
Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Simple Summary
Abstract
1. Introduction
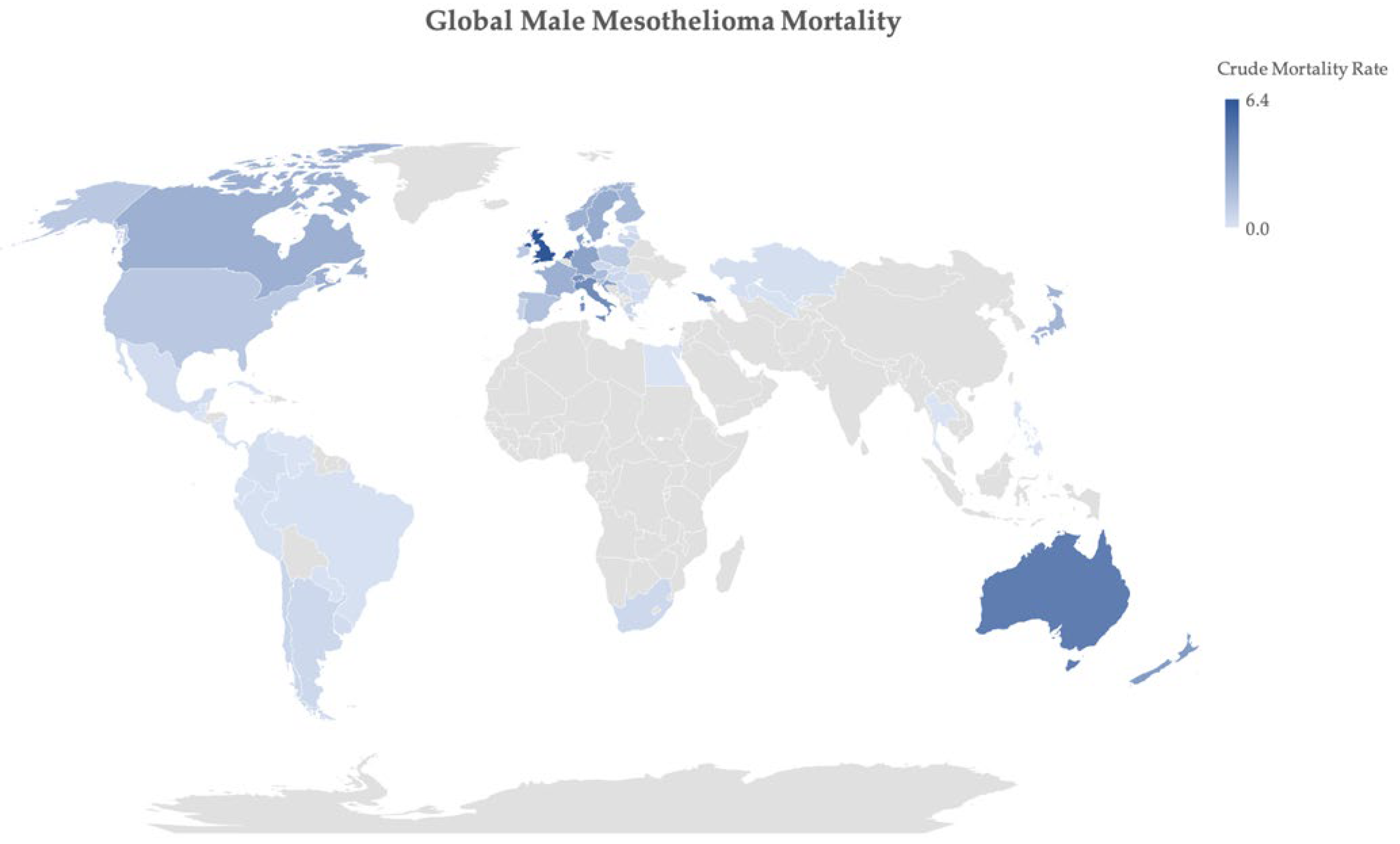
2. Epidemiology of Mesothelioma
3. Histopathology
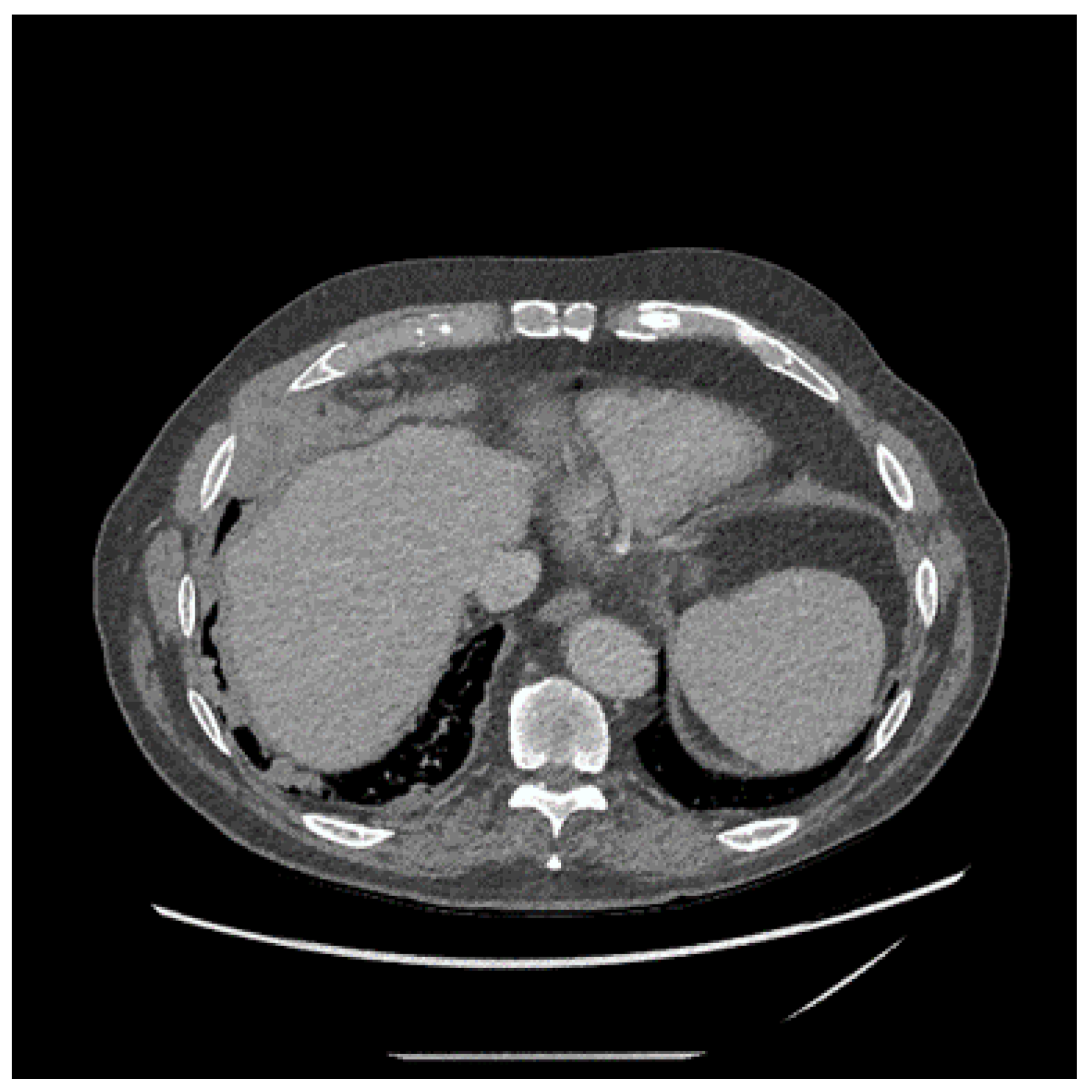
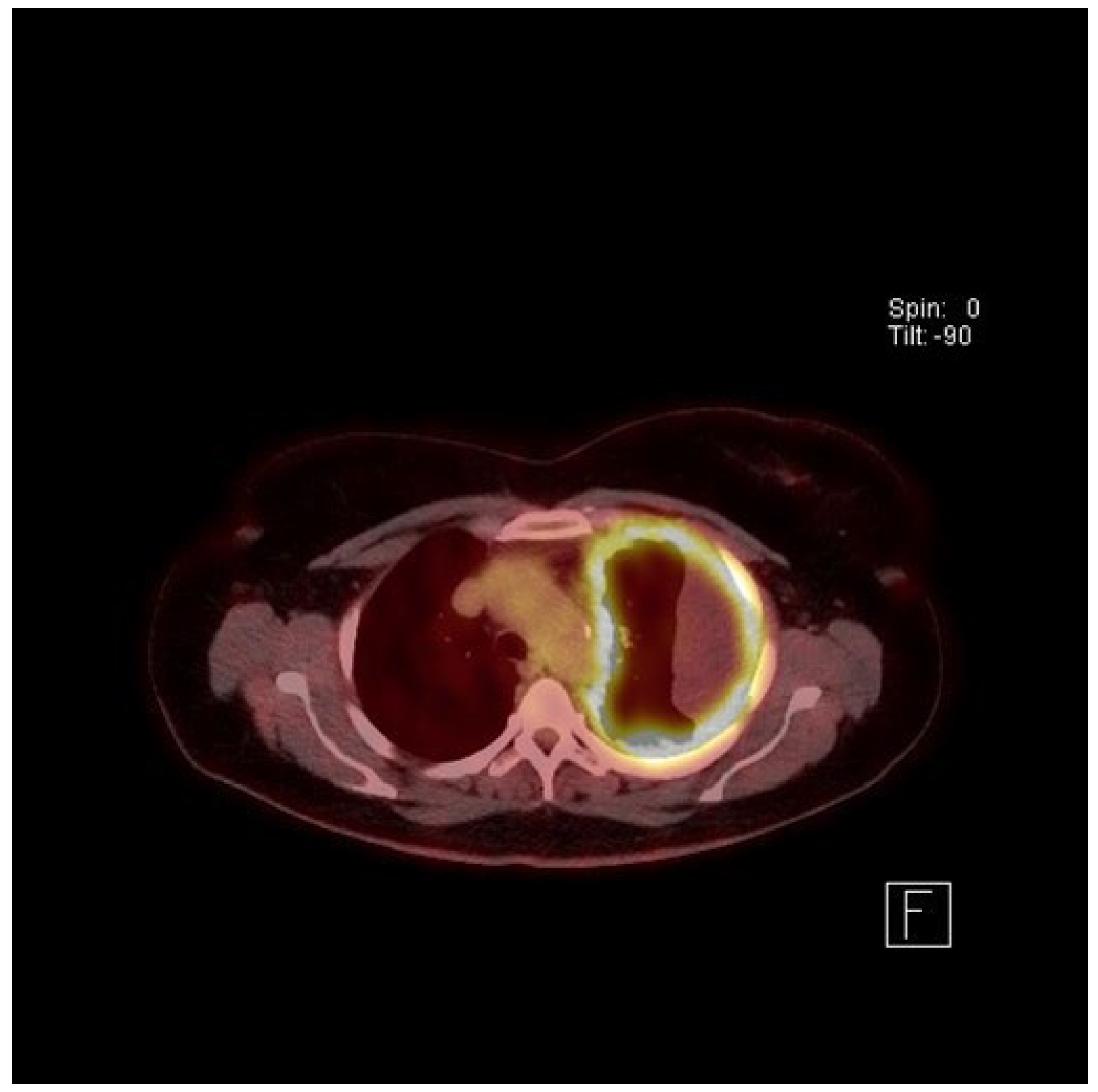
4. Clinical Presentation and Investigations
5. Treatment of Mesothelioma
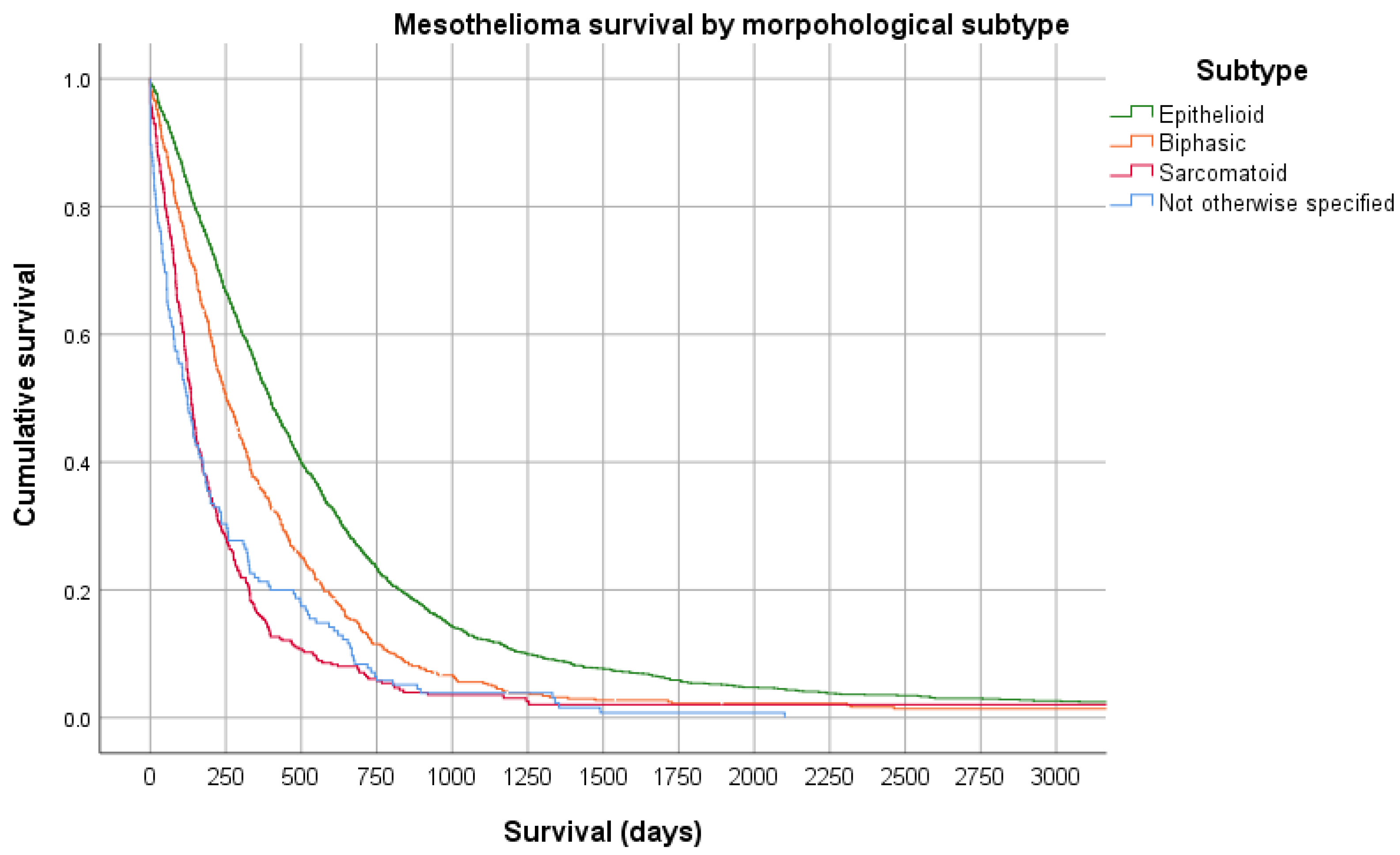
6. Prognosis
7. Conclusions
Funding
Conflicts of Interest
References
- Perry, K.M. Diseases of the lung resulting from occupational dusts other than silica. Thorax 1947, 2, 75–120. [Google Scholar] [CrossRef]
- Doll, R. Mortality from lung cancer in asbestos workers. Br. J. Ind. Med. 1955, 12, 81–86. [Google Scholar] [CrossRef]
- Wagner, J.C.; Sleggs, C.A.; Marchand, P. Diffuse pleural mesothelioma and asbestos exposure in the North Western Cape Province. Br. J. Ind. Med. 1960, 17, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Ross, M.; Nolan, R. History of asbestos discovery and use and asbestos-related disease in context with the occurrence of asbestos within ophiolite complexes. Geol. Soc. Am. Spec. Pap. 2003, 373, 447–470. [Google Scholar]
- Baris, Y.I.; Sahin, A.A.; Ozesmi, M.; Kerse, I.; Ozen, E.; Kolacan, B.; Altinors, M.; Goktepeli, A. An outbreak of pleural mesothelioma and chronic fibrosing pleurisy in the village of Karain/Urgup in Anatolia. Thorax 1978, 33, 181–192. [Google Scholar] [CrossRef]
- Delgermaa, V.; Takahashi, K.; Park, E.K.; Le, G.V.; Hara, T.; Sorahan, T. Global mesothelioma deaths reported to the World Health Organization between 1994 and 2008. Bull. World Health Organ. 2011, 89, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Rahman, O. Global trends in mortality from malignant mesothelioma: Analysis of WHO mortality database (1994–2013). Clin. Respir. J. 2018, 12, 2090–2100. [Google Scholar] [CrossRef]
- Olsen, N.J.; Franklin, P.J.; Reid, A.; de Klerk, N.H.; Threlfall, T.J.; Shilkin, K.; Musk, B. Increasing incidence of malignant mesothelioma after exposure to asbestos during home maintenance and renovation. Med. J. Aust. 2011, 195, 271–274. [Google Scholar] [CrossRef] [PubMed]
- Odgerel, C.O.; Takahashi, K.; Sorahan, T.; Driscoll, T.; Fitzmaurice, C.; Yoko, O.M.; Sawanyawisuth, K.; Furuya, S.; Tanaka, F.; Horie, S.; et al. Estimation of the global burden of mesothelioma deaths from incomplete national mortality data. Occup. Environ. Med. 2017, 74, 851–858. [Google Scholar] [CrossRef] [PubMed]
- WHO. World Health Organisation Cancer Mortality Database. Available online: https://www-dep.iarc.fr/WHOdb/WHOdb.htm (accessed on 24 May 2021).
- U.S. Geological Survey. Asbestos Data Sheet—Mineral Commodity Summaries 2020. Available online: https://pubs.usgs.gov/periodicals/mcs2020/mcs2020-asbestos.pdf (accessed on 11 August 2021).
- Frank, A.L. Global use of asbestos—legitimate and illegitimate issues. J. Occup. Med. Toxicol. 2020, 15. [Google Scholar] [CrossRef]
- Frank, L.A.; Joshi, T.K. The Global Spread of Asbestos. Ann. Glob. Health 2014, 80, 257. [Google Scholar] [CrossRef] [PubMed]
- Brims, F. Asbestos-a legacy and a persistent problem. J. R. Nav. Med. Serv. 2009, 95, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Landrigan, P.J. A population of children at risk of exposure to asbestos in place. Ann. N. Y. Acad. Sci. 1991, 643, 283–286. [Google Scholar] [CrossRef]
- Walters, G.I.; Robertson, A.S.; Bhomra, P.S.; Burge, P.S. Asbestosis is prevalent in a variety of construction industry trades. NPJ Prim. Care Respir. Med. 2018, 28, 11. [Google Scholar] [CrossRef]
- Peto, J.; Hodgson, J.T.; Matthews, F.E.; Jones, J.R. Continuing increase in mesothelioma mortality in Britain. Lancet 1995, 345, 535–539. [Google Scholar] [CrossRef]
- Peto, J.; Decarli, A.; La Vecchia, C.; Levi, F.; Negri, E. The European mesothelioma epidemic. Br. J. Cancer 1999, 79, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Murayama, T.; Takahashi, K.; Natori, Y.; Kurumatani, N. Estimation of future mortality from pleural malignant mesothelioma in Japan based on an age-cohort model. Am. J. Ind. Med. 2006, 49, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Montanaro, F.; Bray, F.; Gennaro, V.; Merler, E.; Tyczynski, J.E.; Parkin, D.M.; Strnad, M.; Jechov’a, M.; Storm, H.H.; Aareleid, T.; et al. Pleural mesothelioma incidence in Europe: Evidence of some deceleration in the increasing trends. Cancer Causes Control 2003, 14, 791–803. [Google Scholar] [CrossRef] [PubMed]
- Tse, L.A.; Yu, I.T.; Goggins, W.; Clements, M.; Wang, X.R.; Au, J.S.; Yu, K.S. Are current or future mesothelioma epidemics in Hong Kong the tragic legacy of uncontrolled use of asbestos in the past? Environ. Health Perspect 2010, 118, 382–386. [Google Scholar] [CrossRef]
- Reynolds, C.J.; Minelli, C.; Darnton, A.; Cullinan, P. Mesothelioma mortality in Great Britain: How much longer will dockyards dominate? Occup. Environ. Med. 2019, 76, 908–912. [Google Scholar] [CrossRef]
- Marinaccio, A.; Corfiati, M.; Binazzi, A.; Di Marzio, D.; Scarselli, A.; Ferrante, P.; Bonafede, M.; Verardo, M.; Mirabelli, D.; Gennaro, V.; et al. The epidemiology of malignant mesothelioma in women: Gender differences and modalities of asbestos exposure. Occup. Environ. Med. 2018, 75, 254–262. [Google Scholar] [CrossRef]
- Hodgson, J.T.; Darnton, A. The quantitative risks of mesothelioma and lung cancer in relation to asbestos exposure. Ann. Occup. Hyg. 2000, 44, 565–601. [Google Scholar] [CrossRef]
- Musk, A.W.; De Klerk, N.H.; Brims, F.J.H. Asbestos-Related Non-Malignant Pleural Disease and Mesothelioma. In Parkes’ Occupational Lung Disorders, 4th ed.; Newman-Taylor, A., Cullinan, P., Blanc, P., Pickering, A., Eds.; CRC Press: Boca Raton, FL, USA, 2017; pp. 171–187. [Google Scholar]
- Thomsen, R.W.; Riis, A.H.; Flachs, E.M.; Garabrant, D.H.; Bonde, J.P.E.; Toft Sorensen, H. Risk of asbestosis, mesothelioma, other lung disease or death among motor vehicle mechanics: A 45-year Danish cohort study. Thorax 2021. [Google Scholar] [CrossRef] [PubMed]
- Churg, A. Chrysotile, Tremolite, and Malignant Mesothelioma in Man. Chest 1988, 93, 621–628. [Google Scholar] [CrossRef]
- Mcdonald, J.C.; Armstrong, B.; Case, B.; Doell, D.; Mccaughey, W.T.E.; Mcdonald, A.D.; Sebastien, P. Mesothelioma and Asbestos Fiber Type—Evidence from Lung-Tissue Analyses. Cancer 1989, 63, 1544–1547. [Google Scholar] [CrossRef]
- Berry, G.; de Klerk, N.H.; Reid, A.; Ambrosini, G.L.; Fritschi, L.; Olsen, N.J.; Merler, E.; Musk, A.W. Malignant pleural and peritoneal mesotheliomas in former miners and millers of crocidolite at Wittenoom, Western Australia. Occup. Environ. Med. 2004, 61, e14. [Google Scholar] [CrossRef] [PubMed]
- Menon, L.; Franklin, P.; Olsen, N.; Segal, A.; De Klerk, N.H.; Musk, A.W.; Brims, F.J.H. 60 years of the Western Australian Mesothelioma Registry. In Proceedings of the Thoracic Society of Australia & New Zealand, Melbourne, Australia, April 2021; p. 93. [Google Scholar]
- Yang, H.N.; Testa, J.R.; Carbone, M. Mesothelioma Epidemiology, Carcinogenesis, and Pathogenesis. Curr. Treat. Options Oncol. 2008, 9, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Kroczynska, B.; Cutrone, R.; Bocchetta, M.; Yang, H.; Elmishad, A.G.; Vacek, P.; Ramos-Nino, M.; Mossman, B.T.; Pass, H.I.; Carbone, M. Crocidolite asbestos and SV40 are cocarcinogens in human mesothelial cells and in causing mesothelioma in hamsters. Proc. Natl. Acad. Sci. USA 2006, 103, 14128–14133. [Google Scholar] [CrossRef] [PubMed]
- Amin, A.M.H.; Mason, C.; Rowe, P. Diffuse malignant mesothelioma of the peritoneum following abdominal radiotherapy. Eur. J. Surg. Oncol. 2001, 27, 214–215. [Google Scholar] [CrossRef]
- Travis, L.B.; Fossa, S.D.; Schonfeld, S.J.; McMaster, M.L.; Lynch, C.F.; Storm, H.; Hall, P.; Holowaty, E.; Andersen, A.; Pukkala, E.; et al. Second cancers among 40576 testicular cancer patients: Focus on long-term survivors. J. Natl. Cancer Inst. 2005, 97, 1354–1365. [Google Scholar] [CrossRef]
- Brown, L.M.; Howard, R.A.; Travis, L.B. The risk of secondary malignancies over 30 years after the treatment of non-hodgkin lymphoma. Cancer 2006, 107, 2741–2742. [Google Scholar] [CrossRef] [PubMed]
- Teta, M.J.; Lau, E.; Sceurman, B.K.; Wagner, M.E. Therapeutic radiation for lymphoma - Risk of malignant mesothelioma. Cancer 2007, 109, 1432–1438. [Google Scholar] [CrossRef] [PubMed]
- Cavazza, A.; Travis, L.B.; Travis, W.D.; Wolfe, J.T.; Foo, M.L.; Gillespie, D.J.; Weidner, N.; Colby, T.V. Post-irradiation malignant mesothelioma. Cancer 1996, 77, 1379–1385. [Google Scholar] [CrossRef]
- Andersson, M.; Wallin, H.; Jonsson, M.; Nielsen, L.L.; Visfeldt, J.; Vyberg, M.; Bennett, W.P.; Debenedetti, V.M.G.; Travis, L.B.; Storm, H.H. Lung-Carcinoma and Malignant Mesothelioma in Patients Exposed to Thorotrast—Incidence, Histology and P53 Status. Int. J. Cancer 1995, 63, 330–336. [Google Scholar] [CrossRef]
- de Klerk, N.; Alfonso, H.; Olsen, N.; Reid, A.; Sleith, J.; Palmer, L.; Berry, G.; Musk, A.B. Familial aggregation of malignant mesothelioma in former workers and residents of Wittenoom, Western Australia. Int. J. Cancer 2013, 132, 1423–1428. [Google Scholar] [CrossRef] [PubMed]
- Carbone, M.; Ferris, L.K.; Baumann, F.; Napolitano, A.; Lum, C.A.; Flores, E.G.; Gaudino, G.; Powers, A.; Bryant-Greenwood, P.; Krausz, T.; et al. BAP1 cancer syndrome: Malignant mesothelioma, uveal and cutaneous melanoma, and MBAITs. J. Transl. Med. 2012, 10, 179. [Google Scholar] [CrossRef]
- Sneddon, S.; Leon, J.S.; Dick, I.M.; Cadby, G.; Olsen, N.; Brims, F.; Allcock, R.J.; Moses, E.K.; Melton, P.E.; de Klerk, N.; et al. Absence of germline mutations in BAP1 in sporadic cases of malignant mesothelioma. Gene 2015, 563, 103–105. [Google Scholar] [CrossRef]
- Cadby, G.; Mukherjee, S.; Musk, A.W.; Reid, A.; Garlepp, M.; Dick, I.; Robinson, C.; Hui, J.; Fiorito, G.; Guarrera, S.; et al. A genome-wide association study for malignant mesothelioma risk. Lung Cancer 2013, 82, 1–8. [Google Scholar] [CrossRef]
- Finn, R.S.; Brims, F.J.; Gandhi, A.; Olsen, N.; Musk, A.W.; Maskell, N.A.; Lee, Y.C. Postmortem findings of malignant pleural mesothelioma: A two-center study of 318 patients. Chest 2012, 142, 1267–1273. [Google Scholar] [CrossRef]
- Franklin, P.; Alfonso, H.; Reid, A.; Olsen, N.; Shilkin, K.B.; Brims, F.; de Klerk, N.; Musk, A.W. Asbestos exposure and histological subtype of malignant mesothelioma. Occup. Environ. Med. 2016, 73, 749–752. [Google Scholar] [CrossRef]
- Creaney, J.; van Bruggen, I.; Hof, M.; Segal, A.; Musk, A.W.; de Klerk, N.; Horick, N.; Skates, S.J.; Robinson, B.W. Combined CA125 and mesothelin levels for the diagnosis of malignant mesothelioma. Chest 2007, 132, 1239–1246. [Google Scholar] [CrossRef]
- Creaney, J.; Olsen, N.J.; Brims, F.; Dick, I.M.; Musk, A.W.; de Klerk, N.H.; Skates, S.J.; Robinson, B.W. Serum Mesothelin for Early Detection of the Asbestos-Induced Cancer Maligant Mesothelioma. Cancer Epidemiol. Biomark. Prev. 2010. [Google Scholar] [CrossRef]
- Davies, H.E.; Sadler, R.S.; Bielsa, S.; Maskell, N.A.; Rahman, N.M.; Davies, R.J.; Ferry, B.L.; Lee, Y.C. Clinical impact and reliability of pleural fluid mesothelin in undiagnosed pleural effusions. Am. J. Respir. Crit. Care Med. 2009, 180, 437–444. [Google Scholar] [CrossRef]
- Pass, H.I.; Wali, A.; Tang, N.; Ivanova, A.; Ivanov, S.; Harbut, M.; Carbone, M.; Allard, J. Soluble mesothelin-related peptide level elevation in mesothelioma serum and pleural effusions. Ann. Thorac. Surg. 2008, 85, 265–272, discussion 272. [Google Scholar] [CrossRef] [PubMed]
- Pass, H.I.; Levin, S.M.; Harbut, M.R.; Melamed, J.; Chiriboga, L.; Donington, J.; Huflejt, M.; Carbone, M.; Chia, D.; Goodglick, L.; et al. Fibulin-3 as a blood and effusion biomarker for pleural mesothelioma. N. Engl. J. Med. 2012, 367, 1417–1427. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, G.K.; Akin, M.R.; Villanueva, R.R.; Slatnik, J. Cytopathology of malignant mesothelioma of the pleura in fine-needle aspiration biopsy. Diagn. Cytopathol. 1999, 21, 253–259. [Google Scholar] [CrossRef]
- Wolanski, K.D.; Whitaker, D.; Shilkin, K.B.; Henderson, D.W. The use of epithelial membrane antigen and silver-stained nucleolar organizer regions testing in the differential diagnosis of mesothelioma from benign reactive mesothelioses. Cancer 1998, 82, 583–590. [Google Scholar] [CrossRef]
- Segal, A.; Whitaker, D.; Henderson, D.; Shilkin, K. Pathology and mesothelioma. In Mesothelioma; Robinson, B.W.S., Chinanian, A.P., Eds.; Martin Dunitz: London, UK, 2002; pp. 143–184. [Google Scholar]
- Lechner, J.F.; Tesfaigzi, J.; Gerwin, B.I. Oncogenes and tumor-suppressor genes in mesothelioma--a synopsis. Environ. Health Perspect. 1997, 105 (Suppl. 5), 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Lindholm, P.M.; Salmenkivi, K.; Vauhkonen, H.; Nicholson, A.G.; Anttila, S.; Kinnula, V.L.; Knuutila, S. Gene copy number analysis in malignant pleural mesothelioma using oligonucleotide array CGH. Cytogenet. Genome Res. 2007, 119, 46–52. [Google Scholar] [CrossRef]
- Musti, M.; Kettunen, E.; Dragonieri, S.; Lindholm, P.; Cavone, D.; Serio, G.; Knuutila, S. Cytogenetic and molecular genetic changes in malignant mesothelioma. Cancer Genet. Cytogenet. 2006, 170, 9–15. [Google Scholar] [CrossRef]
- Chapel, D.B.; Schulte, J.J.; Berg, K.; Churg, A.; Dacic, S.; Fitzpatrick, C.; Galateau-Salle, F.; Hiroshima, K.; Krausz, T.; Le Stang, N.; et al. MTAP immunohistochemistry is an accurate and reproducible surrogate for CDKN2A fluorescence in situ hybridization in diagnosis of malignant pleural mesothelioma. Mod. Pathol 2020, 33, 245–254. [Google Scholar] [CrossRef]
- Churg, A.; Hwang, H.; Tan, L.; Qing, G.; Taher, A.; Tong, A.; Bilawich, A.M.; Dacic, S. Malignant mesothelioma in situ. Histopathology 2018, 72, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Churg, A.; Galateau-Salle, F.; Roden, A.C.; Attanoos, R.; von der Thusen, J.H.; Tsao, M.S.; Chang, N.; De Perrot, M.; Dacic, S. Malignant mesothelioma in situ: Morphologic features and clinical outcome. Mod. Pathol 2020, 33, 297–302. [Google Scholar] [CrossRef]
- Matsumoto, S.; Hamasaki, M.; Kinoshita, Y.; Kamei, T.; Kawahara, K.; Nabeshima, K. Morphological difference between pleural mesothelioma cells in effusion smears with either BAP1 loss or 9p21 homozygous deletion and reactive mesothelial cells without the gene alterations. Pathol. Int. 2019, 69, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Hjerpe, A.; Ascoli, V.; Bedrossian, C.W.; Boon, M.E.; Creaney, J.; Davidson, B.; Dejmek, A.; Dobra, K.; Fassina, A.; Field, A.; et al. Guidelines for the Cytopathologic Diagnosis of Epithelioid and Mixed-Type Malignant Mesothelioma: A secondary publication. Cytopathology 2015, 26, 142–156. [Google Scholar] [CrossRef] [PubMed]
- Hwang, H.C.; Sheffield, B.S.; Rodriguez, S.; Thompson, K.; Tse, C.H.; Gown, A.M.; Churg, A. Utility of BAP1 Immunohistochemistry and p16 (CDKN2A) FISH in the Diagnosis of Malignant Mesothelioma in Effusion Cytology Specimens. Am. J. Surg Pathol. 2016, 40, 120–126. [Google Scholar] [CrossRef]
- Muruganandan, S.; Alfonso, H.; Franklin, P.; Shilkin, K.; Segal, A.; Olsen, N.; Reid, A.; de Klerk, N.; Musk, A.B.; Brims, F. Comparison of outcomes following a cytological or histological diagnosis of malignant mesothelioma. Br. J. Cancer 2017, 116, 703–708. [Google Scholar] [CrossRef] [PubMed]
- Segal, A.; Sterrett, G.F.; Frost, F.A.; Shilkin, K.B.; Olsen, N.J.; Musk, A.W.; Nowak, A.K.; Robinson, B.W.; Creaney, J. A diagnosis of malignant pleural mesothelioma can be made by effusion cytology: Results of a 20 year audit. Pathology 2013, 45, 44–48. [Google Scholar] [CrossRef]
- Hoon, S.N.; Lawrie, I.; Qi, C.; Rahman, N.; Maskell, N.; Forbes, K.; Gerry, S.; Monterosso, L.; Chauhan, A.; Brims, F.J.H. Symptom Burden and Unmet Needs in Malignant Pleural Mesothelioma: Exploratory Analyses From the RESPECT-Meso Study. J. Palliat. Care 2021, 36, 113–120. [Google Scholar] [CrossRef]
- Yildirim, H.; Metintas, M.; Entok, E.; Ak, G.; Ak, I.; Dundar, E.; Erginel, S. Clinical value of fluorodeoxyglucose-positron emission tomography/computed tomography in differentiation of malignant mesothelioma from asbestos-related benign pleural disease: An observational pilot study. J. Thorac. Oncol. 2009, 4, 1480–1484. [Google Scholar] [CrossRef]
- Kruse, M.; Sherry, S.J.; Paidpally, V.; Mercier, G.; Subramaniam, R.M. FDG PET/CT in the management of primary pleural tumors and pleural metastases. AJR Am. J. Roentgenol. 2013, 201, W215–W226. [Google Scholar] [CrossRef]
- Rusch, V.W. A proposed new international TNM staging system for malignant pleural mesothelioma. From the International Mesothelioma Interest Group. Chest 1995, 108, 1122–1128. [Google Scholar] [CrossRef]
- Musk, A.W.; Dewar, J.; Shilkin, K.B.; Whitaker, D. Miliary spread of malignant pleural mesothelioma without a clinically identifiable pleural tumour. Aust. N. Z. J. Med. 1991, 21, 460–462. [Google Scholar] [CrossRef] [PubMed]
- de Gooijer, C.J.; Borm, F.J.; Scherpereel, A.; Baas, P. Immunotherapy in Malignant Pleural Mesothelioma. Front. Oncol. 2020, 10, 187. [Google Scholar] [CrossRef] [PubMed]
- Ceresoli, G.L.; Pasello, G. Immune checkpoint inhibitors in mesothelioma: A turning point. Lancet 2021, 397, 348–349. [Google Scholar] [CrossRef]
- Vogelzang, N.J.; Rusthoven, J.J.; Symanowski, J.; Denham, C.; Kaukel, E.; Ruffie, P.; Gatzemeier, U.; Boyer, M.; Emri, S.; Manegold, C.; et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J. Clin. Oncol. 2003, 21, 2636–2644. [Google Scholar] [CrossRef] [PubMed]
- Zalcman, G.; Mazieres, J.; Margery, J.; Greillier, L.; Audigier-Valette, C.; Moro-Sibilot, D.; Molinier, O.; Corre, R.; Monnet, I.; Gounant, V.; et al. Bevacizumab for newly diagnosed pleural mesothelioma in the Mesothelioma Avastin Cisplatin Pemetrexed Study (MAPS): A randomised, controlled, open-label, phase 3 trial. Lancet 2016, 387, 1405–1414. [Google Scholar] [CrossRef]
- Popat, S.; Curioni-Fontecedro, A.; Dafni, U.; Shah, R.; O’Brien, M.; Pope, A.; Fisher, P.; Spicer, J.; Roy, A.; Gilligan, D.; et al. A multicentre randomised phase III trial comparing pembrolizumab versus single-agent chemotherapy for advanced pre-treated malignant pleural mesothelioma: The European Thoracic Oncology Platform (ETOP 9-15) PROMISE-meso trial. Ann. Oncol. 2020, 31, 1734–1745. [Google Scholar] [CrossRef] [PubMed]
- Nowak, A.K.; Lesterhuis, W.J.; Kok, P.S.; Brown, C.; Hughes, B.G.; Karikios, D.J.; John, T.; Kao, S.C.; Leslie, C.; Cook, A.M.; et al. Durvalumab with first-line chemotherapy in previously untreated malignant pleural mesothelioma (DREAM): A multicentre, single-arm, phase 2 trial with a safety run-in. Lancet Oncol. 2020, 21, 1213–1223. [Google Scholar] [CrossRef]
- Baas, P.; Scherpereel, A.; Nowak, A.K.; Fujimoto, N.; Peters, S.; Tsao, A.S.; Mansfield, A.S.; Popat, S.; Jahan, T.; Antonia, S.; et al. First-line nivolumab plus ipilimumab in unresectable malignant pleural mesothelioma (CheckMate 743): A multicentre, randomised, open-label, phase 3 trial. Lancet 2021, 397, 375–386. [Google Scholar] [CrossRef]
- Brims, F.J.; Meniawy, T.M.; Duffus, I.; de Fonseka, D.; Segal, A.; Creaney, J.; Maskell, N.; Lake, R.A.; de Klerk, N.; Nowak, A.K. A Novel Clinical Prediction Model for Prognosis in Malignant Pleural Mesothelioma Using Decision Tree Analysis. J. Thorac. Oncol. 2016, 11, 573–582. [Google Scholar] [CrossRef]
- Nowak, A.K.; Francis, R.J.; Phillips, M.J.; Millward, M.J.; van der Schaaf, A.A.; Boucek, J.; Musk, A.W.; McCoy, M.J.; Segal, A.; Robins, P.; et al. A novel prognostic model for malignant mesothelioma incorporating quantitative FDG-PET imaging with clinical parameters. Clin. Cancer Res. 2010, 16, 2409–2417. [Google Scholar] [CrossRef]
- Brosseau, S.; Danel, C.; Scherpereel, A.; Mazieres, J.; Lantuejoul, S.; Margery, J.; Greillier, L.; Audigier-Valette, C.; Gounant, V.; Antoine, M.; et al. Shorter Survival in Malignant Pleural Mesothelioma Patients With High PD-L1 Expression Associated With Sarcomatoid or Biphasic Histology Subtype: A Series of 214 Cases From the Bio-MAPS Cohort. Clin. Lung Cancer 2019, 20, e564–e575. [Google Scholar] [CrossRef]
- Davies, H.E.; Mishra, E.K.; Kahan, B.C.; Wrightson, J.M.; Stanton, A.E.; Guhan, A.; Davies, C.W.; Grayez, J.; Harrison, R.; Prasad, A.; et al. Effect of an indwelling pleural catheter vs chest tube and talc pleurodesis for relieving dyspnea in patients with malignant pleural effusion: The TIME2 randomized controlled trial. JAMA 2012, 307, 2383–2389. [Google Scholar] [CrossRef]
- Bhatnagar, R.; Keenan, E.K.; Morley, A.J.; Kahan, B.C.; Stanton, A.E.; Haris, M.; Harrison, R.N.; Mustafa, R.A.; Bishop, L.J.; Ahmed, L.; et al. Outpatient Talc Administration by Indwelling Pleural Catheter for Malignant Effusion. N. Engl. J. Med. 2018, 378, 1313–1322. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.; Fysh, E.T.H.; Smith, N.A.; Lee, P.; Kwan, B.C.H.; Yap, E.; Horwood, F.C.; Piccolo, F.; Lam, D.C.L.; Garske, L.A.; et al. Effect of an Indwelling Pleural Catheter vs Talc Pleurodesis on Hospitalization Days in Patients with Malignant Pleural Effusion. JAMA 2017, 318, 1903. [Google Scholar] [CrossRef] [PubMed]
- Muruganandan, S.; Azzopardi, M.; Fitzgerald, D.B.; Shrestha, R.; Kwan, B.C.H.; Lam, D.C.L.; De Chaneet, C.C.; Rashid Ali, M.R.S.; Yap, E.; Tobin, C.L.; et al. Aggressive versus symptom-guided drainage of malignant pleural effusion via indwelling pleural catheters (AMPLE-2): An open-label randomised trial. Lancet Respir. Med. 2018, 6, 671–680. [Google Scholar] [CrossRef]
- Agarwal, P.P.; Seely, J.M.; Matzinger, F.R.; MacRae, R.M.; Peterson, R.A.; Maziak, D.E.; Dennie, C.J. Pleural mesothelioma: Sensitivity and incidence of needle track seeding after image-guided biopsy versus surgical biopsy. Radiology 2006, 241, 589–594. [Google Scholar] [CrossRef]
- Bayman, N.; Appel, W.; Ashcroft, L.; Baldwin, D.R.; Bates, A.; Darlison, L.; Edwards, J.G.; Ezhil, V.; Gilligan, D.; Hatton, M.; et al. Prophylactic Irradiation of Tracts in Patients with Malignant Pleural Mesothelioma: An Open-Label, Multicenter, Phase III Randomized Trial. J. Clin. Oncol. 2019, 37, 1200–1208. [Google Scholar] [CrossRef]
- Clive, A.O.; Taylor, H.; Dobson, L.; Wilson, P.; de Winton, E.; Panakis, N.; Pepperell, J.; Howell, T.; Stewart, S.A.; Penz, E.; et al. Prophylactic radiotherapy for the prevention of procedure-tract metastases after surgical and large-bore pleural procedures in malignant pleural mesothelioma (SMART): A multicentre, open-label, phase 3, randomised controlled trial. Lancet Oncol. 2016, 17, 1094–1104. [Google Scholar] [CrossRef]
- Bertoglio, P.; Waller, D.A. The role of thoracic surgery in the management of mesothelioma: An expert opinion on the limited evidence. Expert Rev. Respir. Med. 2016, 10, 663–672. [Google Scholar] [CrossRef]
- Treasure, T.; Lang-Lazdunski, L.; Waller, D.; Bliss, J.M.; Tan, C.; Entwisle, J.; Snee, M.; O’Brien, M.; Thomas, G.; Senan, S.; et al. Extra-pleural pneumonectomy versus no extra-pleural pneumonectomy for patients with malignant pleural mesothelioma: Clinical outcomes of the Mesothelioma and Radical Surgery (MARS) randomised feasibility study. Lancet Oncol. 2011, 12, 763–772. [Google Scholar] [CrossRef]
- McRonald, F.; Baldwin, D.R.; Devaraj, A.; Brain, K.; Eisen, T.; Holeman, J.; Ledson, M.; Screaton, N.; Rintoul, R.C.; Yadegarfar, G.; et al. The uniqueness of the United Kingdom Lung Cancer Screening trial (UKLS)—A population screening study. Lung Cancer 2013, 79, S28–S29. [Google Scholar] [CrossRef]
- Hasani, A.; Alvarez, J.M.; Wyatt, J.M.; Bydder, S.; Millward, M.; Byrne, M.; Musk, A.W.; Nowak, A.K. Outcome for patients with malignant pleural mesothelioma referred for Trimodality therapy in Western Australia. J. Thorac. Oncol. 2009, 4, 1010–1016. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.C. Surgical resection of mesothelioma: An evidence-free practice. Lancet 2014, 384, 1080–1081. [Google Scholar] [CrossRef]
- Ricciardi, S.; Cardillo, G.; Zirafa, C.C.; Carleo, F.; Facciolo, F.; Fontanini, G.; Mutti, L.; Melfi, F. Surgery for malignant pleural mesothelioma: An international guidelines review. J. Thorac. Dis. 2018, 10, S285–S292. [Google Scholar] [CrossRef]
- Rintoul, R.C.; Ritchie, A.J.; Edwards, J.G.; Waller, D.A.; Coonar, A.S.; Bennett, M.; Lovato, E.; Hughes, V.; Fox-Rushby, J.A.; Sharples, L.D.; et al. Efficacy and cost of video-assisted thoracoscopic partial pleurectomy versus talc pleurodesis in patients with malignant pleural mesothelioma (MesoVATS): An open-label, randomised, controlled trial. Lancet 2014, 384, 1118–1127. [Google Scholar] [CrossRef]
- Brims, F.; Gunatilake, S.; Lawrie, I.; Marshall, L.; Fogg, C.; Qi, C.; Creech, L.; Holtom, N.; Killick, S.; Yung, B.; et al. Early specialist palliative care on quality of life for malignant pleural mesothelioma: A randomised controlled trial. Thorax 2019, 74, 354–361. [Google Scholar] [CrossRef]
- Sinclair, C.; Auret, K.A.; Evans, S.F.; Williamson, F.; Dormer, S.; Wilkinson, A.; Greeve, K.; Koay, A.; Price, D.; Brims, F. Advance care planning uptake among patients with severe lung disease: A randomised patient preference trial of a nurse-led, facilitated advance care planning intervention. BMJ Open 2017, 7, e013415. [Google Scholar] [CrossRef] [PubMed]
- Neumann, V.; Rutten, A.; Scharmach, M.; Muller, K.M.; Fischer, M. Factors influencing long-term survival in mesothelioma patients--results of the German mesothelioma register. Int. Arch. Occup. Environ. Health 2004, 77, 191–199. [Google Scholar] [CrossRef]
- Musk, A.W.; Olsen, N.; Alfonso, H.; Reid, A.; Mina, R.; Franklin, P.; Sleith, J.; Hammond, N.; Threlfall, T.; Shilkin, K.B.; et al. Predicting survival in malignant mesothelioma. Eur. Respir. J. 2011, 38, 1420–1424. [Google Scholar] [CrossRef] [PubMed]
- Brims, F.J.; Maskell, N.A. Prognostic factors for malignant pleural mesothelioma. Curr. Respir. Care Rep. 2013, 2, 100–108. [Google Scholar] [CrossRef][Green Version]
- Mirarabshahii, P.; Pillai, K.; Chua, T.C.; Pourgholami, M.H.; Morris, D.L. Diffuse malignant peritoneal mesothelioma—An update on treatment. Cancer Treat. Rev. 2012, 38, 605–612. [Google Scholar] [CrossRef]
- Creaney, J.; Francis, R.J.; Dick, I.M.; Musk, A.W.; Robinson, B.W.; Byrne, M.J.; Nowak, A.K. Serum soluble mesothelin concentrations in malignant pleural mesothelioma: Relationship to tumor volume, clinical stage and changes in tumor burden. Clin. Cancer Res. 2011, 17, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Grigoriu, B.D.; Scherpereel, A.; Devos, P.; Chahine, B.; Letourneux, M.; Lebailly, P.; Gregoire, M.; Porte, H.; Copin, M.C.; Lassalle, P. Utility of osteopontin and serum mesothelin in malignant pleural mesothelioma diagnosis and prognosis assessment. Clin. Cancer Res. 2007, 13, 2928–2935. [Google Scholar] [CrossRef]
- Hollevoet, K.; Nackaerts, K.; Gosselin, R.; De Wever, W.; Bosquee, L.; De Vuyst, P.; Germonpre, P.; Kellen, E.; Legrand, C.; Kishi, Y.; et al. Soluble mesothelin, megakaryocyte potentiating factor, and osteopontin as markers of patient response and outcome in mesothelioma. J. Thorac. Oncol. 2011, 6, 1930–1937. [Google Scholar] [CrossRef]
- Creaney, J.; Dick, I.M.; Meniawy, T.M.; Leong, S.L.; Leon, J.S.; Demelker, Y.; Segal, A.; Bill Musk, A.W.; Lee, Y.C.; Skates, S.J.; et al. Comparison of fibulin-3 and mesothelin as markers in malignant mesothelioma. Thorax 2014, 69, 895–902. [Google Scholar] [CrossRef]
- Kadota, K.; Suzuki, K.; Colovos, C.; Sima, C.S.; Rusch, V.W.; Travis, W.D.; Adusumilli, P.S. A nuclear grading system is a strong predictor of survival in epitheloid diffuse malignant pleural mesothelioma. Mod. Pathol. 2012, 25, 260–271. [Google Scholar] [CrossRef]
- Kao, S.C.; Pavlakis, N.; Harvie, R.; Vardy, J.L.; Boyer, M.J.; van Zandwijk, N.; Clarke, S.J. High blood neutrophil-to-lymphocyte ratio is an indicator of poor prognosis in malignant mesothelioma patients undergoing systemic therapy. Clin. Cancer Res. 2010, 16, 5805–5813. [Google Scholar] [CrossRef]
- Kao, S.C.; Klebe, S.; Henderson, D.W.; Reid, G.; Chatfield, M.; Armstrong, N.J.; Yan, T.D.; Vardy, J.; Clarke, S.; van Zandwijk, N.; et al. Low calretinin expression and high neutrophil-to-lymphocyte ratio are poor prognostic factors in patients with malignant mesothelioma undergoing extrapleural pneumonectomy. J. Thorac. Oncol. 2011, 6, 1923–1929. [Google Scholar] [CrossRef]
- Yeap, B.Y.; De Rienzo, A.; Gill, R.R.; Oster, M.E.; Dao, M.N.; Dao, N.T.; Levy, R.D.; Vermilya, K.; Gustafson, C.E.; Ovsak, G.; et al. Mesothelioma Risk Score: A New Prognostic Pretreatment, Clinical-Molecular Algorithm for Malignant Pleural Mesothelioma. J. Thorac. Oncol. 2021. [Google Scholar] [CrossRef]
- Curran, D.; Sahmoud, T.; Therasse, P.; van Meerbeeck, J.; Postmus, P.E.; Giaccone, G. Prognostic factors in patients with pleural mesothelioma: The European Organization for Research and Treatment of Cancer experience. J. Clin. Oncol. 1998, 16, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Herndon, J.E.; Green, M.R.; Chahinian, A.P.; Corson, J.M.; Suzuki, Y.; Vogelzang, N.J. Factors predictive of survival among 337 patients with mesothelioma treated between 1984 and 1994 by the Cancer and Leukemia Group B. Chest 1998, 113, 723–731. [Google Scholar] [CrossRef] [PubMed]
- van der Bij, S.; Koffijberg, H.; Burgers, J.A.; Baas, P.; van de Vijver, M.J.; de Mol, B.A.; Moons, K.G. Prognosis and prognostic factors of patients with mesothelioma: A population-based study. Br. J. Cancer 2012, 107, 161–164. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Milano, M.T.; Zhang, H. Malignant pleural mesothelioma: A population-based study of survival. J. Thorac. Oncol. 2010, 5, 1841–1848. [Google Scholar] [CrossRef] [PubMed]
- Nojiri, S.; Gemba, K.; Aoe, K.; Kato, K.; Yamaguchi, T.; Sato, T.; Kubota, K.; Kishimoto, T. Survival and prognostic factors in malignant pleural mesothelioma: A retrospective study of 314 patients in the west part of Japan. Jpn. J. Clin. Oncol. 2011, 41, 32–39. [Google Scholar] [CrossRef]
- Montanaro, F.; Rosato, R.; Gangemi, M.; Roberti, S.; Ricceri, F.; Merler, E.; Gennaro, V.; Romanelli, A.; Chellini, E.; Pascucci, C.; et al. Survival of pleural malignant mesothelioma in Italy: A population-based study. Int. J. Cancer 2009, 124, 201–207. [Google Scholar] [CrossRef]
- Marinaccio, A.; Nesti, M.; Regional Operational, C. Analysis of survival of mesothelioma cases in the Italian register (ReNaM). Eur. J. Cancer 2003, 39, 1290–1295. [Google Scholar] [CrossRef]
- Woolhouse, I.; Bishop, L.; Darlison, L.; De Fonseka, D.; Edey, A.; Edwards, J.; Faivre-Finn, C.; Fennell, D.A.; Holmes, S.; Kerr, K.M.; et al. British Thoracic Society Guideline for the investigation and management of malignant pleural mesothelioma. Thorax 2018, 73, i1–i30. [Google Scholar] [CrossRef] [PubMed]
- Harris, E.J.A.; Kao, S.; McCaughan, B.; Nakano, T.; Kondo, N.; Hyland, R.; Nowak, A.K.; de Klerk, N.H.; Brims, F.J.H. Prediction modelling using routine clinical parameters to stratify survival in Malignant Pleural Mesothelioma patients undergoing cytoreductive surgery. J. Thorac. Oncol. 2019, 14, 288–293. [Google Scholar] [CrossRef]
- Bibby, A.C.; Dorn, P.; Psallidas, I.; Porcel, J.M.; Janssen, J.; Froudarakis, M.; Subotic, D.; Astoul, P.; Licht, P.; Schmid, R.; et al. ERS/EACTS statement on the management of malignant pleural effusions. Eur. Respir. J. 2018, 52. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brims, F. Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma. Cancers 2021, 13, 4194. https://doi.org/10.3390/cancers13164194
Brims F. Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma. Cancers. 2021; 13(16):4194. https://doi.org/10.3390/cancers13164194
Chicago/Turabian StyleBrims, Fraser. 2021. "Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma" Cancers 13, no. 16: 4194. https://doi.org/10.3390/cancers13164194
APA StyleBrims, F. (2021). Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma. Cancers, 13(16), 4194. https://doi.org/10.3390/cancers13164194