
Combination of Pembrolizumab with Electrochemotherapy in Cutaneous Metastases from Melanoma: A Comparative Retrospective Study from the InspECT and Slovenian Cancer Registry

 ,
,  ,
,  , , , and
, , , and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. InspECT Database
2.3. Clinical Registry of Skin Melanoma (CRRS)
2.4. Treatment
2.5. Response Evaluation
2.6. Statistical Analysis
3. Results
3.1. Patients
3.2. Toxicity
3.3. Local Tumor Response
3.4. Systemic Response
3.5. Survival
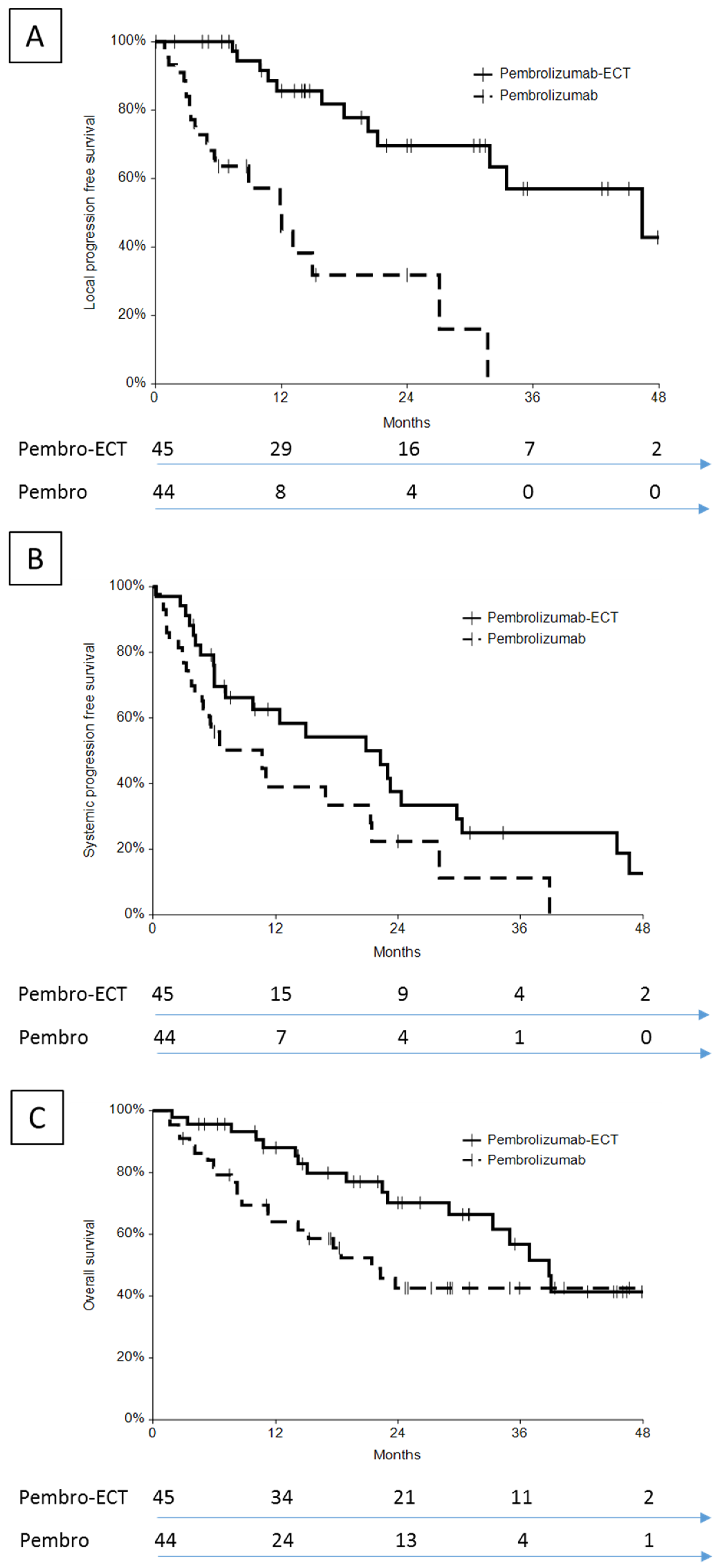
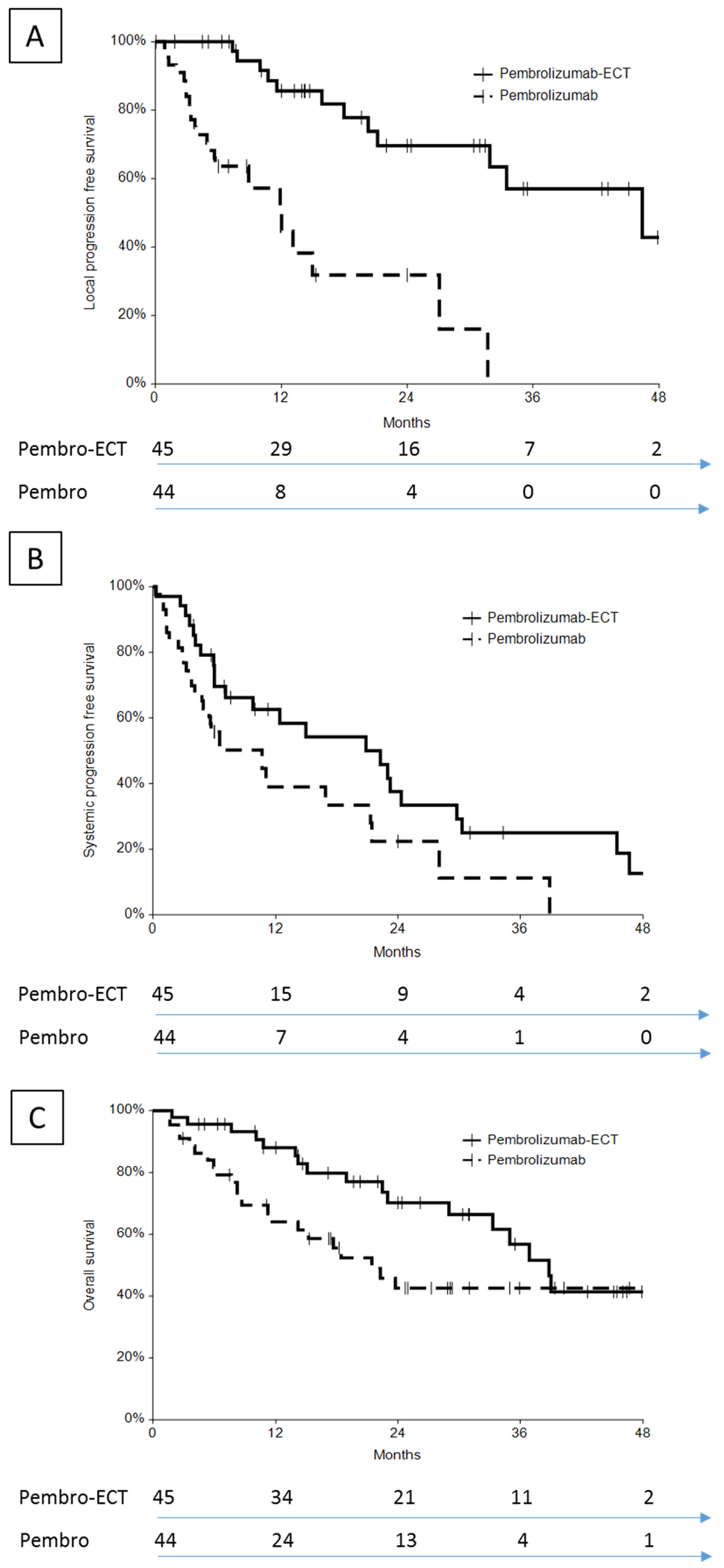
3.5.1. Local Control
3.5.2. Systemic Control
3.5.3. Overall Survival
4. Discussion
4.1. Selection of Patients
4.2. Safety
4.3. Local Effectiveness
4.4. Does ECT Contribute to a Systemic Response?
4.5. Why and How to Combine Local Therapies with Immunotherapy
4.6. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Littman, D.R. Releasing the Brakes on Cancer Immunotherapy. Cell 2015, 162, 1186–1190. [Google Scholar] [CrossRef] [Green Version]
- du Rusquec, P.; de Calbiac, O.; Robert, M.; Campone, M.; Frenel, J.S. Clinical Utility of Pembrolizumab in the Management of Advanced Solid Tumors: An Evidence-Based Review on the Emerging New Data. CMAR 2019, 11, 4297–4312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thompson, J.A. Major Changes in Systemic Therapy for Advanced Melanoma. J. Natl. Compr. Canc. Netw. 2016, 14, 638–640. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, A.; Saleh, S. Checkpoint Inhibitors for Malignant Melanoma: A Systematic Review and Meta-Analysis. CCID 2017, 10, 325–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friedlander, P. The Use of Baseline Tumor Size to Prognosticate Overall Survival in Stage IV Melanoma Patients Treated with the PD-1 Inhibitor Pembrolizumab. Ann. Transl. Med. 2019, 7, S24. [Google Scholar] [CrossRef] [PubMed]
- Savoia, P.; Fava, P.; Osella-Abate, S.; Nardò, T.; Comessatti, A.; Quaglino, P.; Bernengo, M.G. Melanoma of Unknown Primary Site: A 33-Year Experience at the Turin Melanoma Centre. Melanoma Res. 2010, 20, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J.F.; PMSaw, R.; Dalton, J.M.; Stretch, J.R.; Spillane, A.J.; Osborne, N.S.; Williams, G.J.; Lo, S.N. Treatment of In-Transit Melanoma Metastases Using Intralesional PV-10. Melanoma Res. 2021, 31, 232–241. [Google Scholar] [CrossRef]
- Read, R.L.; Thompson, J.F. The Role of Regional Chemotherapy for Advanced Limb Melanoma in the Era of Potentially Effective Systemic Therapies. Melanoma Res. 2021, 31, 290–297. [Google Scholar] [CrossRef]
- Carr, M.J.; Sun, J.; Kroon, H.M.; Miura, J.T.; Beasley, G.M.; Farrow, N.E.; Mosca, P.J.; Lowe, M.C.; Farley, C.R.; Kim, Y.; et al. Oncologic Outcomes After Isolated Limb Infusion for Advanced Melanoma: An International Comparison of the Procedure and Outcomes Between the United States and Australia. Ann. Surg. Oncol. 2020, 27, 5107–5118. [Google Scholar] [CrossRef]
- Ressler, J.M.; Karasek, M.; Koch, L.; Silmbrod, R.; Mangana, J.; Latifyan, S.; Aedo-Lopez, V.; Kehrer, H.; Weihsengruber, F.; Koelblinger, P.; et al. Real-Life Use of Talimogene Laherparepvec (T-VEC) in Melanoma Patients in Centers in Austria, Switzerland and Germany. J. Immunother. Cancer 2021, 9, e001701. [Google Scholar] [CrossRef]
- Troiani, T.; De Falco, V.; Napolitano, S.; Trojaniello, C.; Ascierto, P.A. How We Treat Locoregional Melanoma. ESMO Open 2021, 6, 100136. [Google Scholar] [CrossRef]
- Zaremba, A.; Philip, M.; Hassel, J.C.; Glutsch, V.; Fiocco, Z.; Loquai, C.; Rafei-Shamsabadi, D.; Gutzmer, R.; Utikal, J.; Haferkamp, S.; et al. Clinical Characteristics and Therapy Response in Unresectable Melanoma Patients Stage IIIB-IIID with in-Transit and Satellite Metastases. Eur. J. Cancer 2021, 152, 139–154. [Google Scholar] [CrossRef]
- Spratt, D.E.; Gordon Spratt, E.A.; Wu, S.; DeRosa, A.; Lee, N.Y.; Lacouture, M.E.; Barker, C.A. Efficacy of Skin-Directed Therapy for Cutaneous Metastases from Advanced Cancer: A Meta-Analysis. JCO 2014, 32, 3144–3155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campana, L.G.; Miklavčič, D.; Bertino, G.; Marconato, R.; Valpione, S.; Imarisio, I.; Dieci, M.V.; Granziera, E.; Cemazar, M.; Alaibac, M.; et al. Electrochemotherapy of Superficial Tumors—Current Status. Semin. Oncol. 2019, 46, 173–191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michielin, O.; van Akkooi, A.; Lorigan, P.; Ascierto, P.A.; Dummer, R.; Robert, C.; Arance, A.; Blank, C.U.; Chiarion Sileni, V.; Donia, M.; et al. ESMO Consensus Conference Recommendations on the Management of Locoregional Melanoma: Under the Auspices of the ESMO Guidelines Committee. Ann. Oncol. 2020, 31, 1449–1461. [Google Scholar] [CrossRef] [PubMed]
- Kunte, C.; Letulé, V.; Gehl, J.; Dahlstroem, K.; Curatolo, P.; Rotunno, R.; Muir, T.; Occhini, A.; Bertino, G.; Powell, B.; et al. Electrochemotherapy in the Treatment of Metastatic Malignant Melanoma: A Prospective Cohort Study by InspECT. Br. J. Dermatol. 2017, 176, 1475–1485. [Google Scholar] [CrossRef]
- Quaglino, P.; Mortera, C.; Osella-Abate, S.; Barberis, M.; Illengo, M.; Rissone, M.; Savoia, P.; Bernengo, M.G. Electrochemotherapy with Intravenous Bleomycin in the Local Treatment of Skin Melanoma Metastases. Ann. Surg. Oncol. 2008, 15, 2215–2222. [Google Scholar] [CrossRef] [PubMed]
- Campana, L.G.; Valpione, S.; Mocellin, S.; Sundararajan, R.; Granziera, E.; Sartore, L.; Chiarion-Sileni, V.; Rossi, C.R. Electrochemotherapy for Disseminated Superficial Metastases from Malignant Melanoma. Br. J. Surg. 2012, 99, 821–830. [Google Scholar] [CrossRef] [PubMed]
- Clover, A.J.P.; de Terlizzi, F.; Bertino, G.; Curatolo, P.; Odili, J.; Campana, L.G.; Kunte, C.; Muir, T.; Brizio, M.; Sersa, G.; et al. Electrochemotherapy in the Treatment of Cutaneous Malignancy: Outcomes and Subgroup Analysis from the Cumulative Results from the Pan-European International Network for Sharing Practice in Electrochemotherapy Database for 2482 Lesions in 987 Patients (2008–2019). Eur. J. Cancer 2020, 138, 30–40. [Google Scholar] [CrossRef]
- Calvet, C.Y.; Mir, L.M. The Promising Alliance of Anti-Cancer Electrochemotherapy with Immunotherapy. Cancer Metastasis Rev. 2016, 35, 165–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sersa, G.; Ursic, K.; Cemazar, M.; Heller, R.; Bosnjak, M.; Campana, L.G. Biological Factors of the Tumour Response to Electrochemotherapy: Review of the Evidence and a Research Roadmap. Eur. J. Surg. Oncol. 2021, 47, 1836–1846. [Google Scholar] [CrossRef] [PubMed]
- Sersa, G.; Teissie, J.; Cemazar, M.; Signori, E.; Kamensek, U.; Marshall, G.; Miklavcic, D. Electrochemotherapy of Tumors as in Situ Vaccination Boosted by Immunogene Electrotransfer. Cancer Immunol. Immunother. 2015, 64, 1315–1327. [Google Scholar] [CrossRef] [PubMed]
- Ursic, K.; Kos, S.; Kamensek, U.; Cemazar, M.; Miceska, S.; Markelc, B.; Bucek, S.; Staresinic, B.; Kloboves Prevodnik, V.; Heller, R.; et al. Potentiation of Electrochemotherapy Effectiveness by Immunostimulation with IL-12 Gene Electrotransfer in Mice Is Dependent on Tumor Immune Status. J. Control. Release 2021, 332, 623–635. [Google Scholar] [CrossRef] [PubMed]
- Heppt, M.V.; Eigentler, T.K.; Kähler, K.C.; Herbst, R.A.; Göppner, D.; Gambichler, T.; Ulrich, J.; Dippel, E.; Loquai, C.; Schell, B.; et al. Immune Checkpoint Blockade with Concurrent Electrochemotherapy in Advanced Melanoma: A Retrospective Multicenter Analysis. Cancer Immunol. Immunother. 2016, 65, 951–959. [Google Scholar] [CrossRef]
- Brizio, M.; Ribero, S.; Campana, L.G.; Clover, A.J.P.; Gehl, J.; Kunte, C.; De Terlizzi, F.; Quaglino, P. International Network for Sharing Practices on Electrochemotherapy (InspECT): An Integrative Patients Treatment Consortium. In Handbook of Electroporation; Miklavcic, D., Ed.; Springer: Cham, Germany, 2016; pp. 1–18. ISBN 978-3-319-26779-1. [Google Scholar]
- Gehl, J.; Sersa, G.; Matthiessen, L.W.; Muir, T.; Soden, D.; Occhini, A.; Quaglino, P.; Curatolo, P.; Campana, L.G.; Kunte, C.; et al. Updated Standard Operating Procedures for Electrochemotherapy of Cutaneous Tumours and Skin Metastases. Acta Oncol. 2018, 57, 874–882. [Google Scholar] [CrossRef]
- Matthiessen, L.W.; Chalmers, R.L.; Sainsbury, D.C.G.; Veeramani, S.; Kessell, G.; Humphreys, A.C.; Bond, J.E.; Muir, T.; Gehl, J. Management of Cutaneous Metastases Using Electrochemotherapy. Acta Oncol. 2011, 50, 621–629. [Google Scholar] [CrossRef]
- Marty, M.; Sersa, G.; Garbay, J.R.; Gehl, J.; Collins, C.G.; Snoj, M.; Billard, V.; Geertsen, P.F.; Larkin, J.O.; Miklavcic, D.; et al. Electrochemotherapy—An Easy, Highly Effective and Safe Treatment of Cutaneous and Subcutaneous Metastases: Results of ESOPE (European Standard Operating Procedures of Electrochemotherapy) Study. Eur. J. Cancer Suppl. 2006, 4, 3–13. [Google Scholar] [CrossRef]
- Somarouthu, B.; Lee, S.I.; Urban, T.; Sadow, C.A.; Harris, G.J.; Kambadakone, A. Immune-Related Tumour Response Assessment Criteria: A Comprehensive Review. BJR 2018, 91, 20170457. [Google Scholar] [CrossRef] [PubMed]
- Goggins, C.A.; Khachemoune, A. The Use of Electrochemotherapy in Combination with Immunotherapy in the Treatment of Metastatic Melanoma: A Focused Review. Int. J. Dermatol. 2019, 58, 865–870. [Google Scholar] [CrossRef] [PubMed]
- Brizio, M.; Fava, P.; Astrua, C.; Cavaliere, G.; Savoia, P. Complete Regression of Melanoma Skin Metastases after Electrochemotherapy plus Ipilimumab Treatment: An Unusual Clinical Presentation. Eur. J. Dermatol. 2015, 25, 271–272. [Google Scholar] [CrossRef] [PubMed]
- Mozzillo, N.; Simeone, E.; Benedetto, L.; Curvietto, M.; Giannarelli, D.; Gentilcore, G.; Camerlingo, R.; Capone, M.; Madonna, G.; Festino, L.; et al. Assessing a Novel Immuno-Oncology-Based Combination Therapy: Ipilimumab plus Electrochemotherapy. OncoImmunology 2015, 4, e1008842. [Google Scholar] [CrossRef] [PubMed]
- Karaca, B.; Yayla, G.; Erdem, M.; Gürler, T. Electrochemotherapy with Anti-PD-1 Treatment Induced Durable Complete Response in Heavily Pretreated Metastatic Melanoma Patient. Anti Cancer Drugs 2018, 29, 190–196. [Google Scholar] [CrossRef]
- Delaunay, M.; Prévot, G.; Collot, S.; Guilleminault, L.; Didier, A.; Mazières, J. Management of Pulmonary Toxicity Associated with Immune Checkpoint Inhibitors. Eur. Respir. Rev. 2019, 28, 190012. [Google Scholar] [CrossRef] [PubMed]
- Postow, M.A.; Chesney, J.; Pavlick, A.C.; Robert, C.; Grossmann, K.; McDermott, D.; Linette, G.P.; Meyer, N.; Giguere, J.K.; Agarwala, S.S.; et al. Nivolumab and Ipilimumab versus Ipilimumab in Untreated Melanoma. N. Engl. J. Med. 2015, 372, 2006–2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Algazi, A.P.; Twitty, C.G.; Tsai, K.K.; Le, M.; Pierce, R.; Browning, E.; Hermiz, R.; Canton, D.A.; Bannavong, D.; Oglesby, A.; et al. Phase II Trial of IL-12 Plasmid Transfection and PD-1 Blockade in Immunologically Quiescent Melanoma. Clin. Cancer Res. 2020, 26, 2827–2837. [Google Scholar] [CrossRef] [PubMed]
- Greaney, S.K.; Algazi, A.P.; Tsai, K.K.; Takamura, K.T.; Chen, L.; Twitty, C.G.; Zhang, L.; Paciorek, A.; Pierce, R.H.; Le, M.H.; et al. Intratumoral Plasmid IL12 Electroporation Therapy in Patients with Advanced Melanoma Induces Systemic and Intratumoral T-Cell Responses. Cancer Immunol. Res. 2020, 8, 246–254. [Google Scholar] [CrossRef] [Green Version]
- Bruni, D.; Angell, H.K.; Galon, J. The Immune Contexture and Immunoscore in Cancer Prognosis and Therapeutic Efficacy. Nat. Rev. Cancer 2020, 20, 662–680. [Google Scholar] [CrossRef]
- Galon, J.; Lanzi, A. Immunoscore and Its Introduction in Clinical Practice. Q. J. Nucl. Med. Mol. Imaging 2020, 64. [Google Scholar] [CrossRef]
- Duan, Q.; Zhang, H.; Zheng, J.; Zhang, L. Turning Cold into Hot: Firing up the Tumor Microenvironment. Trends Cancer 2020, 6, 605–618. [Google Scholar] [CrossRef] [PubMed]
- De Guillebon, E.; Dardenne, A.; Saldmann, A.; Séguier, S.; Tran, T.; Paolini, L.; Lebbe, C.; Tartour, E. Beyond the Concept of Cold and Hot Tumors for the Development of Novel Predictive Biomarkers and the Rational Design of Immunotherapy Combination. Int. J. Cancer 2020, 147, 1509–1518. [Google Scholar] [CrossRef]
- Bonaventura, P.; Shekarian, T.; Alcazer, V.; Valladeau-Guilemond, J.; Valsesia-Wittmann, S.; Amigorena, S.; Caux, C.; Depil, S. Cold Tumors: A Therapeutic Challenge for Immunotherapy. Front. Immunol. 2019, 10, 168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calvet, C.Y.; Famin, D.; André, F.M.; Mir, L.M. Electrochemotherapy with Bleomycin Induces Hallmarks of Immunogenic Cell Death in Murine Colon Cancer Cells. OncoImmunology 2014, 3, e28131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Gennaro, P.; Gerlini, G.; Urso, C.; Sestini, S.; Brandani, P.; Pimpinelli, N.; Borgognoni, L. CD4+FOXP3+ T Regulatory Cells Decrease and CD3+CD8+ T Cells Recruitment in TILs from Melanoma Metastases after Electrochemotherapy. Clin. Exp. Metastasis 2016, 33, 787–798. [Google Scholar] [CrossRef] [PubMed]
- Lo, M.C.; Garioch, J.; Moncrieff, M.D. Sequencing in Management of In-Transit Melanoma Metastasis: Diphencyprone versus Isolate Limb Infusion. J. Plast. Reconstr. Aesthetic Surg. 2020, 73, 1263–1267. [Google Scholar] [CrossRef] [PubMed]
- Simioni, A.; Valpione, S.; Granziera, E.; Rossi, C.R.; Cavallin, F.; Spina, R.; Sieni, E.; Aliberti, C.; Stramare, R.; Campana, L.G. Ablation of Soft Tissue Tumours by Long Needle Variable Electrode-Geometry Electrochemotherapy: Final Report from a Single-Arm, Single-Centre Phase-2 Study. Sci. Rep. 2020, 10, 2291. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Variable | Pembrolizumab–ECT | Pembrolizumab | ECT | p |
|---|---|---|---|---|
| No. | 45 | 44 | 41 | |
| Sex | 0.723 | |||
| M | 25 (56%) | 22 (50%) | 24 (60%) | |
| F | 20 (44%) | 22 (50%) | 17 (40%) | |
| Age | 0.132 | |||
| median (range) | 67 (32–87) | 66 (28–82) | 70 (44–85) | |
| Disease stage ° | 0.285 | |||
| IIIC | 16 (35.6%) | 9 (20.5%) | 12 (29.3%) | |
| IV | 29 (64.4%) † | 35 (79.5%) ‡ | 29 (70.7%) | |
| Previous local therapies | <0.001 | |||
| No | 15 (33.3%) | 27 (61.4%) | 5 (12.2%) | |
| Yes | 30 (66.7%) | 17 (38.6%) | 36 (73.2%) | |
| Surg | 14 (31.1%) | 1 (2.3%) | 29 (70.7%) | |
| Surg + RT | 11 (24.4%) | 3 (6.8%) | 4 (9.8%) | |
| Surg + ILP | 4 (8.8%) | 1 (2.3%) | 0 (0%) | |
| Surg + RT + ILP | 0 (0%) | 0 (0%) | 1 (2.4%) | |
| Other | 1 (2.2%) * | 12 (27.3%) ** | 2 (4.9%) *** | |
| Previous Systemic Therapies | 0.004 | |||
| No | 15 (33.3%) | 30 (68.2%) | 19 (46.3%) | |
| Yes | 30 (66.6%) | 14 (31.8%) | 22 (53.7%) | |
| CT | 3 (6.7%) | 1 ((2.3%) | 7 (17.1%) | |
| TT | 2 (4.4%) | 10 (22.7%) | 3 (7.3%) | |
| IT | 14 (31.1%) | 3 (6.8%) | 8 (19.5%) | |
| CT + IT | 6 (13.3%) | 0 (0%) | 1 (2.4%) | |
| CT + TT | 0 (0%) | 0 (0%) | 1 (2.4%) | |
| IT + TT | 3 (6.7%) | 0 (0%) | 1 (2.4%) | |
| CT + IT + TT | 2 (4.4%) | 0 (0%) | 1 (2.4%) | |
| ECOG PS | 0.259 | |||
| 0 | 28 (62.2%) | 20 (45.5%) | 28 (68.3%) | |
| 1 | 11 (24.4%) | 15 (34.1%) | 7 (17.1%) | |
| 2 | 6 (13.3%) | 9 (20.5%) | 6 (14.6%) | |
| Tumor size | 0.187 | |||
| <1 cm | 3 (6.7%) | 7 (15.9%) | 3 (7.3%) | |
| 1–3 cm | 22 (48.9%) | 27 (61.4%) | 22 (53.7%) | |
| >3 cm | 20 (44.4%) | 10 (22.7%) | 16 (39.0%) | |
| Anatomical location | 0.057 | |||
| Head/Neck | 6 (13.3%) | 8 (18.2%) | 8 (19.5%) | |
| Chest | 4 (8.9%) | 16 (36.4%) | 3 (7.3%) | |
| Abdomen | 2 (4.4%) | 1 (2.3%) | 1 (2.4%) | |
| Back | 4 (8.9%) | 4 (9.1%) | 6 (14.6%) | |
| Perigenital | 2 (4.4%) | 0 (0%) | 3 (7.3%) | |
| Gynecological | 1 (2.2%) | 0 (0%) | 0 (0%) | |
| Upper limb | 2 (4.4%) | 2 (4.5%) | 1 (2.4%) | |
| Lower limb | 24 (53.3%) | 13 (29.5%) | 19 (46.3%) | |
| No. of ECT sessions | 0.175 | |||
| 1 | 28 | - | 33 | |
| 2 | 13 | - | 6 | |
| 3 | 4 | - | 2 |
| Toxicity | Pembrolizumab–ECT (n = 45) | Pembrolizumab (n = 44) | ECT (n = 41) | p |
|---|---|---|---|---|
| Odor | 5 (11%) | 0 | 3 (7%) | 0.716 |
| Suppuration | 8 (18%) | 0 | 4 (10%) | 0.358 |
| Ulceration | 9 (20%) | 7 (16%) | 12 (29%) | 0.311 |
| Hyperpigmentation | 9 (20%) | 0 | 9 (22%) | 1.000 |
| Nausea | 7 (16%) | 0 | 0 | 0.012 |
| Pneumonitis | 2 (4%) | 4 (9%) | 0 | 0.434 |
| Pruritus | 2 (4%) | 1 (2%) | 0 | 1.000 |
| Hypothyroidism | 1 (2%) | 2 (5%) | 0 | 0.616 |
| Pancreatitis | 0 | 1 (2%) | 0 | 0.494 |
| Colitis | 1 (2%) | 1 (2%) | 0 | 1.000 |
| Vitiligo | 0 | 1 (2%) | 0 | 0.494 |
| Response | Pembrolizumab–ECT | Pembrolizumab | ECT | p |
|---|---|---|---|---|
| CR | 22 (48.9%) | 14 (31.8%) | 18 (43.9%) | |
| PR | 13 (28.9% | 3 (6.8%) | 15 (36.6%) | |
| SD | 7 (15.6%) | 13 (29.5%) | 7 (17.1%) | |
| PD | 3 (6.7%) | 12 (27.3%) | 1 (2.4%) | |
| NE | 0 (0%) | 2 (4.5%) | 0 (0%) | |
| OR | 35 (77.8%) | 17 (38.6%) | 33 (80.5%) | <0.001 |
| No of pts with local progression | 12 (26.7%) | 23 (56.1%) | 11 (26.2%) | 0.016 |
| Time to local progression (months) | 20 ± 12 | 7 ± 8 | 5 ± 4 | <0.001 |
| Time to disease progression (months) | 22 ± 15 | 8 ± 7 | - | <0.001 |
| Response | Pembrolizumab–ECT | Pembrolizumab | p |
|---|---|---|---|
| CR | 5 (11.1%) | 9 (20.5%) | |
| PR | 6 (13.3%) | 2 (4.5%) | |
| SD | 10 (22.2%) | 3 (6.8%) | |
| PD | 17 (37.8%) | 30 (68.2%) | |
| NA | 7 (15.6%) | 0 (0%) | |
| OR | 11 (24.4%) | 11 (25%) | 1.000 |
| No of pts in systemic progression | 24 (53.3%) | 27 (61.4%) | 0.522 |
| Time to systemic progression (months) | 17 ± 15 | 8 ± 9 | <0.001 |
| Systemic control of disease (months) | 17 ± 16 | 8 ± 8 | 0.001 |
| Pembrolizumab–ECT vs. Pembrolizumab (n = 45) (n = 44) | Kaplan–Meier | Cox Regression (with Correction for Previous Systemic Therapies) | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | RR | 95% CI | p | |
| Local PFS | 4.38 | 2.13–8.99 | <0.001 | 5.76 | 2.41–13.77 | <0.001 |
| Systemic PFS | 1.70 | 1.07–3.60 | 0.042 | 1.06 | 1.07–3.60 | 0.030 |
| OS | 1.80 | 0.95–3.40 | 0.063 | 2.02 | 1.01–4.03 | 0.046 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campana, L.G.; Peric, B.; Mascherini, M.; Spina, R.; Kunte, C.; Kis, E.; Rozsa, P.; Quaglino, P.; Jones, R.P.; Clover, A.J.P.; et al. Combination of Pembrolizumab with Electrochemotherapy in Cutaneous Metastases from Melanoma: A Comparative Retrospective Study from the InspECT and Slovenian Cancer Registry. Cancers 2021, 13, 4289. https://doi.org/10.3390/cancers13174289
Campana LG, Peric B, Mascherini M, Spina R, Kunte C, Kis E, Rozsa P, Quaglino P, Jones RP, Clover AJP, et al. Combination of Pembrolizumab with Electrochemotherapy in Cutaneous Metastases from Melanoma: A Comparative Retrospective Study from the InspECT and Slovenian Cancer Registry. Cancers. 2021; 13(17):4289. https://doi.org/10.3390/cancers13174289
Chicago/Turabian StyleCampana, Luca G., Barbara Peric, Matteo Mascherini, Romina Spina, Christian Kunte, Erika Kis, Petra Rozsa, Pietro Quaglino, Rowan Pritchard Jones, A. James P. Clover, and et al. 2021. "Combination of Pembrolizumab with Electrochemotherapy in Cutaneous Metastases from Melanoma: A Comparative Retrospective Study from the InspECT and Slovenian Cancer Registry" Cancers 13, no. 17: 4289. https://doi.org/10.3390/cancers13174289
APA StyleCampana, L. G., Peric, B., Mascherini, M., Spina, R., Kunte, C., Kis, E., Rozsa, P., Quaglino, P., Jones, R. P., Clover, A. J. P., Curatolo, P., Giorgione, R., Cemazar, M., Terlizzi, F. d., Bosnjak, M., & Sersa, G. (2021). Combination of Pembrolizumab with Electrochemotherapy in Cutaneous Metastases from Melanoma: A Comparative Retrospective Study from the InspECT and Slovenian Cancer Registry. Cancers, 13(17), 4289. https://doi.org/10.3390/cancers13174289