
Prognostic Role of Pre-Treatment [18F]FDG PET/CT in Patients with Anaplastic Thyroid Cancer

Abstract
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Study Subjects
2.2. PET/CT Imaging Protocol
2.3. PET/CT Imaging Analysis
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. PET Parameters
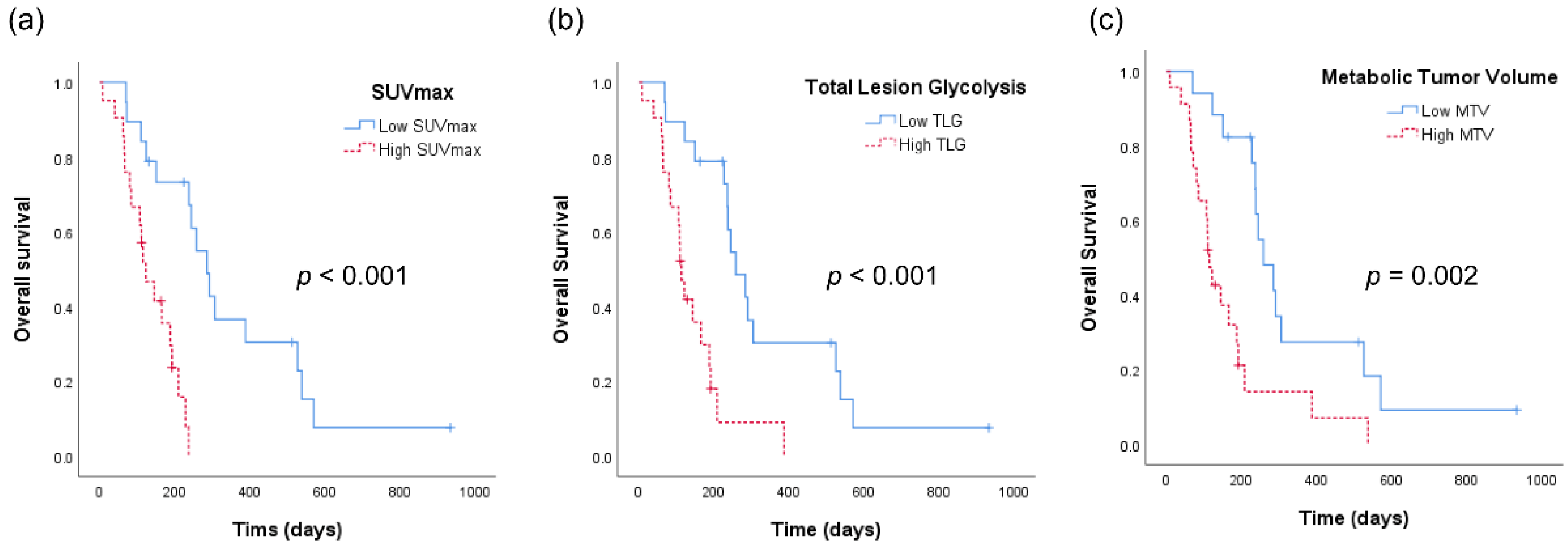
3.3. Kaplan–Meier Survival Analysis
3.4. Univariate and Multivariate Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Smallridge, R.C.; Copland, J.A. Anaplastic thyroid carcinoma: Pathogenesis and emerging therapies. Clin. Oncol. 2010, 22, 486–497. [Google Scholar] [CrossRef] [PubMed]
- Volante, M.; Lam, A.K.; Papotti, M.; Tallini, G. Molecular Pathology of Poorly Differentiated and Anaplastic Thyroid Cancer: What Do Pathologists Need to Know? Endocr. Pathol. 2021, 32, 63–76. [Google Scholar] [CrossRef]
- Ragazzi, M.; Ciarrocchi, A.; Sancisi, V.; Gandolfi, G.; Bisagni, A.; Piana, S. Update on anaplastic thyroid carcinoma: Morphological, molecular, and genetic features of the most aggressive thyroid cancer. Int. J. Endocrinol. 2014, 2014, 790834. [Google Scholar] [CrossRef] [PubMed]
- Hundahl, S.A.; Fleming, I.D.; Fremgen, A.M.; Menck, H.R. A National Cancer Data Base report on 53,856 cases of thyroid carcinoma treated in the US, 1985–1995. Cancer 1998, 83, 2638–2648. [Google Scholar] [CrossRef]
- Are, C.; Shaha, A.R. Anaplastic thyroid carcinoma: Biology, pathogenesis, prognostic factors, and treatment approaches. Ann. Surg. Oncol. 2006, 13, 453–464. [Google Scholar] [CrossRef] [PubMed]
- Cornett, W.R.; Sharma, A.K.; Day, T.A.; Richardson, M.S.; Hoda, R.S.; van Heerden, J.A.; Fernandes, J.K. Anaplastic thyroid carcinoma: An overview. Curr. Oncol. Rep. 2007, 9, 152–158. [Google Scholar] [CrossRef]
- Tuttle, R.M.; Haugen, B.; Perrier, N.D. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for Differentiated and Anaplastic Thyroid Cancer (Eighth Edition): What Changed and Why? Thyroid 2017, 27, 751–756. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Onoda, N.; Sugitani, I.; Ito, K.I.; Suzuki, A.; Higashiyama, T.; Fukumori, T.; Suganuma, N.; Masudo, K.; Nakayama, H.; Uno, A.; et al. Evaluation of the 8th Edition TNM Classification for Anaplastic Thyroid Carcinoma. Cancers 2020, 12, 552. [Google Scholar] [CrossRef]
- Smallridge, R.C.; Ain, K.B.; Asa, S.L.; Bible, K.C.; Brierley, J.D.; Burman, K.D.; Kebebew, E.; Lee, N.Y.; Nikiforov, Y.E.; Rosenthal, M.S.; et al. American Thyroid Association Guidelines for Management of Patients with Anaplastic Thyroid Cancer. Thyroid 2012, 22, 1104–1139. [Google Scholar] [CrossRef]
- Kim, T.Y.; Kim, K.W.; Jung, T.S.; Kim, J.M.; Kim, S.W.; Chung, K.W.; Kim, E.Y.; Gong, G.; Oh, Y.L.; Cho, S.Y.; et al. Prognostic factors for Korean patients with anaplastic thyroid carcinoma. Head Neck 2007, 29, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Akaishi, J.; Sugino, K.; Kitagawa, W.; Nagahama, M.; Kameyama, K.; Shimizu, K.; Ito, K.; Ito, K. Prognostic factors and treatment outcomes of 100 cases of anaplastic thyroid carcinoma. Thyroid 2011, 21, 1183–1189. [Google Scholar] [CrossRef]
- Nagaiah, G.; Hossain, A.; Mooney, C.J.; Parmentier, J.; Remick, S.C. Anaplastic thyroid cancer: A review of epidemiology, pathogenesis, and treatment. J. Oncol. 2011, 2011, 542358. [Google Scholar] [CrossRef] [PubMed]
- Kebebew, E.; Greenspan, F.S.; Clark, O.H.; Woeber, K.A.; McMillan, A. Anaplastic thyroid carcinoma. Treatment outcome and prognostic factors. Cancer 2005, 103, 1330–1335. [Google Scholar] [CrossRef]
- Besic, N.; Hocevar, M.; Zgajnar, J.; Pogacnik, A.; Grazio-Frkovic, S.; Auersperg, M. Prognostic factors in anaplastic carcinoma of the thyroid-a multivariate survival analysis of 188 patients. Langenbecks Arch. Surg. 2005, 390, 203–208. [Google Scholar] [CrossRef]
- Jiang, J.Y.; Tseng, F.Y. Prognostic factors of anaplastic thyroid carcinoma. J. Endocrinol. Investig. 2006, 29, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Kihara, M.; Miyauchi, A.; Yamauchi, A.; Yokomise, H. Prognostic factors of anaplastic thyroid carcinoma. Surg. Today 2004, 34, 394–398. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid Off. J. Am. Thyroid Assoc. 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Strobel, K.; Steinert, H.C.; Bhure, U.; Koma, A.Y.; Gassmann, N.; Stockli, S.J. Tumour thrombus in the superior vena cava from anaplastic carcinoma of the thyroid: FDG-PET/CT imaging findings. Eur. J. Nucl. Med. Mol. Imaging 2007, 34, 813. [Google Scholar] [CrossRef]
- Giannetta, E.; Isidori, A.M.; Durante, C.; Di Gioia, C.; Longo, F.; Tombolini, V.; Bulzonetti, N.; Graziadio, C.; Pofi, R.; Gianfrilli, D.; et al. Anaplastic thyroid carcinoma and foscarnet use in a multitarget treatment documented by 18F-FDG PET/CT: A case report. Medicine 2017, 96, e5621. [Google Scholar] [CrossRef]
- Iagaru, A.; McDougall, I.R. F-18 FDG PET/CT demonstration of an adrenal metastasis in a patient with anaplastic thyroid cancer. Clin. Nucl. Med. 2007, 32, 13–15. [Google Scholar] [CrossRef]
- Zweifel, M.; Stenner-Liewen, F.; Weber, A.; Samaras, P.; Zaugg, K.; Knuth, A.; Soyka, J.D. Increased bone marrow activity on F-18-FDG PET/CT in granulocyte colony stimulating factor producing anaplastic thyroid carcinoma. Clin. Nucl. Med. 2010, 35, 103–104. [Google Scholar] [CrossRef]
- Nguyen, B.D.; Ram, P.C. PET/CT staging and posttherapeutic monitoring of anaplastic thyroid carcinoma. Clin. Nucl. Med. 2007, 32, 145–149. [Google Scholar] [CrossRef] [PubMed]
- Yurkiewicz, I.R.; Ganjoo, K.N.; Iagaru, A. Anaplastic Thyroid Cancer With Extensive Skeletal Muscle Metastases on 18F-FDG PET/CT. Clin. Nucl. Med. 2018, 43, e113–e114. [Google Scholar] [CrossRef] [PubMed]
- Bogsrud, T.V.; Karantanis, D.; Nathan, M.A.; Mullan, B.P.; Wiseman, G.A.; Kasperbauer, J.L.; Reading, C.C.; Hay, I.D.; Lowe, V.J. 18F-FDG PET in the management of patients with anaplastic thyroid carcinoma. Thyroid 2008, 18, 713–719. [Google Scholar] [CrossRef]
- Khan, N.; Oriuchi, N.; Higuchi, T.; Endo, K. Review of fluorine-18-2-fluoro-2-deoxy-D-glucose positron emission tomography (FDG-PET) in the follow-up of medullary and anaplastic thyroid carcinomas. Cancer Control. 2005, 12, 254–260. [Google Scholar] [CrossRef]
- Poisson, T.; Deandreis, D.; Leboulleux, S.; Bidault, F.; Bonniaud, G.; Baillot, S.; Auperin, A.; Al Ghuzlan, A.; Travagli, J.P.; Lumbroso, J.; et al. 18F-fluorodeoxyglucose positron emission tomography and computed tomography in anaplastic thyroid cancer. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 2277–2285. [Google Scholar] [CrossRef]
- Boellaard, R.; Delgado-Bolton, R.; Oyen, W.J.; Giammarile, F.; Tatsch, K.; Eschner, W.; Verzijlbergen, F.J.; Barrington, S.F.; Pike, L.C.; Weber, W.A.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 328–354. [Google Scholar] [CrossRef]
- Contal, C.; O’Quigley, J. An application of changepoint methods in studying the effect of age on survival in breast cancer. Comput. Stat. Data Anal. 1999, 30, 253–270. [Google Scholar] [CrossRef]
- Xu, B.; Fuchs, T.; Dogan, S.; Landa, I.; Katabi, N.; Fagin, J.A.; Tuttle, R.M.; Sherman, E.; Gill, A.J.; Ghossein, R. Dissecting Anaplastic Thyroid Carcinoma: A Comprehensive Clinical, Histologic, Immunophenotypic, and Molecular Study of 360 Cases. Thyroid 2020, 30, 1505–1517. [Google Scholar] [CrossRef] [PubMed]
- Spielman, D.B.; Badhey, A.; Kadakia, S.; Inman, J.C.; Ducic, Y. Rare Thyroid Malignancies: An Overview for the Oncologist. Clin. Oncol. 2017, 29, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Weber, W.A.; Schwaiger, M.; Avril, N. Quantitative assessment of tumor metabolism using FDG-PET imaging. Nucl. Med. Biol. 2000, 27, 683–687. [Google Scholar] [CrossRef]
- Torizuka, T.; Tamaki, N.; Inokuma, T.; Magata, Y.; Sasayama, S.; Yonekura, Y.; Tanaka, A.; Yamaoka, Y.; Yamamoto, K.; Konishi, J. In vivo assessment of glucose metabolism in hepatocellular carcinoma with FDG-PET. J. Nucl. Med. 1995, 36, 1811–1817. [Google Scholar] [PubMed]
- Weber, W.A.; Ziegler, S.I.; Thodtmann, R.; Hanauske, A.R.; Schwaiger, M. Reproducibility of metabolic measurements in malignant tumors using FDG PET. J. Nucl. Med. 1999, 40, 1771–1777. [Google Scholar]
- Pauwels, E.K.; Ribeiro, M.J.; Stoot, J.H.; McCready, V.R.; Bourguignon, M.; Maziere, B. FDG accumulation and tumor biology. Nucl. Med. Biol. 1998, 25, 317–322. [Google Scholar] [CrossRef]
- Fathinul, F.; Nordin, A.J.; Lau, W.F. 18[F]FDG-PET/CT is a useful molecular marker in evaluating tumour aggressiveness: A revised understanding of an in-vivo FDG-PET imaging that alludes the alteration of cancer biology. Cell Biochem. Biophys. 2013, 66, 37–43. [Google Scholar] [CrossRef][Green Version]
- Samih, N.; Hovsepian, S.; Notel, F.; Prorok, M.; Zattara-Cannoni, H.; Mathieu, S.; Lombardo, D.; Fayet, G.; El-Battari, A. The impact of N- and O-glycosylation on the functions of Glut-1 transporter in human thyroid anaplastic cells. Biochim. Biophys. Acta 2003, 1621, 92–101. [Google Scholar] [CrossRef]
- Haddad, R.I.; Lydiatt, W.M.; Ball, D.W.; Busaidy, N.L.; Byrd, D.; Callender, G.; Dickson, P.; Duh, Q.-Y.; Ehya, H.; Haymart, M.; et al. Anaplastic Thyroid Carcinoma, Version 2.2015. J. Natl. Compr. Cancer Netw. 2015, 13, 1140–1150. [Google Scholar] [CrossRef]
- Roche, B.; Larroumets, G.; Dejax, C.; Kwiatkowsi, F.; Desbiez, F.; Thieblot, P.; Tauveron, I. Epidemiology, clinical presentation, treatment and prognosis of a regional series of 26 anaplastic thyroid carcinomas (ATC). Comparison with the literature. Ann. Endocrinol. 2010, 71, 38–45. [Google Scholar] [CrossRef]
- Keutgen, X.M.; Sadowski, S.M.; Kebebew, E. Management of anaplastic thyroid cancer. Gland Surg. 2015, 4, 44–51. [Google Scholar] [CrossRef]
- Bible, K.C.; Kebebew, E.; Brierley, J.; Brito, J.P.; Cabanillas, M.E.; Clark, T.J., Jr.; Di Cristofano, A.; Foote, R.; Giordano, T.; Kasperbauer, J.; et al. 2021 American Thyroid Association Guidelines for Management of Patients with Anaplastic Thyroid Cancer. Thyroid 2021, 31, 337–386. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Characteristics | Value | Percent |
|---|---|---|
| Total number of patients | 40 | 100% |
| Sex (female) | 20 | 50% |
| Age (year, mean) | 67.5 ± 9.9 | |
| Tumor size (cm, mean) | 5.3 ± 2.2 | |
| Stage * | ||
| IVA | 4 | 10% |
| IVB | 7 | 17% |
| IVC | 29 | 73% |
| Distant metastasis | ||
| Distant node | 22 | 55% |
| Lung | 26 | 65% |
| Bone | 7 | 18% |
| Brain | 2 | 5% |
| Treatment | ||
| No treatment | 1 | 3% |
| Surgery | 13 | 33% |
| CTx | 34 | 85% |
| RTx | 31 | 78% |
| CTx + RTx | 22 | 55% |
| Multimodality Tx | 35 | 88% |
| Survival | ||
| 1-year OS | 17.5% | |
| Mean OS (month) | 7.1 | |
| PET parameters (mean) | ||
| SUVmax | 20.7 ± 12.7 | |
| SUVpeak | 17.9 ± 10.1 | |
| MTV | 88.7 ± 82.1 | |
| TLG | 843.0 ± 940.7 |
| Univariate Analysis | Multivariate Analysis (MTV Model) | Multivariate Analysis (TLG Model) | ||||
|---|---|---|---|---|---|---|
| Patient Characteristics | HRs (95% CIs) | pValue | HRs (95% CIs) | pValue | HRs (95% CIs) | pValue |
| Sex (Female) | 2.929 (1.337–6.417) | 0.006 | 1.032 (0.417–2.555) | 0.945 | 1.038 (0.419–2.570) | 0.936 |
| Age (>64 years) | 1.978 (0.937–4.173) | 0.074 | ||||
| Tumor characteristics | ||||||
| Tumor size (>4.7 cm) | 2.946 (1.344–6.460) | 0.007 | 1.854 (0.780–4.410) | 0.163 | 1.844 (0.796–4.271) | 0.153 |
| Association with differentiated cancer | 0.543 (0.237–1.245) | 0.149 | ||||
| Capsular invasion | 1.127 (0.309–4.108) | 0.856 | ||||
| Local extension | 4.999 (1.479–16.897) | 0.010 | 3.720 (0.946–14.634) | 0.060 | 3.343 (0.846–13.203) | 0.085 |
| Lymph node metastasis | 1.931 (0.670–5.562) | 0.223 | ||||
| Distant metastasis | 2.270 (1.078–4.779) | 0.031 | 2.222 (0.957–5.160) | 0.063 | 2.276 (0.997–5.194) | 0.051 |
| PET parameters | ||||||
| High SUVmax | 6.558 (2.319–18.546) | <0.001 | 5.105 (1.489–17.508) | 0.010 | 4.673 (1.325–16.484) | 0.017 |
| High MTV | 3.207 (1.516–6.781) | 0.002 | 1.309 (0.474–3.611) | 0.603 | ||
| High TLG | 4.239 (1.903–9.441) | <0.001 | 1.515 (0.518–4.425) | 0.448 | ||
| Treatment | ||||||
| Surgery | 0.459 (0.207–1.015) | 0.054 | ||||
| R1 resection | 3.198 (0.283–36.091) | 0.347 | ||||
| CTx | 1.360 (0.411–4.500) | 0.615 | ||||
| RTx | 0.891 (0.339–2.341) | 0.815 | ||||
| Multimodality Tx | 0.954 (0.363–2.508) | 0.924 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.J.; Chang, H.-S.; Ryu, Y.H. Prognostic Role of Pre-Treatment [18F]FDG PET/CT in Patients with Anaplastic Thyroid Cancer. Cancers 2021, 13, 4228. https://doi.org/10.3390/cancers13164228
Kim HJ, Chang H-S, Ryu YH. Prognostic Role of Pre-Treatment [18F]FDG PET/CT in Patients with Anaplastic Thyroid Cancer. Cancers. 2021; 13(16):4228. https://doi.org/10.3390/cancers13164228
Chicago/Turabian StyleKim, Hyun Jeong, Hang-Seok Chang, and Young Hoon Ryu. 2021. "Prognostic Role of Pre-Treatment [18F]FDG PET/CT in Patients with Anaplastic Thyroid Cancer" Cancers 13, no. 16: 4228. https://doi.org/10.3390/cancers13164228
APA StyleKim, H. J., Chang, H.-S., & Ryu, Y. H. (2021). Prognostic Role of Pre-Treatment [18F]FDG PET/CT in Patients with Anaplastic Thyroid Cancer. Cancers, 13(16), 4228. https://doi.org/10.3390/cancers13164228