
Blood Arsenic Levels as a Marker of Breast Cancer Risk among BRCA1 Carriers

 , , , , , , ,
, , , , , , , 
 add
Show full author list
add
Show full author list
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Total Arsenic Determination
2.3. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anastasiadi, Z.; Lianos, G.D.; Ignatiadou, E.; Harissis, H.V.; Mitsis, M. Breast Cancer in Young Women: An Overview. Updates Surg. 2017, 69, 313–317. [Google Scholar] [CrossRef]
- Lubinski, J.; Huzarski, T.; Byrski, T.; Lynch, H.T.; Cybulski, C.; Ghadirian, P.; Stawicka, M.; Foulkes, W.D.; Kilar, E.; Kim-Sing, C.; et al. The Risk of Breast Cancer in Women with a BRCA1 Mutation from North America and Poland. Int. J. Cancer 2012, 131, 229–234. [Google Scholar] [CrossRef]
- Kotsopoulos, J. BRCA Mutations and Breast Cancer Prevention. Cancers 2018, 10, 524. [Google Scholar] [CrossRef] [Green Version]
- Terry, P.; Suzuki, R.; Hu, F.B.; Wolk, A. A Prospective Study of Major Dietary Patterns and the Risk of Breast Cancer. Cancer Epidemiol. Biomark. Prev. 2001, 10, 1281–1285. [Google Scholar]
- Playdon, M.C.; Ziegler, R.G.; Sampson, J.N.; Stolzenberg-Solomon, R.; Thompson, H.J.; Irwin, M.L.; Mayne, S.T.; Hoover, R.N.; Moore, S.C. Nutritional Metabolomics and Breast Cancer Risk in a Prospective Study. Am. J. Clin. Nutr. 2017, 106, 637–649. [Google Scholar] [CrossRef]
- Sieri, S.; Krogh, V.; Ferrari, P.; Berrino, F.; Pala, V.; Thiébaut, A.C.; Tjønneland, A.; Olsen, A.; Overvad, K.; Jakobsen, M.U.; et al. Dietary Fat and Breast Cancer Risk in the European Prospective Investigation into Cancer and Nutrition. Am. J. Clin. Nutr. 2008, 88, 1304–1312. [Google Scholar] [CrossRef]
- Gonzalez, C.A.; Riboli, E. Diet and Cancer Prevention: Contributions from the European Prospective Investigation into Cancer and Nutrition (EPIC) Study. Eur. J. Cancer 2010, 46, 2555–2562. [Google Scholar] [CrossRef]
- Coletta, A.M.; Peterson, S.K.; Gatus, L.A.; Krause, K.J.; Schembre, S.M.; Gilchrist, S.C.; Arun, B.; You, Y.N.; Rodriguez-Bigas, M.A.; Strong, L.L.; et al. Diet, Weight Management, Physical Activity and Ovarian & Breast Cancer Risk in Women with BRCA1/2 Pathogenic Germline Gene Variants: Systematic Review. Hered. Cancer Clin. Pract. 2020, 18, 5. [Google Scholar] [CrossRef] [PubMed]
- Kotsopoulos, J.; Narod, S.A. Brief Report: Towards a Dietary Prevention of Hereditary Breast Cancer. Cancer Causes Control 2005, 16, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Palma-Lara, I.; Martínez-Castillo, M.; Quintana-Pérez, J.C.; Arellano-Mendoza, M.G.; Tamay-Cach, F.; Valenzuela-Limón, O.L.; García-Montalvo, E.A.; Hernández-Zavala, A. Arsenic Exposure: A Public Health Problem Leading to Several Cancers. Regul. Toxicol. Pharmacol. 2020, 110, 104539. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.-K.; Tseng, C.-H.; Huang, Y.-L.; Yang, M.-H.; Chen, C.-J.; Hsueh, Y.-M. Arsenic Methylation Capability and Hypertension Risk in Subjects Living in Arseniasis-Hyperendemic Areas in Southwestern Taiwan. Toxicol. Appl. Pharmacol. 2007, 218, 135–142. [Google Scholar] [CrossRef]
- Li, X.; Li, B.; Xu, Y.; Wang, Y.; Jin, Y.; Itoh, T.; Yoshida, T.; Sun, G. Arsenic Methylation Capacity and Its Correlation with Skin Lesions Induced by Contaminated Drinking Water Consumption in Residents of Chronic Arsenicosis Area. Environ. Toxicol. 2011, 26, 118–123. [Google Scholar] [CrossRef]
- Melak, D.; Ferreccio, C.; Kalman, D.; Parra, R.; Acevedo, J.; Pérez, L.; Cortés, S.; Smith, A.H.; Yuan, Y.; Liaw, J.; et al. Arsenic Methylation and Lung and Bladder Cancer in a Case-Control Study in Northern Chile. Toxicol. Appl. Pharmacol. 2014, 274, 225–231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, R.C.; Hsu, K.-H.; Chen, C.-J.; Froines, J.R. Arsenic Methylation Capacity and Skin Cancer. Cancer Epidemiol. Biomark. Prev. 2000, 9, 1259–1262. [Google Scholar]
- IARC. Arsenic, Metals, Fibres, and Dusts; International Agency for Research on Cancer: Lyon, France, 2012; ISBN 978-92-832-1320-8. [Google Scholar]
- Pullella, K.; Kotsopoulos, J. Arsenic Exposure and Breast Cancer Risk: A Re-Evaluation of the Literature. Nutrients 2020, 12, 3305. [Google Scholar] [CrossRef] [PubMed]
- Mandal, B.K.; Suzuki, K.T. Arsenic Round the World: A Review. Talanta 2002, 58, 201–235. [Google Scholar] [CrossRef]
- Hough, R.L.; Fletcher, T.; Leonardi, G.S.; Goessler, W.; Gnagnarella, P.; Clemens, F.; Gurzau, E.; Koppova, K.; Rudnai, P.; Kumar, R.; et al. Lifetime Exposure to Arsenic in Residential Drinking Water in Central Europe. Int. Arch. Occup. Environ. Health 2010, 83, 471–481. [Google Scholar] [CrossRef] [PubMed]
- Marciniak, W.; Derkacz, R.; Muszyńska, M.; Baszuk, P.; Gronwald, J.; Huzarski, T.; Cybulski, C.; Jakubowska, A.; Falco, M.; Dębniak, T.; et al. Blood Arsenic Levels and the Risk of Familial Breast Cancer in Poland. Int. J. Cancer 2020, 146, 2721–2727. [Google Scholar] [CrossRef] [Green Version]
- Jones, D.R.; Jarrett, J.M.; Tevis, D.S.; Franklin, M.; Mullinix, N.J.; Wallon, K.L.; Derrick Quarles, C.; Caldwell, K.L.; Jones, R.L. Analysis of Whole Human Blood for Pb, Cd, Hg, Se, and Mn by ICP-DRC-MS for Biomonitoring and Acute Exposures. Talanta 2017, 162, 114–122. [Google Scholar] [CrossRef] [Green Version]
- Lynch, H.N.; Greenberg, G.I.; Pollock, M.C.; Lewis, A.S. A Comprehensive Evaluation of Inorganic Arsenic in Food and Considerations for Dietary Intake Analyses. Sci. Total Environ. 2014, 496, 299–313. [Google Scholar] [CrossRef]
- Rasheed, H.; Slack, R.; Kay, P. Human Health Risk Assessment for Arsenic: A Critical Review. Crit. Rev. Environ. Sci. Technol. 2016, 46, 1529–1583. [Google Scholar] [CrossRef]
- Cubadda, F.; Jackson, B.P.; Cottingham, K.L.; Van Horne, Y.O.; Kurzius-Spencer, M. Human Exposure to Dietary Inorganic Arsenic and Other Arsenic Species: State of Knowledge, Gaps and Uncertainties. Sci. Total Environ. 2017, 579, 1228–1239. [Google Scholar] [CrossRef] [Green Version]
- Sattar, A.; Xie, S.; Hafeez, M.A.; Wang, X.; Hussain, H.I.; Iqbal, Z.; Pan, Y.; Iqbal, M.; Shabbir, M.A.; Yuan, Z. Metabolism and Toxicity of Arsenicals in Mammals. Environ. Toxicol. Pharmacol. 2016, 48, 214–224. [Google Scholar] [CrossRef] [PubMed]
- Molin, M.; Ulven, S.M.; Meltzer, H.M.; Alexander, J. Arsenic in the Human Food Chain, Biotransformation and Toxicology—Review Focusing on Seafood Arsenic. J. Trace Elem. Med. Biol. 2015, 31, 249–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garbinski, L.D.; Rosen, B.P.; Chen, J. Pathways of Arsenic Uptake and Efflux. Environ. Int. 2019, 126, 585–597. [Google Scholar] [CrossRef] [PubMed]
- TSENG, C.-H. Arsenic Methylation, Urinary Arsenic Metabolites and Human Diseases: Current Perspective. J. Environ. Sci. Health Part C 2007, 25, 1–22. [Google Scholar] [CrossRef]
- Hirano, S. Biotransformation of Arsenic and Toxicological Implication of Arsenic Metabolites. Arch. Toxicol. 2020, 94, 2587–2601. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.H.; Marshall, G.; Roh, T.; Ferreccio, C.; Liaw, J.; Steinmaus, C. Lung, Bladder, and Kidney Cancer Mortality 40 Years After Arsenic Exposure Reduction. J. Natl. Cancer Inst. 2018, 110, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Sun, H.-J.; Xiang, P.; Luo, J.; Hong, H.; Lin, H.; Li, H.-B.; Ma, L.Q. Mechanisms of Arsenic Disruption on Gonadal, Adrenal and Thyroid Endocrine Systems in Humans: A Review. Environ. Int. 2016, 95, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Wong-Brown, M.W.; Meldrum, C.J.; Carpenter, J.E.; Clarke, C.L.; Narod, S.A.; Jakubowska, A.; Rudnicka, H.; Lubinski, J.; Scott, R.J. Prevalence of BRCA1 and BRCA2 Germline Mutations in Patients with Triple-Negative Breast Cancer. Breast Cancer Res. Treat. 2015, 150, 71–80. [Google Scholar] [CrossRef]
- Liu, R.; Nelson, D.O.; Hurley, S.; Hertz, A.; Reynolds, P. Residential Exposure to Estrogen Disrupting Hazardous Air Pollutants and Breast Cancer Risk: The California Teachers Study. Epidemiology 2015, 26, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Loźna, K.; Biernat, J. The occurrence of arsenc in the environment and food. Rocz. Panstw. Zakl. Hig. 2008, 59, 19–31. [Google Scholar] [PubMed]
- Murcott, S. Arsenic Contamination in the World; IWA Publishing: London, UK, 2012; ISBN 978-1-78040-038-9. [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | n (%) | Mean Arsenic Level µg/L (range) |
|---|---|---|
| Age | ||
| ≤50 | 831 (77) | 1.29 (0.26–70.4) |
| >50 | 253 (23) | 1.41 (0.33–13.7) |
| Contraceptive Usage | ||
| Ever | 478 (44) | 1.34 (0.27–17.46) |
| Never | 606 (56) | 1.30 (0.26–70.04) |
| Hormonal Replacement Therapy Usage | ||
| Ever | 167 (15) | 1.81 (0.26–70.04) |
| Never | 917 (85) | 1.23 (0.26–17.46) |
| Smoking Status | ||
| Yes | 341 (31) | 1.23 (0.26–17.46) |
| No | 743 (69) | 1.36 (0.26–70.04) |
| Oophorectomy | ||
| Yes | 510 (47) | 1.42 (0.26–70.04) |
| No | 574 (53) | 1.23 (0.26–12.97) |
| Dietary Supplements Usage | ||
| Ever | 191 (18) | 1.18 (0.26–9.65) |
| Never | 893 (82) | 1.35 (0.26–70.04) |
| Diabetes | ||
| Yes | 34 (3) | 1.60 (0.40–6.94) |
| No | 1050 (97) | 1.31 (0.26–70.04) |
| Body Mass Index (BMI) | ||
| <18.5 | 67 (6.2) | 1.17 (0,29–7.18) |
| 18.5–24.9 | 649 (60) | 1.32 (0.27–70.04) |
| 25.0–29.9 | 263 (24) | 1.24 (0.26–13.70) |
| ≥30.0 | 105 (9.8) | 1.60 (0.34–12.37) |
| Blood Lead Level | ||
| <11.75 | 537 (49.34) | 1.19 (0.26–12.97) |
| ≥11.75 | 547 (50.66) | 1.45 (0.26–70.04) |
| Blood Cadmium Level | ||
| <0.42 | 528 (49.96) | 1.21 (0.26–12.97) |
| ≥0.42 | 556 (50.04) | 1.43 (0.25–70.04) |
| Cancer Site | n | Mean Blood Arsenic Level µg/L (range) |
|---|---|---|
| Breast | 67 | 1.65 (0.39–17.46) |
| Ovarian | 10 | 1.33 (0.38–2.33) |
| Cervix | 3 | 1.28 (0.60–2.26) |
| Peritoneal | 2 | 0.88 (0.59–1.17) |
| Colon and intestine | 1 | 0.36 |
| Bladder | 1 | 0.63 |
| Kidney | 1 | 1.4 |
| Larynx | 1 | 0.98 |
| Leukemia | 1 | 1.06 |
| Skin | 1 | 1.39 |
| Stomach | 1 | 0.7 |
| Thyroid | 1 | 0.85 |
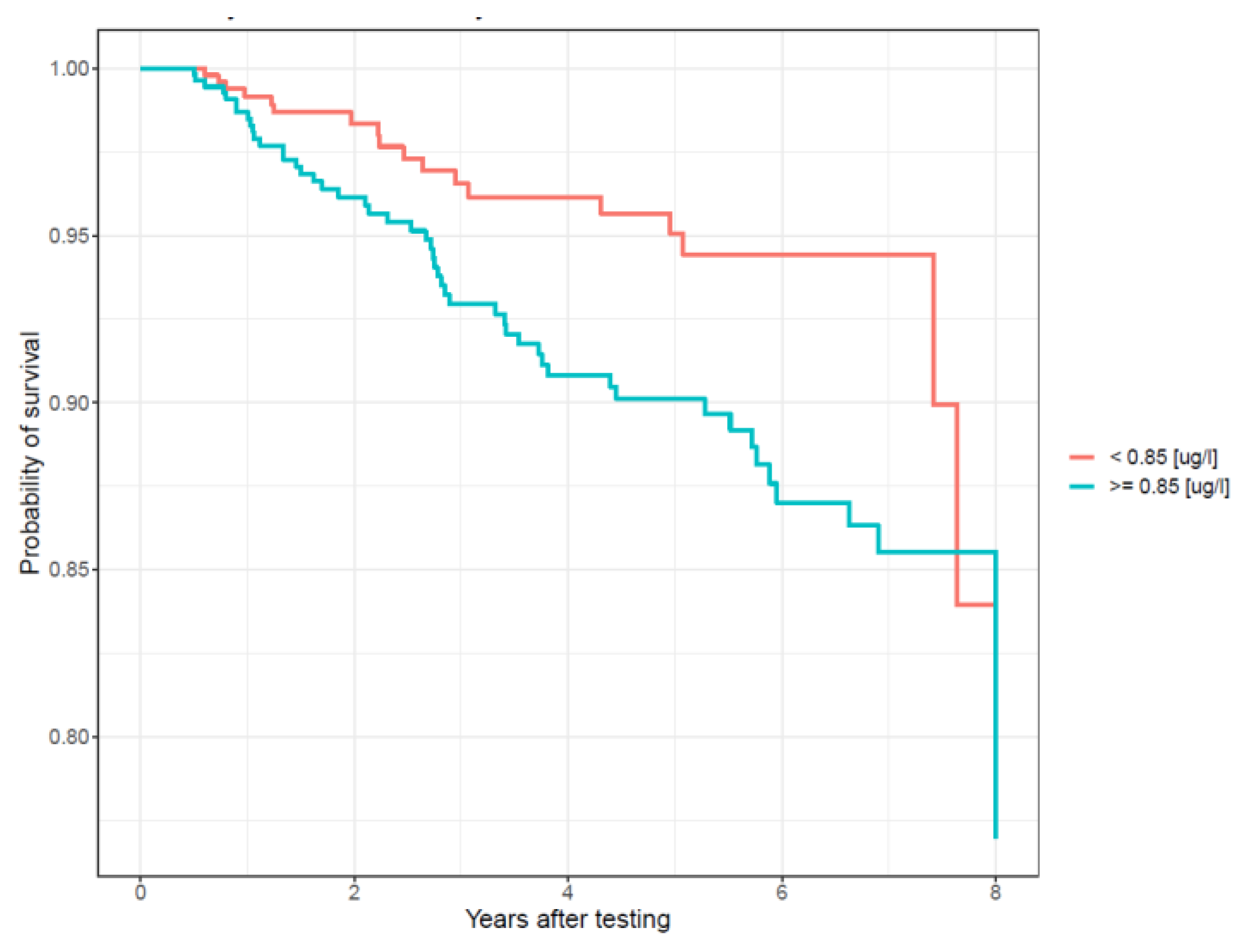
| Arsenic Level (µg/L) | Total | Cancers | Univariate HR (95%CI) | p | Multivariate HR * (95%CI) | p |
|---|---|---|---|---|---|---|
| <0.85 | 513 | 18 | 1 (Ref.) | - | 1 (Ref.) | - |
| ≥0.85 | 548 | 49 | 2.03 (1.18–3.49) | 0.011 | 2.05 (1.18–3.56) | 0.011 |
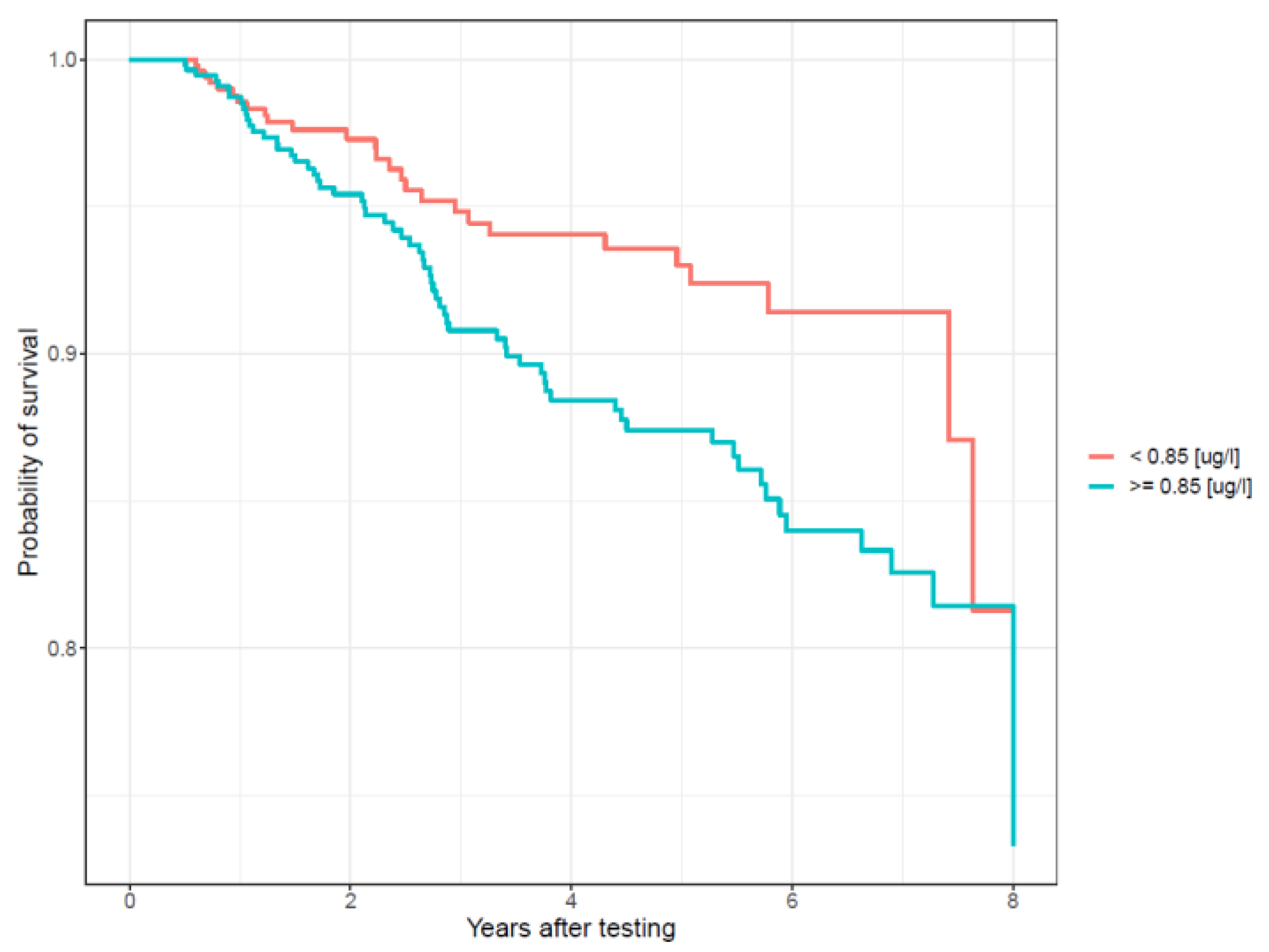
| Arsenic Level (µg/L) | Total | Cancers | Univariate HR (95%CI) | p | Multivariate HR * (95%CI) | p |
|---|---|---|---|---|---|---|
| <0.85 | 522 | 27 | 1 (Ref.) | - | 1 (Ref.) | - |
| ≥0.85 | 562 | 63 | 1.73 (1.10–2.71) | 0.01 | 1.73 (1.09–2.74) | 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marciniak, W.; Matoušek, T.; Domchek, S.; Paradiso, A.; Patruno, M.; Irmejs, A.; Roderte, I.; Derkacz, R.; Baszuk, P.; Kuświk, M.; et al. Blood Arsenic Levels as a Marker of Breast Cancer Risk among BRCA1 Carriers. Cancers 2021, 13, 3345. https://doi.org/10.3390/cancers13133345
Marciniak W, Matoušek T, Domchek S, Paradiso A, Patruno M, Irmejs A, Roderte I, Derkacz R, Baszuk P, Kuświk M, et al. Blood Arsenic Levels as a Marker of Breast Cancer Risk among BRCA1 Carriers. Cancers. 2021; 13(13):3345. https://doi.org/10.3390/cancers13133345
Chicago/Turabian StyleMarciniak, Wojciech, Tomáš Matoušek, Susan Domchek, Angelo Paradiso, Margherita Patruno, Arvids Irmejs, Irita Roderte, Róża Derkacz, Piotr Baszuk, Magdalena Kuświk, and et al. 2021. "Blood Arsenic Levels as a Marker of Breast Cancer Risk among BRCA1 Carriers" Cancers 13, no. 13: 3345. https://doi.org/10.3390/cancers13133345
APA StyleMarciniak, W., Matoušek, T., Domchek, S., Paradiso, A., Patruno, M., Irmejs, A., Roderte, I., Derkacz, R., Baszuk, P., Kuświk, M., Cybulski, C., Huzarski, T., Gronwald, J., Dębniak, T., Falco, M., Lener, M. R., Jakubowska, A., Pullella, K., Kotsopoulos, J., ... Lubiński, J. (2021). Blood Arsenic Levels as a Marker of Breast Cancer Risk among BRCA1 Carriers. Cancers, 13(13), 3345. https://doi.org/10.3390/cancers13133345