
Reconsideration of the Appropriate Dissection Range Based on Japanese Anatomical Classification for Resectable Pancreatic Head Cancer in the Era of Multimodal Treatment

 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Is “Regional LYMPH Node Dissection” Required?
3. Is “Dissection to Achieve R0 RESECTION” Required?
4. The Issue Regarding Tumor Infiltration of Nerve and Fibrous Tissues
5. Determination of the Appropriate Dissection Range
6. Anatomical Landmarks Used to Determine the Appropriate Dissection Range at Each Surgical Site
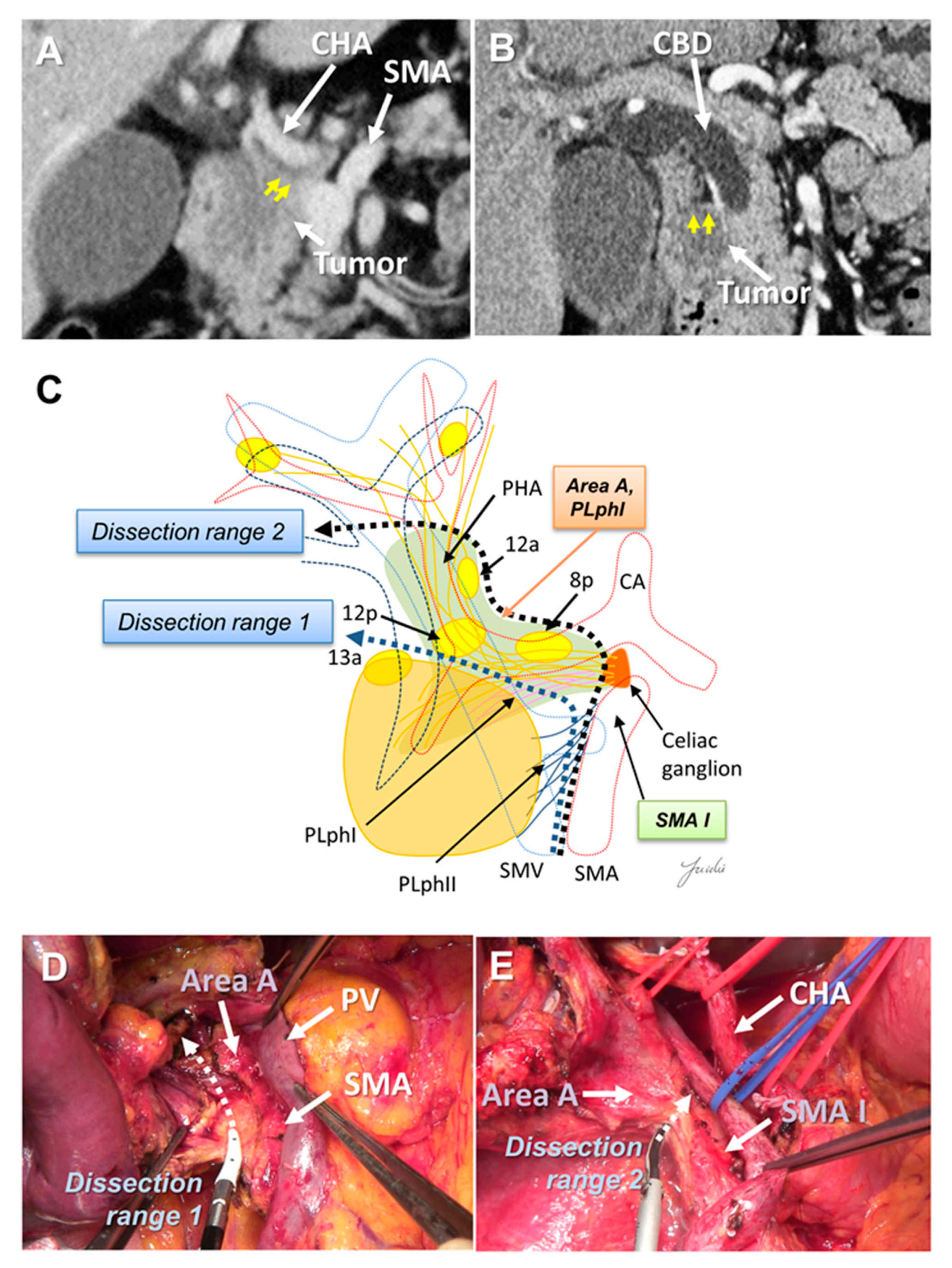
6.1. Dissection around the Hepatoduodenal Ligament and Common Hepatic Artery
6.2. Posterior Dissection
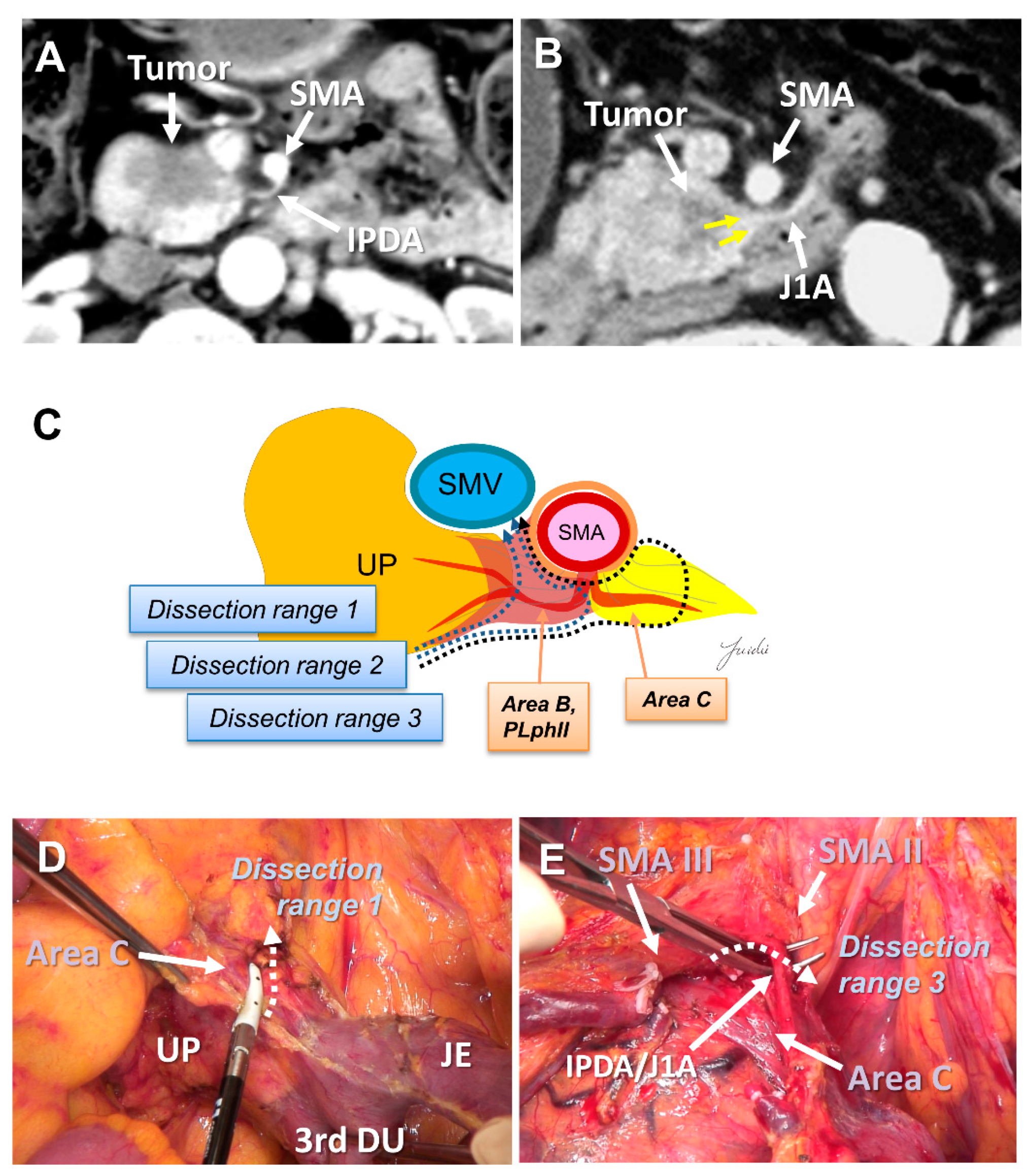
6.3. Dissection around the Superior Mesenteric Artery
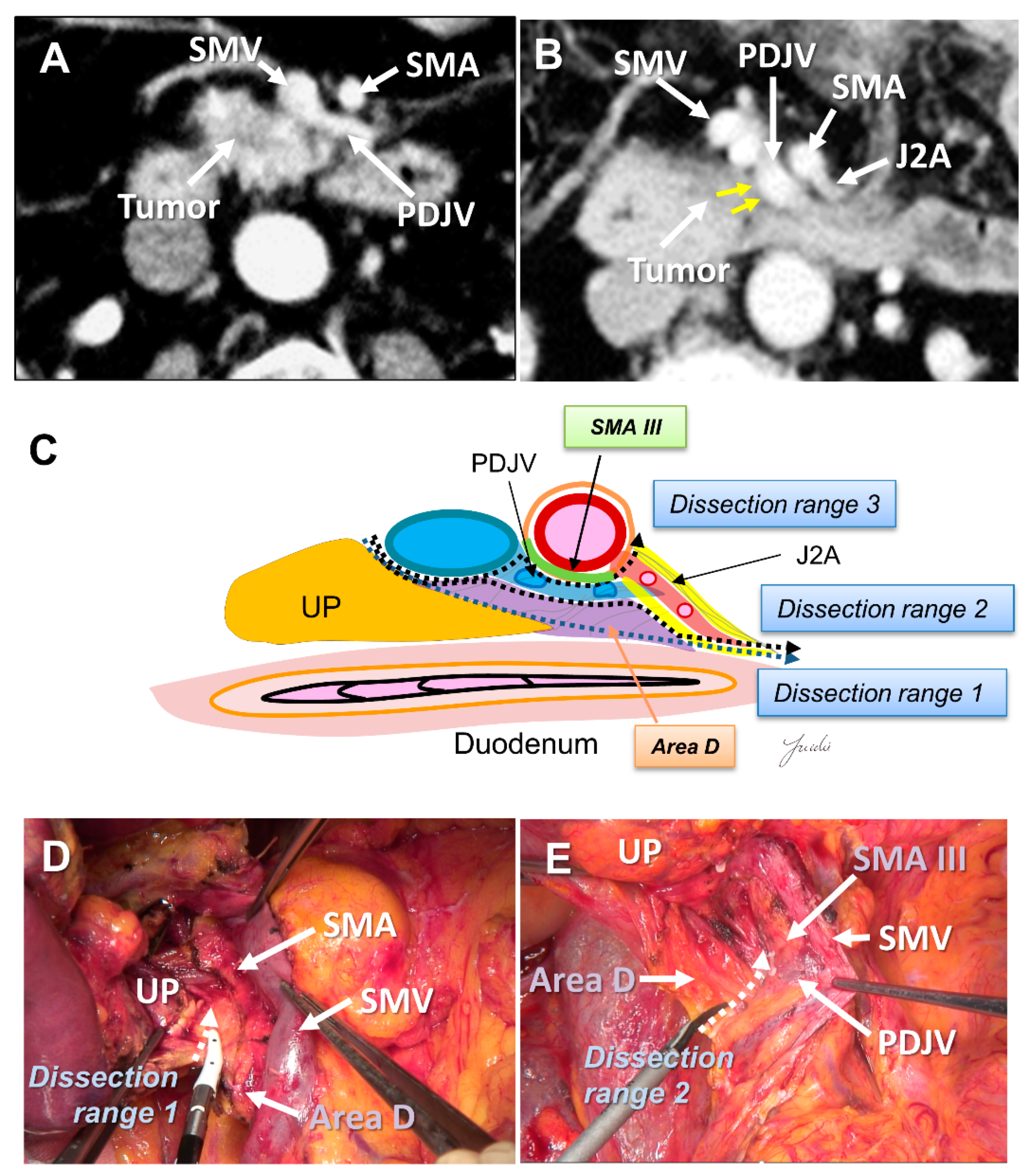
6.4. Portal Vein and/or Superior Mesenteric Vein Resection
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pedrazzoli, S.; DiCarlo, V.; Dionigi, R.; Mosca, F.; Pederzoli, P.; Pasquali, C.; Klöppel, G.; Dhaene, K.; Michelassi, F. Standard Versus Extended Lymphadenectomy Associated with Pancreatoduodenectomy in the Surgical Treatment of Adenocarcinoma of the Head of the Pancreas: A Multicenter, Prospective, Randomized Study. Lymphadenectomy Study Group. Ann. Surg. 1998, 228, 508–517. [Google Scholar] [CrossRef]
- Yeo, C.J.; Cameron, J.L.; Lillemoe, K.D.; Sohn, T.A.; Campbell, K.A.; Sauter, P.K.; Coleman, J.; Abrams, R.A.; Hruban, R.H. Pancreaticoduodenectomy with or without Distal Gastrectomy and Extended Retroperitoneal Lymphadenectomy for Periampullary Adenocarcinoma, Part 2: Randomized Controlled Trial Evaluating Survival, Morbidity, and Mortality. Ann. Surg. 2002, 236, 355–366. [Google Scholar] [CrossRef]
- Farnell, M.B.; Pearson, R.K.; Sarr, M.G.; DiMagno, E.P.; Burgart, L.J.; Dahl, T.R.; Foster, N.; Sargent, D.J.; Pancreas Cancer Working Group. A Prospective Randomized Trial Comparing Standard Pancreatoduodenectomy with Pancreatoduodenectomy with Extended Lymphadenectomy in Resectable Pancreatic Head Adenocarcinoma. Surgery 2005, 138, 618–628. [Google Scholar] [CrossRef]
- Nimura, Y.; Nagino, M.; Takao, S.; Takada, T.; Miyazaki, K.; Kawarada, Y.; Miyagawa, S.; Yamaguchi, A.; Ishiyama, S.; Takeda, Y.; et al. Standard Versus Extended Lymphadenectomy in Radical Pancreatoduodenectomy for Ductal Adenocarcinoma of the Head of the Pancreas: Long-Term Results of a Japanese Multicenter Randomized Controlled Trial. J. Hepato-Bil. Pancreat. Sci. 2012, 19, 230–241. [Google Scholar] [CrossRef]
- Jang, J.Y.; Kang, M.J.; Heo, J.S.; Choi, S.H.; Choi, D.W.; Park, S.J.; Han, S.S.; Yoon, D.S.; Yu, H.C.; Kang, K.J.; et al. A Prospective Randomized Controlled Study Comparing Outcomes of Standard Resection and Extended Resection, Including Dissection of the Nerve Plexus and Various Lymph Nodes, in Patients with Pancreatic Head Cancer. Ann. Surg. 2014, 259, 656–664. [Google Scholar] [CrossRef] [Green Version]
- Oettle, H.; Neuhaus, P.; Hochhaus, A.; Hartmann, J.T.; Gellert, K.; Ridwelski, K.; Niedergethmann, M.; Zülke, C.; Fahlke, J.; Arning, M.B.; et al. Adjuvant Chemotherapy with Gemcitabine and Long-Term Outcomes Among Patients with Resected Pancreatic Cancer: The CONKO-001 Randomized Trial. JAMA 2013, 310, 1473–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, H.; Ioka, T.; Ikeda, M.; Ohkawa, S.; Yanagimoto, H.; Boku, N.; Fukutomi, A.; Sugimori, K.; Baba, H.; Yamao, K.; et al. Randomized phase III Study of Gemcitabine plus S-1, S-1 Alone, or Gemcitabine Alone in Patients with Locally Advanced and Metastatic Pancreatic Cancer in Japan and Taiwan: GEST Study. J. Clin. Oncol. 2013, 31, 1640–1648. [Google Scholar] [CrossRef] [PubMed]
- Motoi, F.; Kosuge, T.; Ueno, H.; Yamaue, H.; Satoi, S.; Sho, M.; Honda, G.; Matsumoto, I.; Wada, K.; Furuse, J.; et al. Randomized phase II/III Trial of Neoadjuvant Chemotherapy with Gemcitabine and S-1 Versus Upfront Surgery for Resectable Pancreatic Cancer (Prep-02/JSAP05). Jpn. J. Clin. Oncol. 2019, 49, 190–194. [Google Scholar] [CrossRef] [Green Version]
- Lim, J.E.; Chien, M.W.; Earle, C.C. Prognostic Factors Following Curative Resection for Pancreatic Adenocarcinoma: A Population-Based, Linked Database Analysis of 396 Patients. Ann. Surg. 2003, 237, 74–85. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, I.; Warschkow, R.; Hackert, T.; Schmied, B.M.; Büchler, M.W.; Strobel, O.; Ulrich, A. Staging of Pancreatic Cancer Based on the Number of Positive Lymph Nodes. Br. J. Surg. 2017, 104, 608–618. [Google Scholar] [CrossRef] [PubMed]
- Lowder, C.Y.; Metkus, J.; Epstein, J.; Kozak, G.M.; Lavu, H.; Yeo, C.J.; Winter, J.M. Clinical Implications of Extensive Lymph Node Metastases for Resected Pancreatic Cancer. Ann. Surg. Oncol. 2018, 25, 4004–4011. [Google Scholar] [CrossRef] [PubMed]
- Fortner, J.G. Regional Pancreatectomy for Cancer of the Pancreas, Ampulla, and Other Related Sites. Tumor Staging and Results. Ann. Surg. 1984, 199, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Nagakawa, T.; Nagamori, M.; Futakami, F.; Tsukioka, Y.; Kayahara, M.; Ohta, T.; Ueno, K.; Miyazaki, I. Results of Extensive Surgery for Pancreatic Carcinoma. Cancer 1996, 77, 640–645. [Google Scholar] [CrossRef]
- Contreras, C.M.; Lin, C.P.; Oster, R.A.; Reddy, S.; Wang, T.; Vickers, S.; Heslin, M. Increased Pancreatic Cancer Survival with Greater Lymph Node Retrieval in the National Cancer Data Base. Am. J. Surg. 2017, 214, 442–449. [Google Scholar] [CrossRef]
- Japan Pancreas Society. Classification of Pancreatic Carcinoma, 4th ed.; Kanehara Press: Tokyo, Japan, 2017; Available online: http://www.suizou.org/pdf/Classification_of_Pancreatic_Carcinoma_4th_Engl_ed.pdf (accessed on 17 June 2021).
- Tol, J.A.; Gouma, D.J.; Bassi, C.; Dervenis, C.; Montorsi, M.; Adham, M.; Andrén-Sandberg, A.; Asbun, H.J.; Bockhorn, M.; Büchler, M.W.; et al. Definition of a Standard Lymphadenectomy in Surgery for Pancreatic Ductal Adenocarcinoma: A Consensus Statement by the International Study Group on Pancreatic Surgery (ISGPS). Surgery 2014, 156, 591–600. [Google Scholar] [CrossRef]
- Imamura, T.; Yamamoto, Y.; Sugiura, T.; Okamura, Y.; Ito, T.; Ashida, R.; Ohgi, K.; Uesaka, K. Reconsidering the Optimal Regional Lymph Node Staion According to Tumor Location for Pancreatic Cancer. Ann. Surg. Oncol. 2021, 28, 1602–1611. [Google Scholar] [CrossRef] [PubMed]
- Bilimoria, K.Y.; Talamonti, M.S.; Sener, S.F.; Bilimoria, M.M.; Stewart, A.K.; Winchester, D.P.; Ko, C.Y.; Bentrem, D.J. Effect of Hospital Volume on Margin Status After Pancreaticoduodenectomy for Cancer. J. Am. Coll. Surg. 2008, 207, 510–519. [Google Scholar] [CrossRef] [PubMed]
- Winter, J.M.; Cameron, J.L.; Campbell, K.A.; Arnold, M.A.; Chang, D.C.; Coleman, J.; Hodgin, M.B.; Sauter, P.K.; Hruban, R.H.; Riall, T.S.; et al. 1423 Pancreaticoduodenectomies for Pancreatic Cancer: A Single-Institution Experience. J. Gastrointest. Surg. 2006, 10, 1199–1210. [Google Scholar] [CrossRef]
- Ghaneh, P.; Kleeff, J.; Halloran, C.M.; Raraty, M.; Jackson, R.; Melling, J.; Jones, O.; Palmer, D.H.; Cox, T.F.; Smith, C.J.; et al. The Impact of Positive Resection Margins on Survival and Recurrence Following Resection and Adjuvant Chemotherapy for Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2019, 269, 520–529. [Google Scholar] [CrossRef]
- Schmocker, R.K.; Delitto, D.; Wright, M.J.; Ding, D.; Cameron, J.L.; Lafaro, K.J.; Burns, W.R.; Wolfgang, C.L.; Burkhart, R.A.; He, J. Impact of Margin Status on Survival in Patients with Pancreatic Ductal Adenocarcinoma Receiving Neoadjuvant Chemotherapy. J. Am. Coll. Surg. 2021, 232, 405–413. [Google Scholar] [CrossRef]
- Verbeke, C.S. Resection Margins and R1 Rates in Pancreatic Cancer—Are We There Yet? Histopathology 2008, 52, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Strobel, O.; Hank, T.; Hinz, U.; Bergmann, F.; Schneider, L.; Springfeld, C.; Jäger, D.; Schirmacher, P.; Hackert, T.; Büchler, M.W. Pancreatic Cancer Surgery: The New R-status Counts. Ann. Surg. 2017, 265, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Hruban, R.H.; Pitman, M.B.; Klimstra, D. Tumors of the pancreas. In Fascicle 6, Atlas of Tumor Pathology, 4th ed.; American Registry of Pathology, Armed Forces Institutes of Pathology: Washington, DC, USA, 2007. [Google Scholar]
- The Royal College of Pathologists. Standards and Datasets for Reporting Cancers. In Dataset for the Histopathological Reporting of Carcinomas of the Pancreas, Ampulla of Vater and Common Bile Duct, 2nd ed.; The Royal College of Pathologists: London, UK, 2019. [Google Scholar]
- Markov, P.; Satoi, S.; Kon, M. Redefining the R1 resection in patients with pancreatic ductal adenocarcinoma. J. Hepatobiliary Pancreat. Sci. 2016, 23, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Ohigashi, H.; Ishikawa, O.; Gotoh, K.; Yamada, T.; Nagata, S.; Tomita, Y.; Eguchi, H.; Doki, Y.; Yano, M. Perineural invasion and lymph node involvement as indicators of surgical outcome and pattern of recurrence in the setting of preoperative gemcitabine-based chemoradiation therapy for resectable pancreatic cancer. Ann. Surg. 2012, 255, 95–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.W.; Bhandari, M.; Astill, D.S.; Wilson, T.G.; Kow, L.; Brooke-Smith, M.; Toouli, J.; Padbury, R.T. Predicting patient survival after pancreaticoduodenectomy for malignancy: Histopathological criteria based on perineural infiltration and lymphovascular invasion. HPB (Oxford) 2010, 12, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagakawa, Y.; Yi, S.Q.; Takishita, C.; Sahara, Y.; Osakabe, H.; Kiya, Y.; Yamaguchi, H.; Miwa, Y.; Sato, I.; Tsuchida, A. Precise Anatomical Resection Based on Structures of Nerve and Fibrous Tissue Around the Superior Mesenteric Artery for Mesopancreas Dissection in Pancreaticoduodenectomy for Pancreatic Cancer. J. Hepato-Bil. Pancreat. Sci. 2020, 27, 342–351. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, P.; Volk, A.; Welsch, T.; Hackl, J.; Reissfelder, C.; Rahbari, M.; Distler, M.; Saeger, H.D.; Weitz, J.; Rahbari, N.N. Impact of Intraoperative Re-resection to Achieve R0 Status on Survival in Patients with Pancreatic Cancer: A Single-center Experience with 483 Patients. Ann. Surg. 2017, 265, 1219–1225. [Google Scholar] [CrossRef]
- Yin, Z.; Zhou, Y.; Hou, B.; Ma, T.; Yu, M.; Zhang, C.; Lu, X.; Jian, Z. Revision of Surgical Margin under Frozen Section to Achieve R0 Status on Survival in Patients with Pancreatic Cancer. J. Gastrointest. Surg. 2018, 22, 1565–1575. [Google Scholar] [CrossRef]
- Hernandez, J.; Mullinax, J.; Clark, W.; Toomey, P.; Villadolid, D.; Morton, C.; Ross, S.; Rosemurgy, A. Survival after Pancreaticoduodenectomy is not Improved by Extending Resections to Achieve Negative Margins. Ann. Surg. 2009, 250, 76–80. [Google Scholar] [CrossRef]
- Barreto, S.G.; Pandanaboyana, S.; Ironside, N.; Windsor, J.A. Does Revision of Resection Margins Based on Frozen Section Improve Overall Survival Following Pancreatoduodenectomy for Pancreatic Ductal Adenocarcinoma? A Meta-analysis. HPB (Oxford) 2017, 19, 573–579. [Google Scholar] [CrossRef] [Green Version]
- Kang, M.J.; Jang, J.Y.; Lee, S.E.; Lim, C.S.; Lee, K.U.; Kim, S.W. Comparison of the Long-Term Outcomes of Uncinate Process Cancer and non-Uncinate Process Pancreas Head Cancer: Poor Prognosis Accompanied by Early Locoregional Recurrence. Langenbecks Arch. Surg. 2010, 395, 697–706. [Google Scholar] [CrossRef]
- El Nakeeb, A.; Roshdy, S.; Ask, W.; Sonbl, A.; Ali, M.; Abdelwahab, K.; Shams, N.; Abdelwahab, M. Comparative Study Between Uncinate Process Carcinoma and Pancreatic Head Carcinoma After Pancreaticodudenectomy (Clincopathological Features and Surgical Outcomes). Hepato-Gastroenterology 2014, 61, 1748–1755. [Google Scholar]
- Padilla-Thornton, A.E.; Willmann, J.K.; Jeffrey, R.B. Adenocarcinoma of the Uncinate Process of the Pancreas: MDCT Patterns of Local Invasion and Clinical Features at Presentation. Eur. Rad. 2012, 22, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Tian, X.; Xie, X.; Gao, H.; Zhuang, Y.; Yang, Y. Comparison of Uncinate Process Cancer and Non-Uncinate Process Pancreatic Head Cancer. J. Cancer 2016, 7, 1242–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, H.; Mori, H.; Matsumoto, S.; Yamada, Y.; Kiyosue, H.; Ohta, M.; Kitano, S. Extrapancreatic Neural Plexus Invasion by Carcinomas of the Pancreatic Head Region: Evaluation Using Thin-Section Helical CT. Radiat. Med. 2007, 25, 141–147. [Google Scholar] [CrossRef]
- Mochizuki, K.; Gabata, T.; Kozaka, K.; Hattori, Y.; Zen, Y.; Kitagawa, H.; Kayahara, M.; Ohta, T.; Matsui, O. MDCT Findings of Extrapancreatic Nerve Plexus Invasion by Pancreas Head Carcinoma: Correlation with en Bloc Pathological Specimens and Diagnostic Accuracy. Eur. Rad. 2010, 20, 1757–1767. [Google Scholar] [CrossRef] [Green Version]
- Bae, J.S.; Kim, J.H.; Joo, I.; Chang, W.; Han, J.K. MDCT Findings Predicting Post-Operative Residual Tumor and Survival in Patients with Pancreatic Cancer. Eur. Rad. 2019, 29, 3714–3724. [Google Scholar] [CrossRef]
- Hirono, S.; Kawai, M.; Tani, M.; Okada, K.; Miyazawa, M.; Shimizu, A.; Kitahata, Y.; Yamaue, H. Indication for the Use of an Interposed Graft During Portal Vein and/or Superior Mesenteric Vein Reconstruction in Pancreatic Resection Based on Perioperative Outcomes. Langenbecks Arch. Surg. 2014, 399, 461–471. [Google Scholar] [CrossRef]
- Inoue, Y.; Saiura, A.; Yoshioka, R.; Ono, Y.; Takahashi, M.; Arita, J.; Takahashi, Y.; Koga, R. Pancreatoduodenectomy with Systematic Mesopancreas Dissection Using a Supracolic Anterior Artery-First Approach. Ann. Surg. 2015, 262, 1092–1101. [Google Scholar] [CrossRef]
- Sharma, D.; Isaji, S. Mesopancreas Is a Misnomer: Time to Correct the Nomenclature. J. Hepato-Bil. Pancreat. Sci. 2016, 23, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Nagakawa, Y.; Yi, S.Q.; Sahara, Y.; Hosokawa, Y.; Takishita, C.; Shirota, T.; Hijikata, Y.; Osakabe, H.; Nishino, H.; Akashi, M.; et al. Anatomical Structures of Nerve and Fibrous Tissues Around the Pancreatic Head -Pancreaticoduodenectomy Based on These Running Patterns for Pancreatic Cancer-, Overcoming Pancreatic Cancer -Focusing on Retro-Pancreatic Invasion-; Tanaka & Shobundo Graphic, Art. Co., Ltd: Kanazawa, Japan, 2019. [Google Scholar]
- Delpero, J.R.; Jeune, F.; Bachellier, P.; Regenet, N.; Le Treut, Y.P.; Paye, F.; Carrere, N.; Sauvanet, A.; Adham, M.; Autret, A.; et al. Prognostic Value of Resection Margin Involvement After Pancreaticoduodenectomy for Ductal Adenocarcinoma: Updates from a French Prospective Multicenter Study. Ann. Surg. 2017, 266, 787–796. [Google Scholar] [CrossRef]
- Kimura, W. Surgical Anatomy of the Pancreas for Limited Resection. J. Hepato-Bil. Pancreat. Surg. 2000, 7, 473–479. [Google Scholar] [CrossRef] [PubMed]
- Nagakawa, Y.; Hosokawa, Y.; Osakabe, H.; Sahara, Y.; Takishita, C.; Nakajima, T.; Hijikata, Y.; Kasahara, K.; Kazuhiko, K.; Saito, K.; et al. Pancreaticoduodenectomy with Right-Oblique Posterior Dissection of Superior Mesenteric Nerve Plexus Is Logical Procedure for Pancreatic Cancer with Extrapancreatic Nerve Plexus Invasion. Hepato-Gastroenterology 2014, 61, 2371–2376. [Google Scholar] [PubMed]
- Patel, B.N.; Giacomini, C.; Jeffrey, R.B.; Willmann, J.K.; Olcott, E. Three-Dimensional Volume-Rendered Multidetector CT Imaging of the Posterior Inferior Pancreaticoduodenal Artery: Its Anatomy and Role in Diagnosing Extrapancreatic Perineural Invasion. Cancer Imaging 2013, 13, 580–590. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gockel, I.; Domeyer, M.; Wolloscheck, T.; Konerding, M.A.; Junginger, T. Resection of the Mesopancreas (RMP): A New Surgical Classification of a Known Anatomical Space. World J. Surg. Oncol. 2007, 5, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaedcke, J.; Gunawan, B.; Grade, M.; Szöke, R.; Liersch, T.; Becker, H.; Ghadimi, B.M. The Mesopancreas Is the Primary Site for R1 Resection in Pancreatic Head Cancer: Relevance for Clinical Trials. Langenbecks Arch. Surg. 2010, 395, 451–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peparini, N.; Chirletti, P. Mesopancreas: A Boundless Structure, Namely R1 Risk in Pancreaticoduodenectomy for Pancreatic Head Carcinoma. Eur. J. Surg. Oncol. 2013, 39, 1303–1308. [Google Scholar] [CrossRef] [PubMed]
- Adham, M.; Singhirunnusorn, J. Surgical Technique and Results of Total Mesopancreas Excision (TMpE) in Pancreatic Tumors. Eur. J. Surg. Oncol. 2012, 38, 340–345. [Google Scholar] [CrossRef]
- Welsch, T.; Bork, U.; Distler, M.; Weitz, J. Top-Down Approach to the Superior Mesenteric Artery and the Mesopancreas During Pancreatoduodenectomy for Pancreatic Cancer. J. Surg. Oncol. 2016, 113, 668–671. [Google Scholar] [CrossRef]
- Kimura, W. Strategies for the Treatment of Invasive Ductal Carcinoma of the Pancreas and How to Achieve Zero Mortality for Pancreaticoduodenectomy. J. Hepato-Bil. Pancreat. Surg. 2008, 15, 270–277. [Google Scholar] [CrossRef]
- Sugiyama, M.; Suzuki, Y.; Nakazato, T.; Yokoyama, M.; Kogure, M.; Matsuki, R.; Abe, N. Vascular Anatomy of Mesopancreas in Pancreatoduodenectomy Using an Intestinal Derotation Procedure. World J. Surg. 2020, 44, 3441–3448. [Google Scholar] [CrossRef] [PubMed]
- Nagakawa, Y.; Hosokawa, Y.; Sahara, Y.; Takishita, C.; Hijikata, Y.; Osakabe, H.; Nakajima, T.; Shirota, T.; Katsumata, K.; Nakamura, M.; et al. Approaching the Superior Mesenteric Artery from the Right Side Using the Proximal-Dorsal Jejunal Vein Preisolation Method During Laparoscopic Pancreaticoduodenectomy. Surg. Endosc. 2018, 32, 4044–4051. [Google Scholar] [CrossRef] [PubMed]
- Nagakawa, Y.; Watanabe, Y.; Kozono, S.; Boggi, U.; Palanivelu, C.; Liu, R.; Wang, S.E.; He, J.; Nishino, H.; Ohtsuka, T.; et al. Surgical Approaches to the Superior Mesenteric Artery During Minimally Invasive Pancreaticoduodenectomy: A Systematic Review. J. Hepato-Bil. Pancreat. Sci. 2021. [Google Scholar] [CrossRef] [PubMed]
- Paiella, S.; Butturini, G.; Bassi, C. Different Ideas of Nodal Grouping in Standard and Extended Lymphadenectomy During Pancreaticoduodenectomy for Pancreatic Head Cancer. Ann. Surg. 2017, 265, E73–E74. [Google Scholar] [CrossRef] [PubMed]
- Jang, J.Y.; Kang, M.J.; Kim, S.W. Reply to “Different Ideas of Nodal Grouping in Standard and Extended Lymphadenectomy During Pancreaticoduodenectomy for Pancreatic Head Cancer”. Ann. Surg. 2017, 265, E74–E75. [Google Scholar] [CrossRef] [PubMed]
- Horiguchi, A.; Ishihara, S.; Ito, M.; Nagata, H.; Shimizu, T.; Furusawa, K.; Kato, R.; Katada, K.; Miyakawa, S. Pancreatoduodenectomy in Which Dissection of the Efferent Arteries of the Head of the Pancreas Is Performed First. J. Hepato-Bil. Pancreat. Surg. 2007, 14, 575–578. [Google Scholar] [CrossRef]
- Horiguchi, A.; Ishihara, S.; Ito, M.; Asano, Y.; Yamamoto, T.; Miyakawa, S. Three-Dimensional Models of Arteries Constructed Using Multidetector-Row CT Images to Perform Pancreatoduodenectomy Safely Following Dissection of the Inferior Pancreaticoduodenal Artery. J. Hepato-Bil. Pancreat. Sci. 2010, 17, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Negoi, I.; Beuran, M.; Hostiuc, S.; Negoi, R.I.; Inoue, Y. Surgical Anatomy of the Superior Mesenteric Vessels Related to Pancreaticoduodenectomy: A Systematic Review and Meta-Analysis. J. Gastrointest. Surg. 2018, 22, 802–817. [Google Scholar] [CrossRef]
- Onda, S.; Okamoto, T.; Kanehira, M.; Suzuki, F.; Ito, R.; Fujioka, S.; Suzuki, N.; Hattori, A.; Yanaga, K. Identification of Inferior Pancreaticoduodenal Artery During Pancreaticoduodenectomy Using Augmented Reality-Based Navigation System. J. Hepato-Bil. Pancreat. Sci. 2014, 21, 281–287. [Google Scholar] [CrossRef]
- Tomimaru, Y.; Tanaka, K.; Noguchi, K.; Morita, S.; Imamura, H.; Dono, K. The Branching Pattern of the Inferior Pancreaticoduodenal Artery in Patients with a Replaced Right Hepatic Artery. Am. Surg. 2018, 84, 796–800. [Google Scholar] [CrossRef]
- Nagakawa, Y.; Hosokawa, Y.; Sahara, Y.; Takishita, C.; Nakajima, T.; Hijikata, Y.; Tago, T.; Kasuya, K.; Tsuchida, A. A Novel “Artery First” Approach Allowing Safe Resection in Laparoscopic Pancreaticoduodenectomy: The Uncinate Process First Approach. Hepato-Gastroenterology 2015, 62, 1037–1040. [Google Scholar]
- Sanjay, P.; Takaori, K.; Govil, S.; Shrikhande, S.V.; Windsor, J.A. ‘Artery-first’ Approaches to Pancreatoduodenectomy. Br. J. Surg. 2012, 99, 1027–1035. [Google Scholar] [CrossRef]
- Nakao, A.; Harada, A.; Nonami, T.; Kaneko, T.; Inoue, S.; Takagi, H. Clinical Significance of Portal Invasion by Pancreatic Head Carcinoma. Surgery 1995, 117, 50–55. [Google Scholar] [CrossRef]
- Chua, T.C.; Saxena, A. Extended Pancreaticoduodenectomy with Vascular Resection for Pancreatic Cancer: A Systematic Review. J. Gastrointest. Surg. 2010, 14, 1442–1452. [Google Scholar] [CrossRef]
- Ravikumar, R.; Sabin, C.; Abu Hilal, M.; Bramhall, S.; White, S.; Wigmore, S.; Imber, C.J.; Fusai, G.; UK Vascular Resection in Pancreatic Cancer Study Group. Portal Vein Resection in Borderline Resectable Pancreatic Cancer: A United Kingdom Multicenter Study. J. Am. Coll. Surg. 2014, 218, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Kulemann, B.; Hoeppner, J.; Wittel, U.; Glatz, T.; Keck, T.; Wellner, U.F.; Bronsert, P.; Sick, O.; Hopt, U.T.; Makowiec, F.; et al. Perioperative and Long-Term Outcome After Standard Pancreaticoduodenectomy, Additional Portal Vein and Multivisceral Resection for Pancreatic Head Cancer. J. Gastrointest. Surg. 2015, 19, 438–444. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Satoi, S.; Motoi, F.; Sho, M.; Kawai, M.; Matsumoto, I.; Honda, G.; Multicentre Study Group of Pancreatobiliary Surgery (MSG-PBS). Portal or Superior Mesenteric Vein Resection in Pancreatoduodenectomy for Pancreatic Head Carcinoma. Br. J. Surg. 2015, 102, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Delpero, J.R.; Boher, J.M.; Sauvanet, A.; Le Treut, Y.P.; Sa-Cunha, A.; Mabrut, J.Y.; Chiche, L.; Turrini, O.; Bachellier, P.; Paye, F. Pancreatic Adenocarcinoma with Venous Involvement: Is Up-Front Synchronous Portal-Superior Mesenteric Vein Resection Still Justified? A Survey of the Association Française de Chirurgie. Ann. Surg. Oncol. 2015, 22, 1874–1883. [Google Scholar] [CrossRef]
- Giovinazzo, F.; Turri, G.; Katz, M.H.; Heaton, N.; Ahmed, I. Meta-Analysis of Benefits of Portal-Superior Mesenteric Vein Resection in Pancreatic Resection for Ductal Adenocarcinoma. Br. J. Surg. 2016, 103, 179–191. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Practice Guidelines for Pancreatic Cancer. Available online: https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf (accessed on 17 June 2021).
- Hosokawa, Y.; Nagakawa, Y.; Sahara, Y.; Takishita, C.; Nakajima, T.; Hijikata, Y.; Osakabe, H.; Shirota, T.; Saito, K.; Yamaguchi, H.; et al. Surgical Outcomes of Pancreaticoduodenectomy for Pancreatic Cancer with Proximal Dorsal Jejunal Vein Involvement. J. Gastrointest. Surg. 2018, 22, 1179–1185. [Google Scholar] [CrossRef]
- Honda, M.; Nagakawa, Y.; Akashi, M.; Hosokawa, Y.; Osakabe, H.; Takishita, C.; Nishino, H.; Tsuchida, A. Clinical Impact of Pancreaticoduodenectomy for Pancreatic Cancer with Resection of the Secondary or Later Branches of the Superior Mesenteric Vein. J. Hepato-Bil. Pancreat. Sci. 2020, 27, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Kang, M.J.; Jang, J.Y.; Chang, Y.R.; Jung, W.; Kim, S.W. Portal Vein Patency after Pancreatoduodenectomy for Periampullary Cancer. Br. J. Surg. 2015, 102, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Ohgi, K.; Sugiura, T.; Yamamoto, Y.; Okamura, Y.; Ito, T.; Ashida, R.; Aramaki, T.; Uesaka, K. Benign Portal Vein Stenosis After Pancreaticoduodenectomy. World J. Surg. 2019, 43, 2623–2630. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Ban, D.; Matsumura, S.; Mitsunori, Y.; Ochiai, T.; Kudo, A.; Tanaka, S.; Tanabe, M. Surgical Pitfalls of Jejunal Vein Anatomy in Pancreaticoduodenectomy. J. Hepato-Bil. Pancreat. Sci. 2017, 24, 394–400. [Google Scholar] [CrossRef]
- Nakamura, M.; Nakashima, H.; Tsutsumi, K.; Matsumoto, H.; Muta, Y.; Ueno, D.; Yoshida, K.; Hino, K.; Urakami, A.; Tanaka, M. First Jejunal Vein Oriented Mesenteric Excision for Pancreatoduodenectomy. J. Gastroenterol. 2013, 48, 989–995. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Number of Cases | Standard Dissection | Extended Dissection | Standard Dissection | Extended Dissection | Prognosis |
|---|---|---|---|---|---|---|---|---|
| Lymph Node Dissection * | SMA Nerve Plexus Dissection | |||||||
| Pedrazzoli S et al. [1] | 1998 | Italy | 81 | 5, 6, 12b, 13, 17 | 5, 6, 9, 12b, 13, 14, 17, 16a2, 16b1 | Not described | MST | |
| Standard: 335 days | ||||||||
| Extended: 500 days | ||||||||
| Yeo C et al. [2] | 2002 | United States | 299 | 12b2, 12c, 13, 14b, 14v, 17 | 3, 4, 5, 6, 9, 12b2, 12c, 13, 14b, 14v, 16a2, 16b1, 17 | Not described | 5-year survival rate | |
| Standard: 23% | ||||||||
| Extended: 29% | ||||||||
| Farnell M et al. [3] | 2005 | United States | 132 | 3, 4, 6, 8a, 12b1, 12b2, 12c, 13a, 13b, 14a, 14b, 17a, 17b | 3, 4, 6, 8a, 8p, 9, 12a1, 12a2, 12b1, 12b2, 12p1, 12p2, 12c, 13a, 13b, 14a, 14b, 14c, 14d, 14v, 16a2, 16b, 17a, 17b | Not described | 5-year survival rate | |
| Standard: 17% | ||||||||
| Extended: 16% | ||||||||
| Nimura Y et al. [4] | 2012 | Japan | 112 | 13a, 13b, 17a, 17b | 8a, 8p, 9, 14p, 1416a2, 16b112a, 12b, 12p | None | full circumference dissection | 5-year survival rate |
| Standard: 15.7% | ||||||||
| Extended: 6.0% | ||||||||
| Jang JY et al. [5] | 2014 | Korea | 244 | 12c, 13, 17 | 9, 12, 13, 14, 16, 17 | None | right half-circumferential dissection | 5-year survival rate |
| Standard: 44.5% | ||||||||
| Extended: 35.7% | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nagakawa, Y.; Nakagawa, N.; Takishita, C.; Uyama, I.; Kozono, S.; Osakabe, H.; Suzuki, K.; Nakagawa, N.; Hosokawa, Y.; Shirota, T.; et al. Reconsideration of the Appropriate Dissection Range Based on Japanese Anatomical Classification for Resectable Pancreatic Head Cancer in the Era of Multimodal Treatment. Cancers 2021, 13, 3605. https://doi.org/10.3390/cancers13143605
Nagakawa Y, Nakagawa N, Takishita C, Uyama I, Kozono S, Osakabe H, Suzuki K, Nakagawa N, Hosokawa Y, Shirota T, et al. Reconsideration of the Appropriate Dissection Range Based on Japanese Anatomical Classification for Resectable Pancreatic Head Cancer in the Era of Multimodal Treatment. Cancers. 2021; 13(14):3605. https://doi.org/10.3390/cancers13143605
Chicago/Turabian StyleNagakawa, Yuichi, Naoya Nakagawa, Chie Takishita, Ichiro Uyama, Shingo Kozono, Hiroaki Osakabe, Kenta Suzuki, Nobuhiko Nakagawa, Yuichi Hosokawa, Tomoki Shirota, and et al. 2021. "Reconsideration of the Appropriate Dissection Range Based on Japanese Anatomical Classification for Resectable Pancreatic Head Cancer in the Era of Multimodal Treatment" Cancers 13, no. 14: 3605. https://doi.org/10.3390/cancers13143605
APA StyleNagakawa, Y., Nakagawa, N., Takishita, C., Uyama, I., Kozono, S., Osakabe, H., Suzuki, K., Nakagawa, N., Hosokawa, Y., Shirota, T., Honda, M., Yamada, T., Katsumata, K., & Tsuchida, A. (2021). Reconsideration of the Appropriate Dissection Range Based on Japanese Anatomical Classification for Resectable Pancreatic Head Cancer in the Era of Multimodal Treatment. Cancers, 13(14), 3605. https://doi.org/10.3390/cancers13143605