
Immunotherapy Discontinuation in Metastatic Melanoma: Lessons from Real-Life Clinical Experience

Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients and Study Design
2.2. Statistical Analysis
2.3. Ethics
3. Results
3.1. Patient and Treatment Characteristics
3.2. Outcome after Treatment Discontinuation
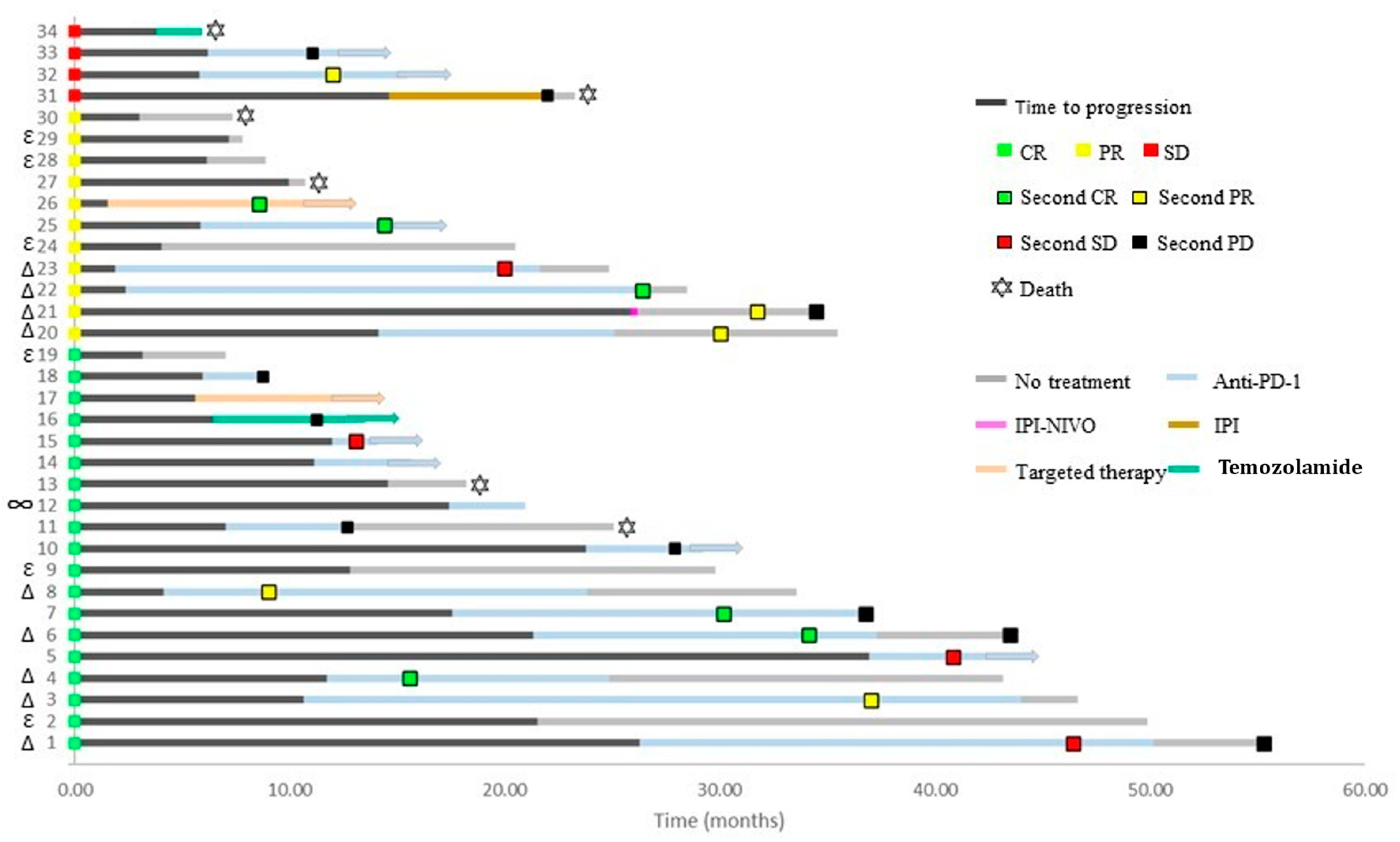
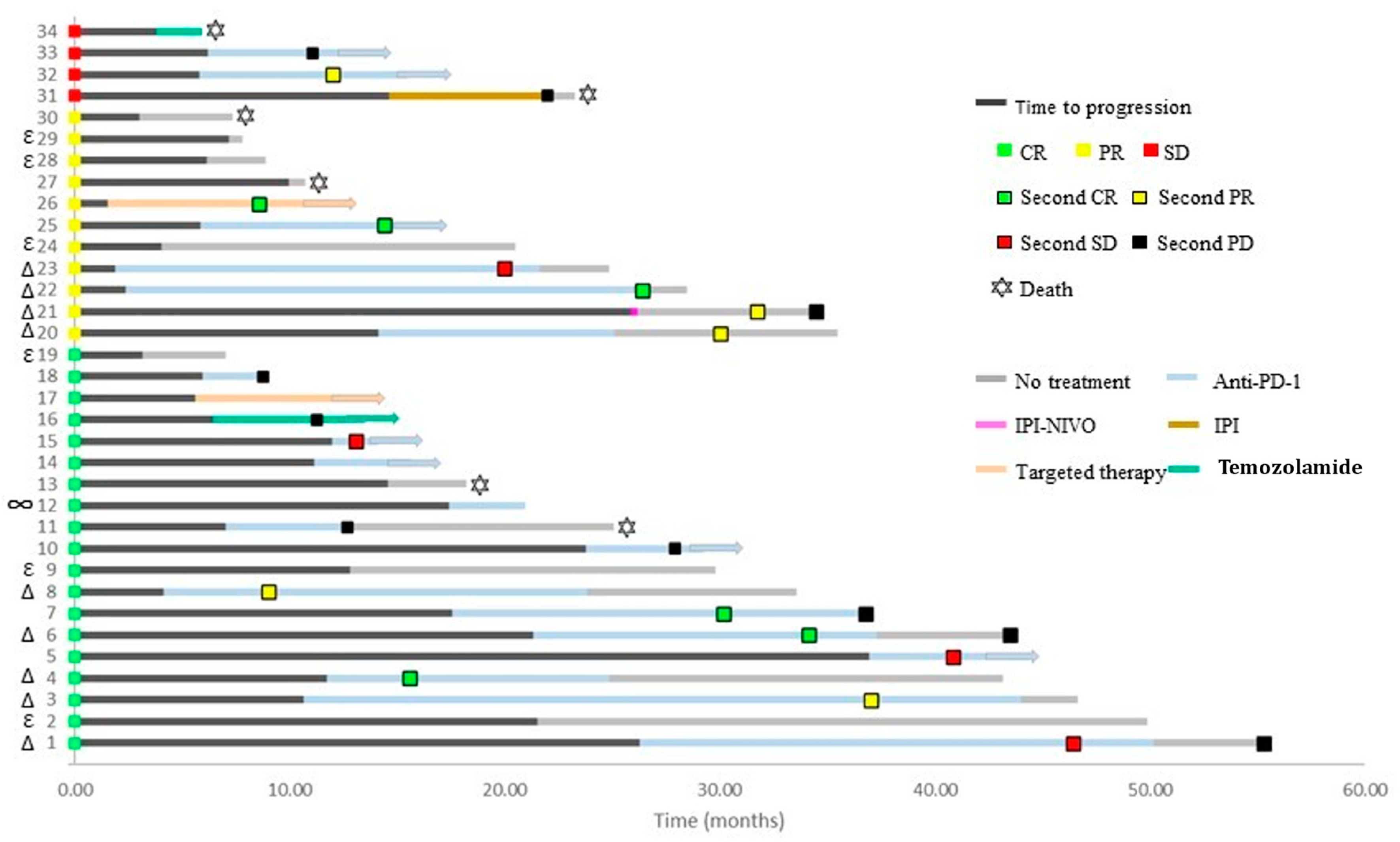
3.3. Treatment Re-Induction
3.4. Factors Associated with Outcome
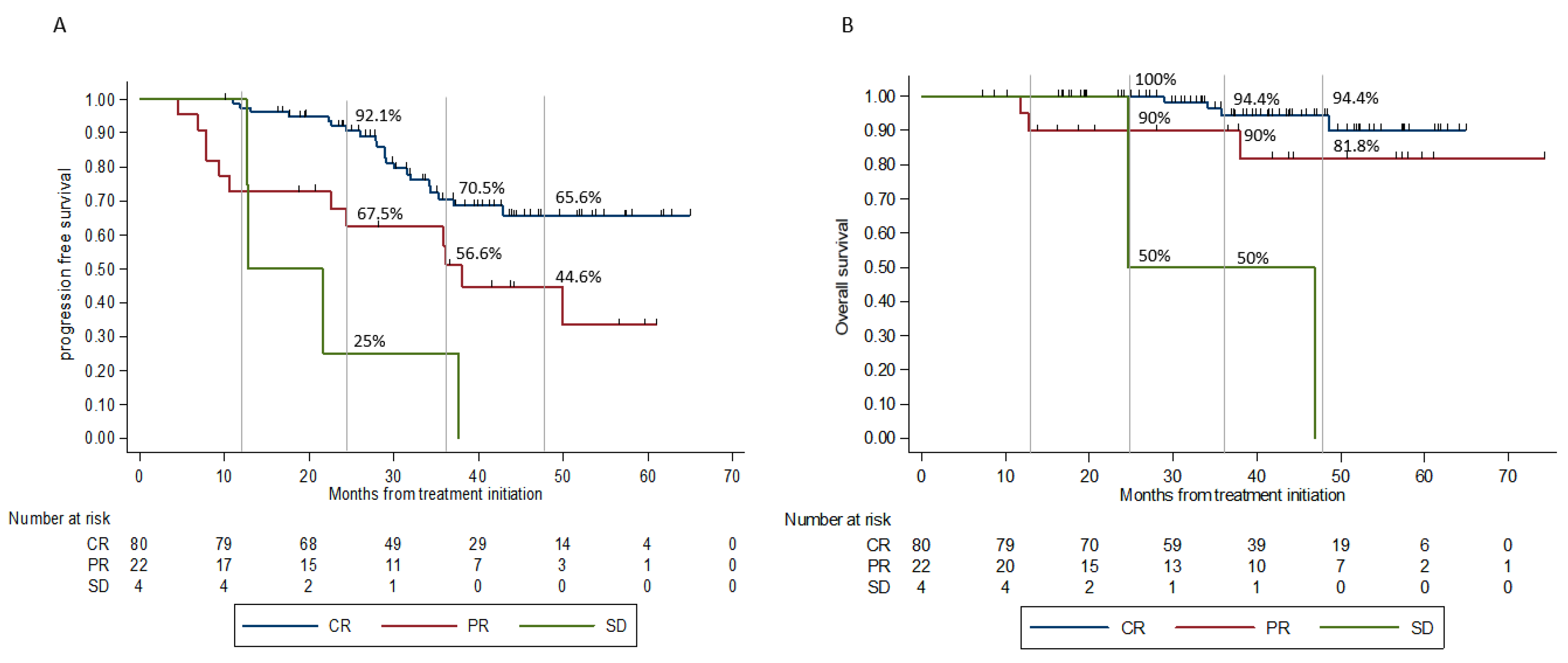
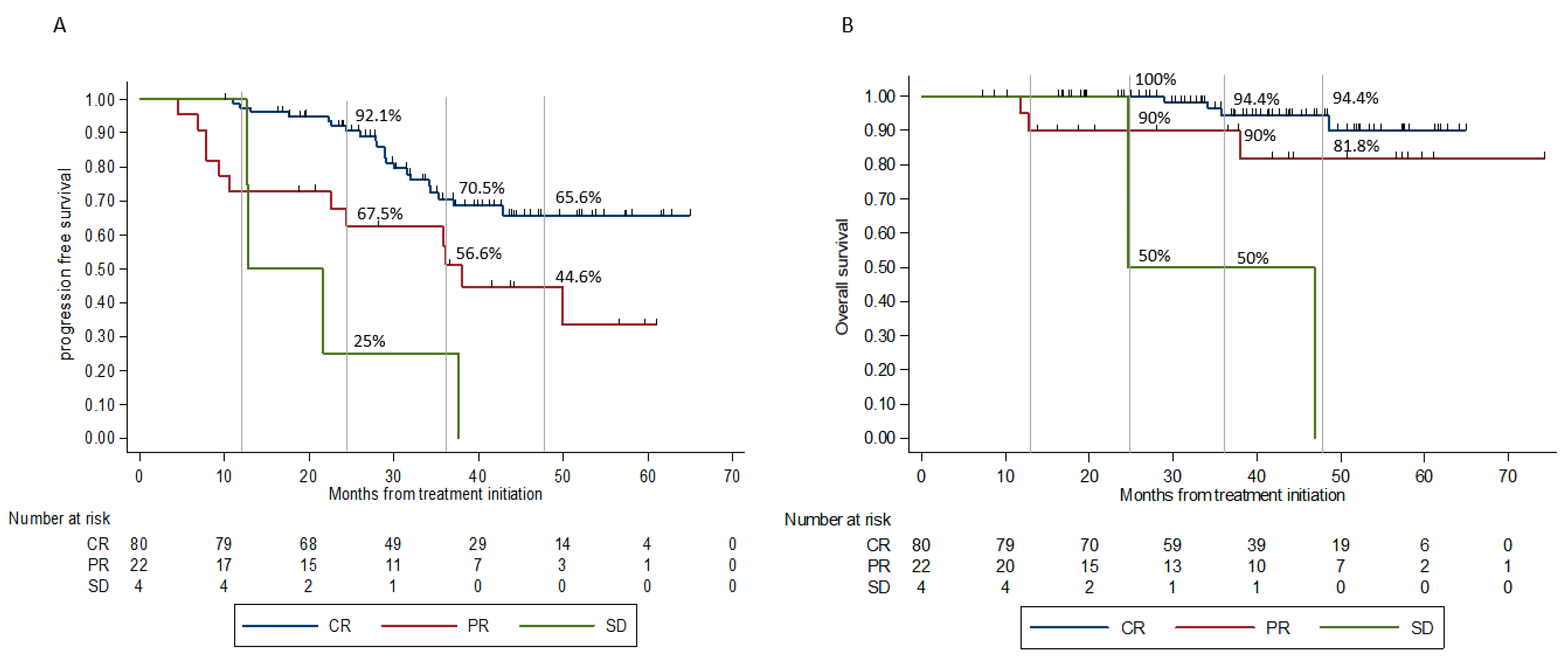
3.4.1. Best Response
3.4.2. Line of Treatment
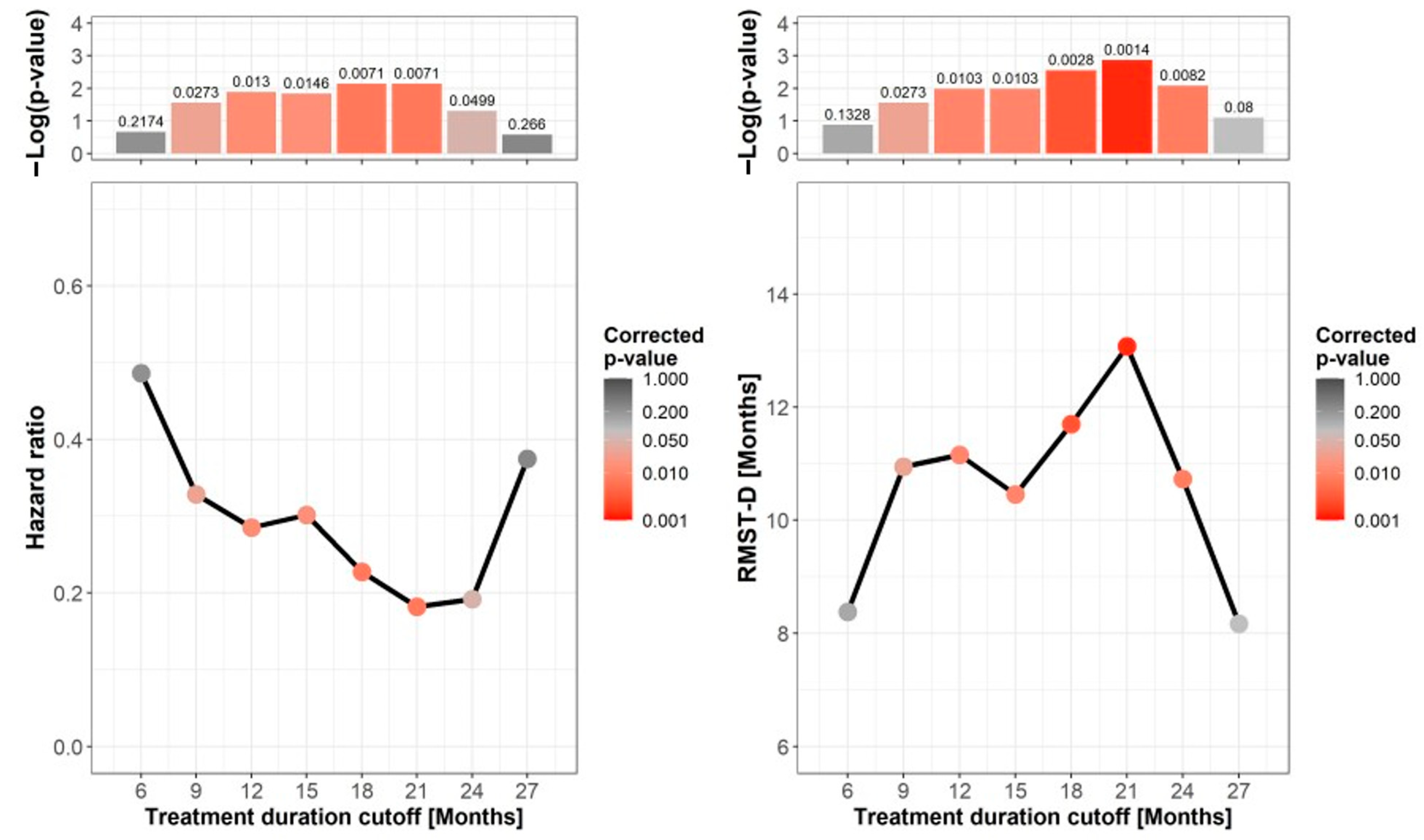
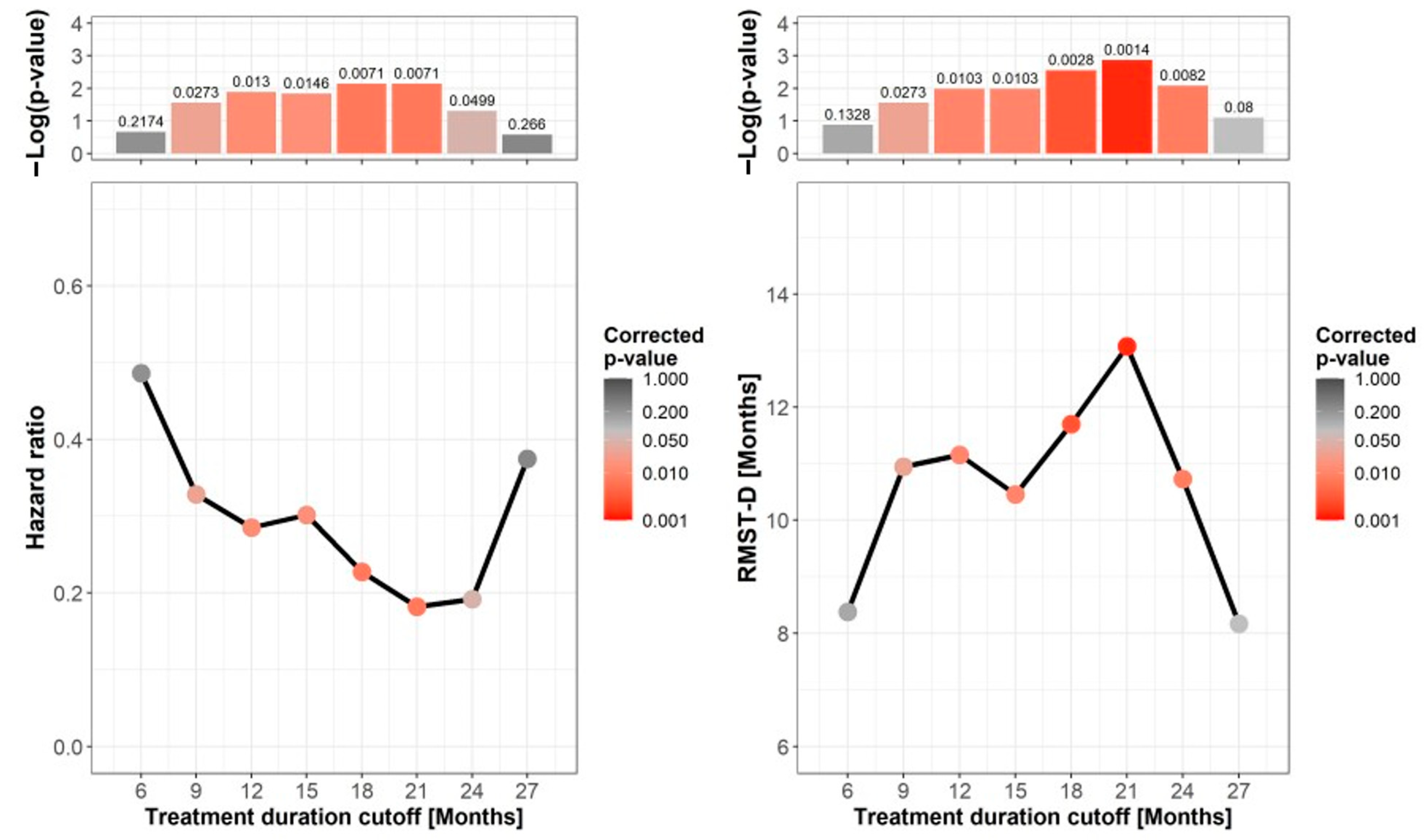
3.4.3. Treatment Duration
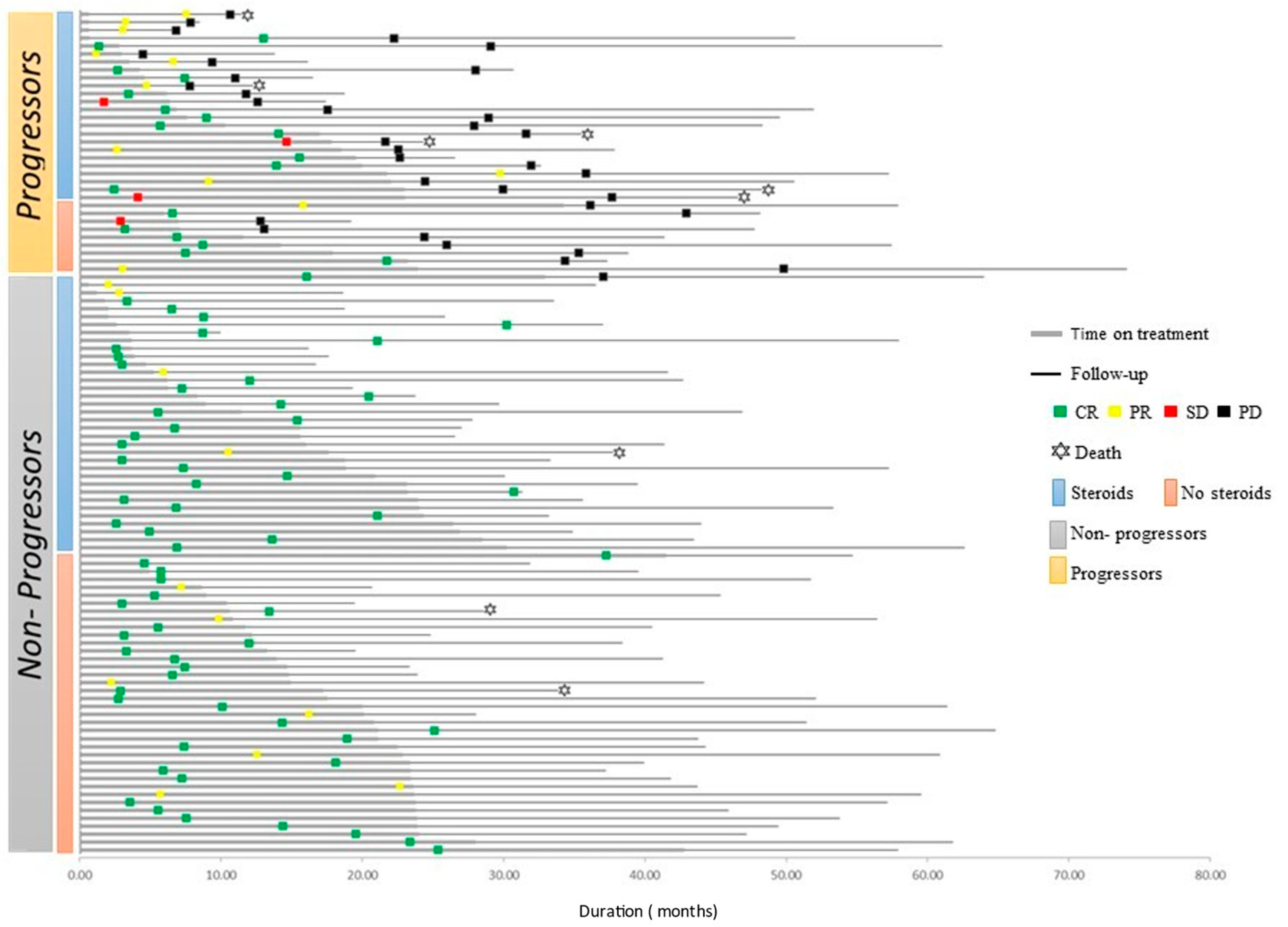
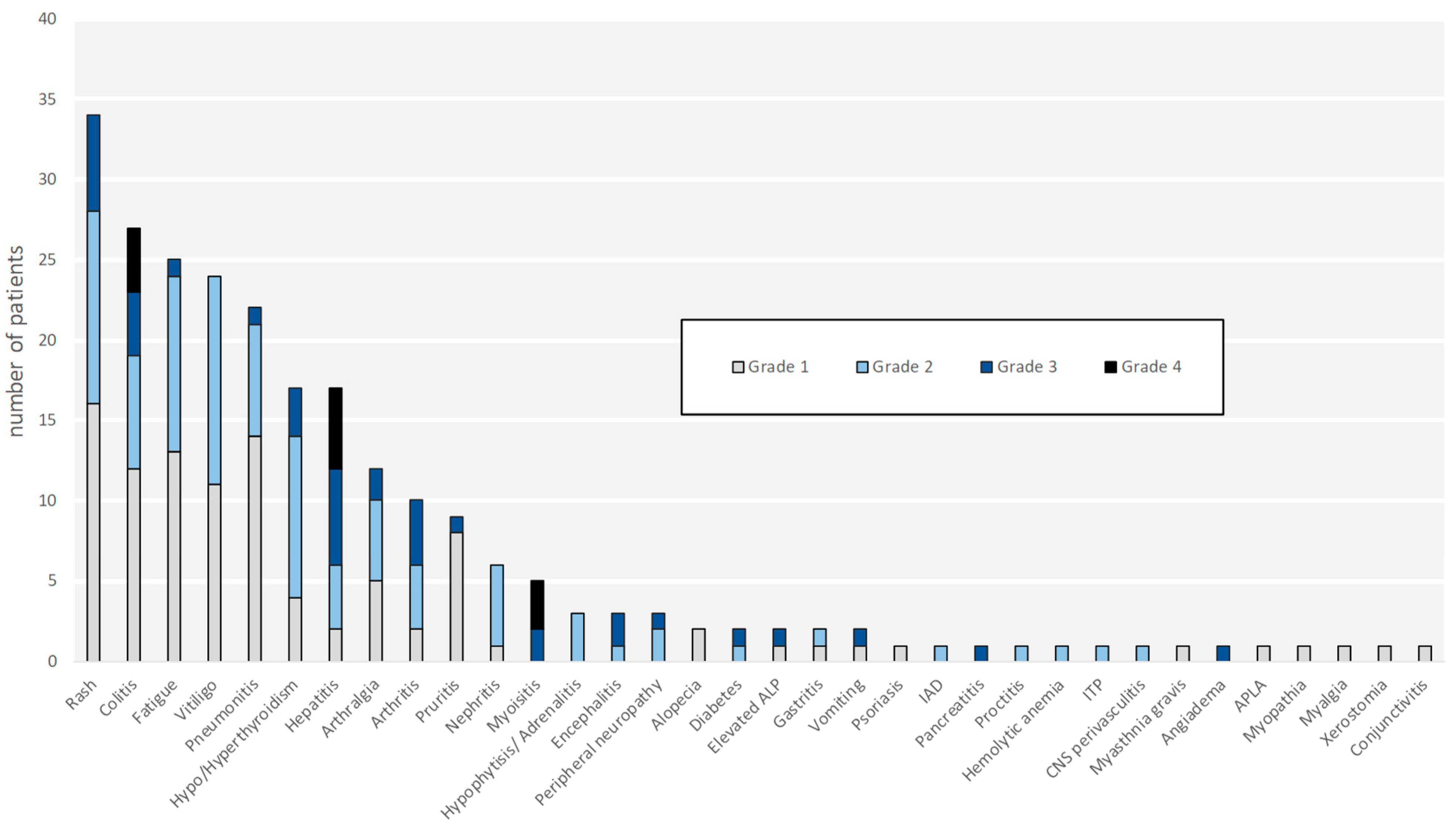
3.4.4. Adverse Events and Steroid Treatment
3.4.5. Multivariate Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Acknowledgments
Conflicts of Interest
References
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Hamid, O.; Robert, C.; Daud, A.; Hodi, F.S.; Hwu, W.J.; Kefford, R.; Wolchok, J.D.; Hersey, P.; Joseph, R.; Weber, J.S.; et al. Five-year survival outcomes for patients with advanced melanoma treated with pembrolizumab in KEYNOTE-001. Ann. Oncol. 2019, 30, 582–588. [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Schachter, J.; Arance, A.; Grob, J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.M.; Lotem, M.; et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): Post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. 2019, 20, 1239–1251. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asher, N.; Ben-Betzalel, G.; Lev-Ari, S.; Shapira-Frommer, R.; Steinberg-Silman, Y.; Gochman, N.; Schachter, J.; Meirson, T.; Markel, G. Real world outcomes of ipilimumab and nivolumab in patients with metastatic melanoma. Cancers 2020, 12, 2329. [Google Scholar] [CrossRef]
- Jansen, Y.J.L.; Rozeman, E.A.; Mason, R.; Goldinger, S.M.; Foppen, M.H.G.; Hoejberg, L.; Schmidt, H.; van Thienen, J.V.; Haanen, J.B.A.G.; Tiainen, L.; et al. Discontinuation of anti-PD-1 antibody therapy in the absence of disease progression or treatment limiting toxicity: Clinical outcomes in advanced melanoma. Ann. Oncol. 2019, 30, 1154–1161. [Google Scholar] [CrossRef] [Green Version]
- Mäkelä, S.; Kohtamäki, L.; Laukka, M.; Juteau, S.; Hernberg, M. Limited-duration anti-PD-1 therapy for patients with metastatic melanoma. Acta Oncol. 2020, 59, 438–443. [Google Scholar] [CrossRef]
- Betof Warner, A.; Palmer, J.S.; Shoushtari, A.N.; Goldman, D.A.; Panageas, K.S.; Hayes, S.A.; Bajwa, R.; Momtaz, P.; Callahan, M.K.; Wolchok, J.D.; et al. Long-term outcomes and responses to retreatment in patients with melanoma treated with PD-1 blockade. J. Clin. Oncol. 2020, 38, 1655–1663. [Google Scholar] [CrossRef]
- Iivanainen, S.; Koivunen, J.P. Early PD-1 therapy discontinuation in responding metastatic cancer patients. Oncology 2019, 96, 125–131. [Google Scholar] [CrossRef]
- Selig, G.N.; Huang, A.C.C.; Karakousis, G.C.; Xu, W.; Zheng, C.; Carberry, M.; Giles, L.; Kreider, K.; McGettigan, S.; Lukens, J.N.; et al. Landmark analysis of immunotherapy duration and disease free survival in advanced melanoma patients with a complete response. J. Clin. Oncol. 2020, 38, 10054, (Abstract). [Google Scholar] [CrossRef]
- Da Silva, I.P.; Ahmed, T.; Lo, S.; Reijers, I.L.M.; Weppler, A.; Warner, A.B.; Patrinely, J.R.; Serra-Bellver, P.; Lebbe, C.; Mangana, J.; et al. Long, ipilimumab (IPI) alone or in combination with anti-PD-1 (IPI+PD1) in patients (pts) with metastatic melanoma (MM) resistant to PD1 monotherapy. J. Clin. Oncol. 2020, 38, 10005, (Abstract). [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Hamid, O.; Daud, A.; Wolchok, J.D.; Joshua, A.M.; Hwu, W.; Weber, J.S.; Gangadhar, T.C.; Joseph, R.W.; et al. Durable complete response after discontinuation of pembrolizumab in patients with metastatic melanoma. J. Clin. Oncol. 2018, 36, 1668–1674. [Google Scholar] [CrossRef]
- Topalian, S.L.; Sznol, M.; McDermott, D.F.; Kluger, H.M.; Carvajal, R.D.; Sharfman, W.H.; Brahmer, J.R.; Lawrence, D.P.; Atkins, M.B.; Powderly, J.D.; et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J. Clin. Oncol. 2014, 32, 1020–1030. [Google Scholar] [CrossRef] [PubMed]
- Schadendorf, D.; Wolchok, J.D.; Hodi, F.S.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.; Cowey, C.L.; Lao, C.D.; Chesney, J.; et al. Efficacy and safety outcomes in patients with advanced melanoma who discontinued treatment with nivolumab and ipilimumab because of adverse events: A pooled analysis of randomized phase II and III trials. J. Clin. Oncol. 2017, 35, 3807–3814. [Google Scholar] [CrossRef] [Green Version]
- Nomura, M.; Otsuka, A.; Kondo, T.; Nagai, H.; Nonomura, Y.; Kaku, Y.; Matsumoto, S.; Muto, M. Efficacy and safety of retreatment with nivolumab in metastatic melanoma patients previously treated with nivolumab. Cancer Chemother. Pharmacol. 2017, 80, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Blasig, H.; Bender, C.; Hassel, J.C.; Eigentler, T.K.; Sachse, M.M.; Hiernickel, J.; Koop, A.; Satzger, I.; Gutzmer, R. Reinduction of PD1-inhibitor therapy: First experience in eight patients with metastatic melanoma. Melanoma Res. 2017, 27, 321–325. [Google Scholar] [CrossRef]
- Long, G.V.; Schachter, J.; Arance, A.; Grob, J.; Mortier, L.; Daud, A.; Carlino, M.S.; Ribas, A.; McNeil, C.M.; Lotem, M.; et al. Long-term survival from pembrolizumab (pembro) completion and pembro retreatment: Phase III KEYNOTE-006 in advanced melanoma. J. Clin. Oncol. 2020, 38, 10013, (Abstract). [Google Scholar] [CrossRef]
- Horiguchi, M.; Uno, H. On permutation tests for comparing restricted mean survival time with small sample from randomized trials. Stat. Med. 2020, 39, 2655–2670. [Google Scholar] [CrossRef]
- Uno, H.; Claggett, B.; Tian, L.; Inoue, E.; Gallo, P.; Miyata, T.; Schrag, D.; Takeuchi, M.; Uyama, Y.; Zhao, L.; et al. Moving beyond the hazard ratio in quantifying the between-group difference in survival analysis. J. Clin. Oncol. 2014, 32, 2380–2385. [Google Scholar] [CrossRef] [PubMed]
- Bomze, D.; Azoulay, D.; Meirson, T. Immunotherapy with programmed cell death 1 vs. programmed cell death ligand 1 inhibitors in patients with cancer. JAMA Oncol. 2020, 6, 1114–1115. [Google Scholar] [CrossRef] [PubMed]
- Gauci, M.; Lanoy, E.; Champiat, S.; Caramella, C.; Ammari, S.; Aspeslagh, S.; Varga, A.; Baldini, C.; Bahleda, R.; Gazzah, A.; et al. Long-term survival in patients responding to Anti-PD-1/PD-L1 therapy and disease outcome upon treatment discontinuation. Clin. Cancer Res. 2019, 25, 946–956. [Google Scholar] [CrossRef] [Green Version]
- Robert, C.; Marabelle, A.; Herrscher, H.; Caramella, C.; Rouby, P.; Fizazi, K.; Besse, B. Immunotherapy discontinuation—How, and when? Data from melanoma as a paradigm. Nat. Rev. Clin. Oncol. 2020, 17, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Donna, A.K.; Steven, C.A. Chapter 4—Introduction to epidemiology. In Clinical and Translational Science; Academic Press: Cambridge, MA, USA, 2017; pp. 53–69. [Google Scholar]
- Indini, A.; di Guardo, L.; Cimminiello, C.; Prisciandaro, M.; Randon, G.; de Braud, F.; del Vecchio, M. Immune-related adverse events correlate with improved survival in patients undergoing anti-PD1 immunotherapy for metastatic melanoma. J. Cancer Res. Clin. Oncol. 2019, 145, 511–521. [Google Scholar] [CrossRef] [PubMed]
- Dupont, R.; Bérard, E.; Puisset, F.; Comont, T.; Delord, J.-P.; Guimbaud, R.; Meyer, N.; Mazieres, J.; Alric, L. The prognostic impact of immune-related adverse events during anti-PD1 treatment in melanoma and non-small-cell lung cancer: A real-life retrospective study. Oncoimmunology 2020, 9, 1682383. [Google Scholar] [CrossRef] [Green Version]
- Pan, E.Y.; Merl, M.Y.; Lin, K. The impact of corticosteroid use during anti-PD1 treatment. J. Oncol. Pharm. Pract. 2020, 26, 814–822. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Kim, M.S.; Kasumova, G.; Chen, T.; Cohen, J.V.; Lawrence, D.P.; Freedman, C.; Fadden, R.; Rubin, K.M.; Sharova, T.; et al. Predictable early onset high-dose-glucocorticoid-associated-irAE and its predictive role in anti-PD-1 monotherapy treated advanced melanoma patients. J. Clin. Oncol. 2019, 37, 9544, (Abstract). [Google Scholar] [CrossRef]
- Weber, J.S.; Hodi, F.S.; Wolchok, J.D.; Topalian, S.L.; Schadendorf, D.; Larkin, J.; Sznol, M.; Long, G.V.; Li, H.; Waxman, I.M.; et al. Safety profile of nivolumab monotherapy: A pooled analysis of patients with advanced melanoma. J. Clin. Oncol. 2017, 35, 785–792. [Google Scholar] [CrossRef]
- Tikkanen, A.; Iivanainen, S.; Koivunen, J.P. Treatment discontinuation and re-initiation of anti-PD-(L)1 agents in metastatic cancers. J. Cancer Res. Clin. Oncol. 2020, 146, 2153–2160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ladwa, R.; Atkinson, V. The cessation of anti-PD-1 antibodies of complete responders in metastatic melanoma. Melanoma Res. 2017, 27, 168–170. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | All Patients (n = 106) | No Progression (n = 72) | Progression (n = 34) | p-Value |
|---|---|---|---|---|
| Age (median, range) | 63.25 (11.4–88.6) | 60.15 (11.4–88.6) | 65.5 (27–82.7) | 0.085 |
| Male (%) | 67 (63.2) | 49 (68.1) | 18 (52.9) | 0.132 |
| BRAF (%) | ||||
| V600 mutant | 27 (25.5) | 19 (26.4) | 8 (23.5) | |
| WT | 70 (66.04) | 46 (63.9) | 24 (70.6) | 0.662 |
| unknown | 9 (8.5) | 7 (9.7) | 2 (5.9) | 0.669 |
| Metastatic upfront | 27 (25.5) | 15 (20.8) | 12 (35.3) | |
| Systemic recurrent disease | 79 (74.5) | 57 (79.2) | 22 (64.7) | 0.111 |
| Primary melanoma (n = 79) | ||||
| Breslow (median, range) | 2.8 (0.2–18) | 2.8 (0.25–18) | 2.55 (0.2–17) | 0.834 |
| Ulceration (%) | 32 (51.6) | 23 (58.9) | 9 (39.1) | 0.131 |
| LDH (%) | ||||
| ≤UNL | 66 (62.3) | 47 (65.3) | 19 (55.9) | |
| >UNL | 21 (19.8) | 15 (20.8) | 6 (17.6) | 0.985 |
| unknown | 19 (17.9) | 10 (13.9) | 9 (26.5) | 0.134 |
| AJCC 8th edition, (%) | ||||
| M1a | 37 (34.9) | 26 (36.1) | 11 (32.3) | |
| M1b | 34 (32.1) | 25 (34.7) | 9 (26.5) | 0.76 |
| M1c | 28 (26.4) | 16 (22.2) | 12 (35.3) | 0.275 |
| M1d | 7 (6.6) | 5 (6.9) | 2 (5.8) | 0.951 |
| Number of disease sites (mean ± sd) | 1.97 ± 1.08 | 1.87 ± 1.09 | 2.17 ± 1.03 | 0.181 |
| ECOG PS 0–1 (%) | 100 (94.3) | 68 (94.4) | 32 (94.1) | 0.224 |
| Treatment Characteristics | ||||
| Regimen (%) | ||||
| Ipi-Nivo | 20 (18.9) | 11 (15.2) | 9 (26.5) | |
| Anti-PD-1 | 86 (81.1) | 61 (84.7) | 25 (73.5) | 0.169 |
| Nivolumab | 31 (29.3) | 23 (31.9) | 8 (23.5) | - |
| pembrolizumab | 55 (51.9) | 38 (52.8) | 17 (50) | - |
| Line of treatment (%) | 0.027 | |||
| 1st | 80 (75.5) | 59 (82) | 21 (61.8) | |
| Advanced * | 26 (24.5) | 13 (18) | 13 (38.2) | |
| Time on treatment, months (median, range) | 15.2 (0.7–42.8) | 15.8 (0.7–42.8) | 8.9 (0.7–34.3) | 0.075 |
| CR | 15.5 (0.7–42.8) | 16.0 (1.8–42.8) | 10.3 (0.72–32.9) | 0.1 |
| PR † | 12.9 (0.7–34.3) | 14.9 (0.69–23.7) | 4.8 (0.69–34.3) | 0.75 |
| SD ℇ | 12.4 (6.4–23) | - | 12.4 (6.4–23) | - |
| Best response (%) | ||||
| CR | 80 (75.5) | 61 (84.7) | 19 (55.9) | |
| PR | 22 (20.7) | 11 (15.3) | 11 (32.3) | 0.02 |
| SD | 4 (3.8) | 0 | 4 (11.8) | - |
| Patients with treatment limiting toxicity, n = 60 (%) | ||||
| CR | 42 (70) | 29 (85.3) | 13 (50) | |
| Non-CR | 18 (30) | 5 (14.7) | 13 (50) | 0.005 |
| Onset of 1st irAE, weeks (median, range), n = 99 | 7.6 (0.14–104) | 8.14 (0.14–104) | 5.86 (0.14–68.14) | 0.206 |
| irAEs G3–4 (%) | 38 (35.8) | 22 (30.6) | 16 (47) | 0.049 |
| Exposure to steroids (>10 mg) (%) | 60 (56.6) | 35 (48.6) | 25 (73.5) | 0.018 |
| Duration of steroid exposure (median, range) | 22.3 (1.5–230) | 14.5 (1.5–143.7) | 26.5 (3–230) | 0.256 |
| prednisolone equivalent-dose | 0.726 | |||
| >2 mg/kg | 4 (6.7) | 2 (5.7) | 2 (8) | |
| ≤2 mg/kg | 56 (93.3) | 33 (94.3) | 23 (92) |
| Variable | Hazard Ratio | p-Value | 95% Confidence Interval |
|---|---|---|---|
| Best tumor response | 2.46 | <0.001 | 1.48–4.07 |
| Line of treatment | 2.20 | 0.042 | 1.03–4.70 |
| Treatment duration | 0.98 | <0.001 | 0.97–0.99 |
| High-grade adverse events | 0.85 | 0.702 | 0.37–1.95 |
| Exposure to steroids | 2.16 | 0.085 | 0.90–5.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asher, N.; Israeli-Weller, N.; Shapira-Frommer, R.; Ben-Betzalel, G.; Schachter, J.; Meirson, T.; Markel, G. Immunotherapy Discontinuation in Metastatic Melanoma: Lessons from Real-Life Clinical Experience. Cancers 2021, 13, 3074. https://doi.org/10.3390/cancers13123074
Asher N, Israeli-Weller N, Shapira-Frommer R, Ben-Betzalel G, Schachter J, Meirson T, Markel G. Immunotherapy Discontinuation in Metastatic Melanoma: Lessons from Real-Life Clinical Experience. Cancers. 2021; 13(12):3074. https://doi.org/10.3390/cancers13123074
Chicago/Turabian StyleAsher, Nethanel, Noa Israeli-Weller, Ronnie Shapira-Frommer, Guy Ben-Betzalel, Jacob Schachter, Tomer Meirson, and Gal Markel. 2021. "Immunotherapy Discontinuation in Metastatic Melanoma: Lessons from Real-Life Clinical Experience" Cancers 13, no. 12: 3074. https://doi.org/10.3390/cancers13123074
APA StyleAsher, N., Israeli-Weller, N., Shapira-Frommer, R., Ben-Betzalel, G., Schachter, J., Meirson, T., & Markel, G. (2021). Immunotherapy Discontinuation in Metastatic Melanoma: Lessons from Real-Life Clinical Experience. Cancers, 13(12), 3074. https://doi.org/10.3390/cancers13123074