
Optimizing External Beam Radiotherapy as per the Risk Group of Localized Prostate Cancer: A Nationwide Multi-Institutional Study (KROG 18-15)

 , , , , ,
, , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Treatment and Follow-Up
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
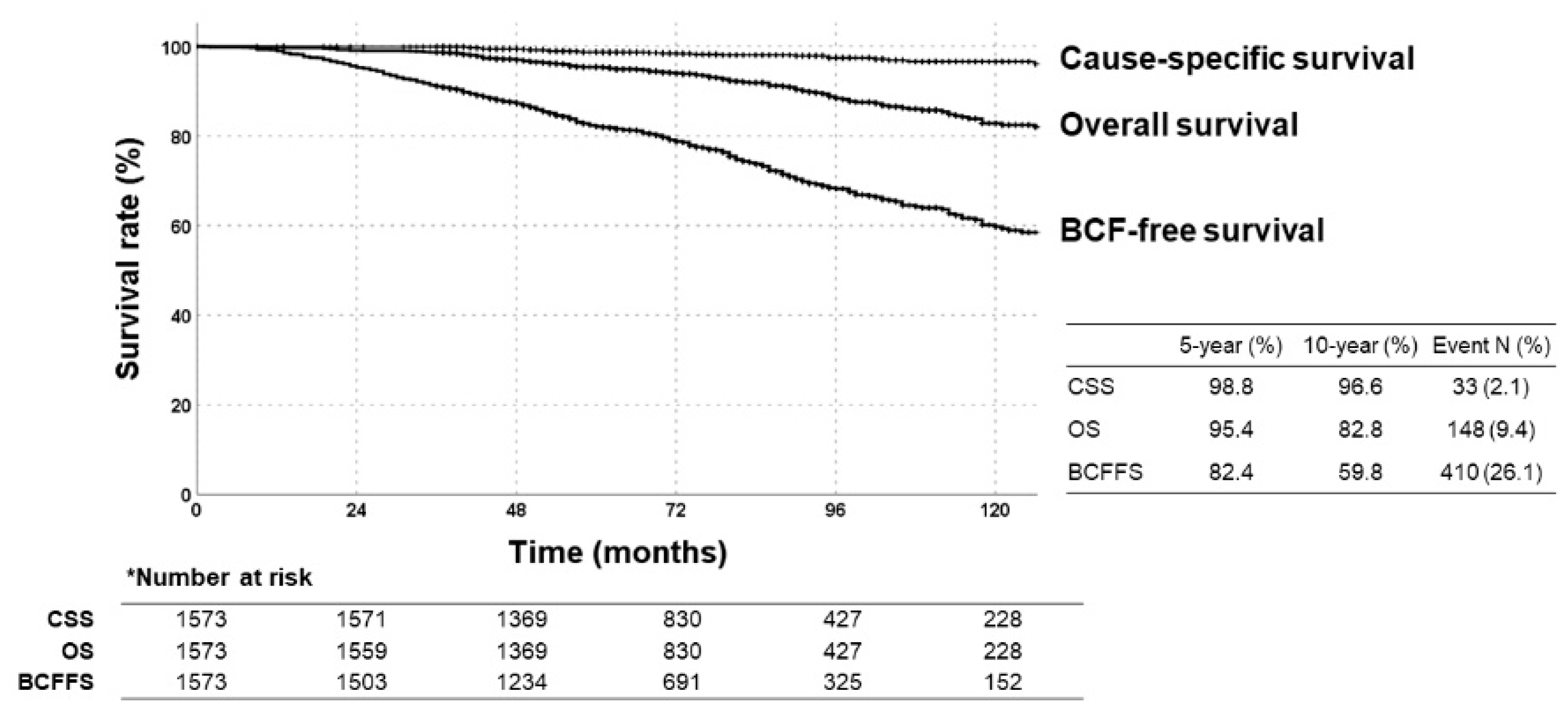
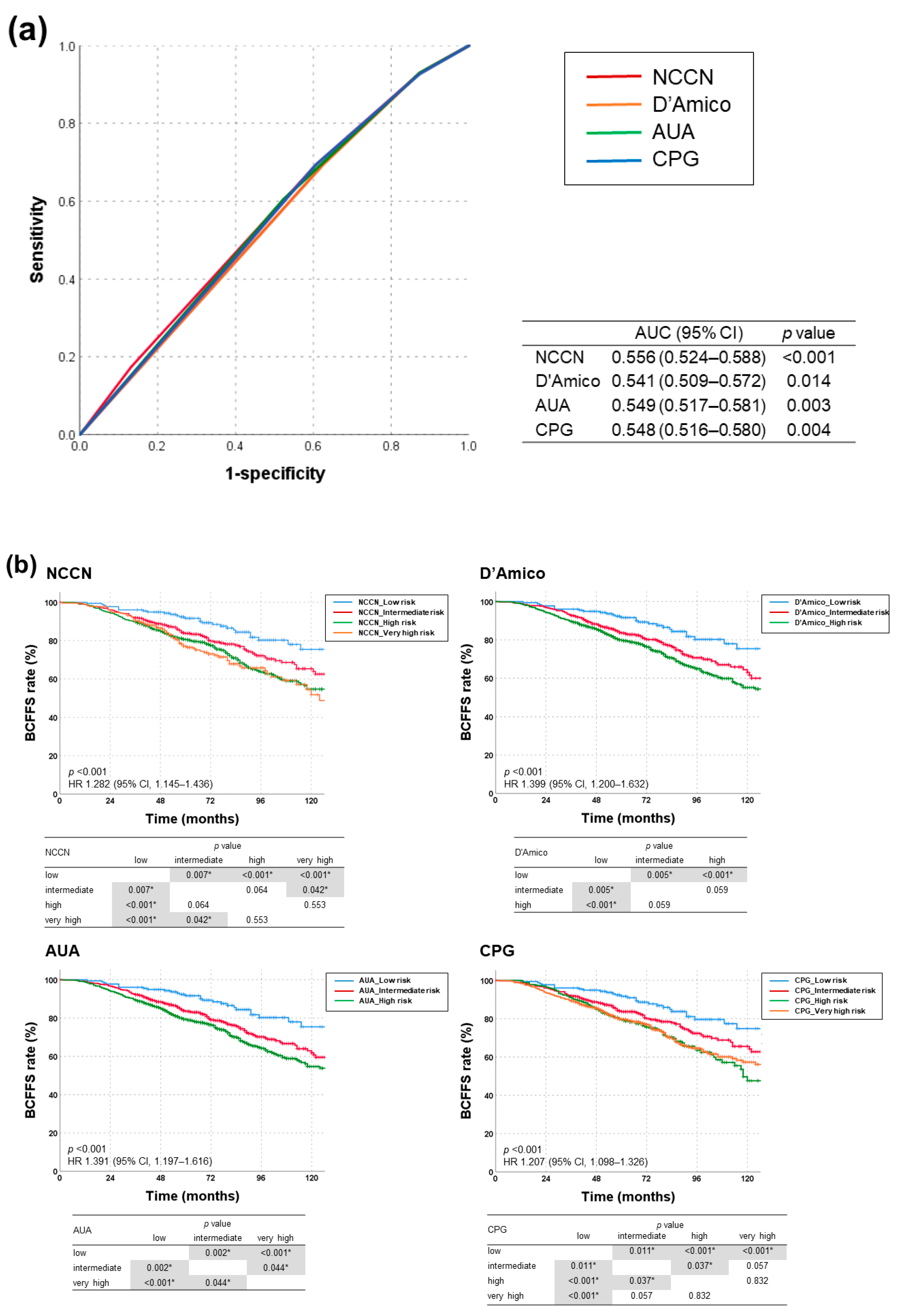
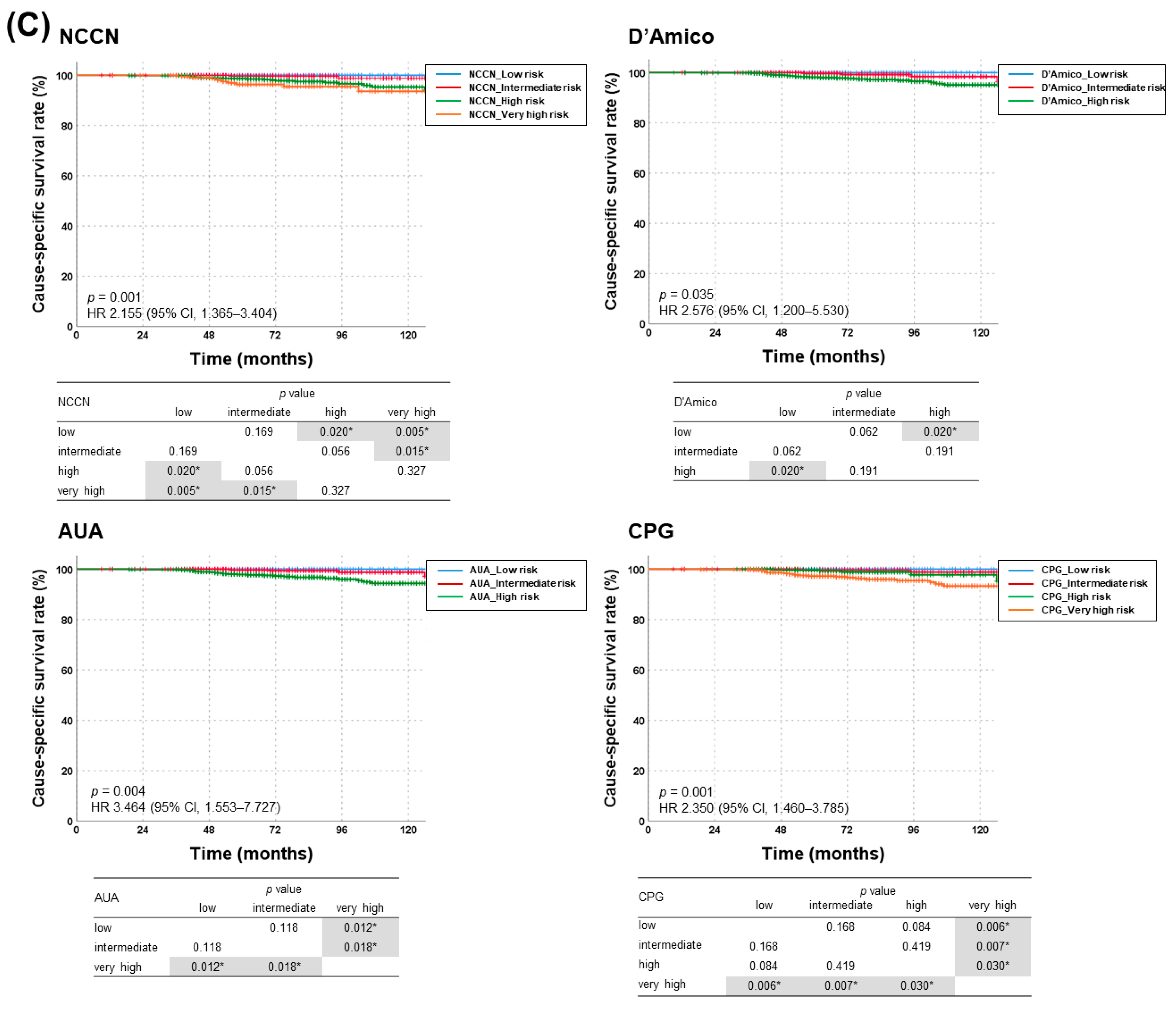
3.2. Treatment Outcomes and Risk Stratification
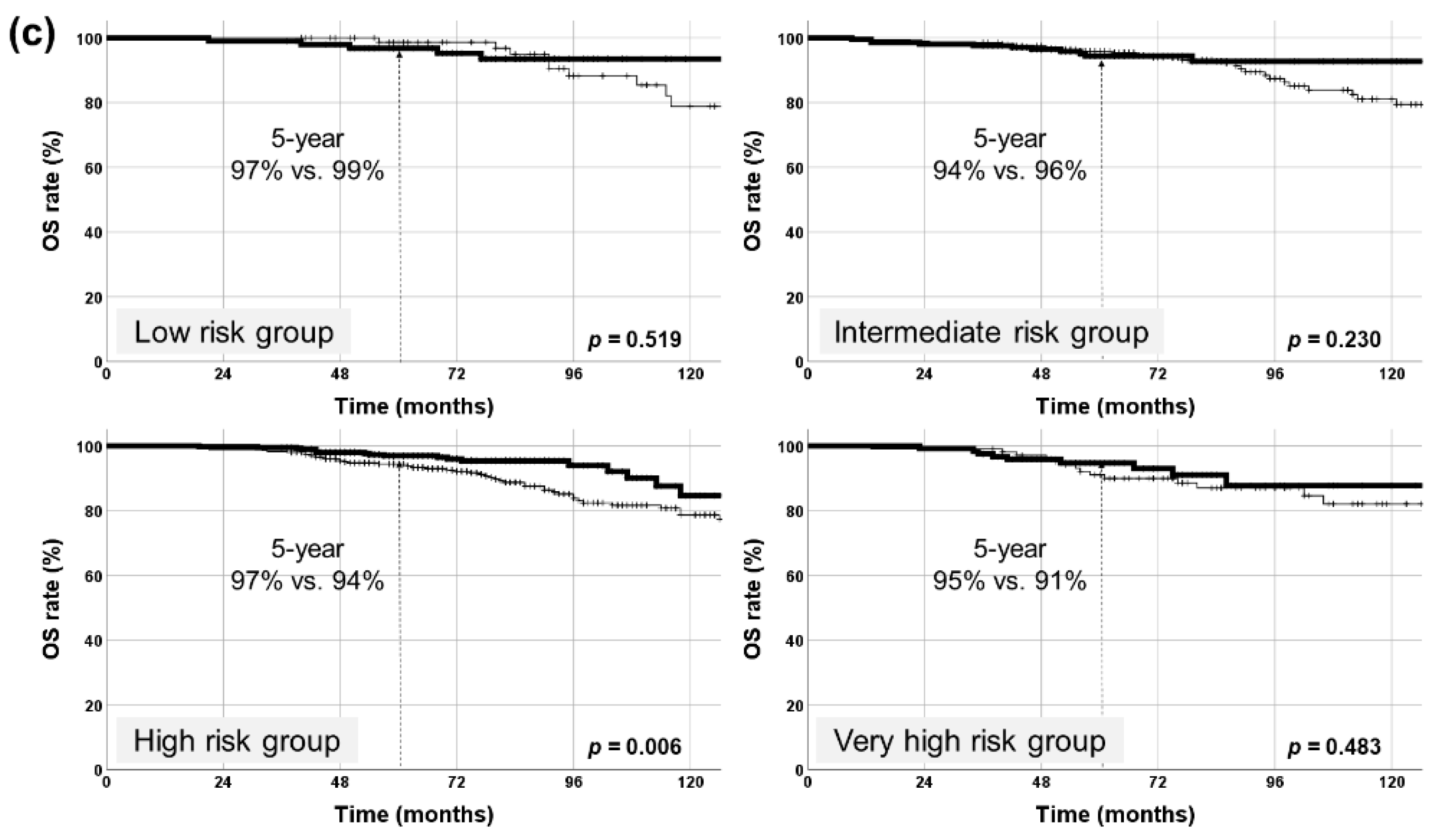
3.3. Prognostic Factors in Each NCCN Risk Group
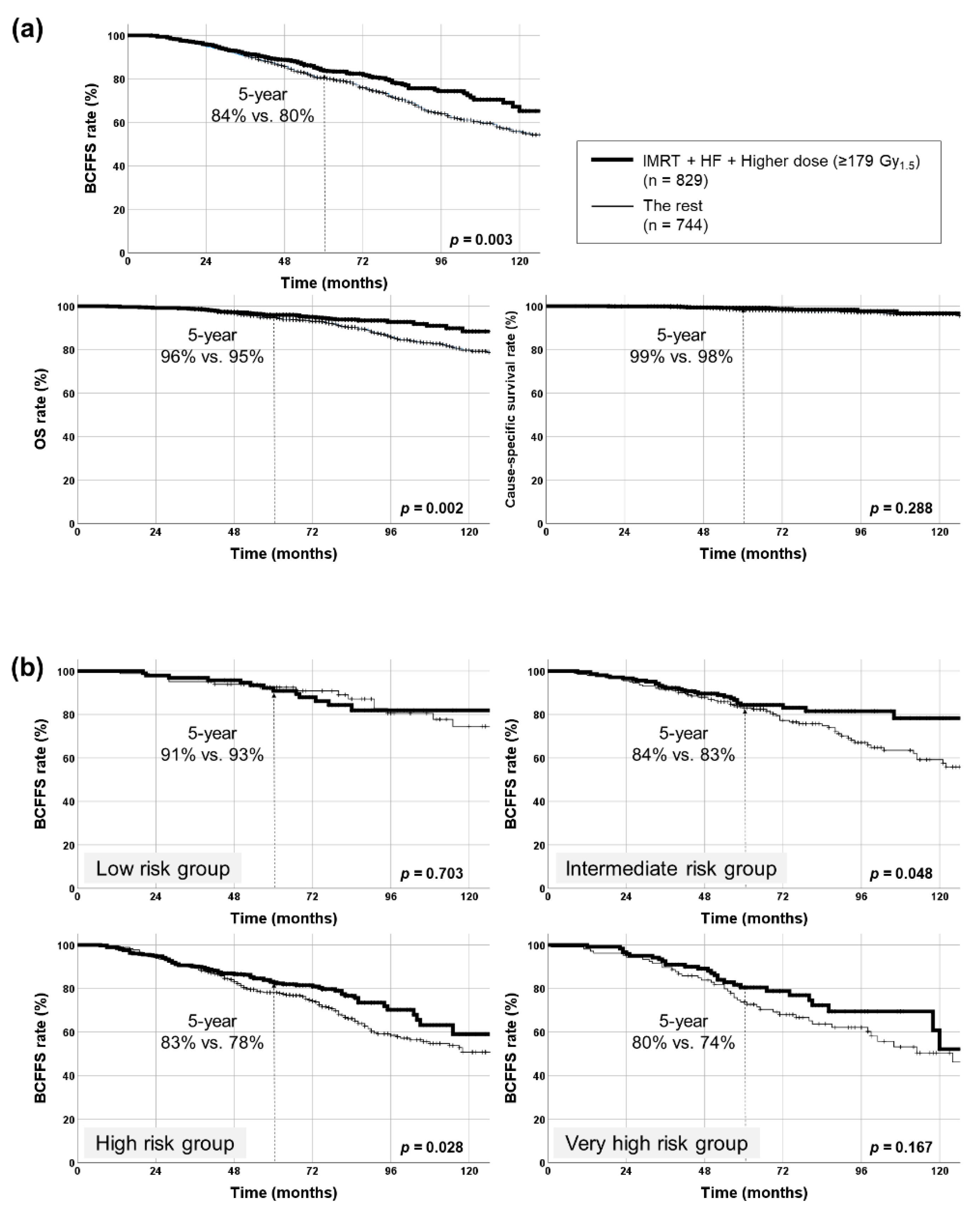
3.4. Radiotherapy-Related Factors
3.5. Toxicities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Roach, M., 3rd; Ceron Lizarraga, T.L.; Lazar, A.A. Radical prostatectomy versus radiation and androgen deprivation therapy for clinically localized prostate cancer: How good is the evidence? Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 1064–1070. [Google Scholar] [CrossRef]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M.; et al. 10-year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N. Engl. J. Med. 2016, 375, 1415–1424. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef]
- Mohler, J.L.; Antonarakis, E.S.; Armstrong, A.J.; D’Amico, A.V.; Davis, B.J.; Dorff, T.; Eastham, J.A.; Enke, C.A.; Farrington, T.A.; Higano, C.S.; et al. Prostate cancer, version 2.2019, nccn clinical practice guidelines in oncology. J. Natl. Compr. Canc. Netw. 2019, 17, 479–505. [Google Scholar] [CrossRef] [PubMed]
- Sanda, M.G.; Cadeddu, J.A.; Kirkby, E.; Chen, R.C.; Crispino, T.; Fontanarosa, J.; Freedland, S.J.; Greene, K.; Klotz, L.H.; Makarov, D.V.; et al. Clinically localized prostate cancer: Aua/astro/suo guideline. Part i: Risk stratification, shared decision making, and care options. J. Urol. 2018, 199, 683–690. [Google Scholar] [CrossRef] [PubMed]
- Gnanapragasam, V.J.; Lophatananon, A.; Wright, K.A.; Muir, K.R.; Gavin, A.; Greenberg, D.C. Improving clinical risk stratification at diagnosis in primary prostate cancer: A prognostic modelling study. PLoS Med. 2016, 13, e1002063. [Google Scholar] [CrossRef] [PubMed]
- Mottet, N.; Bellmunt, J.; Bolla, M.; Briers, E.; Cumberbatch, M.G.; De Santis, M.; Fossati, N.; Gross, T.; Henry, A.M.; Joniau, S.; et al. Eau-estro-siog guidelines on prostate cancer. Part 1: Screening, diagnosis, and local treatment with curative intent. Eur. Urol. 2017, 71, 618–629. [Google Scholar] [CrossRef] [PubMed]
- Eade, T.N.; Hanlon, A.L.; Horwitz, E.M.; Buyyounouski, M.K.; Hanks, G.E.; Pollack, A. What dose of external-beam radiation is high enough for prostate cancer? Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 682–689. [Google Scholar] [CrossRef]
- Jacob, R.; Hanlon, A.L.; Horwitz, E.M.; Movsas, B.; Uzzo, R.G.; Pollack, A. The relationship of increasing radiotherapy dose to reduced distant metastases and mortality in men with prostate cancer. Cancer 2004, 100, 538–543. [Google Scholar] [CrossRef]
- Pollack, A.; Smith, L.G.; von Eschenbach, A.C. External beam radiotherapy dose response characteristics of 1127 men with prostate cancer treated in the psa era. Int. J. Radiat. Oncol. Biol. Phys. 2000, 48, 507–512. [Google Scholar] [CrossRef]
- Zelefsky, M.J.; Fuks, Z.; Hunt, M.; Lee, H.J.; Lombardi, D.; Ling, C.C.; Reuter, V.E.; Venkatraman, E.S.; Leibel, S.A. High dose radiation delivered by intensity modulated conformal radiotherapy improves the outcome of localized prostate cancer. J. Urol. 2001, 166, 876–881. [Google Scholar] [CrossRef]
- Pollack, A.; Zagars, G.K.; Smith, L.G.; Lee, J.J.; von Eschenbach, A.C.; Antolak, J.A.; Starkschall, G.; Rosen, I. Preliminary results of a randomized radiotherapy dose-escalation study comparing 70 gy with 78 gy for prostate cancer. J. Clin. Oncol. 2000, 18, 3904–3911. [Google Scholar] [CrossRef]
- Kuban, D.A.; Tucker, S.L.; Dong, L.; Starkschall, G.; Huang, E.H.; Cheung, M.R.; Lee, A.K.; Pollack, A. Long-term results of the m. D. Anderson randomized dose-escalation trial for prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Zietman, A.L.; Bae, K.; Slater, J.D.; Shipley, W.U.; Efstathiou, J.A.; Coen, J.J.; Bush, D.A.; Lunt, M.; Spiegel, D.Y.; Skowronski, R.; et al. Randomized trial comparing conventional-dose with high-dose conformal radiation therapy in early-stage adenocarcinoma of the prostate: Long-term results from proton radiation oncology group/american college of radiology 95-09. J. Clin. Oncol. 2010, 28, 1106–1111. [Google Scholar] [CrossRef]
- Zietman, A.L.; DeSilvio, M.L.; Slater, J.D.; Rossi, C.J., Jr.; Miller, D.W.; Adams, J.A.; Shipley, W.U. Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: A randomized controlled trial. JAMA 2005, 294, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Al-Mamgani, A.; van Putten, W.L.; Heemsbergen, W.D.; van Leenders, G.J.; Slot, A.; Dielwart, M.F.; Incrocci, L.; Lebesque, J.V. Update of dutch multicenter dose-escalation trial of radiotherapy for localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 980–988. [Google Scholar] [CrossRef] [PubMed]
- Heemsbergen, W.D.; Al-Mamgani, A.; Slot, A.; Dielwart, M.F.; Lebesque, J.V. Long-term results of the dutch randomized prostate cancer trial: Impact of dose-escalation on local, biochemical, clinical failure, and survival. Radiother. Oncol. 2014, 110, 104–109. [Google Scholar] [CrossRef] [PubMed]
- Beckendorf, V.; Guerif, S.; Le Prise, E.; Cosset, J.M.; Bougnoux, A.; Chauvet, B.; Salem, N.; Chapet, O.; Bourdain, S.; Bachaud, J.M.; et al. 70 gy versus 80 gy in localized prostate cancer: 5-year results of getug 06 randomized trial. Int. J. Radiat. Oncol. Biol. Phys. 2011, 80, 1056–1063. [Google Scholar] [CrossRef]
- Michalski, J.M.; Moughan, J.; Purdy, J.; Bosch, W.; Bruner, D.W.; Bahary, J.P.; Lau, H.; Duclos, M.; Parliament, M.; Morton, G.; et al. Effect of standard vs dose-escalated radiation therapy for patients with intermediate-risk prostate cancer: The nrg oncology rtog 0126 randomized clinical trial. JAMA Oncol. 2018, 4, e180039. [Google Scholar] [CrossRef]
- Sheets, N.C.; Goldin, G.H.; Meyer, A.M.; Wu, Y.; Chang, Y.; Sturmer, T.; Holmes, J.A.; Reeve, B.B.; Godley, P.A.; Carpenter, W.R.; et al. Intensity-modulated radiation therapy, proton therapy, or conformal radiation therapy and morbidity and disease control in localized prostate cancer. JAMA 2012, 307, 1611–1620. [Google Scholar] [PubMed]
- Michalski, J.M.; Yan, Y.; Watkins-Bruner, D.; Bosch, W.R.; Winter, K.; Galvin, J.M.; Bahary, J.P.; Morton, G.C.; Parliament, M.B.; Sandler, H.M. Preliminary toxicity analysis of 3-dimensional conformal radiation therapy versus intensity modulated radiation therapy on the high-dose arm of the radiation therapy oncology group 0126 prostate cancer trial. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 932–938. [Google Scholar] [CrossRef]
- Zelefsky, M.J.; Levin, E.J.; Hunt, M.; Yamada, Y.; Shippy, A.M.; Jackson, A.; Amols, H.I. Incidence of late rectal and urinary toxicities after three-dimensional conformal radiotherapy and intensity-modulated radiotherapy for localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1124–1129. [Google Scholar] [CrossRef]
- Brenner, D.J.; Hall, E.J. Fractionation and protraction for radiotherapy of prostate carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 1095–1101. [Google Scholar] [CrossRef]
- Morgan, S.C.; Hoffman, K.; Loblaw, D.A.; Buyyounouski, M.K.; Patton, C.; Barocas, D.; Bentzen, S.; Chang, M.; Efstathiou, J.; Greany, P.; et al. Hypofractionated radiation therapy for localized prostate cancer: An astro, asco, and aua evidence-based guideline. J. Clin. Oncol. 2018. [Google Scholar] [CrossRef] [PubMed]
- Web-R. Available online: http://web-r.org/ (accessed on 31 May 2021).
- Zelic, R.; Garmo, H.; Zugna, D.; Stattin, P.; Richiardi, L.; Akre, O.; Pettersson, A. Predicting prostate cancer death with different pretreatment risk stratification tools: A head-to-head comparison in a nationwide cohort study. Eur. Urol. 2020, 77, 180–188. [Google Scholar] [CrossRef]
- Lee, W.R.; Dignam, J.J.; Amin, M.B.; Bruner, D.W.; Low, D.; Swanson, G.P.; Shah, A.B.; D’Souza, D.P.; Michalski, J.M.; Dayes, I.S.; et al. Randomized phase iii noninferiority study comparing two radiotherapy fractionation schedules in patients with low-risk prostate cancer. J. Clin. Oncol. 2016, 34, 2325–2332. [Google Scholar] [CrossRef]
- Catton, C.N.; Lukka, H.; Gu, C.S.; Martin, J.M.; Supiot, S.; Chung, P.W.M.; Bauman, G.S.; Bahary, J.P.; Ahmed, S.; Cheung, P.; et al. Randomized trial of a hypofractionated radiation regimen for the treatment of localized prostate cancer. J. Clin. Oncol. 2017, 35, 1884–1890. [Google Scholar] [CrossRef]
- Dearnaley, D.; Syndikus, I.; Mossop, H.; Khoo, V.; Birtle, A.; Bloomfield, D.; Graham, J.; Kirkbride, P.; Logue, J.; Malik, Z.; et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 chhip trial. Lancet Oncol. 2016, 17, 1047–1060. [Google Scholar] [CrossRef]
- Pollack, A.; Walker, G.; Horwitz, E.M.; Price, R.; Feigenberg, S.; Konski, A.A.; Stoyanova, R.; Movsas, B.; Greenberg, R.E.; Uzzo, R.G.; et al. Randomized trial of hypofractionated external-beam radiotherapy for prostate cancer. J. Clin. Oncol. 2013, 31, 3860–3868. [Google Scholar] [CrossRef] [PubMed]
- Hickey, B.E.; James, M.L.; Daly, T.; Soh, F.Y.; Jeffery, M. Hypofractionation for clinically localized prostate cancer. Cochrane Database Syst. Rev. 2019, 9, CD011462. [Google Scholar] [CrossRef] [PubMed]
- Avkshtol, V.; Ruth, K.J.; Ross, E.A.; Hallman, M.A.; Greenberg, R.E.; Price, R.A., Jr.; Leachman, B.; Uzzo, R.G.; Ma, C.; Chen, D.; et al. Ten-year update of a randomized, prospective trial of conventional fractionated versus moderate hypofractionated radiation therapy for localized prostate cancer. J. Clin. Oncol. 2020, 38, 1676–1684. [Google Scholar] [CrossRef] [PubMed]
- Aluwini, S.; Pos, F.; Schimmel, E.; van Lin, E.; Krol, S.; van der Toorn, P.P.; de Jager, H.; Dirkx, M.; Alemayehu, W.G.; Heijmen, B.; et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with prostate cancer (hypro): Acute toxicity results from a randomised non-inferiority phase 3 trial. Lancet Oncol. 2015, 16, 274–283. [Google Scholar] [CrossRef]
- Bruner, D.W.; Pugh, S.L.; Lee, W.R.; Hall, W.A.; Dignam, J.J.; Low, D.; Swanson, G.P.; Shah, A.B.; Malone, S.; Michalski, J.M.; et al. Quality of life in patients with low-risk prostate cancer treated with hypofractionated vs conventional radiotherapy: A phase 3 randomized clinical trial. JAMA Oncol. 2019, 5, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Incrocci, L.; Wortel, R.C.; Alemayehu, W.G.; Aluwini, S.; Schimmel, E.; Krol, S.; van der Toorn, P.P.; Jager, H.; Heemsbergen, W.; Heijmen, B.; et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with localised prostate cancer (hypro): Final efficacy results from a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2016, 17, 1061–1069. [Google Scholar] [CrossRef]
- Widmark, A.; Gunnlaugsson, A.; Beckman, L.; Thellenberg-Karlsson, C.; Hoyer, M.; Lagerlund, M.; Kindblom, J.; Ginman, C.; Johansson, B.; Bjornlinger, K.; et al. Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the hypo-rt-pc randomised, non-inferiority, phase 3 trial. Lancet 2019, 394, 385–395. [Google Scholar] [CrossRef]
- Brand, D.H.; Tree, A.C.; Ostler, P.; van der Voet, H.; Loblaw, A.; Chu, W.; Ford, D.; Tolan, S.; Jain, S.; Martin, A.; et al. Intensity-modulated fractionated radiotherapy versus stereotactic body radiotherapy for prostate cancer (pace-b): Acute toxicity findings from an international, randomised, open-label, phase 3, non-inferiority trial. Lancet Oncol. 2019, 20, 1531–1543. [Google Scholar] [CrossRef]
- King, C.R.; Freeman, D.; Kaplan, I.; Fuller, D.; Bolzicco, G.; Collins, S.; Meier, R.; Wang, J.; Kupelian, P.; Steinberg, M.; et al. Stereotactic body radiotherapy for localized prostate cancer: Pooled analysis from a multi-institutional consortium of prospective phase ii trials. Radiother. Oncol. 2013, 109, 217–221. [Google Scholar] [CrossRef]
- Lehrer, E.J.; Kishan, A.U.; Yu, J.B.; Trifiletti, D.M.; Showalter, T.N.; Ellis, R.; Zaorsky, N.G. Ultrahypofractionated versus hypofractionated and conventionally fractionated radiation therapy for localized prostate cancer: A systematic review and meta-analysis of phase iii randomized trials. Radiother. Oncol. 2020, 148, 235–242. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. | % | |
|---|---|---|---|
| Age (year) | Median 73 (30–90) | ||
| ≤70 | 592 | 39.9 | |
| >70 | 981 | 60.1 | |
| Treatment year | 2005 | 53 | 3.4 |
| 2006 | 101 | 6.4 | |
| 2007 | 143 | 9.1 | |
| 2008 | 125 | 7.9 | |
| 2009 | 95 | 6.0 | |
| 2010 | 132 | 8.4 | |
| 2011 | 161 | 10.2 | |
| 2012 | 200 | 12.7 | |
| 2013 | 205 | 13.0 | |
| 2014 | 199 | 12.7 | |
| 2015 | 155 | 9.9 | |
| 2016 | 4 | 0.3 | |
| T stage | T1 | 216 | 12.1 |
| T2 | 680 | 39.6 | |
| T3 | 618 | 42.7 | |
| T4 | 56 | 5.4 | |
| Tx | 3 | 0.3 | |
| Gleason score | Median 7 (2–10) | ||
| ≤6 | 464 | 29.6 | |
| 7 | 515 | 32.7 | |
| 8 | 346 | 22.0 | |
| ≥9 | 241 | 15.3 | |
| Unknown | 7 | 0.4 | |
| Initial PSA (ng/mL) | Median 26.3 (0.03–535.0) | ||
| <10 | 674 | 43.1 | |
| 10~20 | 366 | 23.4 | |
| >20 | 525 | 33.5 | |
| NCCN risk group | Low | 177 | 9.8 |
| Intermediate | 408 | 22.9 | |
| High | 761 | 43.1 | |
| Very high | 227 | 12.9 | |
| D’Amico risk group | Low | 177 | 11.3 |
| Intermediate | 383 | 24.3 | |
| High | 1013 | 64.4 | |
| AUA risk group | Low | 177 | 11.3 |
| Intermediate | 539 | 34.3 | |
| High | 857 | 54.5 | |
| CPG risk group | Low | 178 | 11.3 |
| Intermediate | 407 | 25.9 | |
| High | 366 | 23.3 | |
| Very high | 622 | 39.5 | |
| ADT | No | 543 | 34.5 |
| Before RT | 210 | 13.4 | |
| Before/concurrent RT | 747 | 47.5 | |
| Concurrent RT | 27 | 1.7 | |
| Post-RT | 46 | 2.9 | |
| RT volume | Prostate (±SV) | 1020 | 64.8 |
| Whole pelvis | 534 | 33.9 | |
| Half pelvis | 8 | 0.5 | |
| Unknown | 11 | 0.7 | |
| RT modality | 3D CRT | 378 | 24.0 |
| IMRT | 1119 | 71.1 | |
| Proton therapy | 44 | 2.8 | |
| 3D + IMRT | 21 | 1.3 | |
| Unknown | 11 | 0.7 | |
| RT dose scheme | CF | 692 | 44.0 |
| HF | 738 | 46.9 | |
| Ultra-HF | 143 | 9.1 | |
| Fractional dose (Gy) | Median 2.2 (1.7–7.5) | ||
| Total dose (Gy) | Median 72.6 (35.0–81.0) | ||
| Total dose in BED (Gy1.5) | Median 179.1 (107.3–225.0) | ||
| Variable | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Age (continuous) | 0.995 (0.981–1.008) | 0.430 | ||
| Age (>70 vs. ≤70) | 0.966 (0.793–1.177) | 0.730 | ||
| Age (>60 vs. ≤60) | 0.897 (0.634–1.269) | 0.539 | ||
| T stage | 1.142 (1.015–1.285) | 0.027 | ||
| T3 vs. T1 | 1.434 (1.048–1.961) | 0.024 | ||
| T2, T3, T4 vs. T1 | 1.389 (1.035–1.864) | 0.029 | 0.817 (0.601–1.111) | 0.198 |
| Gleason score | 1.160 (1.071–1.256) | <0.001 | ||
| ≥9 vs. <9 | 1.501 (1.175–1.916) | 0.003 | ||
| ≥9 vs. <6 | 1.783 (1.332–2.386) | <0.001 | 1.359 (1.058–1.746) | 0.016 |
| ≥9 vs. 7–8 | 1.784 (1.333–2.388) | <0.001 | ||
| 7–8 vs. <6 | 1.303 (1.033–1.644) | 0.025 | ||
| initial PSA | 1.004 (1.002–1.006) | <0.001 | ||
| ≥12 vs. <12 | 1.637 (1.343–1.996) | <0.001 | 1.508 (1.227–1.854) | <0.001 |
| ADT combination (Yes vs. No) | 0.744 (0.612–0.905) | 0.003 | ||
| RT volume | ||||
| Prostate ± SV vs. Pelvis | 0.970 (0.866–1.087) | 0.604 | ||
| RT modality | ||||
| IMRT/Proton vs. 3D | 0.719 (0.586–0.881) | 0.001 | 0.761 (0.589–0.983) | 0.036 |
| Proton vs. 3D/IMRT | 1.036 (0.644–1.666) | 0.885 | ||
| RT dose scheme | ||||
| CF vs. HF/ultra-HF | 1.346 (1.104–1.641) | 0.003 | 0.773 (0.512–1.166) | 0.220 |
| HF vs. CF | 0.723 (0.585–0.893) | 0.003 | ||
| Ultra-HF vs. CF | 0.840 (0.585–1.205) | 0.343 | ||
| HF vs. ultra-HF | 0.861 (0.592–1.252) | 0.433 | ||
| Total dose, BED (Gy1.5) (continuous) | 0.993 (0.988–0.999) | 0.026 | ||
| BED ≥ 179 Gy1.5 vs. < 179 Gy1.5 | 0.701 (0.575–0.853) | <0.001 | 0.644 (0.441–0.939) | 0.022 |
| Subgroup | HR for BCFFS | 95% CI | p Value |
|---|---|---|---|
| All patients | 0.735 | 0.601–0.900 | 0.003 |
| NCCN low-risk group | 1.159 | 0.543–2.471 | 0.703 |
| NCCN intermediate-risk group | 0.650 | 0.423–1.000 | 0.048 |
| NCCN high-risk group | 0.731 | 0.553–0.966 | 0.028 |
| NCCN very-high-risk group | 0.712 | 0.441–1.152 | 0.167 |
| HR for BCF Rate | 95% CI | p Value | |
| All patients | 0.580 | 0.450–0.747 | <0.001 |
| NCCN low-risk group | 1.326 | 0.451–3.896 | 0.608 |
| NCCN intermediate-risk group | 0.432 | 0.246–0.761 | 0.004 |
| NCCN high-risk group | 0.634 | 0.449–0.895 | 0.010 |
| NCCN very-high-risk group | 0.432 | 0.234–0.797 | 0.007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, S.H.; Kim, Y.S.; Yu, J.; Nam, T.-K.; Kim, J.-S.; Jang, B.-S.; Kim, J.H.; Kim, Y.; Jeong, B.K.; Chang, A.R.; et al. Optimizing External Beam Radiotherapy as per the Risk Group of Localized Prostate Cancer: A Nationwide Multi-Institutional Study (KROG 18-15). Cancers 2021, 13, 2732. https://doi.org/10.3390/cancers13112732
Choi SH, Kim YS, Yu J, Nam T-K, Kim J-S, Jang B-S, Kim JH, Kim Y, Jeong BK, Chang AR, et al. Optimizing External Beam Radiotherapy as per the Risk Group of Localized Prostate Cancer: A Nationwide Multi-Institutional Study (KROG 18-15). Cancers. 2021; 13(11):2732. https://doi.org/10.3390/cancers13112732
Chicago/Turabian StyleChoi, Seo Hee, Young Seok Kim, Jesang Yu, Taek-Keun Nam, Jae-Sung Kim, Bum-Sup Jang, Jin Ho Kim, Youngkyong Kim, Bae Kwon Jeong, Ah Ram Chang, and et al. 2021. "Optimizing External Beam Radiotherapy as per the Risk Group of Localized Prostate Cancer: A Nationwide Multi-Institutional Study (KROG 18-15)" Cancers 13, no. 11: 2732. https://doi.org/10.3390/cancers13112732
APA StyleChoi, S. H., Kim, Y. S., Yu, J., Nam, T.-K., Kim, J.-S., Jang, B.-S., Kim, J. H., Kim, Y., Jeong, B. K., Chang, A. R., Park, Y.-H., Lee, S. U., Cho, K. H., Kim, J. H., Kim, H., Choi, Y., Kim, Y. J., Lee, D. S., Shin, Y. J., ... Cho, J. (2021). Optimizing External Beam Radiotherapy as per the Risk Group of Localized Prostate Cancer: A Nationwide Multi-Institutional Study (KROG 18-15). Cancers, 13(11), 2732. https://doi.org/10.3390/cancers13112732