
Comprehensive Immunohistochemical Study of the SWI/SNF Complex Expression Status in Gastric Cancer Reveals an Adverse Prognosis of SWI/SNF Deficiency in Genomically Stable Gastric Carcinomas

 , ,
, ,  ,
,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Tissue Microarray Construction
2.3. Immunohistochemistry and In Situ Hybridization
2.4. TCGA Classification
2.5. Statistical Analysis
3. Results
3.1. Cohort
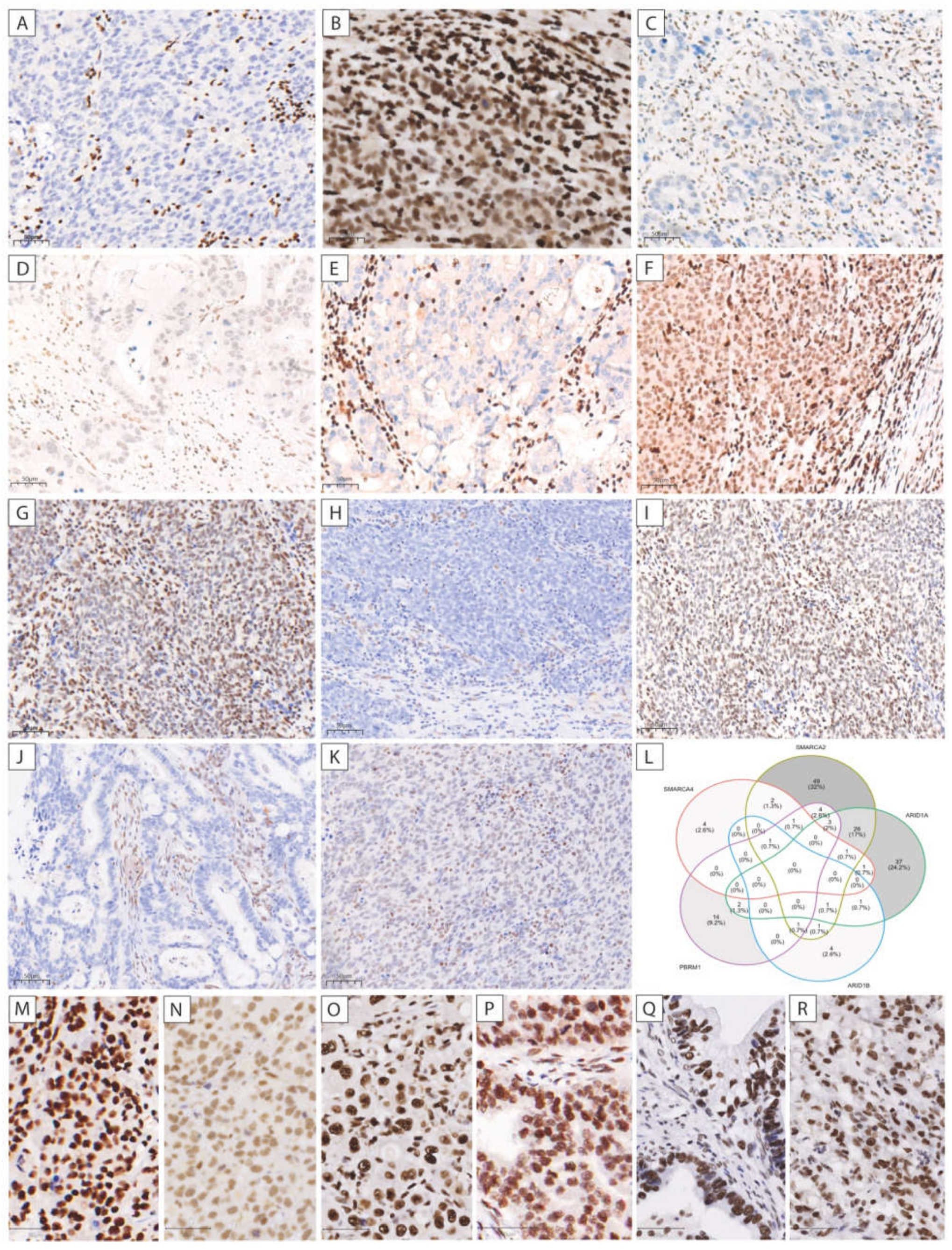
3.2. SMARCA4 Expression
3.3. SMARCA2, SMARCB1, and ARID1A Expression
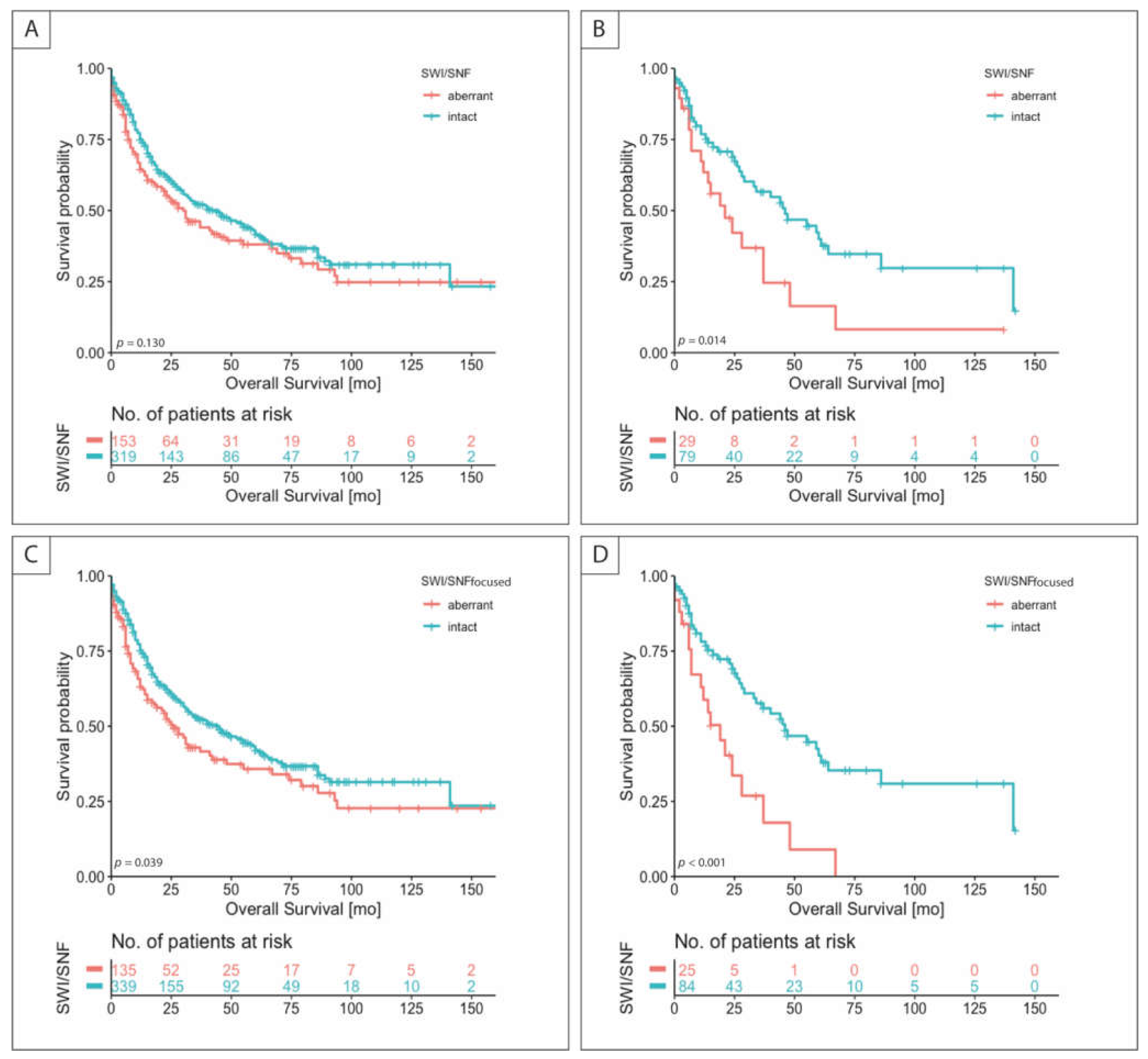
3.4. SWI/SNF Status, Clinicopathologic Characteristics, and Survival
3.5. Determination of SWI/SNF Status Using a Focused Panel of Protein Expression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Brierley, J.D.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 8th ed.; John Wiley & Sons Ltd.: Chichester, UK, 2017; pp. 115–119. [Google Scholar]
- In, H.; Solsky, I.; Palis, B.; Langdon-Embry, M.; A Ajani, J.; Sano, T. Validation of the 8th Edition of the AJCC TNM Staging System for Gastric Cancer using the National Cancer Database. Ann. Surg. Oncol. 2017, 24, 3683–3691. [Google Scholar] [CrossRef] [PubMed]
- Shiraishi, N.; Sato, K.; Yasuda, K.; Inomata, M.; Kitano, S. Multivariate prognostic study on large gastric cancer. J. Surg. Oncol. 2007, 96, 14–18. [Google Scholar] [CrossRef]
- Chen, Y.-C.; Fang, W.-L.; Wang, R.-F.; Liu, C.-A.; Yang, M.-H.; Lo, S.-S.; Wu, C.-W.; Li, A.F.-Y.; Shyr, Y.-M.; Huang, K.-H. Clinicopathological Variation of Lauren Classification in Gastric Cancer. Pathol. Oncol. Res. 2016, 22, 197–202. [Google Scholar] [CrossRef]
- Berlth, F. Pathohistological classification systems in gastric cancer: Diagnostic relevance and prognostic value. World J. Gastroenterol. 2014, 20, 5679–5684. [Google Scholar] [CrossRef]
- Liu, K.; Zhang, W.; Chen, X.; Chen, X.; Yang, K.; Zhang, B.; Chen, Z.; Zhou, Z.; Hu, J. Comparison on Clinicopathological Features and Prognosis Between Esophagogastric Junctional Adenocarcinoma (Siewert II/III Types) and Distal Gastric Adenocarcinoma. Medicine 2015, 94, e1386. [Google Scholar] [CrossRef]
- Cunningham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van De Velde, C.J.; Nicolson, M.; Scarffe, J.H.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative Chemotherapy versus Surgery Alone for Resectable Gastroesophageal Cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef] [Green Version]
- Allemani, C.; Matsuda, T.; Di Carlo, V.; Harewood, R.; Matz, M.; Nikšić, M.; Bonaventure, A.; Valkov, M.; Johnson, C.J.; Estève, J.; et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018, 391, 1023–1075. [Google Scholar] [CrossRef] [Green Version]
- Cancer Genome Atlas Research Network. The Cancer Genome Atlas Research Network Comprehensive molecular characterization of gastric adenocarcinoma. Nat. Cell Biol. 2014, 513, 202–209. [Google Scholar] [CrossRef] [Green Version]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.-M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular analysis of gastric cancer identifies subtypes associated with distinct clinical outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Li, N.; Jiang, W.; Hua, Z.; Xia, L.; Wei, Q.; Wang, L. Prognosis significance of HER-2/neu overexpression/amplification in Chinese patients with curatively resected gastric cancer after the ToGA clinical trial. World J. Surg. Oncol. 2012, 10, 274. [Google Scholar] [CrossRef] [Green Version]
- Böger, C.; Behrens, H.-M.; Mathiak, M.; Krüger, S.; Kalthoff, H.; Röcken, C. PD-L1 is an independent prognostic predictor in gastric cancer of Western patients. Oncotarget 2016, 7, 24269–24283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muro, K.; Chung, H.; Shankaran, V.; Geva, R.; Catenacci, D.; Gupta, S.; Eder, J.P.; Golan, T.; Le, D.T.; Burtness, B.; et al. Pembrolizumab for patients with PD-L1-positive advanced gastric cancer (KEYNOTE-012): A multicentre, open-label, phase 1b trial. Lancet Oncol. 2016, 17, 717–726. [Google Scholar] [CrossRef]
- Baniak, N.; Senger, J.-L.; Ahmed, S.; Kanthan, S.C.; Kanthan, R. Gastric biomarkers: A global review. World J. Surg. Oncol. 2016, 14, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira, P.; Oliveira, M.J.; Beraldi, E.; Mateus, A.R.; Nakajima, T.; Gleave, M.; Yokota, J.; Carneiro, F.; Huntsman, D.; Seruca, R.; et al. Loss of functional E-cadherin renders cells more resistant to the apoptotic agent taxol in vitro. Exp. Cell Res. 2005, 310, 99–104. [Google Scholar] [CrossRef]
- Eberhart, C.G.; A Rubens, J. SWI/SNF complex differences promote cellular heterogeneity in rhabdoid tumors. Neuro-Oncology 2020, 22, 741–742. [Google Scholar] [CrossRef] [PubMed]
- Mittal, P.; Roberts, C.W.M. The SWI/SNF complex in cancer — biology, biomarkers and therapy. Nat. Rev. Clin. Oncol. 2020, 17, 435–448. [Google Scholar] [CrossRef] [PubMed]
- Masliah-Planchon, J.; Bieche, I.; Guinebretière, J.-M.; Bourdeaut, F.; Delattre, O. SWI/SNF Chromatin Remodeling and Human Malignancies. Annu. Rev. Pathol. Mech. Dis. 2015, 10, 145–171. [Google Scholar] [CrossRef]
- Papillon, J.P.N.; Nakajima, K.; Adair, C.D.; Hempel, J.; Jouk, A.O.; Karki, R.G.; Mathieu, S.; Moebitz, H.; Ntaganda, R.; Smith, T.; et al. Discovery of Orally Active Inhibitors of Brahma Homolog (BRM)/SMARCA2 ATPase Activity for the Treatment of Brahma Related Gene 1 (BRG1)/SMARCA4-Mutant Cancers. J. Med. Chem. 2018, 61, 10155–10172. [Google Scholar] [CrossRef]
- Agaimy, A.; Daum, O.; Märkl, B.; Lichtmannegger, I.; Michal, M.; Hartmann, A. SWI/SNF Complex–deficient Undifferentiated/Rhabdoid Carcinomas of the Gastrointestinal Tract. Am. J. Surg. Pathol. 2016, 40, 544–553. [Google Scholar] [CrossRef]
- Huang, S.; Ng, K.; Yeh, T.; Cheng, C.; Chen, M.; Chao, Y.; Chuang, H.; Liu, Y.; Chen, T. The clinicopathological and molecular analysis of gastric cancer with altered SMARCA4 expression. Histopathology 2020, 77, 250–261. [Google Scholar] [CrossRef]
- Tessier-Cloutier, B.; Schaeffer, D.F.; Bacani, J.; E Marginean, C.; Kalloger, S.; Köbel, M.; Lee, C. Loss of switch/sucrose non-fermenting complex protein expression in undifferentiated gastrointestinal and pancreatic carcinomas. Histopathology 2020, 77, 46–54. [Google Scholar] [CrossRef]
- Huang, S.-C.; Ng, K.-F.; Chang, I.Y.-F.; Chang, C.-J.; Chao, Y.-C.; Chang, S.-C.; Chen, M.-C.; Yeh, T.-S.; Chen, T.-C. The clinicopathological significance of SWI/SNF alterations in gastric cancer is associated with the molecular subtypes. PLoS ONE 2021, 16, e0245356. [Google Scholar] [CrossRef]
- Liu, J.; Lichtenberg, T.; Hoadley, K.A.; Poisson, L.M.; Lazar, A.J.; Cherniack, A.D.; Kovatich, A.J.; Benz, C.C.; Levine, D.A.; Lee, A.V.; et al. An Integrated TCGA Pan-Cancer Clinical Data Resource to Drive High-Quality Survival Outcome Analytics. Cell 2018, 173, 400–416.e11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siewert, J.R.; Stein, H.J. Classification of adenocarcinoma of the oesophagogastric junction. BJS 2003, 85, 1457–1459. [Google Scholar] [CrossRef]
- Becker, K.; Mueller, J.D.; Schulmacher, C.; Ott, K.; Fink, U.; Busch, R.; Böttcher, K.; Siewert, J.R.; Höfler, H. Histomorphology and grading of regression in gastric carcinoma treated with neoadjuvant chemotherapy. Cancer 2003, 98, 1521–1530. [Google Scholar] [CrossRef]
- Songun, I.; Putter, H.; Kranenbarg, E.M.-K.; Sasako, M.; van de Velde, C.J. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 2010, 11, 439–449. [Google Scholar] [CrossRef]
- Shuster, J.J. Median follow-up in clinical trials. J. Clin. Oncol. 1991, 9, 191–192. [Google Scholar] [CrossRef]
- Herpel, E.; Rieker, R.J.; Dienemann, H.; Muley, T.; Meister, M.; Hartmann, A.; Warth, A.; Agaimy, A. SMARCA4 and SMARCA2 deficiency in non–small cell lung cancer: Immunohistochemical survey of 316 consecutive specimens. Ann. Diagn. Pathol. 2017, 26, 47–51. [Google Scholar] [CrossRef]
- Ahn, S.; Lee, S.-J.; Kim, Y.; Kim, A.; Shin, N.; Choi, K.U.; Lee, C.-H.; Huh, G.Y.; Kim, K.-M.; Setia, N.; et al. High-throughput Protein and mRNA Expression–based Classification of Gastric Cancers Can Identify Clinically Distinct Subtypes, Concordant With Recent Molecular Classifications. Am. J. Surg. Pathol. 2017, 41, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Setia, N.; Agoston, A.T.; Han, H.S.; Mullen, J.T.; Duda, D.G.; Clark, J.W.; Deshpande, V.; Mino-Kenudson, M.; Srivastava, A.; Lennerz, J.K.; et al. A protein and mRNA expression-based classification of gastric cancer. Mod. Pathol. 2016, 29, 772–784. [Google Scholar] [CrossRef]
- Bronsert, P.; Kohler, I.; Timme, S.; Kiefer, S.; Werner, M.; Schilling, O.; Vashist, Y.; Makowiec, F.; Brabletz, T.; Hopt, U.T.; et al. Prognostic significance of Zinc finger E-box binding homeobox 1 (ZEB1) expression in cancer cells and cancer-associated fibroblasts in pancreatic head cancer. Surgery 2014, 156, 97–108. [Google Scholar] [CrossRef]
- Köbel, M.; Piskorz, A.M.; Lee, S.; Lui, S.; Lepage, C.; Marass, F.; Rosenfeld, N.; Mes-Masson, A.-M.; Brenton, J.D. Optimized p53 immunohistochemistry is an accurate predictor of TP53 mutation in ovarian carcinoma. J. Pathol. Clin. Res. 2016, 2, 247–258. [Google Scholar] [CrossRef]
- Grosser, B.; Kohlruss, M.; Slotta-Huspenina, J.; Jesinghaus, M.; Pfarr, N.; Steiger, K.; Novotny, A.; Gaida, M.M.; Schmidt, T.; Hapfelmeier, A.; et al. Impact of Tumor Localization and Molecular Subtypes on the Prognostic and Predictive Significance of p53 Expression in Gastric Cancer. Cancers 2020, 12, 1689. [Google Scholar] [CrossRef] [PubMed]
- Agaimy, A.; Rau, T.T.; Hartmann, A.; Stoehr, R. SMARCB1 (INI1)-negative Rhabdoid Carcinomas of the Gastrointestinal Tract. Am. J. Surg. Pathol. 2014, 38, 910–920. [Google Scholar] [CrossRef]
- Guerrero-Martínez, J.A.; Reyes, J.C. High expression of SMARCA4 or SMARCA2 is frequently associated with an opposite prognosis in cancer. Sci. Rep. 2018, 8, 2043. [Google Scholar] [CrossRef] [Green Version]
- Schallenberg, S.; Bork, J.; Essakly, A.; Alakus, H.; Buettner, R.; Hillmer, A.M.; Bruns, C.; Schroeder, W.; Zander, T.; Loeser, H.; et al. Loss of the SWI/SNF-ATPase subunit members SMARCF1 (ARID1A), SMARCA2 (BRM), SMARCA4 (BRG1) and SMARCB1 (INI1) in oesophageal adenocarcinoma. BMC Cancer 2020, 20, 12. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; the WHO Classification of Tumours Editorial Board. The 2019 WHO classification of tumours of the digestive system. Histopathology 2019, 76, 182–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogiwara, H.; Takahashi, K.; Sasaki, M.; Kuroda, T.; Yoshida, H.; Watanabe, R.; Maruyama, A.; Makinoshima, H.; Chiwaki, F.; Sasaki, H.; et al. Targeting the Vulnerability of Glutathione Metabolism in ARID1A-Deficient Cancers. Cancer Cell 2019, 35, 177–190.e8. [Google Scholar] [CrossRef] [Green Version]
- Samartzis, E.P.; Gutsche, K.; Dedes, K.J.; Fink, D.; Stucki, M.; Imesch, P. Loss of ARID1A expression sensitizes cancer cells to PI3K- and AKT-inhibition. Oncotarget 2014, 5, 5295–5303. [Google Scholar] [CrossRef]
- Bitler, B.; Aird, K.M.; Garipov, A.; Li, H.; Amatangelo, M.; Kossenkov, A.V.; Schultz, D.C.; Liu, Q.; Shih, I.-M.; Conejo-Garcia, J.; et al. Synthetic lethality by targeting EZH2 methyltransferase activity in ARID1A-mutated cancers. Nat. Med. 2015, 21, 231–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamada, L.; Saito, M.; Min, A.K.T.; Saito, K.; Ashizawa, M.; Kase, K.; Nakajima, S.; Onozawa, H.; Okayama, H.; Endo, H.; et al. Selective sensitivity of EZH2 inhibitors based on synthetic lethality in ARID1A-deficient gastric cancer. Gastric Cancer 2021, 24, 60–71. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Peng, Y.; Wei, L.; Zhang, W.; Yang, L.; Lan, L.; Kapoor, P.; Ju, Z.; Mo, Q.; Shih, I.-M.; et al. ARID1A Deficiency Impairs the DNA Damage Checkpoint and Sensitizes Cells to PARP Inhibitors. Cancer Discov. 2015, 5, 752–767. [Google Scholar] [CrossRef] [Green Version]
- Shorstova, T.; Marques, M.; Su, J.; Johnston, J.; Kleinman, C.L.; Hamel, N.; Huang, S.; Alaoui-Jamali, M.A.; Foulkes, W.D.; Witcher, M. SWI/SNF-Compromised Cancers Are Susceptible to Bromodomain Inhibitors. Cancer Res. 2019, 79, 2761–2774. [Google Scholar] [CrossRef] [Green Version]
- Zhou, M.; Yuan, J.; Deng, Y.; Fan, X.; Shen, J. Emerging role of SWI/SNF complex deficiency as a target of immune checkpoint blockade in human cancers. Oncogenesis 2021, 10, 1–8. [Google Scholar] [CrossRef]
- Soldi, R.; Halder, T.G.; Weston, A.; Thode, T.; Drenner, K.; Lewis, R.; Kaadige, M.R.; Srivastava, S.; Ampanattu, S.D.; Del Villar, R.R.; et al. The novel reversible LSD1 inhibitor SP-2577 promotes anti-tumor immunity in SWItch/Sucrose-NonFermentable (SWI/SNF) complex mutated ovarian cancer. PLoS ONE 2020, 15, e0235705. [Google Scholar] [CrossRef]
- Leruste, A.; Tosello, J.; Ramos, R.N.; Tauziède-Espariat, A.; Brohard, S.; Han, Z.-Y.; Beccaria, K.; Andrianteranagna, M.; Caudana, P.; Nikolic, J.; et al. Clonally Expanded T Cells Reveal Immunogenicity of Rhabdoid Tumors. Cancer Cell 2019, 36, 597–612.e8. [Google Scholar] [CrossRef]
- Jelinic, P.; Ricca, J.; Van Oudenhove, E.; Olvera, N.; Merghoub, T.; A Levine, D.; Zamarin, D. Immune-Active Microenvironment in Small Cell Carcinoma of the Ovary, Hypercalcemic Type: Rationale for Immune Checkpoint Blockade. J. Natl. Cancer Inst. 2018, 110, 787–790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.T.; Cristescu, R.; Bass, A.J.; Kim, K.-M.; Odegaard, J.I.; Kim, K.; Liu, X.Q.; Sher, X.; Jung, H.; Lee, M.; et al. Comprehensive molecular characterization of clinical responses to PD-1 inhibition in metastatic gastric cancer. Nat. Med. 2018, 24, 1449–1458. [Google Scholar] [CrossRef]
- Fuchs, C.S.; Özgüroğlu, M.; Bang, Y.-J.; Di Bartolomeo, M.; Mandalà, M.; Ryu, M.-H.; Fornaro, L.; Olesinski, T.; Caglevic, C.; Chung, H.C.; et al. Pembrolizumab versus paclitaxel for previously treated patients with PD-L1–positive advanced gastric or gastroesophageal junction cancer (GC): Update from the phase III KEYNOTE-061 trial. J. Clin. Oncol. 2020, 38, 4503. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | n = 477 * | SWI/SNF-Aberrant (n = 153) | SWI/SNF Intact (n = 319) | p Value | |||
|---|---|---|---|---|---|---|---|
| Median age (range) (years) | 70.0 (30.0–95.0) | 72.0 (41.0–95.0) | 68.0 (30.0–94.0) | 0.193 | |||
| Median survival (range) (months) | 58.0 (49.9–66.1) | 54.0 (34.7–73.3) | 60.0 (53.5–66.5) | ||||
| Sex | 0.121 | ||||||
| Female | 165 | 35% | 61 | 40% | 104 | 33% | |
| Male | 312 | 65% | 92 | 60% | 215 | 67% | |
| T status | 0.005 | ||||||
| pT1/2 | 159 | 33% | 38 | 25% | 121 | 38% | |
| pT2/3 | 318 | 67% | 115 | 75% | 198 | 62% | |
| N status | 0.448 | ||||||
| Negative | 178 | 37% | 53 | 35% | 122 | 38% | |
| Positive | 299 | 63% | 100 | 65% | 197 | 62% | |
| Distant Metastasis | 0.409 | ||||||
| No | 247 | 52% | 75 | 49% | 171 | 54% | |
| Yes | 197 | 41% | 66 | 43% | 127 | 40% | |
| NA | 33 | 7% | 12 | 8% | 21 | 7% | |
| Grading | 0.471 | ||||||
| Low grade | 162 | 34% | 48 | 31% | 114 | 36% | |
| High grade | 304 | 64% | 100 | 65% | 204 | 64% | |
| NA | 11 | 2% | 5 | 3% | 1 | 0% | |
| Lymphovascular invasion | 0.156 | ||||||
| Negative | 287 | 60% | 85 | 56% | 199 | 62% | |
| Positive | 190 | 40% | 68 | 44% | 120 | 38% | |
| Vascular invasion | 0.922 | ||||||
| Negative | 401 | 84% | 128 | 84% | 268 | 84% | |
| Positive | 76 | 16% | 25 | 16% | 51 | 16% | |
| Laurén | 0.159 | ||||||
| Intestinal | 266 | 56% | 93 | 61% | 172 | 54% | |
| Non-intestinal | 211 | 44% | 60 | 39% | 147 | 46% | |
| Localization | 0.471 | ||||||
| Proximal | 124 | 26% | 36 | 24% | 85 | 27% | |
| Non-proximal | 335 | 70% | 111 | 73% | 222 | 70% | |
| NA | 18 | 4% | 6 | 4% | 12 | 4% | |
| R status | 0.508 | ||||||
| R0 | 403 | 84% | 131 | 86% | 268 | 84% | |
| R1 | 54 | 11% | 15 | 10% | 38 | 12% | |
| Rx | 20 | 4% | 7 | 5% | 13 | 4% | |
| TCGA | <0.001 | ||||||
| EBV+ | 25 | 5% | 14 | 9% | 11 | 3% | |
| MSI | 61 | 13% | 40 | 26% | 21 | 7% | |
| GS | 110 | 23% | 29 | 19% | 79 | 25% | |
| CIN | 151 | 32% | 27 | 18% | 123 | 39% | |
| No classification | 130 | 27% | 43 | 28% | 85 | 27% | |
| Death | 0.218 | ||||||
| No | 227 | 48% | 67 | 44% | 159 | 50% | |
| Yes | 250 | 52% | 86 | 56% | 160 | 50% | |
| nCTx | 0.972 | ||||||
| No | 347 | 73% | 112 | 73% | 234 | 73% | |
| Yes | 130 | 27% | 41 | 27% | 85 | 27% | |
| TRG | (n = 130 **) | (n = 41) | (n = 85) | 0.023 | |||
| 1b | 10 | 7% | 0 | 0% | 9 | 11% | |
| 2 | 37 | 28% | 9 | 22% | 28 | 33% | |
| 3 | 83 | 63% | 32 | 78% | 48 | 56% | |
| CTx regimen | 0.142 | ||||||
| Cis/Ox + 5-FU or Cap | 36 | 27% | 14 | 34% | 20 | 24% | |
| Ox + 5-FU + Doc | 46 | 35% | 11 | 27% | 34 | 40% | |
| Cis + 5-FU + Epi | 41 | 32% | 12 | 29% | 28 | 33% | |
| Ox + Epi + Cap | 5 | 4% | 2 | 5% | 3 | 4% | |
| Others | 2 | 2% | 2 | 5% | 0 | 0% | |
| Variable | Overall Survival (n = 472) | Overall Survival (n = 108) | ||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |||
| T-status | 1.829 | 1.266 | 2.643 | 0.001 | 1.898 | 0.734 | 4.911 | 0.186 |
| N-status | 1.708 | 1.209 | 2.414 | 0.002 | 2.664 | 1.212 | 5.853 | 0.015 |
| Age | 1.015 | 1.003 | 1.027 | 0.017 | 1.027 | 1.002 | 1.052 | 0.033 |
| M-status | 2.517 | 1.820 | 3.480 | <0.001 | 2.045 | 1.027 | 4.073 | 0.042 |
| R-status | 1.977 | 1.368 | 2.857 | <0.001 | 1.626 | 0.842 | 3.142 | 0.148 |
| SWI/SNF | 1.218 | 0.898 | 1.651 | 0.205 | 1.904 | 1.035 | 3.503 | 0.039 |
| TCGA | - | - | - | 0.440 | - | - | - | - |
| EBV+ | 1.737 | 0.747 | 4.036 | 0.200 | - | - | - | - |
| MSI | 1.753 | 0.781 | 3.934 | 0.173 | - | - | - | - |
| GS | 2.047 | 0.921 | 4.552 | 0.079 | - | - | - | - |
| CIN | 1.670 | 0.744 | 3.751 | 0.214 | - | - | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glückstein, M.-I.; Dintner, S.; Arndt, T.T.; Vlasenko, D.; Schenkirsch, G.; Agaimy, A.; Müller, G.; Märkl, B.; Grosser, B. Comprehensive Immunohistochemical Study of the SWI/SNF Complex Expression Status in Gastric Cancer Reveals an Adverse Prognosis of SWI/SNF Deficiency in Genomically Stable Gastric Carcinomas. Cancers 2021, 13, 3894. https://doi.org/10.3390/cancers13153894
Glückstein M-I, Dintner S, Arndt TT, Vlasenko D, Schenkirsch G, Agaimy A, Müller G, Märkl B, Grosser B. Comprehensive Immunohistochemical Study of the SWI/SNF Complex Expression Status in Gastric Cancer Reveals an Adverse Prognosis of SWI/SNF Deficiency in Genomically Stable Gastric Carcinomas. Cancers. 2021; 13(15):3894. https://doi.org/10.3390/cancers13153894
Chicago/Turabian StyleGlückstein, Marie-Isabelle, Sebastian Dintner, Tim Tobias Arndt, Dmytro Vlasenko, Gerhard Schenkirsch, Abbas Agaimy, Gernot Müller, Bruno Märkl, and Bianca Grosser. 2021. "Comprehensive Immunohistochemical Study of the SWI/SNF Complex Expression Status in Gastric Cancer Reveals an Adverse Prognosis of SWI/SNF Deficiency in Genomically Stable Gastric Carcinomas" Cancers 13, no. 15: 3894. https://doi.org/10.3390/cancers13153894
APA StyleGlückstein, M.-I., Dintner, S., Arndt, T. T., Vlasenko, D., Schenkirsch, G., Agaimy, A., Müller, G., Märkl, B., & Grosser, B. (2021). Comprehensive Immunohistochemical Study of the SWI/SNF Complex Expression Status in Gastric Cancer Reveals an Adverse Prognosis of SWI/SNF Deficiency in Genomically Stable Gastric Carcinomas. Cancers, 13(15), 3894. https://doi.org/10.3390/cancers13153894