
Role of Inflammatory and Immune-Nutritional Prognostic Markers in Patients Undergoing Surgical Resection for Biliary Tract Cancers


 ,
,  ,
,  ,
,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Statistical Analysis
3. Results
3.1. Clinical and Pathological Characteristics of the Study Population
3.2. Inflammatory Based and Nutritional Prognostic Scores of the Study Population
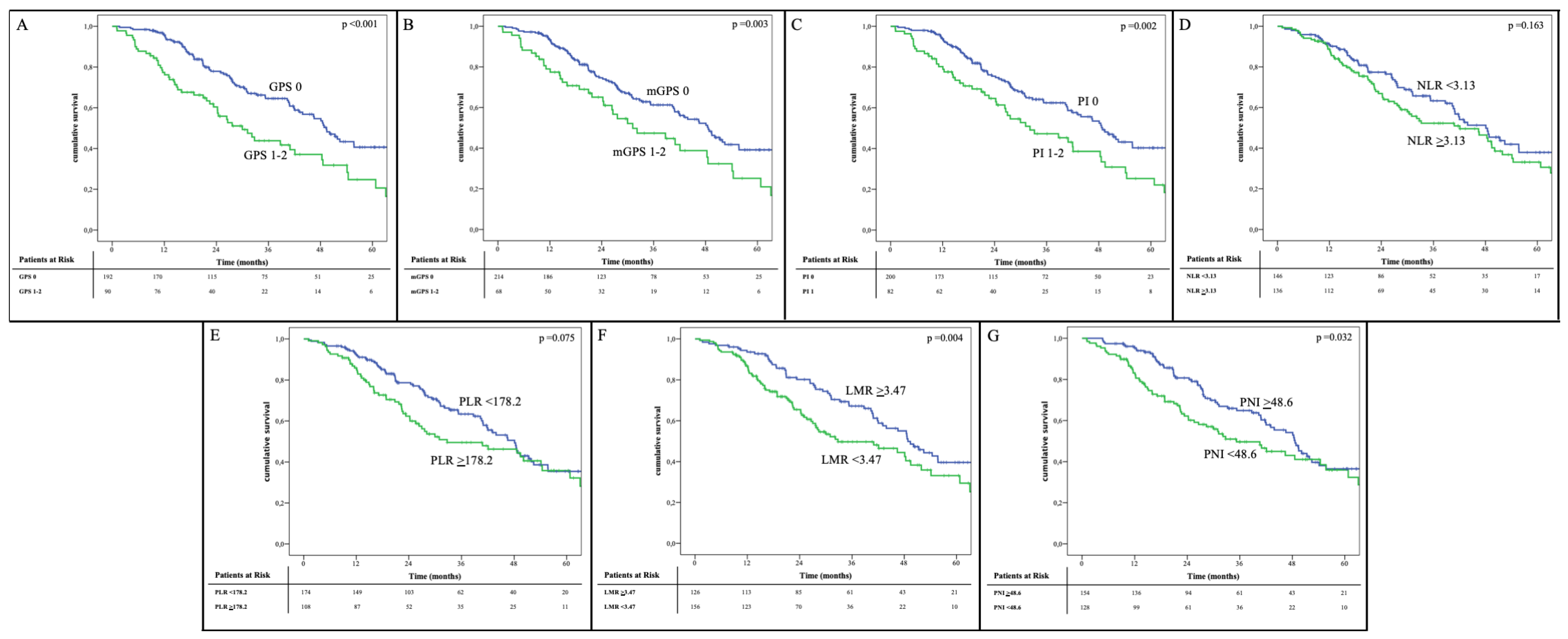
3.3. Prognostic Value of Inflammatory and Immune-Nutritional Prognostic Markers
3.4. Prognostic Factors of Overall Survival
3.5. Short Term Outcomes According to the Inflammatory and Nutritional Prognostic Markers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.Y.; Zhu, A.X. Biliary tract cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef]
- Miyazaki, M.; Ohtsuka, M.; Miyakawa, S.; Nagino, M.; Yamamoto, M.; Kokudo, N.; Sano, K.; Endo, I.; Unno, M.; Chijiiwa, K.; et al. Classification of biliary tract cancers established by the Japanese Society of Hepato-Biliary-Pancreatic Surgery: 3(rd) English edition. J. Hepato-Biliary-Pancreat. Sci. 2015, 22, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Conci, S.; Viganò, L.; Ercolani, G.; Gonzalez, E.; Ruzzenente, A.; Isa, G.; Salaris, C.; Fontana, A.; Bagante, F.; Pedrazzani, C.; et al. Outcomes of vascular resection associated with curative intent hepatectomy for intrahepatic cholangiocarcinoma. Eur. J. Surg. Oncol. 2020, 46, 1727–1733. [Google Scholar] [CrossRef]
- Ruzzenente, A.; Bagante, F.; Ardito, F.; Campagnaro, T.; Scoleri, I.; Conci, S.; Iacono, C.; Giuliante, F.; Guglielmi, A. Comparison of the 7th and 8th editions of the American Joint Committee on Cancer Staging Systems for perihilar cholangiocarcinoma. Surgery 2018, 164, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Ercolani, G.; Dazzi, A.; Giovinazzo, F.; Ruzzenente, A.; Bassi, C.; Guglielmi, A.; Scarpa, A.; D’Errico, A.; Pinna, A.D. Intrahepatic, peri-hilar and distal cholangiocarcinoma: Three different locations of the same tumor or three different tumors? Eur. J. Surg. Oncol. 2015, 41, 1162–1169. [Google Scholar] [CrossRef]
- Birnbaum, D.J.; Viganò, L.; Ferrero, A.; Langella, S.; Russolillo, N.; Capussotti, L. Locally advanced gallbladder cancer: Which patients benefit from resection? Eur. J. Surg. Oncol. 2014, 40, 1008–1015. [Google Scholar] [CrossRef]
- Boilève, A.; Hilmi, M.; Gougis, P.; Cohen, R.; Rousseau, B.; Blanc, J.F.; Ben Abdelghani, M.; Castanié, H.; Dahan, L.; Tougeron, D.; et al. Triplet combination of durvalumab, tremelimumab, and paclitaxel in biliary tract carcinomas: Safety run-in results of the randomized IMMUNOBIL PRODIGE 57 phase II trial. Eur. J. Cancer 2021, 143, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Subbiah, V.; Lassen, U.; Élez, E.; Italiano, A.; Curigliano, G.; Javle, M.; de Braud, F.; Prager, G.W.; Greil, R.; Stein, A.; et al. Dabrafenib plus trametinib in patients with BRAFV600E-mutated biliary tract cancer (ROAR): A phase 2, open-label, single-arm, multicentre basket trial. Lancet Oncol. 2020, 21, 1234–1243. [Google Scholar] [CrossRef]
- Klein, O.; Kee, D.; Nagrial, A.; Markman, B.; Underhill, C.; Michael, M.; Jackett, L.; Lum, C.; Behren, A.; Palmer, J.; et al. Evaluation of Combination Nivolumab and Ipilimumab Immunotherapy in Patients With Advanced Biliary Tract Cancers: Subgroup Analysis of a Phase 2 Nonrandomized Clinical Trial. JAMA Oncol. 2020, 6, 1405–1409. [Google Scholar] [CrossRef]
- Philip, M.; Rowley, D.A.; Schreiber, H. Inflammation as a tumor promoter in cancer induction. Semin. Cancer Biol. 2004, 14, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Bullock, A.F.; Greenley, S.L.; McKenzie, G.A.G.; Paton, L.W.; Johnson, M.J. Relationship between markers of malnutrition and clinical outcomes in older adults with cancer: Systematic review, narrative synthesis and meta-analysis. Eur. J. Clin. Nutr. 2020, 74, 1519–1535. [Google Scholar] [CrossRef]
- Yalcin, S.; Gumus, M.; Oksuzoglu, B.; Ozdemir, F.; Evrensel, T.; Sarioglu, A.A.; Sahin, B.; Mandel, N.M.; Goker, E. Aspect of Cancer Care in Medical Oncology Patients. Clin. Ther. 2019, 41, 2382–2396. [Google Scholar] [CrossRef]
- Forrest, L.M.; McMillan, D.C.; McArdle, C.S.; Angerson, W.J.; Dunlop, D.J. Evaluation of cumulative prognostic scores based on the systemic inflammatory response in patients with inoperable non-small-cell lung cancer. Br. J. Cancer 2003, 89, 1028–1030. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proctor, M.J.; Morrison, D.S.; Talwar, D.; Balmer, S.M.; O’Reilly, D.S.; Foulis, A.K.; Horgan, P.G.; McMillan, D.C. An inflammation-based prognostic score (mGPS) predicts cancer survival independent of tumour site: A Glasgow Inflammation Outcome Study. Br. J. Cancer 2011, 104, 726–734. [Google Scholar] [CrossRef] [Green Version]
- Kasymjanova, G.; MacDonald, N.; Agulnik, J.S.; Cohen, V.; Pepe, C.; Kreisman, H.; Sharma, R.; Small, D. The predictive value of pre-treatment inflammatory markers in advanced non-small-cell lung cancer. Curr. Oncol. 2010, 17, 52–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mano, Y.; Shirabe, K.; Yamashita, Y.; Harimoto, N.; Tsujita, E.; Takeishi, K.; Aishima, S.; Ikegami, T.; Yoshizumi, T.; Yamanaka, T.; et al. Preoperative neutrophil-to-lymphocyte ratio is a predictor of survival after hepatectomy for hepatocellular carcinoma: A retrospective analysis. Ann. Surg. 2013, 258, 301–305. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.A.; Ghaneh, P.; Sutton, R.; Raraty, M.; Campbell, F.; Neoptolemos, J.P. Prognosis of resected ampullary adenocarcinoma by preoperative serum CA19-9 levels and platelet-lymphocyte ratio. J. Gastrointest. Surg. 2008, 12, 1422–1428. [Google Scholar] [CrossRef]
- Li, J.; Jiang, R.; Liu, W.S.; Liu, Q.; Xu, M.; Feng, Q.S.; Chen, L.Z.; Bei, J.X.; Chen, M.Y.; Zeng, Y.X. A large cohort study reveals the association of elevated peripheral blood lymphocyte-to-monocyte ratio with favorable prognosis in nasopharyngeal carcinoma. PLoS ONE 2013, 8, e83069. [Google Scholar] [CrossRef] [Green Version]
- Pinato, D.J.; North, B.V.; Sharma, R. A novel, externally validated inflammation-based prognostic algorithm in hepatocellular carcinoma: The prognostic nutritional index (PNI). Br. J. Cancer 2012, 106, 1439–1445. [Google Scholar] [CrossRef] [PubMed]
- Pedrazzani, C.; Tripepi, M.; Turri, G.; Fernandes, E.; Scotton, G.; Conci, S.; Campagnaro, T.; Ruzzenente, A.; Guglielmi, A. Prognostic value of red cell distribution width (RDW) in colorectal cancer. Results from a single-center cohort on 591 patients. Sci. Rep. 2020, 10, 1072. [Google Scholar] [CrossRef]
- Lin, J.; Fang, T.; Zhu, M.; Xu, X.; Zhang, J.; Zheng, S.; Jing, C.; Zhang, M.; Liu, B.; Zhang, B. Comparative performance of inflammation-based prognostic scores in patients operated for intrahepatic cholangiocarcinoma. Cancer Manag. Res. 2019, 11, 9107–9119. [Google Scholar] [CrossRef] [Green Version]
- Noguchi, D.; Kuriyama, N.; Nakagawa, Y.; Maeda, K.; Shinkai, T.; Gyoten, K.; Hayasaki, A.; Fujii, T.; Iizawa, Y.; Tanemura, A.; et al. The prognostic impact of lymphocyte-to-C-reactive protein score in patients undergoing surgical resection for intrahepatic cholangiocarcinoma: A comparative study of major representative inflammatory/immunonutritional markers. PLoS ONE 2021, 16, e0245946. [Google Scholar] [CrossRef]
- American Joint Committee on Cancer (AJCC). Cancer Staging Manual, 8th ed.; Springer: Berlin, Germany, 2018. [Google Scholar]
- Wehbe, H.; Henson, R.; Meng, F.; Mize-Berge, J.; Patel, T. Interleukin-6 contributes to growth in cholangiocarcinoma cells by aberrant promoter methylation and gene expression. Cancer Res. 2006, 66, 10517–10524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Q.; Jiang, L.; Wang, X.; Wang, M.; She, F.; Chen, Y. Tumor necrosis factor-α promotes the lymphangiogenesis of gallbladder carcinoma through nuclear factor-κB-mediated upregulation of vascular endothelial growth factor-C. Cancer Sci. 2014, 105, 1261–1271. [Google Scholar] [CrossRef] [Green Version]
- Canna, K.; McArdle, P.A.; McMillan, D.C.; McNicol, A.M.; Smith, G.W.; McKee, R.F.; McArdle, C.S. The relationship between tumour T-lymphocyte infiltration, the systemic inflammatory response and survival in patients undergoing curative resection for colorectal cancer. Br. J. Cancer 2005, 92, 651–654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrie, H.T.; Klassen, L.W.; Kay, H.D. Inhibition of human cytotoxic T lymphocyte activity in vitro by autologous peripheral blood granulocytes. J. Immunol. 1985, 134, 230–234. [Google Scholar]
- Zhou, S.L.; Dai, Z.; Zhou, Z.J.; Chen, Q.; Wang, Z.; Xiao, Y.S.; Hu, Z.Q.; Huang, X.Y.; Yang, G.H.; Shi, Y.H.; et al. CXCL5 contributes to tumor metastasis and recurrence of intrahepatic cholangiocarcinoma by recruiting infiltrative intratumoral neutrophils. Carcinogenesis 2014, 35, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, R.; Kimura, K.; Eguchi, S.; Tauchi, J.; Shibutani, M.; Shinkawa, H.; Ohira, G.O.; Yamazoe, S.; Tanaka, S.; Amano, R.; et al. Preoperative Neutrophil-to-lymphocyte Ratio Predicts Tumor-infiltrating CD8+T Cells in Biliary Tract Cancer. Anticancer Res. 2020, 40, 2881–2887. [Google Scholar] [CrossRef] [PubMed]
- Coppinger, J.A.; Cagney, G.; Toomey, S.; Kislinger, T.; Belton, O.; McRedmond, J.P.; Cahill, D.J.; Emili, A.; Fitzgerald, D.J.; Maguire, P.B. Characterization of the proteins released from activated platelets leads to localization of novel platelet proteins in human atherosclerotic lesions. Blood 2004, 103, 2096–2104. [Google Scholar] [CrossRef] [Green Version]
- Jayarajan, S.; Daly, J.M. The relationships of nutrients, routes of delivery, and immunocompetence. Surg. Clin. N. Am. 2011, 91, 737–753. [Google Scholar] [CrossRef]
- Schwegler, I.; von Holzen, A.; Gutzwiller, J.P.; Schlumpf, R.; Mühlebach, S.; Stanga, Z. Nutritional risk is a clinical predictor of postoperative mortality and morbidity in surgery for colorectal cancer. Br. J. Surg. 2010, 97, 92–97. [Google Scholar] [CrossRef]
- Kanda, M.; Fujii, T.; Kodera, Y.; Nagai, S.; Takeda, S.; Nakao, A. Nutritional predictors of postoperative outcome in pancreatic cancer. Br. J. Surg. 2011, 98, 268–274. [Google Scholar] [CrossRef]
- Zhang, W.; Ye, B.; Liang, W.; Ren, Y. Preoperative prognostic nutritional index is a powerful predictor of prognosis in patients with stage III ovarian cancer. Sci. Rep. 2017, 7, 9548. [Google Scholar] [CrossRef] [Green Version]
- Cui, P.; Pang, Q.; Wang, Y.; Qian, Z.; Hu, X.; Wang, W.; Li, Z.; Zhou, L.; Man, Z.; Yang, S.; et al. Nutritional prognostic scores in patients with hilar cholangiocarcinoma treated by percutaneous transhepatic biliary stenting combined with 125I seed intracavitary irradiation: A retrospective observational study. Medicine 2018, 97, e11000. [Google Scholar] [CrossRef]
- Okuno, M.; Ebata, T.; Yokoyama, Y.; Igami, T.; Sugawara, G.; Mizuno, T.; Yamaguchi, J.; Nagino, M. Evaluation of inflammation-based prognostic scores in patients undergoing hepatobiliary resection for perihilar cholangiocarcinoma. J. Gastroenterol. 2016, 51, 153–161. [Google Scholar] [CrossRef]
- Kitano, Y.; Yamashita, Y.I.; Yamamura, K.; Arima, K.; Kaida, T.; Miyata, T.; Nakagawa, S.; Mima, K.; Imai, K.; Hashimoto, D.; et al. Effects of Preoperative Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios on Survival in Patients with Extrahepatic Cholangiocarcinoma. Anticancer Res. 2017, 37, 3229–3237. [Google Scholar] [CrossRef]
- Buettner, S.; Spolverato, G.; Kimbrough, C.W.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; Gamblin, T.C.; Maithel, S.K.; Pulitano, C.; et al. The impact of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio among patients with intrahepatic cholangiocarcinoma. Surgery 2018, 164, 411–418. [Google Scholar] [CrossRef]
- Subimerb, C.; Pinlaor, S.; Lulitanond, V.; Khuntikeo, N.; Okada, S.; McGrath, M.S.; Wongkham, S. Circulating CD14(+) CD16(+) monocyte levels predict tissue invasive character of cholangiocarcinoma. Clin. Exp. Immunol. 2010, 161, 471–479. [Google Scholar] [CrossRef]
- Leyva-Illades, D.; McMillin, M.; Quinn, M.; Demorrow, S. Cholangiocarcinoma pathogenesis: Role of the tumor microenvironment. Transl. Gastrointest. Cancer 2012, 1, 71–80. [Google Scholar]
- Qian, B.Z.; Pollard, J.W. Macrophage diversity enhances tumor progression and metastasis. Cell 2010, 141, 39–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, D.; Lis, C.G. Pretreatment serum albumin as a predictor of cancer survival: A systematic review of the epidemiological literature. Nutr. J. 2010, 9, 69. [Google Scholar] [CrossRef] [Green Version]
- Klek, S.; Kulig, J.; Sierzega, M.; Szybinski, P.; Szczepanek, K.; Kubisz, A.; Kowalczyk, T.; Gach, T.; Pach, R.; Szczepanik, A.M. The impact of immunostimulating nutrition on infectious complications after upper gastrointestinal surgery: A prospective, randomized, clinical trial. Ann. Surg. 2008, 248, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Lobo, D.N.; Williams, R.N.; Welch, N.T.; Aloysius, M.M.; Nunes, Q.M.; Padmanabhan, J.; Crowe, J.R.; Iftikhar, S.Y.; Parsons, S.L.; Neal, K.R.; et al. Early postoperative jejunostomy feeding with an immune modulating diet in patients undergoing resectional surgery for upper gastrointestinal cancer: A prospective, randomized, controlled, double-blind study. Clin. Nutr. 2006, 25, 716–726. [Google Scholar] [CrossRef] [PubMed]
- Burden, S.; Todd, C.; Hill, J.; Lal, S. Pre-operative nutrition support in patients undergoing gastrointestinal surgery. Cochrane Database Syst. Rev. 2012, 11, CD008879. [Google Scholar] [CrossRef]
- Hughes, M.J.; Hackney, R.J.; Lamb, P.J.; Wigmore, S.J.; Christopher Deans, D.A.; Skipworth, R.J.E. Prehabilitation Before Major Abdominal Surgery: A Systematic Review and Meta-analysis. World J. Surg. 2019, 43, 1661–1668. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Patients n 282 | |
|---|---|---|
| Age, years, median (IQR) | 69.5 (61.9–75.0) | |
| Gender, male, n (%) | 167 (59.2) | |
| CA 19.9, U/mL, median (IQR) | 209.0 (33.3–1418.3) | |
| Type of BTC, n (%) | ICC | 129 (45.7) 94 (33.3) 22 (7.8) 37 (13.1) |
| PCC | ||
| DCC | ||
| GBC | ||
| Jaundice, n (%) | 127 (45.0) | |
| Preoperative Biliary Drainage (PBD), n (%) | 113 (40.1) | |
| Preoperative Chemotherapy, n (%) | 12 (4.3) | |
| Portal Vein Embolization (PVE), n (%) | 9 (3.2) | |
| Tumor size, mm, median (IQR) | 50 (30–60) | |
| Type of Surgery, n (%) | Atypical Liver Resection | 5 (1.8) |
| Segmentectomy | 13 (4.6) | |
| Bisegmentectomy | 60 (21.3) | |
| Left Hepatectomy | 79 (28.0) | |
| Right Hepatectomy | 53 (18.8) | |
| Mesohepatectomy | 7 (2.5) | |
| Left Trisectionectomy | 10 (3.5) | |
| Right Trisectionectomy | 7 (2.5) | |
| Other Major Hepatectomy | 7 (2.5) | |
| Pancreaticoduodenectomy | 23 (8.2) | |
| Common Bile Duct Resection | 14 (5.0) | |
| Cholecystectomy | 1 (0.3) | |
| Hepatoduodenectomy | 3 (1.1) | |
| Extent of Hepatectomy, n (%) | Minor | 80 (28.4) |
| Major | 164 (58.2) | |
| n/a | 38 (13.4) | |
| Biliary Resection, n (%) | 168 (59.6) | |
| Vascular resection, n (%) | 28 (9.9) | |
| AJCC 8th Ed. T Stage, n (%) | T1-2 | 129 (45.7) |
| T3-4 | 153 (54.3) | |
| AJCC 8th Ed. N Stage, n (%) | N0 | 153 (54.3) |
| N1-2 | 129 (45.7) | |
| Histologic Grading | G1-2 | 196 (69.5) |
| G3-4 | 73 (25.9) | |
| n/a | 13 (4.6) | |
| Macrovascular invasion, n (%) | 74 (26.2) | |
| Microvascular invasion, n (%) | 199 (70.6) | |
| Radicality of Surgery, n (%) | R0 | 193 (68.4) |
| R1 | 89 (31.6) | |
| Severe Morbidity (Clavien–Dindo ≥ 3), n (%) | 62 (22.0) | |
| Postoperative mortality, n (%) | 5 (1.8) | |
| Hospital stay, days, median (IQR) | 12 (7–19) | |
| Postoperative chemotherapy | 181 (64.2) | |
| Inflammatory or Immune-Nutritional Marker | Score | Patients n 282 n (%) |
|---|---|---|
| Glasgow Prognostic Score (GPS) | ||
| CRP ≤ 10 mg/L and albumin ≥ 35 g/L | 0 | 192 (68.1) |
| CRP ≤ 10 mg/L and albumin < 35 g/L | 1 | 22 (7.8) 41 (14.5) |
| CRP > 10 mg/L and albumin ≥ 35 g/L | 1 | |
| CRP > 10 mg/L and albumin < 35 g/L | 2 | 27 (9.6) |
| Modified Glasgow Prognostic Score (mGPS) | ||
| CRP ≤ 10 mg/L and albumin ≥ 35 g/L | 0 | 192 (68.1) 22 (7.8) |
| CRP ≤ 10 mg/L and albumin < 35 g/L | 0 | |
| CRP > 10 mg/L and albumin ≥ 35 g/L | 1 | 41 (14.5) |
| CRP > 10 mg/L and albumin < 35 g/L | 2 | 27 (9.6) |
| Prognostic Index (PI) | ||
| CRP ≤ 10 mg/L and WBC ≤ 11 × 109/L | 0 | 200 (70.9) |
| CRP ≤ 10 mg/L and WBC > 11 × 109/L | 1 | 50 (17.7) |
| CRP > 10 mg/L and WBC ≤ 11 × 109/L | 1 | 8 (2.8) |
| CRP > 10 mg/L and WBC > 11 × 109/L | 2 | 24 (8.5) |
| Neutrophil to lymphocyte ratio (NLR), median (IQR) | 3.09 (2.04–4.05) | |
| NLR < 3.13 * | 0 | 146 (51.8) |
| NLR ≥ 3.13 * | 1 | 136 (48.2) |
| Platelet to lymphocyte ratio (PLR), median (IQR) | 160.4 (117.3–230.3) | |
| PLR < 178.2 * | 0 | 174 (61.7) |
| PLR ≥ 178.2 * | 1 | 108 (38.3) |
| Lymphocyte to monocyte ratio (LMR), median (IQR) | 3.34 (2.39–4.62) | |
| LMR < 3.47 * | 1 | 156 (55.3) |
| LMR ≥ 3.47 * | 0 | 126 (44.7) |
| Prognostic Nutritional Index (PNI), median (IQR) | 49.4 (44.3–53.6) | |
| Albumin (g/L) + 5 × total lymphocyte count < 48.6 * | 1 | 128 (45.4) |
| Albumin (g/l) + 5 × total lymphocyte count ≥ 48.6 * | 0 | 154 (54.6) |
| Prognostic Marker | 5-Year OS (%) | HR | 95% C.I. | p Values | |
|---|---|---|---|---|---|
| GPS | 0 | 40.7 | 1.628 | 1.217–2.153 | <0.001 |
| 1–2 | 24.7 | ||||
| mGPS | 0 | 39.2 | 1.537 | 1.198–2.019 | 0.004 |
| 1–2 | 25.1 | ||||
| PI | 0 | 40.3 | 1.559 | 1.235–2.105 | 0.001 |
| 1–2 | 25.3 | ||||
| NLR | <3.13 | 37.9 | 1.274 | 0.906–1.793 | 0.164 |
| ≥3.13 | 33.1 | ||||
| PLR | <178.2 | 35.4 | 1.366 | 0.967–1.928 | 0.077 |
| ≥178.2 | 35.8 | ||||
| LMR | ≥3.47 | 39.6 | 1.656 | 1.167–2.351 | 0.005 |
| <3.47 | 33.2 | ||||
| PNI | ≥48.6 | 36.5 | 1.450 | 1.030–2.041 | 0.033 |
| <48.6 | 35.9 | ||||
| Prognostic Marker | Overall Survival AUC * | Sensitivity | Specificity | Youden Index | AIC § | Max K–S # |
|---|---|---|---|---|---|---|
| 12 months | ||||||
| GPS | 0.706 | 0.714 | 0.722 | 0.436 | 104.650 | 0.436 |
| mGPS | 0.642 | 0.500 | 0.789 | 0.289 | 99.128 | 0.289 |
| PI | 0.651 | 0.571 | 0.738 | 0.309 | 98.870 | 0.310 |
| NLR | 0.558 | 0.536 | 0.527 | 0.063 | 101.090 | 0.159 |
| PLR | 0.603 | 0.536 | 0.629 | 0.165 | 99.846 | 0.164 |
| LMR | 0.590 | 0.714 | 0.477 | 0.191 | 99.310 | 0.191 |
| PNI | 0.664 | 0.750 | 0.582 | 0.332 | 100.732 | 0.332 |
| 24 months | ||||||
| GPS | 0.604 | 0.471 | 0.742 | 0.213 | 129.729 | 0.213 |
| mGPS | 0.555 | 0.314 | 0.794 | 0.108 | 128.051 | 0.108 |
| PI | 0.561 | 0.386 | 0.742 | 0.128 | 127.751 | 0.128 |
| NLR | 0.577 | 0.571 | 0.555 | 0.126 | 129.477 | 0.126 |
| PLR | 0.603 | 0.600 | 0.600 | 0.200 | 130.853 | 0.193 |
| LMR | 0.623 | 0.671 | 0.548 | 0.219 | 127.393 | 0.235 |
| PNI | 0.608 | 0.629 | 0.606 | 0.235 | 130.117 | 0.220 |
| 36 months | ||||||
| GPS | 0.602 | 0.439 | 0.776 | 0.215 | 131.604 | 0.214 |
| mGPS | 0.555 | 0.306 | 0.806 | 0.112 | 127.562 | 0.112 |
| PI | 0.559 | 0.378 | 0.745 | 0.123 | 127.022 | 0.122 |
| NLR | 0.576 | 0.551 | 0.541 | 0.092 | 129.026 | 0.092 |
| PLR | 0.563 | 0.480 | 0.643 | 0.123 | 128.589 | 0.122 |
| LMR | 0.652 | 0.633 | 0.633 | 0.266 | 126.807 | 0.265 |
| PNI | 0.611 | 0.643 | 0.571 | 0.214 | 128.579 | 0.184 |
| Characteristics | Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|---|
| 5-Years OS (%) | Median OS (Months) | p Values | HR | 95% C.I. | p Values | ||
| Age, years | <70 | 41.9 | 49.4 | 0.081 | |||
| ≥70 | 27.4 | 38.7 | |||||
| Gender | M | 30.3 | 43.9 | 0.120 | |||
| F | 43.3 | 51.3 | |||||
| Type of BTC | ICC | 42.7 | 50.1 | <0.001 | ref | 0.002 | |
| PCC | 31.8 | 41.8 | 1.512 | 1.016–2.295 | 0.048 | ||
| DCC | 37.2 | 31.2 | 0.935 | 0.461–1.895 | 0.935 | ||
| GBC | 20.7 | 18.6 | 2.698 | 1.580–4.606 | <0.001 | ||
| Preoperative ChT | No | 35.5 | 43.1 | 0.793 | |||
| Yes | 38.1 | 46.5 | |||||
| AJCC 8th T Stage | T1–2 | 48.1 | 55.7 | <0.001 | 1.515 | 1.076–2.352 | 0.014 |
| T3–4 | 23.8 | 30.4 | |||||
| AJCC 8th N Stage | N0 | 53.4 | 64.9 | <0.001 | 2.431 | 1.613–3.664 | <0.001 |
| N1–N2 | 12.8 | 26.3 | |||||
| Histologic grading | G1–2 | 36.9 | 48.5 | 0.002 | 1.494 | 1.008–2.213 | 0.045 |
| G3–4 | 28.5 | 26.9 | |||||
| Radicality | R0 | 38.2 | 48.8 | 0.006 | 1.108 | 0.746–1.647 | 0.611 |
| R1 | 32.1 | 32.8 | |||||
| Macrovascular invasion | No | 39.0 | 48.8 | <0.001 | 1.335 | 0.894–1.991 | 0.157 |
| Yes | 27.4 | 26.6 | |||||
| Postoperative ChT | No | 35.0 | 43.1 | 0.654 | |||
| Yes | 37.3 | 48.1 | |||||
| LMR | ≥3.47 | 39.6 | 48.8 | 0.004 | 1.378 | 1.046–2.007 | 0.025 |
| <3.47 | 33.2 | 32.8 | |||||
| Prognostic Marker | Univariate Analysis | Logistic Regression | ||||
|---|---|---|---|---|---|---|
| n (%) | p Values | OR | 95% C.I. | p Values | ||
| GPS | 0 | 27/192 (14.1) | <0.001 | 3.889 | 2.161–6.998 | <0.001 |
| 1–2 | 35/90 (38.9) | |||||
| mGPS | 0 | 39/214 (18.2) | 0.007 | 2.293 | 1.245–4.223 | 0.008 |
| 1–2 | 23/68 (33.8) | |||||
| PI | 0 | 36/200 (18.0) | 0.010 | 2.115 | 1.174–3.810 | 0.013 |
| 1–2 | 26/82 (31.7) | |||||
| NLR | <3.13 | 22/146 (15.1) | 0.003 | 2.348 | 1.309–4.213 | 0.004 |
| ≥3.13 | 40/136 (29.4) | |||||
| PLR | <178.2 | 28/174 (16.1) | 0.002 | 2.396 | 1.351–4.249 | 0.003 |
| ≥178.2 | 34/108 (31.5) | |||||
| LMR | ≥3.47 | 22/126 (17.5) | 0.066 | 1.630 | 0.909–2.922 | 0.101 |
| <3.47 | 40/156 (25.6) | |||||
| PNI | ≥48.6 | 16/154 (10.4) | <0.001 | 4.838 | 2.574–9.095 | <0.001 |
| <48.6 | 46/128 (35.9) | |||||
| Prognostic Marker/ | Univariate Analysis | Multivariable Analysis | ||||
|---|---|---|---|---|---|---|
| Characteristics | n (%) | p Values | OR | 95% C.I. | p Values | |
| Age, years | <70 | 27/152 (17.8) | 0.044 | 1.785 | 0.927–3.438 | 0.083 |
| ≥70 | 35/130 (26.9) | |||||
| Gender | M | 31/115 (27.0) | 0.064 | |||
| F | 31/167 (18.6) | |||||
| Type of BTC | ICC | 23/129 (17.8) | 0.089 | |||
| PCC | 29/94 (30.9) | |||||
| DCC | 4/22 (18.2) | |||||
| GBC | 6/37 (16.2) | |||||
| PBD | No | 24/169 (14.2) | <0.001 | 2.504 | 1.090–5.753 | 0.031 |
| Yes | 38/113 (33.6) | |||||
| Major | No | 9/80 (11.3) | 0.001 | 1.980 | 0.762–5.140 | 0.161 |
| Hepatectomy | Yes | 47/164 (28.7) | ||||
| Biliary | No | 14/114 (12.3) | <0.001 | 0.859 | 0.313–2.537 | 0.768 |
| Resection | Yes | 48/168 (28.6) | ||||
| Vascular | No | 55/254 (21.7) | 0.421 | |||
| Resection | Yes | 7/28 (25.0) | ||||
| PNI | ≥48.6 | 16/154 (10.4) | <0.001 | 3.109 | 1.475–6.554 | 0.003 |
| <48.6 | 46/128 (35.9) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Conci, S.; Campagnaro, T.; Danese, E.; Lombardo, E.; Isa, G.; Vitali, A.; Marchitelli, I.; Bagante, F.; Pedrazzani, C.; De Bellis, M.; et al. Role of Inflammatory and Immune-Nutritional Prognostic Markers in Patients Undergoing Surgical Resection for Biliary Tract Cancers. Cancers 2021, 13, 3594. https://doi.org/10.3390/cancers13143594
Conci S, Campagnaro T, Danese E, Lombardo E, Isa G, Vitali A, Marchitelli I, Bagante F, Pedrazzani C, De Bellis M, et al. Role of Inflammatory and Immune-Nutritional Prognostic Markers in Patients Undergoing Surgical Resection for Biliary Tract Cancers. Cancers. 2021; 13(14):3594. https://doi.org/10.3390/cancers13143594
Chicago/Turabian StyleConci, Simone, Tommaso Campagnaro, Elisa Danese, Ezio Lombardo, Giulia Isa, Alessandro Vitali, Ivan Marchitelli, Fabio Bagante, Corrado Pedrazzani, Mario De Bellis, and et al. 2021. "Role of Inflammatory and Immune-Nutritional Prognostic Markers in Patients Undergoing Surgical Resection for Biliary Tract Cancers" Cancers 13, no. 14: 3594. https://doi.org/10.3390/cancers13143594
APA StyleConci, S., Campagnaro, T., Danese, E., Lombardo, E., Isa, G., Vitali, A., Marchitelli, I., Bagante, F., Pedrazzani, C., De Bellis, M., Ciangherotti, A., Guglielmi, A., Lippi, G., & Ruzzenente, A. (2021). Role of Inflammatory and Immune-Nutritional Prognostic Markers in Patients Undergoing Surgical Resection for Biliary Tract Cancers. Cancers, 13(14), 3594. https://doi.org/10.3390/cancers13143594