
Comparison of Selected Immune and Hematological Parameters and Their Impact on Survival in Patients with HPV-Related and HPV-Unrelated Oropharyngeal Cancer

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
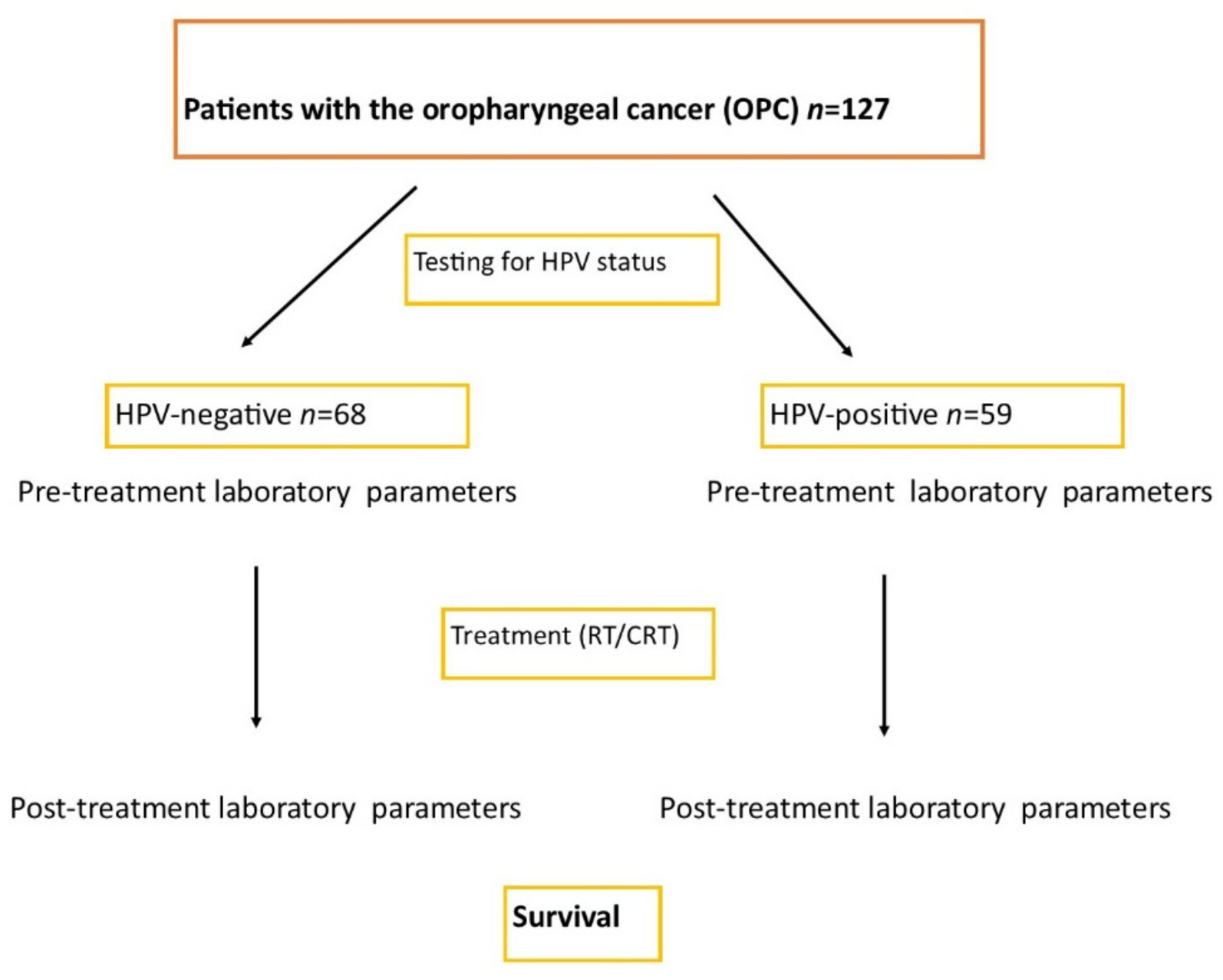
2.1. Patients
2.2. Study Design
2.2.1. The Information on Grant and Ethical Standards
2.2.2. Laboratory Blood Investigations and Analysis
2.2.3. Confirmation of the HPV Etiology
Tissue Material
Analysis of cfHPV16 DNA in Plasma
2.2.4. Histopathological Staging and Grading Classification
2.2.5. Follow-Up
2.3. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Laboratory Results before and after Treatment
3.3. Comparison of Clinical and Pathological Characteristics Depending on the Values of Immune Ratios in HPV− and HPV+ Patients
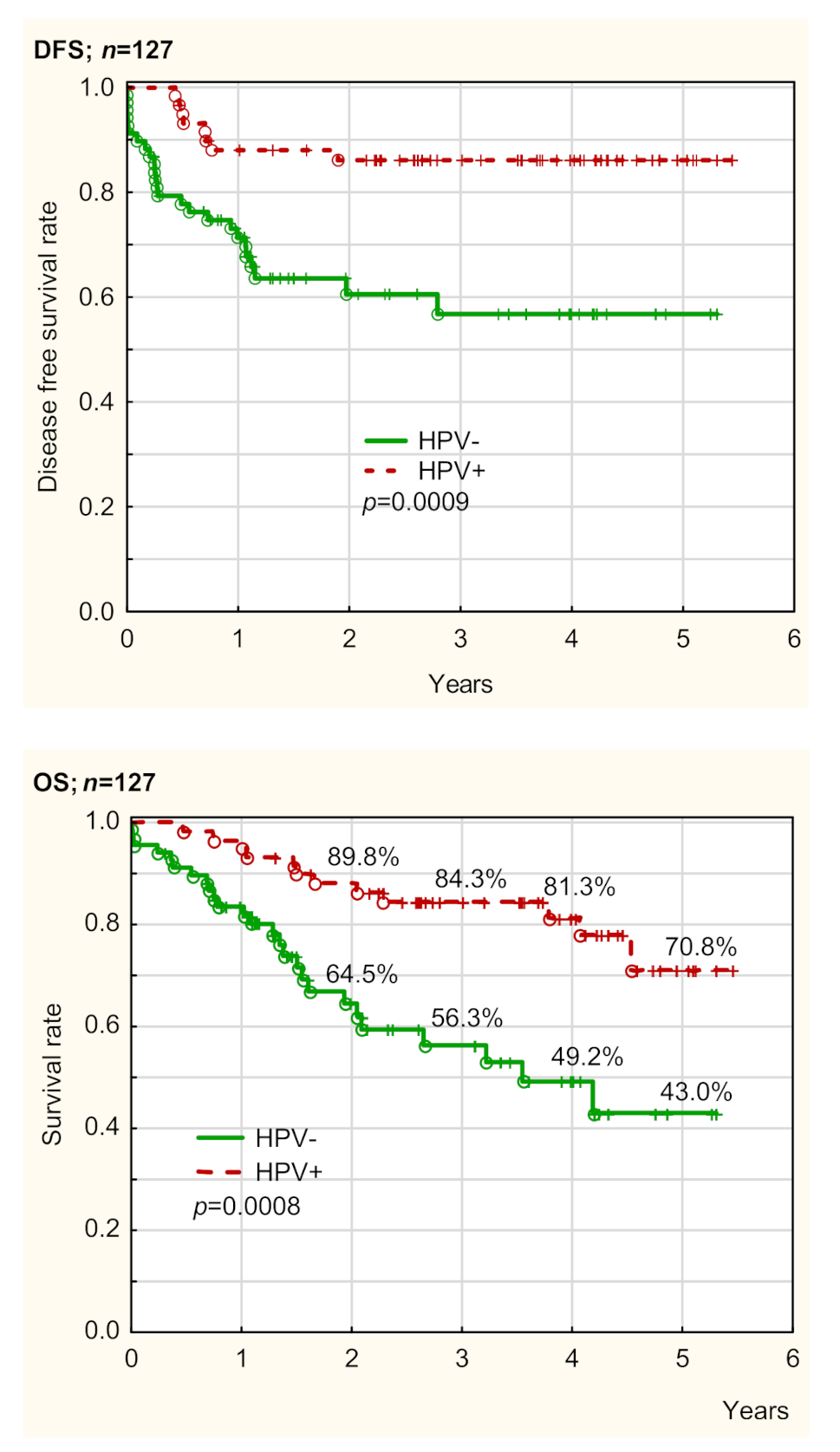
3.4. Overall Survival and Disease-Free Survival Depending on HPV Status
3.4.1. Overall Survival Depending on Pre-Treatment Parameters
HPV−
HPV+
3.4.2. Disease-Free Survival Depending on Pre-Treatment Parameters
HPV−
HPV+
3.4.3. Overall Survival Depending on Post-Treatment Parameters
HPV−
HPV+
3.4.4. Disease-Free Survival Depending on Post-Treatment Parameters
HPV−
HPV+
3.4.5. Summary of the Analysis of OS and DFS in HPV− and HPV+ Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huang, S.H.; Waldron, J.; Milosevic, M.; Shen, X.; Ringash, J.; Su, J.; Tong, L.; Perez-Ordonez, B.; Weinreb, I.; Bayley, A.J.; et al. Prognostic value of pretreatment circulating neutrophils, monocytes, and lymphocytes in oropharyngeal cancer stratified by human papillomavirus status. Cancer 2014, 121, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Sakakura, K.; Tada, H.; Kaira, K.; Oyama, T.; Chikamatsu, K. Prognostic significance and population dynamics of peripheral monocytes in patients with oropharyngeal squamous cell carcinoma. Head Neck 2019, 41, 1880–1888. [Google Scholar] [CrossRef] [PubMed]
- Meshman, J.; Velez, M.A.; Wang, P.-C.; Abemayor, E.; John, M.S.; Wong, D.; Bhuta, S.; Chen, A.M. Immunologic mediators of outcome for irradiated oropharyngeal carcinoma based on human papillomavirus status. Oral Oncol. 2019, 89, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Yamashita, Y.; Ikegami, T.; Hirakawa, H.; Uehara, T.; Deng, Z.; Agena, S.; Uezato, J.; Kondo, S.; Kiyuna, A.; Maeda, H.; et al. Staging and prognosis of oropharyngeal carcinoma according to the 8th Edition of the American Joint Committee on Cancer Staging Manual in human papillomavirus infection. Eur. Arch. Oto. Rhino. Laryngol. 2019, 276, 827–836. [Google Scholar] [CrossRef] [Green Version]
- Mallen-St Clair, J.; Ho, A.S. American Joint Committee on Cancer 8th edition staging-an improvement in prognostication in HPV-associated oropharyngeal cancer? Ann. Transl. Med. 2019, 7 (Suppl. 1), S10. [Google Scholar]
- Lechien, J.R.; Seminerio, I.; Descamps, G.; Mat, Q.; Mouawad, F.; Hans, S.; Julieron, M.; Dequanter, D.; Vanderhaegen, T.; Journe, F.; et al. Impact of HPV Infection on the Immune System in Oropharyngeal and Non-Oropharyngeal Squamous Cell Carcinoma: A Systematic Review. Cells 2019, 8, 1061. [Google Scholar] [CrossRef] [Green Version]
- Snietura, M.; Vanderhaegen, T.; Brewczynski, A.; Kopec, A.; Rutkowski, T. Infiltrates of M2-Like Tumour-Associated Macrophages Are Adverse Prognostic Factor in Patients with Human Papillomavirus-Negative but Not in Human Papillomavirus-Positive Oropharyngeal Squamous Cell Carcinoma. Pathobiology 2020, 87, 75–86. [Google Scholar] [CrossRef]
- Rajjoub, S.; Basha, S.R.; Einhorn, E.; Cohen, M.C.; Marvel, D.M.; Sewell, D.A. Prognostic significance of tumor-infiltrating lymphocytes in oropharyngeal cancer. Ear Nose Throat J. 2007, 86, 506–511. [Google Scholar] [CrossRef]
- Ward, M.J.; Thirdborough, S.M.; Mellows, T.; Riley, C.; Harris, S.B.; Suchak, K.; Webb, A.A.R.; Hampton, C.L.; Patel, N.N.; Randall, C.J.; et al. Tumour-infiltrating lymphocytes predict for outcome in HPV-positive oropharyngeal cancer. Br. J. Cancer 2014, 110, 489–500. [Google Scholar] [CrossRef] [Green Version]
- King, E.V.; Ottensmeier, C.H.; Thomas, G.J. The immune response in HPV+oropharyngeal cancer. Oncoimmunology 2014, 3, e27254. [Google Scholar] [CrossRef] [Green Version]
- Gorphe, P.; Idrissi, Y.C.; Tao, Y.; Schernberg, A.; Ou, D.; Temam, S.; Casiraghi, O.; Blanchard, P.; Mirghani, H. Anemia and neutrophil-to-lymphocyte ratio are prognostic in p16-positive oropharyngeal carcinoma treated with concurrent chemoradiation. Papillomavirus Res. 2018, 5, 32–37. [Google Scholar] [CrossRef]
- Ye, J.; Liao, B.; Jiang, X.; Dong, Z.; Hu, S.; Liu, Y.; Xiao, M. Prognosis Value of Platelet Counts, Albumin and Neutrophil-Lymphocyte Ratio of Locoregional Recurrence in Patients with Operable Head and Neck Squamous Cell Carcinoma. Cancer Manag. Res. 2020, 12, 731–741. [Google Scholar] [CrossRef] [Green Version]
- Shoultz-Henley, S.; Garden, A.; Mohamed, A.S.; Sheu, T.; Kroll, M.H.; Rosenthal, D.; Gunn, G.B.; Hayes, A.J.; French, C.; Eichelberger, H.; et al. Prognostic value of pretherapy platelet elevation in oropharyngeal cancer patients treated with chemoradiation. Int. J. Cancer 2015, 138, 1290–1297. [Google Scholar] [CrossRef] [Green Version]
- Rachidi, S.; Wallace, K.; Wrangle, J.M.; Day, T.A.; Alberg, A.J.; Li, Z. Neutrophil-to-lymphocyte ratio and overall survival in all sites of head and neck squamous cell carcinoma. Head Neck 2016, 38, E1068–E1074. [Google Scholar] [CrossRef] [Green Version]
- Charles, K.A.; Harris, B.D.W.; Haddad, C.R.; Clarke, S.J.; Guminski, A.; Stevens, M.; Dodds, T.; Gill, A.J.; Back, M.; Veivers, D.; et al. Systemic inflammation is an independent predictive marker of clinical outcomes in mucosal squamous cell carcinoma of the head and neck in oropharyngeal and non-oropharyngeal patients. BMC Cancer 2016, 16, 124. [Google Scholar] [CrossRef] [Green Version]
- Kano, S.; Homma, A.; Hatakeyama, H.; Mizumachi, T.; Sakashita, T.; Kakizaki, T.; Fukuda, S. Pretreatment lymphocyte-to-monocyte ratio as an independent prognostic factor for head and neck cancer. Head Neck 2016, 39, 247–253. [Google Scholar] [CrossRef] [Green Version]
- Valero, C.; Pardo, L.; López, M.; García, J.; Camacho, M.; Quer, M.; León, X. Pretreatment count of peripheral neutrophils, monocytes, and lymphocytes as independent prognostic factor in patients with head and neck cancer. Head Neck 2017, 39, 219–226. [Google Scholar] [CrossRef]
- Selzer, E.; Grah, A.; Heiduschka, G.; Kornek, G.; Thurnher, D. Primary radiotherapy or postoperative radiotherapy in patients with head and neck cancer: Comparative analysis of inflammation-based prognostic scoring systems. Strahlenther. Onkol. 2015, 191, 486–494. [Google Scholar] [CrossRef]
- Moon, H.; Roh, J.-L.; Lee, S.-W.; Kim, S.-B.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Prognostic value of nutritional and hematologic markers in head and neck squamous cell carcinoma treated by chemoradiotherapy. Radiother. Oncol. 2016, 118, 330–334. [Google Scholar] [CrossRef]
- Yao, J.-J.; Zhu, F.-T.; Dong, J.; Liang, Z.-B.; Yang, L.-W.; Chen, S.-Y.; Zhang, W.-J.; Lawrence, W.R.; Zhang, F.; Wang, S.-Y.; et al. Prognostic value of neutrophil-to-lymphocyte ratio in advanced nasopharyngeal carcinoma: A large institution-based cohort study from an endemic area. BMC Cancer 2019, 19, 37. [Google Scholar] [CrossRef] [Green Version]
- Lu, A.; Li, H.; Zheng, Y.; Tang, M.; Li, J.; Wu, H.; Zhong, W.; Gao, J.; Ou, N.; Cai, Y. Prognostic Significance of Neutrophil to Lymphocyte Ratio, Lymphocyte to Monocyte Ratio, and Platelet to Lymphocyte Ratio in Patients with Nasopharyngeal Carcinoma. BioMed Res. Int. 2017, 2017, 30478022. [Google Scholar] [CrossRef]
- Gao, Y.; Guo, W.; Cai, S.; Zhang, F.; Shao, F.; Zhang, G.; Liu, T.; Tan, F.; Li, N.; Xue, Q.; et al. Systemic immune-inflammation index (SII) is useful to predict survival outcomes in patients with surgically resected esophageal squamous cell carcinoma. J. Cancer 2019, 10, 3188–3196. [Google Scholar] [CrossRef] [Green Version]
- Coffelt, S.B.; Wellenstein, M.D.; De Visser, S.B.C.M.D.W.K.E. Neutrophils in cancer: Neutral no more. Nat. Rev. Cancer 2016, 16, 431–446. [Google Scholar] [CrossRef] [Green Version]
- De Larco, J.E.; Wuertz, B.R.; Furcht, L.T. The potential role of neutrophils in promoting the metastatic phenotype of tumors releasing interleukin-8. Clin. Cancer Res. 2004, 10, 4895–4900. [Google Scholar] [CrossRef] [Green Version]
- Stanger, B.Z.; Kahn, M.L. Platelets and Tumor Cells: A New Form of Border Control. Cancer Cell 2013, 24, 9–11. [Google Scholar] [CrossRef] [Green Version]
- Gooden, M.J.; de Bock, G.H.; Leffers, N.; Daemen, T.; Nijman, H.W. The prognostic influence of tumour-infiltrating lymphocytes in cancer: A systematic review with meta-analysis. Br. J. Cancer 2011, 105, 93. [Google Scholar] [CrossRef] [Green Version]
- Jia, Q.; Yang, Y.; Wan, Y. Tumor-infiltrating memory T-lymphocytes for prognostic prediction in cancer patients: A meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 1803–1813. [Google Scholar]
- Diao, P.; Wu, Y.; Li, J.; Zhang, W.; Huang, R.; Zhou, C.; Wang, Y.; Cheng, J. Preoperative systemic immune-inflammation index predicts prognosis of patients with oral squamous cell carcinoma after curative resection. J. Transl. Med. 2018, 16, 365. [Google Scholar] [CrossRef]
- Wang, L.; Wang, C.; Wang, J.; Huang, X.; Cheng, Y. A novel systemic immune-inflammation index predicts survival and quality of life of patients after curative resection for esophageal squamous cell carcinoma. J. Cancer Res. Clin. Oncol. 2017, 143, 2077–2086. [Google Scholar] [CrossRef]
- Geng, Y.; Shao, Y.; Zhu, D.; Zheng, X.; Zhou, Q.; Zhou, W.; Ni, X.; Wu, C.; Jiang, J. Systemic Immune-Inflammation Index Predicts Prognosis of Patients with Esophageal Squamous Cell Carcinoma: A Propensity Score-matched Analysis. Sci. Rep. 2016, 6, 39482. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.-F.; Chen, S.; Yang, X. Systemic immune-inflammation index (SII) is a useful prognostic indicator for patients with squamous cell carcinoma of the esophagus. Medicine 2017, 96, e5886. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.-H.; Zhai, E.-T.; Yuan, Y.; Wu, K.-M.; Xu, J.-B.; Peng, J.-J.; Chen, C.-Q.; He, Y.-L.; Cai, S.-R. Systemic immune-inflammation index for predicting prognosis of colorectal cancer. World J. Gastroenterol. 2017, 23, 6261–6272. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.-K.; Chen, P.; Hu, W.-M.; Sun, P.; He, W.-Z.; Jiang, C.; Kong, P.-F.; Liu, S.-S.; Chen, H.-T.; Yang, Y.-Z.; et al. The systemic immune-inflammation index is an independent predictor of survival for metastatic colorectal cancer and its association with the lymphocytic response to the tumor. J. Transl. Med. 2018, 16, 273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tong, Y.-S.; Tan, J.; Zhou, X.-L.; Song, Y.-Q.; Song, Y.-J. Systemic immune-inflammation index predicting chemoradiation resistance and poor outcome in patients with stage III non-small cell lung cancer. J. Transl. Med. 2017, 15, 221. [Google Scholar] [CrossRef]
- Zhang, K.; Hua, Y.-Q.; Wang, D.; Chen, L.-Y.; Wu, C.-J.; Chen, Z.; Liu, L.-M.; Chen, H. Systemic immune-inflammation index predicts prognosis of patients with advanced pancreatic cancer. J. Transl. Med. 2019, 17, 30. [Google Scholar] [CrossRef]
- Man, Y.-N.; Chen, Y.-F. Systemic immune-inflammation index, serum albumin, and fibrinogen impact prognosis in castration-resistant prostate cancer patients treated with first-line docetaxel. Int. Urol. Nephrol. 2019, 51, 2189–2199. [Google Scholar] [CrossRef]
- Hu, B.; Yang, X.-R.; Xu, Y.; Sun, Y.-F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.-M.; Qiu, S.-J.; Zhou, J.; et al. Systemic Immune-Inflammation Index Predicts Prognosis of Patients after Curative Resection for Hepatocellular Carcinoma. Clin. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Jiang, Y.; Cao, H.; Zhu, H.; Chen, B.; Ji, W. Nomogram Based on Systemic Immune-Inflammation Index to Predict Overall Survival in Gastric Cancer Patients. Dis. Markers 2018, 2018, 1787424. [Google Scholar] [CrossRef] [Green Version]
- Zhang, W.; Wang, R.; Ma, W.; Wu, Y.; Maskey, N.; Guo, Y.; Liu, J.; Mao, S.; Zhang, J.; Yao, X.; et al. Systemic immune-inflammation index predicts prognosis of bladder cancer patients after radical cystectomy. Ann. Transl. Med. 2019, 7, 431. [Google Scholar] [CrossRef]
- De Giorgi, U.; Procopio, G.; Giannarelli, D.; Sabbatini, R.; Bearz, A.; Buti, S.; Basso, U.; Mitterer, M.; Ortega, C.; Bidoli, P.; et al. Association of Systemic Inflammation Index and Body Mass Index with Survival in Patients with Renal Cell Cancer Treated with Nivolumab. Clin. Cancer Res. 2019, 25, 3839–3846. [Google Scholar] [CrossRef] [Green Version]
- Huang, H.; Liu, Q.; Zhu, L.; Zhang, Y.; Lu, X.; Wu, Y.; Liu, L. Prognostic Value of Preoperative Systemic Immune-Inflammation Index in Patients with Cervical Cancer. Sci. Rep. 2019, 9, 3284. [Google Scholar] [CrossRef] [Green Version]
- Van Der Willik, K.D.; Koppelmans, V.; Hauptmann, M.; Compter, A.; Ikram, M.A.; Schagen, S.B. Inflammation markers and cognitive performance in breast cancer survivors 20 years after completion of chemotherapy: A cohort study. Breast Cancer Res. 2018, 20, 135. [Google Scholar] [CrossRef] [Green Version]
- De Felice, F.; Tombolini, V.; Valentini, V.; De Vincentiis, M.; Mezi, S.; Brugnoletti, O.; Polimeni, A. Advances in the Management of HPV-Related Oropharyngeal Cancer. J. Oncol. 2019, 2019, 9173729. [Google Scholar] [CrossRef]
- Malm, I.-J.; Fan, C.J.; Yin, L.; Li, D.X.; Koch, W.M.; Gourin, C.G.; Pitman, K.T.; Richmon, J.D.; Westra, W.H.; Kang, H.; et al. Evaluation of proposed staging systems for human papillomavirus-related oropharyngeal squamous cell carcinoma. Cancer 2017, 123, 1768–1777. [Google Scholar] [CrossRef] [Green Version]
- Masterson, L.; Moualed, D.; Liu, Z.W.; Howard, J.E.; Dwivedi, R.C.; Tysome, J.R.; Benson, R.; Sterling, J.C.; Sudhoff, H.; Jani, P.; et al. De-escalation treatment protocols for human papillomavirus-associated oropharyngeal squamous cell carcinoma: A systematic review and meta-analysis of current clinical trials. Eur. J. Cancer 2014, 50, 2636–2648. [Google Scholar] [CrossRef]
- Petar, S.; Marko, S.; Ivica, L. De-escalation in HPV-associated oropharyngeal cancer: Lessons learned from the past? A critical viewpoint and proposal for future research. Eur. Arch. Oto. Rhino. Laryngol. 2021. [Google Scholar] [CrossRef]
- Harrowfield, J.; Isenring, E.; Kiss, N.; Laing, E.; Lipson-Smith, R.; Britton, B. The Impact of Human Papillomavirus (HPV) Associated Oropharyngeal Squamous Cell Carcinoma (OPSCC) on Nutritional Outcomes. Nutrients 2021, 13, 514. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human Papillomavirus and Survival of Patients with Oropharyngeal Cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Licitra, L.; Perrone, F.; Bossi, P.; Suardi, S.; Mariani, L.; Artusi, R.; Oggionni, M.; Rossini, C.; Cantu’, G.; Squadrelli, M.; et al. High-Risk Human Papillomavirus Affects Prognosis in Patients With Surgically Treated Oropharyngeal Squamous Cell Carcinoma. J. Clin. Oncol. 2006, 24, 5630–5636. [Google Scholar] [CrossRef] [Green Version]
- Lindquist, D.; Romanitan, M.; Hammarstedt, L.; Näsman, A.; Dahlstrand, H.; Lindholm, J.; Onelöv, L.; Ramqvist, T.; Ye, W.; Munck-Wikland, E.; et al. Human papillomavirus is a favourable prognostic factor in tonsillar cancer and its oncogenic role is supported by the expression of E6 and E7. Mol. Oncol. 2007, 1, 350–355. [Google Scholar] [CrossRef] [Green Version]
- Lassen, P.; Eriksen, J.G.; Hamilton-Dutoit, S.; Tramm, T.; Alsner, J.; Overgaard, J. Effect of HPV-associated p16INK4A expression on response to radiotherapy and survival in squamous cell carcinoma of the head and neck. J. Clin. Oncol. 2009, 27, 1992–1998. [Google Scholar] [CrossRef] [Green Version]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J. Natl. Cancer Inst. 2008, 100, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Ihloff, A.S.; Petersen, C.; Hoffmann, M.; Knecht, R.; Tribius, S. Human papilloma virus in locally advanced stage III/IV squamous cell cancer of the oropharynx and impact on choice of therapy. Oral Oncol. 2010, 46, 705–711. [Google Scholar] [CrossRef] [PubMed]
- You, E.L.; Henry, M.; Zeitouni, A.G. Human papillomavirus-associated oropharyngeal cancer: Review of current evidence and management. Curr. Oncol. 2019, 26, 119–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, X.J.; Tang, L.L.; Mao, Y.P.; Guo, R.; Sun, Y.; Lin, A.H.; Ma, J. Value of the prognostic nutritional index and weight loss in predicting metastasis and long-term mortality in nasopharyngeal carcinoma. J. Transl. Med. 2015, 13, 364. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Feature | All n = 127 | HPV(−) n = 68 | HPV(+) n = 59 | p |
|---|---|---|---|---|
| Demographic characteristics | ||||
| Age | 60.62 ± 8.54 (30–80) | 60.85 ± 7.48 (37–79) | 60.36 ± 9.67 (30–80) | 0.745 |
| Male | 87(68.5%) | 51 (75.1%) | 36 (61.0%) | 0.133 |
| Female | 40 (31.5%) | 17 (25.0%) | 23 (39.0%) | |
| Tumor location | ||||
| 1. tonsil | 91 (71.70%) | 44 (64.70%) | 47 (79.70%) | 0.010 |
| 2. palate | 10 (7.90%) | 10 (14.70%) | 0 (0.00%) | |
| 3. root of the tongue | 22 (17.30%) | 13 (19.10%) | 9 (15.30%) | |
| 4.other oropharynx | 4 (3.10%) | 1 (1.50%) | 3 (5.10%) | |
| Histopathological grading | ||||
| G1 | 7 (5.5%) | 6 (8.8%) | 1 (1.7%) | 0.054 |
| G2 | 55 (43.3%) | 34 (50.0%) | 21 (35.6%) | |
| G3 | 19 (15.0%) | 7 (10.3%) | 12 (20.3%) | |
| n.d. | 46 (36.2%) | 21 (30.9%) | 25 (42.4%) | |
| Tumor depth (T) | ||||
| T1 | 13 (10.2%) | 8 (11.8%) | 5 (8.5%) | 0.743 |
| T2 | 42 (33.1%) | 24 (35.3%) | 18 (30.5%) | |
| T3 | 44 (34.6%) | 22 (32.4%) | 22 (37.3%) | |
| T4 | 27 (21.3%) | 13 (19.1%) | 14 (23.7%) | |
| Tx | 1 (0.8%) | 1 (1.5%) | 0 (0.0%) | |
| Lymph node metastasis | ||||
| N 0–1 | 52 (40.9%) | 36 (52.9%) | 16 (27.1%) | 0.005 |
| N 2–3 | 74 (58.3%) | 32 (47.1%) | 42 (71.2%) | |
| Nx | 1 (0.8%) | 1 (1.7%) | ||
| General treatment regimen | ||||
| Radiotherapy | 31 (24.4%) | 24 (35.3%) | 7 (11.9%) | 0.003 |
| Radiochemotherapy | 96 (75.6%) | 44 (64.7%) | 52 (88.1%) |
| Variable | OS HPV− | OS HPV+ | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Hb 0 [g/dL] >11.8 vs. <11.8 | 0.65 (0.15–2.79) | 0.563 | 1.65 (0.21–12.86) | 0.635 | ||||
| RetHb 0 [/mm3] >34.0 vs. <34.0 | 0.9 (0.39–2.06) | 0.803 | 2.42 (0.65–9.08) | 0.190 | 4.33 (0.91–20.51) | 0.065 | ||
| RBC 0 [/mm3] >4.6 vs. <4.6 | 0.46 (0.18–1.13) | 0.091 | 0.76 (0.25–2.37) | 0.641 | ||||
| Ret 0 [/mm3] >37.9 vs. <37.9 | 0.6 (0.26–1.38) | 0.229 | 0.22 (0.06–0.82) | 0.025 | ||||
| WBC 0 [/mm3] >8.33 vs. <8.33 | 2.33 (0.99–5.47) | 0.053 | 4.17 (1.25–13.93) | 0.020 | ||||
| CLC 0 [/mm3] >1.10 vs. <1.10 | 0.7 (0.28–1.74) | 0.442 | 0.42 (0.11–1.56) | 0.197 | ||||
| CNC 0 [/mm3] >4.96 vs. <4.96 | 1.82 (0.78–4.22) | 0.166 | 2.54 (0.75–8.52) | 0.132 | ||||
| CMC 0 [/mm3] >0.93 vs. <0.93 | 2.41 (1.01–5.74) | 0.048 | 4.24 (1.52–11.84) | 0.006 | 3.37 (0.72–15.72) | 0.122 | 17.8 (1.89–167.47) | 0.012 |
| PLT 0 [/mm3] >240 vs. <240 | 2.53 (1.07–5.99) | 0.035 | 1.1 (0.34–3.58) | 0.872 | 0.29 (0.07–1.18) | 0.085 | ||
| NLR 0 >2.13 vs. <2.13 | 1.44 (0.65–3.18) | 0.364 | 0.36 (0.12–1.10) | 0.074 | 4.76 (1.29–17.57) | 0.019 | ||
| MLR 0 >0.43 vs. <0.43 | 3.73 (1.71–8.15) | 0.001 | 3.83 (1.46–10.02) | 0.006 | 0.47 (0.06–3.64) | 0.470 | 0.07 (0.00–1.17) | 0.064 |
| PLR 0 >131.29 vs. <131.29 | 1.67 (0.76–3.69) | 0.204 | 3.6 (1.15–11.31) | 0.028 | 1.89 (0.59–6.03) | 0.281 | ||
| SII 0 >448.60 vs. <448.60 | 1.95 (0.81–4.68) | 0.135 | 5.67 (1.24–25.94) | 0.025 | 11.1 (2.02–60.97) | 0.006 | ||
| Treatment regimen RT/CRT | 0.93 (0.42–2.06) | 0.858 | 0.60 (0.08–4.64) | 0.623 | ||||
| Variable | DFS HPV− | DFS HPV+ | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Hb 0 [g/dL] >13.5 vs. <13.5 | 0.38 (0.17–0.87) | 0.021 | 1.15 (0.27–4.82) | 0.848 | 10.44 (1.31–83.38) | 0.027 | ||
| RetHb 0 [/mm3] >36.4 vs. <36.4 | 1.47 (0.57–3.78) | 0.423 | 1.30 (0.26–6.43) | 0.750 | ||||
| RBC 0 [/mm3] >4.6 vs. <4.6 | 0.39 (0.15–0.97) | 0.043 | 0.21 (0.07–0.66) | 0.008 | 0.43 (0.1–1.81) | 0.252 | 0.07 (0.01–0.60) | 0.015 |
| Ret 0 [/mm3] >54.7 vs. <54.7 | 0.64 (0.26–1.56) | 0.323 | 0.23 (0.05–1.12) | 0.068 | ||||
| WBC 0 [/mm3] >8.33 vs. <8.33 | 1.57 (0.67–3.71) | 0.301 | 2.42 (0.49–12.03) | 0.280 | ||||
| CLC 0 [/mm3] >1.28 vs. <1.28 | 0.61 (0.25–1.47) | 0.271 | 0.19 (0.05–0.77) | 0.020 | 0.17 (0.03–0.97) | 0.046 | ||
| CNC 0 [/mm3] >4.23 vs. <4.23 | 1.23 (0.56–2.72) | 0.609 | 1.57 (0.38–6.6) | 0.534 | ||||
| CMC 0 [/mm3] >0.46 vs. <0.46 | 0.77 (0.32–1.85) | 0.557 | 0.16 (0.03–0.8) | 0.026 | 0.20 (0.04–1.07) | 0.060 | ||
| PLT 0 [/mm3] >319 vs. <319 | 2.77 (1.18–6.52) | 0.020 | 1.59 (0.19–12.91) | 0.667 | ||||
| NLR 0 >2.29 vs. <2.29 | 1.63 (0.73–3.63) | 0.232 | 6.02 (1.21–29.87) | 0.028 | ||||
| MLR 0 >0.27 vs. <0.27 | 0.62 (0.28–1.38) | 0.242 | 0.20 (0.06–0.62) | 0.006 | 0.46 (0.11–1.94) | 0.291 | ||
| PLR 0 >173.20 vs. <173.20 | 2.88 (1.30–6.38) | 0.009 | 2.74 (1.02–7.41) | 0.046 | 1.77 (0.36–8.75) | 0.487 | ||
| SII 0 >462.58 vs. <462.58 | 2.22 (0.92–5.35) | 0.075 | 3.11 (0.90–10.77) | 0.074 | 8.48 (1.04–68.98) | 0.046 | ||
| Treatment regimen | 0.71 (0.31–1.64) | 0.422 | 0.00 | 0.993 | ||||
| Variable | OS HPV− | OS HPV+ | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Hb 1 [g/dL] >10.1 vs. <10.1 | 0.27 (0.08–0.93) | 0.037 | 0.47 (0.06–3.77) | 0.478 | ||||
| RetHb 1 [/mm3] >37.8 vs. <37.8 | 1.37 (0.50–3.77) | 0.537 | 0.67 (0.14–3.17) | 0.613 | ||||
| RBC 1 [/mm3] >3.75 vs. <3.75 | 0.53 (0.24–1.17) | 0.118 | 0.32 (0.12–0.86) | 0.024 | 0.72 (0.23–2.29) | 0.580 | ||
| Ret 1 [/mm3] >27.5 vs. <27.5 | 4.15 (0.56–30.94) | 0.166 | 11.24 (0.99–127.94) | 0.051 | 0.48 (0.14–1.65) | 0.245 | ||
| WBC 1 [/mm3] >3.74 vs. <3.74 | 0.83 (0.36–1.93) | 0.664 | 0.16 (0.03–0.93) | 0.042 | 2.60 (0.70–9.64) | 0.152 | ||
| CLC 1 [/mm3] >0.83 vs. <0.83 | 0.90 (0.36–2.27) | 0.823 | 8.70 (2.26–33.54) | 0.002 | 11.37 (2.61–49.64) | 0.001 | ||
| CNC 1 [/mm3] >2.32 vs. <2.32 | 1.15 (0.43–3.06) | 0.782 | 7.48 (1.00–56.06) | 0.050 | 1.51 (0.40–5.61) | 0.541 | ||
| CMC 1 [/mm3] >0.42 vs. <0.42 | 1.70 (0.68–4.27) | 0.260 | 0.94 (0.30–2.90) | 0.908 | ||||
| PLT 1 [/mm3] >313 vs. <313 | 2.06 (0.89–4.77) | 0.092 | 3.37 (1.18–9.62) | 0.023 | 2.05 (0.26–16.14) | 0.495 | ||
| NLR 1 >6.45 vs. <6.45 | 1.15 (0.48–2.79) | 0.754 | 0.43 (0.12–1.60) | 0.209 | ||||
| MLR 1 >0.63 vs. <0.63 | 0.85 (0.38–1.91) | 0.697 | 0.35 (0.12–1.03) | 0.057 | 0.36 (0.09–1.39) | 0.138 | ||
| PLR 1 >404.17 vs. <404.17 | 2.55 (1.13–5.77) | 0.024 | 0.87 (0.28–2.72) | 0.815 | ||||
| SII 1 >2763 vs. <2763 | 3.54 (1.28–9.80) | 0.015 | 4.69 (1.23–17.97) | 0.024 | 2.12 (0.46–9.81) | 0.338 | 4.17 (0.76–22.88) | 0.100 |
| Variable | DFS HPV− | DFS HPV+ | ||||||
|---|---|---|---|---|---|---|---|---|
| Univariate Analysis | Multivariate Analysis | Univariate Analysis | Multivariate Analysis | |||||
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | |
| Hb 1 [g/dL] >10.8 vs. <10.8 | 0.37 (0.15–0.89) | 0.027 | 2.35 (0.29–19.11) | 0.424 | ||||
| RetHb 1 [/mm3] >38.0 vs. <38.0 | 2.28 (0.76–6.82) | 0.142 | 0.72 (0.09–5.98) | 0.761 | ||||
| RBC 1 [/mm3] >3.75 vs. <3.75 | 0.42 (0.19–0.93) | 0.033 | 0.26 (0.11–0.66) | 0.004 | 1.56 (0.31–7.71) | 0.589 | ||
| Ret 1 [/mm3] >27.5 vs. <27.5 | 4.03 (0.54–30.11) | 0.174 | 0.39 (0.09–1.76) | 0.221 | ||||
| WBC 1 [/mm3] >3.21 vs. <3.21 | 0.57 (0.23–1.44) | 0.233 | 17780630 | 0.994 | ||||
| CLC 1 [/mm3] >0.37 vs. <0.37 | 0.56 (0.22–1.42) | 0.226 | 4.03 (0.50–32.73) | 0.193 | ||||
| CNC 1 [/mm3] >2.69 vs. <2.69 | 0.98 (0.40–2.35) | 0.956 | 1.66 (0.40–6.95) | 0.488 | ||||
| CMC 1 [/mm3] >0.47 vs. <0.47 | 0.50 (0.22–1.11) | 0.087 | 1.31 (0.33–5.22) | 0.706 | ||||
| PLT 1 [/mm3] >261 vs. <261 | 1.07 (0.48–2.39) | 0.873 | 4.26 (1.06–17.07) | 0.041 | 7.97 (1.55–41.00) | 0.013 | ||
| NLR 1 >13.24 vs. <13.24 | 3.16 (1.18–8.50) | 0.022 | 1.17 (0.14–9.52) | 0.882 | ||||
| MLR 1 >0.63 vs. <0.63 | 0.66 (0.29–1.51) | 0.325 | 0.40 (0.15–1.03) | 0.058 | 0.48 (0.10–2.38) | 0.368 | 0.21 (0.04–1.31) | 0.095 |
| PLR 1 >380 vs. <380 | 2.17 (0.95–4.99) | 0.068 | 3.96 (1.46–10.77) | 0.007 | 0.80 (0.20–3.18) | 0.747 | ||
| SII 1 >2730 vs. <2730 | 3.25 (1.27–8.28) | 0.014 | 1.33 (0.16–10.81) | 0.790 | ||||
| Prognostic Factors | OS HPV− | DFS HPV− | OS HPV+ | DFS HPV+ |
|---|---|---|---|---|
| Poor prognostic factors in UVA (before treatment) | Higher CMC Higher PLT Higher MLR | Higher PLT Higher PLR Lower Hb Lower RBC | Higher WBC Higher NLR Higher SII Lower Ret | Higher NLR Higher SII Lower CLC Lower CMC |
| Poor prognostic factors in MVA (before treatment) | Higher CMC Higher MLR Higher PLR | Higher PLR Lower RBC Lower MLR | Higher CMC Higher SII | Higher Hb Lower RBC Lower CLC |
| Poor prognostic factors in UVA (after treatment) | Higher PLR Higher SII Lower Hb | Higher NLR Higher SII Lower Hb Lower RBC | Higher CLC | Higher PLT |
| Poor prognostic factors in MVA (after treatment) | Higher PLT Higher SII Lower RBC Lower WBC | Higher PLR Lower RBC | Higher CLC | Higher PLT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brewczyński, A.; Jabłońska, B.; Mazurek, A.M.; Mrochem-Kwarciak, J.; Mrowiec, S.; Śnietura, M.; Kentnowski, M.; Kołosza, Z.; Składowski, K.; Rutkowski, T. Comparison of Selected Immune and Hematological Parameters and Their Impact on Survival in Patients with HPV-Related and HPV-Unrelated Oropharyngeal Cancer. Cancers 2021, 13, 3256. https://doi.org/10.3390/cancers13133256
Brewczyński A, Jabłońska B, Mazurek AM, Mrochem-Kwarciak J, Mrowiec S, Śnietura M, Kentnowski M, Kołosza Z, Składowski K, Rutkowski T. Comparison of Selected Immune and Hematological Parameters and Their Impact on Survival in Patients with HPV-Related and HPV-Unrelated Oropharyngeal Cancer. Cancers. 2021; 13(13):3256. https://doi.org/10.3390/cancers13133256
Chicago/Turabian StyleBrewczyński, Adam, Beata Jabłońska, Agnieszka Maria Mazurek, Jolanta Mrochem-Kwarciak, Sławomir Mrowiec, Mirosław Śnietura, Marek Kentnowski, Zofia Kołosza, Krzysztof Składowski, and Tomasz Rutkowski. 2021. "Comparison of Selected Immune and Hematological Parameters and Their Impact on Survival in Patients with HPV-Related and HPV-Unrelated Oropharyngeal Cancer" Cancers 13, no. 13: 3256. https://doi.org/10.3390/cancers13133256
APA StyleBrewczyński, A., Jabłońska, B., Mazurek, A. M., Mrochem-Kwarciak, J., Mrowiec, S., Śnietura, M., Kentnowski, M., Kołosza, Z., Składowski, K., & Rutkowski, T. (2021). Comparison of Selected Immune and Hematological Parameters and Their Impact on Survival in Patients with HPV-Related and HPV-Unrelated Oropharyngeal Cancer. Cancers, 13(13), 3256. https://doi.org/10.3390/cancers13133256