
The Effects of Multidisciplinary Team Meetings on Clinical Practice for Colorectal, Lung, Prostate and Breast Cancer: A Systematic Review

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.3. Study Selection Criteria
2.4. Data Collection and Extraction
2.5. Quality Assessment
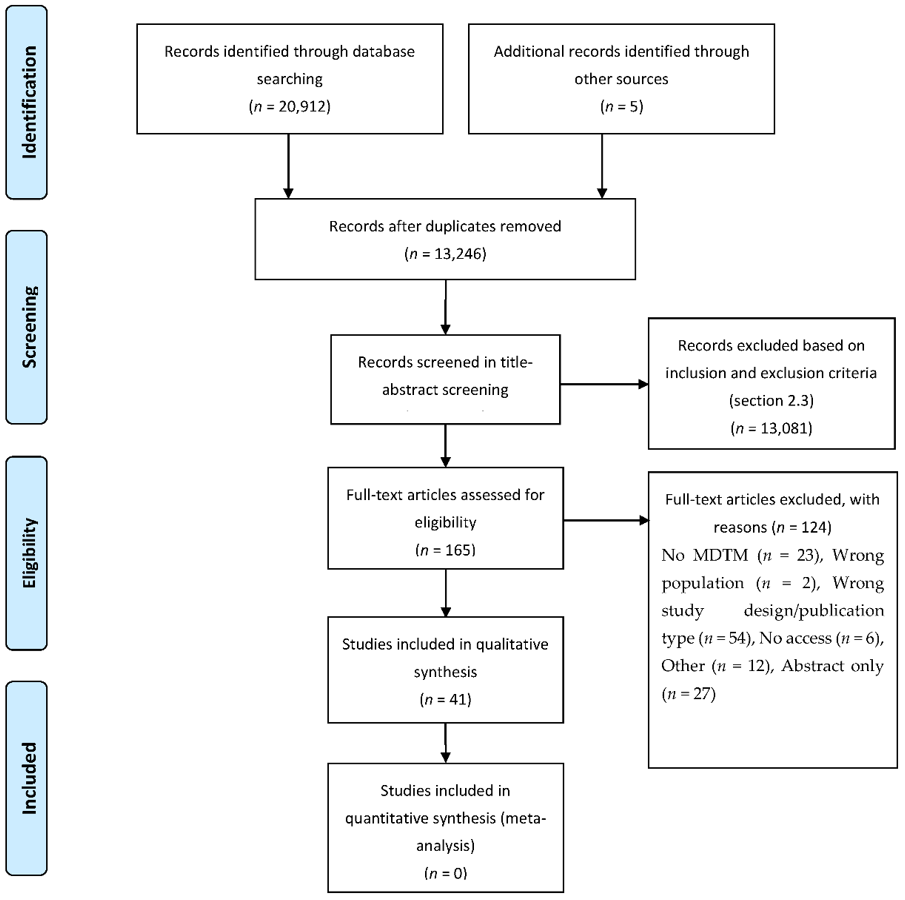
3. Results
3.1. Study Characteristics
3.2. Risk of Bias and Quality of Evidence Assessment
3.3. Patient Management
Changes in Overall Management Plans
3.4. Effect on Diagnostics and Treatment
3.4.1. Diagnostics
3.4.2. Surgery
3.4.3. Radiotherapy, Chemotherapy and Palliative Care
3.4.4. Patient Outcomes
4. Discussion
4.1. Summary of Evidence
4.2. Strengths and Limitations
4.3. Future Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lamb, B.W.; Brown, K.F.; Nagpal, K.; Vincent, C.; Green, J.S.; Sevdalis, N. Quality of care management decisions by multidisciplinary cancer teams: A systematic review. Ann. Surg. Oncol. 2011, 18, 2116–2125. [Google Scholar] [CrossRef] [PubMed]
- El Saghir, N.S.; Keating, N.L.; Carlson, R.W.; Khoury, K.E.; Fallowfield, L. Tumor boards: Optimizing the structure and improving efficiency of multidisciplinary management of patients with cancer worldwide. Am. Soc. Clin. Oncol. Educ. Book 2014, 34, e461–e466. [Google Scholar] [CrossRef]
- Calman, K.; Hine, D. Report by the Expert Advisory Group on Cancer to the Chief Medical Officers of England and Wales. In A Policy Framework for Comissioning Cancer Services (The Calman-Hine Report); Department of Health: London, UK, 1995. [Google Scholar]
- Fitzmaurice, C.; Akinyemiju, T.F.; Al Lami, F.H.; Alam, T.; Alizadeh-Navaei, R.; Allen, C.; Alsharif, U.; Alvis-Guzman, N.; Amini, E.; Anderson, B.O.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2016: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2018, 4, 1553–1568. [Google Scholar] [CrossRef] [PubMed]
- Globocan. Cancer Today—International Agency for Research on Cancer. Available online: https://gco.iarc.fr/today/online-analysispie?v=2018&mode=cancer&mode_population=continents&population=900&populations=900&key=total&sex=0&cancer=39&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&nb_items=7&group_cancer=1&include_nmsc=1&include_nmsc_other=1&half_pie=0&donut=0&population_group_globocan_id= (accessed on 7 December 2020).
- Basta, Y.L.; Bolle, S.; Fockens, P.; Tytgat, K.M. The value of multidisciplinary team meetings for patients with gastrointestinal malignancies: A systematic review. Ann. Surg. Oncol. 2017, 24, 2669–2678. [Google Scholar] [CrossRef]
- Pillay, B.; Wootten, A.C.; Crowe, H.; Corcoran, N.; Tran, B.; Bowden, P.; Crowe, J.; Costello, A.J. The impact of multidisciplinary team meetings on patient assessment, management and outcomes in oncology settings: A systematic review of the literature. Cancer Treat. Rev. 2016, 42, 56–72. [Google Scholar] [CrossRef] [PubMed]
- Prades, J.; Remue, E.; Van Hoof, E.; Borras, J.M. Is it worth reorganising cancer services on the basis of multidisciplinary teams (MDTs)? A systematic review of the objectives and organisation of MDTs and their impact on patient outcomes. Health Policy 2015, 119, 464–474. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Group, P.-P. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef]
- Koco, L.; Weekenstroo, H. The effects of implementing multidisciplinary team meetings in breast, prostate and lung cancer pathways: A systematic review. 2019. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=127476 (accessed on 7 December 2020).
- Bramer, W.M.; Giustini, D.; de Jonge, G.B.; Holland, L.; Bekhuis, T. De-duplication of database search results for systematic reviews in EndNote. JMLA 2016, 104, 240. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Sterne, J.A.; Hernán, M.A.; McAleenan, A.; Reeves, B.C.; Higgins, J.P. Assessing risk of bias in a non-randomized study. In Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley: Hoboken, NJ, USA, 2019; pp. 621–641. [Google Scholar]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S.; et al. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Anania, G.; Resta, G.; Marino, S.; Fabbri, N.; Scagliarini, L.; Marchitelli, I.; Fiorica, F.; Cavallesco, G. Treatment of colorectal cancer: A multidisciplinary approach. J. Gastrointest. Cancer 2019, 50, 458–468. [Google Scholar] [CrossRef]
- Chen, C.H.; Hsieh, M.C.; Lao, W.T.; Lin, E.K.; Lu, Y.J.; Wu, S.Y. Multidisciplinary team intervention associated with improved survival for patients with colorectal adenocarcinoma with liver or lung metastasis. Am. J. Cancer Res. 2018, 8, 1887. [Google Scholar]
- Chinai, N.; Bintcliffe, F.; Armstrong, E.; Teape, J.; Jones, B.; Hosie, K. Does every patient need to be discussed at a multidisciplinary team meeting? Clin. Radiol. 2013, 68, 780–784. [Google Scholar] [CrossRef] [PubMed]
- Fernando, C.; Frizelle, F.; Wakeman, C.; Frampton, C.; Robinson, B. Colorectal multidisciplinary meeting audit to determine patient benefit. ANZ J. Surg. 2017, 87, E173–E177. [Google Scholar] [CrossRef] [PubMed]
- Jung, S.M.; Hong, Y.S.; Kim, T.W.; Park, J.H.; Kim, J.H.; Park, S.H.; Kim, A.Y.; Lim, S.B.; Lee, Y.J.; Yu, C.S. Impact of a multidisciplinary team approach for managing advanced and recurrent colorectal cancer. World J. Surg. 2018, 42, 2227–2233. [Google Scholar] [CrossRef] [PubMed]
- Karagkounis, G.; Stocchi, L.; Lavery, I.C.; Liska, D.; Gorgun, E.; Veniero, J.; Plesec, T.; Amarnath, S.; Khorana, A.A.; Kalady, M.F. Multidisciplinary conference and clinical management of rectal cancer. J. Am. Coll. Surg. 2018, 226, 874–880. [Google Scholar] [CrossRef] [PubMed]
- Lan, Y.T.; Jiang, J.K.; Chang, S.C.; Yang, S.H.; Lin, C.C.; Lin, H.H.; Wang, H.S.; Chen, W.S.; Lin, T.C.; Lin, J.K. Improved outcomes of colorectal cancer patients with liver metastases in the era of the multidisciplinary teams. Int. J. Colorectal Dis. 2016, 31, 403–411. [Google Scholar] [CrossRef]
- MacDermid, E.; Hooton, G.; MacDonald, M.; McKay, G.; Grose, D.; Mohammed, N.; Porteous, C. Improving patient survival with the colorectal cancer multi-disciplinary team. Colorectal Dis. 2009, 11, 291–295. [Google Scholar] [CrossRef]
- Munro, A.; Brown, M.; Niblock, P.; Steele, R.; Carey, F. Do Multidisciplinary Team (MDT) processes influence survival in patients with colorectal cancer? A population-based experience. BMC Cancer 2015, 15, 686. [Google Scholar] [CrossRef]
- Nikolovski, Z.; Watters, D.A.; Stupart, D.; Guest, G.D. Colorectal multidisciplinary meetings: How do they affect the timeliness of treatment? ANZ J. Surg. 2017, 87, E112–E115. [Google Scholar] [CrossRef]
- Palmer, G.; Martling, A.; Cedermark, B.; Holm, T. Preoperative tumour staging with multidisciplinary team assessment improves the outcome in locally advanced primary rectal cancer. Colorectal Dis. 2011, 13, 1361–1369. [Google Scholar] [CrossRef]
- Richardson, B.; Preskitt, J.; Lichliter, W.; Peschka, S.; Carmack, S.; de Prisco, G.; Fleshman, J. The effect of multidisciplinary teams for rectal cancer on delivery of care and patient outcome: Has the use of multidisciplinary teams for rectal cancer affected the utilization of available resources, proportion of patients meeting the standard of care, and does this translate into changes in patient outcome? Am. J. Surg. 2016, 211, 46–52. [Google Scholar] [CrossRef]
- Ryan, J.; Faragher, I. Not all patients need to be discussed in a colorectal cancer MDT meeting. Colorectal Dis. 2014, 16, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Snelgrove, R.C.; Subendran, J.; Jhaveri, K.; Thipphavong, S.; Cummings, B.; Brierley, J.; Kirsch, R.; Kennedy, E.D. Effect of multidisciplinary cancer conference on treatment plan for patients with primary rectal cancer. Dis. Colon Rectum 2015, 58, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Swellengrebel, H.; Peters, E.; Cats, A.; Visser, O.; Blaauwgeers, H.; Verwaal, V.; van Velthuysen, M.; Cense, H.; Bruin, S.; Marijnen, C. Multidisciplinary discussion and management of rectal cancer: A population-based study. World J. Surg. 2011, 35, 2125–2133. [Google Scholar] [CrossRef]
- Vaughan-Shaw, P.; Wheeler, J.; Borley, N. The impact of a dedicated multidisciplinary team on the management of early rectal cancer. Colorectal Dis. 2015, 17, 704–709. [Google Scholar] [CrossRef]
- Wanis, K.N.; Pineda-Solis, K.; Tun-Abraham, M.E.; Yeoman, J.; Welch, S.; Vogt, K.; Van Koughnett, J.A.M.; Ott, M.; Hernandez-Alejandro, R. Management of colorectal cancer with synchronous liver metastases: Impact of multidisciplinary case conference review. Hepatobiliary Surg. Nutr. 2017, 6, 162. [Google Scholar] [CrossRef] [PubMed]
- Wille-Jørgensen, P.; Sparre, P.; Glenthøj, A.; Holck, S.; Nørgaard Petersen, L.; Harling, H.; Stub Højen, H.; Bülow, S. Result of the implementation of multidisciplinary teams in rectal cancer. Colorectal Dis. 2013, 15, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.J.; Shen, Z.L.; Sun, X.T.; Wang, Z.F.; Shen, D.H.; Liu, H.J.; Zhang, W.L.; Chen, Y.L.; Jing, Z.; Poston, J. Impact of multidisciplinary team working on the management of colorectal cancer. Chin. Med. J. 2012, 125, 172–177. [Google Scholar] [CrossRef]
- Maurizi, A.C.R. Improved Utilization of Resources as an Improvement of Outcome: The Effect of Multidisciplinary Team for Rectal Cancer in a District Hospital. Clin. Oncol. 2017, 2, 1267. [Google Scholar]
- Foucan, A.S.; Grosclaude, P.; Bousser, V.; Bauvin, E.; Smith, D.; Andre-Fardeau, C.; Daubisse-Marliac, L.; Mathoulin-Pelissier, S.; Amadeo, B.; Coureau, G. Management of colon cancer patients: A comprehensive analysis of the absence of multidisciplinary team meetings in two French departments. Clin. Res. Hepatol. Gastroenterol. 2020, 45, 101413. [Google Scholar] [CrossRef]
- Boxer, M.M.; Vinod, S.K.; Shafiq, J.; Duggan, K.J. Do multidisciplinary team meetings make a difference in the management of lung cancer? Cancer 2011, 117, 5112–5120. [Google Scholar] [CrossRef]
- Bydder, S.; Nowak, A.; Marion, K.; Phillips, M.; Atun, R. The impact of case discussion at a multidisciplinary team meeting on the treatment and survival of patients with inoperable non-small cell lung cancer. Intern. Med. J. 2009, 39, 838–841. [Google Scholar] [CrossRef] [PubMed]
- Freeman, R.K.; Ascioti, A.J.; Dake, M.; Mahidhara, R.S. The effects of a multidisciplinary care conference on the quality and cost of care for lung cancer patients. Ann. Thorac. Surg. 2015, 100, 1834–1838. [Google Scholar] [CrossRef] [PubMed]
- Pan, C.C.; Kung, P.T.; Wang, Y.H.; Chang, Y.C.; Wang, S.T.; Tsai, W.C. Effects of multidisciplinary team care on the survival of patients with different stages of non-small cell lung cancer: A national cohort study. PLoS ONE 2015, 10, e0126547. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, H.M.; Roberts, J.M.; Bodnar, A.M.; Kunz, S.; Kirtland, S.H.; Koehler, R.P.; Hubka, M.; Low, D.E. Thoracic multidisciplinary tumor board routinely impacts therapeutic plans in patients with lung and esophageal cancer: A prospective cohort study. Ann. Thorac. Surg. 2015, 99, 1719–1724. [Google Scholar] [CrossRef]
- Stone, E.; Rankin, N.; Kerr, S.; Fong, K.; Currow, D.C.; Phillips, J.; Connon, T.; Zhang, L.; Shaw, T. Does presentation at multidisciplinary team meetings improve lung cancer survival? Findings from a consecutive cohort study. Lung Cancer 2018, 124, 199–204. [Google Scholar] [CrossRef]
- Tamburini, N.; Maniscalco, P.; Mazzara, S.; Maietti, E.; Santini, A.; Calia, N.; Stefanelli, A.; Frassoldati, A.; Santi, I.; Rinaldi, R. Multidisciplinary management improves survival at 1 year after surgical treatment for non-small-cell lung cancer: A propensity score-matched study. Eur. J. Cardio Thorac. Surg. 2018, 53, 1199–1204. [Google Scholar] [CrossRef]
- Ung, K.A.; Campbell, B.A.; Duplan, D.; Ball, D.; David, S. Impact of the lung oncology multidisciplinary team meetings on the management of patients with cancer. Asia Pac. J. Clin. Oncol. 2016, 12, e298–e304. [Google Scholar] [CrossRef] [PubMed]
- Hung, H.Y.; Tseng, Y.H.; Chao, H.S.; Chiu, C.H.; Hsu, W.H.; Hsu, H.S.; Wu, Y.C.; Chou, T.Y.; Chen, C.K.; Lan, K.L. Multidisciplinary team discussion results in survival benefit for patients with stage III non-small-cell lung cancer. PLoS ONE 2020, 15, e0236503. [Google Scholar] [CrossRef] [PubMed]
- Muthukrishnan, P.T.; Ratnam, M.; Nguyen, M.T.; Le, M.; Gunzler, D.; Bruno, D.; Infeld, M. Pre-diagnosis Multidisciplinary Tumor Board and Time to Staging in Lung Cancer: The Case Western MetroHealth Experience. Cureus 2020, 12, e6595. [Google Scholar] [CrossRef] [PubMed]
- Acher, P.L.; Young, A.J.; Etherington-Foy, R.; McCahy, P.J.; Deane, A.M. Improving outcomes in urological cancers: The impact of “multidisciplinary team meetings”. Int. J. Surg. 2005, 3, 121–123. [Google Scholar] [CrossRef][Green Version]
- De Luca, S.; Fiori, C.; Tucci, M.; Poggio, M.; Allis, S.; Bollito, E.; Solitro, F.; Passera, R.; Buttigliero, C.; Porpiglia, F. Prostate cancer management at an Italian tertiary referral center: Does multidisciplinary team meeting influence diagnostic and therapeutic decision-making process? A snapshot of the everyday clinical practice. Ital. J. Urol. Nephrol. 2019, 71, 576–582. [Google Scholar] [CrossRef]
- El Khoury, R.; Chahrouri, M.; Hachem, C.; Abi Zeid, J.; El Alam, P.; Abdessater, M. Evaluation of Multidisciplinary Team Meetings in Uro-Oncology. Leban. Med. J. 2016, 64, 84–90. [Google Scholar] [CrossRef]
- Kurpad, R.; Kim, W.; Rathmell, W.K.; Godley, P.; Whang, Y.; Fielding, J.; Smith, L.; Pettiford, A.; Schultz, H.; Nielsen, M. A multidisciplinary approach to the management of urologic malignancies: Does it influence diagnostic and treatment decisions? Urol. Oncol. Semin. Orig. Investig. 2011, 29, 378–382. [Google Scholar] [CrossRef]
- Rao, K.; Manya, K.; Azad, A.; Lawrentschuk, N.; Bolton, D.; Davis, I.D.; Sengupta, S. Uro-oncology multidisciplinary meetings at an Australian tertiary referral centre–impact on clinical decision-making and implications for patient inclusion. BJU Int. 2014, 114, 50–54. [Google Scholar] [CrossRef]
- Scarberry, K.; Ponsky, L.; Cherullo, E.; Larchian, W.; Bodner, D.; Cooney, M.; Ellis, R.; MacLennan, G.; Johnson, B.; Tabayoyong, W. Evaluating the impact of the genitourinary multidisciplinary tumour board: Should every cancer patient be discussed as standard of care? Can. Urol. Assoc. J. 2018, 12, E403. [Google Scholar] [CrossRef]
- Murthy, V.; Nobre, S.; Sparber, L.; Schaefer, S.; Santoro, E.; McDermott, J.; Chamberlain, R.; Blackwood, M. Multidisciplinary breast conference improves patient management and treatment. Surg. Sci. 2014, 5, 314–319. [Google Scholar] [CrossRef]
- Brandão, M.; Guisseve, A.; Bata, G.; Firmino-Machado, J.; Alberto, M.; Ferro, J.; Garcia, C.; Zaqueu, C.; Jamisse, A.; Lorenzoni, C. Survival impact and cost-effectiveness of a multidisciplinary tumor board for breast cancer in Mozambique, Sub-Saharan Africa. Oncologist 2020, 26, e996–e1008. [Google Scholar] [CrossRef]
- Tsai, C.H.; Hsieh, H.F.; Lai, T.W.; Kung, P.T.; Kuo, W.Y.; Tsai, W.C. Effect of multidisciplinary team care on the risk of recurrence in breast cancer patients: A national matched cohort study. Breast 2020, 53, 68–76. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Huang, J.; Zhu, X.; Shen, K.; Zhu, J.; Chen, X. Compliance with multidisciplinary team recommendations and disease outcomes in early breast cancer patients: An analysis of 4501 consecutive patients. Breast 2020, 52, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Ke, K.M.; Blazeby, J.M.; Strong, S.; Carroll, F.E.; Ness, A.R.; Hollingworth, W. Are multidisciplinary teams in secondary care cost-effective? A systematic review of the literature. Cost Eff. Resour. Alloc. 2013, 11, 7. [Google Scholar] [CrossRef] [PubMed]
- Jacobsen, M.M.; Silverstein, S.C.; Quinn, M.; Waterston, L.B.; Thomas, C.A.; Benneyan, J.C.; Han, P.K.J. Timeliness of access to lung cancer diagnosis and treatment: A scoping literature review. Lung Cancer 2017, 112, 156–164. [Google Scholar] [CrossRef] [PubMed]
- Coory, M.; Gkolia, P.; Yang, I.A.; Bowman, R.V.; Fong, K.M. Systematic review of multidisciplinary teams in the management of lung cancer. Lung Cancer 2008, 60, 14–21. [Google Scholar] [CrossRef]
- Hong, N.J.; Wright, F.C.; Gagliardi, A.R.; Paszat, L.F. Examining the potential relationship between multidisciplinary cancer care and patient survival: An international literature review. J. Surg. Oncol. 2010, 102, 125–134. [Google Scholar] [CrossRef]
- Ioannidis, A.; Konstantinidis, M.; Apostolakis, S.; Koutserimpas, C.; Machairas, N.; Konstantinidis, K.M. Impact of multidisciplinary tumor boards on patients with rectal cancer. Mol. Clin. Oncol. 2018, 9, 135–137. [Google Scholar] [CrossRef] [PubMed]
- Holmes, A.; Kelly, B.D.; Perera, M.; Eapen, R.S.; Bolton, D.M.; Lawrentschuk, N. A systematic scoping review of multidisciplinary cancer team and decision-making in the management of men with advanced prostate cancer. World J. Urol. 2020, 39, 297–306. [Google Scholar] [CrossRef]
- Blackwood, O.; Deb, R. Multidisciplinary team approach in breast cancer care: Benefits and challenges. Indian J. Pathol. Microbiol. 2020, 63, 105–112. [Google Scholar] [CrossRef]
- Shao, J.; Rodrigues, M.; Corter, A.L.; Baxter, N.N. Multidisciplinary care of breast cancer patients: A scoping review of multidisciplinary styles, processes, and outcomes. Curr. Oncol. 2019, 26, e385–e397. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author & Year | Cancer Type | Country | Aim | Hospital Type | Study Design | Inclusion Period | Participants |
|---|---|---|---|---|---|---|---|
| Acher et al., 2005 [48] | Urological cancers (prostate cancer) | UK | To examine the impact of MDTM on changes in management. | William Harvey Hospital (General hospital) | Prospective cohort study | 6 months (date not specified) | 124 discussions |
| Anania et al., 2019 [17] | Colorectal cancer (rectal cancer) | Italy | To compare the multidisciplinary experience group with the previous approach before the advent of the multidisciplinary program. | S. Anna Hospital (University hospital) | Retrospective before–after study | February 2007–April 2017 MDTM implementation in 2012 | Non-MDTM: 45 patients MDTM: 51 patients Total: 96 patients |
| Boxer et al., 2011 [38] | Lung cancer | Australia | To evaluate the impact of MDTMs by comparing patterns of care among patients who were presented at an MDTM with those who were not presented at a meeting during the same period. | The Liverpool and Macarthur Cancer therapy centers (General hospital) | Prospective case-control study | 1 December 2005–31 December 2008 | Non-MDTM: 484 patients MDTM: 504 patients Total: 988 patients |
| Brandão et al., 2020 [55] | Breast cancer | Mozambique | To assess the impact of implementing an MDTM on the cost-effectiveness, care and survival. | Maputo Central hospital (General Hospitals) | Prospective before–after study | January 2015 and August 2017 Follow-up until November 2019 MDTM implementation: March 2016 | Non-MDTM: 98 patients MDTM: 107 patients Total: 205 patients |
| Bydder et al., 2009 [39] | Non-small cell lung cancer | Australia | To examine the proportion of patients that is discussed by the MDTM and the impact on the treatment and survival. | Sir Charles Gairdner Hospital (Tertiary Hospitals) | Prospective case-control study | 2006 Follow-up until 31 March 2008 | Non-MDTM: 17 patients MDTM: 81 patients Total: 98 patients |
| Chen et al., 2018 [18] | Colorectal cancer with lung or liver metastasis | Taiwan | To investigate whether MDTM intervention is associated with improved survival. | Wan Fang Hospital (University hospital) | Case-control study | January 2007–December 2017 Mean follow-up: 84 months ± 35 months | Non-MDTM: 86 patients MDTM: 75 patients Total: 161 patients |
| Chinai et al., 2013 | Colorectal cancer | UK | To evaluate the clinical impact and cost-effectiveness of a MDTM. | Derriford Hospital Plymouth Hospitals (General hospitals) | Prospective cohort study | 3 months (date not specified) | 47 patients |
| De Luca et al., 2019 [49] | Prostate cancer | Italy | To investigate the impact on clinical management of the uro-oncology MDTM. | San Luigi Hospital (Tertiary hospital) | Prospective cohort study | Jan 2016–June 2017 | 201 patients/272 discussions |
| El Khoury et al., 2016 [50] | Urological cancers (prostate cancer) | Lebanon | To examine the impact of MDTMs on the management decision for urological cancers. | Notre-Dame de Secours University Medical Centre (University hospital) | Prospective cohort study | July 2012–July 2014. | Prostate: 82 patients |
| Fernando et al., 2017 [20] | Colorectal cancer | New Zealand | The primary objective to determine which patients benefit most from MDTMs, and secondarily to determine whether there was a group of patients which could be managed by protocol without discussion at the MDTM. | Christchurch Hospital (Tertiary hospital) | Prospective case-control study | 1 September 2013–1 November 2014 | Non-MDTM: 182 patients MDTM: 459 patients Total: 641 patients |
| Foucan et al., 2020 [37] | Colorectal cancer (colon cancer) | France | To evaluate the factors associated with the non-presentation in MDTM, and to assess the association between non-MDTM and therapeutic care management. | Multicenter | Retrospective case-control study | 2010 (date not specified) | Non-MDTM: 142 patients MDTM: 431 patients Total: 573 patients |
| Freeman et al., 2015 [40] | Non-small cell lung cancer | US | To compare quality and cost metrics for propensity-matched MDTM patients to patients without access to such care coordination across a geographically diverse system of hospitals. | Multicenter | Retrospective case-control study | 2008–2012 (date not specified) | Non-MDTM: 6627 patients MDTM: 6627 patients Total: 13,254 patients |
| Hung et al., 2020 [46] | Non-small cell lung cancer | Taiwan | To prove MDTM discussion could prolong the average time of survival for patients with stage III NSCLC. | Taipei Veterans General Hospital (General hospital) | Retrospective before–after study | January 2013–December 2018 MDTM implementation February 2016 | Non-MDTM: 273 patients MDTM: 242 patients Total: 515 patients |
| Jung et al., 2018 [21] | Colorectal cancer | Korea | To assess the impact of MDTM on clinical decision making. | Asan Medical Center (Tertiary hospital) | Prospective cohort study | 1 January 2011–31 December 2014 | 1383 patients |
| Karagkounis et al., 2018 [22] | Colorectal cancer (rectal cancer) | US | To determine the frequency and manner in which MDTM changed the management of patients. | Cleveland clinic (University hospital) | Prospective cohort study | July 2015–June 2016 | 316 patients/414 discussions |
| Kurpad et al., 2011 [51] | Genitourinary cancers (prostate cancer) | US | To study the effect of MDTMs on the diagnosis and treatment decisions of new patients. | Lineberger Comprehensive Cancer Center (University hospital) | Prospective cohort study | June 2007–June 2008 | Prostate: 92 patients |
| Lan et al., 2016 [23] | Colorectal cancer | Taiwan | Analyzing and comparing the outcomes of colorectal cancer patients with metastatic disease before and after the era of MDTM. | Taipei Veterans General Hospital (Tertiary hospital) | Before–after study | January 2001–December 2010 MDTM implementation: October 2007 | Non-MDTM: 636 patients MDTM: 439 patients Total: 1075 patients |
| MacDermid et al., 2009 [24] | Colorectal cancer | UK | To assess the effect of this on patient’s survival, and trends in the use of adjuvant chemotherapy. | Royal Alexandra Hospital (General hospital) | Before–after study | January 1997–December 2005 MDTM implementation: June 2002 | Non-MDTM: 176 patients MDTM: 134 patients Total: 310 patients |
| Maurizi et al., 2017 [36] | Colorectal cancer (rectal cancer) | Italy | To evaluate the improvements on rectal cancer treatment outcomes after the introduction of the MDTMs. | Carlo Urbani hospital (General hospital) | Before–after study | January 2014–December 2015 MDTM implementation: January 2015 | Non-MDTM: 30 patients MDTM: 35 patients Total: 65 patients |
| Munro et al., 2015 [25] | Colorectal cancer | UK | To review the effect of MDTM, and implementation of recommendations, on survival. | Hospitals in Tayside region in Eastern Scotland (General hospitals) | Case-control study | 1 January 2006–31 December 2007 Mean follow-up: 73.3 months | Non-MDTM: 175 patients MDTM: 411 patients Total: 586 patients |
| Murthy et al., 2014 [54] | Breast | US | To investigate the role of MDTM on patient management and how this led to treatment modifications. | Saint Barnabas Medical Center (General hospital) | Prospective cohort study | June 2010–June 2011 | 242 patients |
| Muthukrishnan et al., 2020 [47] | Lung cancer | US | To investigate whether early MDTM discussions affected the time required to complete a lung cancer evaluation. | Metrohealth Medical Center (University hospital) | Retrospective case-control study | December 2015–January 2017 | Non-MDTM: 106 patients MDTM: 55 patients Total: 161 patients |
| Nikolovski et al., 2017 [26] | Colorectal cancer | Australia | To determine whether the introduction of MDTM altered the length of time to treatment. | Geelong Hospital (University hospital) | Before–after study | 1 January 2006–3 February 2011 | Non-MDTM Historical control: 56 patients Non-MDTM: 259 patients MDTM: 82 patients Total: 397 patients |
| Palmer et al., 2011 [27] | Colorectal cancer (rectal cancer) | Sweden | To assess outcome in relation to preoperative local and distant staging, with or without MDTM. | Hospitals in Stockholm-Gotland region (University hospitals) | Prospective case-control study | 1995–2004 Follow-up: March 2008 | Non MDTM: 99 patients MDTM: 65 patients Total: 303 patients |
| Pan et al., 2015 [41] | Non-small cell lung cancer | Taiwan | To analyze the factors affecting survival, at each stage of NSCLC. | Multicenter | Retrospective cohort study | 2005–2011 | Non-MDTM: 27,937 patients MDTM: 4632 patients Total: 32,569 patients |
| Rao et al., 2014 [52] | Urological cancers (prostate cancer) | Australia | To analyze the impact of the uro-oncology MDTMs on patient management decisions, and to develop criteria for patient inclusion in MDTMs. | Austin Hospital (Tertiary hospital) | Prospective cohort study | 3 month period in 2012 (date not specified) | Prostate: 47 discussions |
| Richardson et al., 2016 [28] | Colorectal cancer (rectal cancer) | US | To assess whether MDTM participation improves process evaluation, outcomes and technical aspects of surgery. | Baylor University Medical Center (University hospital) | Retrospective before–after study | 2011–2014 MDTM implementation: January 2013 | Non-MDTM: 42 patients MDTM (2013): 41 patients MDTM (2014): 47 patients Total: 130 patients |
| Ryan et al., 2014 [29] | Colorectal cancer | Australia | To evaluate prospectively the colorectal MDTM to determine the utility of the meeting. | Western Health Melbourne (General hospital) | Prospective cohort study | 6 months (date not specified) | 197 patients/261 discussions |
| Scarberry et al., 2018 [53] | Genitourinary cancers (prostate cancer) | US | To prospectively evaluate the effectiveness of MDTM on altering treatment plans. | University hospital Cleveland Medical Center (University hospital) | Prospective cohort study | September 2011–April 2013 | Prostate cancer: 125 patients |
| Schmidt et al., 2015 [42] | Thoracic cancer (lung cancer) | US | To analyze the actual impact of MDTM presentation on decision making in thoracic cancer cases. | Virginia Mason Medical Center (General hospital) | Prospective cohort study | 1 June 2010–31 December 2012 | Lung cancer: 294 patients (451 discussions) |
| Snelgrove et al., 2015 [30] | Colorectal cancer (rectal cancer) | Canada | To assess: (1) the quality of MDTM, (2) the effect of MDTM on the initial treatment plan, (3) compliance with the MDTM treatment recommendation and (4) clinical outcomes. | Mount Sinai Hospital (University hospital) | Prospective cohort study | 1 September 2012–30 June 2013 | 42 patients |
| Stone et al., 2018 [43] | Lung cancer | Australia | To evaluate outcomes including survival, according to MDTM presentation and to explore the utility of data obtained from local clinical sources. | St Vincent’s Hospital (University hospital) | Prospective case-control study | 1 January 2006–31 December 2012 Follow-up: 23 May 2014. | Non-MDTM: 295 patients MDTM: 902 patients Total: 1197 patients |
| Swellengrebel et al., 2011 [31] | Colorectal cancer (rectal cancer) | The Netherlands | To evaluate the additional value of MDTM discussion, with the occurrence of a positive CRM as an endpoint. | Antoni van Leeuwenhoek Netherlands cancer Institute (Tertiary hospital) | Case-control study | January 2006–January 2008 | Non- MDTM: 94 patients MDTM: 116 patients Total: 210 patients |
| Tamburini et al., 2018 [44] | Non-small cell lung cancer | Italy | To evaluate the impact of MDTM on survival of patients undergoing surgery for NSCLC. | Ferrara University Hospital (University hospital) | Before–after study | January 2008–December 2015 MDTM implementation: 2012 | Non-MDTM: 246 patients MDTM: 186 patients Total: 432 patients |
| Tsai et al., 2020 [56] | Breast cancer | Taiwan | To investigate the influence of MDTM on the risk of recurrence and death. | Multicenter | Retrospective case-control study | 2004–2010 | Non-MDTM: 9266 patients MDTM: 9266 patients Total: 18,532 patients |
| Ung et al., 2016 [45] | Lung cancer | Australia | To measure the impact of MDTM on clinicians’ management plans, and the implementation rate of the meeting recommendations. | Peter MacCallum Cancer Centre (Tertiary referral center) | Prospective cohort study | March–May 2011 | 68 patients |
| Vaughan-Shaw et al., 2015 [32] | Colorectal cancer (rectal cancer) | UK | To assess the impact of the introduction of a specialist early rectal cancer MDTM on the investigation and management of rectal cancer. | Cheltenham General Hospital (General hospital) | Before–after study | 24 months (2006 and 2011) MDTM implementation: 2011 | Non-MDTM: 19 patients MDTM: 24 patients Total: 43 patients |
| Wanis et al., 2017 [33] | Colorectal cancer with liver metastasis | Canada | To determine the access to and association between MDTM review and management amongst patients with colorectal cancer and synchronous liver metastases. | London Health Sciences Centre (University Hospital) | Retrospective case-control study | January 2008–June 2015 | Non-MDTM: 37 patients MDTM: 29 patients Total: 66 patients |
| Wille-Jørgensen et al., 2013 [34] | Colorectal cancer (rectal cancer) | Denmark | To compare the outcomes of patients before and after the establishment of MDTMs in the two surgical departments in Copenhagen. | Bispebjerg and Hvidovre Hospitals (University hospitals) | Before–after study | 1 May 2001–31 August 2006 MDTM implementation: September 2004 | Non-MDTM: 467 patients MDTM: 344 patients Total: 811 patients |
| Yang et al., 2020 [57] | Breast cancer | China | To identify which clinicopathological characteristics may influence compliance with MDTM recommendations, and to evaluate whether MDTM compliance affects the prognosis of early breast cancer. | Shanghai Ruijin Hospital (General hospital) | Retrospective cohort study | April 2013–August 2018 Mean follow-up: 32.75 months | 4501 patients |
| Ye et al., 2012 [35] | Colorectal cancer | China | To assess the effect on management of colorectal cancer after the inception of an MDTM. | Peking University People’s Hospital (University hospital) | Before–after study | January 1999–September 2006 MDTM implementation: December 2002 | Non-MDTM: 297 patients MDTM: 298 patients Total: 595 patients |
| Author and Year | Cancer Type | Outcomes | Study Results | |
|---|---|---|---|---|
| Time Management | ||||
| Boxer et al., 2011 [38] | Lung cancer | Time from diagnosis to treatment (days) | Surgery | 50 vs. 42 days, p = 0.49 |
| Curative radiotherapy | 91 vs. 106 days, p = 0.65 | |||
| Palliative radiotherapy | 89 vs. 87 days, p = 0.89 | |||
| Curative chemotherapy | 45 vs. 45 days, p = 0.97 | |||
| Palliative chemotherapy | 44 vs. 60 days, p = 0.03 | |||
| Palliative care | 100 vs. 110 days, p = 0.37 | |||
| Brandão et al., 2020 [55] | Breast cancer | Time from diagnosis to treatment (% patients) | Less than 45 days | 44.7% vs. 51.9% |
| 45 days or longer | 55.3% vs. 48.1% | |||
| p = 0.324 | ||||
| Foucan et al., 2020 [37] | Colorectal cancer (colon cancer) | Time from diagnosis to surgery (days) | All surgeries | 21.7 vs. 34.6 days |
| Emergency surgery | 8.0 vs. 10.1 days | |||
| Non-emergency surgery | 26.2 vs. 38.7 days | |||
| Freeman et al., 2015 [40] | Non-small cell lung cancer | Time from diagnosis to treatment (days) | 32 ± 11 vs. 19 ± 8 days, p < 0.001 | |
| Muthukrishnan et al., 2020 [47] | Lung cancer | Time from diagnosis to treatment (days) | Imaging to staging: Total 49.33 vs. 70.15 days p < 0.001 | |
| Stage I–III 65.45 vs. 75.77 days p = 0.39 | ||||
| Imaging to diagnosis: Total 37.36 vs. 61.71 days p < 0.001 | ||||
| Stage I–III 54.31 vs. 69.71 days p = 0.13 | ||||
| Diagnosis to staging: Total 11.97 vs. 8.44 days p = 0.07 | ||||
| Stage I–III 11.14 vs. 6.06 days p = 0.07 | ||||
| Staging to therapy: Total 25.23 vs. 44.69 days p = 0.01 | ||||
| Stage I–III 24.24 vs. 41.46 days p = 0.03 | ||||
| Diagnosis to therapy: Total 37.20 vs. 53.13 days p = 0.06 | ||||
| Stage I–III 35.37 vs. 47.51 days p = 0.28 | ||||
| Imaging to therapy: Total 74.56 vs. 114.84 days p < 0.001 | ||||
| Stage I–III 89.69 vs. 117.23 days p = 0.15 | ||||
| Nikolovski et al., 2017 [26] | Colorectal cancer | Time from diagnosis to treatment (days) Time from diagnosis to surgery (days) | Historical control vs. MDTM group | Concurrent control vs. MDTM group |
| Total: 19.5 vs. 30 days, p = 0.001 | Total: 18 vs. 30 days, p < 0.001 | |||
| Colon: 14 vs. 18 days, p = 0.338 | Colon: 15 vs. 18 days, p = 0.348 | |||
| Rectal: 25 vs. 32.5 days, p = 0.090 | Rectal: 23 vs. 32.5 days, p < 0.001 | |||
| Total: 17 vs. 22 days, p = 0.061 | Total: 17 vs. 22 days, p = 0.002 | |||
| Colon: 14 vs. 18 days, p = 0.406 | Colon: 15 vs. 18 days, p = 0.384 | |||
| Rectal: 21 vs. 24 days, p = 0.367 | Rectal: 21 vs. 24 days, p = 0.085 | |||
| Stone et al., 2018 [43] | Lung cancer | Time to referral to palliative care for stage IV patients (days) | 26 vs. 69 days | |
| Costs | ||||
| Brandão et al., 2020 [55] | Breast cancer | Cost-effectiveness (USD $) | 3-year cost increase of implementing MDTM: $119.83 per patient. Incremental cost-effectiveness ratio: $802.96 per QALY. MDTM implementation is a cost-effective measure. | |
| Chinai et al., 2013 [19] | Colorectal cancer | Estimated costs (£) | Estimated annual costs of MDTM: £162,734 | |
| Freeman et al., 2015 [40] | Non-small cell lung cancer | Mean cost of care (USD $) | $10,213 vs. $7,212; p < 0.001 | |
| Other | ||||
| Freeman et al., 2015 [40] | Non-small cell lung cancer | (1) Research participation offered (2) Adherence to NCCN guidelines | (1) 6% vs. 17%, p < 0.001 (2) 71% vs. 88%, p < 0.001 | |
| Ryan et al., 2014 [29] | Colorectal cancer | Benefit of MDTM discussion | Discussions were considered beneficial in 26.8% * of all discussions. | |
| Author and Year | Cancer Type | Proportion of Cases with Changed Overall Management Plans | Proportion of Changed Cases Stratified per Stage or MDTM Type | Type of Changes |
|---|---|---|---|---|
| Acher et al., 2005 [48] | Urological cancers (prostate cancer) | 1.6% * | - | - |
| Chinai et al., 2013 [19] | Colorectal cancer | 6.4% | - | - |
| De Luca et al., 2019 [49] | Prostate cancer | 35.8% * | Local disease: 23.2%, advanced disease: 46.9%, metastatic disease: 33.4% | - |
| El Khoury et al., 2016 [50] | Urological cancers (prostate cancer) | 42.7% | Gleason score 6: 27.3% Gleason score 7: 51.7% Gleason score 8: 44.4% Gleason score 9: 50.0% Gleason score 10: 40.0% | - |
| Fernando et al., 2017 [20] | Colorectal cancer | 23% | - | Proportion of changed clinical staging cases: 4% |
| Jung et al., 2018 [21] | Colorectal cancer | 12.9% | Newly diagnosed cancer: 7.6%, recurrence cancer patients: 16.4% (p < 0.001) | Treatment plans overall: 12.9% Nonsurgical treatment in 66.5% of cases, modifications to the surgical approach: 3.4% no treatment: 30.2%. |
| Karagkounis et al., 2018 [22] | Rectal cancer | 26.1% | Initial discussion: 32.4%, Follow-up discussions: 35.2%, Postoperative discussions: 6.3% (p < 0.001) | Diagnostic plan: 9.7% * of cases Treatment plans: 20.5% * Decided to operate: 2.1% * of cases; Decided not to operate: 12.4% *; Changed operative approach: 18.6% *. Neoadjuvant therapy added: 39.2% *; Adjuvant therapy added: 6.2% *. Additional workup biopsy/pathology: 10.3% *; Additional workup imaging: 26.8% *. Changes were more frequent when the pre-MDTM plan was considered tentative by the attending physician (45.5%, p < 0.001). |
| Kurpad et al., 2011 [51] | Urological cancers (prostate cancer) | 50% | - | Treatment changed in 18.5%, diagnosis changed in 6.5%, both diagnosis and treatment changed in 3.3%, other changes in 7.6% and N/A in 14.1% of cases. |
| Murthy et al., 2014 [54] | Breast cancer | 42% | Stage 0: 21%, stage IA: 27%, stage IB: 8%, stage IIA: 15%, stage IIB: 17%, stage IIIA: 7%, stage IIIB: 0%, stage IIIC: 1%, stage IV: 2%. | Surgical treatment: 38.2% of all changes. medical management (chemotherapy/endocrine therapy): 33.3% Radiation treatment: 16.6% Combined medical and radiation therapy: 6.8% Imaging changes (e.g., MRI, mammogram): 4.9% |
| Rao et al., 2014 [52] | Urological cancers (prostate cancer) | 26% | T1: 0%, T2: 25%, T3: 21% (p = 0.62). Localized disease: 23% Metastatic disease: 38% (p < 0.05). | - |
| Scarberry et al., 2018 [53] | Genitourinary cancers (Prostate) | 17.6% | - | - |
| Schmidt et al., 2015 [42] | Lung cancer | 53% | - | Changes in treatment: 41% of cases Staging recommendations changed: 59% of cases |
| Snelgrove et al., 2015 [30] | Rectal cancer | 29% | - | Changes in initial treatment: Primary surgery 58% * Neoadjuvant chemoradiation: 25% * Systemic chemotherapy: 16.7% * |
| Ung et al., 2016 [45] | Lung cancer | 58% | - | Additional investigations: 59% Treatment modality: 19% Treatment intent: 9% Tumor histology: 6% Tumor stage: 6% |
| Author and Year | Cancer Type | Outcomes | Study Results (Proportion of Patients Received) |
|---|---|---|---|
| Imaging/Staging/Diagnostics | |||
| Anania et al., 2019 [17] | Colorectal cancer | (1) Colonoscopy (2) CT (3) MRI (4) Ultrasound | (1) 57.7% * vs 78.4% * (2) 24.4% vs. 82.4%; p < 0.01 (3) 4.4% vs. 62.7%; p < 0.01 (4) 15.6% vs. 23.5%; p = NS |
| Fernando et al., 2017 [20] | Colorectal cancer | (1) CT abdomen (2) CT chest (3) Colonography (4) MRI (5) FDG-PET CT (6) X-ray chest (7) Ultrasound (8) col/sigmoidoscopy (9) biopsy (10) liver function tests (11) Carcinoembryonic antigen | (1) 96.2% vs. 96.3%; p = 0.545 (2) 23.6% vs. 49.5%; p < 0.001 (3) 25.8% vs. 19.6%; p = 0.054 (4) 9.3% vs. 67.5%; p < 0.001 (5) 2.2% vs. 17.9%; p < 0.001 (6) 75.3% vs. 43.4% p < 0.001 (7) 5.5% vs. 6.1%; p = 0.467 (8) 85.7% vs. 89.3%; p = 0.127 (9) 81.9% vs. 88.2%; p = 0.025 (10) 23.6% vs. 29.8%; p = 0.068 (11) 79.1% vs. 78.2%; p = 0.446 |
| Foucan et al., 2020 [37] | Colon cancer | CT scans | 46.6% vs. 66.6%; p < 0.001 |
| Freeman et al., 2015 [40] | NSCLC | Complete staging | 67% vs. 91%; p < 0.001 |
| Maurizi et al., 2017 [36] | Rectal cancer | (1) MRI, (2) CEA testing (3) colonoscopy (4) CT (5) Endoscopic rectal ultrasound (6) Post-therapy preoperative restaging with MRI | (1) 23.33% vs. 51.43%; p = 0.010 (2) 46.67% vs. 65.71%; p = 0.061 (3) 86.67% vs. 85.71; p = 0.456 (4) 90.00% vs. 97.14%; p = 0.116 (5) 16.67% vs. 25.71%; p = 0.188 (6) 26.67% vs. 34.29%; p = 0.254 |
| Richardson et al., 2016 [28] | Rectal cancer | (1) Colonoscopy | (1) 95% vs. 100% (MDTM year 1) vs. 96% (MDTM year (2) p = 0.3828 |
| Palmer et al., 2011 [27] | Rectal cancer | Preoperative local staging: (1) MRI exams (2) Endorectal ultrasonography Preoperative distant staging (3) CT/MRI abdomen (4) Ultrasound abdomen (5) Chest CT or X-ray | (1) 89.9% * vs. 98.5% * (2) 21.2% * vs 4.6% * (3) 57.6% * vs. 75.4% * (4) 52.5% * vs 40.0% * (5) 100% * vs 100%* |
| Tamburini et al., 2018 [44] | NSCLC | Rate of complete preoperative evaluation | 64% vs. 93% (p < 0.001). |
| Ye at al. 2012 [35] | Colorectal cancer | (1) CT examination performed before operation (2) CT TNM staging performed before operation (3) accurate TNM staging | (1) 30.3% vs. 55.7%; p < 0.001 (2) 41.1% vs. 81.3%; p < 0.001 (3) 45.9% vs. 64.0%; p = 0.044 |
| Surgery | |||
| Anania et al., 2019 [17] | Colorectal cancer | Surgical type: (1) Total mesorectal excision (2) Laparoscopic total mesorectal excision (3) Open miles procedure (4) Laparoscopic miles procedure | (1) 2.2% vs. 13.7% (2) 88.9% vs. 68.6% (3) 2.2% vs. 0% (4) 6.7% vs 17.6 |
| Boxer et al., 2011 [38] | Lung cancer | (1) Surgery (2) Surgery stratified per stage | (1) 13% vs. 12%; p = 0.84 (2) NSCLC stages I +II (61% vs. 49%; p = 0.25) NSCLC stage III (26% vs. 16%; p = 0.16) NSCLC stage IV (0% vs. 2%; p = 0.13) |
| Brandão et al., 2020 [55] | Breast cancer | (1) Surgery (ever) (2) Surgery type (first treatment) (a) Total mastectomy (b) Tumorectomy | (1) 80.6% vs. 82.2% (p = 0.858) (2) (a) 94.9% vs. 89.8% (b) 5.1% vs. 10.2 p = 0.257 |
| Foucan et al., 2020 [37] | Colon cancer | Surgery | 61.3% vs. 86.8%; p = 0.004 |
| Freeman et al., 2015 [40] | NSCLC | Non-therapeutic surgical procedure | 4% vs. 2%; p < 0.001 |
| Lan et al., 2016 [23] | Colorectal cancer | Surgical resection of: (1) primary tumor (2) metastatic foci (3) liver metastasis (4) lung metastasis | (1) 88.5% vs 82.7%; p = 0.007 (2) 21.7% vs. 29.8%; p = 0.003 (3) 19.6% vs. 35.2%; p < 0.001 (4) 12.4% vs. 14.3%; p = 0.803 |
| Muthukrishnan et al., 2020 [47] | Lung cancer | Surgery | 17.0% vs. 16.4% |
| Palmer et al.* 2011 [27] | Rectal cancer | Types of surgery: (1) no surgery (2) explorative laparotomy (3) resection of rectal cancer | (1) 4.0% vs. 7.7% (2) 21.1% vs. 10.8% (3) 74.7% vs. 81.5% p = 0.024 |
| Richardson et al., 2016 [28] | Rectal cancer | (1) Appropriate abdomino-peritoneal resections treatment (2) Surgical type: (a) Transanal (minimally) invasive surgery (b) Low Anterior Resection (c) Transanal Transabdominal Low Anterior Resection (d) Abdominal-peritoneal resection | (1) 50% vs. 71% (MDTM year 1) vs. 78% (MDTM year 2); p = 0.191 (2) (a) 22% vs. 18% (MDTM year 1) vs. 9% (MDTM year 2) (b) 69% vs. 63% (MDTM year 1) vs. 40% (MDTM year 2) (c) 0% vs. 3% (MDTM year 1) vs. 7% (MDTM year 2) (d) 10% vs. 18% (MDTM year 1) vs. 43% (MDTM year 2); p = 0.002 |
| Swellengrebel et al., 2011 [31] | Rectal cancer | (1) Surgical type: (a) Low Anterior Resection (b) Hartmann procedure (c) Abdominal Perineal Resection (d) No surgery | (1) (a) 71% vs 41% (b) 9% vs 17% (c) 19% vs 40% (d) 1% vs 2% |
| Tamburini et al., 2018 [44] | NSCLC | (1) Surgical type: (a) video-assisted thoracoscopic surgery (b) exploratory thoracotomy | (1) (a) 48% vs. 9%; p = 0.001 (b) 3% vs 1.8%; p = 0.31 |
| Vaughan-Shaw et al., 2015 [32] | Rectal cancer | Surgical treatment: (1) local excision (2) less resection (3) declined surgery | (1) 15.8% vs 83.3% (2) 79.0% vs. 16.7% (3) 5.3% vs. 0% |
| Wanis et al., 2017 [33] | Colorectal cancer with liver metastasis | Resection order | MDTM group significantly more likely (p < 0.001) to undergo simultaneous resection of the primary colorectal tumor and liver metastases. |
| Wille-Jørgensen et al., 2013 [34] | Rectal cancer | Surgery | 88% vs. 86% |
| Radiotherapy and Chemotherapy | |||
| Boxer et al., 2011 [38] | Lung cancer | (1) Radiotherapy (a) overall (b) stratified per NSCLC stage (c) stratified per SCLC stage (2) Chemotherapy (a) overall (b) stratified per NSCLC stage (c) stratified per SCLC stage | (1) (a) 33% vs. 66%; p < 0.001. (b) stages I + II (17% vs. 54%; p < 0.001) stage III (46% vs. 71%; p = 0.01) stage IV (43% vs. 68%; p < 0.001) (c) limited stage (71% vs. 89%; p = 0.28), extensive stage (46% vs. 50%; p = 0.72). (2) (a) 29% vs. 46%; p = 0.001. (b) stages I + II (15% vs. 18%; p = 0.67), stage III (39% vs. 43%; p = 0.72), stage IV (29% vs. 42%; p = 0.01), (c) SCLC limited stage (71% vs. 100%; p = 0.72), SCLC extensive stage (76% vs. 75%; p = 0.89). |
| Brandão et al., 2020 [55] | Breast cancer | (1) Radiotherapy (first treatment) (2) Chemotherapy | (1) p = 0.175 (2) 91.8% vs. 96.3%; p = 0.237 |
| Bydder et al., 2009 [39] | NSCLC | (1) Radical radiotherapy/Chemoradiotherapy (2) Chemotherapy | (1) 6% vs. 10%; p = 0.318 (2) 29% vs. 42%; p = 0.141 |
| Freeman et al., 2015 [40] | NSCLC | Radio and/or chemotherapy before tissue diagnosis | 5% vs. 3%; p < 0.001 |
| Lan et al., 2016 [23] | Colorectal cancer | (1) Chemotherapy (2) Radiotherapy | (1) 75.9% vs. 83.8 %; p = 0.002 (2) 9.6% vs. 20.5 %; p < 0.001 |
| MacDermid et al., 2009 [24] | Colorectal cancer | (1) Primary adjuvant chemotherapy (a) Overall (b) Dukes B (c) Dukes C (2) Preoperative radiotherapy | (1) (a) 13% vs. 31.3%; p < 0.001 (b)1.5% vs. 17.6%; p = 0.002 (c) 31.9% vs. 58.6%; p = 0.004(2) 24.4% vs. 32.5%; p = 0.462 |
| Muthukrishnan et al., 2020 [47] | Lung cancer | (1) Radiation (2) Chemotherapy (3) Chemo-radiation. | (1) 17.9% vs. 20.0% (2) 14.2% vs. 18.2% (3) 28.3% vs. 32.7% |
| Palmer et al., * 2011 [27] | Rectal cancer | Preoperative treatments: (1) No treatment (2) Short radiotherapy (3) Long radiotherapy (4) Radio-chemotherapy (5) Chemotherapy (6) Unknown | (1) 42.4% vs. 21.5% (2) 41.4% vs. 13.8% (3) 5.1% vs. 30.8% (4) 9.1% vs. 29.2% (5) 1.0% vs 1.5% (6) 1.0% vs. 3.1% |
| Wanis et al., 2017 [33] | Colorectal cancer with liver metastasis | Chemotherapy | NS |
| Wille-Jørgensen et al., 2013 [34] | Rectal cancer | Preoperative (chemo)radiotherapy | 19% vs. 25% |
| Ye et al., 2012 [35] | Colorectal cancer | (1) Adjuvant chemotherapy (a) Overall (b) stage I (c) stage IIA (d) stage IIB (e) stage IIIA (f) stage IIIB (g) stage IIIC (h) stage IV (2) Adjuvant radiotherapy | (1) (a) 82.8%* vs. 49.3% *; p < 0.001 (b) 64.4%* vs 0% *; p < 0.001 (c) 82.2%* vs. 12.2% *; p < 0.001 (d) 80.0%* vs. 100% *; p = 0.183 (e) 84.6%* vs. 90.9%; p = 0.577 (f) 93.0% * vs. 91.1% *; p = 0.728 (g) 93.1% * vs. 86.1% *; p = 616 (h) 83.3% * vs. 88.4% *; p = 0.750 2) 0.3% * vs. 10.1% *; p < 0.001 |
| Palliative Care and Hospice Referral | |||
| Boxer et al., 2011 [38] | Lung cancer | Referral to palliative care | 53% vs 66%; p < 0.001 |
| Bydder et al., 2009 [39] | NSCLC | (1) Palliative radiotherapy only (2) Palliative care only | (1) 35% vs. 25%; p = 0.152 (2) 29% vs. 23%; p = 0.204 |
| Freeman et al., 2015 [40] | NSCLC | Palliative or hospice care | 4% vs. 9%; p < 0.001 |
| MacDermid et al., 2009 [24] | Colorectal cancer | Palliative chemotherapy | 32.5% vs. 44%; p = 0.431 |
| Muthukrishnan et al., 2020 [47] | Lung cancer | Hospice referral | 22.6% vs. 12.7% |
| Stone et al., 2018 [43] | Lung cancer | Referral to palliative care | 78.0% vs. 85.3%; p = 0.06 |
| Other | |||
| Anania et al., 2019 [17] | Colorectal cancer | Neo-adjuvant therapy | The MDTM cohort showed a significantly higher use of neo-adjuvant therapy (22.2% vs. 56.9%; p < 0.01). |
| Brandão et al., 2020 [55] | Breast cancer | Endocrine therapy (first treatment) | p = 0.888 |
| Bydder et al., 2009 [39] | NSCLC | ‘Active’ treatment | 35% vs. 52%; p = 0.288 |
| Foucan et al., 2020 [37] | Colon cancer | Treatment type (surgery and chemotherapy): (1) Overall (2) Stratified per stage: (a) Stage I (b) Stage II (c) Stage III (d) Stage IV | (1) NS (2) (a) p = 1.00 (b) 0.869 (c) p = 0.042 (d) p < 0.001 |
| Maurizi et al., 2017 [36] | Rectal cancer | Neoadjuvant therapy | 33.33% vs. 42.86%; p = 0.216 |
| Tsai et al., 2020 [56] | Breast cancer | Treatment combinations | p = 0.211 |
| Author and Year | Cancer Type | Outcomes | Study Results |
|---|---|---|---|
| Survival | |||
| Brandão et al., 2020 [55] | Breast cancer | (1) 3-year survival (2) 3-year survival—disease-free stage 0–III (3) 3-year survival—overall stage 0–III (4) Survival duration—stage IV | (1) 44.8% vs. 62.6% p = 0.039 (2) 41.7% vs. 56.8% p = 0.103 (3) 48.0% vs. 73.0% p = 0.003 (4) 19.4 months vs. 13.6 months (median) p = 0.059 |
| Bydder et al., 2009 [39] | NSCLC | (1) 1-year survival (2) Survival duration | (1) 18% vs. 33% (2) 208 days vs. 237 days (median), 205 days vs. 280 days (mean), p = 0.048 |
| Chen et al., 2018 [18] | CRA-LLM | (1) 1-year survival (2) 3-year survival (3) 5-year survival (4) 5-year survival—curative treatment | (1) 53.45% vs. 74.52% p < 0.001 (2) 24.21% vs. 48.75% p < 0.001 (3) 17.41% vs. 44.32% p < 0.001 (4) 41.31% vs. 64.57% p = 0.062 |
| Foucan et al., 2020 [37] | Colon cancer | Survival duration | After diagnosis 264.9 days vs. 338.0 days p = 0.014 After surgery 252.1 days vs. 312.2 days p = 0.068 |
| Hung et al., 2020 [46] | Stage III NSCLC | Survival duration | 25.7 months vs. 41.2 months, p = 0.018 (median) |
| Lan et al., 2016 [23] | Colorectal cancer | (1) 3-year survival (2) 3-year survival—liver metastasis (3) 3-year survival—lung metastasis | (1) 25.4% vs. 38.2% p < 0.001 (2) 22.3% vs. 32.9% p < 0.001 (3) 24.5% vs. 42.6% p < 0.001 |
| MacDermid et al., 2009 [24] | Colorectal cancer | (1) 3-year survival—Dukes B (2) 3-year survival—Dukes C (3) Survival duration—surgical treatment for metastatic disease | (1) 76% vs. 70% p = 0.486 (2) 58% vs. 66% p = 0.023 (3) 8 months vs. 11.9 months; p = 0.234 (median) |
| Munro et al., 2015 [25] | Colorectal cancer | (1) 5-year survival (2) 5-year survival—cause-specific (CSS) (3) 5-year survival—early disease (4) 5-year survival—advanced disease (5) survival—>6 weeks after diagnosis | (1) 33.6% vs. 52.3% p < 0.001 (2) 48.2% vs. 63.1% p < 0.001 (3) 86.4% vs. 80.6% p = 0.598 (4) 8.4% vs. 18.0% p < 0.001 (5) 57.7% vs. 63.2% p = 0.064 |
| Palmer et al., 2011 [27] | Rectal cancer | (1) 5-year survival (2) 5-year survival—resected without metastasis | (1) 28% vs. 30% (2) 52% vs. 34% |
| Pan et al., 2015 [41] | Non-small cell lung cancer | 2-year survival—stage-specific | Stage I 78% vs. 81% Stage II 59% vs. 64% Stage III 31% vs. 37% Stage IV 20% vs. 22% |
| Stone et al., 2018 [43] | Lung cancer | Survival probability—HR | 0.54 95% CI 0.45–0.65 a p < 0.001 0.70 95% CI 0.58–0.85 b p < 0.001 |
| Tamburini et al., 2018 [44] | Non-small cell lung cancer | Survival—OR | 0.48 95% CI 0.25–0.92 |
| Wille-Jørgensen et al., 2013 [34] | Rectal cancer | Survival | No significant differences in survival, p = 0.33 |
| Yang et al., 2020 [57] | Breast cancer | (1) Survival (2) Survival—HR (3) Survival—disease-free (4) Survival—disease-free (HR) (5) Survival—disease-free per treatment (HR) | (1) 97.19% vs. 98.98% p < 0.001 (2) 2.760, 95% CI 1.642–4.641 a p < 0.001 2.478, 95% CI 1.431–4.291b p = 0.001 (3) 89.69% vs. 93.89% p < 0.001 (4) 1.888 95% CI 1.451–2.456 a p < 0.001 1.813 95% CI 1.367-2.405 b p < 0.001 (5) Chemotherapy 1.502, 95% CI 1.033–2.183 b p = 0.131 Radiotherapy 2.313, 95% CI 1.540–3.475 b p < 0.001 Endocrine therapy 2.482, 95% CI 1.560–3.947 b p < 0.001 Targeted therapy 1.763, 95% CI 1.001–3.105 b p = 0.095 |
| Ye et al., 2012 [35] | Colorectal cancer | (1) 1-year survival (2) 3-year survival (3) 5-year survival | (1) 94.5% vs. 95.8% (2) 75.7% vs. 87.1% (3) 62.4% vs. 79.1% p = 0.015 |
| Recurrence or Metastasis | |||
| Brandão et al., 2020 [55] | Breast cancer | Recurrence | 29% vs. 18%, p = 0.07 |
| Richardson et al., 2016 [28] | Rectal cancer | Recurrence | Local only 10% vs. 0% (MDTM year 1) vs. 0% (MDTM year 2) Distant only 5% vs. 0% (MDTM year 1) vs. 2% (MDTM year 2) Local and distant 5% vs. 0% (MDTM year 1) vs. 0% (MDTM year 2) |
| Tsai et al., 2020 [56] | Breast cancer | Recurrence—HR | 0.84, 95% CI 0.70-0.99 b p = 0.047 |
| Wille-Jørgensen et al., 2013 [34] | Rectal cancer | (1) Local recurrence (2) Distant metastasis | (1) 4% vs. 3% (NS) (2) 15% vs. 21% (NS) |
| Ye et al., 2012 [35] | Colorectal cancer | (1) Recurrence rate | (1) Lower tumor recurrence in the MDTM group: p < 0.001 |
| Mortality | |||
| Brandão et al., 2020 [55] | Breast cancer | (1) HR of death (2) HR for recurrence or death (3) Death | (1) Overall population 0.77 (95% CI, 0.49–1.19) b Stage 0–III 0.47 (95% CI, 0.27–0.81) b (2) Overall population 0.72 (95% CI, 0.46–1.13) b (3) 23% vs. 10%, p = 0.07 |
| Chen et al., 2018 [18] | CRA-LLM | HR of death | 1.949 95% Cl 1.299–2.923 a p < 0.001 0.403 95% CI 0.251–0.647 b p < 0.001 |
| Lan et al., 2016 [23] | Colorectal cancer | Surgical mortality | 4.9% vs. 2.5%, p = 0.049 |
| Munro et al., 2015 [25] | Colorectal cancer | HR for death | 0.53, 95% CI 0.40–0.69 a p < 0.001 0.73, 95% CI 0.53–1.00 b p = 0.047 |
| Pan et al., 2015 [41] | Non-small cell lung cancer | (1) Death rate and HR of death—stage-specific | (1) Stage I–II 84.65% vs. 15.36% 0.89, 95% CI 0.78–1.01 b p = 0.060 Stage III–IV 85.97% vs. 14.03% 0.87, 95% CI 0.84–0.90 b p < 0.001 |
| Tamburini et al., 2018 [44] | Non-small cell lung cancer | (1) Mortality | 18% vs. 8%; p = 0.006 |
| Tsai et al., 2020 [56] | Breast cancer | (1) Mortality (2) Risk of mortality—HR | (1) 13.05% vs. 12.48% (2) 0.89, 95% CI 0.82–0.96 p = 0.004 |
| Wille-Jørgensen et al., 2013 [34] | Rectal cancer | Post-operative mortality | 9% vs. 5% p = 0.007 |
| Other | |||
| Brandão et al., 2020 [55] | Breast cancer | (1) Clean surgical margins (2) Axillary surgery completeness: (a) Complete (b) incomplete | (1) 88.4% vs. 92.3% p = 0.575 (2) (a) 58.4% vs. 67.9% (b) 29.9% vs. 21.4% p = 0.423 |
| Richardson et al., 2016 [28] | Colorectal cancer (rectal cancer) | (1) Time to recurrence (months) (2) Quality of surgery | (1) 27 months vs. 14.5 months (MDTM year 1) vs. 6.5 months (MDTM year 2) (2) Completeness of TME (Complete/Nearly complete) 6% vs. 61% (MDTM year 1) vs. 76% (MDTM year 2) |
| Swellengrebel et al., 2011 [31] | Rectal cancer | Positive circumferential resection margins rate | 10% vs. 14% p = 0.392 |
| Tamburini et al., 2018 [44] | NSCLC | (1) completeness of resection (2) postoperative complications | (1) 92.4% vs. 94.1% p = 0.52 (2) 40.6% vs. 40.0% p = 0.91 |
| Ye et al., 2012 [35] | Colorectal cancer | Time to recurrence (months) | 11.0 vs. 14.1 months p < 0.001 |
| Colorectal Cancer | Lung Cancer | Breast Cancer | Prostate Cancer | |
|---|---|---|---|---|
| Process outcomes | Time to treatment: increased in MDTM group [26,37] | Time to treatment: increased in MDTM group [38,47], no effect [38], decreased in MDTM group [40] Costs: mean cost of care reduced in MDTM group [40] Other: increased guideline adherence and research participation in MDTM group [40] | Time to treatment: no effect [55] Costs: MDTM is cost-effective [55] | N/A |
| Proportion of cases with changed overall management plans in % | Range: 6–29% Weighted average: 16.2% [19,20,21,22,30] | Range: 53–58% Weighted average: 53.2% [42,45] | Range: 42.1% Weighted average: - [54] | Range: 1.6–43% Weighted average: 27.1% [48,49,50,51,52,53] |
| Diagnostics, treatments and palliative care | MRI: increase in MDTM group [17,20,36] CT: increase in MDTM group [17,20,35,37], no effect [20,36] US: no effect [17,20,36] Colonoscopy: no effect [20,28,36] Surgery: reduced in MDTM group [23,37] Surgery type: significant effect [27,28,33] Radiotherapy: increase in MDTM group [23], no effect [24] Chemotherapy: increase in MDTM group [23], decrease or no effect in MDTM group [35] Palliative care: increase in MDTM group [23], no effect [24] | Diagnostics: N/A Surgery: no effect [38], reduced in MDTM group [40] Surgery type: significant effect [44] Radiotherapy: increase in MDTM group [38], no effect [39] Chemotherapy: increase in MDTM group [38], no effect [39] Palliative care: increase in MDTM group [38,40], no effect [39,43] | Diagnostics: N/A Surgery: no effect [55] Surgery type: no effect [55] Radiotherapy: no effect [55] Chemotherapy: no effect [55] Palliative care: no effect [56] | N/A |
| Patient outcomes | Survival: improved in MDTM group [18,23,24,25,35,37], no effect [34] | Survival: improved in MDTM group [39,41,43,44,46] | Survival: improved in MDTM group [55,56,57] | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kočo, L.; Weekenstroo, H.H.A.; Lambregts, D.M.J.; Sedelaar, J.P.M.; Prokop, M.; Fütterer, J.J.; Mann, R.M. The Effects of Multidisciplinary Team Meetings on Clinical Practice for Colorectal, Lung, Prostate and Breast Cancer: A Systematic Review. Cancers 2021, 13, 4159. https://doi.org/10.3390/cancers13164159
Kočo L, Weekenstroo HHA, Lambregts DMJ, Sedelaar JPM, Prokop M, Fütterer JJ, Mann RM. The Effects of Multidisciplinary Team Meetings on Clinical Practice for Colorectal, Lung, Prostate and Breast Cancer: A Systematic Review. Cancers. 2021; 13(16):4159. https://doi.org/10.3390/cancers13164159
Chicago/Turabian StyleKočo, Lejla, Harm H. A. Weekenstroo, Doenja M. J. Lambregts, J. P. Michiel Sedelaar, Mathias Prokop, Jurgen J. Fütterer, and Ritse M. Mann. 2021. "The Effects of Multidisciplinary Team Meetings on Clinical Practice for Colorectal, Lung, Prostate and Breast Cancer: A Systematic Review" Cancers 13, no. 16: 4159. https://doi.org/10.3390/cancers13164159
APA StyleKočo, L., Weekenstroo, H. H. A., Lambregts, D. M. J., Sedelaar, J. P. M., Prokop, M., Fütterer, J. J., & Mann, R. M. (2021). The Effects of Multidisciplinary Team Meetings on Clinical Practice for Colorectal, Lung, Prostate and Breast Cancer: A Systematic Review. Cancers, 13(16), 4159. https://doi.org/10.3390/cancers13164159