Simple Summary
Since the 1940s, radioactive iodine has been used for functional imaging and for treating patients with differentiated thyroid cancer (DTC). During this long-lasting experience, the use of iodine isotopes evolved, especially during the last years due to improved knowledge of thyroid cancer biology and improved performances of imaging tools. The present review summarizes recent advances in the field of functional imaging and theragnostic approach of DTC.
Abstract
The present review provides a description of recent advances in the field of functional imaging that takes advantage of the functional characteristics of thyroid neoplastic cells (such as radioiodine uptake and FDG uptake) and theragnostic approach of differentiated thyroid cancer (DTC). Physical and biological characteristics of available radiopharmaceuticals and their use with state-of-the-art technologies for diagnosis, treatment, and follow-up of DTC patients are depicted. Radioactive iodine is used mostly with a therapeutic intent, while PET/CT with 18F-FDG emerges as a useful tool in the diagnostic management and complements the use of radioactive iodine. Beyond 18F-FDG PET/CT, other tracers including 124I, 18F-TFB and 68Ga-PSMA, and new methods such as PET/MR, might offer new opportunities in selecting patients with DTC for specific imaging modalities or treatments.
1. Introduction
Radioactive iodine (RAI) has been used since the 1940s as a specific radiopharmaceutical agent for functional imaging and for treating patients with differentiated thyroid cancer (DTC) [1,2,3,4,5,6]. During this long-lasting experience, the use of RAI (123I/131I) for imaging [7] and for therapy evolved, especially during the last years. This is related to the improved knowledge of the biology and natural history of thyroid cancer. In fact, a standard initial treatment was advocated for all DTC > 1.5 cm in diameter, consisting of a total thyroidectomy, followed by a post-operative administration of a high activity of 131I (>3700 MBq) and then by a thyroid hormone treatment that suppressed the serum TSH [8]. Currently, this has changed toward a more selective approach based on prognostic indicators and on the presence or absence of evidence of persistent disease [4,9].
Theragnostic is a treatment strategy that combines therapeutics with diagnostics. It associates a diagnostic test that identifies patients most likely to be helped or harmed by a targeted therapy and the use of this therapy based on the test results. In metastatic DTC patients, the RAI diagnostic whole-body scan (WBS) will search for foci of uptake to be treated and will quantify uptake for dosimetry and the post-therapy WBS will control that these foci have been treated and may also quantify the radiation dose to each neoplastic focus [10]. This appealing strategy that is followed by many nuclear medicine experts needs to be validated by prospective trials in terms of clinical benefits for the patients.
Another area of remarkable progress is the improvement in performances of scintigraphy devices with hybrid imaging implementation both for single photon emission tomography (SPECT) and positron emission tomography (PET) techniques [11]. The integration of SPECT with computed tomography (CT) in SPECT/CT tools improved the quality and accuracy of 131I imaging and allows a quantitation of any uptake and potentially a lesion dosimetry evaluation before and after RAI treatment. PET/CT has become an integral part of DTC management using the non-specific 18F-fluorodeoxyglucose (18F-FDG) tracer both for diagnostic and prognostic purposes and, where available, using 124I that is a highly performing radiopharmaceutical to evaluate in vivo iodine avid lesions [12,13]. Unfortunately, most evidence concerning the use of these tracers relies on retrospective data or on expert opinion or consensus statements. Only few prospective studies that provide unbiased data are available and are detailed in the present review that summarizes recent advances in the field of functional imaging and theragnostic approach of DTC.
2. Natural History of Differentiated Thyroid Cancer
There are four histological types of differentiated thyroid cancer: papillary the most frequent, follicular, oncocytic (or Hürthle) and poorly differentiated [14,15]. The TNM classification evaluates the risk of thyroid cancer death [16], and the American Thyroid Association (ATA) risk stratification evaluates the risk of structural recurrence [4]. Most thyroid cancers (>80%) are at low risk of death and of recurrence and only require limited treatment and limited follow-up modalities.
Papillary thyroid cancer spreads to neck lymph nodes and then to lungs; lung metastases are usually multiple, diffuse and frequently with a miliary aspect. Follicular and oncocytic cancers spread to lungs and bones, but lymph node involvement is less frequent than in papillary thyroid cancer. The other organs (brain and liver) are less frequently involved. Currently, distant metastases are observed in less than 5% of all thyroid cancer patients and are mostly observed in high-risk patients [17,18].
Differentiated thyroid cancer produces thyroglobulin (Tg) that is used as a specific and sensitive serum marker of the disease [4,9]. Interferences due to the presence of serum Tg antibodies should be excluded because they may lead to false negative results and less frequently to false positive results. After total ablation of the thyroid gland with surgery and post-operative administration of RAI, serum Tg should be undetectable and any detectable Tg signals the persistence of thyroid cells. After surgery only, remnants of normal thyroid tissue may produce detectable amounts of Tg in the serum; however, following total thyroidectomy the size of these remnants is normally small and serum Tg is frequently undetectable or detectable at a low level on thyroid hormone treatment. False negative serum Tg measurements are rare and mostly observed in patients with small tumor foci in neck lymph nodes or in lungs.
Functional imaging is a sensitive tool for locating a residual thyroid cancer focus and can also provide prognostic information. RAI uptake in neoplastic foci is associated with the efficacy of RAI treatment and with a better prognosis, while FDG uptake on PET/CT can be associated with a more aggressive behavior and RAI refractoriness [4].
3. Radiopharmaceuticals for DTC Patients
3.1. Available Radioactive Isotopes of Iodine for Clinical Use Include 123I, 131I and 124I
The metabolism of RAI in thyroid cells depends on several steps, including iodine uptake and organification that are altered in thyroid cancer tissues, resulting in a low iodine concentration and in a short effective half-life of iodine in the cells compared to normal thyroid tissue [5]. These abnormalities are related to a strongly reduced expression of the Natrium/Iodide Symporter (NIS) and of thyroid peroxidase (TPO) mRNA, but Tg, SLC26A4 (which encodes pendrin), Dual oxidase (Duox) and thyroid stimulating hormone receptor (TSH-R) gene expression is still present in most differentiated thyroid cancers [6,19]. The TTF-1, FOXE1, PAX-8 and HEX transcription factors are implicated in thyroid development 19. Altered expression levels of TTF-1 and PAX-8, have been demonstrated in DTC [20], and NIS expression levels were significantly related to PAX-8 and to HEX expression levels. Immunohistochemistry confirmed that NIS protein expression is profoundly decreased in differentiated thyroid cancer tissues, and in positive samples, NIS protein is detected in only a few malignant cells that appear to be polarized [21]. Other studies suggested that in some thyroid cancer tissues the NIS protein is present in the intra-cellular compartments but is not transported to the cell membrane, and this may explain why it is not biologically active [22]. TPO biological activity is reduced [23] and TPO immunostaining is weak or absent in most carcinomas when using the monoclonal antibody MoAb47 [24].
During thyroid hormone treatment in the absence of TSH stimulation there is no detectable uptake of RAI in neoplastic lesions.
Following TSH stimulation, RAI uptake is detectable in 70% of patients with metastases and serum Tg level increases in nearly all patients with metastases [25,26]. These data clearly show that TSH stimulates functional parameters of thyroid cancer cells
DTC are characterized by several genomic alterations [27]. In particular, the BRAF V600E point mutation is the most frequent alteration in papillary thyroid cancers (PTC) (45–60%); RAS and then TERT promoter point mutations can be also found and gene fusions (TRK 1/3, RET, ALK, BRAF) are detectable in only 15% of tumor samples [28]. These alterations result in an aberrant activation of the MAPK pathway that is found in 85% of PTC and has a crucial role in the impairment of iodide uptake and metabolism. RAS, TERT promoter, TP53, EIF1AX, PTEN, RB1, GNAS point mutations and PAX8-PPARG, ALK, NTRK 1/3, RET fusions can be detected in follicular thyroid carcinomas [29,30]. The spectrum of mutations that can be found in Hürthle cell carcinoma is slightly different [31]. The density of mutations is higher in poorly differentiated thyroid cancers, BRAF and RAS point mutations being the most frequent alterations [32].
In pre-clinical models of DTC, a forced expression of the BRAF V600E mutated gene in thyroid cells impaired the expression of almost all functional genes, which could be restored by ceasing its expression or by suppressing the MAPK pathway activity with a BRAF or a MEK inhibitor [33,34]. PTC patients with a BRAF V600E mutation demonstrate decreased or absent expression of thyroid functional genes coding for NIS and TPO [35,36]. The presence of a TERT promoter mutation is associated with a poor outcome [27,28]. Of note, while about 30% of all DTC patients with metastases do not demonstrate any RAI uptake following TSH stimulation [9], this proportion increases to 70% in those with BRAF V600E mutation and to 97% in presence of both BRAF V600E and TERT promoter mutations [37]. In conclusion, PTC classified as BRAF-like tumors are more dedifferentiated than RAS-like PTC, and metastases with RAI uptake are enriched in RAS mutated tumors [38]. Furthermore, in BRAF V600E mutated tumors besides the decrease in iodine gene expression there is an increase in the Glucose Transporter-1 (GLUT-1) gene expression [39] (see Section 3.4) indicating a more aggressive disease [40].
3.2. Physical Characteristics of Radioactive Iodine Isotopes
Physical characteristics of radioactive iodine isotopes are summarized in Table 1.

Table 1.
RAI isotopes available for diagnosis and treatment of DTC.
123I has a physical half-life of 13 hours and decays by electron capture with emission of a photon with an energy of 159 keV allowing good imaging quality. However, its high cost and limited availability make its clinical use limited in routine practice [41]. 131I is characterized by a physical half-life of 8.02 days. From its decay beta particles are emitted with a maximal energy of 606 keV and a mean energy of 191 keV and gamma rays, with a main gamma ray energy of 364 keV that make this radioisotope suitable for both therapeutic purpose and imaging. Beta particles can cause multiple ionizations before losing their energy and are responsible for most of the therapeutic effect. The penetration of electrons in soft tissue is about 1 mm and their damaging effect is restricted to a large extent to thyroid cells. The detection of gamma rays allows diagnostic imaging after low activity administration and post-therapeutic imaging after the administration of a high activity [42]. This detection can also be used for dosimetry purposes. 131I is cheaper than the other radioactive iodine isotopes and is widely available. 124I is a positron emitting isotope suitable for PET imaging. Its half-life is 4.2 days with a complex decay scheme and approximately 23% of the disintegrations result in positron emissions. The main clinical application of 124I is diagnostic imaging [3] and lesion dosimetry [43,44,45,46,47]. Unfortunately, 124I is expensive, not available in all countries and is mostly used for research purposes.
Thyroid-cancer tissue concentrates RAI only following TSH stimulation. Elevated serum TSH concentrations can be obtained by withdrawing thyroxine for three to six weeks [4,9]. The resulting hypothyroidism can be attenuated by replacing the thyroxine with triiodothyronine (that is more rapidly metabolized) for 3 weeks (25 µg/day during the first week, 50 µg/day during the second week, 75 µg/day during the third week), and then withdrawing it for 2 weeks. Various protocols are used for this preparation to RAI administration and to assure a significant uptake of 131I the serum TSH concentration should be higher than 30 mIU/L but the optimal TSH level to be attained is not well defined [4,48]. An alternative method for TSH stimulation of thyroid tissue is the use of recombinant human TSH (rhTSH) that is given intramuscularly (0.9mg) (Thyrogen, Sanofi-Genzyme, Cambridge, USA) for two consecutive days and RAI is administered on the day following the second injection. RhTSH stimulation is performed during thyroid hormone treatment. It is well tolerated; its use avoids hypothyroid symptoms and maintains the quality of life [49]. Clinical trials have demonstrated an efficacy of rhTSH similar to thyroid hormone withdrawal both for diagnostic use during follow-up with serum Tg determination and 131I diagnostic whole-body scan (d-WBS) [50] and for post-operative administration of 131I [51,52,53]; however, in patients with distant metastases, metastatic RAI uptake was lower following rhTSH than following thyroid hormone withdrawal [54,55].
When RAI administration is planned iodine-containing medications and iodine-rich foods should be avoided, and a delay of 4 weeks should be observed after an injection of contrast medium for CT [56]. In women of childbearing age, pregnancy must be excluded, and RAI should not be administered in breastfeeding women [4,48,57].
3.3. Methods Used for Functional Imaging with 131I: WBS and SPECT/CT
For diagnostic 131I WBS, 74 to 185 MBq (2 to 5 mCi) of 131I is normally given to obtain images with adequate quality, while the recommended activity following rhTSH stimulation is 148 MBq (4 mCi) [50]. Higher activities may reduce the uptake of a subsequent therapeutic activity of 131I; this phenomenon is called stunning, but its relevance is still controversial and probably does not contraindicate pre-therapy RAI d-WBS in patients for whom it might be beneficial [58,59]. Scanning is performed 2 to 3 days after the administration, using a double-head whole-body gamma camera equipped for the high energy of the main photon emitted by 131I (364 keV) with thick crystals and high-energy collimators.
Fractional uptake in neoplastic foci is assumed to be equivalent after the administration of a low or a high activity of 131I, and low uptake that may be no detectable after 74 to 185 MBq (2 to 5 mCi) and may be detectable only after the administration of 3700 MBq (100 mCi) or more. This is the rationale for performing a WBS 3 to 7 days after each therapeutic administration of 131I, that will also control and quantitate the RAI uptake in neoplastic foci [60].
Accurate anatomic localization of all foci of uptake is feasible with the use of SPECT/CT that ensures differentiation between uptake in lymph nodes and that in normal thyroid remnants in the neck, in ribs or in lungs in the chest, in the urinary or digestive tract or in bones in the pelvis [61,62,63]. Both pre-therapeutic diagnostic and post-therapeutic WBS can be associated with SPECT/CT that also permits a quantitation of uptake and a dosimetry evaluation.
Patient education is mandatory before any 131I administration to attenuate body radiation exposure, for image quality improvement and for reduction in false positive images. Thus, lemon juice is suggested to limit salivary gland uptake, ingestion of large quantities of liquid and laxatives may decrease bladder, gonad and colon irradiation. Stimulation of saliva flow with lemon juice given right after 131I administration is associated with an increased risk of alterations of salivary gland function [64]. Thus, lemon juice should be given after 24 h following 131I therapy. Finally, patients are invited to take a shower and to wear clean clothes before scanning. False positive results are infrequent [65] and are mostly observed on high activity 131I WBS.
Even in the presence of high serum TSH concentration, and in the absence of any iodine contamination, only two-thirds of patients with metastatic disease exhibit some 131I uptake. Uptake is more frequently observed and is more important in young patients with small metastases from a well-differentiated thyroid tumor [66].
3.4. 18F-FDG
18F-FDG is the most commonly used PET radiotracer for metabolic characterization, detection of recurrence, staging and evaluation of response to therapy especially in most aggressive or less differentiated tumors [67,68]. It is entrapped into cells through glucose transporters (GLUT). The expression of GLUT genes is increased in aggressive differentiated and dedifferentiated thyroid tumors and is related to TSH levels [69]. 18F-FDG PET/CT can be performed while the patient is on thyroid hormone treatment, but 18F-FDG uptake in neoplastic foci will increase following thyroid hormone treatment withdrawal or following injections of rhTSH, thus slightly increasing both its specificity and sensitivity, but with limited clinical benefits d. Semi-quantitation of uptake is performed using various parameters, including Standardized Uptake Value (SUV) [70].
The sensitivity of 18F-FDG PET/CT increases with higher serum Tg levels and with larger size of the tumor foci. Nevertheless, in case of highly proliferating disease and in those with a short Tg doubling time, the sensitivity can be very high, even in the presence of low Tg levels [71]. 18F-FDG uptake can be detected in neck lymph nodes, even in nodes of less than 1 cm in diameter, in lung and in bone metastases. However, PET scan failed to detect abnormal 18F-FDG uptake in small miliary lung metastases detected by CT scan, due to an absence of 18F-FDG uptake in these well differentiated and slow growing neoplastic cells, and partial volume effect, consisting of the combined effect of poor spatial resolution and the contamination of activity from neighboring tissues or spillover effect (Figure 1) [72,73].
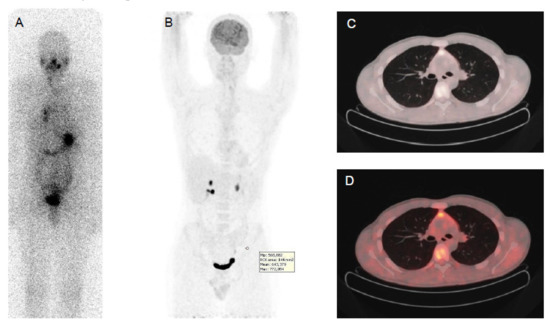
Figure 1.
Papillary thyroid cancer in a 41-year-old man with a high thyroid stimulating hormone stimulated serum thyroglobulin level (475 ng/mL). Post-therapy (A) 131I whole-body scan showed pulmonary uptake and uptake and in neck lymph nodes. 18F-FDG PET-CT (B,C,D): CT images evidenced multiple small millimetric lung metastases (B,C,D), without significant 18F-FDG uptake.
In DTC patients, the “flip-flop phenomenon” consists of a mismatch between high glucose and low iodine uptake, due to the elevated glucose metabolism coupled to the dedifferentiation process and has an important prognostic significance (Figure 2). This is observed in patients with iodine refractory thyroid cancer, with poorly differentiated, Hürthle cell cancer, PTC with aggressive features (tall cell variant) or with the BRAF V600E mutation and less frequently in patients with well differentiated papillary or follicular carcinoma. This indicates clinically more aggressive lesions [74,75,76] and the presence of 18F-FDG uptake in lesions with also radioiodine uptake indicates that these lesions are less likely to respond to radioiodine treatment [77].
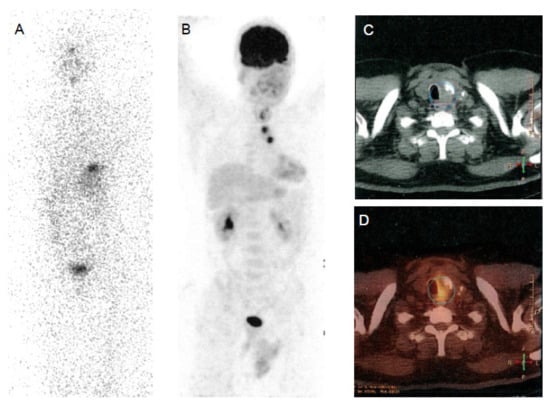
Figure 2.
Papillary thyroid cancer in a 30-year-old woman. Post-therapy (A) 131I whole-body scan and 18F-FDG PET-CT (B,C,D) images. Post-therapy 131I whole-body scan did not show areas of uptake (A). 18F-FDG PET-CT images evidenced multiple areas of increased uptake in the left retrosternal and latero-cervical region.
3.5. Other Tracers
The 18F-tetrafluoroborate (18F-TFB) is an analog of iodine that can be used for imaging the NIS expressing cells but that will not undergo organification in the thyroid cells, that is decreased or non-existent in thyroid cancer cells. 18F-TFB biodistribution in patients with thyroid cancer is similar to that of 99mTc-pertechnetate [78]. The potential 18F-TFB advantages come from the possibility of using a more rapid synthesis of this PET tracer over the less available and more costly 124I. In small series of patients, results obtained with 18F-TFB appeared similar to those obtained with 124I PET/CT [79] or with 131I d-WBS [80].
The prostate-specific membrane antigen (PSMA) is a transmembrane glycoprotein receptor that is highly expressed in prostate carcinoma cells. However, its expression has been associated with neovascular development in several tumors, including DTC [81]. Its expression seems related with a lower differentiation level and more aggressive histology or refractoriness. The 68Ga-PSMA was used in small series of DTC patients with some promising results as a theragnostic radiopharmaceutical, giving the possibility in case of positive imaging results to select DTC patients for 177-Lutetium (177Lu)-PSMA therapy [82]. Recently, two patients underwent (177Lu)-PSMA therapy and achieved a minor tumor response [82]. The agent 2-(3- {1-carboxy-5- [(6- [(18)F] fuoropyridine-3-carbonyl)-amino]-pentyl}-ureido)-pentanedioic acid (DCPyl) labeled with 18F is another PSMA-PET imaging agent with the advantage of imaging obtained with 18F consisting in a potential widely available and easily low cost produced tracer (Figure 3) [43]. 18F-Fluoride has been used for evaluating with PET patients with bone metastases from thyroid cancer in small series of patients, but these lesions are lytic, frequently with a low uptake and this makes their evaluation difficult [83]. This is in accordance with the absence of efficacy of 223Radium in treating bone metastases from DTC [84]. Further studies are needed for evaluating the utility of these tracers in DTC patients.
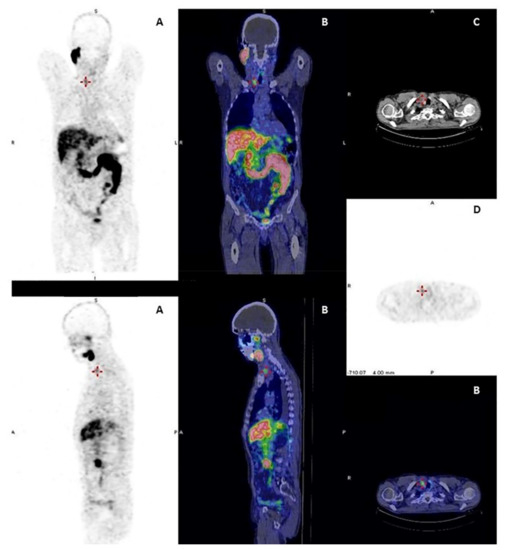
Figure 3.
A 76-year-old patient with prostate cancer and a right thyroid nodule of 15 mm in diameter. Multiple image projections (A), fusion PET-CT images (B), CT images (C) and PET images (D), respectively, of 68Ga-PSMA imaging with high-intensity PSMA accumulation. Fine needle aspiration biopsy of PSMA-avid thyroid lesion was performed revealing an indeterminate cytology. Final histology revealed papillary thyroid cancer.
4. PET Imaging Methods
4.1. PET/CT
The ring detector system of PET technology benefits of positron emitting radionuclides for detection of coincidences. The positron and electron annihilation results in two 511 keV photons [85,86]. The relatively long half-life of 18F (110 minutes) and 124I (4.2 days) allows transportation of these radionuclides from the production facility to the imaging sites. The integration of PET stand-alone modality with CT in a single PET/CT device provides several advantages, including a complementary accurate localization and characterization of tumor foci [87]. Moreover, the addition of CT permits attenuation correction. Beyond visual analysis, PET/CT allows semi-quantitative evaluation of tracer uptake, by using several parameters including standardized uptake values (SUV).
4.2. PET/MR
Magnetic resonance (MR) imaging is a sensitive diagnostic technique for evaluation of DTC recurrence extent in the neck, mediastinum, bones, and liver. Simultaneous PET/MR provides complementary data. However, high costs and limited spread in diagnostic units limit its clinical routine use. Few studies on limited series of DTC patients found an excellent correlation between the two imaging techniques (PET/MR vs. PET/CT) despite, as expected, an inferior sensitivity of MR in the detection of lung metastases [88]. In a recent work, 40 consecutive DTC patients were evaluated at follow-up by sequential 18F-FDG PET/CT and 18F-FDG PET/MR imaging scans [89]. 18F-FDG PET/MR was positive in 11 patients detecting 33 lesions, while 10 patients showed positive findings with 30 lesions detected at 18F-FDG PET/CT.
Indeed, PET/MR when available might be performed in selected patients with bone, soft tissue or liver lesions for whom a MR imaging is indicated (Figure 4).
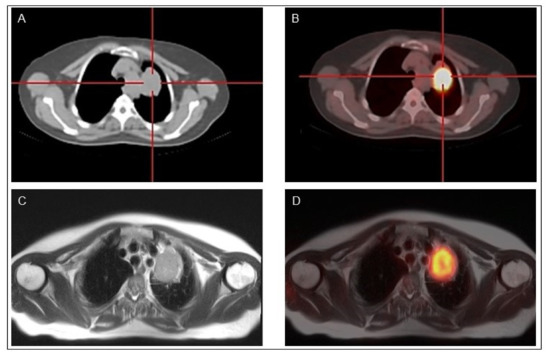
Figure 4.
Classical papillary thyroid cancer in a 45-year-old man18F-FDG PET-CT (A,B) and 18F-FDG PET-MR (C,D) show a mediastinal lymph node with high 18F-FDG uptake.
5. Indications for the Use of Radioactive Iodine
Radioiodine exposure has raised major concerns. The radiation dose delivered to the bone marrow after the administration of 3700 MBq in hypothyroid condition was estimated at 0.50 Gy [90]. However, despite reassuring data demonstrating the absence of untoward pregnancy outcome and the low risk of second primary malignancies observed only following the administration of high cumulative activities of radioiodine [91,92,93], the administered activities should be reduced as much as possible.
5.1. Post-Operative Administration of RAI
In low-risk patients, retrospective studies did not demonstrate consistent benefits of the post-operative 131I administration in terms of recurrence and mortality [4,9,94,95,96,97,98]. Discrepant results are, at least in part, related to differences in risk assessment: the TNM classification of the risk of cancer related death was used in many studies to predict the risk of recurrence and a retrospective study based on the ATA risk stratification of recurrence did not show any benefit of the post-operative administration of 131I in low-risk patients [98]. This is not surprising given a risk of persistent structural disease after surgery of less than 5% that can be frequently cured with a later treatment and a risk of mortality of less than 1%. Additionally, after total thyroidectomy that normally leaves only small remnants of non-tumoral thyroid tissue, the follow-up can reliably be based on serum Tg determination obtained on thyroid hormone treatment and neck ultrasound, even in the absence of post-operative 131I administration (Figure 5) [4,9].
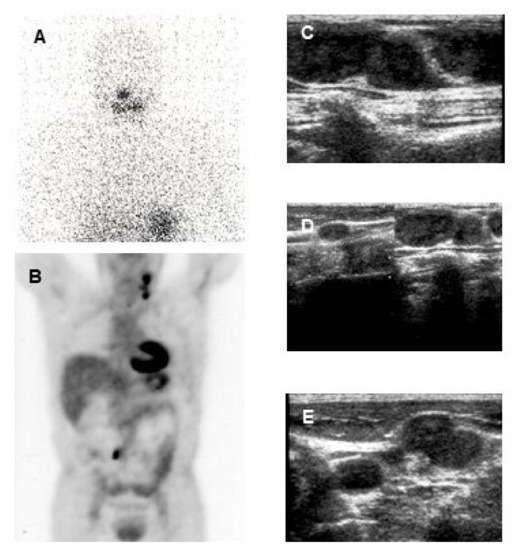
Figure 5.
37-year-old woman with a papillary thyroid cancer (tall cell variant) with a post-operative TSH-stimulated serum thyroglobulin (Tg) level of 230 ng/mL. Post-therapy 131I whole-body scan (A) did not show any area of increased uptake. 18F-FDG PET-CT (B) evidenced multiple areas of increased uptake in the left latero-cervical region and homogeneous cardiac 18F-FDG uptake (that is not an infrequent finding, also in patients without overt cardiac disease). Ultrasound (C,D,E) evidenced multiple suspicious lymph-nodes in the left latero-cervical region, with round shape, loss of echogenic hilus and micro lobulated margins. At fine needle aspiration cytology confirmed lymph node metastases from the papillary thyroid cancer and the Tg concentration was elevated (3800 ng/mL) in the aspirate fluid.
The possibility that post-operative 131I might be administered only in a selected subset of low-risk patients derives from several studies and should consider the following points:
- The current definition of excellent response to treatment (and of complete ablation in case of post-operative administration of 131I) at 6–12 months is based, in the absence of a control radioiodine WBS [99,100], on undetectable serum Tg level in the absence of Tg-Ab (either < 1ng/mL following rhTSH when using a traditional assay or < 0.2 ng/mL on L-T4 treatment when using a sensitive assay) and a neck ultrasound (US) without any abnormal findings [4,9,101].
- In two prospective randomized non-inferiority trials in low-risk patients, the percentage of complete ablation was similar when using for preparation either rhTSH injections on L-T4 treatment or withdrawal of thyroid hormone treatment and administration of either 1100 or 3700 MBq 131I [52,53]. Indeed, with rhTSH there was no hypothyroid symptom, and the quality of life was maintained [49]. With a 5-year follow-up, only few patients (<5%) received further treatments and the same favorable outcome was observed regardless of the initial ablation protocol used [102,103]. In conclusion, when indicated in low-risk patients a post-operative administration of 131I should consist in the administration of 1100 MBq following rhTSH injections.
- Less than 5% of these low-risk patients had persistent disease, and this suggests that 131I might be not beneficial and may represent over-treatment in the other 95% [4,47]; low-risk patients might be selected for ablation on the basis of the post-operative neck US and serum Tg level, the risk of persistent disease being low in patients with undetectable Tg and increases with higher serum Tg levels [101,102,103,104]. It is, however, still unclear whether the post-operative 131I administration may improve the outcome of these patients with detectable post-operative Tg levels. This is being evaluated within two ongoing prospective randomized non-inferiority trials (ESTIMABL2 and ION) that compare the outcome of low-risk patients treated either with 1100 MBq following rhTSH or followed-up with no post-operative 131I.
Intermediate-risk patients represent a heterogeneous group of patients, and their management is still under debate. RAI treatment should be planned according to risk factors and post-operative findings [105]. A longitudinal and observational study compared the outcomes of low and lower-intermediate risk (minimal extra-thyroid extension or ≤5 central compartment lymph node metastases) DTC patients undergoing either systematic or selective use of RAI treatment [106]. After 3 years of follow-up, the rate of structural incomplete response was low (1–3%) and did not differ with either approach. After 1 year of follow-up, a significantly higher rate of patients with residual detectable serum Tg was observed after selective RAI as compared to the systematic RAI cohort. Interestingly, this difference was no more statistically significant after a longer follow-up. These data suggest that selective use of RAI permits to achieve comparable low rates of structural disease but poses the issue of the management of persistent residual Tg or Tg-Ab. It is likely that intermediate risk patients with a post-operative low or undetectable serum Tg level have a low risk of persistent disease and can probably be managed such as low-risk patients, but prospective trials in well-defined groups of patients are needed such as the INTERMEDIATE trial currently ongoing in France.
In high-risk patients, high 131I activities (3700 MBq or even more) should be administered post-operatively following withdrawal of thyroid hormone treatment [9]. Radioactive iodine in this case aims at ablation of normal thyroid remnants and at eradication of persistent neoplastic foci that may be occult (adjuvant treatment) or known (treatment) with a reported positive impact on patient outcome [107,108].
The ASTRA phase III study (NCT01843062) in high-risk DTC patients failed to demonstrate an improved disease-free survival with selumetinib (a MEK inhibitor)-enhanced adjuvant RAI administration compared with placebo and adjuvant RAI. This may be due to the low inhibitory efficacy of selumetinib. As already pointed out, in patients with a BRAF V600E mutation, in particular if a TERT mutation is also present, the RAI uptake in the neoplastic tissue is frequently absent, and these patients might benefit from a redifferentiation program before being treated with RAI, but further trials are needed (see Section 7).
5.2. Use of Radioiodine for Diagnosis
In the past, 131I d-WBS was routinely used in many situations, post-operatively to assess the completeness of surgical resection and the potential indication for the administration of a high activity of radioiodine, during follow-up to assess excellent response or to detect persistent and recurrent disease and before any therapeutic administration for persistent or recurrent disease to assess the presence of radioiodine uptake in neoplastic foci. At the present time, d-WBS is less frequently performed: post-operative administration of 131I is mostly based on the surgical report, on prognostic indicators and on post-operative serum Tg level and neck US findings; additionally, the completeness of total thyroidectomy is improved, leaving in most patients only small remnants of non-tumoral thyroid tissue and in this condition the post-therapy WBS is frequently more informative than the d-WBS that is currently not routinely performed in many centers in low risk patients. A recent statement proposed that a d-WBS might be selectively performed in intermediate risk patients in the post-operative staging to guide, in addition to clinical and surgical data the decision of a therapeutic RAI administration and select a personalized patient-based activity [105]; however, in the absence of prospective data, the benefits afforded by the d-WBS remain uncertain. A randomized trial in lower-intermediate risk DTC patients (estimated risk of recurrence about 8%) comparing systematic RAI administration (3700 MBq) to a selective RAI administration based on post-operative rhTSH stimulated Tg, neck US and RAI d-WBS is ongoing in France (INTERMEDIATE trial, NCT04290663).
Follow-up is currently based on the combination of serum Tg determination and of neck US and when performed, 131I d-WBS does not improve the detection of persistent/recurrent disease in the neck and control d-WBS is not indicated in patients with undetectable serum Tg and neck US with no abnormal finding [99,100,101]; control d-WBS may be indicated in patients with large thyroid remnants in whom the post-therapy WBS was poorly informative, in those with equivocal foci of uptake on the post-therapy WBS, and in high risk patients with detectable serum Tg-Ab in whom serum Tg determination is not reliable [4].
6. Comparison between 131I and 124I
124I PET/CT imaging offers several benefits, including improved spatial resolution and better diagnostic sensitivity, over 131I SPECT imaging [109]. 124I PET scanning can be performed up to 120 hours after the tracer administration. The sensitivity of 124I PET/CT in identifying DTC lesions was excellent (94.2%), being better than 123I/131I d-WBS, and at least equivalent to post-therapy 131I WBS planar imaging and even demonstrates more lesions in some patients [43]. In DTC patients, 124I can also be used for the pre-therapeutic lesion dosimetry.
7. Use of Radioactive Iodine for Treatment of Distant Metastases
Treatment of distant metastases with RAI is based on the administration of high 131I activities [110,111,112]. A relationship between the radiation dose delivered to tumor foci and its efficacy has been reported. The mean recommended radiation dose to treat metastases is 100 Gy [113,114] and the clinical issue is to administer an activity of 131I high enough to deliver an effective radiation dose to tumor foci. The absorbed dose depends on the initial radioactive concentration of 131I in the tissue, namely the ratio between the initial total uptake and the mass of neoplastic tissue and on its effective half-life in the tissue, i.e., the time after which the radioactivity in the tissue has decreased by a factor of 2. The effective half-life is related to both 131I physical half-life (8.02 days) and to its biological half-life, which is related to its elimination from the tissue. Even though the administered activity of 131I is high, the absorbed dose delivered to neoplastic foci might be suboptimal for successful therapy due to a low radioiodine concentration and to a decreased organification rate resulting in a short effective half-life of RAI in the lesion. While iodine uptake is about 1%/g of the administered activity in normal thyroid tissues, it ranges from 0.1% to 0.001%, or is even lower in neoplastic tissues and the effective half-life of 131I ranges from 6–8 days in normal thyroid tissues and only 2–5 days or even less in neoplastic tissues [5]. Attempts have been made to improve RAI efficacy, including prolonged withdrawal of thyroid hormone treatment that stimulates higher metastatic uptake than rhTSH injections [54,55], avoiding iodine contamination and optimizing the administered activity of 131I. The administered activity can be standard or determined by pre-therapeutic dosimetry [44,45,46,47,115]. Pre-therapeutic lesion dosimetry from repeated three-dimensional imaging with 131I SPECT/CT or 124I PET/CT after a tracer administration enables reconstruction of the time–activity curve within the lesion and will permit to determine the activity to be administered to deliver an optimal radiation dose to the lesion. The volume in which uptake occurs can be estimated with the current use of three-dimensional imaging, using 131I and SPECT/CT. The poor spatial resolution of this imaging technique is a limiting factor for accurate measurement of small volumes. Moreover, the absolute quantitation of 131I concentration in small lesions is challenging because of the complex detection and image reconstruction processes [116]. PET/CT using 124I provides a higher spatial resolution and a semi-quantitative measurement of radioactivity [44,45,46,47].
Whole-body/blood clearance dosimetry determines the maximal activity that can be administered so that the absorbed dose to blood does not exceed 200 cGy and in the presence of iodine-avid diffuse lung metastases that the whole-body retention does not exceed 2960 MBq (80 mCi) at 48 h after administration, in order to prevent toxic effects, respectively, on the bone marrow and lungs [117,118,119,120].
A retrospective study showed a similar overall survival of DTC patients with distant metastases treated either with a standard activity of 3700 MBq or with higher activities determined with blood dosimetry [115]. This investigation is in accordance with other studies that found no evidence that pre-therapeutic dosimetry might improve the outcome of metastatic patients [44,45,46,47]. Indeed, prospective studies are needed in metastatic patients to define the role and the impact of dosimetry.
Between 131I treatment courses, thyroid hormone treatment decreases serum TSH to low or undetectable levels. Complete tumor responses were observed in one third of patients with distant metastases, mostly in young patients with small metastases from a well differentiated cancer, with initial high 131I uptake [66]. Unfortunately, not all metastases with 131I uptake respond to 131I treatment, and this is frequently the case of large metastases, elderly patients or in the presence of high 18F-FDG uptake on PET/CT scan [77]. Several explanations have been proposed [5]: the radiation dose might be not high enough to induce cell killing, but as already mentioned increasing the administered activity may not increase enough the dose to the tumor to improve anti-tumor efficacy; anti-tumor efficacy depends also on the sensitivity of thyroid cancer cells to radiation and this is not routinely taken into account; tumor heterogeneity with radiation doses that may differ from one focus to another [44] and also heterogeneous expression of NIS among tumor cells within a single metastasis [5,21]. Finally, the dose estimated by pre-therapy dosimetry with a low activity may differ from the dose effectively delivered during a 131I treatment due to a stunning effect induced by the high radiation dose delivered during treatment and this can be assessed by a post-therapy WBS with quantitation of uptake.
When there is no evidence of RAI uptake in the metastases or when 131I avid metastases progress despite RAI treatment, the disease is considered 131I refractory and RAI is of no further utility becomes useless. This occurs in about two-thirds of patients with extensive disease, who have then a reduced 10-year life expectancy of only ~10%, and who will require other treatment modalities, particularly in case of large tumor burden, symptoms or risk of local complication or documented rapid tumor progression [121]. A redifferentiation program has been used in several trials in patients with advanced refractory thyroid cancer with a RAS or a BRAF mutation [122,123]. The administration for 4–6 weeks of a BRAF or a MEK inhibitor either alone or in combination induced the re-apparition of radioiodine uptake in 40 to more than 60 % of patients that allowed treatment with 131I after rhTSH stimulation [124,125,126]. This treatment is also capable of restoring a more differentiated histologic appearance and induces an increased production of Tg and thyroid hormones in the serum. A RECIST partial tumor response was then achieved in 25% up to more than 40% [127]. This strategy may apply also to DTC harboring other molecular abnormalities treated with selective inhibitors, as suggested by the RAI uptake restoration observed in a RAI refractory DTC patient with a NTRK fusion treated with Larotrectinib [128] and in a patient with a RET fusion treated with Selpercatinib [129] An open label multicentric clinical trial is ongoing in France (NCT 03244956) testing the efficacy in terms of objective response rate of an anti-MEK or anti-MEK and anti-BRAF selective inhibition before RAI treatment in metastatic RAI-refractory DTC with, respectively, a RAS or BRAF mutation.
8. Use of 18F-FDG PET/CT in Clinical Practice
8.1. 18F-FDG PET/CT for the Post-Operative Staging of Aggressive Disease
Patients with a histologically aggressive disease (Hürthle cell, poorly differentiated, widely invasive follicular carcinoma or with an aggressive variant of papillary thyroid cancer, including tumors harboring a BRAF V600E mutation) may demonstrate less differentiated cancer cells, with low serum Tg and no 131I uptake. These patients may be referred to initial 18F-FDG PET/CT before any treatment or after surgery when there is a suspicion of persistent disease [75,130], since the TSH-stimulated serum Tg and the 131I WBS cannot exclude persistent disease.
8.2. 18F-FDG PET/CT for Elevated Serum Tg and No Other Evidence of Disease
Patients with detectable serum Tg level on thyroid hormone treatment (>5–10 ng/mL) and no other evidence of disease (i.e., with a biochemically incomplete response) need further imaging modalities, especially when the serum Tg level increases over time. In the past, administration of large empiric activities of 131I have been encouraged due to the poor sensitivity of the gamma camera detectors available at that time [131]. Currently, 18F-FDG PET/CT is a reliable technique to identify occult neoplastic foci in these patients [70]. In 34 DTC patients with elevated serum Tg that increased over time, 18F-FDG PET/CT was more sensitive than 131I post-therapy WBS in detecting neoplastic foci (88% vs. 16% of 75 foci, respectively) [131]. The frequency of abnormal findings in 18F-FDG PET/CT increases with higher serum Tg levels, and this is the rationale for considering 18F-FDG PET/CT only in patients with a serum Tg level above 5–10 ng/mL on thyroid hormone treatment or in case of rapid Tg doubling time, independently of its absolute value [71]. As already mentioned, the use of rhTSH stimulation before 18F-FDG PET/CT in patients with low serum Tg and no other evidence of disease slightly increases its sensitivity for the detection of neoplastic foci, but with limited clinical benefits [74]. Additionally, tumors with high 18F-FDG uptake generally fail to concentrate 131I and in case of detectable 131I uptake they frequently fail to respond to 131I treatment [77], and thus 131I treatment could be less appropriate in these patients. The use of empiric 131I therapy could be suggested only in the few patients with serum Tg levels increasing over time and without 18F-FDG uptake.
Furthermore, an overall 84% sensitivity and a 78% specificity of 18F-FDG PET/CT has been observed for the detection of recurrent disease in the presence of elevated Tg-Ab levels and negative 131I WBS [132].
8.3. 18F-FDG PET/CT in Patients with Structural Disease
In these patients with structural disease, imaging could visualize neoplastic foci, the extent of disease ranging from small lymph node metastases in the neck to large multiple distant metastases.
Small lymph node metastases (< 1 cm in diameter) may be treated with 131I in the presence of radioiodine uptake and with surgical resection either as first line treatment or in case of persistence after several 131I treatment courses [132,133,134]. In patients with a more extended neck recurrence and in those with distant metastases, 18F-FDG PET/CT is performed before defining treatment: it provides an extensive work-up of the extent of the disease both in the neck and at distant sites. In patients with metastatic RAI uptake, 18F-FDG PET/CT may identify some lesions with low or absent RAI uptake and, therefore, not seen on RAI WBS. This can be complemented with CT scan with contrast medium and/or MRI of the neck and mediastinum that will better define the local extent of the disease. There is usually no 18F-FDG uptake in miliary lung metastases that are typically observed in young patients. These miliary lung metastases might be visualized on CT scan, but in some patients because of their small size they are visualized only on post therapeutic RAI WBS. MRI of the liver, bones and brain may also be useful. 18F-FDG PET/CT also provides prognostic information, with tumor with high 18F-FDG uptake characterized by a more aggressive course [74] and responding less frequently to 131I treatment [77]. However, in a given patient, the tumor growth rate of a given metastasis at 1 year is not related to the intensity of its 18F-FDG uptake [135]. Semi-quantitative 18F-FDG uptake is a parameter used in complement to tumor volume assessment for the follow-up of patients with tumor foci and to help deciding their treatment. 18F-FDG PET/CT is also useful for assessing the completeness of focal treatment modalities, such as thermal ablation [74] and the efficacy of systemic treatment using either tyrosine kinase inhibitors or immunotherapy with check point inhibitors [4,9,76].
18F-FDG uptake is not specific and false positive results have been reported in up to 39 % of patients [68]. For this reason, a fine needle aspiration biopsy should confirm the thyroid origin of any focus of uptake in neck lymph node areas before defining a therapeutic strategy.
9. Conclusions
Functional imaging plays a central role in the management of DTC patients, in particular in those at intermediate or high risk. Radioactive iodine is used in DTC patients mostly with a therapeutic intent, either post-operatively or in patients with known structural disease for whom it is often the first line systemic treatment, and a sensitive WBS is performed a few days after the administration. 124I showed encouraging results in a dosimetric approach, but its potential clinical benefit is still not demonstrated.
PET/CT with 18F-FDG complements the use of radioactive iodine at the initial evaluation in patients with high-risk DTC, during follow-up in those with rising serum Tg levels over time and in the work-up of patients with documented structural disease.
Author Contributions
All authors made substantial contributions to this work; writing—original draft preparation: M.K., E.Z., C.N., L.L., E.C., R.A., E.N.; supervision and review of the paper: M.S., A.C., D.D., D.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| ATA | American Thyroid Association |
| CT | Computed tomography |
| DTC | Differentiated thyroid cancer |
| 18F-FDG | 18F-fluorodeoxyglucose |
| 18F-TFB | 18F-tetrafluoroborate |
| GLUT | Glucose Transporter |
| GLUT-1 | Glucose Transporter-1 |
| MR | Magnetic resonance |
| NIS | Natrium/Iodide Symporter |
| PET | Positron emission tomography |
| PSMA | Prostate specific membrane antigen |
| RAI | Radioactive iodine |
| SPECT | Single photon emission tomography |
| Tg | Thyroglobulin |
| TPO | Thyroid peroxidase |
| TSH | Thyroid stimulating hormone |
| US | Ultrasound |
| WBS | Whole-body scan |
| d-WBS | Diagnostic-WBS |
References
- Hertz, S.; Roberts, A. Radioactive Iodine as an Indicator in Thyroid Physiology. V. The Use of Radioactive Iodine in the Differential Diagnosis of Two Types of Graves’ Disease. J. Clin. Investig. 1942, 21, 31–32. [Google Scholar] [CrossRef] [PubMed]
- Hertz, S.; Roberts, A.; Salter, W.T. Radioactive Iodine as an Indicator in Thyroid Physiology. IV. The Metabolism of Iodine in Graves’ Disease. J. Clin. Investig. 1942, 21, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Keston, A.S.; Ball, R.P.; Frantz, V.K.; Palmer, W.W. Storage of Radioactive Iodine in a Metastasis from Thyroid Carcinoma. Science 1942, 95, 362–363. [Google Scholar] [CrossRef] [PubMed]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: The American Thyroid Association Guidelines Task Force on thyroid nodules and differentiated thyroid cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Schlumberger, M.; Lacroix, L.; Russo, D.; Filetti, S.; Bidart, J.M. Defects in iodide metabolism in thyroid cancer and implications for the follow-up and treatment of patients. Nat. Clin. Pract. Endocrinol. Metab. 2007, 3, 260–269. [Google Scholar] [CrossRef]
- Lazar, V.; Bidart, J.M.; Caillou, B.; Mahé, C.; Lacroix, L.; Filetti, S.; Schlumberger, M. Expression of the Na+/I- symporter gene in human thyroid tumors: A comparison study with other thyroid-specific genes. J. Clin. Endocrinol. Metab. 1999, 84, 3228–3234. [Google Scholar] [CrossRef]
- Durski, J.M.; Hruska, C.B.; Bogsrud, T.V.; Ryder, M.; Johnson, G.B. 123I Scan With Whole-Body Retention Measurement at 48 Hours for Simplified Dosimetry Before 131I Treatment of Metastatic Thyroid Cancer. Clin. Nucl. Med. 2021, 46, e151–e153. [Google Scholar] [CrossRef]
- Mazzaferri, E.L.; Jhiang, S.M. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am. J. Med. 1994, 97, 418–428, Erratum in 1995, 98, 215. [Google Scholar] [CrossRef]
- Filetti, S.; Durante, C.; Hartl, D.; Leboulleux, S.; Locati, L.D.; Newbold, K.; Papotti, M.G.; Berruti, A.; ESMO Guidelines Committee. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann. Oncol. 2019, 30, 1856–1883. [Google Scholar] [CrossRef]
- Avram, A.M.; Dewaraja, Y.K. Thyroid Cancer Radiotheragnostics: The case for activity adjusted 131I therapy. Clin. Transl. Imaging 2018, 6, 335–346. [Google Scholar] [CrossRef]
- Ciappuccini, R.; Heutte, N.; Lasne-Cardon, A.; Saguet-Rysanek, V.; Leroy, C.; Le Hénaff, V.; Vaur, D.; Babin, E.; Bardet, S. Tumor burden of persistent disease in patients with differentiated thyroid cancer: Correlation with postoperative risk-stratification and impact on outcome. BMC Cancer 2020, 20, 765. [Google Scholar] [CrossRef] [PubMed]
- Lodi Rizzini, E.; Repaci, A.; Tabacchi, E.; Zanoni, L.; Vicennati, V.; Cavicchi, O.; Pagotto, U.; Morganti, A.G.; Fanti, S.; Monari, F. Impact of 18F-FDG PET/CT on Clinical Management of Suspected Radio-Iodine Refractory Differentiated Thyroid Cancer (RAI-R-DTC). Diagnostics 2021, 11, 1430. [Google Scholar] [CrossRef] [PubMed]
- Freudenberg, L.S.; Antoch, G.; Jentzen, W.; Pink, R.; Knust, J.; Görges, R.; Müller, S.P.; Bockisch, A.; Debatin, J.F.; Brandau, W. Value of (124)I-PET/CT in staging of patients with differentiated thyroid cancer. European radiology. Eur. Radiol. 2004, 14, 2092–2098. [Google Scholar] [CrossRef] [PubMed]
- D’Avanzo, A.; Treseler, P.; Ituarte, P.H.; Wong, M.; Streja, L.; Greenspan, F.S.; Siperstein, A.E.; Duh, Q.Y.; Clark, O.H. Follicular thyroid carcinoma: Histology and prognosis. Cancer 2004, 100, 1123–1129. [Google Scholar] [CrossRef] [PubMed]
- Ibrahimpasic, T.; Ghossein, R.; Shah, J.P.; Ganly, I. Poorly Differentiated Carcinoma of the Thyroid Gland: Current Status and Future Prospects. Thyroid 2019, 29, 311–321. [Google Scholar] [CrossRef]
- Kim, K.; Kim, J.K.; Lee, C.R.; Kang, S.W.; Lee, J.; Jeong, J.J.; Nam, K.H.; Chung, W.Y. Comparison of long-term prognosis for differentiated thyroid cancer according to the 7th and 8th editions of the AJCC/UICC TNM staging system. Ther. Adv. Endocrinol. Metab. 2020, 11, 2042018820921019. [Google Scholar] [CrossRef]
- Simões-Pereira, J.; Mourinho, N.C.; Ferreira, T.; Limbert, E.; Cavaco, B.M.; Leite, V. Avidity and outcomes of radioiodine therapy for distant metastasis of distinct types of differentiated thyroid cancer. J. Clin. Endocrinol. Metab. 2021, dgab436. [Google Scholar] [CrossRef]
- Avram, A.M.; Zukotynski, K.; Nadel, H.R.; Giovanella, L.M. Management Of Differentiated Thyroid Cancer: The Standard Of Care. J. Nucl. Med. 2021, 121, 262402. [Google Scholar] [CrossRef]
- Fernández, L.P.; López-Márquez, A.; Santisteban, P. Thyroid transcription factors in development, differentiation and disease. Nat. Rev. Endocrinol. 2015, 11, 29–42. [Google Scholar] [CrossRef]
- Fabbro, D.; Di Loreto, C.; Beltrami, C.A.; Belfiore, A.; Di Lauro, R.; Damante, G. Expression of thyroid-specific transcription factors TTF-1 and PAX-8 in human thyroid neoplasms. Cancer Res. 1994, 54, 4744–4749. [Google Scholar]
- Ravera, S.; Reyna-Neyra, A.; Ferrandino, G.; Amzel., L.M.; Carrasco, N. The Sodium/Iodide Symporter (NIS): Molecular Physiology and Preclinical and Clinical Applications. Annu. Rev. Physiol. 2017, 79, 261–289. [Google Scholar] [CrossRef] [PubMed]
- Dohán, O.; Baloch, Z.; Bánrévi, Z.; Livolsi, V.; Carrasco, N. Rapid communication: Predominant intracellular overexpression of the Na(+)/I(-) symporter (NIS) in a large sampling of thyroid cancer cases. J. Clin. Endocrinol. Metab. 2001, 86, 2697–2700. [Google Scholar] [CrossRef] [PubMed]
- Fragu, P.; Nataf, B.M. Human thyroid peroxidase activity in benign and malign thyroid disorders. J. Clin. Endocrinol. Metab. 1997, 45, 1089–1096. [Google Scholar] [CrossRef] [PubMed]
- Di Cristofaro, J.; Silvy, M.; Lanteaume, A.; Marcy, M.; Carayon, P.; De Micco, C. Expression of tpo mRNA in thyroid tumors: Quantitative PCR analysis and correlation with alterations of RET, BRAF, RAS and PAX8 genes. Endocr.-Relat. Cancer 2006, 13, 485–495. [Google Scholar] [CrossRef]
- Schlumberger, M.; Charbord, P.; Fragu, P.; Lumbroso, J.; Parmentier, C.; Tubiana, M. Circulating thyroglobulin and thyroid hormones in patients with metastases of differentiated thyroid carcinoma: Relationship to serum thyrotropin levels. J. Clin. Endocrinol. Metab. 1980, 51, 513–519. [Google Scholar] [CrossRef]
- Schlumberger, M.; Charbord, P.; Fragu, P.; Gardet, P.; Lumbroso, J.; Parmentier, C.; Tubiana, M. Relationship between thyrotropin stimulation and radioiodine uptake in lung metastases of differentiated thyroid carcinoma. J. Clin. Endocrinol. Metab. 1983, 57, 148–151. [Google Scholar] [CrossRef]
- Xing, M.; Alzahrani, A.S.; Carson, K.A.; Viola, D.; Elisei, R.; Bendlova, B.; Yip, L.; Mian, C.; Vianello, F.; Tuttle, R.M.; et al. Association between BRAF V600E mutation and mortality in patients with papillary thyroid cancer. JAMA 2013, 309, 1493–1501. [Google Scholar] [CrossRef]
- Xing, M.; Alzahrani, A.S.; Carson, K.A.; Shong, Y.K.; Kim, T.Y.; Viola, D.; Elisei, R.; Bendlová, B.; Yip, L.; Mian, C.; et al. Association between BRAF V600E mutation and recurrence of papillary thyroid cancer. J. Clin. Oncol. 2015, 33, 42–50. [Google Scholar] [CrossRef]
- Yoo, S.K.; Lee, S.; Kim, S.J.; Jee, H.G.; Kim, B.A.; Cho, H.; Song, Y.S.; Cho, S.W.; Won, J.K.; Shin, J.Y.; et al. Comprehensive analysis of the transcriptional and mutational landscape of follicular and papillary thyroid cancers. PLoS Genet. 2016, 12, e1006239. [Google Scholar] [CrossRef]
- Pozdeyev, N.; Gay, L.M.; Sokol, E.S.; Hartmaier, R.; Deaver, K.E.; Davis, S.; French, J.D.; Borre, P.V.; LaBarbera, D.V.; Tan, A.C.; et al. Genetic analysis of 779 advanced differentiated and anaplastic thyroid cancers. Clin. Cancer Res. 2018, 24, 3059–3068. [Google Scholar] [CrossRef]
- Ganly, I.; Makarov, V.; Deraje, S.; Dong, Y.; Reznik, E.; Seshan, V.; Nanjangud, G.; Eng, S.; Bose, P.; Kuo, F.; et al. Integrated genomic analysis of Hürthle cell cancer reveals oncogenic drivers, recurrent mitochondrial mutations, and unique chromosomal landscapes. Cancer Cell 2018, 34, 256–270.e5. [Google Scholar] [CrossRef]
- Landa, I.; Ibrahimpasic, T.; Boucai, L.; Sinha, R.; Knauf, J.A.; Shah, R.H.; Dogan, S.; Ricarte-Filho, J.C.; Krishnamoorthy, G.P.; Xu, B.; et al. Genomic and transcriptomic hallmarks of poorly differentiated and anaplastic thyroid cancers. J. Clin. Investig. 2016, 126, 1052–1066. [Google Scholar] [CrossRef]
- Knauf, J.A.; Ma, X.; Smith, E.P.; Zhang, L.; Mitsutake, N.; Liao, X.H.; Refetoff, S.; Nikiforov, Y.E.; Fagin, J.A. Targeted expression of BRAFV600E in thyroid cells of transgenic mice results in papillary thyroid cancers that undergo dedifferentiation. Cancer Res. 2005, 65, 4238–4245. [Google Scholar] [CrossRef]
- Chakravarty, D.; Santos, E.; Ryder, M.; Knauf, J.A.; Liao, X.H.; West, B.L.; Bollag, G.; Kolesnick, R.; Thin, T.H.; Rosen, N.; et al. Small-molecule MAPK inhibitors restore radioiodine incorporation in mouse thyroid cancers with conditional BRAF activation. J. Clin. Investig. 2011, 121, 4700–4711. [Google Scholar] [CrossRef] [PubMed]
- Durante, C.; Puxeddu, E.; Ferretti, E.; Morisi, R.; Moretti, S.; Bruno, R.; Barbi, F.; Avenia, N.; Scipioni, A.; Verrienti, A.; et al. BRAF mutations in papillary thyroid carcinomas inhibit genes involved in iodine metabolism. J. Clin. Endocrinol. Metab. 2007, 92, 2840–2843. [Google Scholar] [CrossRef]
- Romei, C.; Ciampi, R.; Faviana, P.; Agate, L.; Molinaro, E.; Bottici, V.; Basolo, F.; Miccoli, P.; Pacini, F.; Pinchera, A.; et al. BRAFV600E mutation; but not RET/PTC rearrangements, is correlated with a lower expression of both thyroperoxidase and sodium iodide symporter genes in papillary thyroid cancer. Endocr.-Relat. Cancer 2008, 15, 511–520. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Liu, R.; Shen, X.; Zhu, G.; Li, B.; Xing, M. The genetic duet of BRAF V600E and TERT promoter mutations robustly predicts loss of radioiodine avidity in recurrent papillary thyroid cancer. J. Nucl. Med. 2020, 61, 177–182. [Google Scholar] [CrossRef]
- Sabra, M.M.; Dominguez, J.M.; Grewal, R.K.; Larson, S.M.; Ghossein, R.A.; Tuttle, R.M.; Fagin, J.A. Clinical outcomes and molecular profile of differentiated thyroid cancers with radioiodine-avid distant metastases. J. Clin. Endocrinol. Metab. 2013, 98, E829–E836. [Google Scholar] [CrossRef]
- Yoon, M.; Jung, S.J.; Kim, T.H.; Ha, T.K.; Urm, S.H.; Park, J.S.; Lee, S.M.; Bae, S.K. Relationships between transporter expression and the status of BRAF V600E mutation and F-18 FDG uptake in papillary thyroid carcinomas. Endocr. Res. 2016, 41, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Grabellus, F.; Worm, K.; Schmid, K.W.; Sheu, S.Y. The BRAF V600E mutation in papillary thyroid carcinoma is associated with glucose transporter 1 overexpression. Thyroid 2012, 22, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Giovanella, L.; Avram, A.M.; Iakovou, I.; Kwak, J.; Lawson, S.A.; Lulaj, E.; Luster, M.; Piccardo, A.; Schmidt, M.; Tulchinsky, M.; et al. EANM practice guideline/SNMMI procedure standard for RAIU and thyroid scintigraphy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2514–2525. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, P.S.; Gupta, M. Differentiated thyroid cancer theranostics: Radioiodine and beyond. Br. J. Radiol. 2018, 91, 20180136. [Google Scholar] [CrossRef]
- Santhanam, P.; Taieb, D.; Solnes, L.; Marashdeh, W.; Ladenson, P.W. Utility of I-124 PET/CT in identifying radioiodine avid lesions in differentiated thyroid cancer: A systematic review and meta-analysis. Clin. Endocrinol. 2017, 86, 645–651. [Google Scholar] [CrossRef] [PubMed]
- Sgouros, G.; Kolbert, K.S.; Sheikh, A.; Pentlow, K.S.; Mun, E.F.; Barth, A.; Robbins, R.J.; Larson, S.M. Patient-specific dosimetry for 131I thyroid cancer therapy using 124I PET and 3-dimensional-internal dosimetry (3D-ID) software. J. Nucl. Med. 2004, 45, 1366–1372. [Google Scholar] [PubMed]
- Lassmann, M.; Reiners, C.; Luster, M. Dosimetry and thyroid cancer: The individual dosage of radioiodine. Endocr.-Relat. Cancer 2010, 17, R161–R172. [Google Scholar] [CrossRef] [PubMed]
- Klubo-Gwiezdzinska, J.; Van Nostrand, D.; Atkins, F.; Burman, K.; Jonklaas, J.; Mete, M.; Wartofsky, L. Efficacy of dosimetric versus empiric prescribed activity of 131I for therapy of differentiated thyroid cancer. J. Clin. Endocrinol. Metab. 2011, 96, 3217–3225. [Google Scholar] [CrossRef]
- Wierts, R.; Brans, B.; Havekes, B.; Kemerink, G.J.; Halders, S.G.; Schaper, N.N.; Backes, W.H.; Mottaghy, F.M.; Jentzen, W. Dose-response relationship in differentiated thyroid cancer patients undergoing radioiodine treatment assessed by means of 124I PET/CT. J. Nucl. Med. 2016, 57, 1027–1032. [Google Scholar] [CrossRef]
- Luster, M.; Clarke, S.E.; Dietlein, M.; Lassmann, M.; Lind, P.; Oyen, W.J.; Tennvall, J.; Bombardieri, E. Guidelines for radioiodine therapy of differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2008, 35, 1941–1959. [Google Scholar] [CrossRef]
- Borget, I.; Bonastre, J.; Catargi, B.; Déandréis, D.; Zerdoud, S.; Rusu, D.; Bardet, S.; Leenhardt, L.; Bastie, D.; Schvartz, C.; et al. Quality of life and cost-effectiveness assessment of radioiodine ablation strategies in patients with thyroid cancer: Results from the randomized phase III ESTIMABL trial. J. Clin. Oncol. 2015, 33, 2885–2892. [Google Scholar] [CrossRef]
- Haugen, B.R.; Pacini, F.; Reiners, C.; Schlumberger, M.; Ladenson, P.W.; Sherman, S.; Cooper, D.S.; Graham, K.E.; Braverman, L.E.; Skarulis, M.C.; et al. A comparison of recombinant human thyrotropin and thyroid hormone withdrawal for the detection of thyroid remnant or cancer. J. Clin. Endocrinol. Metab. 1999, 84, 3877–3885. [Google Scholar] [CrossRef]
- Pacini, F.; Ladenson, P.W.; Schlumberger, M.; Driedger, A.; Luster, M.; Kloos, R.T.; Sherman, S.; Haugen, B.; Corone, C.; Molinaro, E.; et al. Radioiodine ablation of thyroid remnants after preparation with recombinant human thyrotropin in differentiated thyroid carcinoma: Results of an international, randomized, controlled study. J. Clin. Endocrinol. Metab. 2006, 91, 926–932. [Google Scholar] [CrossRef]
- Schlumberger, M.; Catargi, B.; Borget, I.; Deandreis, D.; Zerdoud, S.; Bridji, B.; Bardet, S.; Leenhardt, L.; Bastie, D.; Schvartz, C.; et al. Tumeurs de la thyroïde refractaires network for the essai stimulation ablation equivalence trial. Strategies of radioiodine ablation in patients with low-risk thyroid cancer. N. Engl. J. Med. 2012, 366, 1663–1673. [Google Scholar] [CrossRef] [PubMed]
- Mallick, U.; Harmer, C.; Yap, B.; Wadsley, J.; Clarke, S.; Moss, L.; Nicol, A.; Clark, P.M.; Farnell, K.; McCready, R.; et al. Ablation with low-dose radioiodine and thyrotropin alfa in thyroid cancer. N. Engl. J. Med. 2012, 366, 1674–1685. [Google Scholar] [CrossRef]
- Pötzi, C.; Moameni, A.; Karanikas, G.; Preitfellner, J.; Becherer, A.; Pirich, C.; Dudczak, R. Comparison of iodine uptake in tumour and nontumour tissue under thyroid hormone deprivation and with recombinant human thyrotropin in thyroid cancer patients. Clin. Endocrinol. 2006, 65, 519–523. [Google Scholar] [CrossRef]
- Plyku, D.; Hobbs, R.F.; Huang, K.; Atkins, F.; Garcia, C.; Sgouros, G.; Van Nostrand, D. Recombinant human thyroid-stimulating hormone versus thyroid hormone withdrawal in 124I PET/CT-based dosimetry for 131I therapy of metastatic differentiated thyroid cancer. J. Nucl. Med. 2017, 58, 1146–1154. [Google Scholar] [CrossRef] [PubMed]
- Padovani, R.P.; Kasamatsu, T.S.; Nakabashi, C.C.; Camacho, C.P.; Andreoni, D.M.; Malouf, E.Z.; Marone, M.M.; Maciel, R.M.; Biscolla, R.P. One month is sufficient for urinary iodine to return to its baseline value after the use of water-soluble iodinated contrast agents in post-thyroidectomy patients requiring radioiodine therapy. Thyroid 2012, 22, 926–930. [Google Scholar] [CrossRef] [PubMed]
- Sacks, W.; Fung, C.H.; Chang, J.T.; Waxman, A.; Braunstein, G.D. The effectiveness of radioactive iodine for treatment of low-risk thyroid cancer: A systematic analysis of the peer-reviewed literature from 1966 to April 2008. Thyroid 2010, 20, 1235–1245. [Google Scholar] [CrossRef] [PubMed]
- Yap, B.K.; Murby, B. No adverse effect in clinical outcome using low preablation diagnostic (131) I activity in differentiated thyroid cancer: Refuting thyroid-stunning effect. J. Clin. Endocrinol. Metab. 2014, 99, 2433–2440. [Google Scholar] [CrossRef][Green Version]
- Leger, F.A.; Izembart, M.; Dagousset, F.; Barritault, L.; Baillet, G.; Chevalier, A.; Clerc, J. Decreased uptake of therapeutic doses of iodine-131 after 185-MBq iodine-131 diagnostic imaging for thyroid remnants in differentiated thyroid carcinoma. Eur. J. Nucl. Med. Mol. Imaging 1998, 25, 242–246. [Google Scholar] [CrossRef]
- Schlumberger, M.; Mancusi, F.; Baudin, E.; Pacini, F. 131I therapy for elevated thyroglobulin levels. Thyroid 1997, 7, 273–276. [Google Scholar] [CrossRef]
- Aide, N.; Heutte, N.; Rame, J.P.; Rousseau, E.; Loiseau, C.; Henry-Amar, M.; Bardet, S. Clinical relevance of single-photon emission computed tomography/computed tomography of the neck and thorax in postablation (131) I scintigraphy for thyroid cancer. J. Clin. Endocrinol. Metab. 2009, 94, 2075–2084. [Google Scholar] [CrossRef] [PubMed]
- Grewal, R.K.; Tuttle, R.M.; Fox, J.; Borkar, S.; Chou, J.F.; Gonen, M.; Strauss, H.W.; Larson, S.M.; Schöder, H. The effect of posttherapy 131I SPECT/CT on risk classification and management of patients with differentiated thyroid cancer. J. Nucl. Med. 2010, 51, 1361–1367. [Google Scholar] [CrossRef]
- Wong, K.K.; Sisson, J.C.; Koral, K.F.; Frey, K.A.; Avram, A.M. Staging of differentiated thyroid carcinoma using diagnostic 131I SPECT/CT. AJR Am. J. Roentgenol. 2010, 195, 730–736. [Google Scholar] [CrossRef]
- Nakada, K.; Ishibashi, T.; Takei, T.; Hirata, K.; Shinohara, K.; Katoh, S.; Zhao, S.; Tamaki, N.; Noguchi, Y.; Noguchi, S. Does lemon candy decrease salivary gland damage after radioiodine therapy for thyroid cancer? J. Nucl. Med. 2005, 46, 261–266. [Google Scholar] [PubMed]
- Carlisle, M.R.; Lu, C.; McDougall, I.R. The interpretation of 131I scans in the evaluation of thyroid cancer; with an emphasis on false positive findings. Nucl. Med. Commun. 2003, 24, 715–735. [Google Scholar] [CrossRef] [PubMed]
- Durante, C.; Haddy, N.; Baudin, E.; Leboulleux, S.; Hartl, D.; Travagli, J.P.; Caillou, B.; Ricard, M.; Lumbroso, J.D.; De Vathaire, F.; et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: Benefits and limits of radioiodine therapy. J. Clin. Endocrinol. Metab. 2006, 91, 2892–2899. [Google Scholar] [CrossRef] [PubMed]
- Gallamini, A.; Zwarthoed, C.; Borra, A. Positron Emission Tomography (PET) in Oncology. Cancers 2014, 6, 1821–1889. [Google Scholar] [CrossRef] [PubMed]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. European Association of Nuclear Medicine (EANM) FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Schönberger, J.; Rüschoff, J.; Grimm, D.; Marienhagen, J.; Rümmele, P.; Meyringer, R.; Kossmehl, P.; Hofstaedter, F.; Eilles, C. Glucose transporter 1 gene expression is related to thyroid neoplasms with an unfavorable prognosis: An immunohistochemical study. Thyroid 2002, 12, 747–754. [Google Scholar] [CrossRef]
- Leboulleux, S.; Schroeder, P.R.; Schlumberger, M.; Ladenson, P.W. The role of PET in follow-up of patients treated for differentiated epithelial thyroid cancers. Nat. Clin. Pract. Endocrinol. Metab. 2007, 3, 112–121. [Google Scholar] [CrossRef]
- Giovanella, L.; Trimboli, P.; Verburg, F.A.; Treglia, G.; Piccardo, A.; Foppiani, L.; Ceriani, L. Thyroglobulin levels and thyroglobulin doubling time independently predict a positive 18F-FDG PET/CT scan in patients with biochemical recurrence of differentiated thyroid carcinoma. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 874–880. [Google Scholar] [CrossRef]
- Marcus, C.; Whitworth, P.W.; Surasi, D.S.; Pai, S.I.; Subramaniam, R.M. PET/CT in the management of thyroid cancers. AJR Am. J. Roentgenol. 2014, 202, 1316–1329. [Google Scholar] [CrossRef] [PubMed]
- Salvatori, M.; Biondi, B.; Rufini, V. Imaging in endocrinology: 2-[18F]-fluoro-2-deoxy-D-glucose positron emission tomography/computed tomography in differentiated thyroid carcinoma: Clinical indications and controversies in diagnosis and follow-up. Eur. J. Endocrinol. 2015, 173, R115–R130. [Google Scholar] [CrossRef]
- Deandreis, D.; Al Ghuzlan, A.; Leboulleux, S.; Lacroix, L.; Garsi, J.P.; Talbot, M.; Lumbroso, J.; Baudin, E.; Caillou, B.; Bidart, J.M.; et al. Do histological, immunohistochemical, and metabolic (radioiodine and fluorodeoxyglucose uptakes) patterns of metastatic thyroid cancer correlate with patient outcome? Endocr.-Relat. Cancer 2011, 18, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum-Krumme, S.J.; Görges, R.; Bockisch, A.; Binse, I. 18F-FDG PET/CT changes therapy management in high-risk DTC after first radioiodine therapy. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 1373–1380. [Google Scholar] [CrossRef] [PubMed]
- Grewal, R.K.; Ho, A.; Schöder, H. Novel approaches to thyroid cancer treatment and response assessment. Semin. Nucl. Med. 2016, 46, 109–118. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Robbins, R.J.; Wan, Q.; Grewal, R.K.; Reibke, R.; Gonen, M.; Strauss, H.W.; Tuttle, R.M.; Drucker, W.; Larson, S.M. Real-time prognosis for metastatic thyroid carcinoma based on 2-[18F] fluoro-2-deoxy-D-glucose-positron emission tomography scanning. J. Clin. Endocrinol. Metab. 2006, 91, 498–505. [Google Scholar] [CrossRef]
- Samnick, S.; Al-Momani, E.; Schmid, J.S.; Mottok, A.; Buck, A.K.; Lapa, C. Initial clinical investigation of [18F] Tetrafluoroborate PET/CT in comparison to [124I] Iodine PET/CT for imaging thyroid cancer. Clin. Nucl. Med. 2018, 43, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; DeGrado, T.R. [18F] Tetrafluoroborate ([18F] TFB) and its analogs for PET imaging of the sodium/iodide symporter. Theranostics 2018, 8, 3918–3931. [Google Scholar] [CrossRef] [PubMed]
- Dittmann, M.; Gonzalez Carvalho, J.M.; Rahbar, K.; Schäfers, M.; Claesener, M.; Riemann, B.; Seifert, R. Incremental diagnostic value of [18F] tetrafluoroborate PET-CT compared to [131I] iodine scintigraphy in recurrent differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 2639–2646. [Google Scholar] [CrossRef]
- Lawhn-Heath, C.; Yom, S.S.; Liu, C.; Villanueva-Meyer, J.E.; Aslam, M.; Smith, R.; Narwal, M.; Juarez, R.; Behr, S.C.; Pampaloni, M.H.; et al. Gallium-68 prostate-specific membrane antigen ([68Ga] Ga-PSMA-11) PET for imaging of thyroid cancer: A feasibility study. EJNMMI Res. 2020, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- De Vries, L.H.; Lodewijk, L.; Braat, A.; Krijger, G.C.; Valk, G.D.; Lam, M.; Borel Rinkes, I.; Vriens, M.R.; de Keizer, B. 68Ga-PSMA PET/CT in radioactive iodine-refractory differentiated thyroid cancer and first treatment results with 177Lu-PSMA-617. EJNMMI Res. 2020, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Schirrmeister, H.; Buck, A.; Guhlmann, A.; Reske, S.N. Anatomical distribution and sclerotic activity of bone metastases from thyroid cancer assessed with F-18 sodium fluoride positron emission tomography. Thyroid 2001, 11, 677–683. [Google Scholar] [CrossRef]
- Deandreis, D.; Maillard, A.; Zerdoud, S.; Bournaud, C.; Vija, L.; Sajous, C.; Terroir, M.; Leenhardt, L.; Schlumberger, M.; Borget, I.; et al. RADTHYR: An open-label, single-arm, prospective multicenter phase II trial of Radium-223 for the treatment of bone metastases from radioactive iodine refractory differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 3238–3249. [Google Scholar] [CrossRef] [PubMed]
- Brink, J.A. PET/CT unplugged: The merging technologies of PET and CT imaging. AJR Am. J. Roentgenol. 2005, 184, S135–S137. [Google Scholar] [CrossRef] [PubMed]
- Costa, D.C.; Visvikis, D.; Crosdale, I.; Pigden, I.; Townsend, C.; Bomanji, J.; Prvulovich, E.; Lonn, A.; Ell, P.J. Positron emission and computed X-ray tomography: A coming together. Nucl. Med. Commun. 2003, 24, 351–358. [Google Scholar] [CrossRef]
- Shammas, A.; Degirmenci, B.; Mountz, J.M.; McCook, B.M.; Branstetter, B.; Bencherif, B.; Joyce, J.M.; Carty, S.E.; Kuffner, H.A.; Avril, N. 18F-FDG PET/CT in patients with suspected recurrent or metastatic well-differentiated thyroid cancer. J. Nucl. Med. 2007, 48, 221–226. [Google Scholar]
- Vrachimis, A.; Burg, M.C.; Wenning, C.; Allkemper, T.; Weckesser, M.; Schäfers, M.; Stegger, L. [(18)F]FDG PET/CT outperforms [(18)F]FDG PET/MRI in differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Klain, M.; Nappi, C.; Nicolai, E.; Romeo, V.; Piscopo, L.; Giordano, A.; Gaudieri, V.; Zampella, E.; Pace, L.; Carlo, C.; et al. Comparison of simultaneous 18F-2-[18F] FDG PET/MR and PET/CT in the follow-up of patients with differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 3066–3073. [Google Scholar] [CrossRef]
- M’Kacher, R.; Legal, J.D.; Schlumberger, M.; Voisin, P.; Aubert, B.; Gaillard, N.; Parmentier, C. Biological dosimetry in patients treated with iodine-131 for differentiated thyroid carcinoma. J. Nucl. Med. 1996, 37, 1860–1864. [Google Scholar]
- Rubino, C.; De Vathaire, F.; Dottorini, M.E.; Hall, P.; Schvartz, C.; Couette, J.E.; Dondon, M.-G.; Abbas, M.T.; Langlois, C.; Schlumberger, M. Second primary malignancies in thyroid cancer patients. Br. J. Cancer 2003, 89, 1638–1644. [Google Scholar] [CrossRef] [PubMed]
- Garsi, J.P.; Schlumberger, M.; Rubino, C.; Ricard, M.; Labbé, M.; Ceccarelli, C.; Schvartz, C.; Henri-Amar, M.; Bardet, S.; de Vathaire, F. Therapeutic administration of 131I for differentiated thyroid cancer: Radiation dose to ovaries and outcome of pregnancies. J. Nucl. Med. 2008, 49, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Verburg, F.A.; Hoffmann, M.; Iakovou, I.; Konijnenberg, M.W.; Mihailovic, J.; Gabina, P.M.; Ovčariček, P.P.; Reiners, C.; Vrachimis, A.; Zerdoud, S.; et al. Errare humanum est, sed in errare perseverare diabolicum: Methodological errors in the assessment of the relationship between I-131 therapy and possible increases in the incidence of malignancies. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 519–522. [Google Scholar] [CrossRef]
- Hay, I.D.; Johnson, T.R.; Kaggal, S.; Reinalda, M.S.; Iniguez-Ariza, N.M.; Grant, C.S.; Pittock, S.T.; Thompson, G.B. Papillary Thyroid Carcinoma (PTC) in Children and Adults: Comparison of Initial Presentation and Long-Term Postoperative Outcome in 4432 Patients Consecutively Treated at the Mayo Clinic During Eight Decades (1936–2015). World J. Surg. 2018, 42, 329–342. [Google Scholar] [CrossRef] [PubMed]
- Sawka, A.M.; Brierley, J.D.; Tsang, R.W.; Thabane, L.; Rotstein, L.; Gafni, A.; Straus, S.; Goldstein, D.P. An updated systematic review and commentary examining the effectiveness of radioactive iodine remnant ablation in well-differentiated thyroid cancer. Endocrinol. Metab. Clin. North Am. 2008, 37, 457–480. [Google Scholar] [CrossRef]
- Schlumberger, M.; Leboulleux, S. Current practice in patients with differentiated thyroid cancer. Nat. Rev. Endocrinol. 2021, 17, 176–188. [Google Scholar] [CrossRef] [PubMed]
- Schvartz, C.; Bonnetain, F.; Dabakuyo, S.; Gauthier, M.; Cueff, A.; Fieffé, S.; Pochart, J.M.; Cochet, I.; Crevisy, E.; Dalac, A.; et al. Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients. J. Clin. Endocrinol. Metab. 2012, 97, 1526–1535. [Google Scholar] [CrossRef] [PubMed]
- Lamartina, L.; Durante, C.; Filetti, S.; Cooper, D.S. Low-risk differentiated thyroid cancer and radioiodine remnant ablation: A systematic review of the literature. J. Clin. Endocrinol. Metab. 2015, 100, 1748–1761. [Google Scholar] [CrossRef]
- Cailleux, A.F.; Baudin, E.; Travagli, J.P.; Ricard, M.; Schlumberger, M. Is diagnostic iodine-131 scanning useful after total thyroid ablation for differentiated thyroid cancer? J. Clin. Endocrinol. Metab. 2000, 85, 175–178. [Google Scholar] [CrossRef] [PubMed]
- Pacini, F.; Capezzone, M.; Elisei, R.; Ceccarelli, C.; Taddei, D.; Pinchera, A. Diagnostic 131-iodine whole-body scan may be avoided in thyroid cancer patients who have undetectable stimulated serum Tg levels after initial treatment. J. Clin. Endocrinol. Metab. 2002, 87, 1499–1501. [Google Scholar] [CrossRef]
- Lamartina, L.; Grani, G.; Durante, C.; Borget, I.; Filetti, S.; Schlumberger, M. Follow-up of differentiated thyroid cancer—What should (and what should not) be done. Nat. Rev. Endocrinol. 2018, 14, 538–551. [Google Scholar] [CrossRef]
- Schlumberger, M.; Leboulleux, S.; Catargi, B.; Deandreis, D.; Zerdoud, S.; Bardet, S.; Rusu, D.; Godbert, Y.; Buffet, C.; Schvartz, C.; et al. Outcome after ablation in patients with low-risk thyroid cancer (ESTIMABL1): 5-year follow-up results of a randomised, phase 3, equivalence trial. Lancet Diabetes Endocrinol. 2018, 6, 618–626. [Google Scholar] [CrossRef]
- Dehbi, H.M.; Mallick, U.; Wadsley, J.; Newbold, K.; Harmer, C.; Hackshaw, A. Recurrence after low-dose radioiodine ablation and recombinant human thyroid-stimulating hormone for differentiated thyroid cancer (HiLo): Long-term results of an open-label, non-inferiority randomised controlled trial. Lancet Diabetes Endocrinol. 2019, 7, 44–51. [Google Scholar] [CrossRef]
- Matrone, A.; Gambale, C.; Piaggi, P.; Viola, D.; Giani, C.; Agate, L.; Bottici, V.; Bianchi, F.; Materazzi, G.; Vitti, P.; et al. Postoperative thyroglobulin and neck ultrasound in the risk restratification and decision to perform 131I ablation. J. Clin. Endocrinol. Metab. 2017, 102, 893–902. [Google Scholar] [CrossRef]
- Gulec, S.A.; Ahuja, S.; Avram, A.M.; Bernet, V.J.; Bourguet, P.; Draganescu, C.; Elisei, R.; Giovanella, L.; Grant, F.; Greenspan, B.; et al. A Joint Statement from the American Thyroid Association, the European Association of Nuclear Medicine, the European Thyroid Association, the Society of Nuclear Medicine and Molecular Imaging on Current Diagnostic and Theranostic Approaches in the Management of Thyroid Cancer. Thyroid 2021, 31, 1009–1019. [Google Scholar] [CrossRef] [PubMed]
- Grani, G.; Lamartina, L.; Alfò, M.; Ramundo, V.; Falcone, R.; Giacomelli, L.; Biffoni, M.; Filetti, S.; Durante, C. Selective use of radioactive iodine therapy for papillary thyroid cancers with low or lower-intermediate recurrence risk. J. Clin. Endocrinol. Metab. 2021, 106, e1717–e1727. [Google Scholar] [CrossRef] [PubMed]
- Verburg, F.A.; Mäder, U.; Reiners, C.; Hänscheid, H. Long-term survival in differentiated thyroid cancer is worse after low-activity initial post-surgical 131I therapy in both high- and low-risk patients. J. Clin. Endocrinol. Metab. 2014, 99, 4487–4496. [Google Scholar] [CrossRef]
- Gray, K.D.; Bannani, S.; Caillard, C.; Amanat, S.; Ullmann, T.M.; Romanov, P.; Brunaud, L.; Beninato, T.; Fahey, T.J., 3rd; Mirallie, E.; et al. High-dose radioactive iodine therapy is associated with decreased risk of recurrence in high-risk papillary thyroid cancer. Surgery 2019, 165, 37–43. [Google Scholar] [CrossRef]
- Wu, D.; Ylli, D.; Heimlich, S.L.; Burman, K.D.; Wartofsky, L.; Van Nostrand, D. 124I Positron emission tomography/computed tomography versus conventional radioiodine imaging in differentiated thyroid cancer: A review. Thyroid 2019, 29, 1523–1535. [Google Scholar] [CrossRef]
- Hertz, S.; Roberts, A. Radioactive iodine in the study of thyroid physiology; the use of radioactive iodine therapy in hyperthyroidism. J. Am. Med. Assoc. 1946, 131, 81–86. [Google Scholar] [CrossRef]
- Seidlin, S.M.; Marinelli, L.D.; Oshry, E. Radioactive iodine therapy; effect on functioning metastases of adenocarcinoma of the thyroid. J. Am. Med. Assoc. 1946, 132, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Coliez, R.; Tubiana, M.; Sung, S. Disappearance of pulmonary metastases of a thyroid cancer under the action of radioactive iodine 131. J. Radiol. Electrol. Arch. Electr. Med. 1951, 32, 396–399. [Google Scholar]
- Maxon, H.R., 3rd; Smith, H.S. Radioiodine-131 in the diagnosis and treatment of metastatic well differentiated thyroid cancer. Endocrinol. Metab. Clin. N. Am. 1990, 19, 685–718. [Google Scholar] [CrossRef]
- Maxon, H.R.; Thomas, S.R.; Hertzberg, V.S.; Kereiakes, J.G.; Chen, I.W.; Sperling, M.I.; Saenger, E.L. Relation between effective radiation dose and outcome of radioiodine therapy for thyroid cancer. N. Engl. J. Med. 1983, 309, 937–941. [Google Scholar] [CrossRef] [PubMed]
- Deandreis, D.; Rubino, C.; Tala, H.; Leboulleux, S.; Terroir, M.; Baudin, E.; Larson, S.; Fagin, J.A.; Schlumberger, M.; Tuttle, R.M. Comparison of Empiric Versus Whole-Body/-Blood Clearance Dosimetry-Based Approach to Radioactive Iodine Treatment in Patients with Metastases from Differentiated Thyroid Cancer. J. Nucl. Med. 2017, 58, 717–722. [Google Scholar] [CrossRef]
- Dewaraja, Y.K.; Ljungberg, M.; Green, A.J.; Zanzonico, P.B.; Frey, E.C.; SNMMI MIRD Committee; Bolch, W.E.; Brill, A.B.; Dunphy, M.; Fisher, D.R.; et al. MIRD pamphlet No. 24: Guidelines for quantitative 131I SPECT in dosimetry applications. J. Nucl. Med. 2013, 54, 2182–2188. [Google Scholar] [CrossRef]
- Rall, J.E.; Alpers, J.B.; Lewallen, C.G.; Sonenberg, M.; Berman, M.; Rawson, R.W. Radiation pneumonitis and fibrosis: A complication of radioiodine treatment of pulmonary metastases from cancer of the thyroid. J. Clin. Endocrinol. Metab. 1957, 17, 1263–1276. [Google Scholar] [CrossRef]
- Benua, R.S.; Cicale, N.R.; Sonenberg, M.; Rawson, R.W. The relation of radioiodine dosimetry to results and complications in the treatment of metastatic thyroid cancer. Am. J. Roentgenol. Radium Ther. Nucl. Med. 1962, 87, 171–182. [Google Scholar] [PubMed]
- Sgouros, G.; Song, H.; Ladenson, P.W.; Wahl, R.L. Lung toxicity in radioiodine therapy of thyroid carcinoma: Development of a dose-rate method and dosimetric implications of the 80-mCi rule. J. Nucl. Med. 2006, 47, 1977–1984. [Google Scholar]
- Tuttle, R.M.; Leboeuf, R.; Robbins, R.J.; Qualey, R.; Pentlow, K.; Larson, S.M.; Chan, C.Y. Empiric radioactive iodine dosing regimens frequently exceed maximum tolerated activity levels in elderly patients with thyroid cancer. J. Nucl. Med. 2006, 47, 1587–1591. [Google Scholar]
- Schlumberger, M.; Brose, M.; Elisei, R.; Leboulleux, S.; Luster, M.; Pitoia, F.; Pacini, F. Definition and management of radioactive iodine-refractory differentiated thyroid cancer. Lancet Diabetes Endocrinol. 2014, 2, 356–358. [Google Scholar] [CrossRef]
- Wirth, L.J. Still Perfecting Radioiodine in Thyroid Cancer, After All These Years. J. Clin. Endocrinol. Metab. 2019, 104, 1655–1657. [Google Scholar] [CrossRef]
- Jhiang, S.M.; Konda, B.; Sipos, J.A.; Nabhan, F.A. Prospects for redifferentiating agents in the use of radioactive Iodine therapy for thyroid cancer. Thyroid 2020, 30, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Ho, A.L.; Grewal, R.K.; Leboeuf, R.; Sherman, E.J.; Pfister, D.G.; Deandreis, D.; Pentlow, K.S.; Zanzonico, P.B.; Haque, S.; Gavane, S.; et al. Selumetinib-enhanced radioiodine uptake in advanced thyroid cancer. N. Engl. J. Med. 2013, 368, 623–632. [Google Scholar] [CrossRef]
- Rothenberg, S.M.; McFadden, D.G.; Palmer, E.L.; Daniels, G.H.; Wirth, L.J. Redifferentiation of iodine-refractory BRAF V600E-mutant metastatic papillary thyroid cancer with dabrafenib. Clin Cancer Res. 2015, 21, 1028–1035. [Google Scholar] [CrossRef] [PubMed]
- Leboulleux, S.; Dupuy, C.; Lacroix, L.; Attard, M.; Grimaldi, S.; Corre, R.; Ricard, M.; Nasr, S.; Berdelou, A.; Hadoux, J.; et al. Redifferentiation of a BRAFK601E-mutated poorly differentiated thyroid cancer patient with Dabrafenib and Trametinib treatment. Thyroid 2019, 29, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Lamartina, L.; Anizan, N.; Dupuy, C.; Leboulleux, S.; Schlumberger, M. Redifferentiation-facilitated radioiodine therapy in thyroid cancer. Endocr.-Relat. Cancer 2021, 28, T179–T191. [Google Scholar] [CrossRef]
- Groussin, L.; Clerc, J.; Huillard, O. Larotrectinib-enhanced radioactive iodine uptake in advanced thyroid cancer. N. Engl. J. Med. 2020, 383, 1686–1687. [Google Scholar] [CrossRef] [PubMed]
- Groussin, L.; Bessiene, L.; Arrondeau, J.; Garinet, S.; Cochand-Priollet, B.; Lupo, A.; Zerbit, J.; Clerc, J.; Huillard, O. Selpercatinib-Enhanced Radioiodine Uptake in RET-Rearranged Thyroid Cancer. Thyroid 2021. [Google Scholar] [CrossRef]
- Nascimento, C.; Borget, I.; Al Ghuzlan, A.; Deandreis, D.; Hartl, D.; Lumbroso, J.; Berdelou, A.; Lepoutre-Lussey, C.; Mirghani, H.; Baudin, E.; et al. Postoperative fluorine-18-fluorodeoxyglucose positron emission tomography/computed tomography: An important imaging modality in patients with aggressive histology of differentiated thyroid cancer. Thyroid 2015, 25, 437–444. [Google Scholar] [CrossRef]
- Leboulleux, S.; El Bez, I.; Borget, I.; Elleuch, M.; Déandreis, D.; Al Ghuzlan, A.; Chougnet, C.; Bidault, F.; Mirghani, H.; Lumbroso, J.; et al. Postradioiodine treatment whole-body scan in the era of 18-fluorodeoxyglucose positron emission tomography for differentiated thyroid carcinoma with elevated serum thyroglobulin levels. Thyroid 2012, 22, 832–838. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Lee, S.W.; Pak, K.; Shim, S.R. Diagnostic performance of PET in thyroid cancer with elevated anti-Tg Ab. Endocr. Relat. Cancer 2018, 25, 643–652. [Google Scholar] [CrossRef] [PubMed]
- Lamartina, L.; Borget, I.; Mirghani, H.; Al Ghuzlan, A.; Berdelou, A.; Bidault, F.; Deandreis, D.; Baudin, E.; Travagli, J.-P.; Schlumberger, M.; et al. Surgery for neck recurrence of differentiated thyroid cancer: Outcomes and risk factors. J. Clin. Endocrinol. Metab. 2017, 102, 1020–1031. [Google Scholar] [CrossRef] [PubMed]
- Pacini, F.; Cetani, F.; Miccoli, P.; Mancusi, F.; Ceccarelli, C.; Lippi, F.; Martino, E.; Pinchera, A. Outcome of 309 patients with metastatic differentiated thyroid carcinoma treated with radioiodine. World J. Surg. 1994, 18, 600–604. [Google Scholar] [CrossRef]
- Terroir, M.; Borget, I.; Bidault, F.; Ricard, M.; Deschamps, F.; Hartl, D.; Tselikas, L.; Dercle, L.; Lumbroso, J.; Baudin, E.; et al. The intensity of 18FDG uptake does not predict tumor growth in patients with metastatic differentiated thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 638–646. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).