
The Presence of Small Nerve Fibers in the Tumor Microenvironment as Predictive Biomarker of Oncological Outcome Following Partial Hepatectomy for Intrahepatic Cholangiocarcinoma


 ,
,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Cohort
2.2. Oncological Staging and Surgical Technique
2.3. Adjuvant Therapy and Patient Follow-Up
2.4. Assessment of Nerve Fibers
2.5. Statistical Analysis
3. Results
3.1. Patient Cohort
3.2. Group Categorization and Comparative Analysis with Respect to Nerve Fiber Density
3.3. Cox Regression Analysis
3.4. Suvival Analysis
3.5. Histological Characteristics
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef]
- Banales, J.M.; Cardinale, V.; Carpino, G.; Marzioni, M.; Andersen, J.B.; Invernizzi, P.; Lind, G.E.; Folseraas, T.; Forbes, S.J.; Fouassier, L.; et al. Expert consensus document: Cholangiocarcinoma: Current knowledge and future perspectives consensus statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 261–280. [Google Scholar] [CrossRef]
- Khan, S.A.; Tavolari, S.; Brandi, G. Cholangiocarcinoma: Epidemiology and risk factors. Liver Int. Off. J. Int. Assoc. Study Liver 2019, 39 (Suppl. S1), 19–31. [Google Scholar] [CrossRef] [Green Version]
- Rizvi, S.; Khan, S.A.; Hallemeier, C.L.; Kelley, R.K.; Gores, G.J. Cholangiocarcinoma—Evolving concepts and therapeutic strategies. Nat. Rev. Clin. Oncol. 2018, 15, 95–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clements, O.; Eliahoo, J.; Kim, J.U.; Taylor-Robinson, S.D.; Khan, S.A. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma: A systematic review and meta-analysis. J. Hepatol. 2020, 72, 95–103. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus gemcitabine versus gemcitabine for biliary tract cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bednarsch, J.; Czigany, Z.; Lurje, I.; Strnad, P.; Bruners, P.; Ulmer, T.F.; den Dulk, M.; Lurje, G.; Neumann, U.P. The role of ALPPS in intrahepatic cholangiocarcinoma. Langenbeck’s Arch. Surg. Dtsch. Ges. Fur Chir. 2019, 404, 885–894. [Google Scholar] [CrossRef] [PubMed]
- Primrose, J.N.; Fox, R.P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): A randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019, 20, 663–673. [Google Scholar] [CrossRef] [Green Version]
- Palen, A.; Garnier, J.; Hobeika, C.; Ewald, J.; Gregoire, E.; Delpero, J.R.; Le Treut, Y.P.; Turrini, O.; Hardwigsen, J. Oncological relevance of major hepatectomy with inferior vena cava resection for intrahepatic cholangiocarcinoma. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2021. [Google Scholar] [CrossRef]
- Li, J.; Moustafa, M.; Linecker, M.; Lurje, G.; Capobianco, I.; Baumgart, J.; Ratti, F.; Rauchfuss, F.; Balci, D.; Fernandes, E.; et al. ALPPS for Locally Advanced Intrahepatic Cholangiocarcinoma: Did Aggressive Surgery Lead to the Oncological Benefit? An International Multi-center Study. Ann. Surg. Oncol. 2020, 27, 1372–1384. [Google Scholar] [CrossRef] [Green Version]
- Clavien, P.A.; Petrowsky, H.; DeOliveira, M.L.; Graf, R. Strategies for safer liver surgery and partial liver transplantation. N. Engl. J. Med. 2007, 356, 1545–1559. [Google Scholar] [CrossRef]
- Reames, B.N.; Ejaz, A.; Koerkamp, B.G.; Alexandrescu, S.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Impact of major vascular resection on outcomes and survival in patients with intrahepatic cholangiocarcinoma: A multi-institutional analysis. J. Surg. Oncol. 2017, 116, 133–139. [Google Scholar] [CrossRef]
- Bagante, F.; Spolverato, G.; Weiss, M.; Alexandrescu, S.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Defining Long-Term Survivors Following Resection of Intrahepatic Cholangiocarcinoma. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2017, 21, 1888–1897. [Google Scholar] [CrossRef]
- Si, A.; Li, J.; Xiang, H.; Zhang, S.; Bai, S.; Yang, P.; Zhang, X.; Xia, Y.; Wang, K.; Yan, Z.; et al. Actual over 10-year survival after liver resection for patients with intrahepatic cholangiocarcinoma. Oncotarget 2017, 8, 44521–44532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lurje, G.; Bednarsch, J.; Czigany, Z.; Lurje, I.; Schlebusch, I.K.; Boecker, J.; Meister, F.A.; Tacke, F.; Roderburg, C.; Den Dulk, M.; et al. The prognostic role of lymphovascular invasion and lymph node metastasis in perihilar and intrahepatic cholangiocarcinoma. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2019, 45, 1468–1478. [Google Scholar] [CrossRef]
- Bednarsch, J.; Kather, J.; Tan, X.; Sivakumar, S.; Cacchi, C.; Wiltberger, G.; Czigany, Z.; Ulmer, F.; Neumann, U.P.; Heij, L.R. Nerve Fibers in the Tumor Microenvironment as a Novel Biomarker for Oncological Outcome in Patients Undergoing Surgery for Perihilar Cholangiocarcinoma. Liver Cancer 2021. [Google Scholar] [CrossRef] [PubMed]
- Albo, D.; Akay, C.L.; Marshall, C.L.; Wilks, J.A.; Verstovsek, G.; Liu, H.; Agarwal, N.; Berger, D.H.; Ayala, G.E. Neurogenesis in colorectal cancer is a marker of aggressive tumor behavior and poor outcomes. Cancer 2011, 117, 4834–4845. [Google Scholar] [CrossRef] [PubMed]
- Zhao, C.M.; Hayakawa, Y.; Kodama, Y.; Muthupalani, S.; Westphalen, C.B.; Andersen, G.T.; Flatberg, A.; Johannessen, H.; Friedman, R.A.; Renz, B.W.; et al. Denervation suppresses gastric tumorigenesis. Sci. Transl. Med. 2014, 6, 250ra115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwasaki, T.; Hiraoka, N.; Ino, Y.; Nakajima, K.; Kishi, Y.; Nara, S.; Esaki, M.; Shimada, K.; Katai, H. Reduction of intrapancreatic neural density in cancer tissue predicts poorer outcome in pancreatic ductal carcinoma. Cancer Sci. 2019, 110, 1491–1502. [Google Scholar] [CrossRef] [PubMed]
- Heij, L.R.; Tan, X.; Kather, J.N.; Niehues, J.M.; Sivakumar, S.; Heussen, N.; van der Kroft, G.; Damink, S.W.M.O.; Lang, S.; Aberle, M.R.; et al. Nerve Fibers in the Tumor Microenvironment Are Co-Localized with Lymphoid Aggregates in Pancreatic Cancer. J. Clin. Med. 2021, 10, 490. [Google Scholar] [CrossRef] [PubMed]
- Spolverato, G.; Kim, Y.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; Clark Gamblin, T.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; et al. Management and Outcomes of Patients with Recurrent Intrahepatic Cholangiocarcinoma Following Previous Curative-Intent Surgical Resection. Ann. Surg. Oncol. 2016, 23, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Alabraba, E.; Joshi, H.; Bird, N.; Griffin, R.; Sturgess, R.; Stern, N.; Sieberhagen, C.; Cross, T.; Camenzuli, A.; Davis, R.; et al. Increased multimodality treatment options has improved survival for Hepatocellular carcinoma but poor survival for biliary tract cancers remains unchanged. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2019, 45, 1660–1667. [Google Scholar] [CrossRef]
- Preston, M.; Sherman, L.S. Neural stem cell niches: Roles for the hyaluronan-based extracellular matrix. Front. Biosci. 2011, 3, 1165–1179. [Google Scholar] [CrossRef] [Green Version]
- Gritsenko, P.G.; Ilina, O.; Friedl, P. Interstitial guidance of cancer invasion. J. Pathol. 2012, 226, 185–199. [Google Scholar] [CrossRef] [PubMed]
- Godinho-Silva, C.; Cardoso, F.; Veiga-Fernandes, H. Neuro-Immune Cell Units: A New Paradigm in Physiology. Annu. Rev. Immunol. 2019, 37, 19–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, X.; Sivakumar, S.; Bednarsch, J.; Wiltberger, G.; Kather, J.N.; Niehues, J.; de Vos-Geelen, J.; Valkenburg-van Iersel, L.; Kintsler, S.; Roeth, A.; et al. Nerve fibers in the tumor microenvironment in neurotropic cancer-pancreatic cancer and cholangiocarcinoma. Oncogene 2020. [Google Scholar] [CrossRef]
- Liu, H.P.; Tay, S.S.; Leong, S.; Schemann, M. Colocalization of ChAT, DbetaH and NADPH-d in the pancreatic neurons of the newborn guinea pig. Cell Tissue Res. 1998, 294, 227–231. [Google Scholar] [CrossRef]
- Dang, N.; Meng, X.; Song, H. Nicotinic acetylcholine receptors and cancer. Biomed. Rep. 2016, 4, 515–518. [Google Scholar] [CrossRef] [Green Version]
- Sha, M.; Cao, J.; Sun, H.Y.; Tong, Y.; Xia, Q. Neuroendocrine regulation of cholangiocarcinoma: A status quo review. Biochim. Biophys. Acta Rev. Cancer 2019, 1872, 66–73. [Google Scholar] [CrossRef]
- Franchitto, A.; Onori, P.; Renzi, A.; Carpino, G.; Mancinelli, R.; Alvaro, D.; Gaudio, E. Recent advances on the mechanisms regulating cholangiocyte proliferation and the significance of the neuroendocrine regulation of cholangiocyte pathophysiology. Ann. Transl. Med. 2013, 1, 27. [Google Scholar] [CrossRef]
- Shirai, K.; Ebata, T.; Oda, K.; Nishio, H.; Nagasaka, T.; Nimura, Y.; Nagino, M. Perineural invasion is a prognostic factor in intrahepatic cholangiocarcinoma. World J. Surg. 2008, 32, 2395–2402. [Google Scholar] [CrossRef]
- Fisher, S.B.; Patel, S.H.; Kooby, D.A.; Weber, S.; Bloomston, M.; Cho, C.; Hatzaras, I.; Schmidt, C.; Winslow, E.; Staley, C.A., 3rd; et al. Lymphovascular and perineural invasion as selection criteria for adjuvant therapy in intrahepatic cholangiocarcinoma: A multi-institution analysis. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2012, 14, 514–522. [Google Scholar] [CrossRef] [Green Version]
- Partecke, L.I.; Kading, A.; Trung, D.N.; Diedrich, S.; Sendler, M.; Weiss, F.; Kuhn, J.P.; Mayerle, J.; Beyer, K.; von Bernstorff, W.; et al. Subdiaphragmatic vagotomy promotes tumor growth and reduces survival via TNFalpha in a murine pancreatic cancer model. Oncotarget 2017, 8, 22501–22512. [Google Scholar] [CrossRef] [Green Version]
- Kamiya, A.; Hayama, Y.; Kato, S.; Shimomura, A.; Shimomura, T.; Irie, K.; Kaneko, R.; Yanagawa, Y.; Kobayashi, K.; Ochiya, T. Genetic manipulation of autonomic nerve fiber innervation and activity and its effect on breast cancer progression. Nat. Neurosci. 2019, 22, 1289–1305. [Google Scholar] [CrossRef]
- Zhao, Q.; Yang, Y.; Liang, X.; Du, G.; Liu, L.; Lu, L.; Dong, J.; Han, H.; Zhang, G. The clinicopathological significance of neurogenesis in breast cancer. BMC Cancer 2014, 14, 484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakanuma, Y.; Kakuda, Y. Pathologic classification of cholangiocarcinoma: New concepts. Best Pract. Res. Clin. Gastroenterol. 2015, 29, 277–293. [Google Scholar] [CrossRef]
- Kendall, T.; Verheij, J.; Gaudio, E.; Evert, M.; Guido, M.; Goeppert, B.; Carpino, G. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. Off. J. Int. Assoc. Study Liver 2019, 39 (Suppl. S1), 7–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komuta, M.; Govaere, O.; Vandecaveye, V.; Akiba, J.; Van Steenbergen, W.; Verslype, C.; Laleman, W.; Pirenne, J.; Aerts, R.; Yano, H.; et al. Histological diversity in cholangiocellular carcinoma reflects the different cholangiocyte phenotypes. Hepatology 2012, 55, 1876–1888. [Google Scholar] [CrossRef] [PubMed]
- Akita, M.; Fujikura, K.; Ajiki, T.; Fukumoto, T.; Otani, K.; Azuma, T.; Itoh, T.; Ku, Y.; Zen, Y. Dichotomy in intrahepatic cholangiocarcinomas based on histologic similarities to hilar cholangiocarcinomas. Mod. Pathol. 2017, 30, 986–997. [Google Scholar] [CrossRef] [Green Version]
- Borger, D.R.; Tanabe, K.K.; Fan, K.C.; Lopez, H.U.; Fantin, V.R.; Straley, K.S.; Schenkein, D.P.; Hezel, A.F.; Ancukiewicz, M.; Liebman, H.M.; et al. Frequent mutation of isocitrate dehydrogenase (IDH)1 and IDH2 in cholangiocarcinoma identified through broad-based tumor genotyping. Oncologist 2012, 17, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Lowery, M.A.; Ptashkin, R.; Jordan, E.; Berger, M.F.; Zehir, A.; Capanu, M.; Kemeny, N.E.; O’Reilly, E.M.; El-Dika, I.; Jarnagin, W.R.; et al. Comprehensive Molecular Profiling of Intrahepatic and Extrahepatic Cholangiocarcinomas: Potential Targets for Intervention. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2018, 24, 4154–4161. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, H.; Arai, Y.; Totoki, Y.; Shirota, T.; Elzawahry, A.; Kato, M.; Hama, N.; Hosoda, F.; Urushidate, T.; Ohashi, S.; et al. Genomic spectra of biliary tract cancer. Nat. Genet. 2015, 47, 1003–1010. [Google Scholar] [CrossRef] [PubMed]
- Mavros, M.N.; Economopoulos, K.P.; Alexiou, V.G.; Pawlik, T.M. Treatment and Prognosis for Patients With Intrahepatic Cholangiocarcinoma: Systematic Review and Meta-analysis. JAMA Surg. 2014, 149, 565–574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buettner, S.; Koerkamp, B.G.; Ejaz, A.; Buisman, F.E.; Kim, Y.; Margonis, G.A.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; et al. The effect of preoperative chemotherapy treatment in surgically treated intrahepatic cholangiocarcinoma patients-A multi-institutional analysis. J. Surg. Oncol. 2017, 115, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Bednarsch, J.; Czigany, Z.; Heij, L.R.; Liu, D.; den Dulk, M.; Wiltberger, G.; Bruners, P.; Ulmer, T.F.; Neumann, U.P.; Lang, S.A. Compelling Long-Term Results for Liver Resection in Early Cholangiocarcinoma. J. Clin. Med. 2021, 10, 2959. [Google Scholar] [CrossRef] [PubMed]
- Nickkholgh, A.; Ghamarnejad, O.; Khajeh, E.; Tinoush, P.; Bruckner, T.; Kulu, Y.; Mieth, M.; Goeppert, B.; Roessler, S.; Weiss, K.H.; et al. Outcome after liver resection for primary and recurrent intrahepatic cholangiocarcinoma. BJS Open 2019, 3, 793–801. [Google Scholar] [CrossRef]
- Hyder, O.; Hatzaras, I.; Sotiropoulos, G.C.; Paul, A.; Alexandrescu, S.; Marques, H.; Pulitano, C.; Barroso, E.; Clary, B.M.; Aldrighetti, L.; et al. Recurrence after operative management of intrahepatic cholangiocarcinoma. Surgery 2013, 153, 811–818. [Google Scholar] [CrossRef]
- Jonas, S.; Thelen, A.; Benckert, C.; Biskup, W.; Neumann, U.; Rudolph, B.; Lopez-Haanninen, E.; Neuhaus, P. Extended liver resection for intrahepatic cholangiocarcinoma: A comparison of the prognostic accuracy of the fifth and sixth editions of the TNM classification. Ann. Surg. 2009, 249, 303–309. [Google Scholar] [CrossRef]
- Hu, J.H.; Tang, J.H.; Lin, C.H.; Chu, Y.Y.; Liu, N.J. Preoperative staging of cholangiocarcinoma and biliary carcinoma using 18F-fluorodeoxyglucose positron emission tomography: A meta-analysis. J. Investig. Med. Off. Publ. Am. Fed. Clin. Res. 2018, 66, 52–61. [Google Scholar] [CrossRef]
- Koerkamp, B.G.; Wiggers, J.K.; Allen, P.J.; Busch, O.R.; D’Angelica, M.I.; DeMatteo, R.P.; Fong, Y.; Gonen, M.; Gouma, D.J.; Kingham, T.P.; et al. American Joint Committee on Cancer staging for resected perihilar cholangiocarcinoma: A comparison of the 6th and 7th editions. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2014, 16, 1074–1082. [Google Scholar] [CrossRef] [Green Version]
- Kizy, S.; Altman, A.M.; Marmor, S.; Wirth, K.; Ching Hui, J.Y.; Tuttle, T.M.; Denbo, J.W.; Jensen, E.H. Surgical resection of lymph node positive intrahepatic cholangiocarcinoma may not improve survival. HPB Off. J. Int. Hepato Pancreato Biliary Assoc. 2019, 21, 235–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | Overall Cohort (n = 96) | NF Positive (n = 45) | NF Negative (n = 51) | p Value |
|---|---|---|---|---|
| Gender, m/f (%) | 41 (43)/55 (57) | 18 (40)/27 (60) | 23 (45)/28 (55) | 0.614 |
| Age (years) | 65 (58–73) | 66 (60–75) | 62 (56–72) | 0.330 |
| BMI (kg/m2) | 25 (22–29) | 25 (22–29) | 25 (23–29) | 0.733 |
| ASA, n (%) | 0.230 | |||
| I | 3 (3) | 1 (2) | 2 (4) | |
| II | 42 (44) | 21 (47) | 21 (41) | |
| III | 48 (50) | 20 (44) | 28 (55) | |
| IV | 3 (3) | 3 (7) | 0 | |
| V | 0 | 0 | 0 | |
| Clinical chemistry | ||||
| Albumin (g/dL) | 44 (41–46) | 43 (40–46) | 44 (41–46) | 0.314 |
| AST (U/L) | 34 (26–47) | 32 (24–44) | 37 (29–53) | 0.077 |
| ALT (U/L) | 29 (20–53) | 25 (17–50) | 31 (22–57) | 0.169 |
| GGT (U/L) | 114 (65–304) | 88 (65–501) | 118 (62–265) | 0.876 |
| Total bilirubin (mg/dL) | 0.5 (0.4–0.7) | 0.5 (0.4–0.7) | 0.6 (0.4–0.8) | 0.117 |
| Platelet count (/nL) | 245 (197–307) | 251 (194–303) | 238 (198–315) | 0.925 |
| Alkaline Phosphatase (U/L) | 117 (90–258) | 108 (78–301) | 125 (91–246) | 0.628 |
| Prothrombin time (%) | 100 (95–109) | 100 (96–111) | 102 (94–108) | 0.942 |
| INR | 0.98 (0.95–1.03) | 0.97 (0.93–1.03) | 0.99 (0.96–1.03) | 0.386 |
| Hemoglobin (g/dL) | 13 (12–14) | 13 (12–14) | 13 (12–14) | 0.248 |
| Operative Data | ||||
| Operative time (minutes) | 285 (221–345) | 285 (227–338) | 285 (212–345) | 0.895 |
| Operative procedure, n (%) | 0.410 | |||
| Monosegmentectomy/atypical | 9 (9) | 6 (13) | 3 (6) | |
| Bisegmentectomy | 7 (7) | 4 (9) | 3 (6) | |
| Right/left hepatectomy | 31 (32) | 17 (38) | 14 (28) | |
| Ext. right/left hepatectomy | 20 (21) | 7 (16) | 13 (26) | |
| Right/left trisectionectomy | 13 (14) | 4 (9) | 9 (18) | |
| Others | 16 (17) | 7 (16) | 9 (18) | |
| Intraoperative blood transfusion | 0 (0–2) | 0 (0–2) | 0 (0–2) | 0.750 |
| Pathological examination | ||||
| R0 resection, n (%) | 88 (93) | 41 (93) | 47 (92) | 0.849 |
| pT category, n (%) | 0.400 | |||
| 1 | 38 (40) | 23 (51) | 15 (29) | |
| 2 | 41 (42) | 15 (34) | 26 (51) | |
| 3 | 12 (13) | 5 (11) | 7 (14) | |
| 4 | 5 (5) | 2 (4) | 3 (6) | |
| pN category | 0.854 | |||
| N0 | 63 (70) | 29 (69) | 34 (71) | |
| N1 | 27 (30) | 13 (31) | 14 (29) | |
| Tumor grading, n (%) | 0.114 | |||
| G1 | 0 | 0 | 0 | |
| G2 | 66 (76) | 35 (83) | 31 (69) | |
| G3 | 21 (24) | 7 (17) | 14 (31) | |
| G4 | 0 | 0 | 0 | |
| MVI, n (%) | 32 (35) | 12 (28.6) | 20 (40) | 0.252 |
| LVI, n (%) | 17 (19) | 7 (17) | 10 (21) | 0.618 |
| PNI, n (%) | 22 (46) | 11 (58) | 11 (38) | 0.175 |
| Postoperative Data | ||||
| Intensive care, days | 1 (1–2) | 1 (1–1) | 1 (1–2) | 0.114 |
| Hospitalization, days | 13 (8–24) | 14 (8–26) | 12 (8–22) | 0.769 |
| Postoperative complications, n (%) | 0.898 | |||
| No complications | 36 (38) | 15 (33) | 21 (41) | |
| Clavien–Dindo I | 2 (2) | 1 (2) | 1 (2) | |
| Clavien–Dindo II | 24 (25) | 13 (29) | 11 (22) | |
| Clavien–Dindo IIIa | 19 (20) | 10 (22) | 9 (18) | |
| Clavien–Dindo IIIb | 9 (9) | 4 (9) | 5 (10) | |
| Clavien–Dindo IVa | 6 (6) | 2 (4) | 4 (8) | |
| Clavien–Dindo IVb | 0 | 0 | 0 | |
| Clavien–Dindo V | 0 | 0 | 0 | |
| Oncologic Data | ||||
| Adjuvant therapy | 30 (31) | 10 (22) | 20 (39) | 0.073 |
| Neoadjuvant therapy, n (%) | 8 (8) | 3 (7) | 5 (10) | 0.579 |
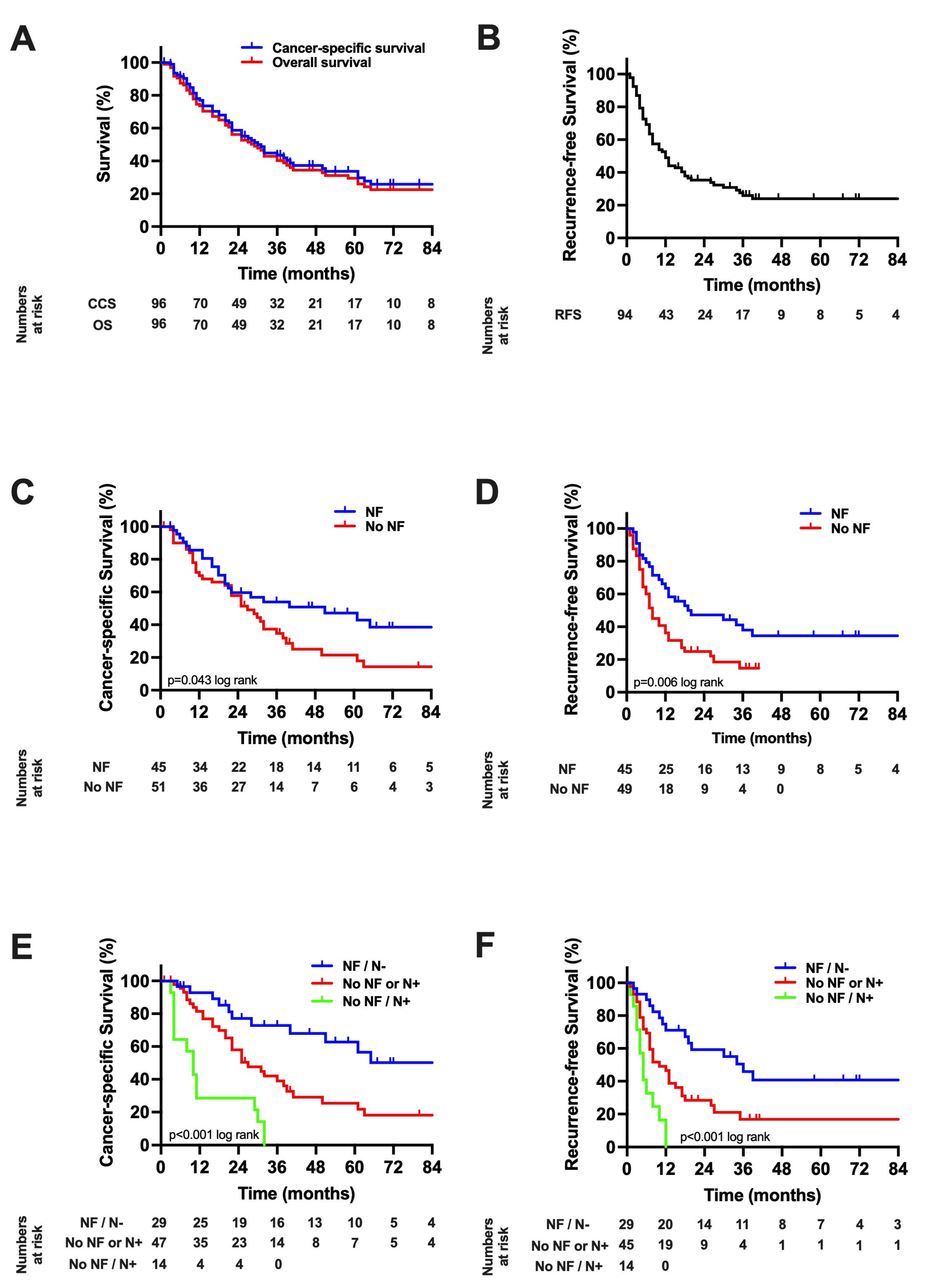
| Median RFS, months (95% CI) | 12 (8–16) | 20 (0–41) | 8 (5–11) | 0.006 |
| Median CSS, months (95% CI) | 30 (23–37) | 51 (12–90) | 27 (19–35) | 0.043 |
| Univariate Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Demographics | ||||
| Sex (male = 1) | 0.76 (0.45–1.27) | 0.297 | ||
| Age (≤65 years = 1) | 1.30 (0.77–2.15) | 0.330 | ||
| BMI (≤25 kg/m2 = 1) | 1.17 (0.67–1.96) | 0.549 | ||
| ASA (I/II = 1) | 1.31 (0.79–2.19) | 0.299 | ||
| Clinical chemistry | ||||
| Albumin (≤45 g/L = 1) | 0.86 (0.52–1.43) | 0.560 | ||
| AST (≤35 U/L = 1) | 1.15 (0.69–1.93) | 0.588 | ||
| ALT (≤30 U/L = 1) | 1.38 (0.82–2.35) | 0.228 | ||
| GGT (≤120 U/L = 1) | 1.39 (0.83–2.34) | 0.214 | ||
| Bilirubin (≤0.5 mg/dL = 1) | 1.53 (0.91–2.57) | 0.105 | ||
| Alkaline phosphatase (≤115 U/L = 1) | 1.69 (0.99–2.89) | 0.054 | excluded | |
| Platelet count (≤250/nL = 1) | 0.82 (0.49–1.37) | 0.445 | ||
| INR (≤1 = 1) | 1.54 (0.91–2.61) | 0.107 | ||
| Hemoglobin (≤13 g/dL = 1) | 0.61 (0.37–1.03) | 0.063 | 0.51 (0.27–0.93) | 0.024 |
| Operative data | ||||
| Operative time (≤300 min = 1) | 1.11 (0.68–1.80) | 0.682 | ||
| Type of hepatectomy | 0.935 | |||
| Right/left hepatectomy | 1 | |||
| Others | 0.92 (0.541–1.62) | |||
| Blood transfusion (no = 1) | 1.52 (0.91–2.57) | 0.113 | ||
| Postoperative data | ||||
| Clavien–Dindo Score (CD I/II = 1) | 2.05 (1.22–3.47) | 0.007 | exlcuded | |
| Intensive care (≤1 day = 1) | 1.49 (0.85–2.62) | 0.168 | ||
| Hospitalization (≤13 days = 1) | 1.52 (0.91–2.54) | 0.106 | ||
| Pathological data | ||||
| R1 resection (no = 1) | 1.58 (0.63–3.96) | 0.329 | ||
| pT category (T1/T2 = 1) | 1.49 (0.81–2.77) | 0.203 | ||
| pN category (N0 = 1) | 4.32 (2.48–7.52) | 0.001 | 4.78 (2.54–9.01) | 0.001 |
| Tumor grading (G1/G2 = 1) | 2.13 (1.16–3.89) | 0.014 | excluded | |
| MVI (no = 1) | 1.59 (0.95–2.68) | 0.078 | excluded | |
| LVI (no = 1) | 3.60 (1.92–6.76) | 0.001 | excluded | |
| PNI (no = 1) | 2.49 (1.23–5.01) | 0.011 | ||
| NF (no = 1) | 0.58 (0.34–0.99) | 0.048 | 0.47 (0.24–0.90) | 0.024 |
| Oncological data | ||||
| Neoadjuvant therapy (no = 1) | 2.18 (0.87–5.50) | 0.098 | 8.84 (2.20–35.49) | 0.002 |
| Adjuvant therapy (no = 1) | 1.17 (0.67–2.04) | 0.587 | ||
| Univariate Analysis | Multivariable Analysis | |||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Demographics | ||||
| Sex (male = 1) | 1.00 (0.60–1.66) | 0.993 | ||
| Age (≤65 years = 1) | 0.92 (0.56–1.52) | 0.755 | ||
| BMI (≤25 kg/m2 = 1) | 0.84 (0.51–1.38) | 0.486 | ||
| ASA (I/II = 1) | 1.25 (0.76–2.05) | 0.383 | ||
| Clinical chemistry | ||||
| Albumin (≤45 g/L = 1) | 0.96 (0.59–1.58) | 0.872 | ||
| AST (≤35 U/L = 1) | 0.97 (0.59–1.60) | 0.916 | ||
| ALT (≤30 U/L = 1) | 1.34 (0.81–2.24) | 0.258 | ||
| GGT (≤120 U/L = 1) | 1.47 (0.89–2.45) | 0.137 | ||
| Bilirubin (≤0.5 mg/dL = 1) | 1.31 (0.79–2.17) | 0.302 | ||
| Alkaline phosphatase (≤115 U/L = 1) | ||||
| Platelet count (≤250/nL = 1) | 0.79 (0.48–1.32) | 0.373 | ||
| INR (≤1 = 1) | 1.56 (0.92–2.65) | 0.099 | excluded | |
| Hemoglobin (≤13 g/dL = 1) | 0.67 (0.40–1.10) | 0.112 | ||
| Operative data | ||||
| Operative time (≤300 min = 1) | 1.05 (0.64–1.74) | 0.837 | ||
| Type of hepatectomy | 0.538 | |||
| Right/left hepatectomy | 1 | |||
| Others | 1.18 (0.68–2.03) | |||
| Blood transfusion (no = 1) | 1.74 (1.04–2.90) | 0.034 | excluded | |
| Postoperative data | ||||
| Clavien–Dindo Score (CD I/II = 1) | 1.78 (1.06–2.99) | 0.028 | excluded | |
| Intensive care (≤1 day = 1) | 1.27 (0.73–2.21) | 0.410 | ||
| Hospitalization (≤13 days = 1) | 1.73 (1.05–2.85) | 0.031 | 1.78 (1.00–3.15) | 0.049 |
| Pathological data | ||||
| R1 resection (no = 1) | 1.62 (0.64–4.07) | 0.310 | ||
| pT category (T1/T2 = 1) | 0.98 (0.48–1.98) | 0.943 | ||
| pN category (N0 = 1) | 2.84 (1.61–5.03) | 0.001 | 2.36 (1.23–4.52) | 0.010 |
| Tumor grading (G1/G2 = 1) | 1.32 (0.71–2.47) | 0.386 | ||
| MVI (no = 1) | 1.93 (1.15–3.21) | 0.012 | excluded | |
| LVI (no = 1) | 2.22 (1.19–4.17) | 0.013 | excluded | |
| PNI (no = 1) | 1.38 (0.69–2.87) | 0.382 | ||
| NF (no = 1) | 1.98 (1.19–3.31) | 0.009 | 0.39 (0.21–0.71) | 0.002 |
| Oncological data | ||||
| Neoadjuvant therapy (no = 1) | 1.96 (0.84–4.60) | 0.121 | ||
| Adjuvant therapy (no = 1) | 1.15 (0.68–1.95) | 0.597 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bednarsch, J.; Tan, X.; Czigany, Z.; Liu, D.; Lang, S.A.; Sivakumar, S.; Kather, J.N.; Appinger, S.; Rosin, M.; Boroojerdi, S.; et al. The Presence of Small Nerve Fibers in the Tumor Microenvironment as Predictive Biomarker of Oncological Outcome Following Partial Hepatectomy for Intrahepatic Cholangiocarcinoma. Cancers 2021, 13, 3661. https://doi.org/10.3390/cancers13153661
Bednarsch J, Tan X, Czigany Z, Liu D, Lang SA, Sivakumar S, Kather JN, Appinger S, Rosin M, Boroojerdi S, et al. The Presence of Small Nerve Fibers in the Tumor Microenvironment as Predictive Biomarker of Oncological Outcome Following Partial Hepatectomy for Intrahepatic Cholangiocarcinoma. Cancers. 2021; 13(15):3661. https://doi.org/10.3390/cancers13153661
Chicago/Turabian StyleBednarsch, Jan, Xiuxiang Tan, Zoltan Czigany, Dong Liu, Sven Arke Lang, Shivan Sivakumar, Jakob Nikolas Kather, Simone Appinger, Mika Rosin, Shiva Boroojerdi, and et al. 2021. "The Presence of Small Nerve Fibers in the Tumor Microenvironment as Predictive Biomarker of Oncological Outcome Following Partial Hepatectomy for Intrahepatic Cholangiocarcinoma" Cancers 13, no. 15: 3661. https://doi.org/10.3390/cancers13153661
APA StyleBednarsch, J., Tan, X., Czigany, Z., Liu, D., Lang, S. A., Sivakumar, S., Kather, J. N., Appinger, S., Rosin, M., Boroojerdi, S., Dahl, E., Gaisa, N. T., den Dulk, M., Coolsen, M., Ulmer, T. F., Neumann, U. P., & Heij, L. R. (2021). The Presence of Small Nerve Fibers in the Tumor Microenvironment as Predictive Biomarker of Oncological Outcome Following Partial Hepatectomy for Intrahepatic Cholangiocarcinoma. Cancers, 13(15), 3661. https://doi.org/10.3390/cancers13153661