
A Prospective Real-World Multi-Center Study to Evaluate Progression-Free and Overall Survival of Radiotherapy with Cetuximab and Platinum-Based Chemotherapy with Cetuximab in Locally Recurrent Head and Neck Cancer

 ,
, 
 , , ,
, , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Study Design and Treatments
2.3. Endpoints and Assessments
2.4. Study Oversight
2.5. Statistical Analysis
3. Results
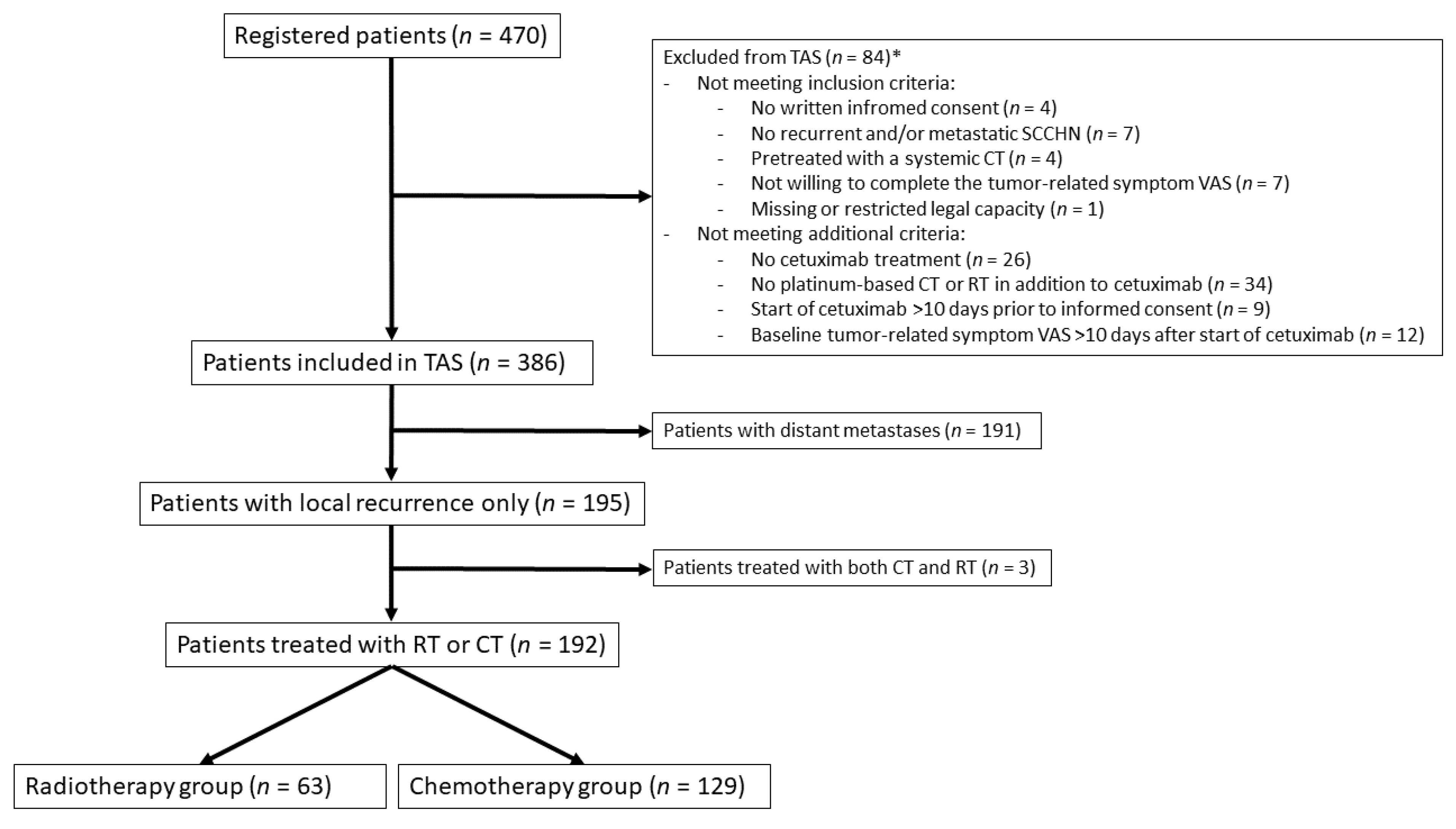
3.1. Patients
3.2. Treatment
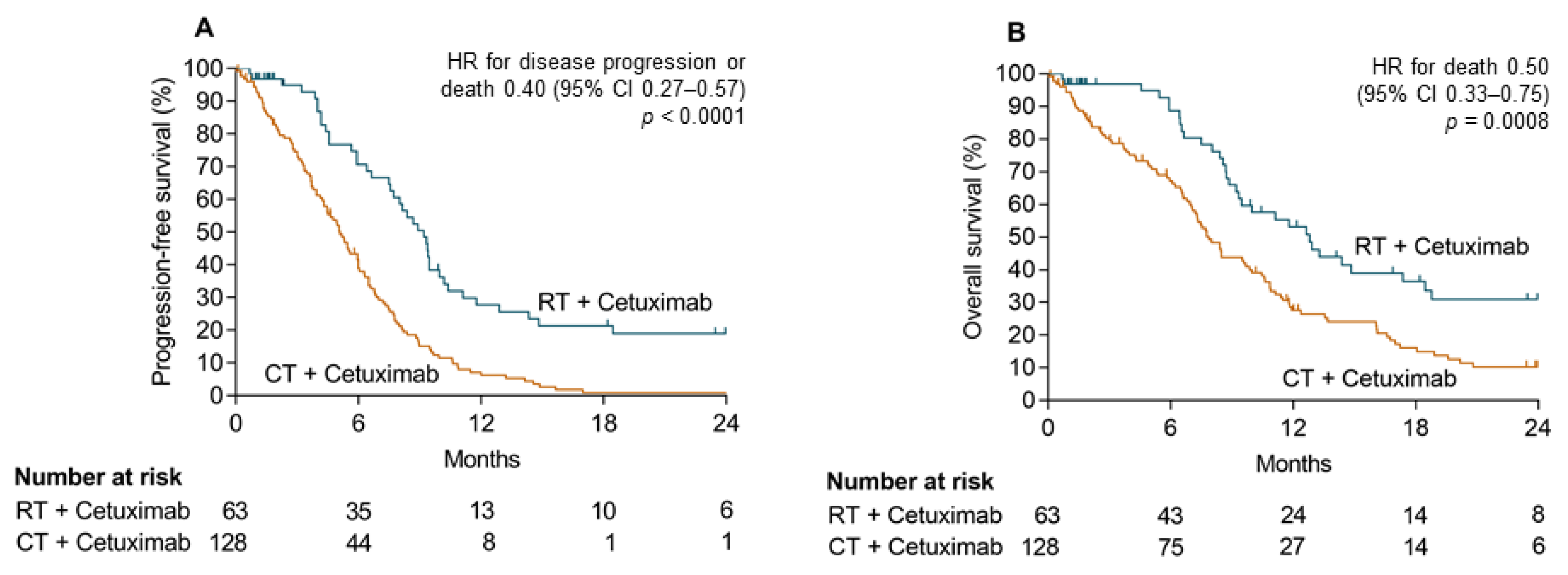
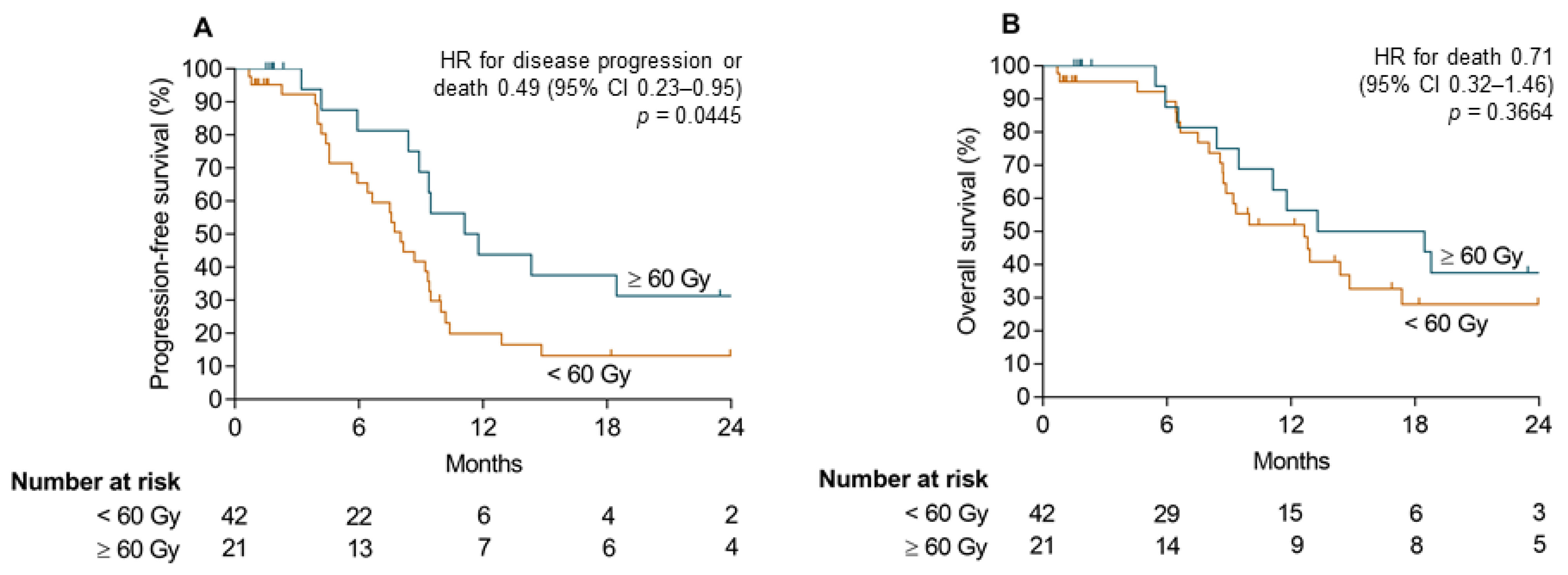
3.3. Efficacy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cooper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Campbell, B.H.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef] [Green Version]
- Ang, K.K.; Zhang, Q.; Rosenthal, D.I.; Nguyen-Tan, P.F.; Sherman, E.J.; Weber, R.S.; Galvin, J.M.; Bonner, J.A.; Harris, J.; El-Naggar, A.K.; et al. Randomized phase III trial of concurrent accelerated radiation plus cisplatin with or without cetuximab for stage III to IV head and neck carcinoma: RTOG 0522. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2014, 32, 2940–2950. [Google Scholar] [CrossRef]
- Fietkau, R.; Hecht, M.; Hofner, B.; Lubgan, D.; Iro, H.; Gefeller, O.; Rodel, C.; Hautmann, M.G.; Kolbl, O.; Salay, A.; et al. Randomized phase-III-trial of concurrent chemoradiation for locally advanced head and neck cancer comparing dose reduced radiotherapy with paclitaxel/cisplatin to standard radiotherapy with fluorouracil/cisplatin: The PacCis-trial. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2020, 144, 209–217. [Google Scholar] [CrossRef]
- Chuang, S.C.; Scelo, G.; Tonita, J.M.; Tamaro, S.; Jonasson, J.G.; Kliewer, E.V.; Hemminki, K.; Weiderpass, E.; Pukkala, E.; Tracey, E.; et al. Risk of second primary cancer among patients with head and neck cancers: A pooled analysis of 13 cancer registries. Int. J. Cancer 2008, 123, 2390–2396. [Google Scholar] [CrossRef] [PubMed]
- Vermorken, J.B.; Mesia, R.; Rivera, F.; Remenar, E.; Kawecki, A.; Rottey, S.; Erfan, J.; Zabolotnyy, D.; Kienzer, H.R.; Cupissol, D.; et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N. Engl. J. Med. 2008, 359, 1116–1127. [Google Scholar] [CrossRef] [Green Version]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulieres, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Baste, N.; Neupane, P.; Bratland, A.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Harrington, K.J.; Cohen, E.E.W.; Soulières, D.; Dinis, J.; Licitra, L.; Ahn, M.-J.; Soria, A.; Machiels, J.-P.H.; Mach, N.; Mehra, R.; et al. Pembrolizumab (pembro) for recurrent head and neck squamous cell carcinoma (HNSCC): Post hoc analyses of phase 3 KEYNOTE-040 prior radiation treatment (RT) and disease state. J. Clin. Oncol. 2019, 37, 6026. [Google Scholar] [CrossRef]
- Chang, J.H.; Wu, C.C.; Yuan, K.S.; Wu, A.T.H.; Wu, S.Y. Locoregionally recurrent head and neck squamous cell carcinoma: Incidence, survival, prognostic factors, and treatment outcomes. Oncotarget 2017, 8, 55600–55612. [Google Scholar] [CrossRef] [Green Version]
- Salama, J.K.; Vokes, E.E.; Chmura, S.J.; Milano, M.T.; Kao, J.; Stenson, K.M.; Witt, M.E.; Haraf, D.J. Long-term outcome of concurrent chemotherapy and reirradiation for recurrent and second primary head-and-neck squamous cell carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Hecht, M.; Hahn, D.; Wolber, P.; Hautmann, M.G.; Reichert, D.; Weniger, S.; Belka, C.; Bergmann, T.; Gohler, T.; Welslau, M.; et al. Treatment response lowers tumor symptom burden in recurrent and/or metastatic head and neck cancer. BMC Cancer 2020, 20, 933. [Google Scholar] [CrossRef]
- Modesto, A.; Galissier, T.; Lusque, A.; Delord, J.P.; Uro-Coste, E.; Sarini, J.; Mouchet, F.; Lopez, R.; Laprie, A.; Graff, P.; et al. Definitive radiochemotherapy or initial surgery for oropharyngeal cancer: To what extent can p16 expression be used in the decision process? Strahlenther. Onkol. 2019, 195, 496–503. [Google Scholar] [CrossRef]
- Balermpas, P.; Keller, C.; Hambek, M.; Wagenblast, J.; Seitz, O.; Rodel, C.; Weiss, C. Reirradiation with cetuximab in locoregional recurrent and inoperable squamous cell carcinoma of the head and neck: Feasibility and first efficacy results. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, e377–e383. [Google Scholar] [CrossRef]
- Lartigau, E.F.; Tresch, E.; Thariat, J.; Graff, P.; Coche-Dequeant, B.; Benezery, K.; Schiappacasse, L.; Degardin, M.; Bondiau, P.Y.; Peiffert, D.; et al. Multi institutional phase II study of concomitant stereotactic reirradiation and cetuximab for recurrent head and neck cancer. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2013, 109, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Dornoff, N.; Weiss, C.; Rodel, F.; Wagenblast, J.; Ghanaati, S.; Atefeh, N.; Rodel, C.; Balermpas, P. Re-irradiation with cetuximab or cisplatin-based chemotherapy for recurrent squamous cell carcinoma of the head and neck. Strahlenther. Onkol. 2015, 191, 656–664. [Google Scholar] [CrossRef]
- Weykamp, F.; Seidensaal, K.; Rieken, S.; Green, K.; Mende, S.; Zaoui, K.; Freier, K.; Adeberg, S.; Debus, J.; Welte, S.E. Age-dependent hemato- and nephrotoxicity in patients with head and neck cancer receiving chemoradiotherapy with weekly cisplatin. Strahlenther. Onkol. 2020, 196, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Caudell, J.J.; Ward, M.C.; Riaz, N.; Zakem, S.J.; Awan, M.J.; Dunlap, N.E.; Isrow, D.; Hassanzadeh, C.; Vargo, J.A.; Heron, D.E.; et al. Volume, Dose, and Fractionation Considerations for IMRT-based Reirradiation in Head and Neck Cancer: A Multi-institution Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 606–617. [Google Scholar] [CrossRef]
- Gillison, M.L.; Trotti, A.M.; Harris, J.; Eisbruch, A.; Harari, P.M.; Adelstein, D.J.; Jordan, R.C.K.; Zhao, W.; Sturgis, E.M.; Burtness, B.; et al. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): A randomised, multicentre, non-inferiority trial. Lancet 2019, 393, 40–50. [Google Scholar] [CrossRef]
- Guigay, J.; Fayette, J.; Mesia, R.; Lafond, C.; Saada-Bouzid, E.; Geoffrois, L.; Martin, L.; Cupissol, D.; Capitain, O.; Castanie, H.; et al. TPExtreme randomized trial: TPEx versus Extreme regimen in 1st line recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC). J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2019, 37, 6002. [Google Scholar] [CrossRef]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; Castro, G.D.; Psyrri, A.; Baste Rotllan, N.; Neupane, P.C.; Bratland, A.; et al. KEYNOTE-048: Phase III study of first-line pembrolizumab (P) for recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC). Ann. Oncol. 2018, 29, viii729. [Google Scholar] [CrossRef]
- Rischin, D.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; Castro, G.D.; Psyrri, A.; Baste, N.; Neupane, P.C.; Bratland, A.; et al. Protocol-specified final analysis of the phase 3 KEYNOTE-048 trial of pembrolizumab (pembro) as first-line therapy for recurrent/metastatic head and neck squamous cell carcinoma (R/M HNSCC). J. Clin. Oncol. 2019, 37, 6000. [Google Scholar] [CrossRef]
- Derer, A.; Frey, B.; Fietkau, R.; Gaipl, U.S. Immune-modulating properties of ionizing radiation: Rationale for the treatment of cancer by combination radiotherapy and immune checkpoint inhibitors. Cancer Immunol. Immunother. CII 2015. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Patients’ Characteristics | RT + Cet (n = 63) | CT + Cet (n = 129) | p-Value |
|---|---|---|---|
| Age at Study Inclusion [years], mean ± SD | 66.6 ± 9.3 | 62.2 ± 9.5 | 0.003 |
| Weight [kg], mean ± SD | 66.2 ± 12.6 | 66.3 ± 13.0 | 0.959 |
| Sex, n (%) | 0.938 | ||
| Female | 13 (21) | 26 (20) | |
| Male | 50 (79) | 103 (80) | |
| Location of Primary Tumor *, n (%) | |||
| Oropharynx | 20 (32) | 34 (26) | 0.436 |
| Hypopharynx | 14 (22) | 27 (21) | 0.838 |
| Larynx | 5 (8) | 23 (18) | 0.068 |
| Oral cavity | 21 (33) | 43 (33) | 1.000 |
| Other location | 6 (10) | 12 (9) | 1.000 |
| Stage of Disease at Initial Diagnosis | 0.396 | ||
| I | 4 (6) | 12 (9) | |
| II | 9 (14) | 12 (9) | |
| III | 11 (17) | 15 (12) | |
| IV | 37 (59) | 87 (67) | |
| unknown | 2 (3) | 3 (2) | |
| Prior Therapy, n (%) | |||
| Radiotherapy (with or without concomitant chemotherapy) | 44 (70) | 119 (92) | <0.001 |
| Chemotherapy concomitant to radiotherapy | 28 (44) | 81 (63) | 0.0134 |
| Surgery | 42 (67) | 87 (67) | 0.915 |
| Time Interval since Initial Diagnosis, median (years) | 2.2 | 1.2 | <0.001 |
| Charlson Comorbidity Index at study inclusion, n (%) | 0.089 | ||
| 0 | 25 (40) | 70 (54) | |
| 1 | 12 (19) | 25 (19) | |
| >1 | 26 (41) | 34 (26) | |
| ECOG Performance Status at treatment initiation, n (%) | 0.909 | ||
| 0 | 11 (18) | 20 (17) | |
| 1 | 38 (62) | 74 (62) | |
| ≥2 | 12 (20) | 23 (19) | |
| Alcohol Consumption, n (%) | 0.061 | ||
| Never | 18 (29) | 26 (20) | |
| Several times per month | 18 (29) | 26 (20) | |
| Several times per week or daily | 16 (25) | 31 (24) | |
| Missing | 11 (17) | 46 (36) | |
| Smoking Habits, n (%) | 0.247 | ||
| Never smoked | 20 (32) | 35 (27) | |
| Former smoker | 27 (43) | 45 (35) | |
| Current smoker | 16 (25) | 48 (38) | |
| Pack Years of former/current smoker, mean ± SD | 35.8 ± 24.7 | 37.5 ± 31.7 | 0.775 |
| Treatment | RT + Cet (n = 63) | CT + Cet (n = 129) | p-Value |
|---|---|---|---|
| Radiotherapy | |||
| Conventional fractionation, n (%) | 58 (92) | ||
| Dose per fraction [Gy], mean ± SD | 1.9 ± 0.1 | ||
| Total dose | |||
| <60 Gy, n (%) | 42 (67) | ||
| ≥60 Gy, n (%) | 21 (33) | ||
| Mean ± SD [Gy] | 51.8 ± 15.4 | ||
| Location | |||
| Local relapse | 44 (70) | ||
| Lymph node | 21 (33) | ||
| Duration of radiotherapy [weeks], mean ± SD | 6.6 ± 2.2 | ||
| Radiotherapy completed as planned, n (%) | 54 (86) | ||
| Chemotherapy | |||
| Cisplatin + 5-Flurouracil, n (%) | 52 (40) | ||
| Carboplatin + 5-Flurouracil, n (%) | 37 (29) | ||
| Carboplatin, n (%) | 18 (14) | ||
| Cisplatin, n (%) | 12 (9) | ||
| Carboplatin + Paclitaxel, n (%) | 7 (5) | ||
| Other, n (%) | 3 (2) | ||
| Duration of chemotherapy [weeks], mean ± SD | 12.8 ± 10.6 | ||
| Cetuximab | |||
| Total duration of Cetuximab treatment [weeks], mean ± SD | 8.6 ± 7.7 | 18.9 ± 19.6 | <0.001 |
| Cetuximab maintenance performed, n (%) | 8 (13) | 47 (36) | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hecht, M.; Hahn, D.; Wolber, P.; Hautmann, M.G.; Reichert, D.; Weniger, S.; Belka, C.; Bergmann, T.; Göhler, T.; Welslau, M.; et al. A Prospective Real-World Multi-Center Study to Evaluate Progression-Free and Overall Survival of Radiotherapy with Cetuximab and Platinum-Based Chemotherapy with Cetuximab in Locally Recurrent Head and Neck Cancer. Cancers 2021, 13, 3413. https://doi.org/10.3390/cancers13143413
Hecht M, Hahn D, Wolber P, Hautmann MG, Reichert D, Weniger S, Belka C, Bergmann T, Göhler T, Welslau M, et al. A Prospective Real-World Multi-Center Study to Evaluate Progression-Free and Overall Survival of Radiotherapy with Cetuximab and Platinum-Based Chemotherapy with Cetuximab in Locally Recurrent Head and Neck Cancer. Cancers. 2021; 13(14):3413. https://doi.org/10.3390/cancers13143413
Chicago/Turabian StyleHecht, Markus, Dennis Hahn, Philipp Wolber, Matthias G. Hautmann, Dietmar Reichert, Steffi Weniger, Claus Belka, Tobias Bergmann, Thomas Göhler, Manfred Welslau, and et al. 2021. "A Prospective Real-World Multi-Center Study to Evaluate Progression-Free and Overall Survival of Radiotherapy with Cetuximab and Platinum-Based Chemotherapy with Cetuximab in Locally Recurrent Head and Neck Cancer" Cancers 13, no. 14: 3413. https://doi.org/10.3390/cancers13143413
APA StyleHecht, M., Hahn, D., Wolber, P., Hautmann, M. G., Reichert, D., Weniger, S., Belka, C., Bergmann, T., Göhler, T., Welslau, M., Große-Thie, C., Guntinas-Lichius, O., von der Grün, J., Balermpas, P., Orlowski, K., Messinger, D., Stenzel, K. G., & Fietkau, R. (2021). A Prospective Real-World Multi-Center Study to Evaluate Progression-Free and Overall Survival of Radiotherapy with Cetuximab and Platinum-Based Chemotherapy with Cetuximab in Locally Recurrent Head and Neck Cancer. Cancers, 13(14), 3413. https://doi.org/10.3390/cancers13143413