
Urinary PGE-M in Men with Prostate Cancer

 , ,
, , 
Abstract
:Simple Summary
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Laboratory Assay for Urinary PGE-M Measurement
2.3. Assessment of Aspirin Use
2.4. Statistical Analysis
3. Results
3.1. Clinical and Demographic Characteristics of Participants in the NCI–Maryland (NCI–MD) Prostate Cancer Case–Control Study
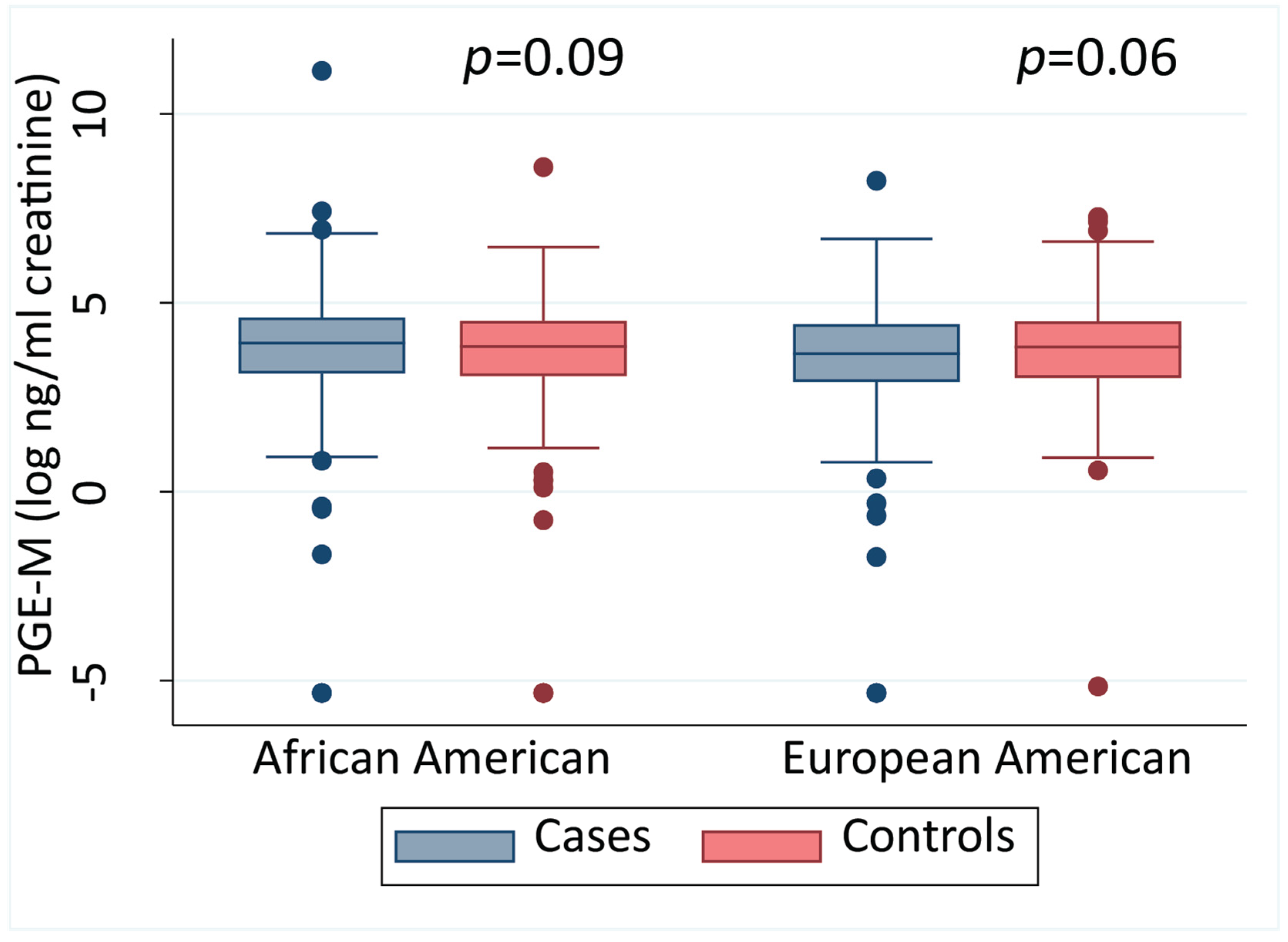
3.2. Urinary PGE-M Levels Do Not Differ between Men with Prostate Cancer and Population-Based Controls
3.3. High PGE-M Is Associated with Moderately Decreased Odds of Prostate Cancer in EA Men in the Multivariable Analysis
3.4. PGE-M and Prostate Cancer Mortality
3.5. Aspirin Use Attenuates the Association between Elevated PGE-M and All-Cause Mortality in Prostate Cancer Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Tang, W.; Wallace, T.A.; Yi, M.; Magi-Galluzzi, C.; Dorsey, T.H.; Onabajo, O.O.; Obajemu, A.; Jordan, S.V.; Loffredo, C.A.; Stephens, R.M.; et al. IFNL4-DeltaG Allele Is Associated with an Interferon Signature in Tumors and Survival of African-American Men with Prostate Cancer. Clin. Cancer Res. 2018, 24, 5471–5481. [Google Scholar] [CrossRef] [Green Version]
- Gurel, B.; Lucia, M.S.; Thompson, I.M., Jr.; Goodman, P.J.; Tangen, C.M.; Kristal, A.R.; Parnes, H.L.; Hoque, A.; Lippman, S.M.; Sutcliffe, S.; et al. Chronic Inflammation in Benign Prostate Tissue is Associated with High-Grade Prostate Cancer in the Placebo Arm of the Prostate Cancer Prevention Trial. Cancer Epidemiol. Biomark. Prev. 2014, 23, 847–856. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klink, J.C.; Banez, L.L.; Gerber, L.; Lark, A.; Vollmer, R.T.; Freedland, S.J. Intratumoral Inflammation is Associated with More Aggressive Prostate Cancer. World J. Urol. 2013, 31, 1497–1503. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.G.; Zhou, X.K.; Milne, G.L.; Goldstein, D.; Hawks, L.C.; Dang, C.T.; Modi, S.; Fornier, M.N.; Hudis, C.A.; Dannenberg, A.J. Increased Levels of Urinary PGE-M, a Biomarker of Inflammation, Occur in Association with Obesity, Aging, and lung Metastases in Patients with Breast Cancer. Cancer Prev. Res. 2013, 6, 428–436. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardsen, E.; Uglehus, R.D.; Due, J.; Busch, C.; Busund, L.-T. COX-2 is Overexpressed in Primary Prostate Cancer with Metastatic Potential and may Predict Survival. A Comparison Study between COX-2, TGF-β, IL-10 and Ki67. Cancer Epidemiol. 2010, 34, 316–322. [Google Scholar] [CrossRef]
- Garg, R.; Blando, J.M.; Perez, C.J.; Lal, P.; Feldman, M.D.; Smyth, E.M.; Ricciotti, E.; Grosser, T.; Benavides, F.; Kazanietz, M.G. COX-2 Mediates pro-Tumorigenic Effects of PKCε in Prostate Cancer. Oncogene 2018, 37, 4735–4749. [Google Scholar] [CrossRef]
- Ko, C.; Lan, S.; Lu, Y.; Cheng, T.; Lai, P.; Tsai, C.; Hsu, T.; Lin, H.; Shyu, H.; Wu, S. Inhibition of Cyclooxygenase-2-Mediated Matriptase Activation Contributes to the Suppression of Prostate Cancer Cell Motility and Metastasis. Oncogene 2017, 36, 4597–4609. [Google Scholar] [CrossRef]
- Mason, M.D.; Clarke, N.W.; James, N.D.; Dearnaley, D.P.; Spears, M.R.; Ritchie, A.W.S.; Attard, G.; Cross, W.; Jones, R.J.; Parker, C.C.; et al. Adding Celecoxib With or Without Zoledronic Acid for Hormone-Naïve Prostate Cancer: Long-Term Survival Results From an Adaptive, Multiarm, Multistage, Platform, Randomized Controlled Trial. J. Clin. Oncol. 2017, 35, 1530–1541. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Dubois, R.N. The role of COX-2 in Intestinal Inflammation and Colorectal Cancer. Oncogene 2010, 29, 781–788. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Fu, L.; Sun, H.; Guo, L.; DuBois, R.N. Prostaglandin E2 Promotes Colorectal Cancer Stem Cell Expansion and Metastasis in Mice. Gastroenterology 2015, 149, 1884–1895.e4. [Google Scholar] [CrossRef] [Green Version]
- Cen, B.; Lang, J.D.; Du, Y.; Wei, J.; Xiong, Y.; Bradley, N.; Wang, D.; DuBois, R.N. Prostaglandin E2 Induces miR675-5p to Promote Colorectal Tumor Metastasis via Modulation of p53 Expression. Gastroenterology 2020, 158, 971–984. [Google Scholar] [CrossRef] [PubMed]
- Catella, F.; Nowak, J.; Fitzgerald, G.A. Measurement of Renal and Non-Renal Eicosanoid Synthesis. Am. J. Med. 1986, 81, 23–29. [Google Scholar] [CrossRef]
- Frölich, J.; Wilson, T.W.; Sweetman, B.J.; Smigel, M.; Nies, A.S.; Carr, K.; Watson, J.T.; Oates, J.A. Urinary prostaglandins. Identification and Origin. J. Clin. Investig. 1975, 55, 763–770. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnson, J.C.; Schmidt, C.R.; Shrubsole, M.J.; Billheimer, D.D.; Joshi, P.R.; Morrow, J.D.; Heslin, M.J.; Washington, M.K.; Ness, R.M.; Zheng, W. Urine PGE-M: A Metabolite of Prostaglandin E2 as a Potential Biomarker of Advanced Colorectal Neoplasia. Clin. Gastroenterol. Hepatol. 2006, 4, 1358–1365. [Google Scholar] [CrossRef]
- Kim, S.; Campbell, J.; Yoo, W.; Taylor, J.A.; Sandler, D.P. Systemic Levels of Estrogens and PGE2 Synthesis in Relation to Postmenopausal Breast Cancer Risk. Cancer Epidemiol. Prev. Biomark. 2017, 26, 383–388. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Wang, J.; Du, J.; Xu, H.; Zhang, W.; Ni, Q.-X.; Yu, H.; Risch, H.A.; Gao, Y.-T.; Gao, Y. Urinary Prostaglandin E 2 Metabolite and Pancreatic Cancer Risk: Case-Control Study in Urban Shanghai. PLoS ONE 2015, 10, e0118004. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, T.; Cai, H.; Zheng, W.; Michel, A.; Pawlita, M.; Milne, G.; Xiang, Y.-B.; Gao, Y.-T.; Li, H.-L.; Rothman, N. A Prospective Study of Urinary Prostaglandin E2 Metabolite, Helicobacter Pylori Antibodies, and Gastric Cancer Risk. Clin. Infect. Dis. 2017, 64, 1380–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnard, M.E.; Beeghly-Fadiel, A.; Milne, G.L.; Akam, E.Y.; Chan, A.T.; Eliassen, A.H.; Rosner, B.A.; Shu, X.-O.; Terry, K.L.; Xiang, Y.-B. Urinary PGE-M Levels and Risk of Ovarian Cancer. Cancer Epidemiol. Prev. Biomark. 2019, 28, 1845–1852. [Google Scholar] [CrossRef] [Green Version]
- De Marzo, A.M.; Platz, E.A.; Sutcliffe, S.; Xu, J.; Gronberg, H.; Drake, C.G.; Nakai, Y.; Isaacs, W.B.; Nelson, W.G. Inflammation in Prostate Carcinogenesis. Nat. Rev. Cancer 2007, 7, 256–269. [Google Scholar] [CrossRef] [Green Version]
- Bibbins-Domingo, K. Aspirin Use for the Primary Prevention of Cardiovascular Disease and Colorectal Cancer: US Preventive Services Task Force recommendation statement. Ann. Intern. Med. 2016, 164, 836–845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dehmer, S.P.; Maciosek, M.V.; Flottemesch, T.J.; LaFrance, A.B.; Whitlock, E.P. Aspirin for the Primary Prevention of Cardiovascular Disease and Colorectal Cancer: A Decision Analysis for the US Preventive Services Task Force. Ann. Intern. Med. 2016, 164, 777–786. [Google Scholar] [CrossRef] [Green Version]
- Drew, D.A.; Schuck, M.M.; Magicheva-Gupta, M.V.; Stewart, K.O.; Gilpin, K.K.; Miller, P.; Parziale, M.P.; Pond, E.N.; Takacsi-Nagy, O.; Zerjav, D.C. Effect of Low-Dose and Standard-Dose Aspirin on PGE2 Biosynthesis Among Individuals with Colorectal Adenomas: A Randomized Clinical Trial. Cancer Prev. Res. 2020, 13, 877–888. [Google Scholar] [CrossRef]
- Tang, W.; Fowke, J.H.; Hurwitz, L.M.; Steinwandel, M.; Blot, W.J.; Ambs, S. Aspirin Use and Prostate Cancer among African-American Men in the Southern Community Cohort Study. Cancer Epidemiol. Prev. Biomark. 2021, 30, 539–544. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.J.; Dorsey, T.H.; Tang, W.; Jordan, S.V.; Loffredo, C.A.; Ambs, S. Aspirin Use Reduces the Risk of Aggressive Prostate Cancer and Disease Recurrence in African-American Men. Cancer Epidemiol. Prev. Biomark. 2017, 26, 845–853. [Google Scholar] [CrossRef] [Green Version]
- Downer, M.K.; Allard, C.B.; Preston, M.A.; Gaziano, J.M.; Stampfer, M.J.; Mucci, L.A.; Batista, J.L. Regular Aspirin Use and the Risk of Lethal Prostate Cancer in the Physicians’ Health Study. Eur. Urol. 2017, 72, 821–827. [Google Scholar] [CrossRef]
- Hurwitz, L.M.; Joshu, C.E.; Barber, J.R.; Prizment, A.E.; Vitolins, M.Z.; Jones, M.R.; Folsom, A.R.; Han, M.; Platz, E.A. Aspirin and Non-Aspirin NSAID Use and Prostate Cancer Incidence, Mortality, and Case Fatality in the Atherosclerosis Risk in Communities Study. Cancer Epidemiol Biomark. Prev. 2019, 28, 563–569. [Google Scholar] [CrossRef] [Green Version]
- Minas, T.Z.; Tang, W.; Smith, C.J.; Onabajo, O.O.; Obajemu, A.; Dorsey, T.H.; Jordan, S.V.; Obadi, O.M.; Ryan, B.M.; Prokunina-Olsson, L.; et al. IFNL4-DeltaG is Associated with Prostate Cancer Among men at Increased Risk of Sexually Transmitted Infections. Commun. Biol. 2018, 1, 191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphey, L.J.; Williams, M.K.; Sanchez, S.C.; Byrne, L.M.; Csiki, I.; Oates, J.A.; Johnson, D.H.; Morrow, J.D. Quantification of the Major Urinary Metabolite of PGE2 by a Liquid Chromatographic/Mass Spectrometric Assay: Determination of Cyclooxygenase-Specific PGE2 Synthesis in Healthy Humans and those with Lung Cancer. Anal. Biochem. 2004, 334, 266–275. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. The NCCN Clinical Practice Guidelines in Oncology for Prostate Cancer, V4. 2019. Available online: https://www.nccn.org/professionals/physician_gls/default.aspx#prostate (accessed on 16 November 2020).
- Ogino, S.; Kirkner, G.J.; Nosho, K.; Irahara, N.; Kure, S.; Shima, K.; Hazra, A.; Chan, A.T.; Dehari, R.; Giovannucci, E.L. Cyclooxygenase-2 Expression is an Independent Predictor of Poor Prognosis in Colon Cancer. Clin. Cancer Res. 2008, 14, 8221–8227. [Google Scholar] [CrossRef] [Green Version]
- Farooqui, M.; Li, Y.; Rogers, T.; Poonawala, T.; Griffin, R.; Song, C.; Gupta, K. COX-2 Inhibitor Celecoxib Prevents Chronic Morphine-Induced Promotion of Angiogenesis, Tumour Growth, Metastasis and Mortality, without Compromising Analgesia. Br. J. Cancer 2007, 97, 1523–1531. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, A.T.; Ogino, S.; Fuchs, C.S. Aspirin and the Risk of Colorectal Cancer in Relation to the Expression of COX-2. N. Engl. J. Med. 2007, 356, 2131–2142. [Google Scholar] [CrossRef] [PubMed]
- Connolly, E.M.; Harmey, J.H.; O’Grady, T.; Foley, D.; Roche-Nagle, G.; Kay, E.; Bouchier-Hayes, D.J. Cyclo-Oxygenase Inhibition Reduces Tumour Growth and Metastasis in an Orthotopic Model of Breast Cancer. Br. J. Cancer 2002, 87, 231–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bezawada, N.; Song, M.; Wu, K.; Mehta, R.S.; Milne, G.L.; Ogino, S.; Fuchs, C.S.; Giovannucci, E.L.; Chan, A.T. Urinary PGE-M Levels are Associated with Risk of Colorectal Adenomas and Chemopreventive Response to Anti-Inflammatory Drugs. Cancer Prev. Res. 2014, 7, 758–765. [Google Scholar] [CrossRef] [Green Version]
- Dong, L.M.; Shu, X.-O.; Gao, Y.-T.; Milne, G.; Ji, B.-T.; Yang, G.; Li, H.-L.; Rothman, N.; Zheng, W.; Chow, W.-H. Urinary Prostaglandin E2 Metabolite and Gastric Cancer Risk in the Shanghai Women’s Health Study. Cancer Epidemiol. Prev. Biomark. 2009, 18, 3075–3078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cui, Y.; Shu, X.-O.; Gao, Y.-T.; Cai, Q.; Ji, B.-T.; Li, H.-L.; Rothman, N.; Wu, J.; Yang, G.; Xiang, Y.-B. Urinary Prostaglandin E2 Metabolite and Breast Cancer Risk. Cancer Epidemiol. Prev. Biomark. 2014, 23, 2866–2873. [Google Scholar] [CrossRef] [Green Version]
- Fedirko, V.; Bradshaw, P.T.; Figueiredo, J.C.; Sandler, R.S.; Barry, E.L.; Ahnen, D.J.; Milne, G.L.; Bresalier, R.S.; Baron, J.A. Urinary Metabolites of Prostanoids and Risk of Recurrent Colorectal Adenomas in the Aspirin/Folate Polyp Prevention Study (AFPPS). Cancer Prev. Res. 2015, 8, 1061–1068. [Google Scholar] [CrossRef] [Green Version]
- Kiely, M.; Milne, G.L.; Minas, T.Z.; Dorsey, T.H.; Tang, W.; Smith, C.J.; Baker, F.; Loffredo, C.A.; Yates, C.; Cook, M.B. Urinary Thromboxane B2 and Lethal Prostate Cancer in African American Men. JNCI J. Natl. Cancer Inst. 2021. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Odds of Case Status N, (%) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| All Cases | African American | European American | |||||||||
| PGE-M | Control | Case | OR (95% CI) * | Control | Case | OR (95% CI) * | Control | Case | OR (95% CI) * | P Heterogeneity | P Interaction |
| ≤Median a | 499 (50) | 482 (51) | Reference | 231 (50) | 216 (46) | Reference | 268 (50) | 266 (56) | Reference | 0.03 | 0.04 |
| >Median | 499 (50) | 466 (49) | 0.86 (0.72–1.04) | 234 (50) | 256 (54) | 1.0 (0.75–1.31) | 265 (50) | 210 (44) | 0.76 (0.59–0.99) | ||
| Continuous b | 0.96 (0.89–1.03) | 1.03 (0.93–1.14) | 0.88 (0.79–0.98) | ||||||||
| NCCN Risk Score | OR (95% CI) * | p Value |
|---|---|---|
| Low | Reference | |
| Intermediate | 0.96 (0.65–1.43) | 0.85 |
| High/Very High | 1.13 (0.71–1.81) | 0.60 |
| Regional/Metastatic | 0.93 (0.44–1.97) | 0.85 |
| Title | PGE-M | Alive | Dead | HR (95% CI) | HR (95% CI) † | HR (95% CI) * |
|---|---|---|---|---|---|---|
| All Cases | ≤Median a | 376 (53) | 105 (44) | Reference | Reference | Reference |
| >Median | 329 (47) | 135 (56) | 1.43 (1.11–1.84) | 1.35 (1.05–1.74) | 1.16 (0.89–1.52) | |
| Continuous b | 1.12 (1.02–1.24) | 1.09 (0.99–1.21) | 1.00 (0.90–1.12) | |||
| African American | ≤Median a | 165 (49) | 50 (37) | Reference | Reference | Reference |
| >Median | 171 (51) | 84 (63) | 1.47 (1.04–2.08) | 1.39 (0.98–1.96) | 1.30 (0.91–1.87) | |
| Continuous b | 1.09 (0.96–1.23) | 1.07 (0.94–1.23) | 1.02 (0.88–1.17) | |||
| European American | ≤Median a | 211 (57) | 55 (52) | Reference | Reference | Reference |
| >Median | 158 (43) | 51 (48) | 1.26 (0.86–1.84) | 1.14 (0.78–1.67) | 0.97 (0.64–1.47) | |
| Continuous b | 1.12 (0.96–1.32) | 1.05 (0.89–1.24) | 0.95 (0.80–1.13) |
| Title | PGE-M | Alive | Death from PC | Death from Other Cause | HR (95% CI) | HR (95% CI) † | Alive * | Death from PC * | Death from Other Cause * | HR (95% CI) * |
|---|---|---|---|---|---|---|---|---|---|---|
| All Cases | ≤Median a | 388 (53) | 28 (42) | 80 (44) | Reference | Reference | 375 (53) | 27 (42) | 78 (45) | Reference |
| >Median | 339 (47) | 38 (58) | 100 (56) | 1.47 (0.90–2.41) | 1.39 (0.85–2.28) | 327 (47) | 38 (58) | 96 (55) | 1.46 (0.86–2.46) | |
| Continuous b | 1.24 (1.03–1.50) | 1.23 (1.01–1.49) | 1.21 (0.97–1.50) | |||||||
| African American | ≤Median a | 172 (49) | 15 (38) | 36 (38) | Reference | Reference | 165 (49) | 15 (38) | 35 (37) | Reference |
| >Median | 178 (51) | 25 (63) | 60 (63) | 1.43 (0.75–2.70) | 1.33 (0.70–2.52) | 171 (51) | 25 (62) | 59 (63) | 1.49 (0.75–2.98) | |
| Continuous b | 1.18 (0.94–1.48) | 1.17 (0.92–1.50) | 1.13 (0.85–1.48) | |||||||
| European American | ≤Median a | 216 (57) | 13 (50) | 44 (52) | Reference | Reference | 210 (57) | 12 (48) | 43 (54) | Reference |
| >Median | 161 (43) | 13 (50) | 40 (48) | 1.28 (0.58–2.81) | 1.16 (0.53–2.56) | 156 (43) | 13 (52) | 37 (46) | 1.30 (0.54–3.14) | |
| Continuous b | 1.27 (0.91–1.78) | 1.20 (0.85–1.70) | 1.43 (0.95–2.15) |
| Title | All Cases | African American | European American | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| PGE-M | Alive | Dead | HR (95% CI) * | Alive | Dead | HR (95% CI) * | P Heterogeneity | Alive | Dead | HR (95% CI) * | P Interaction # | P Interaction † |
| Aspirin use | ||||||||||||
| ≤Median | 182 (53) | 62 (50) | Reference | 61 (43) | 25 (42) | Reference | 0.04 | 121 (60) | 37 (56) | Reference | 0.11 | 0.38 |
| >Median | 162 (47) | 63 (50) | 0.92 (0.63–1.34) | 81 (57) | 34 (58) | 0.70 (0.40–1.23) | 81 (40) | 29 (44) | 1.05 (0.63–1.75) | |||
| Continuous b | 0.93 (0.81–1.07) | 0.85 (0.70–1.02) | 1.00 (0.81–1.23) | |||||||||
| No aspirin use | ||||||||||||
| ≤Median | 193 (53) | 43 (38) | Reference | 104 (54) | 25 (33) | Reference | 89 (54) | 18 (46) | Reference | |||
| >Median | 165 (46) | 71 (62) | 1.52 (1.03–2.24) | 90 (46) | 50 (67) | 2.04 (1.23–3.37) | 75 (46) | 21 (54) | 0.99 (0.48–2.07) | |||
| Continuous b | 1.14 (0.96–1.35) | 1.27 (1.03–1.57) | 0.91 (0.67–1.22) | |||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiely, M.; Milne, G.L.; Minas, T.Z.; Dorsey, T.H.; Tang, W.; Smith, C.J.; Baker, F.; Loffredo, C.A.; Yates, C.; Cook, M.B.; et al. Urinary PGE-M in Men with Prostate Cancer. Cancers 2021, 13, 4073. https://doi.org/10.3390/cancers13164073
Kiely M, Milne GL, Minas TZ, Dorsey TH, Tang W, Smith CJ, Baker F, Loffredo CA, Yates C, Cook MB, et al. Urinary PGE-M in Men with Prostate Cancer. Cancers. 2021; 13(16):4073. https://doi.org/10.3390/cancers13164073
Chicago/Turabian StyleKiely, Maeve, Ginger L. Milne, Tsion Z. Minas, Tiffany H. Dorsey, Wei Tang, Cheryl J. Smith, Francine Baker, Christopher A. Loffredo, Clayton Yates, Michael B. Cook, and et al. 2021. "Urinary PGE-M in Men with Prostate Cancer" Cancers 13, no. 16: 4073. https://doi.org/10.3390/cancers13164073
APA StyleKiely, M., Milne, G. L., Minas, T. Z., Dorsey, T. H., Tang, W., Smith, C. J., Baker, F., Loffredo, C. A., Yates, C., Cook, M. B., & Ambs, S. (2021). Urinary PGE-M in Men with Prostate Cancer. Cancers, 13(16), 4073. https://doi.org/10.3390/cancers13164073