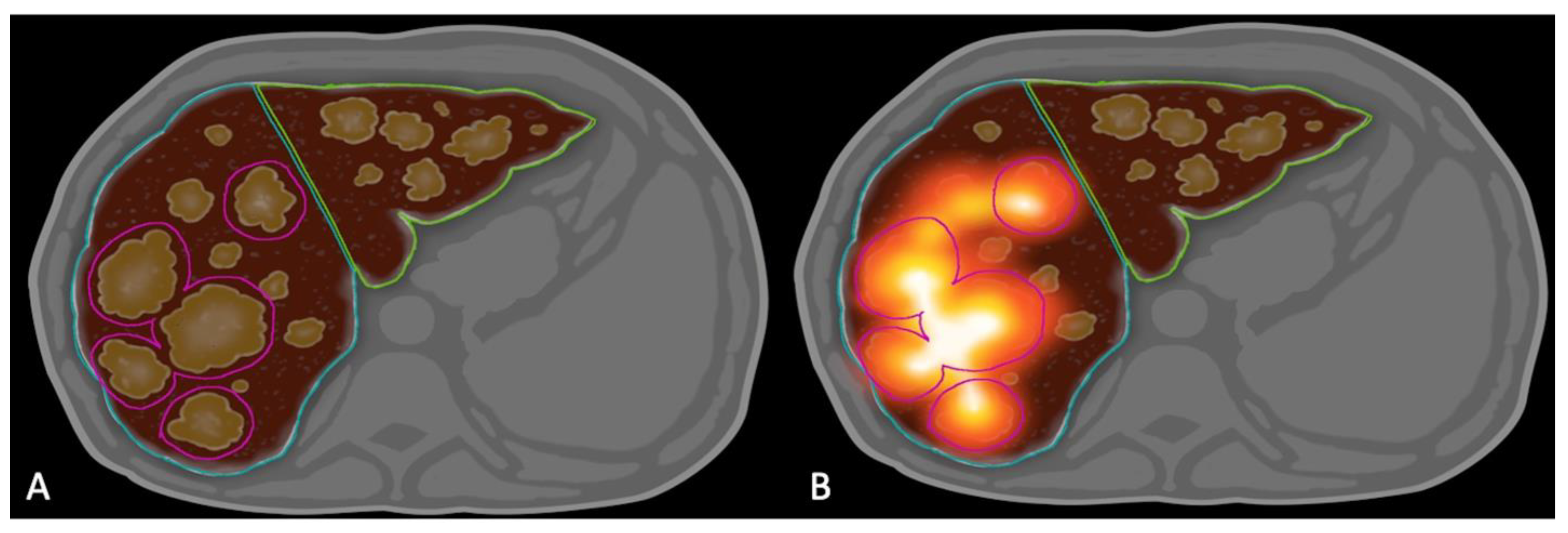
4.4. Image Analysis
4.5. Treatment Related Toxicity
4.6. Variables and Definitions
- Mean TD: Mean dose delivered to all the tumor conglomerate in each lobe in Gray.
- TD 30: Average of dose delivered to at least 30% of the conglomerate tumor volume in Gray.
- TD 50: Dose delivered to at least 50% of the conglomerate tumor volume in Gray.
- TD 70: Dose delivered to at least 70% of the conglomerate tumor volume in Gray.
- TD 99: Dose delivered to at least 99% of the conglomerate tumor volume in Gray; i.e., minimum dose delivered to the tumors.
- Maximum TD: Maximum dose delivered to the conglomerate tumor volume in Gray.
- OR: Objective response by RECIST 1.0 Criteria in the 5 targeted tumors [46].
- Overall survival: Survival from time of first Y90 SIRT.
- Mean NTL Dose: Mean dose delivered to non-tumoral liver lobe in each treatment session.
4.7. Survival and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Sauer, A.G.; Fedewa, S.A.; Butterly, L.F.; Anderson, J.C.; Cercek, A.; Smith, R.A.; Jemal, A. Colorectal cancer statistics. CA A Cancer J. Clin. 2020, 70, 145–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomlinson, J.S.; Jarnagin, W.R.; DeMatteo, R.P.; Fong, Y.; Kornprat, P.; Gonen, M.; Kemeny, N.; Brennan, M.F.; Blumgart, L.H.; D’Angelica, M. Actual 10-year survival after resection of colorectal liver metastases defines cure. J. Clin. Oncol. 2007, 25, 4575–4580. [Google Scholar] [CrossRef] [PubMed]
- Cosimelli, M.; Golfieri, R.; Cagol, P.P.; Carpanese, L.; Sciuto, R.; Maini, C.L.; Mancini, R.; Sperduti, I.; Pizzi, G.; Diodoro, M.G.; et al. Multi-centre phase II clinical trial of yttrium-90 resin microspheres alone in unresectable, chemotherapy refractory colorectal liver metastases. Br. J. Cancer 2010, 103, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Fahmueller, Y.N.; Nagel, D.; Hoffmann, R.T.; Tatsch, K.; Jakobs, T.; Stieber, P.; Holdenrieder, S. Predictive and prognostic value of circulating nucleosomes and serum biomarkers in patients with metastasized colorectal cancer undergoing Selective Internal Radiation Therapy. BMC Cancer 2012, 12, 5. [Google Scholar] [CrossRef] [Green Version]
- Seidensticker, R.; Denecke, T.; Kraus, P.; Seidensticker, M.; Mohnike, K.; Fahlke, J.; Kettner, E.; Hildebrandt, B.; Dudeck, O.; Pech, M.; et al. Matched-pair comparison of radioembolization plus best supportive care versus best supportive care alone for chemotherapy refractory liver-dominant colorectal metastases. Cardiovasc. Intervent. Radiol. 2012, 35, 1066–1073. [Google Scholar] [CrossRef]
- Sofocleous, C.T.; Garcia, A.R.; Taskar, N.P.; Do, K.G.; Brody, L.A.; Petre, E.N.; Capanu, M.; Longing, A.P.; Chou, J.F.; Carrasquillo, J.A.; et al. Phase I trial of selective internal radiation therapy for chemorefractory colorectal cancer liver metastases progressing after hepatic arterial pump and systemic chemotherapy. Clin. Colorectal. Cancer 2014, 13, 27–36. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, A.; Cohn, M.; Coldwell, D.M.; Drooz, A.; Ehrenwald, E.; Kaiser, A.; Nutting, C.W.; Rose, S.C.; Wang, E.A.; Savin, M.A. Updated survival outcomes and analysis of long-term survivors from the MORE study on safety and efficacy of radioembolization in patients with unresectable colorectal cancer liver metastases. J. Gastrointest. Oncol. 2017, 8, 614–624. [Google Scholar] [CrossRef] [Green Version]
- Lewandowski, R.J.; Memon, K.; Mulcahy, M.F.; Hickey, R.; Marshall, K.; Williams, M.; Salzig, K.; Gates, V.L.; Atassi, B.; Vouche, M.; et al. Twelve-year experience of radioembolization for colorectal hepatic metastases in 214 patients: Survival by era and chemotherapy. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 1861–1869. [Google Scholar] [CrossRef]
- Wasan, H.; Gibbs, P.; Sharma, N.; Taieb, J.; Heinemann, V.; Ricke, J.; Peeters, M.; Findlay, M.; Weaver, A.; Mills, J.; et al. First-line selective internal radiotherapy plus chemotherapy versus chemotherapy alone in patients with liver metastases from colorectal cancer (FOXFIRE, SIRFLOX, and FOXFIRE-Global): A combined analysis of three multicentre, randomised, phase 3 trials. Lancet Oncol. 2017, 18, 1159–1171. [Google Scholar] [CrossRef] [Green Version]
- Network NCC. NCCN Clinical Practice Guidelines in Oncology-Colon Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed on 10 July 2021).
- Dabrowiecki, A.; Sankhla, T.; Shinn, K.; Bercu, Z.L.; Ermentrout, M.; Shaib, W.; Cardona, K.; Newsome, J.; Kokabi, N. Impact of Genomic Mutation and Timing of Y90 Radioembolization in Colorectal Liver Metastases. Cardiovasc. Intervent. Radiol. 2020, 43, 1006–1014. [Google Scholar] [CrossRef]
- Chauhan, N.; Mulcahy, M.F.; Salem, R.; Benson, A.; Boucher, E.; Bukovcan, J.; Cosgrove, D.; Laframboise, C.; Lewandowski, R.J.; Master, F. TheraSphere Yttrium-90 Glass Microspheres Combined With Chemotherapy Versus Chemotherapy Alone in Second-Line Treatment of Patients With Metastatic Colorectal Carcinoma of the Liver: Protocol for the EPOCH Phase 3 Randomized Clinical Trial. JMIR Res. Protoc. 2019, 8, e11545. [Google Scholar] [CrossRef]
- Sirtex Medical Ltd. SIR-Spheres® Y-90 Resin Microspheres (Yttrium-90 Microspheres); Sirtex Medical Ltd.: Woburn, MA, USA, 2017. [Google Scholar]
- Garin, E.; Tselikas, L.; Guiu, B.; Chalaye, J.; Edeline, J.; de Baere, T.; Assenat, E.; Tacher, V.; Robert, C.; Mounat, M.T.C.; et al. Personalised versus standard dosimetry approach of selective internal radiation therapy in patients with locally advanced hepatocellular carcinoma (DOSISPHERE-01): A randomised, multicentre, open-label phase 2 trial. Lancet Gastroenterol. Hepatol. 2021, 6, 17–29. [Google Scholar] [CrossRef]
- Elsayed, M.; Ermentrout, R.M.; Sethi, I.; Bercu, Z.L.; Galt, J.R.; Whitmore, M.; Brandon, D.C.; Schuster, D.M.; Kokabi, N. Incidence of Radioembolization-Induced Liver Disease and Liver Toxicity Following Repeat 90Y-Radioembolization: Outcomes at a Large Tertiary Care Center. Clin. Nucl. Med. 2020, 45, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Kokabi, N.; Galt, J.R.; Xing, M.; Camacho, J.C.; Barron, B.J.; Schuster, D.M.; Kim, H.S. A simple method for estimating dose delivered to hepatocellular carcinoma after yttrium-90 glass-based radioembolization therapy: Preliminary results of a proof of concept study. J. Vasc. Interv. Radiol. 2014, 25, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Garin, E.; Rolland, Y.; Laffont, S.; Edeline, J. Clinical impact of (99m)Tc-MAA SPECT/CT-based dosimetry in the radioembolization of liver malignancies with (90)Y-loaded microspheres. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 559–575. [Google Scholar] [CrossRef] [Green Version]
- Demirelli, S.; Erkilic, M.; Oner, A.O.; Budak, E.S.; Gunduz, S.; Ozgur, O.; Bozcuk, H.; Sindel, H.T.; Boz, A. Evaluation of factors affecting tumor response and survival in patients with primary and metastatic liver cancer treated with microspheres. Nucl. Med. Commun. 2015, 36, 340–349. [Google Scholar] [CrossRef]
- Hermann, A.; Dieudonné, A.; Maxime, R.; Manuel, S.; Helena, P.; Gilles, C.; Laurent, C.; Rachida, L.; Vilgrain, V. Role of 99mTc-Macroaggregated Albumin SPECT/CT based dosimetry in predicting survival and tumor response of patients with locally advanced and inoperable hepatocellular carcinoma (HCC) treated by selective intra-arterial radiation therapy (SIRT) with yttrium-90 resin microspheres, a cohort from SARAH study. J. Hepatol. 2018, 68, S13. [Google Scholar]
- Ghosn, M.; Derbel, H.; Kharrat, R.; Oubaya, N.; Mulé, S.; Chalaye, J.; Regnault, H.; Amaddeo, G.; Itti, E.; Luciani, A.; et al. Prediction of overall survival in patients with hepatocellular carcinoma treated with Y-90 radioembolization by imaging response criteria. Diagn. Interv. Imaging 2021, 102, 35–44. [Google Scholar] [CrossRef]
- Kennedy, A.S.; Ball, D.S.; Cohen, S.J.; Cohn, M.; Coldwell, D.M.; Drooz, A.; Ehrenwald, E.; Kanani, S.; Nutting, C.W.; Moeslein, F.M.; et al. Hepatic imaging response to radioembolization with yttrium-90-labeled resin microspheres for tumor progression during systemic chemotherapy in patients with colorectal liver metastases. J. Gastrointest. Oncol. 2015, 6, 594–604. [Google Scholar]
- Dendy, M.S.; Ludwig, J.M.; Kim, H.S. Predictors and prognosticators for survival with Yttrium-90 radioembolization therapy for unresectable colorectal cancer liver metastasis. Oncotarget 2017, 8, 37912–37922. [Google Scholar] [CrossRef] [Green Version]
- Flamen, P.; Vanderlinden, B.; Delatte, P.; Ghanem, G.; Ameye, L.; van den Eynde, M.; Hendlisz, A. Multimodality imaging can predict the metabolic response of unresectable colorectal liver metastases to radioembolization therapy with Yttrium-90 labeled resin microspheres. Phys. Med. Biol. 2008, 53, 6591–6603. [Google Scholar] [CrossRef] [PubMed]
- Levillain, H.; Derijckere, I.D.; Marin, G.; Guiot, T.; Vouche, M.; Reynaert, N.; Hendlisz, A.; Vanderlinden, B.; Flamen, P. (90)Y-PET/CT-based dosimetry after selective internal radiation therapy predicts outcome in patients with liver metastases from colorectal cancer. EJNMMI Res. 2018, 8, 60. [Google Scholar] [CrossRef] [PubMed]
- van den Hoven, A.F.; Rosenbaum, C.E.N.M.; Elias, S.G.; de Jong, H.W.A.M.; Koopman, M.; Verkooijen, H.M.; Alavi, A.; van den Bosch, M.A.A.J.; Lam, M.G.E.H. Insights into the Dose-Response Relationship of Radioembolization with Resin 90Y-Microspheres: A Prospective Cohort Study in Patients with Colorectal Cancer Liver Metastases. J. Nucl. Med. 2016, 57, 1014–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willowson, K.P.; Hayes, A.R.; Chan, D.L.H.; Tapner, M.; Bernard, E.J.; Maher, R.; Pavlakis, N.; Clarke, S.J.; Bailey, D.L. Clinical and imaging-based prognostic factors in radioembolisation of liver metastases from colorectal cancer: A retrospective exploratory analysis. EJNMMI Res. 2017, 7, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsultan, A.A.; van Roekel, C.; Barentsz, M.W.; Smits, M.L.J.; Kunnen, B.; Koopman, M.; Bruijnen, R.C.G.; de Keizer, B.; Lam, M.G.E.H. Dose-response and dose-toxicity relationships for yttrium-90 glass radioembolization in patients with colorectal cancer liver metastases. J. Nucl. Med. 2021, 62. [Google Scholar] [CrossRef]
- Strigari, L.; Sciuto, R.; Rea, S.; Carpanese, L.; Pizzi, G.; Soriani, A.; Iaccarino, G.; Benassi, M.; Ettorre, G.M.; Maini, C.L. Efficacy and toxicity related to treatment of hepatocellular carcinoma with 90Y-SIR spheres: Radiobiologic considerations. J. Nucl. Med. 2010, 51, 1377–1385. [Google Scholar] [CrossRef] [Green Version]
- Hermann, A.L.; Dieudonné, A.; Ronot, M.; Sanchez, M.; Pereira, H.; Chatellier, G.; Garin, E.; Castera, L.; Lebtahi, R.; Vilgrain, V.; et al. Relationship of Tumor Radiation-absorbed Dose to Survival and Response in Hepatocellular Carcinoma Treated with Transarterial Radioembolization with (90)Y in the SARAH Study. Radiology 2020, 296, 673–684. [Google Scholar] [CrossRef]
- Garin, E.; Rolland, Y.; Edeline, J. (90)Y-Loaded Microsphere SIRT of HCC Patients With Portal Vein Thrombosis: High Clinical Impact of 99mTc-MAA SPECT/CT-Based Dosimetry. Semin Nucl. Med. 2019, 49, 218–226. [Google Scholar] [CrossRef]
- Levillain, H.; Bagni, O.; Deroose, C.M.; Dieudonné, A.; Gnesin, S.; Grosser, O.S.; Kappadath, S.C.; Kennedy, A.; Kokabi, N.; Liu, D.M.; et al. International recommendations for personalised selective internal radiation therapy of primary and metastatic liver diseases with yttrium-90 resin microspheres. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1570–1584. [Google Scholar] [CrossRef]
- Fendler, W.P.; Ilhan, H.; Paprottka, P.M.; Jakobs, T.F.; Heinemann, V.; Bartenstein, P.; Khalaf, F.; Ezziddin, S.; Hacker, M.; Haug, A.R. Nomogram including pretherapeutic parameters for prediction of survival after SIRT of hepatic metastases from colorectal cancer. Eur. Radiol. 2015, 25, 2693–2700. [Google Scholar] [CrossRef]
- Kurilova, I.; Tan, R.G.H.B.; Flynn, J.; Gönen, M.; Ulaner, G.; Petre, E.N.; Boas, F.E.; Ziv, E.; Yarmohammadi, H.; Klompenhouwer, E.G.; et al. Factors Affecting Oncologic Outcomes of 90Y Radioembolization of Heavily Pre-Treated Patients With Colon Cancer Liver Metastases. Clin. Colorectal. Cancer 2019, 18, 8–18. [Google Scholar] [CrossRef] [PubMed]
- Damm, R.; Seidensticker, R.; Ulrich, G.; Breier, L.; Steffen, I.G.; Seidensticker, M.; Garlipp, B.; Mohnike, K.; Pech, M.; Amthauer, H.; et al. Y90 Radioembolization in chemo-refractory metastastic, liver dominant colorectal cancer patients: Outcome assessment applying a predictive scoring system. BMC Cancer 2016, 16, 509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sofocleous, C.T.; Violari, E.G.; Sotirchos, V.S.; Shady, W.; Gonen, M.; Taskar, N.P.; Petre, E.N.; Brody, L.A.; Alago, W.; Do, R.K.; et al. Radioembolization as a Salvage Therapy for Heavily Pretreated Patients With Colorectal Cancer Liver Metastases: Factors That Affect Outcomes. Clin. Colorectal. Cancer 2015, 14, 296–305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiner, A.A.; Gui, B.; Newman, N.B.; Nosher, J.L.; Yousseff, F.; Lu, S.E.; Foltz, G.M.; Carpizo, D.; Lowenthal, J.; Zuckerman, D.A.; et al. Predictors of Survival after Yttrium-90 Radioembolization for Colorectal Cancer Liver Metastases. J. Vasc. Interv. Radiol. 2018, 29, 1094–1100. [Google Scholar] [CrossRef] [PubMed]
- Boas, F.E.; Brody, L.A.; Erinjeri, J.P.; Yarmohammadi, H.; Shady, W.; Kishore, S.; Sofocleous, C.T. Quantitative Measurements of Enhancement on Preprocedure Triphasic CT Can Predict Response of Colorectal Liver Metastases to Radioembolization. AJR Am. J. Roentgenol. 2016, 207, 671–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahl, R.L.; Jacene, H.; Kasamon, Y.; Lodge, M.A. From RECIST to PERCIST: Evolving Considerations for PET response criteria in solid tumors. J. Nucl. Med. 2009, 50 (Suppl. 1), 122s–150s. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [Green Version]
- Atass, B.; Bangash, A.K.; Bahrani, A.; Pizzi, G.; Lewandowski, R.J.; Ryu, R.K.; Sato, K.T.; Gates, V.L.; Mulcahy, M.F.; Kulik, L.; et al. Multimodality imaging following 90Y radioembolization: A comprehensive review and pictorial essay. Radiographics 2008, 28, 81–99. [Google Scholar] [CrossRef] [Green Version]
- Shady, W.; Sotirchos, V.S.; Do, R.K.; Taskar, N.P.; Carrasquillo, J.A.; Gonen, M.; Sofocleous, C.T. Surrogate Imaging Biomarkers of Response of Colorectal Liver Metastases After Salvage Radioembolization Using 90Y-Loaded Resin Microspheres. AJR Am. J. Roentgenol. 2016, 207, 661–670. [Google Scholar] [CrossRef] [Green Version]
- Shady, W.; Kishore, S.; Gavane, S.; Do, R.K.; Osborne, J.R.; Ulaner, G.A.; Gonen, M.; Ziv, E.; Boas, F.E.; Sofocleous, C.T. Metabolic tumor volume and total lesion glycolysis on FDG-PET/CT can predict overall survival after (90)Y radioembolization of colorectal liver metastases: A comparison with SUVmax, SUVpeak, and RECIST 1. Eur. J. Radiol. 2016, 85, 1224–1231. [Google Scholar] [CrossRef] [Green Version]
- Fendler, W.P.; Tiega, D.B.P.; Ilhan, H.; Paprottka, P.M.; Heinemann, V.; Jakobs, T.F.; Bartenstein, P.; Hacker, M.; Haug, A.R. Validation of several SUV-based parameters derived from 18F-FDG PET for prediction of survival after SIRT of hepatic metastases from colorectal cancer. J. Nucl. Med. 2013, 54, 1202–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziv, E.; Bergen, M.; Yarmohammadi, H.; Boas, F.E.; Petre, E.N.; Sofocleous, C.T.; Yaeger, R.; Solit, D.B.; Solomon, S.B.; Erinjeri, J.P. PI3K pathway mutations are associated with longer time to local progression after radioembolization of colorectal liver metastases. Oncotarget 2017, 8, 23529–23538. [Google Scholar] [CrossRef]
- Koran, M.E.; Stewart, S.; Baker, J.C.; Lipnik, A.J.; Banovac, F.; Omary, R.A.; Brown, D.B. Five percent dextrose maximizes dose delivery of Yttrium-90 resin microspheres and reduces rates of premature stasis compared to sterile water. Biomed. Rep. 2016, 5, 745–748. [Google Scholar] [CrossRef]
- Therasse, P.; Arbuck, S.G.; Eisenhauer, E.A.; Wanders, J.; Kaplan, R.S.; Rubinstein, L.; Verweij, J.; van Glabbeke, M.; van Oosterom, A.T.; Christian, M.C.; et al. New guidelines to evaluate the response to treatment in solid tumors. European Organization for Research and Treatment of Cancer, National Cancer Institute of the United States, National Cancer Institute of Canada. J. Natl. Cancer Inst. 2000, 92, 205–216. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) Version 5; U.S. Department of Health and Human Services: Washington, DC, USA, 2017.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Groups | Number | |
|---|---|---|---|
| Age | ≥65 | 26 | 58% |
| <65 | 19 | 42% | |
| Gender | Male | 29 | 64% |
| Female | 16 | 36% | |
| ECOG | 0 | 27 | 60% |
| 1 | 13 | 29% | |
| ≥2 | 4 | 9% | |
| Unknown | 1 | 2% | |
| Pre-Op Lab Values | International Normalized Ratio | 1.08 | Range: 0.91–1.8 |
| Aspartate Aminotransferase | 35.5 IU/L | Range: 21–78 | |
| Alanine Aminotransferase | 27.0 IU/L | Range: 17–59 | |
| Total Bilirubin | 0.68 mg/dL | Range: 0.41–1.81 | |
| Creatinine | 0.85 mg/dL | Range: 0.51–1.72 | |
| Albumin | 3.6 g/dL | Range: 2.9–4.8 | |
| Sodium | 137 mmol/L | Range: 131–148 | |
| Multifocal Disease | Yes | 45 | 100% |
| No | 0 | 0% | |
| Any Genomic Mutation | Yes | 25 | 56% |
| No | 20 | 44% | |
| MAPK Pathway Mutation | Yes | 21 | 47% |
| No | 24 | 53% | |
| Baseline Ascites | Yes | 4 | 9% |
| No | 41 | 91% | |
| Baseline CEA Level | >20 ng/mL | 28 | 62% |
| ≤20 ng/mL | 17 | 38% | |
| CEA Decrease post Y90 SIRT | Yes | 23 | 51% |
| No | 22 | 49% | |
| Diffuse Disease (>10 Intrahepatic Tumors/hepatic lobe) | Yes | 32 | 71% |
| No | 13 | 29% | |
| Extra Hepatic Metastatic Disease | Yes | 25 | 56% |
| No | 20 | 44% | |
| Index Tumor Size | Mean | 3.2 cm | |
| Range | 1.8–8.7 cm | ||
| Index Tumor | ≥5 cm | 14 | 31% |
| <5 cm | 31 | 69% | |
| Bilobar Intrahepatic Tumors | Yes | 28 | 62% |
| No | 17 | 38% |
| Mean TD | Mean | 68.7 Gy |
| Range | 18.1–744.5 Gy | |
| Maximum TD | Mean | 94.1 Gy |
| Range | 34.7–866.1 Gy | |
| TD 30% | Mean | 70.31 Gy |
| Range | 22.5–421.3 Gy | |
| TD 50% | Mean | 63.17 Gy |
| Range | 11.0–325.9 Gy | |
| TD 70% | Mean | 57.6 Gy |
| Range | 7.0–290.8 Gy | |
| TD 99% (Minimum TD) | Mean | 35.3 Gy |
| Range | 3.1–232.1 Gy |
| Variables | Median OS (Months) | p Value | |
|---|---|---|---|
| Any Mutation | No | 15.4 | 0.020 |
| Yes | 9.1 | ||
| MAPK | No | 16.3 | 0.001 |
| Yes | 8.4 | ||
| Age | ≤65 | 14.2 | 0.201 |
| >65 | 12.1 | ||
| Sex | Male | 11.6 | 0.212 |
| Female | 13.8 | ||
| ECOG | 0 | 15.1 | 0.077 |
| ≥1 | 10.3 | ||
| Baseline Ascites | Yes | 12.0 | 0.311 |
| No | 13.5 | ||
| Baseline CEA level | >20 ng/mL | 11.9 | 0.975 |
| ≤20 ng/mL | 12.7 | ||
| CEA decrease post Y90 RE | Yes | 15.3 | 0.075 |
| No | 11.1 | ||
| Bilobar Hepatic Metastases | Yes | 10.2 | 0.029 |
| No | 16.9 | ||
| Index lesion | ≥5 cm | 12.5 | 0.254 |
| <5 cm | 12.8 | ||
| Diffuse Hepatic Metastases | Yes | 9.2 | <0.001 |
| No | 18.1 | ||
| Extra-hepatic Metastases | Yes | 11.9 | 0.961 |
| No | 12.7 |
| Factor | Relative Risk (RR) | p-Value | Standard Error |
|---|---|---|---|
| MAPK Mutation | 1.137 | 0.502 | 0.559 |
| Any Mutation | 3.297 | 0.027 | 0.479 |
| Mean TD ≥ 100 Gy | 0.245 | <0.001 | 0.443 |
| Bilobar Disease | 1.213 | 0.623 | 0.414 |
| Diffuse Disease | 3.219 | 0.012 | 0.421 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sankhla, T.; Cheng, B.; Nezami, N.; Xing, M.; Sethi, I.; Bercu, Z.; Brandon, D.; Majdalany, B.; Schuster, D.M.; Kokabi, N. Role of Resin Microsphere Y90 Dosimetry in Predicting Objective Tumor Response, Survival and Treatment Related Toxicity in Surgically Unresectable Colorectal Liver Metastasis: A Retrospective Single Institution Study. Cancers 2021, 13, 4908. https://doi.org/10.3390/cancers13194908
Sankhla T, Cheng B, Nezami N, Xing M, Sethi I, Bercu Z, Brandon D, Majdalany B, Schuster DM, Kokabi N. Role of Resin Microsphere Y90 Dosimetry in Predicting Objective Tumor Response, Survival and Treatment Related Toxicity in Surgically Unresectable Colorectal Liver Metastasis: A Retrospective Single Institution Study. Cancers. 2021; 13(19):4908. https://doi.org/10.3390/cancers13194908
Chicago/Turabian StyleSankhla, Tina, Bernard Cheng, Nariman Nezami, Minzhi Xing, Ila Sethi, Zachary Bercu, David Brandon, Bill Majdalany, David M. Schuster, and Nima Kokabi. 2021. "Role of Resin Microsphere Y90 Dosimetry in Predicting Objective Tumor Response, Survival and Treatment Related Toxicity in Surgically Unresectable Colorectal Liver Metastasis: A Retrospective Single Institution Study" Cancers 13, no. 19: 4908. https://doi.org/10.3390/cancers13194908
APA StyleSankhla, T., Cheng, B., Nezami, N., Xing, M., Sethi, I., Bercu, Z., Brandon, D., Majdalany, B., Schuster, D. M., & Kokabi, N. (2021). Role of Resin Microsphere Y90 Dosimetry in Predicting Objective Tumor Response, Survival and Treatment Related Toxicity in Surgically Unresectable Colorectal Liver Metastasis: A Retrospective Single Institution Study. Cancers, 13(19), 4908. https://doi.org/10.3390/cancers13194908